expert panel on invasive cardiology
TRANSCRIPT

Final Report and Recomme
ndations
Expert Panel on Invasive Cardiology
in Ontario
Cardiac Care Network of Cardiac Care Network of Cardiac Care Network of Cardiac Care Network of
OntarioOntarioOntarioOntario
4211 Yonge Street, Suite 210 Toronto, Onta
rio M2P 2A9
Telephone: (416) 512-7472 Fax: (416
) 512-6425
e-mail: mail@ccn
.on.ca
Website: http://www
.ccn.on.ca
© Cardiac Care Network of Ont
ario, 2001
Submitted to the Ontario MinistrySubmitted to the Ontario MinistrySubmitted to the Ontario MinistrySubmitted to the Ontario Ministry
of Health of Health of Health of Health
and Long-Term Cand Long-Term Cand Long-Term Cand Long-Term C
areareareare
June 20June 20June 20June 20
01010101

Mission
We are an advisory body to the Ministry of Health and Long-Term Carethat is dedicated to improving quality, efficiency, access and equity in the
delivery of the continuum of adult cardiac services in Ontario.
Using data- and consensus-driven methods, we offer planning advice forthe future of cardiac services and the provision of exemplary care, in
collaboration with the Ministry and others.
VisionAs a dynamic partnership between professional providers, institutions,community members, and government, providing advice based on data
analysis and scientifically valid information, we will become an essentialresource in improving the delivery of adult cardiac care in Ontario.
Page i
Expert Panel on Invasive Cardiology in Ontario
TABLE OF CONTENTSEXECUTIVE SUMMARY ....................................................................................................... I
Section A: INTRODUCTION1. INTRODUCTION.............................................................................................................1
1.1 BACKGROUND TO THE EXPERT PANEL............................................................................................... 11.2 PANEL SCOPE........................................................................................................................................... 2
Section B: METHODOLOGY2. METHODOLOGY............................................................................................................3
2.1 LITERATURE REVIEW............................................................................................................................. 32.2 EXPERT OPINIONS................................................................................................................................... 32.3 OTHER RESEARCH .................................................................................................................................. 32.4 DECISION-MAKING FRAMEWORK........................................................................................................ 42.5 EXTERNAL REVIEW................................................................................................................................ 52.6 LEVELS OF EVIDENCE............................................................................................................................ 6
Section C: FINDINGS3. THE KNOWLEDGE BASE..............................................................................................7
3.1 THE CARDIAC CARE POLICY ENVIRONMENT .................................................................................... 73.2 THE CARDIAC CARE CLINICAL ENVIRONMENT ................................................................................ 83.3 OPERATOR STANDARDS ...................................................................................................................... 143.4 INSTITUTIONAL STANDARDS ............................................................................................................. 153.5 TRAINING PROGRAMS.......................................................................................................................... 163.6 PCI AND ON-SITE CARDIAC SURGERY............................................................................................... 17
4. CURRENT DELIVERY OF INVASIVE CARDIOLOGY SERVICES........................184.1 HUMAN RESOURCES ............................................................................................................................ 184.2 TRAINING FOR INVASIVE CARDIOLOGY........................................................................................... 194.3 CERTIFICATION, RECERTIFICATION, AND CREDENTIALLING....................................................... 204.4 QUALITY ASSURANCE ......................................................................................................................... 214.5 LOCATION OF CARDIAC CENTRES AND PROGRAMS ...................................................................... 214.6 DEMAND FOR SERVICES...................................................................................................................... 234.7 CAPACITY CONSIDERATIONS ............................................................................................................. 25
Section D: RECOMMENDATIONS
CONTEXT FOR THE RECOMMENDATIONS ..................................................................275. OPERATOR STANDARDS............................................................................................28
5.1 OPERATOR TRAINING........................................................................................................................... 285.2 MAINTENANCE OF COMPETENCE...................................................................................................... 35
6. INSTITUTIONAL STANDARDS ..................................................................................386.1 INFRASTRUCTURE REQUIREMENTS .................................................................................................. 386.2 QUALITY ASSURANCE ......................................................................................................................... 38
7. TRAINING ISSUES........................................................................................................417.1 TRAINING PROGRAMS.......................................................................................................................... 417.2 ACCREDITATION OF TRAINING PROGRAMS..................................................................................... 457.3 FUNDING OF TRAINING........................................................................................................................ 46
8. SUPPORTING INFRASTRUCTURE............................................................................478.1 EMERGENCY TRANSPORTATION........................................................................................................ 478.2 COMMUNICATION INFRASTRUCTURE............................................................................................... 478.3 RESEARCH.............................................................................................................................................. 48
9. LOCATION OF INTERVENTIONAL CARDIOLOGY SERVICES...........................499.1 EVALUATION CRITERIA AND PERSPECTIVE .................................................................................... 499.2 RATIONALE............................................................................................................................................ 49
GLOSSARY ................................................................................................................................................. 101
Page ii
Expert Panel on Invasive Cardiology in Ontario
LIST OF TABLESTable 1: Risks of Cardiac Catheterization and Coronary Angiography .........................................9Table 2: Self-reported Complication Rates for PCI, Four Full-Service Cardiac Centres in Ontario
(percent of cases)...............................................................................................................10Table 3: Same Day Mortality and CABG as percent of PCI procedures, Royal Alexandra Hospital
Site, Calendar years 1998 to 2000......................................................................................11Table 4: Minimum Training Requirements from Published Guidelines and Expert Opinion, Cath
and PCI, number of cases ..................................................................................................14Table 5: Minimum Operator Volumes in Published Guidelines and Expert Opinion, Cath and
PCI, procedures/year .........................................................................................................15Table 6: Minimum Institutional Volumes in Published Guidelines and Expert Opinion, Cath and
PCI, procedures/year .........................................................................................................15Table 7: Estimated Annual Operator Volumes, Cath and PCI, Ontario, 2000 ............................18Table 8: Number of Cardiac Service Centres in Ontario, January 2001 ......................................22Table 9: Procedural Volumes and Target Rates, 2000/01, Ontario..............................................23Table 10: Proposed Target Procedure Rates per 100,000 adult population, Cath and PCI, Ontario
..........................................................................................................................................23
LIST OF FIGURESFigure 1: Trends in PCI Volume and Same Day CABG, 1991 to 1998.......................................10Figure 2: Cath Volumes, Actual and Target, 1993/94 to 2005/06 ...............................................24Figure 3: PCI Volumes, Actual and Target, 1993/94 to 2005/06 ................................................24
LIST OF APPENDICESAppendix 1: TERMS OF REFERENCE....................................................................................55Appendix 2: CCN EXPERT PANEL ON INVASIVE CARDIOLOGY MEMBERSHIP ...........57Appendix 3: LITERATURE REVIEW......................................................................................58Appendix 4: PUBLISHED GUIDELINES FOR CATH AND PCI.............................................71Appendix 5: EXPERT OPINIONS AND ORGANIZATIONAL RESPONSES..........................73Appendix 6: COMMUNIQUE ANNOUNCING THE PANEL ..................................................74Appendix 7: STAKEHOLDER SUBMISSIONS .......................................................................75Appendix 8: SECONDARY REVIEW PANEL........................................................................76Appendix 9: CARDIAC CARE NETWORK COMMITTEE ....................................................77Appendix 10: CLINICAL SERVICES COMMITTEE MEMBERSHIP .....................................78Appendix 11: PUBLISHED OPERATOR GUIDELINES AND EXPERT OPINION - CATH...79Appendix 12: PUBLISHED OPERATOR GUIDELINES AND EXPERT OPINION - PCI .......80Appendix 13: PUBLISHED INSTITUTIONAL GUIDELINES AND EXPERT OPINION –
CATH AND PCI ...............................................................................................................81Appendix 14: PUBLISHED GUIDELINES AND EXPERT OPINION – QUALITY
ASSURANCE...................................................................................................................82Appendix 15: PUBLISHED GUIDELINES AND EXPERT OPINION – PCI WITHOUT ON-
SITE CARDIAC SURGERY.............................................................................................83Appendix 16: INVASIVE CARDIOLOGISTS BY CENTRE....................................................85Appendix 17: CAPACITY ANALYSIS....................................................................................87Appendix 18: CARDIAC SERVICE CENTRES IN ONTARIO ................................................95Appendix 19: CATH LABS IN ONTARIO ...............................................................................96Appendix 20: CANADIAN CARDIOVASCULAR SOCIETY STANDARDS..........................97
Page i
Expert Panel on Invasive Cardiology in Ontario
EXECUTIVE SUMMARYOver the past several years, the number of diagnostic and therapeutic invasive cardiologyprocedures1 has increased significantly in Ontario. This increase is attributable to many factorsincluding advances in the clinical efficacy of these procedures and demographic changes.
In late 2000, the Target Setting Working Group of the Cardiac Care Network of Ontario (CCN)proposed new population-based minimum target procedure rates for diagnostic catheterization(cath) and percutaneous coronary interventions (PCI). Combined with the aging of the populationand overall population growth, these new targets imply a substantial further increase in thenumber of invasive procedures in Ontario.
In its report, the Working Group noted that, even with the addition of new tertiary centres,achievement of the recommended targets might strain or exceed available capacity. Inacknowledgement of this challenge, the following recommendation was included in the WorkingGroup’s final report:2
“That CCN, under the auspices of its Clinical Services Committee, convene a group ofexperts to make recommendations about how best to achieve the new PCI targets whilemaintaining quality of care. Their report should include a discussion and broadguidelines related to operator and institutional requirements for PCI, and the qualityassurance process that must be put in place to monitor them. It should also include a fulldiscussion of various options to deal with potential under-capacity, including the optionof PCI in centres without surgical coverage.”
Based on the recommendation of the Working Group, as well as the submission of proposals toperform PCI at centres without on-site surgery, Ontario’s Ministry of Health and Long-Term Care(MOHLTC) requested that CCN study these issues in order to facilitate planning for invasivecardiac services over the next three to five years. In response to that request, CCN established anExpert Panel on Invasive Cardiology (the Panel) under the auspices of its Clinical ServicesCommittee.
The Panel’s mandate was to:• Develop recommendations regarding institutional, operator and infrastructure
requirements for the performance of cath and PCI procedures in Ontario.• Develop recommendations for the implementation of a quality assurance system for
invasive procedures in Ontario.
The foundation of the Panel’s work was a comprehensive review of published guidelines andscientific literature relating procedural outcomes to training, maintenance of competence, qualityassurance, and the presence or absence of on-site surgery. The findings of the literature reviewwere supplemented by unpublished data, by the solicited opinions of acknowledged experts inthis area, by submissions from stakeholders, and by a review of the current delivery of invasivecardiac care in Ontario.
Where existing guidelines from professional bodies (particularly from within Canada) were felt tobe relevant and appropriate, the Panel used such guidelines (e.g., the Canadian Cardiovascular
1 For ease of reference, both diagnostic and therapeutic procedures are referred to collectively as “invasivecardiology” in this report.2 Target Setting Working Group of the Cardiac Care Network of Ontario, Final Report andRecommendations, October, 2000.

Page ii
Expert Panel on Invasive Cardiology in Ontario
Society standards3) as the basis of its own recommendations. Existing guidelines were modifiedas necessary. The Panel’s recommendations are intended to establish or affirm minimumstandards. Individual operators and institutions are strongly encouraged to ensure that theminimums are exceeded.
OPERATOR STANDARDS
The Panel emphasized that the paramount consideration underlying standards of training andmaintenance of competence is to promote the safest and most effective treatment possible. Thefollowing assumptions guided discussion around the safety and efficacy of invasive procedures:
• Although complication rates have fallen in recent years, the overall practice of invasivecardiology (cath and/or PCI) is becoming more complex due to changes in demographicsand the use of these procedures in sicker and more elderly patients.
• The success of an invasive procedure is determined by multiple factors but remainshighly dependent on the skill and judgement of the operator.
Operator Training
All trainees (residents) in formal cardiology training programs receive at least basic instruction indiagnostic cath. Some residents will have met minimum cath training standards on completion ofresidency; others require additional training time beyond residency.
Cardiologists already in practice (or otherwise removed from residency training) who have notbeen performing independent cath procedures and now wish to do so require formal cath training,the duration and nature of which depends upon the time elapsed since completion of cardiologyresidency.
PCI procedures are substantially more complex and carry greater risk than cath procedures;therefore, the training standards for PCI are correspondingly more rigorous. PCI training mustinvolve immersion within a structured training program.
During cardiology residency, only limited if any “hands-on” exposure to PCI is obtained.Therefore, PCI training is currently provided in post-residency fellowship programs and generallyundertaken by new or recent graduates of cardiology residency programs. Cardiologists alreadyin practice who have been performing independent diagnostic cath may be able to train for PCIunder an abbreviated immersion program, combined with additional part-time training.
On completion of training for either cath or PCI, the newly trained invasive cardiologist requiresa period of close supervision and mentoring as he/she commences procedures on an independentbasis.
At present there is no financial support from MOHLTC for training in PCI, nor is there supportfor cath training that takes place outside of the cardiology residency program. The lack of suchsupport is a major barrier to meeting the physician resource needs of Ontario for invasive cardiacprocedures.
The Panel believes that the need for interventional cardiologists can be met if, and only if, there issufficient funding to support the training of enough new specialists to allow a net increase of five
3 Canadian Journal of Cardiology, May 1996. (See Appendix 20.)
Page iii
Expert Panel on Invasive Cardiology in Ontario
to seven per year over the next five years. In the absence of such support (and as pointed out byCCN last year4) “these shortages will become critical.”
Maintenance of Competence
A number of studies have demonstrated a consistent relationship between the number ofprocedures performed by an operator and the outcome of these procedures, particularly whenoutcome is defined by the rate of major complications. Procedure volume is acknowledged to bea surrogate measure for clinical and technical competence, and is best viewed as a necessary butnot sufficient condition for ensuring quality outcomes. In addition to minimum volumestandards, maintenance of competence must include participation in an on-going qualityassurance program that involves review of procedural safety and efficacy. Participation incontinuing medical education specific to the type of procedures being performed is also essential.
Care is not necessarily optimized by having a large number of operators attaining or justexceeding minimum volumes. Where feasible, it is desirable that invasive procedures beconcentrated among a relatively limited number of operators so that each operator performs manymore procedures than the minimum needed to maintain competence.
INSTITUTIONAL STANDARDS
The Panel felt that any invasive cardiology program requires a supporting infrastructure to enableit to perform to high standards of safety and efficacy. This infrastructure must include:
• A medical cath lab director responsible for training, credentialing and quality assurance.
• An annual review process of volumes and outcomes.
• Criteria for training and credentialing of physicians, nursing and technical staff.
• On-site cardiac surgery (or formal arrangement for off-site back up); and supportingclinical, administrative and facility infrastructure.
Each institution must have a quality assurance program that monitors both operator andinstitutional volumes and outcomes and reports those results to a central body for review andeventual dissemination.
The cath lab director (or invasive program director) assumes significant responsibilities related toquality assurance. Because of these responsibilities, the minimum experience for this role shouldbe higher than for an invasive cardiologist without this responsibility.
TRAINING ISSUES
Several existing guidelines indicate that training should take place within a formal structuredtraining program. The essential components of such programs were gleaned from the existingguidelines, as well as from solicited expert opinions, and also by way of analogy with the genericstructure of Royal College of Physicians and Surgeons of Canada (Royal College) specialtytraining programs.
There was a widely held belief that invasive procedures are becoming more, rather than less,complex due to their increasing use in patients with unstable conditions or multiple comorbidities.The Panel felt that this trend reaffirms the need for a formal structure around training for these
4 A Discussion Paper by the Consensus Panel on Cardiovascular Human Resources in Ontario, Final Reportand Recommendations, June 2000.

Page iv
Expert Panel on Invasive Cardiology in Ontario
procedures. Because such training is often outside the scope of a Royal College program, aprocess for external review of invasive training programs needs to be implemented.
Much is expected of the individuals and the institutions providing invasive training, in terms oftime and responsibility. The service being provided is an essential one, as trained invasivecardiologists are needed and there is no other mechanism to provide such training. A formalmechanism for funding the development of essential specialists is urgently needed.
SUPPORTING INFRASTRUCTURE
Ontario has developed a regionalized system for invasive cardiac services. Within such a system,a large number of hospitalized patients require transfer between institutions for urgent or semi-urgent invasive procedures. Adequate transportation and communication capabilities areessential components of a regionalized system of cardiac care, and must be adequately supported.At present, there are significant concerns that a lack of adequate ambulance services mayinterfere with the timely delivery of care and the optimal utilization of regionalized invasivefacilities.
LOCATION OF INTERVENTIONAL CARDIOLOGY SERVICES
A number of care providers and stakeholder groups have urged MOHLTC to fund PCI at centresthat do not currently have on-site cardiac surgery. While the Panel’s mandate did not encompassthe evaluation of specific proposals, it was asked to consider the safety and desirability of PCIwithout on-site cardiac surgery, within the context of various options to achieve the proposedtarget volumes while maintaining quality of care.
The Panel evaluated options based on the degree to which each could provide the desirableattributes of care: quality, timeliness, and proximity. Because MOHLTC indicated that economicefficiency would be evaluated in the course of assessing any specific proposal, this parameter wasnot considered by the Panel in a generic sense.
In considering the desirability of performing PCI without on-site surgery, the Panelacknowledged the following factors that would support this practice:
• The acute procedural risk of PCI, particularly the need for emergency bypass surgery, islower than it was prior to the widespread use of stents.
• The literature review (and the Panel’s experience) indicated that PCI is commonlyperformed without on-site cardiac surgery in some jurisdictions (e.g., Germany), and on amore limited scale in North America (including four sites in Canada).
The Panel also recognized that by not restricting PCI to surgical centres, patients could haveimproved access to interventional procedures. Performance of PCI at centres that are currentlystand alone cath centres enhances the opportunity to provide PCI immediately followingdiagnostic cath (ad hoc PCI) and direct or rescue PCI for acute myocardial infarction.
There were a number of issues of potential concern related to the establishment of PCI withouton-site surgery, including:
• The implications for the surgical centre(s) that would be providing off-site backup.
• The impact on case mix at surgical centres attributable to case selection at stand-alonesites.

Page v
Expert Panel on Invasive Cardiology in Ontario
• The value of regular interaction with cardiac surgeons even when emergency surgery isnot required.
• Unresolved problems regarding referral and transport of patients to a surgical centre in anemergency.
• The availability of a sufficient pool of trained personnel.
• Procedure volumes at proposed stand-alone sites and implications for existing sites.
Ultimately, the Panel felt that if a number of specific conditions were met, PCI without on-sitesurgery would be an acceptable option. These conditions would include:
• Documentation of need (e.g., to meet population-based targets, reduce waiting times oraddress geographic issues).
• A formal evaluation of alternatives.
• An expectation of sufficient volumes to support recommended operator and institutionalminimums.
• A minimum complement of experienced interventional cardiologists, nurses, andtechnical staff.
• A formal relationship with a full-service cardiac centre for ongoing consultation andemergency surgical backup.
• A formal relationship with the emergency transportation provider to ensure rapidtransport when required.
Given the uncertainties associated with the establishment of PCI without on-site surgery, thePanel felt that if and when this does take place, it should be on a limited scale (i.e., preferablyone, at most two centres). These pilot sites should be carefully evaluated before this practice isconsidered on a broader scale.
As new facilities are proposed and developed, the system-wide impacts must be assessed, giventhe limited supply of human and financial resources, and the impact of new centres on the referralpatterns and case mix of existing centres. While the establishment of PCI facilities outside ofsurgical centres is one option for meeting PCI target volumes, there are other approaches thatcould be implemented instead of, or in addition to, stand-alone PCI. These include furtherexpansion and/or longer hours (beyond what is currently planned or proposed) at existing centres,and enhancement of infrastructure to facilitate referrals between centres (i.e., communication,transportation).
The Panel was aware that some centres had expressed a desire to provide PCI for acutemyocardial infarction (i.e., primary and/or rescue PCI) in the absence of an elective PCI program.The potential role of emergency PCI as either initial therapy (instead of fibrinolytics), or as rescuetherapy (for failure of fibrinolytic therapy) in remote geographical settings was also raised.Several stakeholders expressed concern regarding the availability of direct and rescue PCI in thecase of patients with acute myocardial infarction (MI).
The Panel did not support emergency or rescue PCI at centres that do not provide an elective PCIservice. However, the Panel recommends that a co-ordinated regional approach be developed toaddress the need for emergency PCI for patients with acute MI with the eventual goal ofproviding these services on a 24/7 basis.

Page vi
Expert Panel on Invasive Cardiology in Ontario
A summary of the Panel’s recommendations follows. The full discussion and rationale for theserecommendations is presented in Section D of the body of the report. Readers are urged toreview the full text to fully appreciate the context for the recommendations.
RECOMMENDATIONS
Recommendation 1: That the Canadian Cardiovascular Society “Standards for Training inAdult Cardiac Catheterization and Angiography” and “Standards for Coronary AngioplastyTraining”5 be adopted (where applicable) by all institutions and programs in Ontarioperforming cath and PCI. Where recommendations in this report exceed minimumstandards in the CCS document, the recommendations herein should take precedence.
Recommendation 2: That physicians who have not previously performed independentdiagnostic catheterization and now wish to do so undergo training equivalent to thatrequired to attain Level 2 of the CCS Standards:
• If residency was completed more than 10 years earlier, then training should includethe attainment of Level 1 before proceeding on to Level 2; if residency wascompleted within the past 10 years, then attainment of Level 1 can be assumed,and training can immediately apply toward attainment of Level 2.
• If residency was completed within the past two years, and if Level 2 was attainedduring residency, then a lesser degree of training may be acceptable, to bedetermined by the cath lab director in consultation with the training programdirector where the residency training was done.
Recommendation 3: That physicians who previously performed diagnostic catheterizationindependently but have a period of absence of greater than one year from this activityundergo retraining as follows:
• If the period of absence was greater than 10 years, then training should include theattainment of Level 1 before proceeding to Level 2.
• If the period of absence was greater than two years, but less than 10 years, thentraining to achieve Level 2 of the CCS standards is required. Attainment ofLevel 1 can be assumed, and training can immediately apply towards attainment ofLevel 2.
• If the period of absence was less than two years, then the retraining should begoverned by the CCS standards on retraining6. The specific re-training programmust be agreed on with the Cath Lab Director.
5 Canadian Journal of Cardiology, May 1996.6 Canadian Journal of Cardiology, May 1996, p 471.
Page vii
Expert Panel on Invasive Cardiology in Ontario
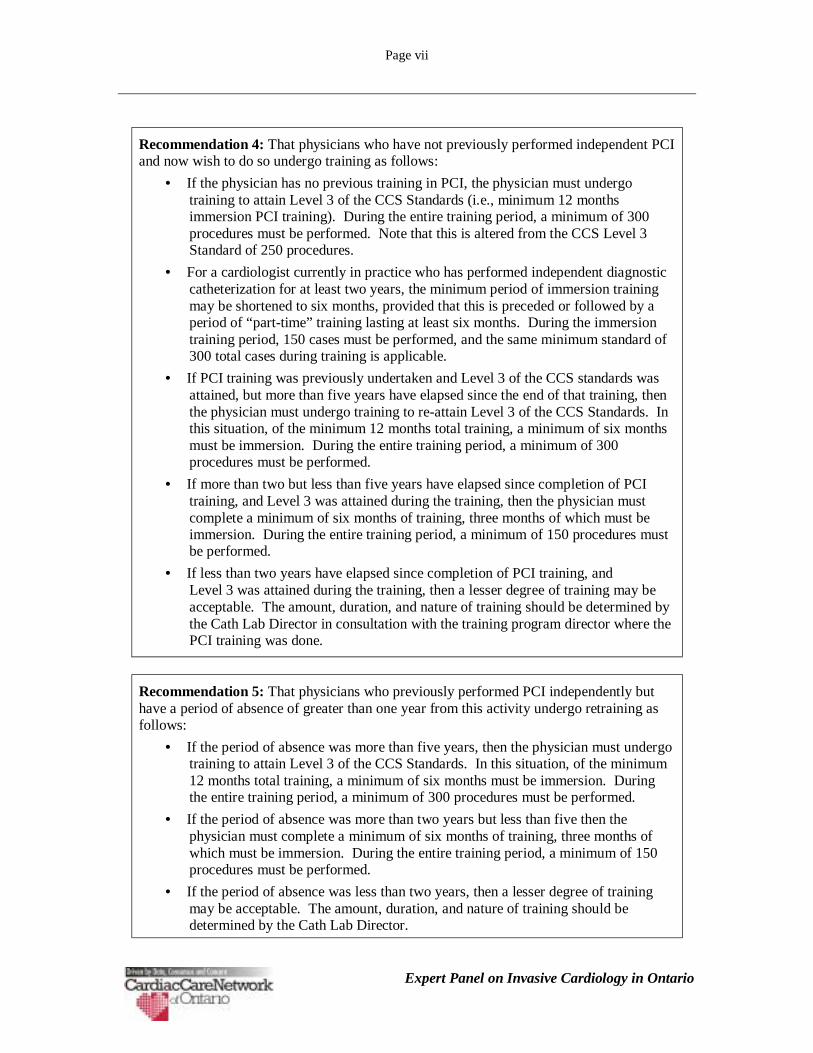
Recommendation 4: That physicians who have not previously performed independent PCIand now wish to do so undergo training as follows:
• If the physician has no previous training in PCI, the physician must undergotraining to attain Level 3 of the CCS Standards (i.e., minimum 12 monthsimmersion PCI training). During the entire training period, a minimum of 300procedures must be performed. Note that this is altered from the CCS Level 3Standard of 250 procedures.
• For a cardiologist currently in practice who has performed independent diagnosticcatheterization for at least two years, the minimum period of immersion trainingmay be shortened to six months, provided that this is preceded or followed by aperiod of “part-time” training lasting at least six months. During the immersiontraining period, 150 cases must be performed, and the same minimum standard of300 total cases during training is applicable.
• If PCI training was previously undertaken and Level 3 of the CCS standards wasattained, but more than five years have elapsed since the end of that training, thenthe physician must undergo training to re-attain Level 3 of the CCS Standards. Inthis situation, of the minimum 12 months total training, a minimum of six monthsmust be immersion. During the entire training period, a minimum of 300procedures must be performed.
• If more than two but less than five years have elapsed since completion of PCItraining, and Level 3 was attained during the training, then the physician mustcomplete a minimum of six months of training, three months of which must beimmersion. During the entire training period, a minimum of 150 procedures mustbe performed.
• If less than two years have elapsed since completion of PCI training, andLevel 3 was attained during the training, then a lesser degree of training may beacceptable. The amount, duration, and nature of training should be determined bythe Cath Lab Director in consultation with the training program director where thePCI training was done.
Recommendation 5: That physicians who previously performed PCI independently buthave a period of absence of greater than one year from this activity undergo retraining asfollows:
• If the period of absence was more than five years, then the physician must undergotraining to attain Level 3 of the CCS Standards. In this situation, of the minimum12 months total training, a minimum of six months must be immersion. Duringthe entire training period, a minimum of 300 procedures must be performed.
• If the period of absence was more than two years but less than five then thephysician must complete a minimum of six months of training, three months ofwhich must be immersion. During the entire training period, a minimum of 150procedures must be performed.
• If the period of absence was less than two years, then a lesser degree of trainingmay be acceptable. The amount, duration, and nature of training should bedetermined by the Cath Lab Director.

Page viii
Expert Panel on Invasive Cardiology in Ontario
Recommendation 6: That newly trained invasive and interventional cardiologists besupervised by an experienced operator and be subject to interim evaluations of competenceat three and six months. During this six month period, a cardiologist experienced in cath orPCI should be available on-site whenever the newly trained physician is performingprocedures.
Recommendation 7: That the Standards for Maintenance of Competence in CardiacCatheterization of the Canadian Cardiovascular Society7 be adopted as the minimumstandard (i.e., 150 procedures per year).
Recommendation 8: That the Standards for the Maintenance of Competence in CoronaryAngioplasty of the Canadian Cardiovascular Society8 be adopted as the minimum standard(i.e., 100 PCI procedures per year). For interventional cardiologists who perform some orall of their procedures at a centre without on-site cardiac surgery, the minimum standard is150 procedures/year.
Recommendation 9: That MOHLTC require all centres providing invasive cardiacservices to maintain an infrastructure that enables it to perform to high standards of safetyand efficacy, including:
• An annual review process to ensure that:o All operators achieve minimum procedure volumes.o The centre performs a minimum of 500 diagnostic cath procedures and
400 interventional procedures (where PCI is provided)
• Training and credentialing standards for physician, nursing and technical staff.The physician standards should, at a minimum, be consistent with therecommendations in this report.
• Sufficient number of operators performing PCI to ensure the availability of PCIservices 24 hours a day, seven days per week. Ideally, this would imply that therebe at least three PCI operators affiliated with the centre.
• Supporting clinical and facility infrastructure, including, for example, imagingfacilities, acute care beds, nursing coverage, and pharmacy.
• A medical cath lab director who is responsible for training, credentialling andquality assurance.
• An appropriate administrative structure.
• On-site cardiac surgery or formal arrangement for off-site surgical back up withdocumentation that safety is not compromised by this arrangement (SeeRecommendation 20.)
7 Canadian Journal of Cardiology, May 1996.8 Canadian Journal of Cardiology, May 1996.

Page ix
Expert Panel on Invasive Cardiology in Ontario
Recommendation 10: That the MOHLTC instruct all centres providing invasivecardiology services to demonstrate that the institution has a quality assurance program inplace to document that the standards for safety and efficacy are in fact met. Thefoundation of such a program will be the establishment and ongoing maintenance of adatabase to collect and analyze (at a minimum) the following data:
• Operator and cath lab volumes.• Demographic, clinical, and co-morbidity data.• Major complications (with standard definitions across all institutions, including
standardized protocol for peri-procedural enzyme evaluation):o Death, emergency surgeryo Peri-procedural MI, peri-procedural stroke.
All centres should have an internal process for review of appropriateness and quality ofdiagnostic angiograms under the direction of the Cath Lab Director. The review processshould include participation from an interventional cardiologist and cardiac surgeon, evenat stand-alone cath labs.
In the longer term, the database should be expanded to include effectiveness measures(again with standardized definitions) such as:
• TVR rate (repeat angioplasty or surgery)• Survival rate for AMI interventions• QOL, return to work, symptom and activity measures.
CCN should coordinate, through an existing working group, and with input fromappropriate professional organizations, standardized definitions and assessment protocolsfor the data elements mentioned above.
Recommendation 11: That the findings of each institution’s QA program be reported to acentral body for review and eventual dissemination, and that public accountability beestablished through this process. Further, that since the cath/PCI databases of CCN alreadycontain relevant data elements (e.g., demographics, co-morbidity), and given the precedentthat exists for cardiac surgery, that CCN serve as this central body. To enhance thevalidity of the overall QA process, periodic data validation, including audits against sourcerecords, should be undertaken in collaboration with an arms length body (e.g., ICES),similar to the current process for cardiac surgery.
Recommendation 12: That all training and retraining of physicians to perform cath andPCI take place within a structured training program with all of the requirements andsupporting infrastructure that is typically present in a Royal College program. Such aprogram would include, at a minimum:
• Standards regarding the qualifications of the training institution (e.g., training forthe trainers, volume and variety of cases, on-site surgery [to ensure exposure to afull range of patients and cases], academic activities such as rounds).
• A selection process that identifies which candidates be accepted for training.• Explicitly documented training goals and objectives. At least a core set of these
objectives should be common across all training programs.• A formal evaluation process.• An Education Committee that meets regularly to review the program, including a
designated Director of Training.• An external review process.

Page x
Expert Panel on Invasive Cardiology in Ontario
Recommendation 13: That MOHLTC encourage stakeholder groups, including the CCS,to approach the Royal College of Physicians and Surgeons with the goal of workingtogether to establish an accreditation process for invasive cardiology training programs,and to explore the feasibility of establishing a Royal College certificate of specialcompetence in Interventional Cardiology.
Recommendation 14: Until an accreditation process for invasive cardiology training hasbeen developed and implemented, as an interim measure each program offering invasivetraining outside the context of the Royal College cardiology residency should document inwriting the centre’s adherence to the training standards proposed in Recommendation 12.Furthermore, the Education Directors and/or Cath Lab Directors from each of these centresshould meet at least once per year to discuss issues of common interest and to review eachcentre’s adherence to the training standards.
Recommendation 15: That MOHLTC provide financial support for training in PCI. Thissupport should include reasonable salary support for trainees and funds to offset theadministrative and other costs of the training program itself, including the costs associatedwith external review and accreditation. To qualify for such support, the training programmust meet certain criteria as specified in Recommendation 12.
Recommendation 16: That MOHLTC ask CCN to convene a sub-committee withappropriate representation to assess in detail the costs associated with providing invasivetraining, in order that specific recommendations regarding the amount of support can beformulated. This assessment should include the costs associated with attaining a portion oftraining away from the trainee’s home institution.
Recommendation 17: That MOHLTC provide sufficient funding for a transportationinfrastructure that is capable of providing reliable and efficient service to allow optimalutilization of a regionalized system. Because this affects all invasive cardiac centres inOntario, as well as all referring physicians and institutions, MOHLTC should work withCCN to review this issue and coordinate a response. This work should begin immediately.
Recommendation 18: That MOHLTC coordinate and support the development of anelectronic network to permit rapid and secure transfer of digital angiographic images andother relevant clinical data in order to facilitate timely referral of patients between centres.
Recommendation 19: That research continue (and be updated) into the relationshipbetween institutional and operator characteristics (such as, but not limited to, procedurevolume) and outcomes of invasive cardiac procedures. Specifically, that such research beextended to encompass not only complications but also efficacy measures, such as, forexample, long term freedom from reintervention and symptom status.

