executive function determinants of attention-deficit
TRANSCRIPT

University of Calgary
PRISM: University of Calgary's Digital Repository
Graduate Studies The Vault: Electronic Theses and Dissertations
2013-10-02
Executive Function Determinants of
Attention-Deficit/Hyperactivity Disorder Medication
Response
Kubas, Hanna
Kubas, H. (2013). Executive Function Determinants of Attention-Deficit/Hyperactivity Disorder
Medication Response (Unpublished master's thesis). University of Calgary, Calgary, AB.
doi:10.11575/PRISM/26036
http://hdl.handle.net/11023/1117
master thesis
University of Calgary graduate students retain copyright ownership and moral rights for their
thesis. You may use this material in any way that is permitted by the Copyright Act or through
licensing that has been assigned to the document. For uses that are not allowable under
copyright legislation or licensing, you are required to seek permission.
Downloaded from PRISM: https://prism.ucalgary.ca

UNIVERSITY OF CALGARY
Executive Function Determinants of Attention-Deficit/Hyperactivity
Disorder Medication Response
by
Hanna Alexandra Kubas
A THESIS
SUBMITTED TO THE FACULTY OF GRADUATE STUDIES
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE
DEGREE OF MASTER OF SCIENCE
DEPARTMENT OF EDUCATIONAL PSYCHOLOGY
CALGARY, ALBERTA
SEPTEMBER, 2013
© Hanna A. Kubas 2013

ii
Abstract
Focusing on behavioural criteria for attention-deficit/hyperactivity disorder (ADHD) diagnosis
leads to considerable neuropsychological profile heterogeneity among diagnosed children and
variable response to methylphenidate (MPH) treatment. Documenting “cool” executive/working
memory (EWM) or “hot” self-regulation (SR) neuropsychological impairments could aid in
differential diagnosis of ADHD subtypes and may help determine the optimal MPH treatment
dose. In this study, children with ADHD Inattentive Type (n = 18) (IT) and Combined (n = 35)
(CT) underwent a randomized double-blind placebo-controlled 4-week MPH trial.
Neuropsychological, behavioural, and observational data were collected to evaluate medication
response. Results from individual neuropsychological tests suggest that performance was not
uniform; those with moderate or significant baseline EWM/SR impairment showed robust MPH
response, while response for those with lower baseline executive impairment was minimal.
Implications for medication titration, academic achievement, and long-term treatment efficacy
were examined.

iii
Acknowledgements
I would like to take this opportunity to sincerely thank all of those who helped make this
thesis a reality. First, I would like to thank my committee members, Dr. James B. Hale, Dr.
Gabrielle Wilcox, and Dr. Deborah Dewey, for agreeing to share this exciting educational
milestone with me.
To all of the former and current BrainGain Laboratory members: Andrea Schneider,
Emilie Crevier-Quintin, Jessica Carmichael, Kim Fitzer, and Erica Backenson, your constant
encouragement and unwavering support helped me get through the tough times. To my UVic and
U of C cohorts, thanks for the memories; I was lucky enough to be a part of two amazing groups.
Thank you to the Social Sciences and Humanities Research Council for their continued
support throughout my studies. Without their support I would not have been able to dedicate as
much of my time to developing and growing as a researcher and an academic.
To my family, Jacek, Joanna, Karol, Pisiu, and Mila: thank you for putting up with my
grumpiness, and school work obligations on evenings, weekends, and holidays, for reminding me
to relax during the stressful times, and for helping me realize that work is not always the most
important part of life.
And last, but certainly not least, I would like to express my deepest gratitude to my
supervisor, Dr. James B. Hale, for his continued guidance and patience, for always believing in
me and pushing me to be best that I can be, and for never being afraid to challenge current
practice. Together we will accomplish great things.

iv
Dedication
To my family and friends,
I could not have done this without you.
Enjoy.

