experimental nephrotoxicity, hepatotoxicity and pharmacokinetics of cyclosporin g versus cyclosporin...
TRANSCRIPT
Kidney International, Vol. 45 (1994), pp. 684—691
Experimental nephrotoxicity, hepatotoxicity andpharmacokinetics of cyclosporin G versus cyclosporin A
EMMANUEL A. BURDMANN, TAKESHI F. ANDOH, SEYMOUR ROSEN, JESSIE LINDSLEY,MYRNA Y. MUNAR, LAWRENCE W. ELZINGA, and WILLIAM M. BENNETT
Division of Nephrology, Hypertension and Clinical Pharmacology, Oregon Health Sciences University, Portland, Oregon and Department ofPathology, Harvard Medical School and Beth Israel Hospital, Boston, Massachusetts, USA
Experimental nephrotoxicity, hepatotoxicity and pharmacokinetics ofcyclosporin G versus cyclosporin A. Cyclosporin G (CsG) is an analogueof cyclosporin A (CsA) with strong immunosuppressive activity. Wecompared these two drugs in a rat model in which salt depletionpromotes irreversible renal interstitial fibrosis with renal dysfunction inanimals given CsA for three weeks. When both drugs were given in thesame dosage on a weight basis (15 mg/kg/day, subcutaneously), CsAblood levels were higher than CsG (3305 vs. 1824 ng/ml, P < 0.001).This could be explained by a higher CsG clearance (6.4 vs. 4.3mi/mm/kg in CsA, P < 0.0001) resulting in smaller CsG area under thecurve. There was also lower renal and hepatic CsG tissue concentra.tions. CsA induced a dramatic decrease in GFR, 0.14 in CsA versus0.67 ml/min/100 g in control, P < 0.001, and increased urinary excretionof N-acetyl /3-D-glucosaminidase (NAG), 21 in CsA versus 13 IU/gCr incontrol rats, P < 0.001. CsG-treated and control rats had similar GFRand urinary NAG. When CsA dosage was decreased to 7.5 mg/kg bloodlevels were similar to those found with CsG 15 mg/kg. CsA at this dosecaused a reduced GFR (0.29 ml/min/l00 g) and an increased urinaryNAG (20 IU/gCr) (P < 0.01 vs. control for both). Both dosages of CsAinduced considerable cortical and medullary injury (interstitial fibrosisand tubular atrophy), more severe than the histological damage found inCsG-treated rats. Neither drug promoted significant changes in liverfunction or histology. These results demonstrate that CsG caused lessrenal interstitial fibrosis and functional changes than CsA when thedrugs were given at the same dosage or when similar blood levels ofeach drug were achieved.
Cyclosporin A (CsA) has more than 700 analogues, but fewhave significant immunosuppressive activity [1]. Cyclosporin G(CsG) or Nva-2 cyclosporine is a natural analogue of cyclospo-rifle with strong immunosuppressive activity in which L-norva-line has replaced aipha-aminobutyric acid in position 2. In vitroand in vivo immunological studies have shown similar immuno-suppressive efficacy between CsA and CsG [2—5]. In renal andheart transplantation in rats CsG has been shown to be aseffective as CsA at doses of 10 mg/kg/day or more [6—8].Preliminary results of clinical trials comparing CsA and CsGimmunosuppressive efficacy in solid-organ transplantation dem-onstrated similar outcomes of patient and graft survival [9—11].The nephrotoxicity of CsA and CsG has been compared with
Received for publication August 5, 1993and in revised form October 12, 1993Accepted for publication October 14, 1993
© 1994 by the International Society of Nephrology
conflicting results [2, 3, 8—20]. Hepatotoxicity has been re-ported in experimental animals [3, 15, 18, 20] or patients givenCsG [9—11, 191.
In this study we compared the toxicity and pharmacokineticsof CsA and CsG in an experimental model of chronic cyclo-sporine-induced nephropathy. In this model, rats given CsA ona salt-depleted diet develop severe decreases in glomerularfiltration rate as well as irreversible striped tubulointerstitialinjury similar to the histological lesion found in human chronicCsA-induced nephrotoxicity [21, 22].
Methods
Animals
Adult male Sprague-Dawley rats (Charles River, Wilmington,Massachusetts, USA) weighing 250 g were housed in individualcages in a temperature- and light-controlled environment. Theyreceived a salt-free boiled rice diet (8.5% of protein, 76.6% ofcarbohydrate, less than 4.3% of fat, enriched with ferric or-thophosphate and thiamine mononitrate) and were allowed freeaccess to tap water.
DrugsCsA and CsG (Sandoz Research Institute, East Hanover,
New Jersey, USA) were dissolved in anhydrous ethanol(12.5%) and mixed with olive oil (87.5%) to a final concentrationof 7.5 mg/mi and 15 mg/mi of CsA, and 15 mg/ml and 25 mg/mIof CsG.
Basic protocol
The rats received one intraperitoneal injection of furosemide(4 mg/kg) and started the rice diet. After one week weight-matched pairs of rats were randomly assigned to receive a dailysubcutaneous injection of CsA 15 mg/kg (CsA15, N = 20), CsG15 mg/kg (CsG15, N = 21) or an identical volume of vehicle(VH, N = 27). In order to obtain similar blood levels of CsA andCsG, an additional group of rats were randomized to receiveCsA 7.5 mg/kg (CsA7.5, N = 15) or CsG 25 mg/kg (CsG25, N =13). Body weight was measured daily throughout the experi-ment. After three weeks of treatment on rice diet the rats hadthe tail blood pressure (BP) measured with a plethysmograph(Narco Bio-systems, Houston, Texas, USA) and were placed inmetabolic cages (Nalge Company, Rochester, New York, USA)
684

Burdmann et a!: Pharmacokinetics of CsG vs. CsA 685
for urine collection. After 24 hours, a blood sample was drawnand, as previously designated for each rat, the glomerularfiltration rate (GFR) was measured by '4C-inulin clearance orthe left kidney was collected for histology after in situ perfu-sion.