Page xi
Expert Panel on Invasive Cardiology in Ontario
Recommendation 20: The weight of opinion clearly favours the availability of on-sitecardiac surgery in centres that perform angioplasty.
However, the Panel acknowledged that developments in angioplasty technology haveoccurred that may permit some flexibility in the organization of angioplasty services.
If the following criteria are met, then angioplasty without on-site cardiac surgery can beconsidered as an option and established on a pilot basis:
• There should be documentation of need, which may relate to population-basedtargets, excessive waiting times or geographic considerations. It is outside thisPanel’s scope to develop specific criteria of need.
• There should be a formal evaluation of alternatives to meet the identified need,such as increased capacity at nearby full-service centre(s) (if one exists), and/orenhanced transportation and communication infrastructure.
• Projected volumes must be sufficient to support at least the minimum operator andinstitutional volumes recommended for maintenance of competence.
• Sufficient human resources exist such that a new program can be staffed with asufficient number of providers (physicians, nurses, and technologists) who havemet all the necessary training requirements.
• New programs have at least a minimum complement of highly experiencedinterventional cardiologists, nurses, and technical staff.
• A formal relationship is established with a full-service cardiac centre to provideongoing consultation and emergency surgical backup.
• A formal relationship is established with the emergency transportation provider toensure the capability exists to transfer the patient and associated equipment in theevent of an emergency, and that the appropriate protocols are in place to ensurerapid transport within an established time frame.
Recommendation 21: That there be a formal assessment of the broader systems impacts(e.g., human resources, volumes, infrastructure) prior to the approval of any new cardiaccentre and significant expansion of services at an existing centre. This assessment shouldinclude the impact on existing programs and programs that are currently in development.The Panel recommends that the MOHLTC recognize the need to pace the development ofnew centres.
Recommendation 22: That emergency angioplasty for acute MI (direct or rescue PCI) notbe performed in a centre that does not have an established elective angioplasty program.
Recommendation 23: That MOHLTC request that CCN develop, either through adedicated Panel or an existing working group, a coordinated regional approach thatfacilitates the provision of emergency PCI services for patients with acute MI
The Panel also recommends that MOHLTC support the necessary infrastructure to provide,where appropriate, emergency PCI services to patients with acute MI with the eventualgoal of providing these services on a 24/7 basis.
MOHLTC should also support one or more pilot projects to evaluate the feasibility andeconomic impact of providing these services on a 24/7 basis.

Page 1
Expert Panel on Invasive Cardiology in Ontario
SECTION A: INTRODUCTION
1. INTRODUCTION
1.1 BACKGROUND TO THE EXPERT PANEL
Over the past several years, the number of diagnostic and therapeutic invasive cardiologyprocedures9 has increased significantly in Ontario. This increase is attributable to many factors.
In 1997, the Cardiac Care Network of Ontario (CCN) recommended that the rate of PCI inOntario be increased to achieve a ratio of PCI to coronary artery bypass surgery (CABG) of 1:1.10
The resulting target rate for PCI of 100 procedures per 100,000 adult population resulted in asignificant increase in the number of PCI procedures over the past few years.
In late 1999, the CCN established a Target Setting Working Group to reassess the currentprocedure rates for cath and PCI. The Working Group developed population-based minimumtarget procedure rates for these procedures (as well as coronary artery bypass surgery) in Ontarioand recommended to the Ministry of Health and Long-Term Care (the MOHLTC) that these ratesbe adopted for funding. Adoption of these targets, combined with the aging of the population andoverall population growth, would result in a substantial further increase in the number of cath andPCI procedures in Ontario.
In its report, the Working Group noted that, even with the addition of new tertiary centres,achievement of the recommended targets might strain or exceed available capacity. The cardiaccare system faces a challenge in balancing the need to accommodate increased volumes and thegoal of delivering care “as close to home as possible” with the fundamental principles of quality,timeliness, and efficiency. In acknowledgement of this challenge, the following recommendationwas included in the Working Group’s final report:11
“That CCN, under the auspices of its Clinical Services Committee, convene a group ofexperts to make recommendations about how best to achieve the new PCI targets whilemaintaining quality of care. Their report should include a discussion and broadguidelines related to operator and institutional requirements for PCI, and the qualityassurance process that must be put in place to monitor them. It should also include a fulldiscussion of various options to deal with potential under-capacity, including the optionof PCI in centres without surgical coverage.”
To accommodate the growth in procedures, additional invasive facilities have been (or are in theprocess of being) developed, some as part of full-service tertiary cardiac programs (with surgery),
9 Diagnostic catheterization is hereafter referred to as “cath.” Percutaneous coronary intervention, whichincludes percutaneous transluminal coronary angioplasty (PTCA) is hereafter referred to as “PCI.” Thisencompasses coronary stenting (currently performed in approximately 90% of all angioplasty cases inOntario) and various other techniques and modalities such as atherectomy and thrombectomy that may beperformed alone or (more often) in conjunction with coronary stenting. For ease of reference, bothdiagnostic and therapeutic procedures are referred to collectively as “invasive cardiology.” Relevant termsare defined in a Glossary at the end of this report.10 CCN Expert Panel on Intracoronary Stents, Final Recommendations, January 199711 Target Setting Working Group of the Cardiac Care Network of Ontario, Final Report andRecommendations, October, 2000
Page 2
Expert Panel on Invasive Cardiology in Ontario
and others as stand alone cath labs. Additional proposals have been made to the MOHLTC toexpand services at existing centres, including proposals to perform PCI at centres without on-sitecardiac surgery.
It is generally appreciated that in planning the delivery of complex services such as cath and PCI,minimum institutional and operator volumes are important for the attainment and maintenance ofhigh quality and efficient care. This concept necessitates trade-offs against the desire to delivercare as close to home as possible.
The development of new facilities (or the provision of new services in existing facilities) issignificantly influenced by human resource issues. Such issues encompass concerns around thegeneral shortage of medical personnel (physicians, nurses, and technologists), as well as specificconcerns regarding the availability of cardiologists with sufficient training and experience ininvasive procedures.
Based on the recommendation of the Target Setting Working Group, MOHLTC requested thatCCN study these issues in order to facilitate planning for invasive cardiac services over the nextthree to five years. In response to that request, CCN established an Expert Panel on InvasiveCardiology (the Panel) under the auspices of its Clinical Services Committee.
1.2 PANEL SCOPE
The Panel’s mandate was to:
• Conduct a literature review of existing guidelines for diagnostic and therapeuticcatheterization procedures, and of literature relating outcomes to operator and institutiontraining and volumes.
• Review existing literature regarding the performance of coronary angioplasty in centreswithout on-site surgical back up and elicit expert opinion to supplement availableliterature on this issue.
• Develop recommendations regarding institutional, operator and infrastructurerequirements for the performance of diagnostic catheterization and PCI procedures inOntario.
• Develop recommendations for the implementation of a quality assurance system forinvasive procedures in Ontario.
Although it was outside the Panel’s scope to make recommendations regarding specific sites, itwas within its scope to recommend criteria for evaluating locations for invasive cardiologyservices. The Panel was advised by the MOHLTC representative not to consider issues ofeconomic efficiency in its deliberations, as the MOHLTC would conduct its own economicevaluation of any proposed program development or expansion.
The Terms of Reference for the Expert Panel are provided in Appendix 1. The Panel’smembership is listed in Appendix 2.

Page 3
Expert Panel on Invasive Cardiology in Ontario
SECTION B: METHODOLOGY
2. METHODOLOGY
2.1 LITERATURE REVIEW
The first step in gathering information on the issues of interest to the Panel was the conduct of aliterature review. The scope of this review included:
• Existing policies, initiatives and guidelines for training, maintenance of competency,credentialing and quality assurance for cath and PCI.
• Data and literature on the validity of various outcome measures for cath and PCI.
• Data and literature for cath and PCI on the relationship between outcomes and volume,training, quality assurance initiatives, and hospital setting.
• Existing data and literature on outcomes of PCI according to the presence or absence ofon-site cardiac surgery and the necessary infrastructure to support PCI without on-sitesurgery.
The literature review was conducted by Dr. Curry Grant at the Institute for Clinical EvaluativeSciences (ICES). The review included searches on PREMEDLINE, MEDLINE, EMBASE,Healthstar, and other relevant websites for the above noted areas of research. The full report fromDr. Grant is provided in Appendix 3. A list of the published guidelines that were identified by theliterature review is provided in Appendix 4.
2.2 EXPERT OPINIONS
The Panel anticipated that there would be limited published literature on some of the topics ofinterest. To supplement published sources, the Panel contacted cardiologists within and outsideof Canada who are acknowledged subject matter experts. The Panel also contacted organizationsthat might have direct practical experience, opinions and/or policies of relevance to this work.The experts and organizations contacted are listed in Appendix 5.
2.3 OTHER RESEARCH
In addition to the formal literature review, the Panel also identified sources of unpublished data,reviewed submissions from interested stakeholders, and reviewed the existing organization ofinvasive cardiology in Ontario.
2.3.1 Unpublished Data
At the first meeting of the Panel, members found that the published literature on the outcomes ofcath and PCI was dated and did not reflect current experience at existing centres in Ontario.Thus, the research was expanded to include unpublished data on provincial, national andinternational experience in areas of interest to this Panel, including the review of PCI programswithout on-site cardiac surgery both in and outside of Canada.
Page 4
Expert Panel on Invasive Cardiology in Ontario
2.3.2 Stakeholder Submissions
As part of the launch of this work, the Panel issued a communiqué notifying health careorganizations in Ontario and other relevant stakeholders that it would review any relevant writteninformation submitted by these organizations. A copy of the communiqué about the Panel isprovided as Appendix 6. In response to this communiqué, twelve organizations (includinghospitals, professional associations, individual cardiologists, a district health council and acommunity group) made submissions to the Panel, as listed in Appendix 7. Each submission wasdistributed to and discussed by the Panel.
Although the Panel did not invite oral presentations, one group was granted the opportunity tomake a presentation and discuss its implications directly with the Panel.
2.3.3 Current Organization of Resources
To provide a context for the deliberations and recommendations, the Panel conducted a review ofthe current organization of invasive cardiology care in Ontario. This review included thefollowing components:
• Existing, approved and proposed facilities.
• Types and volumes of procedures that are currently performed, including recent trends inprocedure volumes and expansions in capacity.
• Projected procedure volumes for the next five years.
• The physician resources (cardiologists) currently performing these procedures as well asthose in training.
• The existing approach to training and credentialing for invasive cardiology.
• Existing quality standards and outcome measures.
Projections on procedure volumes and capacity were based on the work of the CCN TargetSetting Working Group and on updated surveys carried out by CCN.
2.4 DECISION-MAKING FRAMEWORK
The Panel was asked to conduct its deliberations and produce a final report within four months.Four meetings were held between the beginning of January and the end of February 2001. Thefirst meeting was organizational and focussed on a preliminary literature review and identifyingadditional information that would be needed to assist Panel members in reaching a consensus andagreeing on a process. Three additional meetings and one teleconference were held to reviewrelevant data and literature, and to develop the recommendations.
2.4.1 Reaching Consensus
In advance of its deliberations, the Panel members agreed on the following process fordeveloping recommendations. It was clearly preferred and hoped that a consensus could bereached on all issues, leading to a series of consensus recommendations. The Panel agreed inadvance that, should consensus not be possible, it was still important that the Panel providerecommendations, even on difficult or controversial issues.
Therefore, if consensus were not reached, the Panel’s recommendation on a specific issue wouldbe based on a majority opinion. However, the opportunity to present, in the report itself, a

Page 5
Expert Panel on Invasive Cardiology in Ontario
minority or dissenting recommendation, was to be provided. The Panel also reserved the right todecide to provide no recommendation on certain issues that were not fundamental to its mandate.
2.4.2 Context for Deliberations
In developing recommendations, the Panel considered several dimensions relevant to theorganization and provision of invasive cardiac care:
• The perspective from which various stakeholders view the care system (e.g., as viewedby patient, provider or administrator; as it affects individual institution, region or system)and the potentially differing values that underlie stakeholders’ beliefs and opinions.
• The desirable attributes of care (e.g., quality of outcomes, timeliness, close to home)and the need to establish priorities for these attributes when they cannot besimultaneously achieved.
• The extent to which the need for re-organization of care (such as PCI without on-sitecardiac surgery) should be demonstrated, and the extent to which alternative means ofachieving similar care goals should be considered and evaluated.
2.4.3 Ethical Perspective
The Panel recognized explicitly that some of its key decisions, such as the environment in whichPCI services should be provided, involved consideration of the tradeoffs inherent in the prioritiesof the various attributes of care (as listed above). Clearly there may be differing values thatinfluence decisions. For example, some people may be willing to trade-off small differences inprocedural risk for the ability to receive care sooner or closer to home; whereas for others, anypotential difference in outcome, no matter how small, may justify waiting or travelling a longdistance for care.
Some of the recommendations in this report, if implemented, may affect patients’ decisions aboutwhat type of care to receive and where. The Panel assumed that, as a part of the consent process,patients will be provided with the information necessary to allow them to participate in thisdecision-making process.
While it was beyond the scope of the Panel to reach specific conclusions about quantifying suchtradeoffs, it was felt important to explicitly recognize the nature of this decision-making process.Furthermore, the Panel felt that because individual values play such a potentially important rolein establishing these tradeoffs, public input would be both important and useful to help guidefuture decisions in this area. Dr. Peter Singer12 provided advice to the Panel on this issue, andsuggested that a “citizen’s jury” might be an effective means of informing future policy decisions.
2.5 EXTERNAL REVIEW
A secondary panel of individuals or organizations representing constituencies with relatedexpertise and interest in the issues addressed by the Expert Panel was invited to review the draftreport. Physicians who had responded to the Panel’s original solicitation of expert opinion werealso invited to review the draft report. A list of the members of the secondary panel is providedin Appendix 8.
12 Dr. Singer is the Director, Centre for Bioethics, University of Toronto.

Page 6
Expert Panel on Invasive Cardiology in Ontario
The draft recommendations were presented to a full meeting of the CCN Committee.Subsequently, a draft version of the entire report was submitted to the CCN Executive Committeeand the Clinical Services Committee at the same time that it was sent to the Secondary ReviewPanel. The membership of the CCN Committee and CCN’s Clinical Services Committee areprovided in Appendix 9 and 10 respectively.
2.6 LEVELS OF EVIDENCE
In making recommendations, the Panel evaluated published scientific literature, guidelinestatements, and expert opinion. Standard grading systems for levels of evidence have beenemployed by most of the CCN consensus and expert panels that preceded this one. Gradingsystems have also been developed for the evaluation of guideline and consensus statements. ThisPanel did not subject guideline publications from other organizations to a formal grading process,but did consider their temporality and relevance to current practice in Ontario, as well as thestature and constituency of the organization that developed each set of guidelines.
The preamble that accompanies each recommendation describes the evidence that wasconsidered, the Panel’s interpretation of such evidence, and the weighting given to the variouspieces of supporting evidence. In situations where the Panel relied primarily on expert opinionfrom multiple sources, the degree of concordance among the opinions was taken into account.

Page 7
Expert Panel on Invasive Cardiology in Ontario
SECTION C: FINDINGS
3. THE KNOWLEDGE BASEThis chapter presents the findings of the Panel’s research, and analysis of those findings. Sourcesof information for the material in this chapter include the literature review, expert opinion,stakeholder submissions, and the experience and knowledge of the Panel members. Full detailsof the scope and findings of the literature review are provided in Appendix 3.
3.1 THE CARDIAC CARE POLICY ENVIRONMENT
The overriding context for the planning of healthcare services in Ontario is the policyenvironment that drives the MOHLTC’s decisions around resource allocation. In deliveringhealthcare in Ontario, the MOHLTC has articulated the following vision in its 2000-2001Business Plan:
An accessible health system that promotes wellness and improves people’shealth at every stage of their lives and as close to their homes as possible.
The MOHLTC also states that it is:
“committed to ensuring that all Ontarians have access to modern technologiesand treatments. Our vision also encourages all health care professionals andinstitutions to work together to ensure accountability to the patient and thesystem.”
Expanding on the MOHLTC’s vision, the Panel developed the following principles to guide itswork:
• Quality of outcomes. The safety and effectiveness of care has a high priority in planningdecisions.
• Timeliness of service delivery. The burden on the patient and his or her family ofinappropriate wait times for services is well recognized.
• Care delivered “as close to home as possible.” The need to travel long distances for careimposes a further burden on the patient and his or her family. While complex serviceshave traditionally been delivered at regional centres, population growth and increasedvolume may make it practical to deliver such services closer to home.
• Efficiency. It is imperative that health care resources be deployed as efficiently and cost-effectively as possible.
The need for cardiac services in general and invasive services in particular has grownsignificantly over the past several years, due in part to the aging of our population and in part to

Page 8
Expert Panel on Invasive Cardiology in Ontario
the rapid development of new and effective therapies. In response to this increasing need,substantial increases in the targeted minimum procedure rates have been recommended.13
It will be a challenge to meet this need while also striving to simultaneously satisfy all fourprinciples. Because it is not possible to optimize all of the competing priorities at the same time,certain trade-offs are inevitable.
3.2 THE CARDIAC CARE CLINICAL ENVIRONMENT
3.2.1 Contemporary Procedure Outcomes
3.2.1.1 Diagnostic Cath
Diagnostic catheterization is used most often for the evaluation of patients with known orsuspected coronary artery disease (CAD). Other less frequent indications include the evaluationof valvular heart disease and cardiomyopathy. When used in the setting of CAD, the purpose ofdiagnostic catheterization may be to establish or refute the diagnosis of CAD. However, moreoften it is used to determine the extent and severity of coronary obstructions, to help defineprognosis, and, importantly, to establish a therapeutic plan by determining the suitability forrevascularization via PCI or CABG.
The successful outcome of a diagnostic cath procedure is defined by the acquisition of sufficientinformation about coronary anatomy (and often ventricular structure and function) to allowdetailed planning of subsequent treatment, without the occurrence of any complications. Inpractice, while there have been studies of the accuracy and reproducibility of specific aspects ofangiogram interpretation, there are no validated or broadly applicable measures of overalldiagnostic quality. For purposes of quality assurance, therefore, the outcome of diagnostic cathhas been defined primarily by the rate of major and minor complications arising from theprocedure.
Because serious complications of diagnostic cath (e.g., myocardial infarction, stroke, and death)are rare in the overall cath population, a large dataset is needed to define the rates of specificcomplications with reasonable accuracy and precision. The Society for Cardiac Angiography andIntervention (SCAI) has maintained such a database on a voluntary basis. The most recentpublication from this database reports the complication rates presented in Table 1.
13 Target Setting Working Group of the Cardiac Care Network of Ontario, Final Report andRecommendations, October, 2000

Page 9
Expert Panel on Invasive Cardiology in Ontario
Table 1: Risks of Cardiac Catheterization and Coronary Angiography(No. of Patients = 59,792)14
%Mortality 0.11Myocardial infarction 0.05Cerebrovascular accident 0.07Arrhythmia 0.38Vascular complications 0.43Contrast reaction 0.37Hemodynamic complications 0.26Perforation of heart chamber 0.03 Other complications 0.28Total of major complications 1.70
As with other procedures, the total number of serious complications is made up of those that are,to a degree, predictable (based on the underlying characteristics of the patient or the clinicalscenario), and those that arise unexpectedly. The former category would, for example, include astroke that occurred in a very elderly patient with severe generalized vasculopathy, or proceduraldeath in a patient who arrives at the cath lab in cardiogenic shock. The latter category mightinclude a patient with a catheter-induced coronary dissection, or a severe contrast media reactionin the absence of risk factors.
In recent years there has been a trend to perform diagnostic cath on patients who are older, moreunstable, and with more comorbidity. Whether this gradual change in the patient population hasaffected procedural complication rates is not clear.
3.2.1.2 PCI
As for diagnostic cath, clinical outcome for PCI in terms of quality assurance has been definedprimarily by the rate of major complications (death and emergency bypass surgery), rather thanby the effectiveness of the procedure (which would include, for example, relief of symptoms,absence of restenosis and avoidance of the need for surgical revascularization). A reduction overtime in the frequency of these major complications is noted for PCI in several articles, despitetrends over the same time period to intervene on patients who are less stable or have more co-morbidity.
Although all of the studies addressing complication rates of PCI were published since the mid1990s, the Panel felt that they did not necessarily reflect the current reality. Two countervailingtrends were identified that may influence contemporary outcomes:
• One trend was the reduction in death and emergency bypass surgery, the latter largelyrelated to the introduction of coronary stents.
• The other trend was the increased acuity, age, and co-morbidity of patients undergoingcath or PCI, coupled with the development of adjunctive devices and pharmacology,resulting in an overall increase in the complexity of PCI.15
14 Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, et al. ACC/AHA guidelines forcoronary angiography. A report of the American College of Cardiology/American Heart Association TaskForce on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with theSociety for Cardiac Angiography and Interventions. J Am Coll Cardiol 1999; 33: p1760, Modified withpermission from Noto et al.

Page 10
Expert Panel on Invasive Cardiology in Ontario
To place the current Ontario situation in context, ICES prepared an analysis of PCI procedurevolumes and the rate of same day CABG for the period 1991 to 1998. These data were providedby ICES and based on Canadian Institute for Health Information (CIHI) data. As shown inFigure 1 below, PCI procedure volumes almost doubled in the eight-year period (from 3,700procedures to 7,100), while the rate of same day CABG fell from 1.8% in 1991 to 0.43% of totalPCI volume in 1998.
Figure 1: Trends in PCI Volume and Same Day CABG, 1991 to 1998
To gain a better understanding of current complication rates, the Panel asked CCN memberhospitals to provide data on the incidence of major PCI complications. The results of this surveyare summarized in Table 2 below.
Table 2: Self-reported Complication Rates for PCI, Four Full-Service Cardiac Centres inOntario (percent of cases)
Centre Period EmergencyCABG
CABGduring same
admissionMyocardialInfarction
Deathwithin sameadmission
Centre A Calendar 2000 0.67 N/A N/A N/A
Centre B Fiscal 1998/99 0.00 0.00 0.00 N/A
Centre B Fiscal 1999/00 0.33 0.33 0.00 0.33
Centre C Calendar 2000 0.19 0.45 0.51 0.32
Centre D Calendar 2000 0.25 0.41 0.16 N/A
Source: Self-reported from CCN member tertiary cardiac centres, based on non-standardizeddefinitions of emergency CABG and myocardial infarction, in response to Panel’s request.
The complication rates shown in the table should be interpreted with some caution. For example,not all centres use the same definition of emergency CABG. Further, the incidence of peri-procedural MI is influenced by the intensity of post-procedure monitoring of cardiac enzymes; 15 Ho V, Evolution of the volume-outcome relation for hospitals performing coronary angioplasty,Circulation 2000; 101:1806-1811; Rill V, Brown DL, Practice of Coronary Angioplasty in California in1995, Circulation 1999;99:E12; and Rogers WJ et al, Temporal trends in the treatment of over 1.5 millionpatients with myocardial infarction in the U.S. from 1990 through 1999, JACC 2000;36(7):2056-63.
0.00
0.50
1.00
1.50
2.00
2.50
91 92 93 94 95 96 97 9801,0002,0003,0004,0005,0006,0007,0008,000
Same Day CABG %PTCA Volume

Page 11
Expert Panel on Invasive Cardiology in Ontario
most centres do not routinely monitor enzymes outside the setting of a clinical trial. (Incontemporary clinical trials, the incidence of peri-procedural MI is generally 3-6%).
To capture the most contemporary data on emergency bypass surgery as a complication of PCI,the CCN Cardiaccess database was queried for all cases in which a patient had PCI and CABG onthe same day. (In most, but not all cases, this situation represents emergency surgery after failedPCI). Based on 4,739 cases from June 2000 to December 2000 inclusive, the rate of same dayCABG and PCI in Ontario was found to be 0.51%, or approximately one in every 200 PCI cases.The values for individual centres ranged from 0.28% to 1.06%.
These outcomes are comparable to the recent experience reported by the Royal AlexandraHospital, one of the sites in Canada that provides PCI without on-site surgery. The mortality andemergency CABG rates are shown in Table 3 (again, definitions are non-standardized).
Table 3: Same Day Mortality and CABG as percent of PCI procedures, Royal AlexandraHospital Site, Calendar years 1998 to 200016
1998 1999 2000Number of PTCAs 544 785 1,204Death17 (%) 1.3 0.4 0.6CABG 0.2 0.1 0.2
It was pointed out in one expert submission and by Panel members that the nature of the PCIcomplications that necessitate emergency surgery has changed since the introduction of coronarystents and glycoprotein (GP) IIb/IIIa inhibitors. In the past, bailout surgery was most oftenrequired for acute vessel closure resulting from extensive dissection and/or thrombosis of thetarget coronary artery. While stents and GP IIb/IIIa inhibitors are generally effective atpreventing or treating acute vessel closure, they may contribute to other rare but seriouscomplications that potentially require immediate surgical treatment, such as coronary perforationwith resultant tamponade, stent dislodgement, and aortic dissection.
Overall, the Panel felt that there was sufficient data to support the widely held belief that the needfor emergency bypass surgery has become an infrequent complication of PCI in recent years.
3.2.2 Important trends in invasive cardiology
Although the Panel did not undertake a comprehensive review of all the factors influencing thecontemporary practice of invasive cardiology, a number of themes surfaced repeatedly, either insubmissions to the Panel, or in the Panel’s own discussions. Because these themes were felt to berelevant to the planning and delivery of invasive cardiology services, and because they influencedseveral of the Panel’s recommendations, they are discussed in the following sub-sections infurther detail.
3.2.2.1 Increased use of diagnostic catheterization and PCI
Over the past decade there has been a steady increase in the age-adjusted utilization rate for bothdiagnostic catheterization and PCI. While some of this increase may relate to improved access,there has been a clear trend to refer patients for cath earlier in the course of their disease, with lessstringent symptom and non-invasive criteria. This in turn has been driven by enhanced
16 From the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH)database. Used with permission.17 Includes cardiogenic shock patients.

Page 12
Expert Panel on Invasive Cardiology in Ontario
capabilities in both PCI and cardiac surgery, and the ensuing perception that a broader spectrumof patients is likely to benefit from revascularization. Recent clinical trials18,19 have shown betteroutcomes among patients with an acute coronary syndrome (unstable angina or non-ST elevationMI) who undergo routine early catheterization followed by revascularization when feasible, ascompared to the more traditional strategy of reserving catheterization for those who haverecurrence of symptoms or evidence of residual ischemia. While some controversy still existsregarding aggressive versus conservative management, many cardiologists and/or institutionshave already modified their practice in keeping with these research findings. However, aspractice patterns evolve more broadly, there is likely to be a further increase in the use ofdiagnostic cath and PCI, particularly in the acute setting.
The Target Setting Working Group recommendations for an increase in the age-adjustedpopulation-based rates of cath and PCI already incorporated many of the factors listed. However,some of the evidence cited above, in particular the TIMI-18 / TACTICS trial addressing the roleof a routine invasive strategy in acute coronary syndrome, was not yet available at the time of theWorking Group’s deliberations.
3.2.2.2 Diagnostic cath followed by immediate PCI: Ad hoc PCI
Traditionally, PCI was performed as a distinct procedure, during a separate cath lab session fromthe diagnostic cath procedure that defined the coronary anatomy. This was necessary for avariety of reasons:
• Since there was no digital playback system, review of the diagnostic images (and hencedetermination of suitability for PCI) had to await processing of cine-angiographic film.
• Acceptance for PCI often required prior review by a cardiac surgeon.
• The more frequent need for emergency surgery necessitated scheduling in co-ordinationwith the cardiac operating room (OR).
Today, high quality digital images provide immediate diagnostic quality information during thecath procedure; review by a cardiac surgeon is generally limited to complex or high-risk cases,and cath labs rarely if ever require a cardiac OR on standby before proceeding with PCI.Therefore, there is much greater flexibility today around the scheduling of PCI procedures.Furthermore, a much greater proportion of patients undergoing diagnostic cath are in an unstablephase of their disease, and any delay between cath and revascularization carries a greater risk ofinterim events for such patients. For these reasons, there is an increasing trend to perform “adhoc” PCI (also known as same sitting, plus-minus, or double set-up PCI). In 2000/01, 34% ofPCI procedures were performed as ad hoc procedures, compared to only 25% in 1999/00.
Ad hoc PCI is popular with patients, since it is generally more convenient and quicker thanhaving to return on a separate occasion, and avoids the discomfort and potential risk of anotheraccess site puncture. It also can be (but is not always, see below) an efficient use of cath lab time,since diagnostic cath and PCI accomplished at the same session take less time than at twoseparate sessions.
18 Cannon CP et al. Oral Presentation at AHA Scientific Session, November 2000 and Cannon C.TACTICS (Treat Angina with Aggrastat + Determine Cost of Therapy with an Invasive or ConservativeStrategy)-TIMI 18 Clin Cardiol 2001;24(1)86 (Study Design).19 Wallentin L, Lagerqvist B, Husted S, Kontny F, Stahle E, Swahn E Outcome at one year after an invasivecompared with a non-invasive strategy in unstable coronary-artery disease: the FRISC II invasiverandomised trial. FRISC II Investigators. Fast Revascularisation during Instability in Coronary arterydisease. Lancet 2000; 356(9223):9-16

Page 13
Expert Panel on Invasive Cardiology in Ontario
There are circumstances in which PCI should not be performed on an ad hoc basis, particularlywhen the need for or appropriateness of PCI is uncertain. For example, in a patient who is notcurrently unstable, the finding of a single lesion of borderline severity, or the finding ofmultivessel disease with several highly complex lesions, may prompt further assessment orsurgical consultation respectively prior to undertaking PCI. There is also the potential to forcecancellation of other scheduled cases if several diagnostic caths proceed to same sitting PCI on agiven day; for this reason many centres limit the proportion of PCI cases done on an ad hoc basis.The use of ad hoc PCI is more likely to enhance rather than reduce efficiency in a facility that hasseveral cath suites, with the flexibility to shuffle cases between rooms.
3.2.2.3 PCI in the management of acute myocardial infarction
Complete thrombotic occlusion of an epicardial coronary artery is the cause of at least 90% ofcases of acute myocardial infarction (MI) associated with ST-segment elevation on theelectrocardiogram (ST-elevation MI). The cornerstone of therapy for this life-threateningemergency is the restoration of coronary blood flow (reperfusion). This can be accomplishedpharmacologically using fibrinolytic (clot dissolving) drugs, or mechanically by performing PCIat the site of the acute occlusion.
Several randomized clinical trials over the past decade have demonstrated that immediate (ordirect) PCI is superior to fibrinolytic therapy for the treatment of ST-elevation MI. However, innon-randomized registries that attempt to define outcomes in routine practice rather than withinhighly selected clinical trials, the benefits of direct PCI have not been as dramatic or consistent.The experience and expertise of the centre and operator performing direct PCI have been cited asimportant factors influencing outcome; the relative merits of direct PCI and fibrinolytic therapythus depend, at least in part, on the practice environment. Patients with ST-elevation MI who canbe treated promptly in a centre that regularly performs a large number of both elective andurgent/emergent PCI cases should undergo direct PCI; otherwise they should receive afibrinolytic drug (unless contraindicated), with subsequent consideration of transfer to a PCIcentre.
Research is ongoing into the use of combination treatment, or “facilitated reperfusion.” Shouldearly results be confirmed in large scale trials, the role of PCI in the treatment of ST-elevation MImay be considerably expanded. For example, a patient with ST-elevation MI without immediateaccess to a PCI-capable cath lab might be treated with a reduced dose of a fibrinolytic drugtogether with a GP IIb/IIIa inhibitor, then transferred as soon as possible to an interventionalcentre where diagnostic cath and possible PCI would be performed. The drug combination maybe more effective at restoring coronary blood flow than the fibrinolytic drug alone, and unlike fulldose fibrinolytic therapy used alone, the combination does not appear to increase the risksassociated with a PCI procedure performed within the ensuing several hours. Conversely, in asituation in which a cath lab is immediately or very promptly available, a patient with ST-elevation MI might receive the GP IIb/IIIa inhibitor as soon as (and in whatever location) thediagnosis is established, followed by immediate cath and PCI.
Since cath and PCI are already used in a significant proportion of acute MI patients (albeit later inthe index hospitalization or after discharge), not all patients treated as outlined above represent“new” demand. However, an expanded role for PCI in the acute phase of MI would alter thetiming of the existing demand from semi-urgent or urgent to emergent. This has implications forthe infrastructure to facilitate rapid transfer between institutions, as well as for the number andlocation of PCI capable facilities.

