experimentalposteriorperforating injury - british journal...
TRANSCRIPT

British Journal of Ophthalmology, 1986, 70, 561-569
Experimental posterior perforating ocular injury: acontrolled study of the gross effects of localised gammairradiationU CHAKRAVARTHY, C J F MAGUIRE, AND D B ARCHER
From the Department of Ophthalmology, Royal Victoria Hospital, Belfast, Northern Ireland
SUMMARY A pilot study on the effect of localised irradiation applied to the site of a standardperforating injury in the rabbit eye, showed that gamma rays limited the formation of post-traumatic vitreoretinal membranes. A controlled study was therefore undertaken to confirm thisobservation. Twenty-four pairs of rabbits underwent a standard perforating injury in the right eye.One rabbit of each pair received a radioactive ophthalmic '0Cobalt applicator and the other adummy applicator. Nineteen of 24 non-irradiated eyes developed vitreoretinal membranes, withassociated traction retinal detachment. Only four of 24 irradiated eyes developed traction retinaldetachment.
Post-traumatic retinal dysfunction is a major cause ofpartial or complete visual loss following perforatinginjuries of the eye.' 2 In such eyes the proliferation ofcells at the site of injury gives rise to vitreoretinalmembranes, a condition known as proliferativevitreoretinopathy (PVR).3-5 The subsequent contrac-tion of these membranes may detach the retina fromthe underlying pigment epithelium and choroid,resulting in damage to retinal structure and impair-ment of retinal function.
Histological studies of post-traumatic vitreoretinalmembranes have shown that the majority of the cellsare fibroblasts, retinal pigment epithelial cells, glialcells, and macrophages embedded in a collagen andfibrin matrix.°"' Some cells with the properties offibroblasts are seen in ultrastructural studies tocontain contractile proteins and to have certaincharacteristics of smooth muscle cells." 12 Such cellsare termed myofibroblasts, and their contractileproperties are probably responsible for active con-traction of vitreoretinal membranes. '" The matrix onwhich the myofibroblasts exert traction is providedby the vitreous framework or collagen elaborated bythe fibroblasts themselves.'3The management of PVR is principally surgical,
involving vitrectomy and removal of membranesto permit repositioning of the retina.'4 AlthoughCorrespondence to Miss U Chakravarthy, FRCS, Department ofOphthalmology, Royal Victoria Hospital, Grosvenor Road, BelfastBT12 6BA, Northern Ireland.
anatomical success may be achieved, visual resultsmay be disappointing."' Furthermore the manipula-tion and cutting of vitreous bands during vitrectomymay promote the formation of new membranes.'6Attempts have been made to limit membrane forma-tion by the use of corticosteroids.'" These drugs notonly limit the invasion and lysis of the vitreouscollagen by inflammatory cells but also have aninhibitory effect on the growth of fibroblasts. How-ever, intraocular structures are largely inaccessible todrugs administered on conventional lines, and, des-pite intravitreal injection of large doses of cortico-steroids, the drug disappears too rapidly to providesustained inhibition.'7
Antimitotic agents, which are inhibitors of cellularproliferation, particularly 5 fluorouracil, have beenused recently with some success in patients withproliferative vitreoretinopathy.'8 This drug is toxicto the retina and capable of abolishing the electro-retinogram at doses very close to the therapeuticrange.'9 Because of increased clearance of fluoro-uracil from eyes subjected to vitrectomy, repeatedadministration of the drug is necessary to achieve atherapeutic effect. This can result in peak intraocularlevels of the drug after each injection, and itsintraocular use in conjunction with gas tamponademay result in its concentration at toxic levels on theretinal surface.20
P-aminopropionitrile2' and penicillamine22 havebeen tried in experimental animal studies. Both
561
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

U Chakravarthy, CJ FMaguire, andD B Archer
drugs reduce the formation of new collagen byinhibiting enzymes that are responsible for the crosslinking between collagen molecules. The fibroblastsare therefore deprived of a scaffolding on which togrow and exert their contractile force.Haematoporphyrin photoradiation therapy has
been tested in the animal model.' Haematopor-phyrin derivative binds wells to the cell membrane ofdividing cells and, when followed by photoradiation,results in destruction of the cell.
lonising irradiation offers an alternative approachin the management ofproliferative vitreoretinopathy.It had long been known to inhibit the growth anddivision of cells, and this property of gamma rayshas been studied extensively in tissue culture.2425Belkin et al. used single-dose, whole-eyeball, gammairradiation with some success to inhibit the formationof experimental post-traumatic intraocular mem-branes.I Such vitreoretinal membranes can be createdsuccessfully and reproducibly in the experimentalanimal model,27 and the cellular proliferation andmembrane formation is most pronounced at the siteof perforation.27I We therefore considered the localapplication of gamma rays to the site of injury as alogical method of preventing the formation of vitreo-retinal membranes.Radioactive 'cobalt applicators originally devised
by Stallard' working in conjunction with Innes3"have been used extensively in the treatment ofneoplasms of the eye. The ophthalmic 'cobalt appli-cator was therefore chosen as a convenient source ofionising rays to provide continuous irradiation at thesite of injury. The CKA 1 applicator (AmershamInternational PLC) has an external diameter of 7 mmand a distribution of radioactive wcobalt (internaldiameter 5 mm) within a platinum casing (activity 26MBq). When it is applied to the sclera, the tissue-absorbed dose in the central axis of the plaque,
Rads/6 daysTumour
Sciera
CKA1 dish typeFig. lA Isodose curvesforCKA 1 plaque (reproduced bycourtesy ofAmersham International PLC).
calculated by established dosimetry curves,3" at adepth of 1 mm, is 50 Gy/24 hours, and at a depth of 4mm is 11 Gy in 24 hours (Figs. 1A and 1B). It wasconsidered advantageous to have such a depth-doserelationship, since the proliferating membrane has itsorigins at the wound. This site would thereforereceive maximum irradiation, while the level ofirradiation received by tissues at a greater distancefrom the plaque and remote to the central axis wouldbe greatly reduced.
Radiation retinopathy following application of a'0cobalt plaque to neoplasms of the eye has beenreported with doses in excess of 50 Gy to the tumourapex when the height of the tumour was 5-10 mm.32This resulted in doses in excess of450 Gy to the retinaand choroid, which are anatomically closer to theplaque. With localised doses of less than 200 Gy tothe retina and choroid, radiation retinopathy doesnot occur, though scarring results with nerve fibreloss. However, even this dose may be toxic if theplaque is applied over the central retina or the majorblood vessels.33 We chose to apply the radioactive'cobalt plaque to the peripheral sclera for 48 hours,at which time the sclera received a dose of 100 Gy andthe retina and choroid received a dose of approxi-mately 80 Gy. This dose was less than the minimum
Grays/dayin tissue
50- 0
40\
30-
20-
10-9\8-
5-
4-
3-
2-
0 1 2 3 4 5 6 7 8 9 101112131415
Depth from plaque in mmFig. lB Central axis dose ratefor CKA 1 plaque.
562
1
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

Experimentalposteriorperforating ocular injury:
Table 1 Details ofpost-mortem appearance ofthefour non-irradiated andfour irradiated eyes which constituted thepilotstudy. Two animals, one irradiated and the other a control, developed an infective endophthalmitis and were excludedfromthepilotstudy
Time ofdeath Non-irradiated eyes Irradiated eyesafter injury
Serial Post-mortem appearance Serial Post-mortem appearancenumber number
7 Days 10 The blood clot was loculated in mid- 5 The blood clot was loculated in mid-vitreous. Condensed vitreous and fibrin vitreous and fibrin bands extendedbands extended from the site of perforation from the site of perforation into theto retina opposite the wound vitreal blood clot and to retina
diametrically opposite the wound14 Days 7 A greyish membrane stretched from the 1 The wound was sealed on the retinal
wound into the vitreous, and along the aspect by greyish fibrous tissue.surface of the retina, adjacent to the site of Tenuous fibrinous bands extendedperforation from the wound into the vitreous
21 Days 2 A vitreoretinal membrane was present at 3 The site of injury was represented by athe site of perforation, attaching distally to pigmented chorioretinal scar. Thethe medullary rays, ciliary body, nasal vitreous was clear apart from bloodretina, and lens. A traction retinal remnantsdetachment involved the medullary rays andnasal retina
42 Days 6 There was extensive membrane formation 4 A membranous stalk stretched fromwith a total retinal detachment the site of perforation into the
vitreous with no distal attachment. Atthe base of the stalk a chorioretinalscar with surrounding pigmentationindicated the site of injury
tumoricidal doses used in the past and half theminimum reported dose likely to cause radiationretinopathy.We performed a pilot study on 10 rabbit eyes that
were subjected to a standard perforating injury basedon the Cleary and Ryan animal model.3 Five of theserabbits acted as controls, and the injured eye of theremaining five rabbits was irradiated with the 5 mmCKA 1 ophthalmic 6'cobalt applicator (externaldiameter of 7 mm) for 48 hours after injury. Therabbits were killed sequentially for a period of up tosix weeks and the details of the post-mortem findingsare given in Table 1. Non-irradiated eyes developedextensive vitreoretinal membranes, with associatedtraction retinal detachement. Irradiated eyes bycontrast developed focal scars at the site of injury,and, if a membrane was present, it was attenuatedwithout distal attachment to other intraocular struc-tures. A controlled study was therefore carried outon 48 pigmented rabbits in order to confirm thisfinding statistically.
Materials and methods
Pigmented rabbits, weight 2 kg, of either sex wereused. The animals were randomly divided into twogroups of 24 each, one of which was assigned toreceive the radioactive 'cobalt plaque and the other adummy plaque, the key to the code being held by the
animal technician. The dummy plaque was identicalin appearance with the radioactive applicator, so thatobserver bias was eliminated, and both radiated andcontrol rabbits underwent standardised surgical pro-ceedures. The rabbits were anaesthetised in pairswith pentobarbitone 60 mg/kg body weight, andthe anaesthesia supplemented with 1% retrobulbarlignocaine. The right eye of each animal was sub-jected to a standard perforating injury,3 whichconsisted of a conjunctival peritomy that was per-formed in the inferior temporal quadrant, and theglobe was then perforated by a full-thickness 5 mmcircumferential incision 4mm behind the limbus witha Bard-Parker scalpel blade. 0-2 ml of vitreous wasaspirated through the wound with a 20 gauge needleand replaced with the same quantity of autologousblood drawn from the rabbit's ear vein. The scleralwound was approximated with two 5-0 Ethibondsutures. On the basis of the preselected code either aradioactive or a dummy plaque was sutured over thesclera to cover the site of perforation (Fig. 2). Theconjunctiva was drawn up over the plaque andsecured to the limbus by a single stitch.The injured eyes were examined daily for the first
week and weekly thereafter. The extent and densityof vitreous haemorrhage and haze were assessed andscored on days 3 and 5; and later, when presentvitreoretinal membranes were graded on their extentand traction effects, on weeks, 2, 4, 6, 8, and 12
563
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

U Chakravarthy, CJ FMaguire, andD B Archer
Table 2 Details ofophthalmoscopic appearance as gradedandscored on day 3 and day 5 and weeks 2-12: key to codesusedfor ophthalmoscopic detail
Fig. 2 Site ofperforating injury ofrabbit eye covered by theophthalmic 'cobalt applicator.
Grade
Days3andS1 Retina clearly visible2 Retina visible through haze3 Retina obscured 1 quadrant4 Retina obscured >1 quadrant5 Retina obscured entirelyWeeks2-121 Scar only2 Fibrinous strands3 Membrane with no distal attachments4 Membrane attached to intraocular structures
with or without early detachment5 Membrane causing extensive retinal detachment
(Table 2). Four eyes suffered an accidental traumaticlens injury at the time of injection of blood into thevitreous, and subsequently developed lens opacities.One rabbit was found to have a second full-thicknessperforation of the globe just inferior to the medullaryrays in the temporal quadrant caused by the injectingneedle. All these animals were included in the study.The animals were killed sequentially at 1, 2, 3, 4, 6,and 12 weeks. Eight injured eyes were harvested ateach time interval, four ofwhich had been irradiated.The eyes were fixed in 10% formalin for 24 hours,after which the anterior segment was removed andthe posterior half of the globe photographed.The size and extent of the vitreal blood clot, the
length of the proliferative tissue, and its tractioneffects and the presence of a retinal detachment weregraded and scored (Table 3). Scleral wound healingwas assessed on the ability of the granulation tissue towithstand the stress of sectioning the eyeball. If thelips of the wound stayed together, it was consideredthat healing was established. If the granulation tissuebridging the wound disintegrated on sectioning theeyeball, the wound was considered as poorly healed.The wound and proliferative tissue were processedfor light microscopy and 7 gm sections were stainedwith haematoxylin and eosin.
Results
OPHTHALMOSCOPIC APPEARANCEThe results are summarised in Table 4. In both non-irradiated and irradiated eyes immediately afterinjury and injection of blood the vitreous haem-orrhage obscured all retinal details.
Non-irradiated eyes. At day 3 vitreous haze wasquite marked and prevented examination of theretina. By day 5 clearing of peripheral vitreousopacities had begun, and the injured retina was
visible on ophthalmoscopy. Fibrinous strands andcondensed vitreal fibrils extended from the site ofinjury into the mid-vitreal blood clot and towards themedullary rays of the retina. During week 2 greyishmembranes appeared initially at the site of perfora-tion but later extended along the fibrinous tracks intothe vitreous. The membranes typically attachedthemselves to the medullary rays and retina directlyopposite the wound, causing retinal folding at thesesites. They also became attached to the ciliary body,retina adjacent to the wound, and the posteriorsurface of the lens. At week 3 localised tractionretinal detachments were established at some pointswhere the proliferative membrane was adherent to
Table 3 Codes used to score appearance ofthe vitreal bloodclot, length ofvitreoretinal membrane, and the tractioneffects
Grade
Blood clotNoneClot <2mm diameterClot 2-5 mm diameterClot 5-10mm diameterClot filling vitreous chamberLength ofstalk orproliferating membraneStalk absentStalk <2mm longStalk 2-5 mm longStalk 5-10mm longStalk filling vitreous chamberTraction effects and distal attachments ofstalkAbsent stalk with no tractionStalk with no distal attachments and no tractionStalk attached to one intraocular structure with or without
local retinal detachmentStalk attached to more than one intraocular structure with
or without local retinal detachmentExtensive stalk with total retinal detachment
12345
2345
2
3
45
564
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

Experimentalposteriorperforating ocular injury:
Table 4 The ophthalmoscopic scores ofnon-irradiated and irradiated eyes arranged by week ofanimal's death. At laterweeks irradiated eyes had lowerscores when compared with non-irradiated eyes.