Inulin clearanceAfter anesthesia polyethylene tubes (PE-50) were placed in
the jugular vein for blood collection and in the femoral vein forinfusion. A polyethylene tube (PE-90) was also placed andsutured in the bladder. A loading dose of 0.25 Ci '4C-inulin in6 ml 1% NaHCO3 was given followed by a maintenance infusionof 2.5 Ci 14C-inulin in 10 ml 1% NaHCO3 at a rate of 52 1.dlmin.After a 30-minute equilibration time, urine was collected overfour periods of at least 20 minutes each in preweighed vials. Ablood sample (0.35 ml) was drawn at the midpoint of each urinecollection and replaced with an equal volume of 1% NaHCO3.Inulin clearances values expressed as ml/min/l00 g body wtrepresent the mean of the four clearance periods. After the endof the inulin clearance the rat was euthanized, the left kidneywas removed and weighed.
In situ perfusionAfter anesthesia the rat received 500 U of heparin i.v. and a
ventral midline incision was made exposing the abdominalaorta, posterior vena cava, left and right renal vessels. Theaorta and vena cava just above the bifurcation to the legs plusthe mesenteric and right kidney arteries were tied. A ligaturewas loosely tied around the aorta and vena cava above the renalarteries. An 18-gauge needle was introduced in the abdominalaorta pointing towards the kidneys. An infusion of 10 ml ofsaline was started at the same time as the ligature above therenal arteries was tied and a hole was made in the left renalvein. After the saline flush, six minutes of perfusion with 1%glutaraldehyde in a modified 3/4 Tyrode buffer was done. Thepressure in the system was kept stable at 140 to 160 mm Hg andthe flow at 10 to 12 mI/mm. After the perfusion the left kidneywas removed, weighed and placed in a vial with the perfusionsolution.
Renal histologyThe renal tissue was processed, embedded in plastic and cut
at I p. as in previous studies [21, 22]. The extent of tubuloin-terstitial injury (fibrosis and tubular atrophy) was evaluatedsemi-quantitatively (0 to 4+) in a blinded way (Dr. S. Rosen).Approximately six sections (3 x 3 mm) were analyzed peranimal. These sections included both horizontal and the tradi-tional sagittal sections. Interstitial fibrosis and tubular atrophyin the cortex was first seen predominantly in the medullary ray.These first recognizable changes were graded as trace. As theinjury involved the medullary ray more extensively, thechanges were considered 1+. When the medullary ray changeswere widespread, a 2+ grade was given. With increasingdegrees of fibrosis, the labyrinth was involved and dependingon the extent, the grades were 3 or 4+. In the medulla, the firstchanges related to tubular atrophy were often associated withcasts. Initially, these alterations were unaccompanied by fi-brotic change. Occasional atrophic tubules were graded trace.As the changes became more extensive, a grade 1+ was given.When the process became somewhat diffuse, a 2+ score was
given. At this time, a fibrotic component began to be seen.Higher scores depended on further increases in atrophic changeand the degree of accompanying fibrosis.
Liver histology
Liver specimens were fixed in 10% neutral buffered formalinand processed and embedded in paraffin using standard tech-niques. Histologic sections, 5 p. in thickness, were cut from theparaffin block and stained with hematoxylin and eosin, Mal-lory's trichrome, and periodic acid-Schiff's stain followingdiastase digestion. The sections were examined and morpho-logic features assessed without knowledge of the experimentalmanipulation (Dr. Randall G. Lee).
Pharmacokinetic study
CsA and CsG solutions were prepared diluting the drug withethanol (12.5%) and intralipid (87.5%) (KabiVitrum, Clayton,North Carolina, USA) to a final concentration of 15 mglml. Ratsweighing 300 g were kept for seven days on rice diet and in theeighth day polyethylene tubes (PE-50) were placed in bothjugular veins and CsA (N = 6) or CsG (N = 7)15 mg/kg wasgiven by the left jugular vein over an average time of oneminute. Blood samples were drawn from the right jugular veinat 2, 5, 15, 30, 60, 120, 180, 360 and 1440 minutes after the
infusion of the drug. Animals were kept under light anesthesiathroughout the procedure. CsA and CsG concentration versustime data were analyzed using noncompartmental analysis. Theelimination rate constant (kel) was determined as the terminalslope of the linear least-squares regression line of a semiloga-rithmic plot of concentration versus time data. Area under theconcentration versus time curve (AUC) was calculated by thelinear trapezoidal rule and extrapolated to infinity (AUC0OO).The terminal area was determined by dividing the last measuredconcentration by the terminal slope (kel). Noncompartmentalanalysis was used to calculate total body clearance (CL) andapparent volume of distribution (Varea)according to the follow-ing equations:
CL = Dose/AUC0
Varea = CL/kel
Half-life (t112) was calculated by the equation t112 = 0.693/kel.
Tissue concentrations of cyclosporine
Rats kept on rice diet were given CsA (N = 5) or CsG (N =4) s.c. as already described. After three weeks of treatment theanimals were euthanized and kidney and liver samples werecollected. The tissue was weighed and homogenized with 3 mlof methanol (50°C) in a glass jar with Teflon. Tissue homoge-nized was centrifuged at 3000 x g during 10 minutes (roomtemperature) and the supernatant was saved. Then, 3 ml ofmethanol was added again to the tissue and the procedurerepeated. The total obtained supematant was dried undernitrogen and saved at —20°C to further analysis. Kidney andliver samples from a rat given only the vehicle were used ascontrol.