Page 14
Expert Panel on Invasive Cardiology in Ontario
3.2.2.4 Mode of revascularization: PCI vs. CABG
An increasing proportion of patients is being revascularized by PCI as opposed to CABG. Thenumber of PCI procedures for each isolated coronary bypass operation in Ontario has risen from0.71 in 1995/96 to 1.3 in 2000/01. In many jurisdictions outside Ontario, including severalCanadian provinces, this number exceeds 1.5. This has occurred because the technologicalenhancements that have broadened the scope of both modes of revascularization in recent yearshave been more numerous and pivotal for PCI. Such enhancements include ongoingimprovements in catheter and wire technology, coronary stents to prevent restenosis, GP IIb/IIIainhibitors to reduce procedural ischemic complications, thienopyridines to prevent stentthrombosis, and further miniaturization to facilitate safe and effective vascular access.
As diagnostic cath becomes more widely used, particularly for unstable presentations, the numberof patients referred on for PCI will rise at a faster rate than the number referred on for CABG.This too has implications for the planning of PCI services.
3.3 OPERATOR STANDARDS
Published guidelines address a range of operator (physician) and institutional issues for both cathand PCI. Major issues include the structure, content, and duration (or minimum case volume) oftraining programs, credentialing, requirements for maintenance of competence (includingminimum case volumes), and benchmarks for procedural outcomes. The guidelines originatefrom various professional societies in a number of countries, including Canada. (See Appendix 4for a list of the published guidelines referred to in this report.)
3.3.1 Training Requirements
Cath and PCI are complex procedures that require specific technical and cognitive skills to beperformed safely and effectively. While such skills are refined by ongoing practice andexperience, they are initially acquired through a process of formal training. The Panel reviewed anumber of published guidelines dealing with training requirements, and also considered theopinions of a number of experts internal and external to the Panel.
The expert opinions submitted to the Panel and the published guidelines for minimum trainingrequirements for operators are detailed in Appendix 11 and Appendix 12 for cath and PCIrespectively and summarized in Table 4.
Table 4: Minimum Training Requirements from Published Guidelines and Expert Opinion,Cath and PCI, number of cases
Published Guidelines Expert OpinionCath PCI Cath PCI
Operator Training
• As primary operator
• Total procedures
200 to 300
300 to 500
125 to 150
50 to 400
300 150 to 250
150 to 300
3.3.2 Maintenance of Competence
A number of observational studies demonstrate a consistent relationship between procedurevolume (by operator and by institution) and clinical outcome. This theme is also reflected in all

Page 15
Expert Panel on Invasive Cardiology in Ontario
of the published guidelines and most of the expert opinion received by the Panel. In this context,PCI has been studied far more intensely than diagnostic cath.
The expert opinions submitted to the Panel and the published guidelines for minimum procedurevolumes for operators are detailed in Appendix 11 and Appendix 12 for cath and PCI respectivelyand summarized in Table 5.
Table 5: Minimum Operator Volumes in Published Guidelines and Expert Opinion, Cathand PCI, procedures/year
Published Guidelines Expert OpinionCath PCI Cath PCI
Operator Maintenance of Competence 150 to 250 75 to 125 150 to 250 50 to 150
As shown in the table, the minimum volumes suggested by the invited experts tend to be higherthan the existing published guidelines for PCI. This difference supports the view that theprocedures are becoming more complicated, and the expert opinion better reflects the currentenvironment than the published guidelines.
3.4 INSTITUTIONAL STANDARDS
3.4.1 Minimum Procedure Volumes
The published literature demonstrates that high volume institutions tend to have superioroutcomes. Once again, there is more evidence in this regard for PCI than for diagnostic cath.Some studies supported an interaction between operator and institutional volume, such that lowvolume operators tended to have better outcomes at high volume institutions; this may reflect thevalue of the supporting infrastructure (e.g., an experienced team) for these procedures.
Very few studies address truly contemporary interventional practice, with its high use of GPIIb/IIIa inhibition and stents. No studies have investigated the relationship betweenoperator/institution volume and longer-term outcome after PCI (e.g., freedom from death, MI,repeat intervention). In other words, for the purposes of quality assurance, clinical outcome ofPCI has been defined in terms of procedural failure rather than ultimate procedural success.
The expert opinions submitted to the Panel and the published guidelines for minimum procedurevolumes for institutions are detailed in Appendix 13 and summarized in Table 6.
Table 6: Minimum Institutional Volumes in Published Guidelines and Expert Opinion,Cath and PCI, procedures/year
Published Guidelines Expert OpinionCath PCI Cath PCI
Institutional Volumes 200 to 1,000 100 to 400 500 250 to 600
As with the recommended minimum procedural volumes, expert opinion favours higherinstitutional volumes than the published guidelines for PCI.

Page 16
Expert Panel on Invasive Cardiology in Ontario
3.4.2 Quality Assurance
The role of the institution in assuring quality depends on its ability to provide, enhance, andmonitor the following:
• A highly skilled cardiac care team, including invasive and non-invasive cardiologists,cardiac surgeons, cath lab and acute care nurses, and imaging and hemodynamictechnologists. The necessary skills include cognitive skills and technical skills thattogether facilitate the making and implementing of appropriate care decisions, and permitrapid and effective responses to emergencies. Such skills are partly, but not entirely,related to experience.
• Opportunities for invasive cardiologists to interact among themselves and with cardiacsurgeons to increase each other’s knowledge base and develop trust in each other’sjudgment.
• High quality facilities and equipment, with a preventive maintenance program andprompt and effective service when necessary.
• An administrative structure that facilitates attainment of the above objectives.
The College of Physicians and Surgeons of Ontario (CPSO) has developed and coordinated anumber of physician assessment and review programs, although not in this specific area ofinvasive cardiology. In the process of secondary review, the CPSO expressed interest incollaborating with other stakeholders in the assessment and review of these services.
Published guidelines and expert opinion support the following minimum requirements for aquality assurance program at the institutional level:
• A rigorous privilege granting process to ensure that physicians applying for privileges atthe institution are appropriately qualified.
• A formal mentoring relationship with an experienced operator for any physician that isnewly trained and/or operating at low volumes.
• A medical cath lab director who is given responsibility and resources for establishing andmaintaining the quality assurance program.
• A monitoring system that tracks basic measures of quality (e.g., complication rates),supplemented by a peer review process which may include regular clinical meetings toreview quality indicators.
• Reporting of data to a centralized, independent body for further analysis and review.
Published guidelines and expert opinion on quality assurance are summarized in Appendix 14.
3.5 TRAINING PROGRAMS
Training is most effective when it is conducted within a formal program. An accredited, formalprogram offers more than just tutoring by an experienced cardiologist. It offers a process thatexposes the trainee to the entire spectrum of practice (e.g., case selection, preassessment, postprocedural care, discussions with the surgeon). It also allows the trainee to be immersed in theeducational experience, without a multitude of distractions.
Published guidelines and expert opinion highlight the following minimum components of aninvasive cardiology training program:
• The program should be accredited (or at least would be eligible for accreditation if noformal accreditation exists). One guideline also suggested that the training institution beaffiliated with a university.

Page 17
Expert Panel on Invasive Cardiology in Ontario
• The program should be under the direction of a cath lab director who is responsible forthe documentation of the trainee’s competence, judgement, and technical ability.
• The training institution should issue a certificate of competence.
• In some instances, the cardiologist is encouraged to take the training at an institutionother than his home institution (e.g., after a long absence from practice).
Cardiologists who “retrain” are, on average, older than cardiologists who receive trainingimmediately after residency. Thus, the use of retraining to build capacity for the growingvolumes of procedures may cause the average age of invasive cardiologists to increase. It wassuggested that retraining for complex procedures is not the preferred long-term solution to ahuman resource shortage.
3.6 PCI AND ON-SITE CARDIAC SURGERY
In Ontario today, cath is performed at some centres without on-site cardiac surgery, but PCI isnot. However, many of the stakeholder submissions received by the Panel indicated that localhospitals had either already made, or were planning to make, proposals to MOHLTC to providePCI without on-site cardiac surgery.
The published literature, expert opinion, and the Panel’s experience were consistent in the viewthat having on-site cardiac surgery was the preferred approach to providing cath and PCI services.However, there was no consensus in the literature or in the expert opinions as to whether on-sitesurgery should be considered mandatory, or whether, in the presence of an enablinginfrastructure, PCI without on-site surgery was an acceptable alternative for addressing particularneeds.
In some jurisdictions (e.g., Germany), PCI is commonly performed without on-site cardiacsurgery, but the practice has been much less common in North America. In the United States, onesource20 estimates that 68 sites perform PCI without on-site cardiac surgery (out of a total ofapproximately 800 PCI programs), but only 22 of those sites perform elective PCI, and many ofthese sites have very low volumes. In Canada, the Panel identified only four such sites21 (out ofapproximately 42).
There are no randomized controlled trials comparing outcomes at institutions with and withouton-site cardiac surgery. Published outcomes of PCI at sites without on-site cardiac surgery are ingeneral comparable to benchmark rates overall, although these are not adjusted for the potentiallylower-risk baseline characteristics of the patient population undergoing intervention at a stand-alone PCI site. Note that “outcome” in this context essentially refers to the rates of death andemergency bypass surgery.
Published guidelines and expert opinion on providing PCI without on-site surgery are provided inAppendix 15.
20 Thomas P Wharton Jr MD, et al, Non-Emergent Coronary Intervention Without Cardiac Surgery OnSite: Outcomes in 2,645 Patients in the US Poster presentation at the 73rd Scientific Sessions of theAmerican Heart Association New Orleans, LA, November, 2000, Circulation 2000;102:II-731-221 Hôpital Hôtel-Dieu de Québec in Quebéc City, Centre hôspitalier Pierre-Boucher in Longueuil, Centrehôspitalier régional de l’Outaouais in Hull, and Royal Alexandra Hospital in Edmonton.

Page 18
Expert Panel on Invasive Cardiology in Ontario
4. CURRENT DELIVERY OF INVASIVE CARDIOLOGY SERVICESAs at January 2001, Ontario has eight full-service cardiac centres that provide cath, PCI andcardiac surgery, and five centres that provide cath only. In 2000/01, these 13 performed close to40,000 caths and over 10,000 PCI procedures, an increase of approximately 15% over theprevious year.
This chapter provides a detailed description of the resources currently involved in the delivery ofinvasive cardiology services in Ontario:
• Human resources (including number of operators and annual volumes, number intraining, certification of competence, and quality assurance).
• Physical resources (including the organization of care and supporting resources).• The relationship between the demand for invasive cardiology services and the capacity to
meet that demand over the next five years.
This chapter is descriptive only and is included to provide context for the Panel’s deliberationsand recommendations presented in the following chapters.
4.1 HUMAN RESOURCES
As of January 2001, the CCN’s Cardiaccess database indicated that there were 97 cardiologists inOntario performing diagnostic cath only (i.e., not PCI), and another 45 cardiologists performingboth cath and PCI, for a total of 142 invasive cardiologists in Ontario. The distribution of theseresources by centre is provided in Appendix 16. Because of entry into and exit from the invasivecardiology physician workforce, the number of physicians as determined from Cardiaccess maynot be precise at any given point in time.
Based on an analysis of procedure volumes as reported to CCN between July 2000 and January2001, approximately one-quarter of cathing cardiologists had an annualized volume of less than150 cath procedures per year (the CCS recommended minimum). Approximately 9% ofinterventional cardiologists were performing less than 100 PCI cases per year (the CCSrecommended minimum). Of those cardiologists performing PCI, almost all (98%) performedover 150 procedures in total (cath plus PCI).
These findings are summarized in Table 7, below. A description of the data sources and analysisis provided in Appendix 17.
Table 7: Estimated Annual Operator Volumes, Cath and PCI, Ontario, 2000Cathing Cardiologists Interventional Cardiologists
CathN = 97
PCIN = 47
TotalN = 47
CCS recommended minimum22 150/year 100/year 150/year
Performing fewer than minimum• Number of cardiologists• Percent of cardiologists
2526
49
12
Number of procedures/year• Median• Interquartile range
203141 to 284
190157 to 240
393312 to 561
22 Based on Canadian Cardiovascular Society standards, May 1996.

Page 19
Expert Panel on Invasive Cardiology in Ontario
4.2 TRAINING FOR INVASIVE CARDIOLOGY
In Ontario today, training for invasive cardiology is a mix of formal and informal programs thattake place at teaching hospitals and other cardiac centres. Basic initial training in diagnostic cathis provided during cardiology residency training. In addition, residents learn about the potentialscope and limitations of PCI, but receive little if any hands-on PCI training during residency.
While cath training received during cardiology residency is supported financially by MOHLTC,there is no funding support from MOHLTC for invasive training outside of the formal cardiologyresidency. Specifically, this means that additional training for cath beyond cardiology residency,and training for PCI at any time, are not funded by MOHLTC. Cath training beyond thecardiology residency is necessary for recent graduates wishing or needing to refine their skills, aswell as for cardiologists in practice wishing to begin or return to invasive work. PCI training, asnoted above, is always provided in its entirety outside (i.e., beyond) cardiology residency.
There is no funding support from the MOHLTC for invasive training beyondthe basic cath training provided during the cardiology residency.
Training for invasive procedures may take place at different time-points in a cardiologist’s career.
4.2.1 Cath Training During Cardiology Residency
Training in the subspecialty of cardiology takes place within a Royal College of Physician andSurgeons of Canada (Royal College) program and, as such, is affiliated with a university andsubject to a process of accreditation. (University-affiliated cardiac centres in Ontario that providecardiology training are identified in Appendix 18.) Cardiology residency includes basic trainingin cath, with one or more cath lab rotations totaling at least four months. With the recentextension of the cardiology residency program from two to three years, residents can elect tospend up to four additional months on a cath rotation, for a total of up to eight months of cathtraining during residency.
A resident with a particular interest in invasive cardiology might include among his/her rotationsan introduction to PCI, which may involve a limited amount of hands-on training. While thisexposure may help the resident decide on an ultimate career plan, and provide a running start tosubsequent formal PCI training, existing guidelines from CCS (and other professional groups)generally require a full year of dedicated PCI training over and above any exposure duringcardiology residency.
4.2.2 Cath Training After Cardiology Residency
Training in diagnostic cath outside of a cardiology residency program has been undertaken bycardiologists already in practice who have not been performing invasive procedures, as well as bynew graduates of cardiology residency who did not receive sufficient training during residency.
Many practicing cardiologists have obtained additional training or “retraining”23 to performdiagnostic cath, particularly in recent years. This training has generally been conducted on a part-
23 “Retraining” has been used by some to mean training for a physician currently in practice, regardless ofwhether the physician was fully trained to perform the procedure in the first place. However, in this report,and in the CCS Standards publication, “retraining” refers to the training required by a physician who haspreviously performed a given procedure independently and now wishes to resume such activity after aperiod of absence.
Page 20
Expert Panel on Invasive Cardiology in Ontario
time basis, and has been provided in many cath labs, including full service centres and standalone labs.
The CCS Standards include minimum requirements for training in diagnostic cath and PCI, whichare applicable at any stage of the trainee’s career. The same document discusses (separately)requirements for “retraining” – i.e., that required by a physician who has previously performedcath or PCI independently but has been absent from such activity for a period of time. Thesestandards have not been formally adopted or operationalized in Ontario, so that outside ofcardiology residency programs, there is at present no formal training structure or evaluationprocess.
As noted above, MOHLTC does not fund cath training or retraining outside the cardiologyresidency. This means that there is no formal support for cardiologists who leave an establishedpractice to train or retrain in invasive procedures (i.e., to compensate for lost income or to providecoverage for the practice). Furthermore, there is no support provided to the cardiologists orcentres providing such training. This is problematic because the presence of a trainee usuallymeans that cases take longer to complete, resulting in a reduction of throughput (and thus loss ofprofessional income for the trainer) or a necessary extension of hours (and thus increasedoperating costs for the training centre).
4.2.3 PCI Training
Interventional cardiology is not recognized as a subspecialty by the Royal College. Therefore,training in PCI is outside the Royal College accredited program and the MOHLTC does notprovide funding for either the trainee or the cardiologists who do the training. In general, funding(for trainee salaries) has been provided out of the supervising cardiologists’ income, or by thehospital, or by industry (or some combination thereof).
Residents wishing to perform PCI independently must proceed on completion of the corecardiology training program to a full-time dedicated training period of at least one year, referredto as a fellowship. Trainees are formally appointed in the host university’s post-graduate medicalprogram, and receive evaluations modeled after the Royal College ITER (In-Training EvaluationReport). They generally receive a certificate of completion at the end of the training period, butthere is no formal specialty designation or specific licensing provision that results from successfulcompletion of the fellowship.
4.3 CERTIFICATION, RECERTIFICATION, AND CREDENTIALLING
At present, there are no agreed upon or defined performance standards or benchmarks applied toinvasive cardiology procedures in Ontario. Once initial training is completed, there is no formalrequirement for on-going or periodic evaluation or recertification in these procedures.
Annual procedure volume has been used as a simple and objective surrogate measure forcompetence. Although there are no formal criteria around the number of procedures to achieveand maintain competence, there is a clear consensus that there is a minimum acceptable numberof procedures that should be performed within a defined time period.
Despite the absence of formal standards, the onus is nonetheless on the institution providinginvasive services to exercise appropriate due diligence through its bylaws and credentialingprocess (with possible input from the cath lab director). This would encompass confirmation ofadequate training and assessment of competence for a physician commencing invasiveprocedures, as well as periodic review of performance and renewal of credentials for physicians
Page 21
Expert Panel on Invasive Cardiology in Ontario
already performing such procedures. It is not known whether institutions have made reference toexisting guidelines to aid in these tasks.
4.4 QUALITY ASSURANCE
At present, there is no standardized approach for tracking and reporting outcomes of procedures.Most if not all centres providing PCI track rates of death and emergency bypass surgery, andmany track peri-procedural myocardial infarction (MI). However, the definitions of emergencysurgery and peri-procedural MI are not uniform. While many centres track total CK enzyme onall PCI patients, only a minority routinely measure the more sensitive CK-MB fraction.
One centre routinely tracks 15 specific outcome indicators. Several centres formally review allPCI cases that result in emergency surgery or death. All of these initiatives are locally driven;there is no provincial quality assurance program in place.
The CCN database, Cardiaccess, contains data elements related to cath and revascularizationprocedures, with a primary focus on monitoring waiting lists and wait times. This database wasoriginally established to track cardiac surgery, and has only recently begun to track cath and PCIprocedures across the province.24
4.5 LOCATION OF CARDIAC CENTRES AND PROGRAMS
4.5.1 Existing and Approved Centres
Until recently, there were eight full-service cardiac centres (i.e., those providing cath, PCI, andcardiac surgery) in the province. Five additional centres provided diagnostic cath services only.To-date, PCI has only been performed at sites that also provide cardiac surgery.
In 1998, the MOHLTC approved three new full service centres, with a mandate to providediagnostic cath, PCI and cardiac surgery:
• Trillium Health Centre in Mississauga began providing cath services in spring 2000 andexpanded to full cardiac services in late 2000.
• Southlake Regional Health Centre in Newmarket has been performing caths since 1999,and is scheduled to expand to full cardiac services by 2003/04.
• St. Mary’s General Hospital in Kitchener is scheduled to begin performing caths in early2001 and is scheduled to begin PCI and surgery by 2003/04.
The MOHLTC also approved two new centres to provide caths only:
• Peterborough Regional Health Centre began providing caths in mid 2000.
• A cath lab was approved at Toronto East General Hospital in late 2000 and is expected tobe operational by the end of 2001.
The number of centres providing cath, PCI and cardiac surgery is provided in Table 8. Toillustrate the recent and rapid expansion in services, the table differentiates between establishedcentres (i.e., were operational prior to January 1, 2000), and new centres (i.e., opened afterJanuary 1, 2000). A listing of the individual centres within each category is provided inAppendix 18. 24 As of January 2001, all cardiac centres are providing data to CCN on cath and PCI procedures.

Page 22
Expert Panel on Invasive Cardiology in Ontario
Table 8: Number of Cardiac Service Centres in Ontario, January 2001
Cath Only Full ServiceEstablished centres 4 8
New centres (opened after Jan 1 2000) 1 1
Approved centres25 1 2
Subtotal existing and approved 6 11
In addition to the expansion in capacity that has been achieved (or will be shortly) through thedevelopment of new facilities, Ontario will also enjoy increased capacity from expansion ofexisting centres (e.g., the construction of additional cath suites [rooms] at established centres).Within the next 12 months, the number of cath rooms in operation in Ontario is expected toincrease by 16% from 32 to 37. The details of this expansion are provided in Appendix 19.
4.5.2 Supporting Resources
The provision of invasive cardiology services in Ontario relies on many supporting systems, mostof which are ad hoc or informal, as noted below:
• Availability of very urgent or emergent PCI or surgery for stand-alone diagnostic cathlabs. The Panel was not aware of any formal arrangements that exist between cath onlyfacilities and nearby (or in some cases distant) full service cardiac centres.
• Availability of emergency surgery to deal with rare but serious PCI complications. Atone time much earlier in the development of PCI, a surgical team and an operating roomwere on standby during all PCI cases (because of the much more frequent need foremergency surgery). This degree of case-by-case backup does not occur (and is notrequired) in contemporary practice, except in very special circumstances.
• Electronic communication capabilities. At present, clinical information is transmittedbetween centres and physicians verbally by telephone or by FAX, while angiographicdata is transmitted by physically transporting a compact disc (CD) between sites. Apartfrom a high-bandwidth link that permits transfer of angiograms between the TorontoWestern and Toronto General sites of University Health Network, the Panel was notmade aware of any other such capabilities in Ontario at present.
• Ambulance services. In Windsor, an arrangement has been made with the localambulance service, which has equipped two units with special brackets and power outletsto support transportation of an intra-aortic balloon pump (IABP). A mechanism exists toensure that the ambulance service is notified when this special equipment may be needed.However, the Panel was not made aware of any other existing formal arrangements withAmbulance Services to handle the specific emergency needs of patients undergoinginvasive cardiac procedures. In fact, serious concern exists at many cardiac centres thatambulance services are not currently capable of supporting the urgent and semi-urgentpatient transport that is an inherent requirement of Ontario’s regionalized system ofinvasive cardiac care.
25 Approved but not yet operational.

Page 23
Expert Panel on Invasive Cardiology in Ontario
4.6 DEMAND FOR SERVICES
Approximately 39,551 diagnostic cath procedures and 10,339 PCI procedures were performed inOntario in 2000/01. This corresponds to a provincial rate of 458 caths and 120 PCIs per 100,000adult population, as shown in Table 9. These procedure rates are in excess of the target minimumrates for Ontario that were approved by MOHLTC several years ago. However, the TargetSetting Working Group of CCN proposed to MOHLTC, in October 2000, revised minimumtargets, as indicated in Table 9. It should be noted that there are substantial regional variations inprocedure rates that are not reflected in the province-wide rates.
Table 9: Procedural Volumes and Target Rates, 2000/01, Ontario
ProceduresProcedure Rate
(per 100,000 adults)(Actual) Actual Target
CATH 39,551 458 357
PCI 10,339 120 100
Procedure volumes for both cath and PCI have been increasing rapidly in Ontario since the mid-1990s. This growth is attributable in part to the aging and overall growth of Ontario’s population,but more importantly to a continuing (and accelerating) change in practice related to the optimalmanagement of patients with coronary artery disease, particularly acute coronary syndromes.Recent clinical data support the widespread and early utilization of diagnostic cath and, wherefeasible and appropriate, early revascularization for patients with acute MI or unstable angina.Because of compelling technical advances, PCI has become an increasingly attractive alternativeto CABG or medical therapy, and is being used for an ever-increasing proportion ofrevascularization procedures.
Despite significant provincial growth in cath and PCI over the past several years, Ontario’s ratesremain well below those in many other comparable jurisdictions. These factors formed the basisfor the substantial increases in population-based minimum target rates proposed by the TargetSetting Working Group (shown in Table 10). As of April 2001, MOHLTC had not yet officiallyapproved these proposed rates.
Table 10: Proposed Target Procedure Rates per 100,000 adult population, Cath and PCI,Ontario26
2000/01 2003/04 2005/06
Cath 357 500 540
PCI 100 140 160
The actual procedure volumes achieved in 2000/01 exceeded the estimates used by the TargetSetting Working Group. Nonetheless, even with this revised starting point, attainment of theproposed targets by 2005/06 will require a further 34% increase in diagnostic caths (or 12,000additional procedures) and a 37% increase in PCI (or 3,400 additional procedures) over the nextfive years, based on projected population growth. The actual and projected target cath and PCIvolumes are shown in Figures 1 and 2.
26 Target Setting Working Group of the Cardiac Care Network of Ontario, Final Report andRecommendations, October, 2000.

Page 24
Expert Panel on Invasive Cardiology in Ontario
Figure 2: Cath Volumes, Actual and Target,27 1993/94 to 2005/06
Figure 3: PCI Volumes, Actual and Target,28 1993/94 to 2005/06
The Working Group’s recommendations were based on comparisons with other countries andprovinces, age-adjusted population projections for Ontario, and consensus around the current andfuture role of invasive procedures. Some practitioners believe that in light of recent researchfindings and trends in clinical practice, even the relatively ambitious targets proposed by theTarget Setting Working Group are unduly conservative. Certainly the rapid growth in PCIvolume in the past two fiscal years (14% and 20% respectively) suggests that there was a large,previously unmet demand. Furthermore, although the Working Group recommendations weredesigned to bring Ontario into line with comparable jurisdictions elsewhere, PCI rates in otherCanadian provinces continue to rise, and will likely be significantly higher than Ontario’sproposed rate of 160 per 100,000 adults by 2005/06.
As diagnostic cath rates in Ontario increase further, and the proportion referred on for PCI alsoincreases, it is conceivable that the need for PCI services will be well in excess of the ratesproposed by the Working Group. On the other hand, preliminary analysis of PCI waiting list datanow available through CCN’s expanded Cardiaccess database indicates that the provincial
27 The target volumes are based on projected growth in procedures, using 1999/00 as a base, needed toachieve the recommended population-based target rates by 2005/06, as presented in Table 9. Note thatgrowth of procedures in 2000/01 exceeded this rate.28 See footnote for Figure 2.
0
10,000
20,000
30,000
40,000
50,000
60,000
93/9
4
94/9
5
95/9
6
96/9
7
97/9
8
98/9
9
99/0
0
00/0
1
01/0
2
02/0
3
03/0
4
04/0
5
05/0
6
Num
ber
of p
roce
dure
s
Actual
Target
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
93/9
4
94/9
5
95/9
6
96/9
7
97/9
8
98/9
9
99/0
0
00/0
1
01/0
2
02/0
3
03/0
4
04/0
5
05/0
6
Nu
mb
er
of
pro
ced
ure
s
Actual
Target

Page 25
Expert Panel on Invasive Cardiology in Ontario
median waiting time for PCI is one day (if ad hoc procedures are included) or 11 days (if ad hocprocedures are not included). This suggests that, at least on a provincial basis, current demandfor PCI is being met with reasonable timeliness.
4.7 CAPACITY CONSIDERATIONS
4.7.1 Rationale for Analysis
The Target Setting Working Group requested that this Panel “make recommendations about howbest to achieve the new PCI targets while maintaining quality of care.” This was to includediscussion and guidelines related to operator and institutional requirements, and consideration of“options to deal with potential under-capacity,” including the option of PCI in centres without on-site cardiac surgery.
In order to fulfil its mandate, the Panel recognized that some estimate of the potential scope ofunder-capacity was necessary. For example, in its deliberations over training guidelines, thePanel considered whether the degree of shortfall between the number of invasive cardiologists inOntario and the demand for their services should influence minimum training requirements.
Although provision of high quality care is the paramount consideration in establishing theseguidelines, a genuine crisis in the delivery of invasive services (with the demonstration thatpatients are not receiving necessary care because of a shortage of trained physicians) might justifya short-term modification of minimum training standards. In the absence of such a crisis,whatever training standards were felt to be necessary for provision of high quality care shouldprevail. Similarly, if it could be demonstrated that the physical capacity for PCI within existingor planned surgical centres was substantially less than the future targets (i.e., a crisis of access),then this would influence the criteria for providing PCI without on-site surgery. Alternatively, ifthe future need could be readily accommodated in centres with surgery, then the option of PCIwithout on-site surgery would have to be justified on grounds other than capacity.
Therefore, in order to better understand the potential gap between demand and capacity andaddress the implications for training and for organization of PCI services, the Panel undertook ananalysis of:
• Physician resources, as measured by the number of invasive cardiologists currentlypracticing in Ontario, any latent capacity among these cardiologists, and the expectationof new resources (either through training or net migration to Ontario).
• Physical resources, as measured by the number of cath rooms in operation.
4.7.2 Findings of the Capacity Analysis
Details of the capacity analyses, including the assumptions and scenario descriptions that underliethe conclusions related to PCI physician and physical resources, are provided in Appendix 17.
4.7.2.1 Physician Resources
The Panel determined that the number of cardiologists qualified to perform diagnostic cath is notexpected to be a limiting factor in the further expansion of services over the next five years:
• Because the cardiology residency is now three years in duration, most graduatingresidents can, if they wish, attain at least the minimum training required during residency.
• In addition, a significant number of practicing cardiologists have undergone cath trainingin recent years, thereby supplementing the invasive work force.

Page 26
Expert Panel on Invasive Cardiology in Ontario
• It is anticipated that there may be other practicing cardiologists who wish and intend toobtain cath training in the next few years.
• Finally, the data on individual operator volumes presented earlier in this report suggestthat there is considerable latent capacity, at least among a subset of current cathoperators. (See Table 7.)
The degree to which the availability of trained interventional cardiologists could limit the growthof PCI depends on what assumptions are made about workload parameters and about the numberof new interventional cardiologists entering practice each year through training or migration, netof attrition. Based on the results of scenario analysis (testing for changes in demand and insupply), the Panel has estimated the need for a net increase of between five and seven new PCItrained cardiologists per year over the next five years.29 It is anticipated that fellowship trainingprograms will have the capacity to train sufficient numbers of cardiologists to meet these needs.
There are indications of a current shortage of cardiologists, based on the reported waiting time fora cardiology consultation and on the recruitment needs of many hospitals. While this shortfallhas been documented most clearly in community practice settings,30 there is a perceived shortageof cardiologists available to provide general cardiac care in academic settings as well. Thissituation has likely arisen in part because of an insufficient number of new cardiologists (andother specialists) in the face of demographic changes, and in part because of the increasedcomplexity of cardiac care, many aspects of which are “physician-labour” intensive (e.g., cath,PCI, invasive electrophysiology, trans-esophageal echo).
If new graduates of cardiology residency programs are preferentially streamed toward invasivepractice, this shortage in general cardiology will be exacerbated. On the other hand, if a largenumber of practicing cardiologists re-orient their professional activities to include invasiveprocedures, the impact on the availability of general cardiology services will be similar.Therefore, the overall impact on cardiology physician resources is not dependent on whether thepool of qualified invasive cardiologists is supplemented by new graduates or by the training ofphysicians already in practice. Furthermore, regardless of which physician resource strategy isadopted to meet the growing invasive needs of Ontario, it is clear that for these needs to be metwithout adversely impacting on the overall provision of cardiac services, the net supply ofcardiologists must be increased.
4.7.2.2 Physical Resources
The Panel concluded that additional cath rooms will be required over the next five years toprovide sufficient physical capacity. Even with further expansion at existing or developingsurgical centres, it is likely that at least a limited number of PCI cases will have to be performedat centres without on-site cardiac surgery if targets are to be met (unless further surgical centresare developed).
29 In 2000, CCN identified a pending shortage of interventional cardiologists as an area of concern,estimating a need for between 25 and 29 new physicians over the next five years to meet the proceduralvolumes indicated by the proposed targets. A Discussion Paper by the Consensus Panel on CardiovascularHuman Resources in Ontario, Final Report and Recommendations, June 2000.30 GTACC presentation to the Panel.

Page 27
Expert Panel on Invasive Cardiology in Ontario
SECTION D: RECOMMENDATIONS
CONTEXT FOR THE RECOMMENDATIONSIn the remaining chapters, the Panel’s recommendations are presented for operator andinstitutional guidelines, including quality assurance and the organization of care. In itsdeliberations and discussions, the Panel considered a broad range of issues and contextualinformation, much of which is described in the previous chapters and in the summary of theliterature review in Appendix 3. Where relevant, the key contextual information that guided thePanel’s decision-making is provided for ease of reference in this chapter with the associatedrecommendation.
Where existing guidelines from professional bodies (particularly from within Canada) were felt tobe relevant and appropriate, the Panel used such guidelines (e.g., the Canadian CardiovascularSociety guidelines31) as the basis of its own recommendations. Existing guidelines were modifiedas necessary.
Although each recommendation addresses distinct issues, they are all inter-related. For example,if the quality assurance recommendations are not implemented, then the training guidelines (e.g.,minimum volumes and durations) may no longer be appropriate. The Panel believes that thevalidity of these recommendations would be undermined if individual recommendations wereconsidered or implemented in isolation.
These recommendations are intended to establish or affirm minimum standards. Individualoperators and institutions are strongly encouraged to ensure that the minimums are exceeded.Indeed, for planning purposes, MOHLTC should consider the desirability of individual operatorsand institutions exceeding, on a consistent basis, the minimum volumes specified in therecommendations.
These recommendations are directed to the MOHLTC for implementation, even if that is notindicated in the specific wording of each recommendation.
The MOHLTC is urged to ensure that all centres currently providing or contemplating theprovision of invasive cardiology services be provided with a copy of this report.
31 Canadian Journal of Cardiology, May 1996.
Page 28
Expert Panel on Invasive Cardiology in Ontario
5. OPERATOR STANDARDS
5.1 OPERATOR TRAINING
In developing recommendations on training and maintenance of competence, the Panelemphasized its belief that the paramount consideration behind standards of training andmaintenance of competence is to promote the safest and most effective treatment possible. ThePanel made the following assumptions around the safety and efficacy of invasive procedures:
• Invasive procedures are complex. Although complication rates have fallen in recentyears, the procedures themselves are no less complex. In fact, because they are beingincreasingly performed on unstable patients or those with significant co-morbidity, theoverall practice of invasive cardiology (cath and/or PCI) is becoming more complex.
• The success of an invasive procedure reflects the degree to which the procedure achievesits diagnostic and/or therapeutic goal(s), coupled with the absence of complications.While both of these aspects are heavily influenced by patient characteristics, they alsodepend on the skill and judgement of the operator.
• Performance of invasive procedures encompasses distinct technical and cognitive skills.Physicians performing invasive procedures should be appropriately trained, and mustmeet minimum standards for maintenance of competence in such procedures.
The extent of training is specified by a minimum number of procedures, or by minimum duration,or both. The rationale for a minimum caseload or a minimum time spent in training includes:
• Acquiring proficiency in the “hands-on” aspects using various tools and techniques.
• Having exposure to a variety of unexpected situations or complications while in asupervised setting. This in itself may will have an impact on the duration of training – atrainee may have to spend a longer time in a supervised setting to be exposed to, andlearn how to deal with, increasingly rare but still important complications.
• Developing an appreciation of the capabilities and limitations of interventionaltechniques, in order to develop the consultation skills essential for the cardiologistperforming either diagnostic cath or PCI.
There may be limits to the number of cardiologists required to train in and perform invasiveprocedures, implying the need for a selection process. The following points are relevant in thisregard:
• Individual physicians have varying degrees of proficiency for specific tasks. While allcardiologists require competency in a core set of clinical skills, it is neither realistic nornecessary to expect that all cardiologists can or should attain proficiency in performinginvasive procedures.
• Although decisions as to sub-specialty orientation may be taken at various times in acardiologist’s career, some degree of self-selection likely occurs toward the end ofresidency whereby those with the greatest interest and/or potential for performingcomplex invasive procedures seek further training, and those with lesser degrees ofinterest or potential seek other opportunities.

Page 29
Expert Panel on Invasive Cardiology in Ontario
5.1.1 CCS Guidelines
Guidelines for Adult Cardiac Catheterization and Angiography were developed and published bythe CCS in 1996, and were felt by the Panel to still be relevant. In addition to detailing procedurevolumes for training and maintenance of competence, they include discussion related to contentof training, quality assurance, and other important issues.
The CCS guidelines are based on a tiered approach to developing proficiency and independencein increasingly complex procedures:
• Level 1 encompasses the basic exposure to cath (over at least four months) obtained byall cardiology residents during their core training. While some residents may progresssufficiently to act as primary operator at this stage, it is always under the very closesupervision of a staff cardiologist. Attainment of Level 1 is not considered sufficient toperform independent cath.
• Level 2 is achieved following at least four additional months of full-time cath trainingand involving at least 200 additional cases. At the time that the current CCS guidelineswere developed, cardiology residency was a two-year program and it was not possible toachieve Level 2 (minimum eight months total) without additional training beyondresidency. Recently, the core cardiology training program has been extended to threeyears, and it may now be possible for certain trainees to attain at least the procedurevolume and duration criteria of Level 2 during their cardiology residency. However,because they will still have been subject to close supervision within the context of theresidency program, such trainees may benefit from a staged transition to fullindependence by way of a mentorship structure (see recommendation below).
• Level 3 of the CCS Standards represents intensive training in interventional procedures(PCI) and requires full-time training for at least one year. As a prerequisite to Level 3, atrainee must fulfill the procedure volume requirements of Level 2.
The CCS standards are reproduced in Appendix 20 for reference.
5.1.2 Training for Cath and PCI
Many of the foregoing comments on training are applicable to both cath and PCI training.However, there is a substantially greater range of skills required to perform interventional ascompared to diagnostic procedures. Consequently, the training needed for PCI is more intenseand more prolonged than that for cath.
For a physician in practice who now wishes to perform invasive procedures but did notpreviously do so on an independent basis, the relevance of training received during residencydepends on the nature of that training and the duration since it occurred. To ensure that anobjective and independent evaluation can be provided, some would consider it ideal that aphysician currently in practice who seeks training in diagnostic cath or PCI should obtain at leasta portion of that training at a centre other than his or her home institution. There may also be abenefit from exposure to different teachers and a different cath lab. However, the practicaldifficulties of doing this may be formidable for some cardiologists. Therefore, the Panel chose toindicate that this arrangement was advisable, and that support for training should address thelogistical difficulties involved, but that time away from the home institution was not mandatory.
Physicians who have performed invasive procedures on an independent basis, but then haveperiod of absence from these procedures (e.g., for illness, sabbatical) require a period of

Page 30
Expert Panel on Invasive Cardiology in Ontario
“retraining.” Similar considerations as noted above apply to the value of “retraining” outside thehome institution.
Because it is assumed that a training program involves a gradual increase in the degree ofindependence and responsibility, we have chosen not to distinguish between the number of casesperformed as primary operator and the total number of cases.
Recommendation 1: That the Canadian Cardiovascular Society “Standards forTraining in Adult Cardiac Catheterization and Angiography” and “Standards forCoronary Angioplasty Training”32 be adopted (where applicable) by all institutions andprograms in Ontario performing cath and PCI. Where recommendations in this reportexceed minimum standards in the CCS document, the recommendations herein shouldtake precedence.
Recommendation 2: That physicians who have not previously performed independentdiagnostic catheterization and now wish to do so undergo training equivalent to thatrequired to attain Level 2 of the CCS Standards:
• If residency was completed more than 10 years earlier, then training shouldinclude the attainment of Level 1 before proceeding on to Level 2; if residencywas completed within the past 10 years, then attainment of Level 1 can beassumed, and training can immediately apply toward attainment of Level 2.
• If residency was completed within the past two years, and if Level 2 wasattained during residency, then a lesser degree of training may be acceptable,to be determined by the cath lab director in consultation with the trainingprogram director where the residency training was done.
Recommendation 3: That physicians who previously performed diagnosticcatheterization independently but have a period of absence of greater than one yearfrom this activity undergo retraining as follows:
• If the period of absence was greater than 10 years, then training shouldinclude the attainment of Level 1 before proceeding to Level 2.
• If the period of absence was greater than two years, but less than 10 years,then training to achieve Level 2 of the CCS standards is required.Attainment of Level 1 can be assumed, and training can immediately applytowards attainment of Level 2.
• If the period of absence was less than two years, then the retraining shouldbe governed by the CCS standards on retraining.33 The specific re-trainingprogram must be agreed on with the Cath Lab Director.
32 Canadian Journal of Cardiology, May 1996. These standards are reproduced in Appendix 20 forreference.33 Canadian Journal of Cardiology, May 1996, p 471.
Page 31
Expert Panel on Invasive Cardiology in Ontario
5.1.2.1 Training for PCI
The Panel considered in detail many issues related to training for PCI:
• Interventional training involves more than learning the mechanics of coronary dilationand stent placement. The skills needed by all interventional cardiologists includevascular access (radial as well as femoral), diagnostic angiography of the highest qualityin order to guide the intervention, the use of vascular closure devices, appropriate use ofpharmacologic adjuncts, radiation safety, and a basic exposure to (if not independentproficiency with) some of the niche devices such as atherectomy and thrombectomy usedin contemporary interventional practice. Exposure to the entire spectrum ofinterventional practice, including case selection, pre-assessment, post-procedure care andpatient counselling is also an essential component of interventional training.
• In order to acquire these skills, the trainee must be involved in a substantial number ofprocedures, with an increasing degree of independence, during his/her formal training.Although the number of procedures alone does not define the adequacy or the quality oftraining (and it is therefore inappropriate to focus solely on this number), there is awidely held belief that a minimum standard in this regard is necessary.
• What is an appropriate minimum number of cases during training? Published guidelinesrange from 200 to 400 cases. In 1998 the ACC published a report specifically addressingtraining and maintenance of competence, and recommended 250 procedures as aminimum, with 400 considered optimal. The 2001 revision of the ACC/AHA guidelinesfor PCI endorsed the same recommendation for training. Expert opinion also suggested250 to 300 cases in training. Coronary stents and new pharmacologic agents dofavourably influence the outcome of interventional procedures, but only when they areused optimally. The availability of such tools has not lessened the complexity of PCI northe training needed to perform PCI. In fact, because these tools (and others) havebroadened the scope of PCI, older and sicker patients are undergoing the procedure moreoften and have added to the complexities of care.
• Although serious PCI-related complications are less frequent than in the past, all traineesmust have experience managing such complications if irreversible adverse outcomes areto be avoided or minimized. In order to acquire such experience, the trainee mustparticipate in a greater number of cases overall within a supervised context than wasnecessary several years ago.
• PCI volume has increased in most interventional centres, as has patient throughput perunit of time as average procedure duration has come down. This allows trainees toparticipate in many more cases within a given time period than was possible in the past.Those currently undertaking interventional fellowship training generally participate in250 to 500 cases per year, depending on the number of trainees at the training institutionand the amount of time spent doing research.
• Interventional training requires a period of full-time training. The trainee must be able todevote his or her attention primarily to the acquisition and refinement of the necessaryskills, judgement, and knowledge base. Immersion, in this context, does not necessarilymean full-time in the cath lab itself. It does imply full-time involvement in interventionalcardiology, whether that be the procedures themselves, or the selection, pre-and after-careof patients, or research and education related to PCI. Besides a great many hours spent inthe cath lab itself, the trainee should be available, at least during a portion of his/hertraining, for the ad hoc assessment of patients and angiograms that takes place frequentlyin most busy interventional centres.

Page 32
Expert Panel on Invasive Cardiology in Ontario
The Panel discussed at length the mechanism and requirements by which a physician currently inpractice and currently performing independent diagnostic cath could become trained to performPCI. The following points were noted in this regard:
• Experience as a practicing cardiologist is undoubtedly helpful in terms of understandingthe potential role and limitations of PCI, and placing it in context with alternativetreatments. Similarly, experience in performing diagnostic cath contributes some of thetechnical skills needed to perform PCI. It is difficult, however, to quantify the value ofsuch experience on an individual basis in order to modify the amount of training required.
• A number of individuals currently performing PCI did not participate in a formal trainingprogram. Some were among the earliest practitioners (and pioneers) of the procedure,when little or no formal training was available. Others have been trained by performingcases under the supervision of their interventional colleagues, often at their own centre,for a variable length of time. However, the overwhelming majority of cardiologists whohave begun interventional practice during the past five to ten years in Ontario and acrossCanada have been recent graduates of cardiology residency programs who havesupplemented their training with one or more years of full-time interventional fellowshiptraining. This is the format and minimum duration for interventional training specifiedby the CCS Standards; in addition, other professional bodies and virtually all of thenational and international opinion leaders proposed similar standards for training. Thefact that there have been a small number of exceptions to these standards does notundermine their validity.
• Undertaking full-time training is undoubtedly difficult for a cardiologist in practice.Coverage is needed for all of the existing clinical responsibilities of the practice (e.g.,outpatient care, hospital coverage, supervision and interpretation of non-invasive tests).Such coverage may be difficult to arrange because most cardiologists are very busy andhave little capacity to cover for their colleagues, and there are few trained cardiologistsavailable to provide locum coverage. There are also financial implications for thepracticing cardiologist - a large reduction in income (the salary typically paid to aninterventional trainee is at most equivalent to that of a senior cardiology resident) and theneed to continue covering at least some practice overhead costs.
The Panel was sympathetic to the potential difficulties faced by cardiologists in practice wishingto undertake training for PCI. However, the following arguments persuaded the Panel that analternate or substitute means of training was not appropriate:
• While some individuals may over the course of their career demonstrate exceptionalproficiency and become practice leaders, there is no justification for a system in whichpractitioners are targetted to “first tier” or “second tier” status from the outset. Rather,there must be a set of minimum standards that all trainees achieve during training.
• The capacity analysis detailed in earlier sections and in Appendix 17 suggests that, givensufficient financial support, the current training structure of full-time fellowships iscapable of meeting the need for new interventional cardiologists in Ontario over the nextfive years. A major change in the nature or duration of interventional training in responseto a perceived crisis is not needed and cannot be justified.
• The data on physician-specific procedure volume indicate that most practicinginterventional cardiologists devote a substantial portion of their professional time to thisactivity. Hence, the decision to train in and practice interventional cardiology representsa significant alteration in career focus for the practicing cardiologist who has notpreviously performed PCI. In general, mid-career changes of this magnitude by necessity

Page 33
Expert Panel on Invasive Cardiology in Ontario
involve a degree of personal sacrifice. This is analogous in some ways to the opportunitycost absorbed by those cardiologists who choose to spend one or more years in a full-timeinterventional fellowship after completion of cardiology residency.
The above notwithstanding, there are undoubtedly cardiologists in practice who could, withappropriate training, become excellent interventional cardiologists. Furthermore, while thecapacity analysis suggests that there is not a need to train currently practicing cardiologists to dointerventional work on a large scale, it may be necessary for a limited number to re-orient theirprofessional activities in this direction over the next five years. The issues outlined aboveindicate that some means of facilitating this training is necessary. However, rather thanfundamentally altering the structure and content of training, a more appropriate solution to thedifficulties faced by the practicing cardiologist would be to provide financial and logistic supportto at least partially offset the loss of income and the gap in practice coverage.
A practicing cardiologist wishing to train in PCI would be expected to already have significantexperience independently performing diagnostic cath, in addition to general clinical experience.Furthermore, he/she would not necessarily have the same interest in research activities that a“new graduate” interventional fellow might have. In these circumstances, it is conceivable thatthe training goals could be achieved with a shorter full-time component (six-month minimuminstead of 12).
The minimum procedure volume for training recommended herein is somewhat higher than otherpublished guidelines. The Panel believed that this was justified on the basis of the foregoingdiscussion, and, in reference to other guidelines, for the following specific reasons:
• The current Canadian Cardiovascular Society standards were published in 1996, and werenot believed to fully reflect the current complexity of PCI procedures and the other issuesoutlined above.
• This latest revision of the American College of Cardiology/American Heart Associationguidelines (released May 2001, for publication in June 2001), while endorsing aminimum training volume of 250 procedures, represent a 100% increase from theprevious (1993) guideline.
• The Canadian training standard has historically been more stringent than that in the U.S.,and the Panel believed that the arguments presented above justified a continued, albeitsmaller, discrepancy between minimum training volumes.
• Recommendations regarding specific procedure training (such as PCI) from otherjurisdictions must be considered in the context of differences in the overall structure ofcardiology training. For example, the recommendation of 200 training procedures fromthe British Cardiac Society was not seen as directly applicable to Ontario given thegreater degree of structure that surrounds cardiology training in general in Canada.
A minimum standard for training should be stringent enough that the majority of those reachingthis level can reasonably be expected to have acquired the necessary skills and behaviours. Onthe other hand, the minimum should not be so stringent that the majority of trainees are forced tocontinue formal training when the return, in terms of additional skill and knowledge acquiredrelative to time invested, is diminishing. While a minimum requirement for training thereforerepresents a certain trade-off at a group level, it is important to emphasize that it does notrepresent the optimal or even the minimum training needed by a given individual. Eachindividual trainee must have regular assessments of their progress, with specific adjustments totheir program as necessary, recognizing the potential need for additional training beyond theprocedure volume and program duration specified in the minimum standard. Although 300

Page 34
Expert Panel on Invasive Cardiology in Ontario
procedures is recommended herein as the minimum training volume for PCI, the Panel believed,based on expert opinions available to it, that an optimal training experience would encompass atleast 400 procedures.
Although a minimum duration of training is specified, the Panel has not provided an explicitmaximum duration of training. However, it is clear that the length of the training period shouldallow for a sufficient concentration of experience to meet the training needs. Therefore, a centrethat agrees to provide training should be confident that it can provide adequate case volumes forthe trainee(s) to complete their training within a reasonable time.
Recommendation 4: That physicians who have not previously performed independentPCI and now wish to do so undergo training as follows:
• If the physician has no previous training in PCI, the physician must undergotraining to attain Level 3 of the CCS Standards (i.e., minimum 12 monthsimmersion PCI training). During the entire training period, a minimum of 300procedures must be performed. Note that this is altered from the CCS Level 3Standard of 250 procedures.
• For a cardiologist currently in practice who has performed independentdiagnostic catheterization for at least two years, the minimum period ofimmersion training may be shortened to six months, provided that this ispreceded or followed by a period of “part-time” training lasting at least sixmonths. During the immersion training period, 150 cases must be performed,and the same minimum standard of 300 total cases during training isapplicable.
• If PCI training was previously undertaken and Level 3 of the CCS standardswas attained, but more than five years have elapsed since the end of thattraining, then the physician must undergo training to re-attain Level 3 of theCCS Standards. In this situation, of the minimum 12 months total training, aminimum of six months must be immersion. During the entire training period,a minimum of 300 procedures must be performed.
• If more than two but less than five years have elapsed since completion of PCItraining, and Level 3 was attained during the training, then the physician mustcomplete a minimum of six months of training, three months of which must beimmersion. During the entire training period, a minimum of 150 proceduresmust be performed.
• If less than two years have elapsed since completion of PCI training, andLevel 3 was attained during the training, then a lesser degree of training maybe acceptable. The amount, duration, and nature of training should bedetermined by the Cath Lab Director in consultation with the training programdirector where the PCI training was done.

Page 35
Expert Panel on Invasive Cardiology in Ontario
Recommendation 5: That physicians who previously performed PCI independentlybut have a period of absence of greater than one year from this activity undergoretraining as follows:
• If the period of absence was more than five years, then the physician mustundergo training to attain Level 3 of the CCS Standards. In this situation, ofthe minimum 12 months total training, a minimum of six months must beimmersion. During the entire training period, a minimum of 300 proceduresmust be performed.
• If the period of absence was more than two years but less than five then thephysician must complete a minimum of six months of training, three monthsof which must be immersion. During the entire training period, a minimum of150 procedures must be performed.
• If the period of absence was less than two years, then a lesser degree oftraining may be acceptable. The amount, duration, and nature of trainingshould be determined by the Cath Lab Director.
5.1.2.2 Supervision and Mentoring of New Operators
There is no formal process to integrate newly trained invasive cardiologists into independentpractice, although some guidelines suggest a mentoring program. Panel members felt that evenafter a cardiology residency program or after having been in practice, the newly trained invasivecardiologist may not be prepared to cath on a fully independent basis. He/she may be technicallyproficient, but not yet possess the necessary experience and confidence.
The cath lab director should ensure that during the initial period of independent invasive practice,a newly trained cardiologist is subject to an appropriate degree of supervision, and has readilyavailable support (i.e. on-site presence) from an experienced operator. While such supervisionand support should continue on an informal basis indefinitely, the period for which it is moreformally required will likely vary according to the individual involved and the practiceenvironment. The cath lab director should provide any new operator with frequent informalfeedback, and should conduct a formal evaluation sometime during the first year of independentinvasive practice.
Recommendation 6: That newly trained invasive and interventional cardiologists besupervised by an experienced operator and be subject to interim evaluations ofcompetence at three and six months. During this six month period, a cardiologistexperienced in cath or PCI should be available on-site whenever the newly trainedphysician is performing procedures.
Regardless of the initial training, supplementary training, or retraining required, the need formentorship during the initial period of independence applies as it does for new graduates oftraining programs.
5.2 MAINTENANCE OF COMPETENCE
A consistent volume-outcome relationship has been demonstrated in a number of studies,particularly when outcome is defined by the rate of major complications. It is clear that there is a
Page 36
Expert Panel on Invasive Cardiology in Ontario
low volume threshold below which complication rates rise. Fewer studies have looked at thevolume-outcome relationship at much higher procedure volumes, but those that did havedemonstrated a further reduction in complication rates for operators at the high end of theprocedure volume distribution.
Although the concern about complication rates is heightened in very low volume operators, thestatistical “low-volume paradox” makes this concern difficult to substantiate. This is becauseoperators with the lowest procedural volume will have the widest confidence intervals aroundestimates of their complication rates, limiting the ability to identify outliers with confidence.
Published guidelines generally provide minimum procedure volumes for maintenance ofcompetence. However, care is not necessarily optimized by having a large number of operatorsattaining or just exceeding minimum volumes. Where feasible, it is desirable that invasiveprocedures be concentrated among a relatively limited number of operators so that each operatorperforms many more procedures than the minimum needed to maintain competence. This allowseach operator to acquire sufficient experience with problem solving in a broad range of clinicalsituations, and to acquire and maintain technical skills that are highly specific but infrequentlyneeded – for example, to deal with a serious but rare complication.
Procedure volume is acknowledged to be a surrogate measure for clinical and technicalcompetence, and is best viewed as a necessary but not sufficient condition for ensuring qualityoutcomes. In addition to minimum volume standards, maintenance of competence must includeparticipation in an on-going quality assurance program that involves review of procedural safety(complication rates) and efficacy (diagnostic quality for cath and long-term outcome for PCI).Participation in continuing medical education specific to the type of procedures being performedis also essential.
If PCI is performed where on-site cardiac surgery is not available, the operator should be highlyexperienced, in order to increase the likelihood that he/she has the necessary skill and judgment toappropriately manage any complications that may arise. For this reason, the Panel believes that ahigher standard for the maintenance of competence should apply to interventional cardiologistswho practice at sites without on-site surgery.
The environment in which the operator practices appears to have a significant influence on thequality and outcome of his or her procedures (see Institutional Standards in the next chapter). Arelatively low volume operator may perform better in a high volume institution with continualexposure to more experienced cath, PCI, and surgical operators.
The Royal College has recently implemented a mandatory Maintenance of Certification programfor specialists. However, this program does not address procedure-related maintenance ofcompetence issues like minimum volumes. Monitoring operator adherence to minimum volumestandards, and other essential aspects of maintenance of competence specific to invasiveprocedures, is encompassed within the quality assurance responsibilities of the cath lab and theinstitution in which the operator works. (See the next chapter.)
Recommendation 7: That the Standards for Maintenance of Competence in CardiacCatheterization of the Canadian Cardiovascular Society34 be adopted as the minimumstandard (i.e., 150 procedures per year).
34 Canadian Journal of Cardiology, May 1996.

Page 37
Expert Panel on Invasive Cardiology in Ontario
Recommendation 8: That the Standards for the Maintenance of Competence inCoronary Angioplasty of the Canadian Cardiovascular Society35 be adopted as theminimum standard (i.e., 100 PCI procedures per year). For interventionalcardiologists who perform some or all of their procedures at a centre without on-sitecardiac surgery, the minimum standard is 150 procedures/year.
35 Canadian Journal of Cardiology, May 1996.

Page 38
Expert Panel on Invasive Cardiology in Ontario
6. INSTITUTIONAL STANDARDSThe Panel was also asked to develop recommendations on institutional standards for the provisionof invasive cardiology services. Those recommendations, and the rationale for the specificrecommendations, are presented in this chapter.
6.1 INFRASTRUCTURE REQUIREMENTS
The Panel felt that any invasive cardiology program required a minimum infrastructure to enableit to perform to high standards of safety and efficacy.
Recommendation 9: That MOHLTC require all centres providing invasive cardiacservices to maintain an infrastructure that enables it to perform to high standards ofsafety and efficacy, including:
• An annual review process to ensure that:o All operators achieve minimum procedure volumes.o The centre performs a minimum of 500 diagnostic cath procedures and
400 interventional procedures (where PCI is provided)• Training and credentialing standards for physician, nursing and technical staff.
The physician standards should, at a minimum, be consistent with therecommendations in this report.
• Sufficient number of operators performing PCI to ensure the availability ofPCI services 24 hours a day, seven days per week. Ideally, this would implythat there be at least three PCI operators affiliated with the centre.
• Supporting clinical and facility infrastructure, including, for example, imagingfacilities, acute care beds, nursing coverage, and pharmacy.
• A medical cath lab director who is responsible for training, credentialling andquality assurance.
• An appropriate administrative structure.
• On-site cardiac surgery or formal arrangement for off-site surgical back upwith documentation that safety is not compromised by this arrangement (SeeRecommendation 20.)
6.2 QUALITY ASSURANCE
Both safety and effectiveness are critical components in the quality of care.
Safety reflects the probability of an adverse event or outcome, such as death or a life threateningevent, or a complication that can later affect the quality of life or create a need for additionaltherapy or intervention. Objective measures for safety include the types of event-related dataelements that are already tracked at cardiac centres.
The effectiveness of a procedure reflects:
• Achievement of the desired outcome. An effective cath provides sufficient informationfor the interventionalist or the surgeon to properly plan the revascularization. If a secondcath must be performed, the first cath was not effective. Similarly, the need for repeatrevascularization after PCI may be a result of an ineffective procedure. Although this
Page 39
Expert Panel on Invasive Cardiology in Ontario
does not necessarily indicate a poorly performed procedure, it is not entirely independentof the skill and effort of the operator in that the attainment of a larger angiographic lumen(which might require added skill and effort to achieve) is associated with a lower risk ofrestenosis.
• The appropriateness of the procedure. The interventional cardiologist makesrecommendations and decisions for each patient trading off PCI and other therapies (e.g.,CABG, thrombolysis). Once PCI is determined to be the procedure of choice, thecardiologist must further determine the specific parameters of that procedure, by decidinghow many vessels to treat, how many and what type of stents to use, and what otheradjunct therapies might be required.
The cath lab director (or invasive program director) assumes significant responsibilities related toquality assurance. Because of these responsibilities, the minimum experience for this role shouldbe higher than for an invasive cardiologist without this responsibility.
Recommendation 10: That the MOHLTC instruct all centres providing invasivecardiology services to demonstrate that the institution has a quality assurance programin place to document that the standards for safety and efficacy are in fact met. Thefoundation of such a program will be the establishment and ongoing maintenance of adatabase to collect and analyze (at a minimum) the following data:
• Operator and cath lab volumes.• Demographic, clinical, and co-morbidity data.• Major complications (with standard definitions across all institutions,
including standardized protocol for peri-procedural enzyme evaluation):o Death, emergency surgeryo Peri-procedural MI, peri-procedural stroke.
All centres should have an internal process for review of appropriateness and quality ofdiagnostic angiograms under the direction of the Cath Lab Director. The reviewprocess should include participation from an interventional cardiologist and cardiacsurgeon, even at stand-alone cath labs.
In the longer term, the database should be expanded to include effectiveness measures(again with standardized definitions) such as:
• TVR rate (repeat angioplasty or surgery)• Survival rate for AMI interventions• QOL, return to work, symptom and activity measures.
CCN should coordinate, through an existing working group, and with input fromappropriate professional organizations, standardized definitions and assessmentprotocols for the data elements mentioned above.

Page 40
Expert Panel on Invasive Cardiology in Ontario
Recommendation 11: That the findings of each institution’s QA program be reportedto a central body for review and eventual dissemination, and that public accountabilitybe established through this process. Further, that since the cath/PCI databases of CCNalready contain relevant data elements (e.g., demographics, co-morbidity), and giventhe precedent that exists for cardiac surgery, that CCN serve as this central body. Toenhance the validity of the overall QA process, periodic data validation, includingaudits against source records, should be undertaken in collaboration with an armslength body (e.g., ICES), similar to the current process for cardiac surgery.

Page 41
Expert Panel on Invasive Cardiology in Ontario
7. TRAINING ISSUES
7.1 TRAINING PROGRAMS
Several existing guidelines indicate that training should take place within a formal structuredtraining program. The essential components of such programs were gleaned from the existingguidelines, as well as from the solicited expert opinions, and also by way of analogy with thegeneric structure of Royal College training programs. Once it is acknowledged that trainingprograms should meet specified criteria, it follows that there should be periodic accreditation oftraining programs. The following subsections provide detail on the structure, location, andoversight of training programs for invasive procedures.
7.1.1 Program Structure
There was a widely held belief that invasive procedures are becoming more, rather than less,complex due to their increasing applicability to patients with unstable conditions or multiplecomorbidities. Furthermore, for interventional procedures (PCI) in particular, the incorporationof various adjunct techniques and pharmacology into the standard therapeutic armamentarium hasvastly expanded the technical skill set and knowledge base required. As a result, the Panelbelieves that the need for a formal structure around training in these procedures is greater thanever.
The Panel believed that any training program for invasive procedures must have all thecomponents that an accredited Royal College program possesses. In the context of invasiveprocedures, these components include:
• Standards for the institution and the individuals providing the training (see Section7.1.2.2).
• A designated Training Director and Education Committee.
o Accountability for the structure and performance of a training program must beestablished through a designated Director, who should be assisted by an EducationCommittee. The Training Director need not be the Cath Lab Director, although itwould seem prudent that the Cath Lab Director should be a member of the EducationCommittee. This committee would be responsible for ensuring that the trainingprogram meets the standards set out in this section, for selecting suitable candidatesfor training, and for providing formal evaluation to trainees.
• A selection process to identify suitable candidates for training.
o This applies in all situations but would be particularly important if there are manypotential trainees interested in a limited number of training positions. The specificselection criteria do not have to be uniform across all programs, but should reflectcertain common features and should be documented in advance.
• Explicitly documented training goals and objectives.
o This is a fundamental component of any training program. From the outset, thetrainee and the trainers need to know the essential knowledge, skills, and behavioursthat must be acquired during training. While the full set of goals and objectives neednot be identical to all training programs, there is a core set that is common and mustbe adopted by all programs. Professional bodies such as the ACC/AHA and the

Page 42
Expert Panel on Invasive Cardiology in Ontario
Society for Cardiac Angiography and Intervention (SCAI) have developed traininggoals and objectives. The Panel believes that these form a reasonable starting point,although there may be value in customizing or modifying these objectives for theCanadian context, and that the CCS and/or CAIC may have a role in doing so.
o The essential aspects of a training program should allow the trainee to graduallyassume an increasing degree of independence and responsibility while functioningunder a sufficient degree of supervision.
• A formal evaluation process.
o Feedback must be provided to all trainees regarding their progress in attaining thegoals and objectives of training. While ongoing informal feedback on a day-by-dayor even case-by-case basis is important, formal evaluation with writtendocumentation is essential at interval(s) during the training and on completion oftraining. The Panel felt it was important to emphasize once again that completing therequisite number of procedures does not in itself ensure competence, nor does itconstitute satisfactory completion of training. In addition to fulfillment of minimumprocedure and time requirements, successful completion or training requiresconcurrent documentation (in the form of one or more written evaluations), that thetrainee has, in the opinion of the Training Director and/or Education Committee,acquired sufficient knowledge and skill to be able to perform such proceduresindependently.
o The Panel is cognizant of the fact that this evaluation process imposes a substantialresponsibility on the Training Director and/or members of the Education Committee(with potential legal ramifications), without the benefit of a formal framework suchas might exist within an accredited Royal College program. Nonetheless, the needfor a transparent evaluation process is paramount, and it is hoped that this report andits recommendations provide a structure within which this responsibility can bedischarged. An external review of training programs (see below) would furthersupport the credibility and legitimacy of the evaluation process.
o There should be no assumption that all trainees will acquire competence within thesame time frame. The Panel was reminded of one of the fundamental tenets of adulteducation, namely that individuals learn at varying rates. The evaluation process is,therefore, essential to identify those individuals who may require additional time orcase numbers beyond the specified minimums, and document the underlying reasons.Furthermore (as noted previously), there can be no a priori assumption that a giventrainee embarking on a training program will successfully complete such training andbe considered competent to perform procedures independently. Once again, a formalevaluation process is essential in order to identify such individuals, and to do so in asensible yet objective manner.
• An external review process (see Section 7.1.2.2 below).

Page 43
Expert Panel on Invasive Cardiology in Ontario
7.1.2 The Training Environment
7.1.2.1 Presence of a Royal College Training Program
The CCS Standards indicate that “Training should occur in a program recognized by the RoyalCollege of Physicians and Surgeons of Canada.”36 By definition, this has been the case for allinvasive training received within a cardiology residency program. In Canada, the majority offull-service cardiac centres are situated in University-affiliated teaching hospitals, and thereforemost training outside of a cardiology residency program has taken place in an institution with aRoyal College cardiology program. However, strictly speaking, such training (which includesfellowship training in angioplasty and cath or angioplasty training for the physician already inpractice), has not been within a Royal College program, because there is no formal Royal Collegedesignation or recognition of training in these contexts. (There is a provision in the CCSStandards that retraining can take place, under certain circumstances, “within the homeinstitution,”37 which may not be affiliated with a Royal College cardiology program. See page 19for the definition of retraining as used in this context.)
With the current development in Ontario of full service cardiac centres outside of University-affiliated teaching hospitals, the question arises as to the suitability of these centres for post-residency invasive training. In evaluating this question, the Panel considered the followingcompeting arguments:
1) The presence of a Royal College cardiology program within an institution impliesfamiliarity on the part of the teaching faculty with the various aspects of a formaltraining program, as specified in Section 7.1.2.2 below. In addition, a post-residencytrainee in an institution with a Royal College program would be exposed to a varietyof teaching and research rounds, with the opportunity (or expectation) to participatein research activities.
2) Having specified the standards for an invasive training program, if an institution candemonstrate that it meets those standards, then the fact that it is not university-affiliated and/or does not have a Royal College cardiology residency program shouldnot prevent it from offering invasive cardiology training.
The Panel was persuaded that full adherence to the standards for invasive training proposedherein, monitored by a practical external review process, would provide sufficient assurance as tothe quality and structure of a training program, and hence that the concomitant presence of aRoyal College cardiology program would not be an essential feature. At present, an externalreview process does not exist (see Section 7.1.2.2 below).
7.1.2.2 Characteristics of the Training Centre
A number of characteristics of the training centre and the physicians doing the training were feltto be extremely important in the overall quality of cath training:
• The overall volume of the centre.
• The number and experience level of the physicians and other professionals doing thetraining:
o There must be a sufficient number of willing and capable staff to participate intraining. This applies not only to physicians but to nursing and technical staff as
36 Canadian Journal of Cardiology, May 1996, p 470.37 Canadian Journal of Cardiology, May 1996, p 471.

Page 44
Expert Panel on Invasive Cardiology in Ontario
well, as both these groups are impacted by the presence of a trainee and have much tooffer the trainee.
o CCS standards state that physicians training others to cath “should be recognized asexperts in cardiac catheterization.”
o Exposure to more than one teacher, and hence more than one approach to problemsolving, is important (CCS standards state “more than one faculty cardiologist”).
• The case mix of the training centre:
o Trainees must be exposed to a spectrum of patient characteristics and procedural riskduring the time they are in a supervised environment, in order that they may developthe skills needed to deal with emergencies or unexpected outcomes as they arise.This is important even if the trainee does not plan to cath such patients in his or herpractice, since the potential for problems cannot always be anticipated nor avoided.If the training centre tends to select lower risk patients then the trainee will not havesufficient exposure to the high risk or difficult end of the spectrum.
o The opportunity to interact on a regular basis with interventional cardiologists andcardiac surgeon to build an awareness of contemporary capabilities and limitations ofboth interventional cardiology and cardiac surgery is essential in developing thejudgement necessary to make appropriate management decisions based on the cathresults.
• The maturity of the program offering training:
o A newly established invasive program requires a variable length of time to buildprocedure volume and the overall base of experience among physician, nursing,technical and administrative staff. For this reason, a program within the first one totwo years of being established is not an optimal environment for training.
Recommendation 12: That all training and retraining of physicians to perform cathand PCI take place within a structured training program with all of the requirementsand supporting infrastructure that is typically present in a Royal College program.Such a program would include, at a minimum:
• Standards regarding the qualifications of the training institution (e.g., trainingfor the trainers, volume and variety of cases, on-site surgery [to ensureexposure to a full range of patients and cases], academic activities such asrounds).
• A selection process that identifies which candidates be accepted for training.
• Explicitly documented training goals and objectives. At least a core set ofthese objectives should be common across all training programs.
• A formal evaluation process.
• An Education Committee that meets regularly to review the program,including a designated Director of Training.
• An external review process.

Page 45
Expert Panel on Invasive Cardiology in Ontario
7.2 ACCREDITATION OF TRAINING PROGRAMS
The Panel was concerned that some institutions offering training, and the individuals receivingthe training, have given insufficient consideration to existing guidelines and standards for suchtraining. There has been no adoption of a common standard for training (or for maintenance ofcompetence) for invasive procedures in Ontario.
Professional organizations can develop and disseminate training and practice standards, but itfalls to regulatory or administrative bodies to encourage, and ultimately ensure, the adoption ofsuch standards. For invasive cardiac procedures, this means individual hospitals (via the grantingof privileges for specific procedures, a process that has a defined legal basis), or individual cathlabs and cath lab directors (generally a less formal process with uncertain legal authority).
The training received during a Royal College accredited cardiology residency does notnecessarily satisfy the standards for invasive training advocated by most professional groups,particularly with respect to interventional procedures, for which a minimum one year post-residency fellowship program is generally recommended. There is no Royal Collegeaccreditation or recognition of either cath or PCI training taken beyond the cardiology residency,and hence no Royal College oversight of these training programs. In fairness, the Royal Collegecannot be expected to develop a formal training and certification structure for every newprocedure or knowledge element within a given specialty. When coronary angioplasty beganmore than two decades ago, “training” in a formal sense barely existed, and the eventual scope ofthe procedure could not have been foreseen.
Nonetheless, the developments that tend to define interventional cardiology as a distinctsubspecialty have been evident for many years now. Recently, the American Board of InternalMedicine established a new certification in Interventional Cardiology, available only to thosephysicians already holding certification in Cardiovascular Diseases (analogous to the previouslyintroduced certification in Pacing and Electrophysiology). This would appear to further signifythat the complexity and knowledge base of certain sub-specialties within cardiology haveadvanced far enough to warrant formal criteria for training and evaluation, along with formaldesignation of practitioners who attain the specified criteria.
This report advocates formal adoption of training standards for invasive procedures. Hospitalsand cath labs that are considering the granting of privileges to newly trained invasivecardiologists must have some assurance as to the quality and validity of the applicant’s training.In the absence of Royal College oversight of invasive training programs, an alternate form ofexternal review is therefore needed, and resources will have to be provided to support such aprocess. Because formal accreditation is a labour-intensive and a recurring process, a practicalsolution is needed that strikes a balance between cost and comprehensiveness. Further, the sameneeds exist in other provinces as well. Therefore, the Panel is recommending that MOHLTC askCCN to work with the Canadian Cardiovascular Society to develop and implement a process ofregular external review of invasive training, and that MOHLTC undertake to support such aprocess on an ongoing basis.
In the next section, funding support for the actual training programs is recommended. Ensuringaccountability for these funds is an additional argument in favour of a formal process of externalreview.
As an interim measure toward external review, it is suggested that all centres providing invasivetraining outside the cardiology residency program document their adherence to the trainingstandards specified herein. In addition, the Education Directors and/or Cath Lab Directors fromthese centres should meet on an annual basis to review, as a group, the adherence of each centreto these standards.

Page 46
Expert Panel on Invasive Cardiology in Ontario
Recommendation 13: That MOHLTC encourage stakeholder groups, including theCCS, to approach the Royal College of Physicians and Surgeons with the goal ofworking together to establish an accreditation process for invasive cardiology trainingprograms, and to explore the feasibility of establishing a Royal College certificate ofspecial competence in Interventional Cardiology.
Recommendation 14: Until an accreditation process for invasive cardiology traininghas been developed and implemented, as an interim measure each program offeringinvasive training outside the context of the Royal College cardiology residency shoulddocument in writing the centre’s adherence to the training standards proposed inRecommendation 12. Furthermore, the Education Directors and/or Cath Lab Directorsfrom each of these centres should meet at least once per year to discuss issues ofcommon interest and to review each centre’s adherence to the training standards.
7.3 FUNDING OF TRAINING
It will be evident from the preceding sections that much is expected, in terms of time andresponsibility, of the individuals and the institutions providing invasive training. The servicebeing provided is an essential one, as trained invasive cardiologists are needed and there is noother mechanism to provide such training. Consequently, these individuals and institutions mustbe compensated appropriately. Those receiving the training should also receive reasonable salarysupport. At present, there is no funding from MOHLTC for post-residency invasive training.Some fellows have been paid through funds donated to cath labs or cardiology programs byindustry, some have been paid by private endowments, and many have been supported out of thepractice income of their teachers.
The Panel believes that the need for interventional cardiologists can be met if, and only if, there issufficient funding to support the training of enough new specialists to allow a net increase of fiveto seven per year over the next five years. In the absence of such support, then, as pointed out bythe CCN HR report, "these shortages will become critical.”38 A more rational, stable, andpredictable mechanism for funding the development of essential specialists is needed.
Recommendation 15: That MOHLTC provide financial support for training in PCI.This support should include reasonable salary support for trainees and funds to offsetthe administrative and other costs of the training program itself, including the costsassociated with external review and accreditation. To qualify for such support, thetraining program must meet certain criteria as specified in Recommendation 12.
Recommendation 16: That MOHLTC ask CCN to convene a sub-committee withappropriate representation to assess in detail the costs associated with providinginvasive training, in order that specific recommendations regarding the amount ofsupport can be formulated. This assessment should include the costs associated withattaining a portion of training away from the trainee’s home institution.
38 A Discussion Paper by the Consensus Panel on Cardiovascular Human Resources in Ontario, FinalReport and Recommendations, June 2000.

Page 47
Expert Panel on Invasive Cardiology in Ontario
8. SUPPORTING INFRASTRUCTURE
8.1 EMERGENCY TRANSPORTATION
Ontario has developed a regionalized system for invasive cardiac services. This will remain trueregardless of whether PCI is initiated in the absence of on-site surgery or not. There are and willalways be a large number of hospitalized patients who require an urgent or semi-urgent invasiveprocedure and who must be transferred over variable distances to another hospital for such aprocedure. In light of the trend in clinical management toward an earlier invasive approach topatients with an acute coronary syndrome, the number of hospitalized patients requiring transferis rising and will likely continue to do so.
Such a system is entirely dependent on the availability of an efficient and reliable urgent medicaltransportation service. If patients cannot be transported efficiently and safely betweeninstitutions, then the entire concept of regionalization breaks down, and inequities of access basedon patients’ geographic location become far more pronounced.
All cath labs have shifted as much of their caseload as possible to an outpatient basis, in order toease the demand for in-patient beds. For those patients referred for a diagnostic cath while aninpatient at another hospital, timely ambulance transport is needed to and from the cath centre onthe day of the procedure. Relatively few transports qualify as emergent, but all involve patientswho are potentially unstable either from the underlying cardiac problem, or (on the return trip)from the effects of the procedure itself.
Deficiencies in the current service are evident. There is a chronic shortage of Department ofAmbulance Services vehicles and crews, resulting in frequent and lengthy delays for lowerpriority non-emergent hospital to hospital transports. Delays in arrival or pickup time can haveserious clinical impact in some situations, but more often the impact is on efficiency, asprocedures are delayed or cancelled, or overtime charges incurred.
Private patient transportation services are being used in many situations, but these services havesignificant limitations on the range of emergency care they can provide to patients who becomeunstable enroute. This obviously raises serious concerns about patient safety and medico-legalliability.
An adequate transportation infrastructure is an essential component of a regionalized system ofcardiac care, and must be adequately supported.
Recommendation 17: That MOHLTC provide sufficient funding for a transportationinfrastructure that is capable of providing reliable and efficient service to allow optimalutilization of a regionalized system. Because this affects all invasive cardiac centres inOntario, as well as all referring physicians and institutions, MOHLTC should workwith CCN to review this issue and coordinate a response. This work should beginimmediately.
8.2 COMMUNICATION INFRASTRUCTURE
The ability to rapidly transmit high quality digital images between centres can enhance the qualityand timeliness of care when cath facilities are remote from revascularization services, and is

Page 48
Expert Panel on Invasive Cardiology in Ontario
absolutely essential for safety if PCI is provided at a site geographically separated from a surgicalcentre. Various technology options exists (e.g. dedicated high bandwidth linkages, shared widearea network, or Internet based) with corresponding cost-performance tradeoffs. These linkagescan also be used to electronically transmit non-image portions of patient records (as institutionsmove to electronic records) when speed is essential, for example to facilitate transfer foremergency surgery. Network integrity and security issues must be considered.
Recommendation 18: That MOHLTC coordinate and support the development of anelectronic network to permit rapid and secure transfer of digital angiographic imagesand other relevant clinical data in order to facilitate timely referral of patients betweencentres.
8.3 RESEARCH
Recommendation 19: That research continue (and be updated) into the relationshipbetween institutional and operator characteristics (such as, but not limited to, procedurevolume) and outcomes of invasive cardiac procedures. Specifically, that such researchbe extended to encompass not only complications but also efficacy measures, such as,for example, long term freedom from reintervention and symptom status.

Page 49
Expert Panel on Invasive Cardiology in Ontario
9. LOCATION OF INTERVENTIONAL CARDIOLOGY SERVICESA number of care providers and stakeholder groups have urged MoHTLC to fund PCI at centresthat do not currently have on-site cardiac surgery. While the Panel’s mandate did not encompassthe evaluation of specific proposals, it was asked to consider the safety and desirability of PCIwithout on-site cardiac surgery, within the context of various options to achieve the proposedvolume targets while maintaining quality of care.
9.1 EVALUATION CRITERIA AND PERSPECTIVE
The Panel evaluated options based on the degree to which each could provide the desirableattributes of care: quality, timeliness, and proximity. Because MOHLTC indicated that economicefficiency would be evaluated in the course of assessing any specific proposal, this parameter wasnot considered by the Panel in a generic sense. For the purpose of this discussion, quality wasprimarily defined by procedural safety, which in turn was based on the attainment of minimumvolume criteria. The use of procedure volume as a surrogate measure for quality is based on thevolume-outcome relationship noted in the literature review. However, there are clearly otherrelevant components of quality including, for example, the degree to which the procedureachieves its goal(s) (e.g., sustained relief of symptoms, prevention of MI, the avoidance of minorcomplications, and overall patient satisfaction).
The care attributes may overlap if procedural safety and outcome are taken to be equivalenteverywhere – for example, an earlier procedure (timeliness) may be associated with less riskwhile waiting (quality), and a procedure closer to home (proximity) might be done sooner(timeliness). However, because of the nature of interventional cardiology procedures and thedependence on volume and experience, it is not possible to simultaneously optimize quality,timeliness, and proximity – certain trade-offs are inevitable.
Options for the location and organization of care can be viewed from different perspectives – thatof the individual patient, the individual provider, institutions, regions, and system-wide – and theattractiveness of the view often differs according to the perspective. While most of theseperspectives were directly represented on the Panel, members were urged to consider all of therelevant perspectives and not only their own, when evaluating various options.
9.2 RATIONALE
The Panel identified a number of factors that suggest that PCI can be performed in selectedcentres without on-site surgery:
• The literature review (and the Panel’s experience) indicated that PCI is commonlyperformed without on-site cardiac surgery in some jurisdictions (e.g., Germany), but thepractice has been much less common in North America. In the United States, onesource39 estimates that 68 sites perform PCI without on-site cardiac surgery (out of a totalof approximately 800 PCI programs), but only 22 of those sites perform elective PCI, andmany of these sites have very low volumes. In Canada, the Panel identified only four
39 Thomas P Wharton Jr MD, et al, Non-Emergent Coronary Intervention Without Cardiac Surgery OnSite: Outcomes in 2,645 Patients in the US Poster presentation at the 73rd Scientific Sessions of theAmerican Heart Association New Orleans, LA, November, 2000, Circulation 2000;102:II-731-2

Page 50
Expert Panel on Invasive Cardiology in Ontario
such sites40 (out of approximately 42). There are no randomized controlled trialscomparing outcomes at institutions with and without on-site cardiac surgery, and thePanel could not identify any comparisons of outcome between sites with and withoutcardiac surgery that adjusted for variation in the baseline characteristics of the patientpopulations. There were publications reporting unadjusted outcomes of PCI at siteswithout on-site cardiac surgery; in general these were comparable to benchmark ratesoverall. Note that “outcome” in this context essentially refers to the rates of death andemergency bypass surgery.
• The acute procedural risk of PCI, particularly the need for emergency bypass surgery, islower than it was prior to the widespread use of stents. Published and unpublished dataconfirm that complication rates have decreased significantly in recent years. Careful caseselection may make it feasible to selectively refer high-risk cases to centres with on-sitesurgery.
• Technology exists to permit the immediate electronic transfer of digital images from onelocation to another, facilitating real-time interaction with an off-site cardiac surgeon.
• Even where cardiac surgical services are provided on-site, it may take longer thananticipated to move a patient from the cath lab to the operating room (OR) because of avariety of factors (e.g., time to consult with cardiac surgeon, time until OR is available).Some sources suggested that a well-organized emergency transport service could providetransfer times between institutions that are comparable to the time required within aninstitution with on-site cardiac surgery.
• Allowing local centres to provide PCI (without on-site cardiac surgery) could potentiallyimprove access to catheterization services through more timely service (e.g., shorterwaiting times), and the delivery of care close to patients’ place of residence.
• Providing both cath and PCI at one site (rather than just cath) allows the provision ofad hoc PCI when appropriate, which may enhance the efficiency of resource use andreduce the net waiting time for PCI.
Although the above factors all support the expansion of services to allow PCI without on-sitesurgery, the Panel also identified several factors that suggest caution because of potentialimplications for the safety and effectiveness of the procedure. While case selection wasidentified as a potential approach to minimizing the probability of emergency CABG, many ofthe complications that may arise during PCI are not directly related to underlying patientcharacteristics, and are thus “unpredictable” in the sense that prior risk stratification would notnecessarily have triaged such patients to a centre with on-site cardiac surgery.
The implications for the relationship between the cath lab and the surgical centre providingbackup must also be examined:
• Formal prior arrangements establishing a structure and mechanism for surgical backupwould need to exist between non-surgical centres wishing to provide PCI and a nearby ordesignated surgical centre, because of the potential communication and transportationdelays. If a surgical centre commits to being able to provide emergency backup for failedPCI from another centre, then this has resource implications at the surgical centre overand above its existing commitments.
40 Hôpital Hôtel-Dieu de Québec in Quebéc City, Centre hôspitalier Pierre-Boucher in Longueuil, Centrehôspitalier régional de l’Outaouais in Hull, and Royal Alexandra Hospital in Edmonton.

Page 51
Expert Panel on Invasive Cardiology in Ontario
• Continuous interaction between PCI and surgical programs was felt to be important toenhance the awareness of each other’s capabilities and limitations. In addition,interaction at an individual level between interventional cardiologist(s) and cardiacsurgeon(s) is important to develop and maintain a strong professional relationship inwhich there is inherent trust in each other’s clinical judgement. While the physicalseparation of PCI and surgical programs should not theoretically stand in the way of suchinteractions, it does demand additional effort, planning, and commitment.
• The actual time of surgical referral arising from a failed PCI is not always clear, andhence the contention that transfer to an OR from off-site can be effected as quickly asfrom on-site may not be fully accurate. In some centres with on-site surgery, the surgicalservice is consulted and attends in the cath lab (and thereby contributes to patientmanagement) even before a definite decision on the need for surgery has been made. Ifthe surgeon is off-site, there is no opportunity for this in-person consultation to occur.Although technology exists that could provide immediate transmission of digital images,the surgeon does not have the opportunity to review and speak with the patient directly.
• The medical transport infrastructure must be in place to provide a response that isconsistently rapid and able to deal with the complexities of an emergency cath labtransfer, which might include one or more arterial access sheaths, indwelling coronarycatheters, guide wires and balloons, an intra-aortic balloon pump, and possibleendotracheal intubation, and multiple intravenous infusions (including vasoactive drugs).
The Panel also identified issues regarding procedure volumes and the experience of the operatorsand supporting professionals:
• When planning new centres, there is a need to ensure that there will be sufficient criticalmass to support minimum procedure volumes for the operators and the institution.
• It was generally agreed (in the opinions received and among Panel members) that a centrewithout on-site surgery should have at least one highly experienced operator, or apartnership such that a highly experienced operator is present.
The Panel was aware of the fact that the Guidelines for PCI of the American College ofCardiology/American Heart Association (ACC/AHA) released in May 2001 included a Class I41
recommendation that PCI be performed only in centres with on-site cardiac surgery. Theseguidelines also include a Class IIb recommendation regarding necessary prerequisites should thedecision be taken nonetheless to implement PCI without on-site cardiac surgery. Therecommendation herein (#20) was felt to be consistent with the cautions expressed by theACC/AHA, while allowing a degree of flexibility to deal with issues of need, access, andgeography that may be unique to Ontario.
Acknowledging a degree of uncertainty surrounding the establishment of PCI without on-sitesurgery, the Panel felt that if and when this does take place, it should be on a limited scale (i.e.,
41 Class I: Conditions for which there is evidence for and/or general agreement that the procedure ortreatment is useful and effective.Class II: Conditions for which there is conflicting evidence and/or a divergence of opinion about theusefulness/efficacy of a procedure or treatment.
Class IIa: Weight of evidence/opinion is in favor of usefulness/efficacy.Class IIb: Usefulness/efficacy is less well established by evidence/opinion.
Class III: Conditions for which there is evidence and/or general agreement that the procedure/treatment isnot useful/effective, and in some cases may be harmful.

Page 52
Expert Panel on Invasive Cardiology in Ontario
preferably one, at most two centres) and with careful evaluation before being considered on abroader scale.
Recommendation 20: The weight of opinion clearly favours the availability of on-sitecardiac surgery in centres that perform angioplasty.
However, the Panel acknowledged that developments in angioplasty technology haveoccurred that may permit some flexibility in the organization of angioplasty services.
If the following criteria are met, then angioplasty without on-site cardiac surgery canbe considered as an option and established on a pilot basis:
• There should be documentation of need, which may relate to population-basedtargets, excessive waiting times or geographic considerations. It is outside thisPanel’s scope to develop specific criteria of need.
• There should be a formal evaluation of alternatives to meet the identified need,such as increased capacity at nearby full-service centre(s) (if one exists),and/or enhanced transportation and communication infrastructure.
• Projected volumes must be sufficient to support at least the minimum operatorand institutional volumes recommended for maintenance of competence.
• Sufficient human resources exist such that a new program can be staffed with asufficient number of providers (physicians, nurses, technologists) who havemet all the necessary training requirements.
• New programs have at least a minimum complement of highly experiencedinterventional cardiologists, nurses, and technical staff.
• A formal relationship is established with a full-service cardiac centre toprovide ongoing consultation and emergency surgical backup.
• A formal relationship is established with the emergency transportationprovider to ensure the capability exists to transfer the patient and associatedequipment in the event of an emergency, and that the appropriate protocols arein place to ensure rapid transport within an established time frame.
The development of a new cardiac centre (with or without on-site cardiac surgery), or asignificant expansion of an existing service, may have significant impacts on existing programs(and on those in development). As new facilities are proposed and developed, it is essential toconsider the system-wide impacts, including:
• A potential decrease in volumes at existing centres, possibly even below institutionalminimums. These reduced volumes may also affect individual operators who may decideto relocate from the existing centre (to follow the caseload). Their departure drains theexisting centre of procedural capacity and the other skills of an experienced operator.
• A potential under-utilization of capital resources (e.g., cath labs, including the imagingequipment), and other supporting infrastructure (e.g., CCU beds, outpatient beds).
• A shift in existing referral patterns. As more centres open, patients will have more choiceand may have more opportunity to have a procedure “close to home.”

Page 53
Expert Panel on Invasive Cardiology in Ontario
• A change in the case mix at existing centres. If stand alone centres, through caseselection, send higher risk patients to centres with on-site cardiac surgery, the case load atthe surgical centres (which are often also teaching centres) becomes, on average, morecomplex, which may impact upon efficiency, on the delivery of teaching, and on staffmorale.
• An increased demand on supporting infrastructure (e.g., emergency transport).
While the establishment of PCI facilities outside of surgical centres is one option to meeting PCItarget volumes, there are other potential solutions, including further expansion and/or longerhours (beyond what is currently planned or proposed) at existing centres, and enhancement ofinfrastructure to facilitate referrals (communication, transportation). These potential solutionscan also be evaluated for their ability to satisfy the attributes of quality, timeliness, and proximity.
Recommendation 21: That there be a formal assessment of the broader systemsimpacts (e.g., human resources, volumes, infrastructure) prior to the approval of anynew cardiac centre and significant expansion of services at an existing centre. Thisassessment should include the impact on existing programs and programs that arecurrently in development. The Panel recommends that the MOHLTC recognize theneed to pace the development of new centres.
The Panel had concerns about the expressed desire of some centres to provide PCI in the settingof acute MI (i.e., primary and/or rescue PCI) in the absence of an elective PCI program. Whilesome acute MI interventions are technically straightforward, many are not (there is no advanceknowledge of the coronary anatomy), yet all are carried out under extreme time pressure due tothe relationship between rapidity of reperfusion and successful outcome. Furthermore, the cathlab team is responsible not only for reperfusion of the infarct vessel, but also for generalmanagement of the patient during an acutely unstable illness, a task for which ongoing experienceis crucial. This was addressed in some of the guideline publications and by some expert opinions.The literature review (including a study [C-PORT42] recently presented but not yet published)includes data on the interaction between procedure volume and relative benefits of PCI vs.fibrinolytic therapy for acute MI.
The potential role of emergency PCI as either initial therapy (instead of fibrinolytics), or as rescuetherapy (for failed lytics) in remote geographical settings has been raised and was considered bythe Panel. As initial therapy in patients who are suitable candidates for lytic therapy, it wasagreed that a centre that does not perform PCI on an elective basis should not withhold lytictherapy in favour of emergency PCI for the reasons outlined above.
As rescue therapy for patients who fail to respond to lytic therapy, it is acknowledged that theremay be clinical benefit from PCI in selected cases, although as a broad strategy, this has beendifficult to demonstrate in prospective trials. The problem is that PCI in this patient group, whichtends to be sicker, have larger burden of thrombus, and have larger infarcts, is far morechallenging than routine PCI, and is associated with higher rates of complications, particularlybleeding. Furthermore, when such an intervention is successful, the success is often related to the
42 Aversane T, Atlantic Cardiovascular Patient Outcomes Research Team Trial of Primary PercutaneousCoronary Intervention vs Thrombolysis in Acute MI. Presented at the American Heart Association,November 2000.
Page 54
Expert Panel on Invasive Cardiology in Ontario
use of complex mechanical or pharmacologic adjuncts (e.g., thrombectomy catheters) for whichsufficient experience would not likely exist.
Recommendation 22: That emergency angioplasty for acute MI (direct or rescue PCI)not be performed in a centre that does not have an established elective angioplastyprogram.
Several stakeholders and secondary reviewers pointed out the importance of direct and rescuePCI in the care of patients with acute MI and expressed concern as to its availability. Issuesidentified include the desirability of a coordinated emergency referral and response system foracute MI patients, clearly obviating the need to contact multiple interventional hospitals in anemergency. The institutions currently providing PCI expressed concern at the lack of critical carebeds to support the broader use of interventional therapy for acute MI.
Recommendation 23: That MOHLTC request that CCN develop, either through adedicated Panel or an existing working group, a coordinated regional approach thatfacilitates the provision of emergency PCI services for patients with acute MI.
The Panel also recommends that MOHLTC support the necessary infrastructure toprovide, where appropriate, emergency PCI services to patients with acute MI with theeventual goal of providing these services on a 24/7 basis.
MOHLTC should also support one or more pilot projects to evaluate the feasibility andeconomic impact of providing these services on a 24/7 basis.

Page 55
Expert Panel on Invasive Cardiology in Ontario
Appendix 1: TERMS OF REFERENCE
Expert Panel on Invasive Cardiology in OntarioI. Preamble
In the past several years, the number of diagnostic and therapeutic catheterizationprocedures performed in Ontario has increased dramatically. This has been driven by theenhanced scope and effectiveness of revascularization, particularly angioplasty, and theresulting tendency to refer patients with known or suspected coronary disease forangiography earlier in the course of their management. The recent report of the TargetSetting Working Group indicates that these trends are likely to continue and in factintensify over the next five years. Consequently, the Cardiac Care Network (CCN) hasrecommended an increase in the population-based minimum target rate for angioplastyfrom 100 cases per 100,000 adult population (the province-wide rate in 2000/01) to 160cases per 100,000 by 2005, with a corresponding 51% increase in the rate of diagnosticcatheterization.
Meeting these new targets poses a significant challenge in terms of physical and humanresource infrastructure. In part this has been addressed by opening new catheterizationlaboratories and full-service cardiac centres (which include cardiac surgery). The newfacilities have also helped achieve the goal of delivering care “closer to home” for manypatients. However, the rapid pace of expansion has raised a number of important issuesrelated to the delivery of invasive cardiology services in Ontario. These issues includeappropriate training and quality assurance, the role of guidelines for operator,institutional and infrastructure requirements for invasive cardiology services, and theability to safely perform angioplasty procedures in centres without on-site surgicalbackup.
To address these issues, CCN has, at the request of the Ministry of Health and Long TermCare, convened an Expert Panel to provide advice regarding the delivery of invasivecardiology services in Ontario.
II. Purpose
The Panel will develop recommendations regarding operator, institution, andinfrastructure guidelines for the optimal provision of invasive cardiology services inOntario. These guidelines will be based on the best available evidence from around theworld, supplemented where appropriate by expert opinion.
III. Functions-Deliverables
1. Conduct a literature review of existing guidelines for diagnostic and therapeuticcatheterization procedures, and of literature relating outcomes to operator andinstitution training and volumes.

Page 56
Expert Panel on Invasive Cardiology in Ontario
2. Review existing literature regarding the performance of coronary angioplasty incentres without on-site surgical back up. Elicit expert opinion to supplementavailable literature on this issue.
3. Develop recommendations regarding institutional, operator, and infrastructurerequirements for the performance of diagnostic catheterization and angioplastyprocedures in Ontario.
4. Develop recommendations for the implementation of a quality assurance system forinvasive procedures in Ontario. This may include recommendations for furtherresearch as needed.
IV. Membership
ChairCathing cardiologist(s) from cath centreCathing cardiologist(s) from full-service centreNon-cathing community cardiologist(s)Cardiac surgeonHospital ExecutiveCCN RepresentativeICES Representative(s)Cath Lab Nurse/Nurse ManagerRegional Cardiac Care Coordinator
Ex-officio
CCN CEOMOHLTC Representative
V. External input
The panel will provide an opportunity for all interested parties to have input by way ofwritten submissions. In addition, the panel may choose to solicit expert opinion fromspecific individuals within or outside of Ontario on any particular issue. A preliminarydraft will be circulated to selected Secondary Reviewers and their feedback will beconsidered before finalization of the report.
VI. TERM
The panel will meet over a three-month period. Two to three day-long working sessionsand two to three (short) meetings will be required. The report of the panel is to becompleted and submitted to the Ministry of Health and Long-Term Care by March 31,2001.
VII. ACCOUNTABILITY
The recommendations of this panel will be presented to CCN’s Clinical ServicesCommittee and receive final approval by the CCN Committee prior to their submission tothe ministry.

Page 57
Expert Panel on Invasive Cardiology in Ontario
Appendix 2: CCN EXPERT PANEL ON INVASIVE CARDIOLOGY MEMBERSHIP
MEMBERS
Eric Cohen, (Chair) MD, Director, Cath Lab, Sunnybrook & Women’s College Health SciencesCentre
Debra Campbell RN, Regional Cardiac Care Coordinator, Kingston General Hospital
David Fell, MD, Medical Director, Cath Lab, Southlake Regional Health Centre
Avinash Garg, MD, Cardiac Surgeon, Hôpital régional de Sudbury Regional Hospital
Peter Gladstone, MD, Cardiologist, Rouge Valley Health System
David Gould, MD, Medical Director, Cardiology Services, Sault Area Hospitals
Curry F. Grant, MD, Cardiologist, Institute for Clinical Evaluative Sciences
Robert J. Howard, MD, VP Patient Care Programs/Chief Medical Officer, St. Michael’sHospital
Charles Lazzam, MD, Cath Lab Director, Trillium Health Centre
Roy Masters, MD, Cardiac Surgeon, University of Ottawa Heart Institute
Madhu K. Natarajan, MD, Director, Interventional Cardiology, Hamilton Health SciencesSven Pallie, MD, Cardiologist, Hotel Dieu Health Sciences Hospital, Niagara and Niagara HealthSystem, General Site
Jean Rouleau, MD, Chief of Cardiology, University Health Network, Toronto General Division
Don Shilton, Cath Lab Manager, Hamilton Health Sciences
EX-OFFICIO
Rob Forbes, Director of Informatics, CCN
Linda Hunter, Planning Consultant, Hospital Operational Support, Ministry of Health & LongTerm Care, Operational Policy and Priority Programs
Jillian Ross RN, Director, Projects and Operations, CCN
Marcella Sholdice, Project Manager, CCN
Rachel Solomon, Program Consultant, Hospital Operational Support, Ministry of Health andLong-Term Care, Operational Policy and Priority Programs
Mark Vimr RN, Chief Executive Officer, CCN

Page 58
Expert Panel on Invasive Cardiology in Ontario
Appendix 3: LITERATURE REVIEW
Angiography and Interventional Cardiology:A Review of Practice Guidelines and the Determinants of Procedure Quality
Curry Grant MD FRCPC MSc
Marcella Sholdice BA MBA
June 11, 2001
1. Introduction
Percutaneous transluminal coronary angioplasty (PTCA),∗ introduced by Andreas Gruentzig in1977, has evolved and improved over the years to become a safer and more effective procedurefor the improvement of quality of life and longevity in patients with coronary heart disease(CHD). In early years, the usefulness of the procedure was limited by re-narrowing (restenosis)of the coronary arteries in about a third of cases, and by the abrupt closure of the coronary arteryin 2-5% of cases. By today’s standards, these rates are high, with restenosis requiring arevascularization procedure now occurring in about 17% and abrupt closure requiring coronaryartery bypass graft (CABG) surgery in 1% or fewer cases in spite of rising proportions of urgentand unstable cases1.
The increasing safety of the procedure can be attributed to many factors, including theintroduction of coronary stenting in clinical trials in the early 1990s to complement PTCA. Thesetrials found stenting to be an effective treatment for abrupt coronary closure, as well as aneffective preventive measure for coronary restenosis. As well, safe, effective anticoagulanttreatments have become routine in the prevention of coronary artery blood clots due to theprocedure.
PTCA is now an alternative to CABG in many patients, including those with more extensiveCAD involving more than one artery. PTCA is increasingly being used to open occluded arteriesin patients with acute myocardial infarction (AMI), which is referred to as ‘primary’ or ‘direct’PTCA.
Because of the small likelihood of abrupt artery closure, it has been felt to be necessary to havepersonnel and facilities available for emergency CABG. As the safety of PTCA has improved,cardiologists at some centres in the United States, Europe and Canada have begun doing theprocedure without on-site surgery. Although PTCA is much less invasive than CABG, it is still acomplex procedure requiring a well-trained and experienced cardiologist, expert support staff,and an elaborate laboratory and hospital infrastructure.
The purpose of this paper was to review existing guidelines for PTCA, and the importance offactors including operator training and experience on PTCA outcomes. The potential forperformance of PTCA without on-site surgery was also reviewed.
∗ The more general term "Percutaneous Coronary Intervention (PCI)" is now used to include PTCA,stenting, and other techniques such as atherectomy.

Page 59
Expert Panel on Invasive Cardiology in Ontario
EXISTING GUIDELINES
The British Cardiac Society (BCS) and the British Cardiac Intervention Society (BCIS) issued astatement on peer review in 19992 and a PTCA guideline in Feb. 20003.
European guidelines have been published as follows:
• Guidelines for training and quality control were published in 19964 and 19975.
• The European Board for the Specialty Cardiology (EBSC) published recommendationsfor education and training in basic cardiology in 19966.
• The European Heart Institute (EHI) published standards for revascularizations in 19977.
• The Société française de cardiologie8 published operator and institutional guidelines inFebruary 2000.
The most comprehensive directions are from the American College of Cardiology (ACC) andAmerican Heart Association (AHA), which have maintained a Task Force on Assessment ofDiagnostic and Therapeutic Cardiovascular Procedures to assess the literature and makerecommendations about the appropriate use of cardiac diagnostic and therapeutic procedures.Guidelines for angiography were first issued in 1987, and a revised guideline was published in19999. The first guideline for PTCA was published in 1988, and because of rapid progress in thearea, a second guideline was issued in 199310. A third edition of the PTCA guideline waspublished in June 2001 and is available at www.acc.org11. In 1998 the ACC published a ClinicalCompetence Statement: “Recommendations for the Assessment and Maintenance of Proficiencyin Coronary Interventional Procedures” 12. The following year, the ACC issued a TrainingStatement with recommendations on residency training for interventional cardiology13.
Health Canada published “Cardiovascular Services Guidelines” in 1993, but they have not beenupdated14. The American College of Cardiology held a Core Cardiology Training Symposium(COCATS) in 1994, and the recommendations for training were published in 199515. TheCanadian Cardiovascular Society (CCS) issued standards for training in interventional cardiologyin 199616 which were very similar to the COCATS guidelines. The results of the ConsensusConference on the Indications for and Access to Revascularization were published in 1995 andwere revised in 199717. The Province of Quebec has contributed through the Conseild’Evaluation des Technologies de la Santé du Québec (CET) with a report and recommendationson PTCA in 199718.
The US Society for Cardiac Angiography and Interventions has issued guidelines for internal peerreview in catheterization laboratories and further recommendation19,20.
Although these guidelines are from jurisdictions in Canada, the US and Europe, they includesimilar recommendations for procedural volumes, as summarized in Table 1.

Page 60
Expert Panel on Invasive Cardiology in Ontario
Table 1. Procedure Volume Recommendations
BCS/BCIA2000
SFC2000
ACGME /ACC 1999 & ACC 1998
Quebec1997
EBSC1997
EHI1997
CCS1996
COCATS1994-1995
TRAINING
Angiograms
As 1st
operator
500
300
300 300 300 300 300
125
PTCA 200 250 250(400 optimal)
50 250-300 300
As 1st
operator125 150 125
Maintenance
PTCAOperator
>75/yrIdeally100/yr
>=75/yr 100/yr 50/yr 100/yr
PTCA Trainer 125/yr
Institutionalvolumes forPTCA
> 200/yrminimum
>400/yr600/yr to host
trainingprograms
>250/yr 100/yr 400/yr
PhysicianRetraining
Same asresidency
British Cardiac Society/British Cardiac Intervention Society3
Société française de cardiologie8
American College of Graduate Medical Education and American College of Cardiology12,13,21
Quebec CET18
European Board for the Specialty Cardiology6
European Heart Institute7
Canadian Cardiovascular Society16,17
American College of Cardiology Core Cardiology Training Symposium15
The 1993 ACC/AHA guideline identified two major problems with PTCA: initial abrupt arterialclosure, and late restenosis. At the time, abrupt closure occurred in 3-8% of cases. From 2-5% ofcases required emergency CABG. The Task Force was unequivocal in its recommendation foron-site surgical backup:
“Although technical advances, operator experience, and alternative reperfusionstrategies have somewhat lessened the rate of emergency bypass surgery after failedelective angioplasty, surgical backup has proved life-saving and has effectivelyreduced subsequent morbidity such that it is deemed mandatory by this committee forall elective angioplasty procedures.”

Page 61
Expert Panel on Invasive Cardiology in Ontario
Its recommendation for emergency procedures, including primary PTCA for acute MI wassimilar:
“the committee feels compelled to underscore its conviction that angioplasty/surgicalcentres constitute the best venue for all angioplasty procedures.”
The guideline recommended each institution have a valid peer review mechanism. It endorsedprevious Task Force recommendations on operator training, as noted in Table 1.
The British BCS/BCIS guideline modified a previous BCS/BCIS recommendation that eachcentre have at least 200 procedures per year to maintain competence. This figure was felt to bearbitrary, and it was felt that lower-volume centres could continue to operate, provided that theirperformance was assessed by periodic audits, and was within accepted standards. The risk ofabrupt closure requiring emergency CABG in Britain was 1.5% in 1996. Although coronarystenting has reduced the risk somewhat, more high-risk patients were undergoing PTCA, so thechance of emergency surgery remained about the same. The recommendation was that:
“ …access to emergency surgery, whether on-site or off-site, should be available for allpatients undergoing PTCA, other than for those individuals who have prospectivelyagreed not to require cover.”
A further recommendation was that:
“…all centres, whether with on-site or off-site surgical cover, should be able toestablish cardiopulmonary bypass within 90 minutes of the referral being made to thecardiac surgical service.”
Cases done with off-site coverage should be of a “lower anticipated overall risk and need foremergency CABG.” The covering surgeon should be aware of the PTCA, and appropriatetransfer mechanisms should be available. The requirements for training were similar to those inthe USA (see Table 1.).
The UK Department of Health has funded the Central Cardiac Audit Database (CCAD) projectfor a three-year pilot period2. Patient data were collected from each centre, and mortality postdischarge was tracked. A minimum dataset for annual completion by each centre was defined.The guideline made further recommendations for formal peer review of centres including a sitevisit and formal review every three years. Centres developing a program would be offered adviceand help at start-up, at one year and then every three years at audit time.
The 1997 Québec CET report covered the literature from 1986 to 199618. The report describedthe risks of PTCA, and the role of surgical backup. The original recommendation of the Conseilin 1989 was to avoid performing this procedure without surgical backup. The literature review inthe report included several case series of PTCA without surgical backup from the era prior to theroutine use of stents (1982-1993), but the rates of urgent CABG were under 2.5%. The reportstates:
“The availability of CABG has always been considered a sine qua non for theperformance of PTCA, either within the same hospital (US position) or within rapidtransfer distance (European position). A Canadian position has not been formallyannounced, but most angioplasty centres do have on-site surgical facilities and thosewithout do have a formal arrangement for immediate patient transfer.”

Page 62
Expert Panel on Invasive Cardiology in Ontario
It concluded with the recommendation:
“While the safety profile of angioplasty has improved considerably over the last tenyears, it is nevertheless recommended, as in the earlier Conseil report, that angioplastycontinue to be restricted to centres with on-site cardiac surgery in order to offer thesafest conditions.”
The Conseil recognized that in some circumstances PTCA without surgical backup might beallowed for reasons of access or economics, but it stated:
“If a centre without on-site surgical backup does perform angioplasty it is essential thatonly well defined low risk patients be accepted, and that a formal feasible transferpolicy be operational.”
The literature review to 1996 supported a minimum of 200 cases per centre per year, and perhapsas many as 400/year. A consensus of international experts recommended 75-100 cases peroperator per year. The report recommended the use of primary PTCA for acute MI only in casesineligible for or at high risk with thrombolysis, and who can be treated within 30-60 minutes in ahigh-quality laboratory.
VOLUME-OUTCOME RELATIONSHIPS
The published guidelines have similar recommendations for the maintenance of adequatevolumes of procedures both at an operator and an institutional level based on early observationalstudies that showed higher risks of mortality and/or emergency CABG with low volumes. Mostof the observational studies were carried out prior to the routine use of coronary stents and neweranti-platelet agents. The most recent studies are summarized by indication for PTCA (generalcases and primary PTCA for acute MI), and by operator and institution levels. A complete reviewof volume-outcome relationships in general has been published on the World Wide Web.22
a) PTCA outcomes by hospital volume
Four recent studies of PTCA outcomes by hospital were located in the literature review:
• Ritchie et al., used national US data from the Healthcare Cost and Utilization Project1993-9423. Risk-adjusted mortality and same-admission coronary bypass surgery rateswere lower in high-volume hospitals.
• Maynard et al compared the volume-outcome relationships before and after stenting wasintroduced in California 1993-9624. There was no relationship between mortality andvolume of PTCAs, but the same-admission CABG rate for non-myocardial infarctioncases was lower in hospitals with >400 PTCAs per year than in those with 201-400 casesand 200 or fewer.
• Hannan et al looked at volume-outcome relationships for New York hospitals from 1991to 1994 from the Coronary Angioplasty Reporting System25. Hospitals with low PTCAvolumes had significantly higher mortality rates compared with high volume hospitals,but the absolute differences were small.
• Ho used longitudinal data from California from 1984 to 1996 to examine the changes inmortality and CABG rates over time26. Although there was a significant difference inmortality and CABG rates between low and high volume hospitals, there wasimprovement in both groups of hospitals with time, and the differences were muchnarrower in the more recent time period (i.e., by 1993-96). The differences in emergencyCABG rates were also narrow in the recent time period. The adjusted mortality and
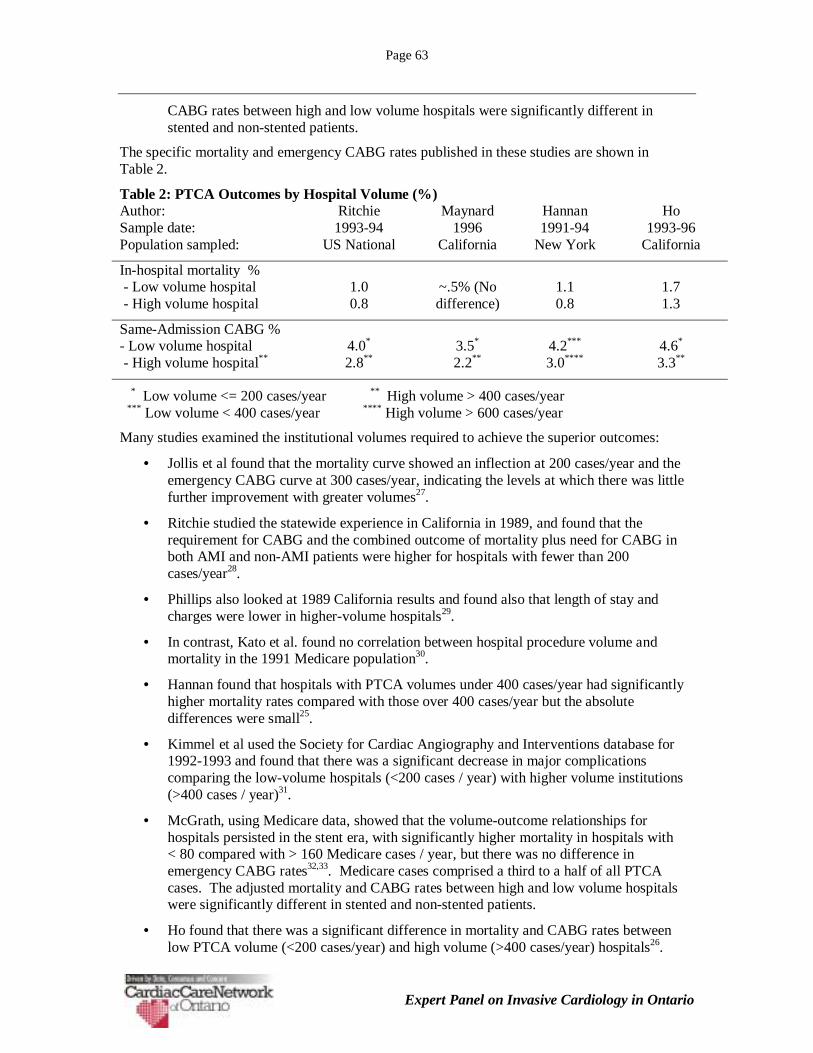
Page 63
Expert Panel on Invasive Cardiology in Ontario
CABG rates between high and low volume hospitals were significantly different instented and non-stented patients.
The specific mortality and emergency CABG rates published in these studies are shown inTable 2.
Table 2: PTCA Outcomes by Hospital Volume (%)Author: Ritchie Maynard Hannan HoSample date: 1993-94 1996 1991-94 1993-96Population sampled: US National California New York California
In-hospital mortality % - Low volume hospital - High volume hospital
1.00.8
~.5% (Nodifference)
1.10.8
1.71.3
Same-Admission CABG %- Low volume hospital - High volume hospital**
4.0*
2.8**3.5*
2.2**4.2***
3.0****4.6*
3.3**
* Low volume <= 200 cases/year ** High volume > 400 cases/year *** Low volume < 400 cases/year **** High volume > 600 cases/year
Many studies examined the institutional volumes required to achieve the superior outcomes:
• Jollis et al found that the mortality curve showed an inflection at 200 cases/year and theemergency CABG curve at 300 cases/year, indicating the levels at which there was littlefurther improvement with greater volumes27.
• Ritchie studied the statewide experience in California in 1989, and found that therequirement for CABG and the combined outcome of mortality plus need for CABG inboth AMI and non-AMI patients were higher for hospitals with fewer than 200cases/year28.
• Phillips also looked at 1989 California results and found also that length of stay andcharges were lower in higher-volume hospitals29.
• In contrast, Kato et al. found no correlation between hospital procedure volume andmortality in the 1991 Medicare population30.
• Hannan found that hospitals with PTCA volumes under 400 cases/year had significantlyhigher mortality rates compared with those over 400 cases/year but the absolutedifferences were small25.
• Kimmel et al used the Society for Cardiac Angiography and Interventions database for1992-1993 and found that there was a significant decrease in major complicationscomparing the low-volume hospitals (<200 cases / year) with higher volume institutions(>400 cases / year)31.
• McGrath, using Medicare data, showed that the volume-outcome relationships forhospitals persisted in the stent era, with significantly higher mortality in hospitals with< 80 compared with > 160 Medicare cases / year, but there was no difference inemergency CABG rates32,33. Medicare cases comprised a third to a half of all PTCAcases. The adjusted mortality and CABG rates between high and low volume hospitalswere significantly different in stented and non-stented patients.
• Ho found that there was a significant difference in mortality and CABG rates betweenlow PTCA volume (<200 cases/year) and high volume (>400 cases/year) hospitals26.
Page 64
Expert Panel on Invasive Cardiology in Ontario
b) PTCA outcomes by operator volume
The relationship between operator volumes and PTCA outcomes has also been well-documentedover the past 10 years:
• Hamad et al studied the outcomes of PTCAs done by lower-volume (<100 cases/year)versus higher-volume (>100 cases/year) operators34. There was a higher success rate inthe higher-volume operators, but no significant difference in mortality and emergencyCABG. The numbers of cases and the absolute complication rates were small.
• Jollis et al, using Medicare data from 1992, showed that low-volume physicians (<25Medicare cases/year) had higher rates of CABG, but no difference in mortality comparedwith higher-volume physicians (>50 Medicare cases/year)35. Low-volume physicianstended to have better results in high-volume hospitals.
• Hannan’s study of 1991-1994 New York cases showed significantly higher mortality andCABG rates for lower-volume cardiologists (<75 cases/year) compared to statewideaverages, but absolute differences were extremely small25.
• McGrath et al studied PTCA outcomes at five New England hospitals from 1990-199336.The 31 cardiologists were divided into terciles by their yearly volumes. Higher-volumecardiologists had greater procedural success, and fewer emergency CABGs than lower-volume operators. There was no difference in mortality. High-volume operators hadgenerally older and sicker patients. The same group extended the study to the 1994 to1996 period37. During this time, there was no difference in adjusted outcomes by volumetercile. The New England studies have been criticized because of the inappropriatecutoffs for “low-volume” operators, most of whom had volumes at or close torecommended levels, and the rather striking selection bias, with the high-volumecardiologists treating sicker patients38. In a study of Medicare patients, the sameinvestigators did find a higher rate of CABG, but not of mortality in lower-volumeoperators (<30 Medicare procedures)33.
• Ellis et al used databases at five high-volume centres to study the role of operator volumeand experience39. Those with caseloads < 30/year were excluded. Both death and thecomposite of death, Q-wave MI, or CABG were inversely related to operator volume, butnot to years of experience. Risk adjustment made a considerable (>30%) difference tothe results of many of the operators.
• Shook et al used a clinical database of 2,204 patients who had PTCA between 1991-1994to study operator volume-outcome relationships. There were eight high-volume (>50cases/year) and 30 low-volume (<50 cases/year) operators40. High-volume operators hadlower CABG rates, but similar mortality rates compared to low-volume operators.
These results are summarized in Table 3.

Page 65
Expert Panel on Invasive Cardiology in Ontario
Table 3: Differences in outcomes between low volume and high volume PTCA operatorsAuthor: Hamad34 Jollis35 Hannan25 McGrath36 Shook40
Sample date: 1986-87 1992 1991-94 1990-93 1991-94
Population: WashingtonDC
Medicare New York New England Los Angeles
Mortality rate Nodifference
Nodifference
Significantlyhigher for low
volumeoperators
Nodifference
Nodifference
Same-stay oremergencyCABG rate
Nodifference
Significantlyhigher for
low volumeoperators
Significantlyhigher for low
volumeoperators
Significantlyhigher for low
volumeoperators
Significantlyhigher for low
volumeoperators
Definition oflow volume
< 100procedures/
year
< 25procedures/
year
< 75procedures/
year
Lowest third < 50procedures/
year
c) Primary PTCA for AMI and hospital outcomes
Several studies have shown an inverse relationship between hospital volume of primary PTCAand mortality:
• A European registry showed a lower mortality in hospitals with > 40 primaryangioplasties/year (8.1%) compared with those with <40/year (11.4%)41.
• The institutional volume-outcome relationship was also present for primary PTCA in theelderly in a study using the Cooperative Cardiovascular Project dataset42. The majorityof US hospitals were in the lowest quartile for primary PTCA procedure volumes in1994-5. Patients admitted to the lowest volume quartile hospitals had a 31% higher 30-day mortality than those in the highest quartile.
• A study of the National Registry of Myocardial Infarction (NRMI) data from 1994 to1998 showed that there was a 28% lower hospital mortality in hospitals with the highestprimary PTCA volumes, but there was no volume-outcome relationship for thrombolytictherapy43.
• Another study using the NRMI data 1994 to 1999 compared outcomes of patients havingPTCA to those having thrombolysis44. Primary PTCA-treated patients had lowermorality rates than those receiving thrombolysis in hospitals having intermediate andhigh PTCA volumes, but there was no difference between the two treatments in lowPTCA-volume hospitals.
• Patients with myocardial infarction appear to do worse if they have a primary PTCA at arural compared with an urban hospital in the USA45.
The observational studies support the “practice makes perfect” hypothesis, with higher-volumeoperators and hospitals generally having better results than those with lower volumes, althoughthe absolute differences are small, and have narrowed with time. The studies support theACC/AHA recommendations of a minimum PTCA caseload of 75 per year for cardiologists, and200 per year for hospitals. There are better hospital results up to a volume of 400 cases per year.

Page 66
Expert Panel on Invasive Cardiology in Ontario
PTCA WITHOUT SURGICAL BACKUP
There have been a number of case series of PTCA procedures done without on-site surgicalbackup. The literature up to 1993 has been summarized by Brophy.18 The studies were difficultto interpret because of weak study designs and possible selection bias.
The Alberta experience has been reported by Klinke and Hui46,47. The complication rates havebeen low, and have improved in the stent era, despite greater patient acuity and lesion complexity.
In Germany and France, the majority of hospitals performing PTCA do not have on-site CABGsurgery48,49. Although the outcomes have been similar, case selection has been an importantdeterminant of the low complication rates of stand-alone centres.
The studies do suggest that PTCA without on-site surgical backup may be done safely, providedthat there is appropriate selection of low-risk cases, a surgical centre is nearby, and that formaltransfer arrangements are in place for emergencies.
There has been controversy over the performance of primary PTCA for AMI in centres withouton-site surgical backup. Wharton et al published a series of 335 cases of primary PTCA withouton-site surgical backup50. The procedural success rate was 94% and the in-hospital mortality ratewas 5.3%. No patient needed emergency CABG as a result of primary PTCA. The PrimaryAngioplasty in Myocardial Infarction-2 Trial (PAMI-2) had a 0.4% rate of emergency CABGafter primary PTCA51. However, 6.1% of patients having primary PTCA still needed later in-hospital CABG, as compared to 44.9% of patients not having primary PTCA because ofunfavourable coronary anatomy.
RISK ADJUSTMENT METHODOLOGY
Comparison of the results of different centres and cardiologists requires adjustment for thecharacteristics of the patient population. Centres and cardiologists treating higher-risk patientsmay have worse outcomes than centres treating lower-risk patients, in spite of a high level oftechnical competence. Block et al tested a list of empirically-derived variables in eight cardiacdatabases51. Univariate and multivariate regression models were used to quantify the predictivevalue of the variables. A list of 29 variables was defined. Categories of variables with highpredictive value included demographics, heart disease severity, acuity/hemodynamic variables,comorbidity and technical considerations
The Northern New England Group has also developed a mulitvariate prediction model, and testedit in an independent data set52,53,54. Their model included age, therapy for AMI, cardiogenicshock, urgent or emergent priority, low ejection fraction, renal dysfunction, any peripheralvascular disease, heart failure, preoperative balloon pump, and lesion type C.
SUMMARY
Several general conclusions may be drawn from this review. PTCA is a complex procedurerequiring extensive training, including the performance of 250-300 procedures under supervisionto achieve competence. Operators should do 75 or more procedures per year to maintaincompetence. Institutions should ideally have at least 400 procedures per year.
There is controversy over the necessity for on-site surgical backup. It is strongly recommendedin guidelines from the United States, but in some European countries PTCA without surgicalbackup is an accepted practice. On-site surgical backup may not be necessary, provided low-riskcases are selected and rapid transport for surgery is available. However, centres without on-sitesurgery may not have enough PTCA cases to maintain competence.
Page 67
Expert Panel on Invasive Cardiology in Ontario
It is important to have an ongoing registry of PTCA cases as a quality assurance measure, and tohave periodic audits of centres. A risk adjustment method including clinical and angiographicvariables is necessary to compare operator and centre performance statistics.
Coronary angioplasty has become increasingly safer and more effective over the last two decadesbut during the same time, it has become more complex and technically difficult. Continuedadherence to guidelines will be necessary to ensure that it will be as safe and effective in thefuture.
Reference List
1. Rankin JM, Spinelli JJ, Carere RG, Ricci DR, Penn IM, Hilton JD. Improved clinicaloutcome after widespread use of coronary-artery stenting in Canada. N Engl J Med 1999;341:1957-1965.
2. Perrins J. Quality assurance in interventional cardiology. Heart 1999; 82 (SupplementII):II23-II26
3. Gray HH. Coronary angioplasty: Guidelines for good practice and training. Heart 2000;83:224-235.
4. Meier B, Bonzel T, Fabian J, Heyndrickx G, Morice M-C, Muhlberger V.Recommendations for training and quality control in coronary angioplasty. Eur Heart J1996; 17:1477-1481.
5. Legrand V, Vrolix M, De Bruyne B, Wijns W, Heyndrickx G, De Scheerder I. BWGICguidelines for training and quality control in adult interventional cardiology. ActaCardiologica 1997; 1.11:507-514.
6. Bayes de Luna A, Block P, Breithardt G, Cherchi A, Daniels O, Kappenberger L, et al.Recommendations of the European Board for the Specialty Cardiology (EBSC) foreducation and training in basic cardiology in Europe. European Heart Journal 1996;17:996-1000.
7. Unger F, Frommer P, Hetzer R, Lüderitz B, Mühlberger V, Rainer WG, Rutishauser W,Sergeant P, Steinbach K, Wanda J. Standards and concepts in cardiac interventions:Coronary artery disease – revascularization. Task Force. European Heart Institute (EHI) ofthe European Academy of Sciences and Arts (EASA) International Society of Cardio-Thoracic Surgeons (ISCTS). Cor Europaeum 1997;6:32-39.
8. Meyer P, Barragan P, Blanchard D, Chevalier B, Commeau P, Danchin N, Fajadet J,Grand A, Lablance J-M, Machecourt J, Metzger J-P, Monassier J-P, Neimann, J-L, Puel J,Steg P-G. Recommandations de la Société française de cardiologie concernant la formationdes médecins coronaragraphistes et angioplastieciens, l’organisation et l’équipement descentres de coronarographie et d’angioplastie coronaire, Achives des maladies du coeur etdes vaisseaux, tome 93, n. 2, février 2000.
9. Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, et al.ACC/AHA guidelines for coronary angiography. A report of the American College ofCardiology/American Heart Association Task Force on practice guidelines (Committee onCoronary Angiography). Developed in collaboration with the Society for CardiacAngiography and Interventions. J Am Coll Cardiol 1999; 33:1756-1824.
10. Ryan TJ, Bauman WB, Kennedy JW, Kereiakes D, King SB, McCallister BD, et al.Guidelines for Percutaneous Transluminal Coronary Angioplasty. Circulation 1993;88:2987-3007.
11. Smith SC, Jr, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, Kuntz RE, PopmaJJ, Schaff HV, Williams DO. ACC/AHA Guidelines for Percutaneous Coronary

Page 68
Expert Panel on Invasive Cardiology in Ontario
Intervention: a report of the American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Committee to Revise the 1993 Guidelines forPercutaneous Transluminal Coronary Angioplasty) J Am Coll Cardiol 2001;37:2239i-lxvi.http://www.acc.org
12. Hirshfeld JW, Ellis SG, Faxon DP. Recommendations for the Assessment andMaintenance of Proficiency in Coronary Intervention Procedures. JACC 1998; 31:722-743.
13. Hirshfeld JW, Banas JS, Ellis SG, Faxon DP, Jacobs A, Magorien RD. American Collegeof Cardiology Training Statement on Recommendations for the Structure of an OptimalAdult Interventional Cardiology Training Program. JACC 1999; 34:2142-2147.
14. Anonymous. Report of the Subcommittee on Health Program Guidelines: Guidelines forestablishing standards for: Cardiovascular Services. 1993; Ottawa, Ont. Canada: HealthServices Division, Health Services Directorate, Health Programs and Services Branch,Health Canada, Ottawa, Ont., K1A 1B4. Cat. No. H39-287/1993E: 83 p.
15. Pepine CJ, Babb JD, Brinkner JA, Douglas JS, Jacobs AK, Johnson WL, et al. Guidelinesfor training in adult cardiovascular medicine: Core Cardiology Training Symposium(COCATS). Task Force 3: Training in cardiac catheterization and interventionalcardiology. JACC 1995; 25:14-16.
16. Miller RM, O'Neill B, Johnstone D, Rae JR, Marquis J-F, Henderson M, et al. CanadianCardiovascular Society Adult Procedure Training Standards Recommendations: Standardsfor Training in Adult Cardiac Catheterization and Angiography. Can J Cardiol 1996;12:469-472.
17. Almond DG, Brister S, Gelfand ET, Higginson LAJ, Kells C, Klinke P. CanadianCardiovascular Society Consensus Conference on Indications for and Access toRevascularization. Can J Cardiol 1997; 13:1D-71D.
18. Brophy J. Percutaneous Transluminal Coronary Angioplasty- Update of Applications andStandards for Utilization. 1997; CETS 97-2 RE
19. Heupler FA, Chambers CE, Dear WE, Angello DA, Heiser M. Guidelines for internal peerreview in the cardiac catheterization laboratory. Catheterization Cardiovascular Diagnosis1997; 40:21-32.
20. Dehmer GJ, Arani D, Noto T, Scanlon P, Hildner F, Clark D, et al. Lessons learned fromthe review of cardiac catheterization laboratories: A report from the Laboratory SurveyCommittee of the Society for Cardiac Angiography and Interventions. CatheterizationCardiovascular Interventions 1999; 46:24-31.
21. Anonymous. Program Requirements for Residency Education in Interventional Cardiology1998; Accredication Council for Graduate Medical Education. 1998 http://www.acgme.org/Accessed April 3, 2001
22. Halm EA, Lee C, Chassin MR. How is volume related to quality in health care? Asystematic review of the research literature. In: Greenfield S, editor. Interpreting theVolume-Outcome Relationship in the Context of Health Care Quality. First ed. Institute ofMedicine, 2000:51-54 http://books.nap.edu/books/ Accessed April 3, 2001
23. Ritchie JL, Maynard C, Chapko MK, Every NR. Association between percutaneoustransluminal coronary angioplasty volumes and outcomes in the Healthcare Cost andUtilization Project 1993-1994. Am J Cardiol 1999; 83:493-497.

Page 69
Expert Panel on Invasive Cardiology in Ontario
24. Maynard C, Every NR, Chapko MK, Ritchie JL. Institutional volumes and coronaryangioplasty outcomes before and after the introduction of stenting. Effective ClinicalPractice 1999; 2:108-113.
25. Hannan EL, Racz M, Ryan TJ, McCallister BD, Johnson LW, Arani DT, et al. Coronaryangioplasty volume-outcome relationships for hospitals and cardiologists. JAMA 1997;277:892-898.
26. Ho V. Evolution of the Volume-Outcome Relation for Hospitals Performing CoronaryAngioplasty. Circulation 2000; 101:1806-1811.
27. Jollis JG, Peterson ED, DeLong ER, Mark DB, Collins SR, Muhlbaier LH, et al. Therelation between the volume of coronary angioplasty procedures at hospitals treatingMedicare beneficiaries and short- term mortality. N Engl J Med 1994; 331:1625-1629.
28. Ritchie JL, Phillips KA, Luft HS. Coronary angioplasty-Statewide experience inCalifornia. Circulation 1993; 88:2735-2743.
29. Phillips KA, Luft HS, Ritchie JL. The association of hospital volumes of percutaneoustransluminal coronary angioplasty with adverse outcomes, length of stay, and charges inCalifornia. Med Care 1995; 33:502-514.
30. Kato NS, Carter GM. Volume-mortality tradeoff for percutaneous transluminal coronaryangioplasty in the United States. JACC 1996; 27:13A Abstract.
31. Kimmel S, Berlin JA, Laskey WK. The relationship between coronary angioplastyprocedure volume and major complications. JAMA 1995; 274:1137-1142.
32. McGrath PD, Dickens JD, Siewers AE, Lucas FL, Kellett MA, Ryan T. Operator andhospital volume in the stent era: Outcomes following 152,212 percutaneous interventions(PCIs) in 1996. Circulation 1999; 100:I-393 Abstract.
33. McGrath PD, Wennberg D, Dickens JD, Siewers AE, Lucas FL, Malenka DJ, et al.Relation between operator volume and hospital volume and outcomes followingpercutaneous coronary interventions in the era of the coronary stent. JAMA 2000;284:3139-3144.
34. Hamad N, Pichard A, Lyle HP, Lindsay J. Results of percutaneous transluminal coronaryangioplasty by multiple, relatively low frequency operators: 1986-1987 experience. Am JCardiol 1988; 61:1229-1231.
35. Jollis JG, Peterson ED, Nelson CL, Stafford JA, DeLong ER, Muhlbaier LH, et al.Relationship between physician and hospital coronary angioplasty volume and outcome inelderly patients. Circulation 1997; 95:2485-2491.
36. McGrath PD, Wennberg D, Malenka DJ, Kellett MA, Ryan T, O'Meara JR. Operatorvolume and outcome in 12,988 percutaneous coronary interventions. JACC 1998; 31:570-576.
37. Malenka DJ, McGrath PD, Wennberg D, Ryan T, Kellett MA, Shubrooks S. Therelationship between operator volume and outcomes after percutaneous coronaryinterventions in high volume hospitals in 1994-1996. JACC 1999; 34:1471-1480.
38. Hannan EL. Percutaneous coronary interventions: Heed the American College ofCardiology volume recommendations, but strive to improve quality. JACC 1999;34:1481-1483.
39. Ellis SG, Weintraub W, Holmes D, Shaw R, Block PC, King SB. Relation of operatorvolume and experience to procedural outcome of percutaneous coronary revascularizationat hospitals with high intervention levels. Circulation 1997; 96:2479-2484.
Page 70
Expert Panel on Invasive Cardiology in Ontario
40. Shook TL, Sun GW, Burstein S, Eisenhauer AC, Matthews RV. Comparison ofpercutaneous transluminal coronary angioplasty outcome and hospital costs for low-volumeand high-volume operators. Am J Cardiol 1996; 77:331-336.
41. Zahn R, Vogt A, Newhaus KL, Shuster S, Senges J. Angioplasty in acute myocardialinfarction clinical practice: Results from 4625 patients from the ALKK AngioplastyRegistry. JACC 1997; 29:15A
42. Every NR, Maynard C, Schulman K, Ritchie JL. The association between institutionalprimary angioplasty procedure volume and outcome in elderly Americans. J Invas Cardiol2000; 12:303-310.
43. Canto JG, Every NR, Magid DJ, Rogers WJ, Malmgren JA, Frederick PD. The volume ofprimary angioplasty procedures and survival after acute myocardial infarction. N Engl JMed 2000; 342:1573-1580.
44. Magid DJ, Calonge BN, Rumsfeld JS, Canto JG, Frederick PD, Every NR, et al. Relationbetween hospital primary angioplasty volume and mortality for patients with acute MItreated with primary angioplasty vs thrombolytic therapy. JAMA 2000; 284:3131-3138.
45. Maynard C, Every NR, Chapko MK, Ritchie JL. Outcomes of coronary angioplastyprocedures performed in rural hospitals. Am J Med 2000; 108:710-713.
46. Klinke P, Hui W. Percutaneous transluminal coronary angioplasty without on-site surgicalfacilities. Am J Cardiol 1992; 70:1520-1525.
47. Hui W, Brass NS, Klinke P. Results of PTCA without on-site cardiac surgery in the stentera. Can J Cardiol 1998; 14 Suppl F:89-89. Abstract.
48. Tebbe U, Carlsson J, Miketic S, Bonzel T, Vogt A, von Leitner ER. Results and outcomeof percutaneous transluminal coronary angioplasty in hospitals with and without on-sitesurgical backup. Eur Heart J 1999; 18:54-54. Abstract.
49. Loubeyre C, Morice MC, Berzin B, Virot P, Commeau P, Drobinski G. Emergencycoronary bypass surgery following coronary angioplasty and stenting. CatheterizationCardiovascular Interventions 1999; 47:441-448.
50. Wharton TP, McNamara NS, Fedele FA, Jacobs MI, Gladstone AR, Funk EJ. Primaryangioplasty for the treatment of acute myocardial infarction: Experience at two communityhospitals without cardiac surgery. JACC 1999; 33:1265
51. Stone GW, Brodie BR, Griffin JJ, Grines L, Boura J, O'Neill WW. Role of cardiac surgeryin the hospital phase management of patients treated with primary angioplasty for acutemyocardial infarction. Am J Cardiol 2000; 85:1292-1296.
52. Block PC, Peterson ED, Krone R, Kesler K, Hannan EL, O'Connor GT, et al.Identification of variables needed to risk adjust outcomes of coronary interventions:Evidence-based guidelines for efficient data collection. JACC 1998; 32:275-282.
53. O'Connor GT, Malenka DJ, Quinton HB, Robb JF, Kellett MA, Shubrooks S. Multivariatepredictor of in-hospital mortality after percutaneous coronary interventions. JACC 1999;34:681-691.
54. Moscucci M, O'Connor GT, Ellis SG, Malenka DJ, Sievers J, Bates ER. Validation of riskadjustment models for in-hospital percutaneous transluminal coronary angioplastymortality on an independent data set. JACC 1999; 34:692-697.

Page 71
Expert Panel on Invasive Cardiology in Ontario
Appendix 4: PUBLISHED GUIDELINES FOR CATH AND PCI
Title Publishing Organization Year ScopeCardiovascular Services Health Services Directorate, Health
Program and Services Branch, HealthCanada
1993 CATHandPCI
AHA/ACC Guidelines forPercutaneous TransluminalCoronary Angioplasty
American Heart Association/AmericanCollege of Cardiology Task Force onAssessment of Diagnostic and TherapeuticCardiovascular Procedures
1993 PCI
Guidelines For Training InAdult CardiovascularMedicine
Core Cardiology Training Symposium(COCATS)
1995 CATHandPCI
Adult Procedure TrainingStandards Recommendations:Standards for Training inAdult Cardiac Catheterizationand Angiography
Canadian Cardiovascular Society 1996 CATHandPCI
Recommendations foreducation and training in basiccardiology in Europe.European Heart Journal 1996;17:996-1000.
European Board for the SpecialtyCardiology (EBSC)
1997
Percutaneous TransluminalCoronary Angioplasty- Updateof Applications and Standardsfor Utilization.
Conseil d’Évaluation des Technologies dela Santé du Quebec (CETS)
1997 PCI
Consensus Panel on CardiacCatheterization Services inOntario
Cardiac Care Network of Ontario 1997 CATHandPCI
Standards and Concepts inCardiac Interventions,Coronary Artery Disease –Revascularization
European Heart Institute (EHI) of theEuropean Academy of Sciences and Arts(EASA) International Society of Cardio-Thoracic Surgeons (ISCTS)
1997 CATHandPCI
Recommendations for theAssessment and Maintenanceof Proficiency in CoronaryInterventional Procedures
Statement of the American College ofCardiology
1998 PCI
Program Requirements forResidency Education inInterventional Cardiology
Accreditation Council for GraduateMedical Education
1998 PCI
ACC/AHA guidelines forcoronary angiography
American College of Cardiology/AmericanHeart Association Task Force on practiceguidelines (Committee on CoronaryAngiography) Developed in collaborationwith the Society for Cardiac Angiographyand Interventions
1999 CATH

Page 72
Expert Panel on Invasive Cardiology in Ontario
Appendix 4: PUBLISHED GUIDELINES FOR CATH AND PCI (CONT’D)
Title Publishing Organization Year ScopeTraining Statement onRecommendations for theStructure of an Optimal AdultInterventional CardiologyTraining Program
American College of Cardiology 1999 PCI
Coronary angioplasty:Guidelines for good practiceand training
Heart (British Cardiac Society (BCS) andthe British Cardiac Intervention Society(BCIS)
2000 PCI
Cardiologie Tertiaire, SituationActuelle, Perspectives etPropositions
Document adopté par le Comité de Travailde Cardiologie Tertiaire, Ministère de laSanté et des Services sociaux
2000 CATHandPCI
Recommandations de laSociété française decardiologie concernant laformation des médecinscoronaragraphistes etangioplastieciens,l’organisation et l’équipementdes centres de coronarographieet d’angioplastie coronaire
Société française de cardiologie (SFC) 2000 CATHandPCI
ACC/AHA Guidelines forPercutaneous CoronaryIntervention
American College of Cardiology/AmericanHeart Association, Revision of the 1993PTCA Guidelines
2001 PCI
Page 73
Expert Panel on Invasive Cardiology in Ontario
Appendix 5: EXPERT OPINIONS AND ORGANIZATIONAL RESPONSES
Opinion ReceivedStephen G. Ellis, MDDirectorSones Cardiac Catheterization LaboratoryDepartment of CardiologyThe Cleveland Clinic Foundation
William K.K. Hui, MBBS, FRCP (Edin),FRCP(C), FACCChief of CardiologyRoyal Alexandra Hospitals
Blair O’Neill, M.D., FRCPC, FACC, FSCAIAssociate Professor and HeadDivision of Cardiology, Dalhousie UniversityChief of ServiceQueen Elizabeth II Health Sciences Centre
Merril L. Knudtson, MD, FRCP(C)Clinical Professor of MedicineDirector, Interventional CardiologyFoothills Medical CentreCalgary Regional Health Authority
Christopher Buller, MD, RFCPC, FACCChairman, Interventional Cardiology CommitteeProvincial Advisory Centre on Cardiac Care,BC.
No Opinion ReceivedDavid R. Holmes, Jr., M.D.Cardiovascular Diseases & Internal MedicineMayo Clinic200 First Street SWRochester, Minnesota
Louis Roy, MDChair, CAICInstitut de Cardiologie de QuébecHôpital Laval2725, chemin Ste-FoySte Foy, Québec
ORGANIZATIONS CONTACTED
Reply received:
Canadian Medical Protective Association (CMPA)
Canadian Association of Interventional Cardiologists (CAIC)
Canadian Cardiovascular Society (CCS)
No reply received:
College of Physicians and Surgeons of Ontario (CPSO)43
Royal College of Physicians and Surgeons of Canada (RCPSC)
43 Asked to be included on the Secondary Review Panel.

Page 74
Expert Panel on Invasive Cardiology in Ontario
Appendix 6: COMMUNIQUE ANNOUNCING THE PANEL

Page 75
Expert Panel on Invasive Cardiology in Ontario
Appendix 7: STAKEHOLDER SUBMISSIONS
Organization ContactEssex, Kent and LambtonDistrict Health Council
Frank ChalmersExecutive Director
Greater Toronto Area CommunityCardiologists (GTACC) Organization44
Dr. M. Gupta, ChairDr. F. Halperin, Vice-ChairDr. B. Lubelsky
Heart Catheter CampaignPeterborough
Linda Willcox WhetungCo-Chair, Community Health Services FoundationCo-Chair, Heart Catheter Campaign
Peterborough Cardiologistsc/o Kawartha Cardiology Clinic
Dr. W. HughesDr. B. MackenzieDr. J. ReesorDr. D. McMillanDr. W. Wilkins
Peterborough Regional Health Centre Rob DevittPresident & CEO
Rouge Valley Health System Peter Gladstone, MD, FRCP(C)
Southlake Regional Health Centre Patricia NormanVice-President, Regional Programs
St. Joseph’s Health Centre Dr. Maria deVilla, Head, Cardiology DivisionF. Meligrana, J.D., FRCP(C)N. Ranganathan, M.D., FRCP(C)J. Reial, M.D., FRCP(C)V. Sivaciyan, M.D., FRCP(C)M. Fisher, M.D., FRCP(C)L.G. Clements, M.D., FRCP(C)
St. Michael’s Hospital Robert J. Chisholm, M.D., FRCPCDivision of Cardiology
Thunder Bay Regional Hospital Dr. Chris LaiCath Lab Director
Thunder Bay Regional Hospital Lori MarshallSenior Vice President, Patient Care Services
McMaster UniversityDivision of Cardiology
D.A. Holder, M.D., F.R.C.P.(C)
44 GTACC was granted an opportunity to present to the Expert Panel at one of its meetings.

Page 76
Expert Panel on Invasive Cardiology in Ontario
Appendix 8: SECONDARY REVIEW PANEL
David Alter, MD, Scientist, Institute for Clinical Evaluative Sciences
Michel Bertrand, MD, Lambersart, France
Gary W. Burggraf, MD, Chair, Professor of Medicine, Division of Cardiology, Queen’sUniversity, Kingston General Hospital
Rajen Chetty, MD, Director Cardiac Cath Lab, Hotel Dieu-Grace Hospital, Windsor
Joy Craighead, Associate Director, Quality Management, College of Physicians and Surgeonsof Ontario
Vladimír Dzavik, MD, Director, Cardiac Catheterization Laboratories, University HealthNetwork
Milan K. Gupta, MD, William Osler Health Centre Chair, Greater Toronto Area CommunityCardiologists,
Paul Hendry, MD, Co-Director, Arrhythmia Dev. Clinic, University of Ottawa Heart Institute
David Holmes, MD, Director, Cardiac Catheterization Laboratory, Mayo Clinic, Rochester
William K. K. Hui, MD, Chief, Division of Cardiology, Royal Alexandra Hospitasl, Edmonton
Arvind Koshal, MD, Division of Cardiac Surgery, University of Alberta Hospital
Warren Laskey, MD, Division of Cardiology, University of Maryland Hospital, Baltimore
Bruce Lubelsky, MD, Co-Chair, Central Ontario Regional Cardiac Care Committee
Jean-Francois Marquis, MD, Director Cardiac Catheterization laboratory, University ofOttawa Heart Institute
Wendy Nelson, V.P., Patient Services, Trillium Health Centre, Co-Chair, Central OntarioRegional Cardiac Care Committee
Blair J. O'Neill, MD, Professor and Head, Division of Cardiology, Dalhousie University, Chiefof Service, Queen Elizabeth II Health Sciences Centre
Malvinder Parmar, MD, Timmins
Dominic Raco, MD, Assistant Professor and Head of Cardiology, St Joseph's Healthcare,MacMaster University, Hamilton
Felix Unger, MD, Landesklinik fur Herzchirurgie, Landeskrankenanstalten Salzburg
T. Wharton Jr, MD, FACC, Chief, Section of Cardiology, Director, Cardiac CatheterizationLaboratory, Exeter Hospital
Prof. Petr Widimský, MD, Professor of Medicine, Head of the University Cardiocenter,Vinohrady, Prague

Page 77
Expert Panel on Invasive Cardiology in Ontario
Appendix 9: CARDIAC CARE NETWORK COMMITTEE
Barry Monaghan, Chair CCN, President and CEO, West Park Healthcare Centre, Toronto
Bruce M. Antonello, President & CEO, St. Mary’s General Hospital, Kitchener, Ontario
Bill Bain, Consumer Representative (former V.P. Corporate Affairs, MDS Inc.), Toronto, Ontario
Susan Burns, Executive Director, Waterloo Region-Wellington-Dufferin District HealthCouncil, Guelph, Ontario
Anthony F. Graham, MD, St. Michael’s Hospital, Toronto, Ontario
Milan K. Gupta, MD, Greater Toronto Area Community Cardiologists/William Osler HealthCentre, Brampton, Ontario
Andrew Hamilton, MD, Chief, CV Surgery, Kingston General Hospital
Lyall Higginson, MD, Chief, Cardiology, University of Ottawa Heart Institute, Ottawa, Ontario
Chris Morgan, MD, Vice-Chair CCN, Deputy Chief Cardiology, Sunnybrook & Women’sCollege Health Sciences Centre, Toronto, Ontario
Sharon Pillon, Administrative Director, University Health Network, Toronto General Division,Toronto, Ontario
Jenny Rajaballey, Director, Institutional Services Branch, Ministry of Health and Long-TermCare, Toronto, Ontario
Donna Riley, RN, Regional Cardiac Care Coordinator, St. Michael’s Hospital, Toronto, Ontario
B. William Shragge, MD, Chief of Staff, Hamilton Health Sciences, Hamilton, Ontario
Neville Suskin, MD, London Health Sciences Centre, London, Ontario
Allan L. Whiting, President & CEO, Rouge Valley Health System, Toronto, Ontario
Ex-Officio:
David Garlin, Director of Communications, Cardiac Care Network of Ontario
Linda Hunter, Program Consultant, Ministry of Health and Long-Term Care
Mark A. Vimr, Executive Director, Cardiac Care Network of Ontario

Page 78
Expert Panel on Invasive Cardiology in Ontario
Appendix 10: CLINICAL SERVICES COMMITTEE MEMBERSHIP
Chris D. Morgan, MD, Vice-Chair CCN, Deputy-Chief Cardiology, Sunnybrook & Women’s College Health Sciences Centre
Lorna Bickerton, Regional Cardiac Care Coordinator, University of Ottawa Heart Institute
Rajen Chetty, MD, Director Cardiac Cath Lab, Hotel Dieu-Grace Hospital
Joseph deMora, President and CEO, Kingston General Hospital
Rob Forbes, Director of Informatics, CCN
Michael Richard Freeman, MD, Medical Director, Heart Program, St. Michael’s Hospital
Wendy Fucile, Vice President, Acute Care, Peterborough Regional Health Centre
David Garlin, Communications Coordinator, CCN
Anup Kumar Gupta, MD, Director, Cardiac Catheterization, Toronto East General Hospital
Linda Hunter, Planning Consultant, Operational Support, Ministry of Health & Long Term Care, Operational Policy and Priority Programs
Jamie W. Hynd, MD, Chief of Medicine, Brockville General Hospital and St. Vincent de Paul Hospital
Charles Lazzam, MD, Cath Lab Director, Trillium Health Centre
Lori Marshall, Senior Vice President, Patient Services, Thunder Bay Regional Hospital
Roy Masters, MD, Cardiac Surgeon, University of Ottawa Heart Institute
Alan Menkis, MD, Cardiac Surgeon, London Health Sciences Centre
Jillian Ross, Director, Projects and Operations, CCN
Rachel Solomon, Program Consultant, Operational Support, Ministry of Health and Long-Term Care, Operational Policy and Priority Programs

Page 79
Expert Panel on Invasive Cardiology in Ontario
Appendix 11: PUBLISHED OPERATOR GUIDELINES AND EXPERT OPINION -CATH
ExistingGuidelines
Yearpublished
OperatorTraining
OperatorMaintenance of Competence
COCATS 1995 Minimum 300200 as primary operator
CCS 1996 Minimum 300200 as primary operator
Minimum 150/year
EHI 1997 Minimum 300 Minimum 250/year
EBSC 1997 Minimum 300
CCN CathConsensus Panel
1997 N/A Minimum 150/year
CardiologieTertiare
2000 N/A Minimum 250/year
SFC 2000 Minimum 500
300 as primary operator
Minimum 250/year
Expert Opinion
Expert A Minimum 300 Minimum 150/year
Expert B Minimum 250/year at new centres
Note: Refer to Appendix 4 for the particulars of the above noted guidelines.

Page 80
Expert Panel on Invasive Cardiology in Ontario
Appendix 12: PUBLISHED OPERATOR GUIDELINES AND EXPERT OPINION - PCI
ExistingGuidelines
YearPublished
Operator Training Operator (Maintaining)
Health Canada 1993 100 procedures
ACC/AHA 1993 Structured training program, minimum125 procedures under supervision
Minimum 75/year
CCS 1996 250 procedures Minimum 100/year
EHI 1997 N/A Minimum 50/year
EBSC 1997 Minimum 50
CET 1997 Minimum 75 to 100/year
CCN CathConsensus Panel
1997 N/A Minimum 100/year
ACC 1998 Minimum 250Optimal 400
Minimum 75/year
HEART 2000(BCS/BCIS)
2000 125 as first operator200 totalTrainers minimum 125/year with 50involving direct supervision of atrainee
Minimum 75/year
Ideal 100/year
CardiologieTertiare
2000 Minimum 100/year
SFC 2000 250 procedures150 as primary operator, including atleast 100 stents
Minimum 125/year
ACC/AHA 2001 More than 250 Minimum 75/year
Expert OpinionExpert A 150 procedures and review cases for
1st two years of practiceIf not recent training, 300 procedures
125 procedures/year
Expert B Minimum 150/year if no on-sitesurgery
Expert C If no on-site surgery, minimum125/year, preferred 150/year
Expert E Training in an accredited programRetraining to have similar criteria250 supervised as primary operator
Non-standard procedures45 minimum50/year
Minimum 50/year with a mentoror 75/year without a mentor,ideally 100/year
Non-standard proceduresminimum 10/year
Note: Refer to Appendix 4 for the particulars of the above noted guidelines.
45 Non-standard refers to procedures considerably different than balloon angioplasty and stenting, such asrotational atherectomy. This cardiologist recommended 5 training cases and 5 cases annual to maintaincompetency for those procedures that are much more similar to balloon angioplasty and stenting.

Page 81
Expert Panel on Invasive Cardiology in Ontario
Appendix 13: PUBLISHED INSTITUTIONAL GUIDELINES AND EXPERT OPINION –CATH AND PCI
PublishedGuidelines
YearPublished CATH PCI
Health Canada 1993 Minimum 300 patients/year 100 to 150/yearCOCATS 1993 Minimum 300 patients/year
Optimum 1,000 patients100 to 150/year
ACC/AHA 1993 Minimum 200/year Minimum 200/year
CCS 1996 Minimum 500/year Minimum 400/yearEHI 1997 N/A Minimum 100/yearCET 1997 Minimum 200/year
Preferred 400/yearCCN CathConsensus Panel
1997 Minimum 500/year Minimum 400/year
ACC 1998 N/A Minimum 400/year
HEART(BCS/BCIS)
2000 N/A Minimum 200/yearLower volume centres subject toperiodic audits
CardiologieTertiare
2000 Minimum 1,000/yearOptimum 1,500/year
Minimum 250/year
SFC 2000 N/A <250/year insufficient to ensurequality> 600 is optimal
ACC/AHA 2001 Minimum 400/year with on-sitesurgery
Expert OpinionExpert A Minimum 500/year Minimum 250/year
Expert C If no on-site surgery, minimum400/year
Expert D Minimum planned volume of 500/yearfor new centres
Expert E Ideal minimum volume of 600/yearFloor at 400/year
Note: Refer to Appendix 4 for the particulars of the above noted guidelines.

Page 82
Expert Panel on Invasive Cardiology in Ontario
Appendix 14: PUBLISHED GUIDELINES AND EXPERT OPINION –QUALITY ASSURANCE
PublishedGuidelines
YearPublished
ACC/AHA 1993 A rigorous mechanism for valid peer review must be established and ongoingin each institution performing PCI.
ACC ClinicalCompetenceStatement
1998 Rigorous privilege-granting and quality assessment monitoring system thatincludes:
1. Established criteria2. Prospective recording of patient characteristic data to permit risk
stratification3. Gathering and tabulating complete objective outcome data by a
disinterested party4. Oversite and privilege granting by a physician program director5. Periodic conferences to review and analyze adverse events6. Periodic review of program and physician quality assessment
statistics and comparison with benchmark rates.Operators who perform < 75 procedures/year should develop a definedmentoring relationship with a highly experienced operator (annual volume >150 procedures/year).
Heart (BCS& BCIS)
2000 Collecting a limited and well defined amount of data on every patient has theadvantage that data collection can realistically be expected to be 100%, truemeasurements of mortality and complication rates can be made, allowance ismade for basic risk stratification, and comparisons can be made betweenoperators, and between individual centres and a national mean.
Audit and compliance with standards can be assessed by peer review.
Expert OpinionExpert A All centres maintain and monitor wait times for cath and PCI
Documentation that procedure was appropriateDocumentation of informed consentProcess for review of safety and quality (including integrity of hemodynamic data andangiographic data)
Expert B Ongoing surveillance of patient selection, procedure complications, and outcome isparticularly critical in the early years of a new program.
Expert C Regular review of PCI result and complication statistics is mandatoryAll complex cases, failed PCI cases, post-PCI MI’s and deaths should be reviewed.There should be regular case reviews with the cardiovascular surgeons.
Expert D Establishment of a province-wide database for diagnostic angiography, percutaneous coronaryinterventions, and cardiac surgery procedures is a key component of evaluating the quality andsafety of care at individual institutions.
Expert E Need to carefully risk adjust and look at sufficiently high volumes to make results meaningful.Hospitals and operators should be evaluated by: procedural success, in-hospital and 30-daymortality, in-hospital need for emergency bypass surgery, in-hospital Q-wave infarction, in-hospital blood transfusion, duration of the interventional procedure, and “door to balloon time”for patient presenting with acute myocardial infarction.

Page 83
Expert Panel on Invasive Cardiology in Ontario
Appendix 15: PUBLISHED GUIDELINES AND EXPERT OPINION –PCI WITHOUT ON-SITE CARDIAC SURGERY
Existing GuidelinesACC/AHA 1993 “Surgical backup …is deemed mandatory ...for all elective angioplasty procedures”
CET 1997 Recommends “While the safety profile of angioplasty has improved considerablyover the last 10 years, it is nevertheless recommended that angioplasty continue tobe restricted to centres with on-site cardiac surgery in order to offer the safestconditions”If performed without on-site surgical backup, essential that only well defined lowrisk patients be accepted and a formal feasible transfer policy be operational
HEART 2000(BCS/BCIS)
“Access to emergency surgery, whether on-site or off-site, should be available for allpatients undergoing PTCA...”Cases done with off-site coverage should be of a “lower anticipated overall risk andneed for emergency CABG”With on or off-site, maximum of 90 minutes to surgical service
ACC/AHA 2001 “Mere convenience should not replace safety and efficacy in establishing an electivePCI program without on-site surgery… At this time, the Committee, therefore,continues to support the recommendation that elective PCI should not be performedin facilities without on-site cardiac surgery.”
Literature reviewWharton 1999 Experienced interventionalists
Experienced nursing & technical staffWell-equipped laboratory (balloon pump)CCU staff trained for hemodynamic monitoring and IABPSupportive hospital administrationFormal transfer protocol24 hour coverageRigorous case selectionOutcomes analysis and case review

Page 84
Expert Panel on Invasive Cardiology in Ontario
Appendix 15 (Cont’d): PUBLISHED GUIDELINES AND EXPERT OPINION –PCI WITHOUT ON-SITE CARDIAC SURGERY
Expert OpinionExpert A On-site surgery is preferable.
High volume operators (greater than 150 cases/year, more than 3 years experience) canperform PCI and stent insertion.Surgical backup within 30 to 40 minutesFormal relationship with high volume surgical centreClear process for transfer and transport of the patient (including use of portable intra-aorticballoon pump support.
Expert B More patients require emergency surgery within 24 hours after diagnostic than afterinterventional procedures, although PCI emergency can be more complex.Increasingly difficult to limit cath to low risk patients.Economic advantages to ad hoc PCIDirect PCI preferred to lytic therapy (in the right hands)
Expert C Supportive of PCI without on-site surgery.Staff training is importantRapport between interventional cardiologists and cardiovascular surgeons creates arelationship of cooperation and trust, which is vital to the acceptance and rapid transfer foremergency surgery.Medical transport system aware of nature of needAmbulance services equipped to transport IVs, ventilator and intra-aortic balloon pump
Expert D Should be considered only in medium-sized centres located very distant from full servicecentresDistribution of these services “closer to home” usually results in a significant loss ofquality… Establishment of stand-alone cath facilities in most instances is plainlyinappropriate… and should be considered only in medium-sized centres located very distantfrom full service centres… it overlooks the importance of frequent formal and informalinteraction between cardiologists, interventional cardiologists, and cardiac surgeons.
Expert E “Other than for intervention for acute myocardial infarction, there is no reason that aninterventional program should exist without on-site surgical backup.”If off-site surgery, detailed transfer arrangements and monitoring of transfer time needed.Maximum 60 to 75 minutes to OR
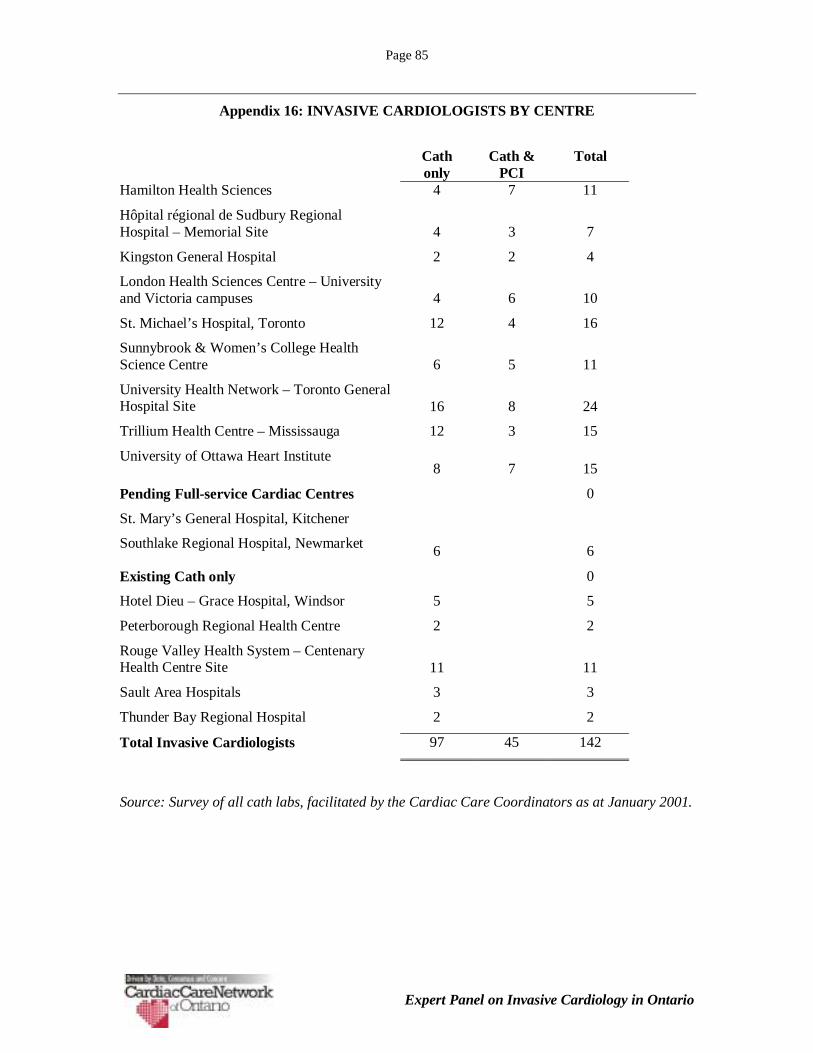
Page 85
Expert Panel on Invasive Cardiology in Ontario
Appendix 16: INVASIVE CARDIOLOGISTS BY CENTRE
Cathonly
Cath &PCI
Total
Hamilton Health Sciences 4 7 11
Hôpital régional de Sudbury RegionalHospital – Memorial Site 4 3 7
Kingston General Hospital 2 2 4
London Health Sciences Centre – Universityand Victoria campuses 4 6 10
St. Michael’s Hospital, Toronto 12 4 16
Sunnybrook & Women’s College HealthScience Centre 6 5 11
University Health Network – Toronto GeneralHospital Site 16 8 24
Trillium Health Centre – Mississauga 12 3 15
University of Ottawa Heart Institute8 7 15
Pending Full-service Cardiac Centres 0
St. Mary’s General Hospital, Kitchener
Southlake Regional Hospital, Newmarket 6 6
Existing Cath only 0
Hotel Dieu – Grace Hospital, Windsor 5 5
Peterborough Regional Health Centre 2 2
Rouge Valley Health System – CentenaryHealth Centre Site 11 11
Sault Area Hospitals 3 3
Thunder Bay Regional Hospital 2 2
Total Invasive Cardiologists 97 45 142
Source: Survey of all cath labs, facilitated by the Cardiac Care Coordinators as at January 2001.

Page 86
Expert Panel on Invasive Cardiology in Ontario
Appendix 16 (cont’d)
Full-time PCI Trainees in Ontario, January 2001
Number ofTrainees
Hamilton Health Sciences 1
Hôpital régional de Sudbury RegionalHospital – Memorial Site
Kingston General Hospital
London Health Sciences Centre – Universityand Victoria campuses
1
St. Michael’s Hospital, Toronto 3
Sunnybrook & Women’s College HealthScience Centre
2
University Health Network – Toronto GeneralHospital Site
2
Trillium Health Centre – Mississauga
University of Ottawa Heart Institute 1
Total PCI Trainees 10
Source: Survey of Cath Labs, January 2001.
Note: Country or province of origin and expected completion date not specified.

Page 87
Expert Panel on Invasive Cardiology in Ontario
Appendix 17: CAPACITY ANALYSIS
In this appendix, we examine the current and projected capacity as measured by the number ofinvasive cardiologists and by cath rooms. Note that the following analysis is based on provincialtotals, and does not take into consideration any regional discrepancies or access issues.
FACTORS THAT AFFECT CAPACITY
Invasive procedures are very complex, and require the combined skills of the entire cath lab teamand supporting resources, including:
• Invasive cardiologists.• Supporting professionals (e.g., cath lab nurses, imaging technicians).• Cath rooms.• Funding for procedures.
If any single element is missing, the capacity will be limited, regardless of any excess capacityamong the other elements.
The availability of funding for these procedures is outside the scope of the Panel’s work; it isnoted only for context. The assessment of the availability of supporting professionals is similarlyoutside the scope of our work. However, some Panel members noted that the availability ofexperienced cath lab nurses already presents a capacity limitation for some centres.
Using Cardiaccess to Understand the Human Resource Issues
As a starting point for the analysis of the human resource capacity issues, we studied the numberof invasive cardiologists that were reported to have performed caths and PCI and the number ofprocedures performed during the seven-month period from July 2000 to January 2001. Thesedata were then annualized to provide an estimate of typical annual activity.
Reporting cath and PCI activity to CCN was only mandatory beginning January 2001; however,most centres were reporting all cases to CCN since July 2000. To ensure that these data wererepresentative of the current situation, we conducted the following validations:
• A comparison of the number of procedures reported manually and the number reported in thedatabase showed that most of the procedures were reported during this period.
• The Regional Cardiac Care Co-ordinators were asked to verify which cardiologists wereperforming procedures at their centre, and whether they were performing cath only, or bothcath and PCI.
Overall, the Panel believed that the resource data presented in this appendix provides a realisticorder-of-magnitude indication of current resources and capacity.
Cathing Cardiologists
The Panel identified several indicators that there is no current shortage of cathing cardiologists inOntario:
• Despite the rapid growth in the number of caths performed in Ontario over the past fiveyears, the growth rate has not slowed, which suggests that the capacity to perform theseprocedures has not been a limiting factor.

Page 88
Expert Panel on Invasive Cardiology in Ontario
• Based on an analysis of the number of procedures by cathing cardiologists, 25 (out of 97)physicians were found to be performing fewer than the recommended minimum numberof procedures to maintain competence (i.e., 150 procedures per year).
Several factors suggest that a significant shortage of cathing cardiologists is not likely to occurover the next five years:
• There is potentially some latent capacity within the existing resources. If everycardiologist who is currently performing fewer than the recommended minimum numberof procedures raised his/her cath caseload to the minimum (150 cases/year), the increasein capacity would be approximately 1,800 procedures.
• The current average (mean) number of procedures per cathing cardiologist isapproximately 215 procedures per year. With each increase of 10 procedures in theaverage caseload, the total capacity will increase by about 1,000 procedures.
• With the extension of the cardiology residency from two years to three years, residentsnow have an opportunity to have two sessions of four months of cath training within theresidency requirements. Although this may not be sufficient training to permit theresident to cath independently, the remaining apprenticeship time will be relatively short.
Although we expect that there will be enough interest in cath training to meet future needs, as thenumber of community cardiologists and cardiology residents who require training in cathincreases, the availability of training centres and training cardiologists may become an issue.
Interventional Cardiologists
The capacity situation for PCI is slightly different than for cath:
• Most (94%) of the interventional cardiologists in Ontario are already performing morethan the recommended minimum number of procedures to maintain their competence.While there is not the same potential to increase capacity through higher caseloads asthere is for cath, there is still some degree of latent capacity in the system. The Panelheard anecdotal reports that many interventional cardiologists would like to increase theircaseload, but are limited by demand at their centre or by funding limitations.Furthermore, many practicing interventional cardiologists believe that their optimalpersonal volume is well in excess of the recommended minimum of 100 per year.
• The training period for PCI is significantly longer than the post residency training forcath. For new cardiologists, the minimum training period post residency is one year, andsome are in training for up to two years. The length of time that must be devoted to thistraining may be a barrier to newly graduating cardiologists, and, perhaps to an evengreater degree, to established cardiologists who wish to train in PCI.
Despite these higher barriers to increasing procedural capacity, the Panel believes that there islatent capacity in the provincial training programs to meet Ontario’s need for new trainees in PCI:
• As noted in Appendix 16, there are currently 10 PCI fellowship trainees (“fellows”) atuniversity-affiliated centres in Ontario. Each of these centres has trained one or morePCI fellows for the past several years, and has informally indicated that they plan tocontinue doing so. Some trainees spend more than one year in fellowship training, sothere will not be 10 new “graduates” this year. While many trainees in previous yearshave been non-Canadian residents (and have returned to their country of origin aftertraining), in the past two years there has been a sharp increase in the number of Canadiancardiology graduates applying for PCI fellowship training. In summary, under the

Page 89
Expert Panel on Invasive Cardiology in Ontario
current training structure (i.e. no funding provided to training centres), approximatelythree to four Canadian-resident interventional cardiologists have “graduated” fromOntario centres in recent years; this is expected to increase to five or six by next year.
• There are strong interventional cardiology fellowship training programs in several otherprovinces, and thus additional Canadian graduates potentially eligible to meet Ontario’sneeds. While some Ontario trainees might move to, or return to, other provinces, thevery rapid expansion of PCI in Ontario has created a greater range of job opportunities(e.g. academic vs. community hospital, larger vs. smaller city) that may help retain orattract graduates of interventional fellowship programs. Furthermore, many Canadiancardiology graduates have sought interventional training at prominent U.S. or Europeancentres, then returned to Canada to take up staff positions. (As an example, in the pastfive years there have been at least six PCI physicians appointed in Ontario who receivedtheir interventional training in the U.S.).
• The Panel estimated that approximately 10% of the interventional cardiologists inOntario are over 60 years of age, and approximately 15% may be expected to retire (or atleast significantly reduce their procedure volumes as a prelude to retirement) within thenext five years. This translates into a loss of one or two experienced interventionalists toretirement annually in Ontario.
In terms of emigration, only a handful of practicing interventional cardiologists have left Ontariofor other provinces or the U.S. in recent years, and there has been at least partially offsettingimmigration. Except for specific (generally isolated) geographic areas, there does not appear tobe a shortage of interventional cardiologists in the U.S. drawing physicians away from Ontario.
Female interventional cardiologists may perform fewer procedures than their male counterparts atcertain points in their career, particularly in relation to pregnancy and associated concerns aboutradiation exposure. While the differential workloads of male and female physicians are highlyrelevant to physician resource planning in some specialties, female physicians presently constituteless than 10% of interventional cardiologists in Ontario. The current distribution of male andfemale cardiology residents suggests that this proportion may not change substantially in the nextthree to five years.
To better understand the potential for a shortfall in capacity for PCI, we analyzed four supplyscenarios:
• Low scenario: In this scenario, a conservative assumption was made about theincrease in caseload, and a very conservative assumption about the number ofinterventional cardiologists. We assumed that the current mean caseload (210procedures/year; median 190) does not change, and that the total number ofinterventional cardiologists would increase by only three per year (net of attrition).
• Low-medium scenario: The mean caseload remains at 210 procedures per year, whilethe total number of interventional cardiologists increases by five per year.
• High-medium scenario: The mean caseload increases to 230 procedures per year, andthe total number of interventional cardiologists increases by five per year.
• High scenario: The mean caseload increases to 230 procedures per year, and the totalnumber of interventional cardiologists increases by seven per year.

Page 90
Expert Panel on Invasive Cardiology in Ontario
There is as much uncertainty around the demand for these services as there is around the supply.Therefore, we also looked at three demand scenarios, where the procedures grow at the targetrates46, the target rates plus 10%, and the target rates plus 20%.
The results of this analysis are shown in Table 17-1. Under the most conservative assumptionson growth in capacity, the demand for services can be expected to exceed capacity by just under2,000 procedures by 2005/06. However, with the more aggressive assumptions (the high-mediumor high scenarios), capacity nearly meets or exceeds the demand, even in the scenario where thedemand exceeds the current targets by 20%.
Table 17-1: Potential Capacity Gap, 2005/06, number of proceduresTarget Target + 10% Target + 20%
Demand: 14,874 16,361 17,849
SCENARIONet annual
increaseAveragecaseload Capacity THE GAP
Low 3 210 13,020 1,854 3,341 4,829
Low-Medium 5 210 15,120 - 1,241 2,729
High-Medium 5 230 16,560 - - 1,289
High 7 230 18,860 - - -
An alternative analysis was carried out to examine the maximum number of interventionalcardiologists that might be required under different demand assumptions. In this scenario, it wasassumed that the mean caseload of existing operators does not change from the current 210procedures/year. To meet the highest projected growth rate (target + 20%), a net increase of 38interventional cardiologists would be required, or just under eight new entrants (net of exits) peryear. However, if this number of interventional cardiologists is added to the pool but the growthrate is actually at the target projection, then the mean caseload per operator will fall to 175/year in2005/06. Although this still exceeds the recommended minimum on an aggregate basis, therewould likely be a significant number of operators who individually fall below an acceptableminimum volume under this scenario.
Finally, to determine the degree of flexibility in terms of caseload that might be required of agiven workforce to deal with unpredictable demands, the mid-range physician growth assumption(five new interventional cardiologists per year) was projected against the lowest and highestdemand assumption (target rate and target rate + 20%). Under these conditions, the meancaseload per physician would be no lower than 206/year, and no higher than 250/year.
Based on these scenarios, the Panel believes that the mid- to high scenarios for physician supply(net increase of five to seven interventional cardiologists per year or 25 to 35 over the next fiveyears) most likely corresponds to actual needs, but may result in capacity constraints if theproposed targets are exceeded by a significant margin. This supply scenario balances theflexibility to meet greater than anticipated demand with the avoidance of over-supply (assumingtargets are not exceeded by a significant margin) and dilution of individual experience.
The Greater Toronto Area Community Cardiologists (GTACC) organization submitted ananalysis of training requirements for PCI prepared by the Hay Group.47 In its report, the Hay
46 As recommended by CCN’s Target Setting Working Group.
Page 91
Expert Panel on Invasive Cardiology in Ontario
Group estimates a need for an additional 52 interventional cardiologists by 2005/06. This higherestimate can be reconciled with the Panel’s estimate as follows:
• The Hay Group assumed a lower average annual volume per operator (150 cases peryear compared to the Panel’s estimate of 210 to 230 cases).
• The Hay Group estimate is based on the projected increase in procedure volumesfrom 1998/99 to 2005/06, a seven-year period, compared to the five-year period inthe Panel’s analysis (2000/01 to 2005/06). Thus, the Panel’s estimate is net of newinterventionalists that began practice in Ontario over the past two years.
Cath Rooms
At the time of this report, there were 32 cath rooms in operation in Ontario, three of which arealso used for electrophysiology studies (EPS) 48An additional five rooms had been approved, andwere expected to be operational within 12 months.
Estimating the capacity of an individual cath room is difficult for many reasons:
• At low volume centres, the room(s) may not be operating at full capacity.
• The effective capacity within a given institution depends on other competing demands forthe same facility. Although diagnostic cath and PCI represent the majority of proceduresperformed within most cath rooms, some are also used for diagnostic and/or ablativeelectrophysiology procedures, temporary or permanent pacemaker implant, peripheral orcerebrovascular interventions, and myocardial biopsies.
• The proportion of ad-hoc PCI (cath and PCI performed at the same sitting) varies fromcentre to centre, and affects the throughput of the room, in that the total time required isless than that for one cath plus one PCI.
• Adding a second cath room generally does not double the capacity of the centre, becausethe support staff is not doubled and some time is lost to the additional administrativeoverhead. It is estimated that each additional room provides about 75-80% increase incapacity beyond that of a single room.
• Room capacity varies with the number of working hours per day. Operating longer hourshas implications not only for the cath lab, but also for associated nursing units (e.g.,outpatient area, coronary care unit). The current and anticipated future nursing shortagemakes assumptions about expansion difficult. On one hand, it may be difficult to recruitstaff to extend hours in a given facility; on the other hand, an existing large facility mayhave a sufficient “critical mass” of nurses to allow flexibility in scheduling that a smallerfacility may not be able to achieve.
The time required to construct and operationalize a new cath room varies widely. In general, anexisting cath facility will be able to add an additional room more quickly than a room can bebrought on line at a new centre. However, in most hospitals, relocation of existing occupantsfollowed by renovation can be time consuming, unless space has previously been “roughed in.”
47 Training Requirements for Providing Angioplasty Services: A submission to the CCNO Expert Panel –February 19th 2001, Hay Group48 Shared cath labs are at Kingston General Hospital, Sunnybrook & Women’s College Health SciencesCentre and the University Health Network.

Page 92
Expert Panel on Invasive Cardiology in Ontario
The CCN Panel on Cardiac Catheterization Laboratory Services49 recommended that existing cathfacilities should ideally operate 10 hours per day, or 2,300 hours per year once maintenance andholiday times were factored in. Based on this recommendation, the 37 cath rooms that areexpected to be operational by the end of 2001/02 will represent about 85,000 working hours peryear. The Cath Panel also estimated that, including changeover time between cases, a diagnosticcath required approximately one hour and PCI approximately two hours. Most interventionalcardiologists believe that routine PCI cases have become quicker due to the use of modern stents.However, a concurrent trend toward increasingly complex multi-vessel or multi-device PCI casesoffsets this trend to some degree, and may result in the procedure time being highly dependent onthe case mix within a given centre.
A complete analysis of the actual capacity represented by these rooms requires more detailedconsideration of other services such as electrophysiology and biopsy. However, as with theanalysis of physician supply, a “ballpark” estimate is possible and provides some context fordiscussion of the need for additional facilities.
To better understand the potential for a shortfall in lab capacity, we analyzed threesupply/demand scenarios:
• Low demand scenario - In this scenario, it was assumed that:
o PCI cases would require 25% less lab time than the current estimate of two hours(i.e., 1.5 hours/PCI)
o Electrophysiology (EPS) would consume about 15% of available lab time wherethese facilities are shared
o The number of procedures performed is as projected by the Target SettingWorking Group
• Medium demand scenario - In this scenario, it was assumed that:
o PCI cases would require 15% less lab time than the current estimate of two hours(i.e., 1.7 hours/PCI).
o EPS would consume about 20% of available lab time where these facilities areshared.
o The number of procedures performed exceeds the projections of the TargetSetting Working Group by 10%.
• High demand scenario: - In this scenario, it was assumed that:
o PCI cases would require the full two hours.
o EPS would consume about 20% of available lab time where these facilities areshared.
o The number of procedures performed exceeds the projections of the TargetSetting Working Group by 20%
In all three scenarios, the labs are assumed to be utilized at full capacity (i.e., 10 hours per day),and a cath is assumed to require one hour.
49 Cardiac Care Network of Ontario, Consensus Panel on Cardiac Catheterization Services in Ontario, FinalReport and Recommendations, September 1997.
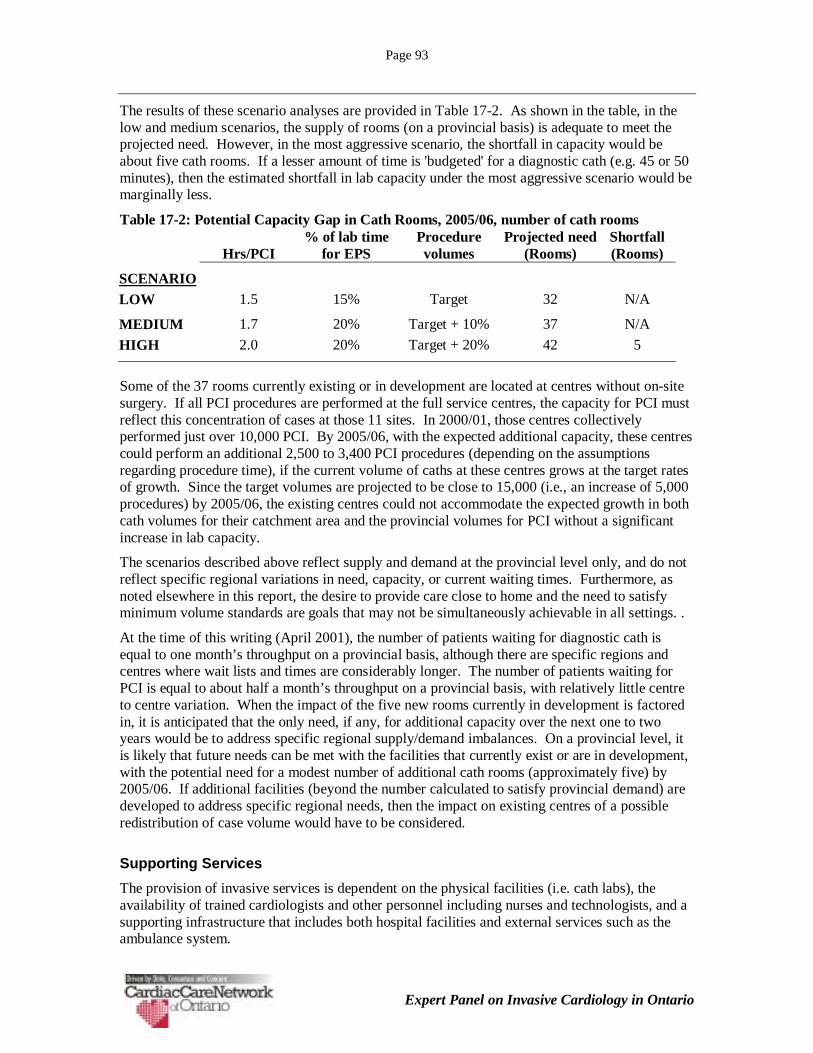
Page 93
Expert Panel on Invasive Cardiology in Ontario
The results of these scenario analyses are provided in Table 17-2. As shown in the table, in thelow and medium scenarios, the supply of rooms (on a provincial basis) is adequate to meet theprojected need. However, in the most aggressive scenario, the shortfall in capacity would beabout five cath rooms. If a lesser amount of time is 'budgeted' for a diagnostic cath (e.g. 45 or 50minutes), then the estimated shortfall in lab capacity under the most aggressive scenario would bemarginally less.
Table 17-2: Potential Capacity Gap in Cath Rooms, 2005/06, number of cath rooms
Hrs/PCI% of lab time
for EPSProcedurevolumes
Projected need(Rooms)
Shortfall(Rooms)
SCENARIOLOW 1.5 15% Target 32 N/A
MEDIUM 1.7 20% Target + 10% 37 N/A
HIGH 2.0 20% Target + 20% 42 5
Some of the 37 rooms currently existing or in development are located at centres without on-sitesurgery. If all PCI procedures are performed at the full service centres, the capacity for PCI mustreflect this concentration of cases at those 11 sites. In 2000/01, those centres collectivelyperformed just over 10,000 PCI. By 2005/06, with the expected additional capacity, these centrescould perform an additional 2,500 to 3,400 PCI procedures (depending on the assumptionsregarding procedure time), if the current volume of caths at these centres grows at the target ratesof growth. Since the target volumes are projected to be close to 15,000 (i.e., an increase of 5,000procedures) by 2005/06, the existing centres could not accommodate the expected growth in bothcath volumes for their catchment area and the provincial volumes for PCI without a significantincrease in lab capacity.
The scenarios described above reflect supply and demand at the provincial level only, and do notreflect specific regional variations in need, capacity, or current waiting times. Furthermore, asnoted elsewhere in this report, the desire to provide care close to home and the need to satisfyminimum volume standards are goals that may not be simultaneously achievable in all settings. .
At the time of this writing (April 2001), the number of patients waiting for diagnostic cath isequal to one month’s throughput on a provincial basis, although there are specific regions andcentres where wait lists and times are considerably longer. The number of patients waiting forPCI is equal to about half a month’s throughput on a provincial basis, with relatively little centreto centre variation. When the impact of the five new rooms currently in development is factoredin, it is anticipated that the only need, if any, for additional capacity over the next one to twoyears would be to address specific regional supply/demand imbalances. On a provincial level, itis likely that future needs can be met with the facilities that currently exist or are in development,with the potential need for a modest number of additional cath rooms (approximately five) by2005/06. If additional facilities (beyond the number calculated to satisfy provincial demand) aredeveloped to address specific regional needs, then the impact on existing centres of a possibleredistribution of case volume would have to be considered.
Supporting Services
The provision of invasive services is dependent on the physical facilities (i.e. cath labs), theavailability of trained cardiologists and other personnel including nurses and technologists, and asupporting infrastructure that includes both hospital facilities and external services such as theambulance system.

Page 94
Expert Panel on Invasive Cardiology in Ontario
It is widely recognized that there is a serious nursing shortage in Canada, and this shortage isprojected to worsen over the next few years. The availability of nurses with the training andexperience needed to work in a cath lab may become a limiting factor in the ability to expandinvasive cardiology services. The Panel did not attempt to analyze the potential impact of nursingshortages. However, it is evident that during a time of reduced supply of qualified nurses,recruitment of experienced nurses away from an existing cath centre to a new or expanding centredoes not necessarily result in a net expansion of system capacity.
A reliable and flexible system of ambulance services is necessary to implement a regionalizedmodel of care such as the cath lab system in Ontario. Transfer of patients from their homehospital to a nearby or occasionally distant cathing hospital may be needed on a scheduled oremergency basis. Efficient utilization of supporting hospital resources demands that a largeproportion of diagnostic cath procedures be done on an outpatient basis, which means thatpatients from other hospitals must often be transferred back to their home hospital by ambulanceshortly after their cath procedure.
If additional services are to be implemented (such as widespread use of direct PCI for acutemyocardial infarction), then additional demands will be placed on the emergency response andtransport system. Unfortunately, there are recent indications that ambulance services are notkeeping pace with the rapid increase in demand for their services that has arisen from the overallincrease in the use of invasive services. This also has the potential to limit further rapidexpansion of invasive services.
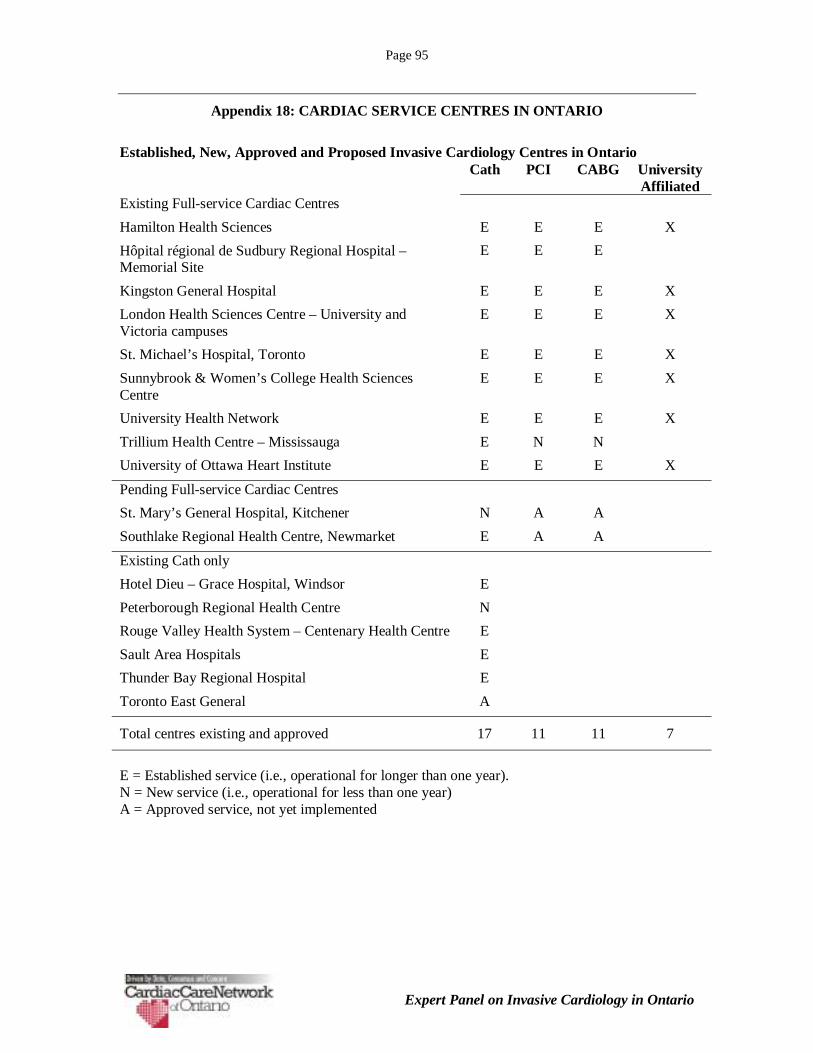
Page 95
Expert Panel on Invasive Cardiology in Ontario
Appendix 18: CARDIAC SERVICE CENTRES IN ONTARIO
Established, New, Approved and Proposed Invasive Cardiology Centres in OntarioCath PCI CABG University
AffiliatedExisting Full-service Cardiac Centres
Hamilton Health Sciences E E E X
Hôpital régional de Sudbury Regional Hospital –Memorial Site
E E E
Kingston General Hospital E E E X
London Health Sciences Centre – University andVictoria campuses
E E E X
St. Michael’s Hospital, Toronto E E E X
Sunnybrook & Women’s College Health SciencesCentre
E E E X
University Health Network E E E X
Trillium Health Centre – Mississauga E N N
University of Ottawa Heart Institute E E E X
Pending Full-service Cardiac Centres
St. Mary’s General Hospital, Kitchener N A A
Southlake Regional Health Centre, Newmarket E A A
Existing Cath only
Hotel Dieu – Grace Hospital, Windsor E
Peterborough Regional Health Centre N
Rouge Valley Health System – Centenary Health Centre E
Sault Area Hospitals E
Thunder Bay Regional Hospital E
Toronto East General A
Total centres existing and approved 17 11 11 7
E = Established service (i.e., operational for longer than one year).N = New service (i.e., operational for less than one year)A = Approved service, not yet implemented

Page 96
Expert Panel on Invasive Cardiology in Ontario
Appendix 19: CATH LABS IN ONTARIO
Established and Approved Cath Rooms in OntarioExisting Approved50
Existing Full-service Cardiac Centres
Hamilton Health Sciences 3
Hôpital régional de Sudbury Regional Hospital –Memorial Site
1 1
Kingston General Hospital 1 1
London Health Sciences Centre – University andVictoria campuses
3
St. Michael’s Hospital, Toronto 3
Sunnybrook & Women’s College Health SciencesCentre
3
University Health Network 6
Trillium Health Centre – Mississauga 2
University of Ottawa Heart Institute 3
Pending Full-service Cardiac Centres
St. Mary’s General Hospital, Kitchener 1 1
Southlake Regional Health Centre, Newmarket 1 1
Existing Cath only
Hotel Dieu – Grace Hospital, Windsor 1
Peterborough Regional Health Centre 1
Rouge Valley Health System – Centenary Health Centre 1
Sault Area Hospitals 1
Thunder Bay Regional Hospital 1
Toronto East General 1
Total cath rooms, existing and approved 32 5
50 Expected to be operational within 12 months.

Page 97
Expert Panel on Invasive Cardiology in Ontario
Appendix 20: CANADIAN CARDIOVASCULAR SOCIETY STANDARDS
Standards for Training in Adult Cardiac Catheterization and Angiography51
CATHETERIZATION AND ANGIOGRAPHY SUBCOMMITTEE OF THE CANADIAN CARDIOVASCULAR SOCIETYCOMMITTEE ON STANDARDS
ROBERT M MILLER MD (CHAIR), BLAIR O'NEILL MD, DAVID JOHNSTONE MD, J ROBERT RAE MD
The ability to intervene successfully, ameliorate symptoms and favourably influence the prognosis has made cardiaccatheterization and angiography essential to modern cardiology. Therefore all cardiologists must be knowledgeable inthese areas.
GENERAL ASPECTS OF TRAINING
There should be three levels of training for cardiologists;
Level 1 Basic - for the cardiologist not performing diagnostic catheterization or angiography.
Level 2 Diagnostic - for the cardiologist performing diagnostic catheterization or angiography.
Level 3 Interventional - for the cardiologist performing diagnostic catheterization, angiography, and angioplasty orother such advanced procedures as they develop.
Level 1 Basic should be achieved by all trainees in the core program. Level 2 Diagnostic may be achieved during the coreprogram using elective time. Level 3 Interventional would normally be acquired during a dedicated fellowship year aftersuccessful completion of an approved core training program.
STRUCTURE OF THE TRAINING PROGRAM
Training should occur in a program recognized by the Royal College of Physicians and Surgeons of Canada.
Faculty - there must be a director of the catheterization laboratory who has primary responsibility for administration andteaching in the laboratory. There should be more than one competent faculty cardiologist participating in the training andall faculty should have their fellowships and be recognized as experts in cardiac catheterization. There should be at leastone faculty physician recognized as expert in angioplasty.
Facilities - there must be a fully equipped and staffed laboratory in compliance with cardiovascular services in hospitals(1). There must be a percutaneous transluminal coronary angioplasty (PTCA) program in operation. The laboratory mustbe within reasonable access to a cardiac and vascular surgery program.
Patients - all trainees must be exposed to a large volume of patients exhibiting varied pathology including a suitablemixture of valvular, myopathic, congenital, pericardial and ischemic heart diseases. There must be exposure to acutely illpatients with cardiogenic shock, myocardial infarction and other unstable conditions. There must be post-PTCA andcardiovascular surgery patients available for assessment and follow-up.
Conferences - all trainees regardless of subsequent career goals must attend a regular schedule of formal and/orinformal teaching conferences to supplement the learning experience of the catheterization laboratory. This shouldencompass many formats from didactic lectures to presurgery conferences. These sessions do not replace the necessaryinteractions between trainee and attending cardiologist involving direct patient care and management.
Research - all trainees should be encouraged to participate in research in the catheterization laboratory.
COMPONENTS OF TRAINING
Level 1 Basic Training
ExpectationsAfter a core cardiology training program the trainee must have a clear understanding of: Indications and contraindicationsfor cardiac catheterization and angiography, angioplasty and cardiac surgery.
51 As reported on the Canadian Cardiovascular Society web-site at www.ccs.ca. Reproduced withpermission of the Canadian Cardiovascular Society.

Page 98
Expert Panel on Invasive Cardiology in Ontario
Complications and their management.Medical and surgical implications of the findings at catheterization. Pathophysiology and ability to interpret thehemodynamic and angiographic data such as:
i. normal and abnormal pressures and wave formsii. cardiac outputiii. resistancesiv. valve areas and intracardiac shuntsv. coronary angiographyvi. intracardiac and great vessel angiography
Methods of training
All trainees will spend a minimum of four months in the cardiac catheterization laboratory during which they mustparticipate in procedures involving at least 100 patients with whom they are involved from precatheterization evaluationto final disposition predischarge. It is recommended that this number should not exceed 200 patients so that themaximum educational value can be derived from each case.
AssessmentThe supervisor(s) should provide written assessment to the program director. This evaluation should include assessmentofthe number of studies performed as well as the technical interpretive and judgemental skills of the trainee. A log bookshould be maintained by the trainee recording for each case the supervising physician, clinical problem, proceduresperformed and outcome including complications. This does not qualify for a letter of competence in cardiaccatheterization.
Level 2 Diagnostic
ExpectationsIn addition to Level 1 Basic Training the trainee should have:A working knowledge of catheterization laboratory equipment to include:
i. physiologic recorders, pressure transducers and blood gas analyzer
ii. practical radiation physics
iii. radiology equipment
iv. quality control methods in the catheterization laboratory
Sufficient practical experience with:
i. right and left heart catheterization, selective coronary angiography, left and right ventriculography and great vessel angiographyii. myocardial biopsyiii. transseptal catheterizationiv. nonfemoral arterial accessv. intra-aortic balloon pump insertion
Method of trainingIn addition to Level 1 training, a minimum of four further months of training in the catheterization laboratory is required.The trainees total experience should include performing at least 300 catheterization procedures with 200 procedures asprimary operator.
AssessmentEvaluation will include documentation in the form of a log book to contain supervising physician, clinical information,procedures performed and outcome of procedure including complications. The competence, judgement and technicalskills of the trainee will be documented by the director of the laboratory and program director or other catheterizingphysician. Such an evaluation may qualify for a letter of competence in diagnostic catheterization. This letter ofcompetence should include a paragraph commenting on the necessity of maintenance of competence.
Level 3 InterventionalExpectationsWill involve post core training.Must meet Canadian Cardiovascular Society standards for training in angioplasty (see next section).

Page 99
Expert Panel on Invasive Cardiology in Ontario
TRAINING FOR ESTABLISHED PHYSICIANS AND PRACTICING CARDIOLOGISTS
CredentialsLevel 2 Diagnostic Training certificates of competence would normally be available to any physician holding certification incardiology who successfully completed Level 2 training at a university affiliated training centre or any other physician whohasa fellowship other than in cardiology and has completed Level 2 training with a suitable period of extra training incardiology.Any physician already credentialled in his/her institution to do these procedures would continue to be expected tomaintain competence at Level 2, performing 150 procedures per year as outlined below. Level 3 Interventional Trainingcertification of competence would normally be reserved for a physician with certification in pediatric or adult cardiologywho has successfully completed Level 3 training in a recognized training program.
RetrainingThe return to catheterization activities in diagnostic catheterization after absence of some period of time from thelaboratory requires retraining. The type and scope of retraining would require individual consideration depending on theextent of previous work experience and time away from the catheterization laboratory. It would be appropriate to allowthe director of cardiology and the residency training director to formulate and supervise the retraining program and toinsist on a minimum of 100 cases with 75 as primary operator.
It is recommended from a hospital and credentialling point of view that retraining be divided into two types:
When an institution is concerned with maintenance of competence due to a short absence caused by a sabbatical leave orshort term illness, retraining may occur within the home institution.
In the case of a prolonged absence, competency concerns by the institution or credentialling body would normally lead tore-training at a centre other than the home institution.
AssessmentThe same assessment process will occur as with Level 2 diagnostic proficiency.
MAINTENANCE OF COMPETENCE
To ensure ongoing expertise it is vital that laboratory staff maintain their skills. It has been shown that laboratories doingmore than 500 catheterizations per year have the lowest rate of complications. Considering modern efficiencyexpectations (1000 cases per year) (1), 500 cases would be considered a minimum per laboratory. It is recommendedthat a minimum of 150 cases per year be performed per operator in the laboratory. The laboratory director should haveinformation available to allow the staff to assess parameters of operator competence such as total procedure time,fluoroscopy time, contrast material usage, complications and diagnostic quality of the studies.
REFERENCES
1."Cardiovascular services in hospitals" Health and Welfare Canada, 1986.2.Task Force 3: Training in cardiac catheterization and interventional cardiology. J Am Coll Cardiol 1995;25:14-6.3.Guidelines for coronary angiography. Circulation 1987;76:963A-77A.4.Guidelines for PTCA. J Am Coll Cardiol 1993;22:2033-54.

Page 100
Expert Panel on Invasive Cardiology in Ontario
Standards for Coronary Angioplasty Training
CORONARY ANGIOPLASTY SUBCOMMITTEE OF THE CANADIAN CARDIOVASCULAR SOCIETY COMMITTEEON STANDARDS
JEAN-FRANCOIS MARQUIS MD (CHAIR), MARK HENDERSON MD, MERRILL KNUDTSON MD, AMINUL HAQ MD(DECEASED)
Training in coronary angioplasty procedures is a Level 3 component of training, which is acquired during a fellowship yearafter the training requirements for cardiology certification have been fulfilled. Institutions supporting an angioplastytraining program should be affiliated with a university training program, perform more than 400 angioplasty proceduresper year and have at least two cardiologists performing angioplasty procedures. The prerequisites and trainingrequirements for this procedure are listed below:
All individuals seeking training in coronary angioplasty must have successfully completed an approved cardiology coretraining program and/or be eligible to write the examinations in cardiology of The Royal College of Physicians andSurgeons of Canada.
During their core training program, trainees must have performed, under appropriate supervision, at least 300 cardiaccatheterization and coronary angiography procedures. They must demonstrate proficiency in the laboratory and an abilityto perform catheterizations independently.
Individuals training in angioplasty require a further 12 months in the cardiac catheterization laboratory under the auspicesof a university cardiology training program. During this time they should gain further general experience in all aspects ofcardiac catheterization and coronary angiography. In addition each individual must perform under appropriate supervision250 to 300 coronary angioplasty procedures which are defined as balloon angioplasties and/or other procedures requiredfor coronary interventions as are deemed clinically necessary, e.g., stents, atherectomies. The candidates must havesupervised exposure and training in new percutaneous therapeutic interventions that are available in the centre wherethe training takes place.
During training, supervisors must ensure that a graded degree of responsibility is assumed by the trainee until theindividual is capable of independent angioplasty. Coronary angioplasty training must include the following:
• patient selection• review of basic pathology of atherosclerotic disease and reaction of vessel wall to injury pre-angioplasty
assessment• the angioplasty procedure• postangioplasty care• long term follow-up care• management of complications
Documentation of the number of angioplasty procedures performed must be maintained in the form of a log book.
The established angiographer, who has been in practice for some time, and who wishes to perform angioplasty mustfulfill the same requirements as standard fellowship training.
At the end of their training and before becoming an independent operator, all individuals must receive a certificate ofcompetence from their training institution.
To maintain competence, approximately 100 cases per year should be performed. These standards will be subject torevision as newer techniques are adopted.

Page 101
Expert Panel on Invasive Cardiology in Ontario
GLOSSARY
Term DefinitionAd hoc PCI When the diagnostic cath and PCI are performed at the same sitting.
Also referred to as same sitting, plus-minus, or double setup PCI.
As close to home aspossible
One of the policy directions articulated in the Business Plan forOntario’s Ministry of Health and Long-Term Care.
Cardiac Care Network ofOntario (CCN)
The Cardiac Care Network of Ontario (CCN) is an advisory body tothe Ontario Ministry of Health and Long-Term Care dedicated toimproving quality, efficiency, access and equity in the delivery ofcardiac services in the Canadian province of Ontario.
Cath or Diagnostic cardiaccatheterization
A diagnostic procedure in which a catheter is introduced into alarge vein and threaded through the circulatory system to the heart.
Coronary Artery BypassGraft (CABG)
Open heart surgery in which a prosthesis or section of blood vesselis grafted onto one of the coronary arteries, bypassing a narrowingor blockage in a coronary artery.
Direct PCI See Primary PCI
Fibrinolytic therapy Therapy with clot dissolving drugs.
Interventional Cardiology The term most often used to refer to the practice of cardiologyrelated to invasive therapeutic cardiac catheterization procedures(i.e., PCI).
Invasive cardiology For ease of reference in this report, both diagnostic and therapeuticprocedures are referred to collectively as “invasive cardiology.”
Ministry of Health andLong-Term Care(MOHLTC)
Ontario’s Ministry with responsibility for Health and Long-TermCare, including cardiac services.
Myocardial infarction (MI) Necrosis of a portion of cardiac muscle caused by obstruction in acoronary artery.
PCI Percutaneous Coronary Intervention
Percutaneous TransluminalCoronary Angioplasty(PTCA)
A technique in the treatment of atherosclerotic coronary heartdisease and angina pectoris in which some plaques in the arteries ofthe heart are flattened against the arterial walls, resulting inimproved circulation. The procedure involves threading a catheterthrough the vessel to the plaque and inflating and deflating a smallballoon at the tip several times, then removing the catheter.
Primary PCI PCI is increasingly being used to open occluded arteries in patientswith acute myocardial infarction (AMI), which is referred to as‘primary’ or ‘direct’ PCI.
Revascularization The restoration by surgical means of blood flow to an organ ortissue being replaced as in bypass surgery.
Stent A tubular metallic scaffold used in supporting body openings.
Thrombolysis Therapy with clot dissolving drugs.