v
Table of Contents
Abstract ............................................................................................................................... ii!
Acknowledgements ........................................................................................................... iii!
Dedication .......................................................................................................................... iv!
Table of Contents .................................................................................................................v!
List of Tables ................................................................................................................... vii!
List of Figures .................................................................................................................. viii!
List of Symbols, Abbreviations and Nomenclature ........................................................... ix
Co-Authorship Statement ................................................................................................. ixi
Chapter 1: Introduction ....................................................................................................1!
1.1 Background ................................................................................................................1!
1.2 Frontal-subcortical circuits and the biological basis of ADHD .................................3!
1.3 “Hot” versus “Cold” frontal-subcortical circuits .......................................................5!
1.4 Methylphenidate treatment in ADHD ........................................................................6!
1.5 Methylphenidate effects on cognitive and neuropsychological functioning .............8!
1.6 Methylphenidate effects on academic functioning ..................................................10!
1.7 Purpose of Current Study .........................................................................................12!
Chapter 2: Method ...........................................................................................................15!
2.1 Participants ...............................................................................................................15!
2.2 Procedure .................................................................................................................16!
2.3 Instrumentation ........................................................................................................20!
2.3.1 Go No-Go Test ................................................................................................20!
2.3.2 Stroop Color-Word Test ..................................................................................21!
2.3.3 Test of Memory and Learning-Digits Backwards ...........................................22!
2.3.4 Wisconsin Selective Reminding Test of Memory ...........................................23!
2.3.5 Trail Making Test–Part B ................................................................................24!
2.3.6 Conners’ Continuous Performance Test–II .....................................................24!
2.3.7 Hale-Denckla Cancellation Test ......................................................................26!

vi
Chapter 3: Results ............................................................................................................27!
3.1 Overview ..................................................................................................................27!
3.2 Individual neuropsychological assessment measure results ....................................30!
3.2.1 Go No-Go Test ................................................................................................30!
3.2.2 Stroop Color-Word Test ..................................................................................31!
3.2.3 Test of Memory and Learning-Digits Backwards ...........................................32!
3.2.4 Wisconsin Selective Reminding Test of Memory ...........................................33!
3.2.5 Trail Making Test Part B .................................................................................33!
3.2.6 Conners’ Continuous Performance Test-II ......................................................34!
3.2.7 Hale-Denckla Cancellation Test ......................................................................36
Chapter 4: Discussion ......................................................................................................37!
4.1 Overview of findings ...............................................................................................37!
4.2 Implications for “hot” and “cool” circuit executive functions ................................38!
4.3 Implications for academic achievement in ADHD ..................................................39!
4.4 Limitations ...............................................................................................................40!
4.5 Future research .........................................................................................................41!
Chapter 5: Conclusion .....................................................................................................43!
References ..........................................................................................................................46
Appendix A: Summary of Means, Standard Deviations, and MPH Dose-Response
Relationships for Executive Working Memory “Cool” Circuit Neuropsychological
Measures Across Impairment Groups .......................................................................69
Appendix B: Summary of Means, Standard Deviations, and MPH Dose-Response
Relationships for Self-Regulation “Hot” Circuit Neuropsychological Measures Across
Impairment Groups ...................................................................................................70
Appendix C: Copyright Permission Letter .......................................................................71!
vii
List of Tables
Table 1. MPH Dose-Response Relationships for EWM/SR Impairment Groups for
Individual Tests ......................................................................................................28

viii
List of Figures
Figure 1. Confirmatory Factor Analysis Frontal-Subcortical Circuit Loadings ....................14
Figure 2. Procedure for the Double-Blind Placebo Protocol ................................................17!
Figure 3. Dose-Response Relationships for Neuropsychological Tests by Impairment Group
................................................................................................................................29
!