Non-irradiated Irradiated
Serial Ophthalmoscopic appearance Serial Ophthalmoscopic appearanceNumber Number
Day 3 Day 5 Week 2 Week 4 Week 6 Week 12 Day 3 Day 5 Week 2 Week 4 Week 6 Week 12
2 3 2 7 3 33 4 3 22 4 312 3 3 4 2 148 3 2 42 4 410( 4 4 4 45 4 3 323 4 3 5 18 3 2 130 3 4 4 14 3 2 233 5 5 5 29 3 2 28 3 3 4 27 3 3 2
20 4 5 4 17 3 3 221 3 3 4 9 3 3 141 5 4 2 40 5 4 3
1 4 4 3 3 35 3 2 1 119 3 3 1 1 26 3 3 3 325 4 5 4 4 16 4 4 3 332 4 4 2 2 43 3 2 1 16 3 3 4 4 4 15 3 2 1 1 113 4 3 3 4 4 44 4 4 2 2 1-38 3 3 2 3 3 39 3 3 3 4 447 4 3 3 4 4 36 4 3 3 2 25 4 3 3 4 4 5 31 4 4 3 3 2 1
11 4 3 2 2 2 2 46 4 3 4 4 4 424 4 3 3 3 3 3 37 4 3 2 2 128 3 3 3 4 4 4 34 3 3 1 1 1
the retina. All four eyes that were observed for 12weeks had subtotal or total retinal detachments, withextensive intraocular proliferation. Two of the non-irradiated eyes (animals 33 and 20) had an inadver-tent lens injury. Both these eyes had a severepostoperative inflammatory reaction, and retinaldetachment was present as early as one week.
Irradiated eyes: On day 3 cloudy vitreous obscuredthe retina as in the control eyes. By day 5 clearing ofthe peripheral vitreal blood clot had begun, and atweek 2 the media were sufficiently clear to permitobservation of the injury site by ophthalmoscopy.The injured retina was oedematous, and strands offibrin, condensed vitreal fibrils, and blood extendedfrom the site of injury into the mid-vitreous. Ataround 10 days these strands became attenuated inapproximately half the eyes, but in others they werereplaced by greyish membranes that stretched forshort distances into the vitreous from the site ofperforation. In most of the latter the distal ends of themembranes appeared to float freely in the vitreouswithout attachment to other intraocular structures.Between weeks 3 and 12 vitreous opacities in most
irradiated eyes continued to clear with no furthermembrane formation. Of the 12 irradiated eyes thatwere followed up for more than four weeks threedeveloped traction retinal detachments due to pro-
liferative vitreoretinopathy. One of the animals(rabbit 16) suffered a lens injury. This eye developeda severe uveitis in the immediate postinjury phase,and by week 2, when the vitreous debris had cleared,a vitreoretinal membrane and traction retinal detach-ment at sites of adherence of the membrane becameobvious. The second of the irradiated eyes thatdeveloped PVR (rabbit 46) suffered a double per-forating injury. This eye developed a vitreoretinalmembrane and traction detachment at the exitwound. The site of the entry wound remained flat.The third of the irradiated eyes that developed retinaldetachment (no 39) had no additional injury and yetfared badly. This eye developed a local retinaldetachment of the medullary rays.
Statistical analysis was performed by the non-parametric Mann-Whitney U test on ophthalmo-scopic scores of non-irradiated and irradiated eyes.The results were insignificant at the 5% level atday 3 and day 5. However, there was a significantdifference in scores between the two groups at all theremaining time intervals studied (p<005).
POST-MORTEM APPEARANCENon-irradiated eyesThe results are summarised in Table 5.Week 1. Three of four non-irradiated eyes had
565
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

U Chakravarthy, CJ FMaguire, andD B Archer
Table 5 Details ofpost-mortem appearance ofnon-irradiated eyes
Time of Serial Wound Vitreoretinal membranedeath number
Length Distal Tractioninmm attachments effects
1 Week 2 Gaping <2 None None3 Healed 2-5 MR RF12 Healed 2-5 MR None48 Healed 5-10 PR, CB, Lens IRF
2 Weeks 10 Healed 5-10 MR, CB, PR STRD23 Gaping >10 PR, OR, Lens LRD30 Healed >10 MR, OR, CB TRD33* Healed >10 MR, CB, Lens TRD
3 Weeks 8 Healed 2-5 PR LRD20* Healed >10 MR, CB TRD21 Healed 2-5 PR LRD41 Healed 2-5 PR None
4 Weeks 1 Healed 2-5 PR RF19 Healed 2-5 None None25 Healed >10 MR LRD32 Healed 5-10 MR LRD
6 Weeks 6 Healed 2-5 PR, CB LRD13 Healed 2-5 MR RF38 Healed 2-5 None None47 Healed 5-10 MR, OR LRD
12Weeks S Healed >10 MR, PR, CB TRD11 Healed >10 MR, PR, CB STRD24 Healed 2-5 PR LRD28 Healed 5-10 OR, CB STRD
Ciliary body CB, localised retinal detachment LRD, medullary raysMR, opposite retina OR, peripheral retina PR, retinal folds RF,subtotal retinal detachment STRD, total retinal detachment TRD.*Animals 33 and 20 suffered an accidental lens injury.
healed scleral wounds. In one eye the granulationtissue bridging the wound disintegrated on sectioningthe eyeball. In all eyes blood clot was present on theinner aspect of the wound and extended into thevitreous. In two eyes fibrinous bands and condensedvitreal fibrils stretched from the site of perforation tothe medullary rays and retina directly opposite thewound. In two other eyes a definite membrane waspresent, and this extended from the wound into thevitreous blood clot. In both these eyes the membranehad distal attachments to the medullary rays, ciliarybody, and opposite retina. Traction at these sites wasevident as retinal folding or wrinkling.Week 2. Three of four non-irradiated eyes had
healed scleral wounds. In all eyes the blood clot wasreplaced by fibrous vitreoretinal membranes (Fig. 3),which were thicker and more extensive than thosepresent at week 1. One eye had extensive exudationinto the vitreous and a total retinal detachment. Thiseye had a lens injury.Week 3. All eyes had healed scleral wounds. One
untreated eye had membrane formation with notraction on the retina. Two eyes had membranesexerting localised traction on the retina, and one had
extensive proliferative vitreoretinopathy and totalretinal detachment. This eye had suffered a lensinjury.Week 4. Scleral wound healingwas well established
in all four eyes. The fibrous membrane, whichwas present in all four eyes harvested at this timeinterval, extended into the vitreous from the site ofinjury and over the retinal surface. Three of the eyeshad localised retinal detachments and one had a totalretinal detachment. Pigmentary changes were pre-sent adjacent to the site of injury.Week 6. Three eyes had a fibrous membrane
adherent to peripheral retina causing a tractionretinal detachment. One eye had a short membranewhose distal end did not become attached to otherstructures, the retina staying flat.Week 12. All four eyes had extensive intraocular
membrane formation (Fig. 4). Three of these hadtotal retinal detachment and one had a localisedretinal detachment. The blood clot had undergonefurther lysis and shrinkage.
Irradiated eyesResults are summarised in Table 6.Week 1. Three of four irradiated eyes had poorly
healed scleral wounds. Blood clot was present in thevitreous adjacent to the wound. Fibrinous bands and
Fig. 3 Two-week non-irradiatedpost-mortem sectionedeyeball (rabbit JO), showingsite ofperforation (double blackarrows), with proliferation spreading over retinal surface.Elevated traction band (p) extending between site ofperforation and medullary rays (white arrow).
566
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

Experimentalposteriorperforating ocular injury:
Fig. 4 Post-mortem non-irradiated 12-week sectionedglobe (rabbitS), showing site ofperforation (white arrow)with proliferation extending oversurrounding retina. Totalretinal detachment, with traction tear ofretina adjacent to thesite ofperforation. mr=medullary rays.
condensed vitreal fibrils extended from the siteof perforation to retina diametrically opposite thewound. Only one of the four eyes had membraneformation, associated with a peripheral retinaldetachment. This animal suffered a lens injury, andan inflammatory exudate filled the eye (rabbit 7).Week 2. Half the irradiated eyes had healed scleral
wounds. The blood clot exhibited signs of lysis andshrinkage. Attenuated membranes were present intwo of the irradiated eyes, with the distal end of thestalk lying free in mid-vitreous. Two eyes had nomembrane formation, and all four eyes had flatretinae.Week 3. All four irradiated eyes had healed scleral
wounds. The retina overlying the site of perforationhad been replaced by flat scar tissue in one eye. Twohad vitreal membranes with no distal attachments,and one eye had a fibrous band which stretched fromthe wound to the opposite retina. In this eye tractionwas not evident and the retina remained flat.Week 4. Two of four irradiated eye had short
vitreoretinal membranes, one of which caused atraction retinal detachment. This eye (rabbit 16) hadsuffered a lens injury. Two others had flat chorio-retinal scars with pigmentary changes in the sur-
rounding peripheral retina.Week 6. One eye had a healed retinal wound
with extensive pigmentary changes in the inferiortemporal quadrant of the retina. Two eyes had
Table 6 Details ofpost-mortem appearance ofirradiatedeyes
Time of Serial Wound Vitreoretinal membranedeath number
Length Distal Tractioninmm attachments effects
1 Week 7* Gaping 2-5 CB, Lens LRD22 Gaping <2 None None4 Gaping <2 None None
42 Gaping 2-5 None None2 Weeks 45 Gaping 2-5 None None
18 Gaping 0 None None14 Healed 0 None None29 Gaping <2 None None
3 Weeks 27 Healed <2 None None17 Healed <2 None None9 Healed 0 None None40 Healed 2-5 PR None
4 Weeks 35 Healed 0 None None26 Healed 2-5 CB None16* Healed >10 MR, OR, CB TRD43 Healed 0 None None
6 Weeks 15 Healed <2 None None44 Healed 0 None None39 Healed >10 MR, Lens STRD36 Healed <2 None None
12 Weeks 31 Healed 0 None None46t Healed 5-10 CB, OR, Lens LRD37 Healed <2 None None34 Healed <2 None None
Ciliary body CB, localised retinal detachment LRD, medullary MR,opposite retina OR, peripheral retina PR, retinal folds RF, subtotalretinal detachment STRD, total retinal detachment TRD.*Animals 7 and 16 suffered a lens injury.tAnimal 47 suffered a double perforation.
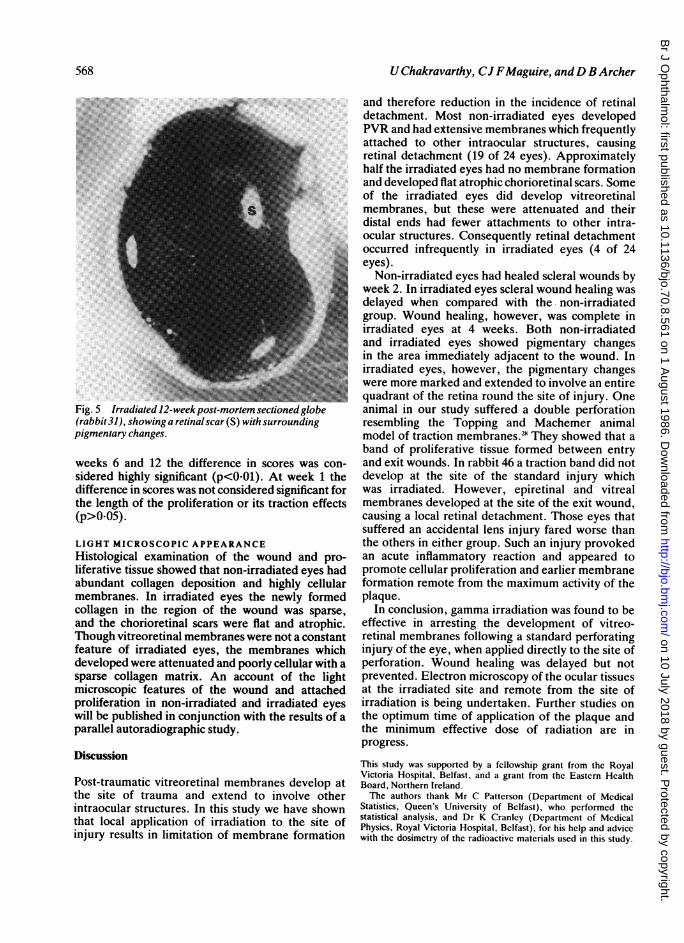
membranes exerting no traction; one had a prolifera-tion attached to the medullary rays, causing a localisedretinal elevation at that site (rabbit 39).Week 12. In all eyes scleral wound healing wascomplete and the blood clot had undergone furtherlysis and disintegration. Pigmentary disturbance waspresent in the injured quadrant in all specimens. Twoeyes showed retinal scarring and no membraneformation (Fig. 5) one had an attenuated membrane,while another which had suffered double perforatinginjury had a vitreoretinal membrane (rabbit 46). Themembrane extended from the exit wound which layin the inferior nasal quadrant to the medullary rays,where it caused a local retinal detachment.
Statistical analysis was performed on the post-mortem scores for each measurement at each timeinterval studied. There was no significant differencebetween the size of blood clot in non-irradiated andirradiated eyes at any of the time intervals studied.However, scores for the length of the proliferativemembrane and its traction effects showed significantdifferences between the two groups for all timeintervals between weeks 2 and 12 (p<0-05), and at
567
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from
U Chakravarthy, CJ FMaguire, andD BArcher
Fig. 5 Irradiated 12-week post-mortem sectioned globe(rabbit3l), showinga retinalscar(S) withsurroundingpigmentary changes.
weeks 6 and 12 the difference in scores was con-sidered highly significant (p<001). At week 1 thedifference in scores was not considered significant forthe length of the proliferation or its traction effects(p>O0O5).LIGHT MICROSCOPIC APPEARANCEHistological examination of the wound and pro-liferative tissue showed that non-irradiated eyes hadabundant collagen deposition and highly cellularmembranes. In irradiated eyes the newly formedcollagen in the region of the wound was sparse,and the chorioretinal scars were flat and atrophic.Though vitreoretinal membranes were not a constantfeature of irradiated eyes, the membranes whichdeveloped were attenuated and poorly cellular with asparse collagen matrix. An account of the lightmicroscopic features of the wound and attachedproliferation in non-irradiated and irradiated eyeswill be published in conjunction with the results of aparallel autoradiographic study.
Discussion
Post-traumatic vitreoretinal membranes develop atthe site of trauma and extend to involve otherintraocular structures. In this study we have shownthat local application of irradiation to the site ofinjury results in limitation of membrane formation
and therefore reduction in the incidence of retinaldetachment. Most non-irradiated eyes developedPVR and had eXtensive membranes which frequentlyattached to other intraocular structures, causingretinal detachment (19 of 24 eyes). Approximatelyhalf the irradiated eyes had no membrane formationand developed flat atrophic chorioretinal scars. Someof the irradiated eyes did develop vitreoretinalmembranes, but these were attenuated and theirdistal ends had fewer attachments to other intra-ocular structures. Consequently retinal detachmentoccurred infrequently in irradiated eyes (4 of 24eyes).
Non-irradiated eyes had healed scleral wounds byweek 2. In irradiated eyes scleral wound healing wasdelayed when compared with the non-irradiatedgroup. Wound healing, however, was complete inirradiated eyes at 4 weeks. Both non-irradiatedand irradiated eyes showed pigmentary changesin the area immediately adjacent to the wound. Inirradiated eyes, however, the pigmentary changeswere more marked and extended to involve an entirequadrant of the retina round the site of injury. Oneanimal in our study suffered a double perforationresembling the Topping and Machemer animalmodel of traction membranes.' They showed that aband of proliferative tissue formed between entryand exit wounds. In rabbit 46 a traction band did notdevelop at the site of the standard injury whichwas irradiated. However, epiretinal and vitrealmembranes developed at the site of the exit wound,causing a local retinal detachment. Those eyes thatsuffered an accidental lens injury fared worse thanthe others in either group. Such an injury provokedan acute inflammatory reaction and appeared topromote cellular proliferation and earlier membraneformation remote from the maximum activity of theplaque.
In conclusion, gamma irradiation was found to beeffective in arresting the development of vitreo-retinal membranes following a standard perforatinginjury of the eye, when applied directly to the site ofperforation. Wound healing was delayed but notprevented. Electron microscopy of the ocular tissuesat the irradiated site and remote from the site ofirradiation is being undertaken. Further studies onthe optimum time of application of the plaque andthe minimum effective dose of radiation are inprogress.
This study was supported by a fellowship grant from the RoyalVictoria Hospital, Belfast, and a grant from the Eastern HealthBoard, Northern Ireland.The authors thank Mr C Patterson (Departmcnt of Medical
Statistics, Queen's University of Belfast), who performed thestatistical analysis, and Dr K Cranley (Department of MedicalPhysics, Royal Victoria Hospital, Belfast), for his help and advicewith the dosimetry of the radioactive materials used in this study.
568
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from

Experimentalposteriorperforating ocular injury:
References
1 Eagling EM. Perforating injuries involving the posterior seg-ment. Trans Ophthalmol Soc UK 1975; 95: 335-9.
2 De Juan E Jr, Stemnberg P Jr, Michels RJ. Penetrating ocularinjuries. Types of injuries and visual results. Ophthalmology(Rochester) 1983; 90: 1318-22.
3 Machemer R. Pathogenesis and classification of massive peri-retinal proliferation. BrJ Ophthalmol 1978; 62: 737-47.
4 Faulborn J, Topping TM. Proliferations of the vitreous cavityafter perforating injuries. Graefes Arch Klin Exp Ophthalmol1978; 205: 157-66.
5 Retina Society Terminology Committee. The classificationof retinal detachment with proliferative vitreoretinopathy.Ophthalmology (Rochester) 1983; 90: 121-5.
6 Kampik A, Kenyon KR, Michels RG, Green RW, De La CruzZC. Epiretinal and vitreous membranes. A comparative study of56 cases. Arch Ophthalmol 1981; 99: 1445-54.
7 Winthrop SR, Cleary PE, Minkler DS, Ryan SJ. Penetrating eyeinjuries: a histopathological review. Br J Ophthalmol 1980; 64:809-17.
8 Newsome D, Rodriguez M, Machemer R. Human massiveperiretinal proliferation. In vitro characteristics of cellular com-ponents. Arch Ophthalmol 1981; 99: 873-80.
9 Hiscott PS, Grierson I, Hitchins GA, Cahi AHS, McLeod D.Epiretinal membranes in vitro. Trans Ophthalmol Soc UK 1983;103: 89-102.
10 Peczon BD, Wolfe JK, Gipson IK, Hirose T, Buzney SM,Schepens CL. Characterisation of membranes removedduring open sky vitrectomy. Invest Ophthalmol Vis Sci 1983; 24:1382-9.
11 Cleary PE, Minkler DS, Ryan SJ. Ultrastructure of tractionretinal detachment in rhesus monkey eyes after a posteriorpenetrating ocular injury. Am J Ophthalmol 1980; 90: 829-45.
12 Ussman J, Lazarides E, Ryan SJ. Traction retinal detachment. Acell mediated event. Arch Ophthalmol 1981; 99: 869-72.
13 Grierson I, Rahi AHS. Structural basis of contraction in vitrealfibrous membranes. BrJ Ophthalmol 1981; 65: 737-49.
14 Machemer R. A new concept for vitreous surgery. 2. Surgicaltechniques. Am J Ophthalmol 1972; 74: 1022-33.
15 Ryan SJ, Allen WA. Pars plana vitrectomy in ocular trauma. AmJ Ophthalmol 1979; 88: 483-91.
16 Stern WH, Fisher SK, Anderson DH, etal. Epiretinal membraneformation after vitrectomy. Am J Ophthalmol 1982; 93: 757-72.
17 Tano Y, Sugita G, Abrams G, Machemer R. Inhibition ofintraocular proliferations with intravitreal corticosteroids. Am JOphthalmol 1980; 89:131-6.
18 Blumenkranz MS, Hernandez E, Ophir A, Norton E. 5-Fluoro-uracil. New applications in complicated retinal detachment for
an established antimetabolite. Ophthalmology (Rochester) 1984;91: 122-30.
19 Stern WH, Guerin CJ, Ericson PA, Lewis GP, Anderson DH,Fisher SK. Ocular toxicity of fluorouracil after vitrectomy. Am JOphthalmol 1983; 96: 43-51.
20 Stern WH. Discussion in: Blumenkranz MS, etal. 5-Fluorouracil.New applications in complicated retinal detachment for anestablished antimetabolite Ophthalmology (Rochester) 1984; 91:129-30.
21 Moorehead LC. Effects of beta-amino proprionitrile after pos-terior penetrating injury in the rabbit. Am J Ophthalmol 1983;95: 97-109.
22 Weiss JF, Belkin M. The effect of penicillamine on post-traumatic vitreous proliferation. Am J Ophthalmol 1981; 92:625-7.
23 Thomas EL, Chong L. Prevention of trans-vitreal band andtraction retinal detachment formation by the use of haemato-porphyrin derivative and photoradiation therapy. Invest Oph-thalmol Vis Sci 1984; 25 (ARVO Suppl): 271.
24 Cox R, Masson WK. Radiosensitivity in cultured human fibro-blasts. Int J Radiat Biol 1980; 38: 575-6.
25 Arlett CF, Harcourt SA. Survey of radiosensitivity in a variety ofhuman cell strains. Cancer Res 1980; 40: 926-32.
26 Belkin M, Avni I, Kessler E, Hereberg A, Spierer A, Treister A.X-irradiation in the prevention of experimental post-traumaticvitreous proliferation. Curr Eye Res 1982/3; 2: 753-6.
27 Cleary PE, Ryan SJ. Experimental posterior penetrating eyeinjury in the rabbit. 2. Histology of wound, vitreous and retina.Br J Ophthalmol 1979; 63: 312-21.
28 Topping TM, Abrams GW, Machemer R. Experimental doubleperforating injury of the posterior segment in the rabbit eye. Thenatural history in intraocular proliferation. Arch Ophthalmol1979; 97:735-42.
29 Stallard HB. The conservative treatment of retinoblastoma.Trans Ophthalmol Soc UK 1962; 82: 473-534.
30 Innes G. In: Bonuik M, ed. Ocular and adnexal tumors. St.Louis: Mosby, 1964: 142.
31 Casebow MP. The calculation and measurement of exposuredistributions from ophthalmic 64cobalt applicators. Br J Radiol1971;44: 618-24.
32 Cruess AF, Augsburger JJ, Shields JA, Donoso LA, Amsel J.Visual results following cobalt plaque radiotherapy for posterioruveal melanomas. Ophthalmology (Rochester) 1984; 91: 131-6.
33 Bedford MA, Bedotto C, Macfaul PA. Retinoblastoma. A studyof 139 cases. BrJ Ophthalmol 1971; 55: 19-27.
34 Cleary PE, Ryan SJ. Posterior perforating eye injury: experi-mental animal model. Trans Ophthalmol Soc UK 1978; 98: 34-7.
Acceptedforpublication 5 November 1985.
569
on 10 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.70.8.561 on 1 August 1986. D
ownloaded from