686 Burdmann et al: Pharmacokinetics of CsG vs. GsA
Table 1. Daily variation of body weight, kidney weight, urinaryvolume and blood pressure after a three week treatment with vehicle,
CsA or CsG on rice diet
Body wtglday
Kidneywt/lOO g
UVml/24 hr
BPmm Hg
VH 1.49 0.18(27)
0.42 0.01(24)
27.7 2.3(27)
116.9 3.7(22)
CsA 15 mg 0.86 0.14(20)
0.41 0.01(20)
22.5 2.5(20)
116.6 3.8(15)
CsG 15mg 1.33 0.13(21)
0.43 0.01(21)
20.9 1.6(20)
118.9 3.4(16)
Data are presented as mean sEM; Number of rats are in parenthe-ses. Abbreviations are: iBody wt, variation in body weight; Kidney wt,kidney weight; UV, urinary volume; BP, blood pressure; VH, vehicle.
a P < 0.05 vs. VH
Analytical methodsUrinary and serum sodium and potassium were measured by
flame photometer (Instrumentation Laboratories, Lexington,Massachusetts, USA). Urinary and serum creatinine, urinaryand serum magnesium, serum aspartate aminotransferase(AST), serum alanine aminotransferase (ALT), serum totalbilirubin (TB) and urinary N-acetyl /3-D-glucosaminidase(NAG) were measured by a Cobas autoanalyzer (Roche Diag-nostics, Hoffman-La Roche Division, Nutley, New Jersey,USA). Urinary enzymes results were normalized by the urinarycreatinine concentration. Cyclosporine whole-blood levels andtissue levels were determined by a specific CsA monoclonalradioimmunoassay (Incstar Corp., Stillwater, Minnesota,USA). CsA antibody has been shown to have equal affinity forCsA and CsG and monoclonal radioimmunoassay have givenresults comparable to HPLC [1, 23]. Serum and urine radioac-tivity were measured by a Beckman LS 100 liquid scintillationcounter (Beckman Instruments, Palo Alto, California, USA).The clearance of inulin (GFR), clearance of creatinine (Car),fractional excretion of sodium (FENa), fractional excretion ofpotassium (FEK) and fractional excretion of magnesium (FEM5)were calculated by the standard formulas.
Statistical analysisResults are presented as mean SEM. Comparisons between
CsA and CsG in the pharmacokinetic and cyclosporine tissueconcentration analysis were done by two-tailed unpaired Stu-dent's f-test or Mann-Whitney test, as appropriate. Multiplecomparisons were done by ANOVA followed by Tukey-Kramer test or by Kruskal-Wallis test followed by Dunn's test,as appropriate. The level of statistical significance was chosenas P < 0.05.
Results
Rats given CsA gained less body weight than those receivingonly vehicle (P < 0.05), while the daily variation in body weightwas similar between CsG and vehicle animals. There were nodifferences in kidney weight, blood pressure or urinary volumeamong the three groups (Table 1).
Twenty-four-hour trough cyclosporine blood levelsWhen CsA and CsG were given in the same dosage on a
weight basis the CsA blood level was almost two times higher
Fig. 1. Comparison between cyclosporine blood levels (CSBL) andglomerular filtration rate decrease after three week treatment with CsA15 and 7.5 mg/kg or CsG 15 and 25 mg/kg. *p < 0.05 vs. CsA 15 mg/kg.
than the CsG blood level (P < 0.001, CsA1S vs. CsG15). Theincrease of CsG daily dosage to 25 mg/kg resulted in cyclospo-rifle blood level similar to that found with CsG 15 and thereforestill lower than CsA1S (P < 0.001). We only achieved compa-rable blood level between CsA and CsG when the CsA dailydosage was decreased to 7.5 mg/kg, which resulted in a cyclo-sporine blood level similar to that found for CsG 15 and signif-icantly lower than the CsA1S value (P < 0.001; Fig. 1).
Renal functionRats given CsA had a lower GFR (P < 0.01, CsA7.5 vs. VH
and P < 0.001, CsA15 vs. VH), lower Cr (P < 0.001, CsA7.5vs. VH and CsA15 vs. VH) and higher serum creatinine (P <0.05, CsA7.5 vs. VH and P < 0.001, CsAl5 vs. VH) ascompared to control animals. There were no significant differ-ences in renal function between CsG and control rats. How-ever, when CsA and CsG rats were compared CsA-treatedanimals showed a lower GFR (P < 0.05, CsAl5 vs. CsG15 andP < 0.01, CsA15 vs. CsG2S), lower Cci (P < 0.05, CsA7.5 VS.CsGL5 and CsA15 vs. CsG2S and P < 0.01, CsA1S vs. CsGl5)and higher serum creatinine (P < 0.001, CsAl5 vs. CsG15) thanCsG rats (Table 2).
The urinary excretion of N-acetyl f3-D-glucosaminidase wassignificantly higher in CsA animals as compared to vehicle (P <0.01, CsA7.5 vs. VH and P < 0.001, CsA1S vs. VH) or CsG rats(P < 0.05, CsA7.5 vs. CsG15 and P < 0.01, CsA15 vs. CsGL5;Table 2).
Serum sodium and FENa were similar among groups. TheFENa was virtually zero reflecting the severe dietary sodiumrestriction. Although serum potassium was higher in CsG group(P < 0.05 vs. VH), FEK was elevated in CsA-treated rats (P <0.05 vs. VH). Both CsA and CsG rats showed decreased serummagnesium as compared to control animals (P < 0.001, CsA15vs. VH and P < 0.05, CsG15 vs. VH) and FEMg higher than thatfound for vehicle-treated animals. Nevertheless, the differencesin FEMg were not statistically significant (Table 3).
Renal histology
The most striking histological changes in cyclosporine-treated animals were interstitial fibrosis and tubular atrophy.The injury was most pronounced in the medullary ray, givingthe characteristic striped appearance and in the inner stripe of
350030002500
C 200015001000500
aa
-40< E -60
-80GsA 15 mg
HCsA 7.5 mg
CsG 15mgCsG 25mg

Burdmann et a!: Pharmacokinetics of CsG vs. GsA 687
Table 2. Glomerular function, renal histology score and NAG enzymuria after a three-week treatment with vehicle, CsA or CsG on rice diet
GFR Ce,. sCrrng/dl
CIFS MIFSNAG/UrlUig Crin/100 gmi/rn 0 to 4+
VH 0.67 0.06(11)
0.431 0.021(27)
0.55 0.02(27)
0.08 0.04(13)
0.02 0.02(12)
13.0 1.0(27)
CsA 7.5 mg 0.29 O.06a
(7)0.264 O.021a
(14)0.72 O.05a
(15)1.68 0.21
(7)1.71 O.15
(7)20.4 i.r
(14)CsA 15 mg 0.14 0.04a 0.256 0.017a 0.87 0.05a 1.08 0.l5a 1.15 0.27a 20.9 l.6CsG 15 mg
CsG 25 mg
(10)0.43 009b
(9)0.53 009b
(8)
(19)0.370 0023b.c
(19)0.354 0021b
(Il)
(19)0.65 0.07k'
(20)0.66 0.05
(11)
(6)0.40 0.06
(11)0.20 0.05"
(5)
(5)0.36 0b.c
(11)0.50 0.34c
(4)
(20)14.1 l.4
(21)18.1 1.6
(13)
Data are presented as: mean sEas; number of rats are in parentheses. Abbreviations are: GFR, glomerular filtration rate; CCr, clearance ofcreatinine; Scr, serum creatinine; CIFS, cortical interstitial fibrosis score; MIFS, medullar interstitial fibrosis score; Ucr, urinary creatinine; VH,vehicle.
ap<005vs VHb P < 0.05 vs. CsA 15 mg
P < 0.05 vs. CsA 7.5 mg
Table 3. Serum electrolytes and fractional excretion of sodium, potassium and magnesium after a three-week treatment with vehicle, CsA, orCsG on rice diet
SN8
mEq/literFENa
%SK
mEq/literFEK
%SMg
rng/diFEEs
%
VH 145 2(24)
0.0001 0.0001(24)
5.3 0.2(24)
7.7 0.6(24)
2.9 0.1(20)
1.0 0.2(11)
CsA 15 mg 141 2(16)
0.0015 0.0010(16)
5.7 0.2(16)
11.0 1.2k(16)
2.3 0.1(16)
2.2 0.5(14)
CsG 15 mg 141 2(17)
0.0016 0.0011(17)
6.0 0.2a(17)
8.0 1.0(17)
2.5 0.28(12)
1.7 0.4(8)
Data are mean SEM; Number of rats are in parentheses. Abbreviations are: SNa, serum sodium; FENa, fractional excretion of sodium; SK,serum potassium; FEK, fractional excretion of potassium; SMg, serum magnesium; FEMS, fractional excretion of magnesium; VH, vehicle.
ap <o5 vs. VH
the outer medulla. Glomerular sclerosis and vascular injurywere not observed. Juxtaglomerular apparatus hyperplasiaseemed present in all animals, probably due the low salt diet,and was not more strikingly evident in cyclosporine-treatedanimals.
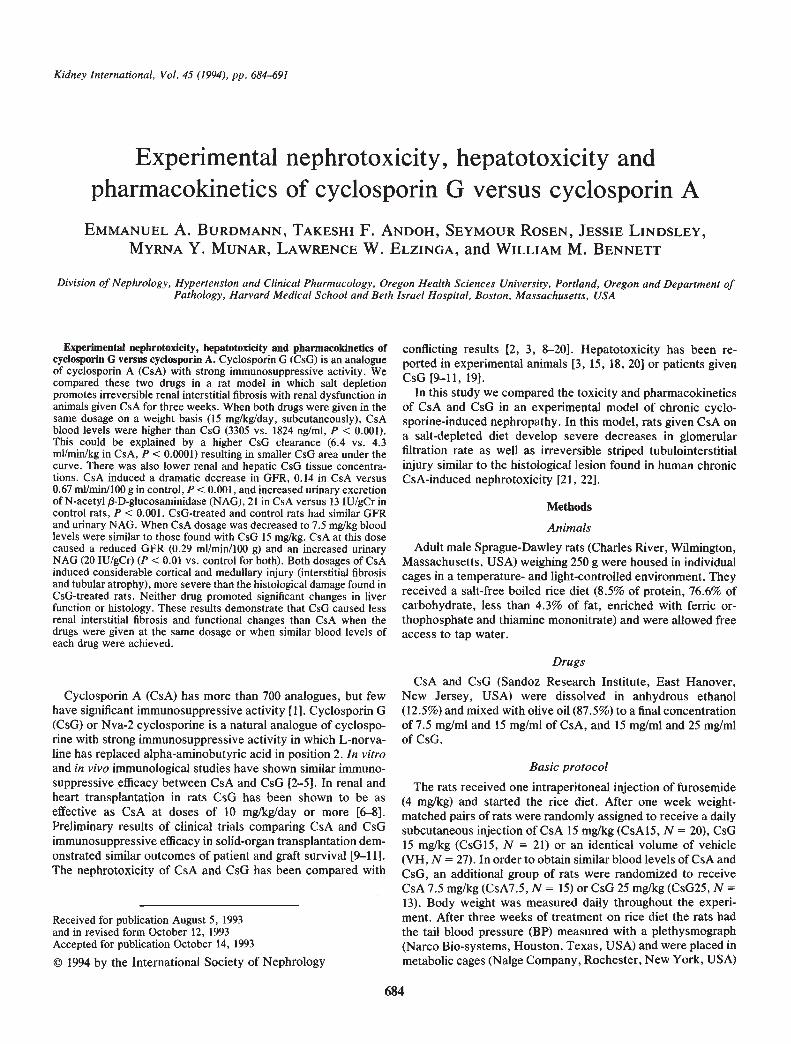
CsA-treated rats had a higher cortical injury score than vehicle(P < 0.001, CsA7.5 vs. VH and CsA15 vs. VH) or CsG-treatedrats (P < 0.001, CsA7.5 vs. CsG15, CsA15 vs. CsGl5, CsA7.5 vs.CsG25 and CsA15 vs. CsG2S). CsA animals also showed a highermedullary injury score than vehicle (P < 0.001, CsA7.5 vs. VHand CsA15 vs. VH) or CsG animals (P < 0.001, CsA7.5 vs.CsG15;P <0.01, CsA15 vs. CsG15; andP <0.001, CsA7.5 vs.CsG25). Although the interstitial fibrosis score of CsG-treatedrats was higher than that found in control animals the differencedid not achieve statistical significance (Table 2, Fig. 2).
Liver function and histologyThe values of AST and ALT of either CsA or CsG animals
were not increased as compared to animals receiving vehicle.Both CsA and CsG rats presented increased TB as compared tocontrol animals. Nevertheless, this difference was not statisti-cally significant (Table 4).
Liver histology was consistently normal or showed mild fattychanges, without differences between cyclosporine- or vehicle-treated animals (Table 4).
Pharmacokineric study
CsG had a higher clearance than CsA resulting in lowertrough blood levels. There was also smaller area under thecurve, higher volume of distribution and lower renal andhepatic levels of CsG. While CsA treated rats had similar renaland hepatic tissue cyclosporine levels, CsG-treated animals hadcyclosporine liver tissue levels two times higher as compared tothe renal tissue levels (Table 5, Fig. 3).
Discussion
The price for the widespread and prolonged use of CsA, evenwith therapeutic drug monitoring, is its chronic nephrotoxicity.The therapeutic window, if one truly exists, is narrow and somedegree of renal dysfunction is the general rule when glomerularfiltration rate is the renal parameter measured [24]. Severalapproaches have been tried to bypass these problems, includinga search for safer yet effective cyclosporine analogues. In 1985,Hienstand and colleagues reported that cyclosporin G (CsG) orNva-2 cyclosporine had similar immunosuppression activity butless nephrotoxicity than CsA in rats [2]. The enthusiasm aboutCsG was tempered by the conflicting results following the initialreport. Comparison among the different studies is difficult sinceanimal species, strain, dosage, route of administration andduration of treatment were not uniform. Most authors have
688 Burdmann et al: Pharmacokinetics of CsG vs. CsA
Fig. 2. Rena! cortex of rats given CsG(A) or CsA (B), 15 mg/kg during 3weeks. In rats treated with CsG onlyslight interstitial fibrosis and tubularatrophy are seen related to a medullaryray (center). When CsA is given, theinterstitial fibrosis and tubular atrophyare much more extensive. x75, x75.
used only serum creatinine or creatinine clearance to measurerenal function. Trough cyclosporine blood levels of CsA andCsG have not always been measured and when they weredifferent no attempt was made to obtain comparable bloodconcentrations. Finally, it is not known if CsG induces chronictubulointerstitial damage to the same extent as CsA. In this studywe took advantage of an experimental model of cyclosporine-induced chronic nephrotoxicity in salt-depleted rats to compareCsA and CsG using both similar doses on a weight basis andsimilar trough blood levels of the two drugs.
While CsA produced a major decrease in GFR and creatinineclearance and increased serum creatinine, CsG-treated rats hadrenal function similar to control animals. These results areconsistent with previous studies which also found increasedserum creatinine in CsA but not CsG-treated rats after three ormore weeks of treatment [12, 15, 16]. Duncan et a!, using
Sprague-Dawley rats, found a slight but significant increase inserum creatinine and decrease in Ce,, with both CsG and CsA.However, these changes were more marked in CsA rats andCsG-treated rats had Ccr significantly higher than CsA animals[3]. Only two other studies have measured GFR by inulinclearance to assess renal function in comparative studies. Onefound decreased GFR and renal plasma flow (RPF) in CsA butnot CsG rats after three weeks of cyclosponne treatment and inthe other the acute intravenous infusion of either CsA or CsG inrats promoted similar falls in GFR and RPF [13, 14]. An elegantstudy by Rooth et a! demonstrated that CsA infusion in miceinduced an almost complete inhibition of subcapsular bloodflow. CsG only decreased blood flow at high infusion rates, butthe inhibition was still significantly below that produced by CsA[25]. in vitro studies showed that CsG was less toxic than CsAto LLC-PK cells [26]. Preliminary results of clinical trials in

Burdmann et a!: Pharmacokinetics of CsG vs. GsA 689
Table 4. Liver enzymes and total bilirubin after a three-weektreatment with vehicle, CsA or CsG on rice diet
AST ALT TBmg/dllU/liter
VH 158 13
(7)42 5
(7)0.67 0.07
(7)CsAl5mg 11O±9
(7)27±2
(7)0.97±0.11
(6)CsGl5mg 1l3±9a
(6)28±2
(6)0.96±0.09
(5)
Data are mean SEM; Number of rats are in parentheses. Abbrevi-ations are: AST, aspartate aminotransferase; ALT, alanine aminotrans-ferase; TB, total bilirubin.
a p < 0.05 vs. VH
renal transplantation have also suggested less nephrotoxicityfor CsG than CsA as measured by serum creatinine and inulinclearance [9—111.
Probably more important than the preservation of GFR wasthe finding of considerably less cortical and medullary histolog-ical injury in CsG rats as compared to CsA. Other experimentalstudies in rats and rabbits also found less interstitial fibrosiswith CsG [1, 8]. There are no clinical data available yet forcomparison. Progressive renal failure and chronic striped inter-stitial fibrosis have been described in solid organ transplanta-tion and in patients with autoimmune diseases receiving CsA[27—29]. The renal dysfunction occurs even with low cyclospo-rine dosage and may be progressive despite drug dose reduction[30—32]. The experimental model used in the present studyreproduces the pattern of striped interstitial fibrosis describedin patients receiving CsA. Elzinga, Rosen and Bennett showedin this model that the tubulointerstitial injury progressed despitewithdrawal of CsA [22]. If our experimental findings are con-firmed by the ongoing clinical trials, CsG may become animportant alternative for long-term transplant and non-transplant immunosuppression.
CsA induced significant NAG enzymuria and a high FEK inpresence of very low FENa and levels of serum potassiumsimilar to that found im placebo rats, suggesting a distal tubulelesion [33, 34]. In contrast CsG-treated rats had urinary excre-tion of NAG and FEK similar to control animals. Both cyclo-sponnes induced hypomagnesemia and an inappropriately highfractional excretion of magnesium, supporting the concept thatthe decrease in serum magnesium is not related with thechanges in GFR [35].
Since CsG has shown immunosuppressive activity equivalentto CsA at dosages lower than those used in this study, theoccurrence of less nephrotoxicity with CsG suggests that themechanisms of cyclosporine toxicity and immunosuppressionmay be independent. However, we did not do a direct compar-ison between CsA and CsG immunosuppressive efficacy, and itremains possible that decreased renal toxicity and decreasedimmunosuppressive activities co-exist at these doses. Presentlyit is not clear why CsG is less nephrotoxic. One possibleexplanation might be related to differences in drug metabolism,but CsG metabolites have structures consistent with thoseidentified for CsA [36]. Both drugs bound to cyclophilin equally[37]. Although the pharmacokinetics of the two drugs wasclearly different, CsG was still less nephrotoxic when equiva-
Table 5. Pharmacokinetics of CsA and CsG after an intravenousinjection of cyclosporine 15 mg/kg, and tissue levels of CsA and CsG
after 3 weeks of cyclosporine treatment (15 mg/kg) on rice diet
CsA (6) CsG (7) PCs blood level after 24 hr 984 62 552 45 0.0002
ng/mlArea under the curve 58.3 3.4 39.5 1.7 0.002
mg x hr/literCs clearance ml/min/kg 4.3 0.3 6.4 0.3 0.0001t½ hr 11.1 1.0 11.0 0.5 0.98Vd liter/kg 4.0 0.1 6.2 0.3 0.0001Cs kidney level after 3 weeks 33.7 l.6a 8.6 0.8a 0.0001
ng/mgCs liver level after 3 weeks 39.8 42b 17.3 2.5a 0.0035
ng/mg
Data are: mean 5EM; Number of rats are in parentheses. Abbrevi-ations are: Cs, cyclosporine; t½, half-life; Vd, volume of distribution.N 4
bN.... 5
900080007000
60005000
4000
3000
2000
1000
0Q 5 15 30 60 120 180 360
Time, minutes
1440
Fig. 3. Cyclosporine blood levels (CSBL) after an intravenous injec-tion of CsA (0) or CsG (. 15 mg/kg (results are mean SEM). *P <0.01, CsA vs. CsG.
lent blood levels of the two drugs were achieved by loweringCsA dosage or when the CsG dose was increased to three timesthe CsA dosage. However, while CsA induced similar renal andhepatic contents of cyclosponne, the renal amount of CsG washalf of the liver CsG content. Rayat et al found that more CsGthan CsA was required to displace 3H-CsA from human periph-eral blood mononuclear cells [38]. Thus, it is possible that CsGand CsA have different cellular uptakes that would explain inpart the distinct toxicological pattern of the two drugs. There isa single study showing that CsA but not CsG reduced PGE2production in cultured rat mesangial cells [39].
Hepatotoxicity disclosed by increased serum bilirubin andelevation in liver enzymes has been reported in experimentalanimals receiving CsA or CsG [3, 13, 18, 28]. Results fromclinical trials are controversial. Huser et al reported increasedbilirubin, increased liver enzymes and abnormal liver histologyin three CsG-treated patients that improved after discontinua-tion of the drug [19]. However, in larger series of CsG-treatedpatients only slight elevations in liver enzymes were observed[9—11]. Both drugs were toxic in vitro to human hepatoblastoma
* * * *
*

690 Burdmann et at: Pharmacokinetics of CsG vs. GsA
cells [40]. In the present study there was a clear trend toincreased serum bilirubin with either CsA or CsG, but liverenzymes and liver histology were normal. It is not clear why theliver enzymes in CsA and CsG-treated animals were below thevalues found for control rats.
Conflicting results have also been reported comparing thepharmacokinetics of CsG and CsA. The variations are likelyrelated to differences in animal species and strain. In rats,similar [3, 8, 16], lower [12, 41], and higher [7, 15] trough CsGblood levels as compared to CsA were observed. Pharmacoki-netic studies in rabbits were consistent with the results found inour study, showing faster elimination and lower blood levels forCsG [1, 42]. In this study, even increasing the dose of CsG from15 to 25 mg/kg we did not observe an increased blood level ofthe drug. In dogs CsG blood levels are higher and CsGclearance lower as compared to CsA [43]. In humans, the firstpublished study suggested similar pharmacokinetics for CsAand CsG [44], but subsequent studies showed that at equivalentdoses cyclosporine blood levels were higher with CsG [9—11,19].
In summary, CsG induced less tubulointerstitial injury andless glomerular and tubular dysfunction than CsA when the twodrugs were given in equivalent dosages by weight or whensimilar trough blood levels of both drugs were achieved. Thesefindings are only partially explained due to differences inpharmacokinetics and suggest innate differences in tissue up-take and nephrotoxic potential of the two drugs. Other media-tors of cyclosporine nephrotoxicity must be studied in experi-mental animals as well as in humans given CsG in order toclarify the mechanisms and implications of these results.
Acknowledgments
Dr. Emmanuel A. Burdmann is a recipient of a grant from "Fundacaode Amparo a Pesquisa do Estado de São Paulo" (FAPESP, São PauloState Research Supporting Foundation), Brazil. CsA and CsG weregifts from Sandoz Research Institute, East Hanover, New Jersey, USA.This paper was presented in part at the 25th annual meeting of theAmerican Society of Nephrology, Baltimore, Maryland, 1992 and at theXIIth International Congress of Nephrology, Jerusalem, Israel, 1993and published in abstract form in the JAm Soc Nephrol 3:841, 1992.
The authors thank Joann Duyn for technical assistance and GayleCox for word processing support. The authors are also grateful toRandall 0. Lee, M.D., Department of Pathology, Oregon HealthSciences University for the liver histology interpretation.
Reprint requests to Emmanuel A. Burdmann, M.D., Division ofNephrology, PP262, Oregon Health Sciences University, 3314 SW USVeterans Road, Portland, Oregon 97201, USA.
References
1. JEFFERY JR: Cyclosporine analogues. Clin Biochem 24:15—21, 19912. HIESTAND PC, GUNN HC, GALE JM, RYFFEL B, BOREL iF:
Comparison of the pharmacological profiles of cyclosporine,(Nva2)-cyclosporine and (Val2)dihydro-cyclosporine. Immunology55:249—255, 1985
3. DUNCAN JI, THOMSON AW, SIMPSON JG, DAVIDSON RJL, WHIT-ING PH: A comparative toxicological study of cyclosporine andNva2-cyclosporine in Sprague-Dawley rats. Transplantation 42:395—399, 1986
4. MCKENNA RM, SzTuRM K, JEFFERY JR, RUSH DN: Inhibition ofcytokine production by cyclosporine A and 0. Transplantation47:343—348, 1989
5. MASRI MA: Comparative Study of skin graft survival rates inBALB/c mice treated with either cyclosporine A, cyclosporine 0,or 1/1 combination of both. Transplant Proc 24:1661—1662, 1992
6. PROP J, HOYT EG, JAMIESON SW: (Nva2)-cyclosporine-less potentthan cyclosporine A in rats with lung and heart transplants.Transplantation 44:5—8, 1987
7. GRANT D, ZHONG R, STILLER C, WALLACE C, KEOWN P. DUFF J:A comparison of cyclosporine A and Nva2-cyclosporine (cyclospo-rifle 0) in a rat renal allograft model. Transplantation 44:9—12, 1987
8. HOYT EG, HAGBERG RC, BILLINOHAM ME, BALDWIN JC, JAMIE-SON SW: Analysis of the immunosuppressive and nephrotoxiceffects of cyclosporin G. J Heart Transplant 7:111—118, 1988
9. ADAMS M, BENNETF W, DANOVITCH G, DAWIDSON I, LEICHTMANA, LIGHT J, SAL0MON D: Preliminary evidence of the safety andefficacy of 00 37-325, a cyclosporine analogue, in human renaltransplantation. (abstract) Am Soc Transplant Phys 11:71, 1992
10. LEICHTMAN AB, SCHMOUDER RL, GRATIOT-DEANS J, MERIONRM, HAM JM, SWARTZ RD, CAMPBELL DA, TURCOTTE JG, TURKAL: Preliminary evidence suggests that OG 37-325, a cyclosporineanalogue, has a wider therapeutic window than cyclosporine A.(abstract) JAm Soc Nephrol 3:866, 1992
11. HENRY ML, TESI RJ, ELKHAMMAS EA, FERGUSON RM: A random-ized, prospective, double-blinded trial of cyclosponne vs. 0037-325 in cadaveric renal transplantation—A preliminary report.Transplantation 55:748—752, 1993
12. COLLIER SJ, CALNE RY, WHITE DJG, WINTERS S, THIRU S: Bloodlevels and nephrotoxicity of cyclosporin A and G in rats. Lancet1:216, 1986
13. PALLER MS, FERRIS TF: Effects of Nva2-cyclosporine on glomer-ular filtration rate and renal blood flow in the rat. Transplantation43:893—895, 1987
14. TEJANI A, LANCMAN I, POMRANTZ A, KHAWAR M, CHEN C:Nephrotoxicity of cyclosporine A and cyclosporine G in a ratmodel. Transplantation 45:184—187, 1988
15. FARACI M, VIGEANT C, YALE JF: Pharmacokinetic profile ofcyclosporine A and 0 and their effects on cellular immunity andglucose tolerance in male and female Wistar rats. Transplantation45:617—621, 1988
16. HAGBERG RC, HOYT EG, BILLINGHAM ME, SIBLEY RK, STARNE5VA, BALDWIN JC: Comparison of cyclosporin A and G with andwithout azathioprine regarding immunosuppressive efficacy, toxic-ity, and pharmacokinetics in Lewis rats. J Heart Transplant7:359—369, 1988
17. KAwASHIMA H, M0cHIzuKI M, OKUMURA A, FUJINO Y, TANGET, HORIUCHI D, HIGASHIHARA E, KAKU H, INABA G: Cyclospo-rine G and D in experimental autoimmune uveoretinitis in the rat.Jpn J Ophthalmol 33:425—440, 1989
18. OGUNNAIKE HO, STARKEY TD, BALDWIN JC, PORTER KA, BILL-INGHAM ME, JAMIESON SW: An assessment of Nva2-cyclosporinein primate cardiac transplantation. Transplantation 43:13—17, 1987
19. HUSER B, THIEL 0, OBERHOLZER M, BEVERIDGE T, BIANCHI L,MIHATSCH MJ, LANDMANN J: The efficacy and tolerability ofcyclosporine G in human kidney transplant recipients. Transplan-tation 54:65—69, 1992
20. MASRI MA, NAIEM M, PINGLE S, DAAR AS: Cyclosporine A versuscyclosporine G: A comparative study of survival, hepatotoxicity,nephrotoxicity, and splenic atrophy in BALB/c mice. Transplantmt 1:13—18, 1988
21. ROSEN 5, GREENFELD Z, BRKzIs M: Chronic cyclosporine-inducednephropathy in the rat. Transplantation 49:445-452, 1990
22. ELZINGA LW, ROSEN S, BENNETT WM: Dissociation of glomerularfiltration rate from tubulointerstitial fibrosis in experimental chroniccyclosporine nephropathy: Role of sodium intake. J Am SocNephrol 4:214—221, 1993
23. YATSCOFF RW, JEFFERY JR: Quantification of cyclosporin G(NVa2 cyclosporin) by radioimmunoassay. Clin Chem 32:700—701,1986
24. RUGGENENTI P, PERICO N, MOSCONI L, GASPARI F, BENIGNI A,AMUCHASTEGUI CS, BRuzzi I, REMuzzI G: Calcium channelblockers protect transplant patients from cyclosporine-induceddaily renal hypoperfusion. Kidney mt 43:706—711, 1993

Burdmann et a!: Pharmacokinetics of CsG vs. GsA 691
25. R00TH P, DAVIDSON I, CLOTHIER N, DILLER K: In vivo fluores-cence microscopy of kidney subcapsular blood flow in mice.Transplantation 46:566—569, 1988
26. BECKER GM, GANDOLFI AJ, NAGLE RB: Effects of cyclosporin Aon a kidney epithelial cell line (LLC-PK1). Res Commun ChemPathol Pharmacol 56:277—280, 1987
27. PALESTINE AG, AUSTIN HA III, BALOW JE, ANTONOVYCH TT,SABNIS SG, PREUSS HG, NUSSENBLATr RB: Renal histopathologicalterations in patients treated with cyclosporine for uveitis. N Eng!J Med 314:1293—1298, 1986
28. MYERS BD, SIBLEY R, NEWTON L, TOMLANOVICH Si, BOSHKOS C,STINSON E, LUETSCHER JA, WHITNEY Di, KRASNY D, COPLONNS, PERLROTH MG: The long-term course of cyclosporine-associ-ated chronic nephropathy. Kidney mt 33:590—600, 1988
29. ZALTZMAN iS, PEI Y, MAURER J, PATTERSON A, CATTRAN DC:Cyclosporine nephrotoxicity in lung transplant recipients. Trans-
plantation 54:875—878, 199230. MYERS BD, NEWTON L, BosHKos C, MACOVIAK JA, FRIST WH,
DERBY GC, PERLROTH MG, SIBLEY RK: Chronic injury of humanrenal microvessels with low-dose cyclosporine therapy. Transplan-tation 46:694—703, 1988
31. BALLETTA M, LIBETTA C, FUIANO G, DELFINO M, BRUNETTI B,UNGARO B, CONTE G: Effects of a two-month treatment with loworal doses of cyclosporin on renal function, Nephrol Dial Trans-plant 6:324—329, 1991
32. ZACHARIAE H, HANSEN HE, KRAGBALLEK K, OLSEN 5: Morpho-logic renal changes during cyclosporine treatment of psoriasis. JAm Acad Dermatol 24:415—419, 1992
33. GNUTZMANN KH, HERING K, GUTSCHE H-U: Effect of cyclospo-
rine on the diluting capacity of the rat kidney. Clin Nephrol25(Suppl l):551—S56, 1986
34. GUDER WG, HOFMANN W: Future markers for the diagnosis ofrenal lesions, in: Nephrotoxicity, Mechanisms, Early Diagnosisand Therapeutic Management, edited by BACH PH, GREGG NJ,WILKSMF, DELACRUZL, New York, Marcel Dekker Inc., 1991, p.575
35. BURDMANN EA, ANDOH TF, LINDSLEY i, HOUGHTON DC, BEN-
NETT WM: Effects of oral magnesium supplementation on acuteexperimental cyclosporine nephrotoxicity. Nephrol Dial Trans-plant (in press)
36. COPELAND KR, YATSCOFF RW: The isolation, structural charac-terization, and immunosuppressive activity of cyclosporin G(NVa2-cyclosporine) metabolites. Ther Drug Monit 13:281—288,1991
37. DONNELLY iG, CHEN Y, YATSCOFF RW, COPELAND KR, PA-LASZYNSKI EW, SOLDIN SJ: Cyclosporin G and metabolite bindingto cyclophilin and a 50-kDa binding protein related to in Vitroimmunosuppression. Clin Chem 39:122—125, 1993
38. RAYAT G, YATSCOFF R, SILVERMAN R, MCKENNA R: A compar-ison of the immunosuppressive effects of cyclosporine A andcyclosporine G in vivo and in vitro. Transplantation 55:623—626,1993
39. MCCAULEY i, STUDER R, CRAVEN P, MURRAY S: The effects ofcyclosporine A, cyclosporine G, and FK 506 upon prostaglandinproduction in renal mesangial cells in culture. Transplant Proc23:3141—3142, 1991
40. BACKMAN L, APPELKVIST EL, SUNDBERG A, TECLEBRHAN H,BRUNK U: Modulation of metabolism in HepG2 cells upon treat-ment with cyclosporin A and NVa2-cyclosporin. Exp Mo! Pathol54:242—254, 1991
41. WHITE DiG, CALNE RY, COLLIER Si, ROLLES K, WINTER S,DRAKOPOULOS 5: Is cyclosporine G more or less immunosuppres-sive than cyclosporine A? Transplant Proc 18:1244—1245, 1986
42. D'SouzA Mi, GOURDIKIAN KB, MUJUKIAN AL: Comparison ofcyclosporine A and G pharmacokinetics. Drug Metab Dispos16:895—897, 1988
43. VENKATARAMANAN R, ToDo S, ZAGHLOUL I, LYNCH S, KAM I,PTACHCINSKI Ri, BURCKART Gi, STARZL TE: Comparative phar-macokinetics of cyclosporine G and Nva2-cyclosporine in dogs.Transplant Proc 19:1265—1266, 1987
44. WENK M, BINDSCHEDLER M, COSTA E, ZUBERM, VOZEH S,THIEL G, ABISCH E, KELLER HP, BEVERIDGE T, FOLLATH F:Pharmacokinetics of cyclosporine 0 in patients with renal failure.
Transplantation 45:558—561, 1988