ix
List of Symbols, Abbreviations and Nomenclature
Abbreviation Definition ADHD Attention-Deficit/Hyperactivity Disorder
EF Executive functions LD Learning Disability DA Dopamine NE Norepinephrine
MPH Methylphenidate EWM Executive Working Memory or “cool” dorsolateral-dorsal cingulate circuit
SR Self-Regulation of “hot” orbital-ventral cingulate circuits ADHD-IT ADHD-Inattentive Type Subtype
ADHD-HIT ADHD-Hyperactive-Impulsive Subtype ADHD-CT ADHD-Combined Type Subtype
SCT Sluggish Cognitive Tempo APA American Psychiatric Association
DSM-IV-TR Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition–Text Revision
SD Standard Deviation M Mean
NPStat Non-Parametric Randomization Test for Statistical Ranks MANOVA Multivariate Analysis of Variance
ODD/CD Oppositional Defiant Disorder/Conduct Disorder A/D Anxiety/Depression
IQ Intelligence PI Principal Investigator B Baseline Condition P Placebo Condition L Low Dose Condition H High Dose Condition
N/A No Apparent Baseline Executive Impairment Low Low Baseline Executive Impairment
Moderate Moderate Baseline Executive Impairment High High Baseline Executive Impairment RCT Randomized Controlled Trial SEM Structural Equation Modeling fMRI Functional Magnetic Resonance Imaging
DTI Diffusion Tensor Imaging
x
Test Abbreviation
Assessment Measure
TEA-CH Test of Everyday Attention for Children CELF-3 Clinical Evaluation of Language Fundamentals 3
WIAT-II Wechsler Individual Achievement Test-II Stroop Stroop Color-Word Test
TOMAL-DB Test of Memory and Learning-Digits Backwards WSRTM Wisconsin Selective Reminding Test of Memory
TMT-B Trail Making Test-Part B CPT-II Conners’ Continuous Performance Test-II HDCT Hale-Denckla Cancellation Test CBCL Child Behavior Checklist
TRF Teacher Report Form CPRS-R:L Conners’ Parent Rating Scales–Revised: Long Form CTRS-R:L Conners’ Teacher Rating Scales–Revised: Long Form
APRS Academic Performance Rating Scale SSQ-R School Situations Questionnaire-Revised SERS Side Effects Rating Scale RAT Restricted Academic Task

xi
Co-Authorship Statement
The results presented in Chapter Three of this thesis have been previously published. The
citation for the journal article publication is:
Kubas, H. A., Backenson, E. M., Wilcox, G., Piercy, J. C., & Hale, J. B. (2012). The effects of
methylphenidate on cognitive functions in children with attention-deficit/hyperactivity
disorder. Postgraduate Medicine, 124(5), 33–48. doi:10.3810/pgm.2012.09.2592
As the first author, I was in charge of the preparation and submission of the manuscript, as well
as the formulation of research questions, literature review, data analyses, and write-up of results.
I was also in charge of writing the manuscript, and the final edits required by the publisher.
The results presented in Chapter Three were also disseminated as a poster presentation at an
international conference. The citation for the poster presentation is:
Kubas, H. A., Backenson, E. M., Wilcox, G., Piercy, J. C., Carmichael, J. A., Fitzer, K. R., &
Hale, J. B. (2013, February). Differentiating frontal-subcortical circuit executive
dysfunction in ADHD medication response. Poster presentation at the 41st annual
International Neuropsychological Society meeting.
As the first author, I was in charge of compiling and preparing all aspect of the presentation, as
well as presenting the poster at the conference.

1
Chapter 1: Introduction
1.1 Background
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder
encompassing a heterogeneous group of children who display persistent age-inappropriate
symptoms of hyperactivity, impulsivity, and inattention across multiple domains of functioning
(American Academy of Pediatrics [AAP], 2011; American Psychiatric Association [APA],
2000). Prevalence estimates suggest that approximately 5-7% of children and adolescents are
affected worldwide (Polanczyk, de Lima, Horta, Biederman, & Rhode, 2007; Willcutt, 2012),
making ADHD one of the most common childhood neuropsychiatric disorders (Barkley, 2006a).
Although still considered a disruptive behaviour disorder (APA, 2000), it is now widely
acknowledged that ADHD is a frontal-subcortical circuit disorder contributing to deficits in
executive functions (EF) including planning, organization, inhibition, working memory,
problem-solving, mental flexibility, monitoring, and evaluation (Biederman et al., 2004; Hale et
al., 2009a; Sonuga-Barke, Sergeant, Nigg, & Willcutt, 2008).
Although ADHD is now widely recognized as a frontal-subcortical circuit disorder
(Castellanos et al., 2002; Hale et al., 2009b), behavioural criteria and rating scales remain the
most commonly used diagnostic tools, leading to heterogeneous grouping of children with very
different manifestations of symptomology (Hale et al., 2012) and ratings that are insensitive to
neurocognitive functioning (Manor et al., 2008). Further, since most frontal-subcortical circuit
disorders lead to impaired attention (Lichter & Cummings, 2001), differential diagnosis of
ADHD becomes difficult when only behavioural criteria are used (Hale, Fiorello, & Brown,
2005).

2
ADHD often shows comorbidity with a wide variety of psychiatric conditions (Taylor,
2011; Willcutt et al., 2012), including externalizing (e.g., oppositional defiant, conduct disorder)
and internalizing (e.g., depression, anxiety) psychopathology (Barkley, 2006b), as well as
associations with specific learning and developmental problems (Thapar, Cooper, Eyre, &
Langley, 2012). ADHD tends to have an especially profound impact on academic functioning
(DuPaul & Stoner, 2003), and children with ADHD often exhibit significantly lower grades and
achievement scores, and higher rates of grade retention and school dropout, when compared to
peers without ADHD (Barkley, 2006a; Loe & Feldman, 2007).
It has been suggested that poor academic achievement in children with ADHD may be
the result of executive function deficits (Biederman et al., 2004), with prevalence rates of
comorbid ADHD and learning disabilities (LD) estimated to be around 31% (DuPaul & Stoner,
2003). Of the cognitive processes that fall under the umbrella of executive functions, working
memory deficits have been the strongest and most consistent impairments found in children with
ADHD (Castellanos, Sonuga-Barke, Milham, & Tannock, 2006; Martinussen, Hayden, Hogg-
Johnson, & Tannock, 2005; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Since
working memory is particularly important for memory encoding and retrieval, it should not be
surprising that impairment in these areas affects classroom learning and academic achievement
(Barkley, 1997; Wilcutt et al., 2005). While the ADHD–LD association may be the result of
common underlying neural pathways (Semrud-Clikeman, 2005), it remains unclear whether
learning difficulties associated with academic skill and/or performance deficits result from a
shared genetic etiology (Isles & Humby, 2006), a predisposition to comorbid disorders such as
conduct problems inadvertently leading to poor academic performance (Rhee, Willcutt, Hartman,
Pennington, & DeFries, 2008), behavioural interference with performance in the classroom (e.g.,

3
noncompliance, limited on-task behaviour) (DuPaul & Stoner, 2004), and/or cognitive and
neuropsychological deficits (Goldstein & Naglieri, 2008; Roth & Saykin, 2004).
Psychotropic medication is the most common form of treatment for children with ADHD
(Barkley, 2006b), and numerous studies have documented significant short-term benefits of
medication on objective measures of academic functioning (Chacko et al., 2006; Evans et al.,
2001; Pelham et al., 2001; Powers, Marks, Miller, Newcorn, & Halperin, 2008). However, the
effects of long-term medication use on academic outcomes in children with ADHD remain
unclear (Langberg & Becker, 2012). The long-term benefits of medication use are important
issues for families of children with ADHD (Hansen & Hansen, 2006), especially since grades
and achievement scores largely determine student acceptance into post-secondary programs and
strongly predict academic performance in college (Zwick & Sklar, 2005). As such, physicians
and other healthcare professionals need to be able to make evidence-based recommendations for
families of children and youth with ADHD that will maximize academic performance, while at
the same time managing problematic behaviours.
1.2 Frontal-subcortical circuits and the biological basis of ADHD
The main cortical areas implicated in ADHD include the prefrontal cortex – in particular,
the dorsolateral prefrontal and inferior prefrontal cortices (Dickstein, Bannon, Castellanos, &
Milham, 2006) – and their associated frontal-subcortical circuits and structures, including the
striatum (caudate, putamen), the thalamus (Castellanos et al., 2002; Hale et al., 2009b; Lichter &
Cummings, 2001), the limbic regions (e.g., nucleus accumbens), the corpus callosum and related
white matter tracts (Valera, Faraone, Murray, & Seidman, 2007), and the cerebellum (Vaidya &
Stollstroff, 2008). For some children with ADHD, other cortical regions, including the temporal

4
and parietal lobes, have also been implicated (Arnsten, 2009a).
Extant meta-analyses document a consistent pattern of frontal hypoactivity in individuals
with ADHD that is widely distributed in the dorsolateral and orbital prefrontal cortices and
related subcortical regions (Dickstein et al., 2006). According to most nomenclatures, there are at
least five major frontal-subcortical circuits, including the dorsolateral, orbitofrontal, anterior
cingulate, motor, and occulomotor circuits (Lichter & Cummings, 2001).
The circuits affected in ADHD are largely governed by catecholamine (e.g., dopamine
[DA] and/or norepinephrine [NE]) neurotransmitters (Arnsten, 2009b; Arnsten & Li, 2005), with
dysregulation affecting optimal frontal-subcortical circuit functioning (Arnsten & Pliszka, 2011;
Castellanos et al., 2002). DA is a critical neurotransmitter for regulatory frontal-subcortical
circuit functioning and is associated with motivation and reward, providing for sustained task
interest and improved performance, especially during inherently unmotivating tasks (Volkow et
al., 2001; Volkow et al., 2009). Insufficient DA in the prefrontal cortex may be the consequence
of an excess of dopamine transporters, which facilitate DA reuptake into the presynaptic
membrane, thereby decreasing DA availability in the synapse (Hood, Baird, Rankin, & Isaacs,
2005). This DA paucity in the synaptic cleft has been associated with both cognitive and
behavioural ADHD symptoms (Voeller, 2001). Furthermore, different frontal-subcortical circuits
are responsible for mediating different aspects of cognition and behaviour. While the dorsolateral
prefrontal circuit has been consistently implicated in mediating EFs, the orbital prefrontal circuit
governs emotional and behavioural regulation (Lichter & Cummings, 2001).
Frontal-subcortical circuit dysregulation not only affects behaviour during cognitive and
neuropsychological assessment, it also affects EFs that are directly or indirectly required for
optimal test performance (Hale et al., 2009b; Hale et al., 2012). Thus, a child with ADHD may

5
perform adequately on many intellectual and cognitive tasks yet show subset variability resulting
in performance decrements due to his or her EF dysfunction (Hale et al., 2012).
1.3 “Hot” versus “Cold” frontal-subcortical circuits
The dorsolateral prefrontal circuit mediates traditional task-related EFs while the orbital
prefrontal circuit controls self-governed emotional and behavioural regulation (Lichter &
Cummings, 2001). Consistent with this position, Zelazo and Muller (2011) suggest a distinction
between the development of “hot” and “cool” EFs. The former represents relatively affective
(reward/punishment) EF aspects more associated with the orbital and medial prefrontal cortices,
and the latter represents cognitive aspects more associated with the dorsolateral circuit.
Accordingly, “hot” EFs are required for problem situations that necessitate high affective
involvement, such as socioemotional and behavioural functioning. Conversely, relatively abstract
or decontextualized problems, such as those requiring automatic response suppression or
preservation of information in working memory for effective problem solving, require the use of
“cool” EFs (Zelazo & Muller, 2011).
It is now widely acknowledged that ADHD is a heterogeneous disorder, with various
neural pathways and different neuropsychological profiles leading to the manifestation of ADHD
(Castellanos & Tannock, 2002; