expense form: ercc team member training - pswfundltc.ca education fund resource packag… · the...
TRANSCRIPT
PSW Education Fund for Long-Term Care 2017-2018
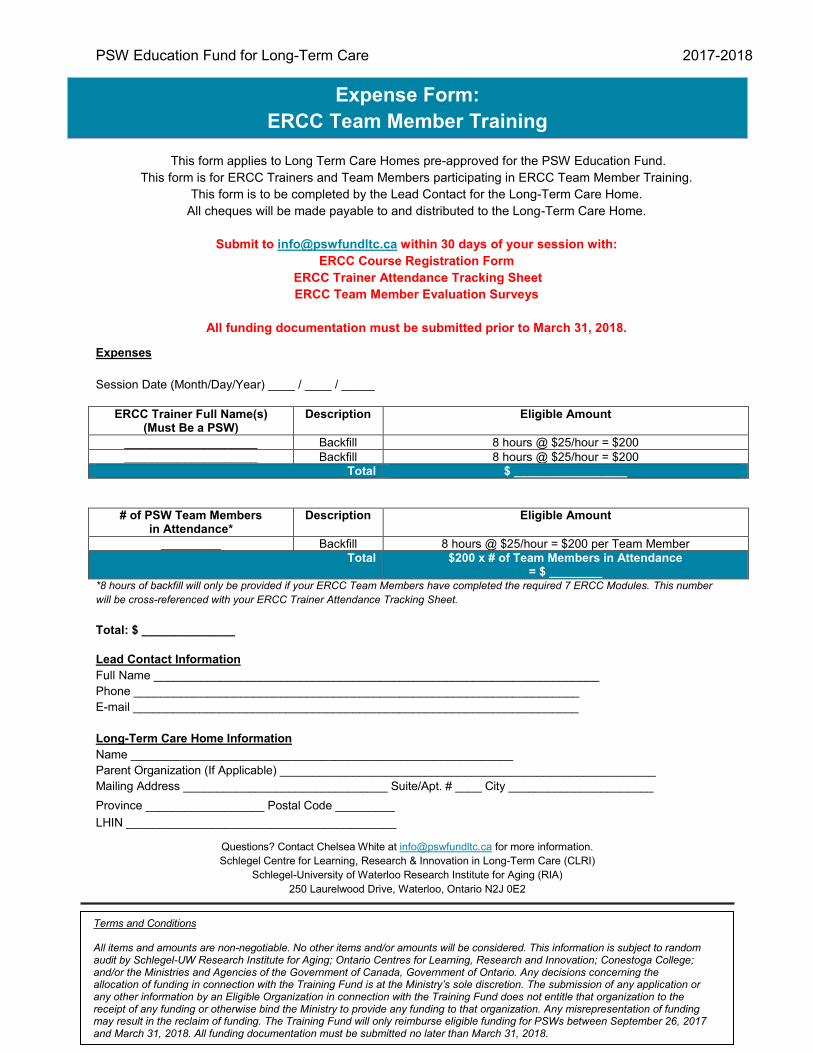
Expenses Session Date (Month/Day/Year) ____ / ____ / _____
ERCC Trainer Full Name(s) (Must Be a PSW)
Description Eligible Amount
____________________ Backfill 8 hours @ $25/hour = $200 ____________________ Backfill 8 hours @ $25/hour = $200
Total $ _________________
# of PSW Team Members in Attendance*
Description Eligible Amount
_________ Backfill 8 hours @ $25/hour = $200 per Team Member Total $200 x # of Team Members in Attendance
= $ ________ *8 hours of backfill will only be provided if your ERCC Team Members have completed the required 7 ERCC Modules. This number will be cross-referenced with your ERCC Trainer Attendance Tracking Sheet. Total: $ ______________
Lead Contact Information Full Name ___________________________________________________________________ Phone ___________________________________________________________________ E-mail ___________________________________________________________________ Long-Term Care Home Information Name __________________________________________________________ Parent Organization (If Applicable) _________________________________________________________ Mailing Address _______________________________ Suite/Apt. # ____ City ______________________ Province __________________ Postal Code _________ LHIN _________________________________________
Expense Form: ERCC Team Member Training
Terms and Conditions All items and amounts are non-negotiable. No other items and/or amounts will be considered. This information is subject to random audit by Schlegel-UW Research Institute for Aging; Ontario Centres for Learning, Research and Innovation; Conestoga College; and/or the Ministries and Agencies of the Government of Canada, Government of Ontario. Any decisions concerning the allocation of funding in connection with the Training Fund is at the Ministry’s sole discretion. The submission of any application or any other information by an Eligible Organization in connection with the Training Fund does not entitle that organization to the receipt of any funding or otherwise bind the Ministry to provide any funding to that organization. Any misrepresentation of funding may result in the reclaim of funding. The Training Fund will only reimburse eligible funding for PSWs between September 26, 2017 and March 31, 2018. All funding documentation must be submitted no later than March 31, 2018.
This form applies to Long Term Care Homes pre-approved for the PSW Education Fund. This form is for ERCC Trainers and Team Members participating in ERCC Team Member Training.
This form is to be completed by the Lead Contact for the Long-Term Care Home. All cheques will be made payable to and distributed to the Long-Term Care Home.
Submit to [email protected] within 30 days of your session with:
ERCC Course Registration Form ERCC Trainer Attendance Tracking Sheet ERCC Team Member Evaluation Surveys
All funding documentation must be submitted prior to March 31, 2018.
Questions? Contact Chelsea White at [email protected] for more information. Schlegel Centre for Learning, Research & Innovation in Long-Term Care (CLRI)
Schlegel-University of Waterloo Research Institute for Aging (RIA) 250 Laurelwood Drive, Waterloo, Ontario N2J 0E2
139
Second Career
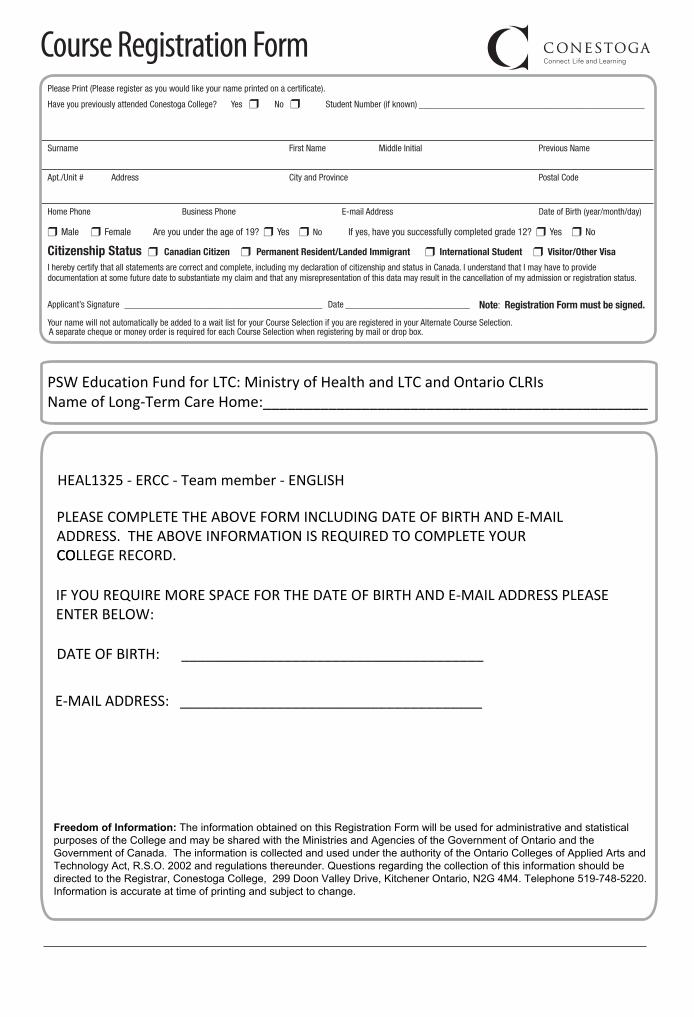
Please Print (Please register as you would like your name printed on a certificate).
Have you previously attended Conestoga College? Yes ❒ No ❒ Student Number (if known) _________________________________________________
Surname First Name Middle Initial Previous Name
Apt./Unit # Address City and Province Postal Code
Home Phone Business Phone E-mail Address Date of Birth (year/month/day)
❒ Male ❒ Female Are you under the age of 19? ❒ Yes ❒ No If yes, have you successfully completed grade 12? ❒ Yes ❒ No
Citizenship Status ❒ Canadian Citizen ❒ Permanent Resident/Landed Immigrant ❒ International Student ❒ Visitor/Other Visa
I hereby certify that all statements are correct and complete, including my declaration of citizenship and status in Canada. I understand that I may have to provide documentation at some future date to substantiate my claim and that any misrepresentation of this data may result in the cancellation of my admission or registration status.
Applicant’s Signature ___________________________________________ Date ___________________________ Note: Registration Form must be signed.
Your name will not automatically be added to a wait list for your Course Selection if you are registered in your Alternate Course Selection. A separate cheque or money order is required for each Course Selection when registering by mail or drop box.
DATE OF BIRTH: ______________________________________
Course Registration Form
IF YOU REQUIRE MORE SPACE FOR THE DATE OF BIRTH AND E-MAIL ADDRESS PLEASE ENTER BELOW:
E-MAIL ADDRESS: ______________________________________
PSW Education Fund for LTC: Ministry of Health and LTC and Ontario CLRIsName of Long-Term Care Home:_______________________________________________
HEAL1325 - ERCC - Team member - ENGLISH
Freedom of Information: The information obtained on this Registration Form will be used for administrative and statistical purposes of the College and may be shared with the Ministries and Agencies of the Government of Ontario and the Government of Canada. The information is collected and used under the authority of the Ontario Colleges of Applied Arts and Technology Act, R.S.O. 2002 and regulations thereunder. Questions regarding the collection of this information should be directed to the Registrar, Conestoga College, 299 Doon Valley Drive, Kitchener Ontario, N2G 4M4. Telephone 519-748-5220. Information is accurate at time of printing and subject to change.
PLEASE COMPLETE THE ABOVE FORM INCLUDING DATE OF BIRTH AND E-MAIL ADDRESS. THE ABOVE INFORMATION IS REQUIRED TO COMPLETE YOUR COLLEGE RECORD.CO

PSW Education Fund for Long-Term Care 2017-2018
PSWs Trained
Cou
rse
Reg
istra
tion
Form
Atta
ched
Each PSW is required to complete 7 modules. Modules 1 and 12 are mandatory.
Date of Completion
Mod
ule
1
Mod
ule
2
Mod
ule
3
Mod
ule
4
Mod
ule
5
Mod
ule
6
Mod
ule
7
Mod
ule
8
Mod
ule
9
Mod
ule
10
Mod
ule
11
Mod
ule
12
Sum
mat
ive
Test
>65
%
Last Name
First Name
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
ERCC Trainer Attendance Tracking Sheet

PSW Education Fund for Long-Term Care 2017-2018 15.
16.
17.
18.
19.
20.
We, as a Long-Term Care Home, confirm that all individuals trained are PSWs and have successfully completed the ERCC Team Member course requirements in accordance with the PSW Education Fund. Long-Term Care Home Name: _________________________________________
Trainer Name: ________________________________________________
Trainer Name: ________________________________________________ Long-Term Care Home Lead Contact Name: _______________________________________
Long-Term Care Home Lead Contact Signature: ____________________________________
We, as a Long-Term Care Home, understand that we may be randomly audited and asked to provide documentation at some future date to substantiate our claims and that any misrepresentation of this data may result in the reclaiming of our funding through the PSW Education Fund.

PSW Education Fund for Long-Term Care 2017-2018
1. What is one thing you will change in your daily routine based on what you have learned in this ERCC Team Member training session?
2. Do you feel this ERCC Team Member training experience helped provide an opportunity for you
to voice your ideas, strategies and solutions?
Strongly Agree
O
Somewhat Agree
O
Agree
O
Neutral
O
Disagree
O
Somewhat Disagree
O
Strongly Disagree
O
3. Do you feel this ERCC Team Member training will enhance resident quality outcomes and care?
Strongly Agree
O
Somewhat Agree
O
Agree
O
Neutral
O
Disagree
O
Somewhat Disagree
O
Strongly Disagree
O
4. What future modules would be helpful for your Long-Term Care Home’s educational initiatives (list all that apply)?
5. Additional comments: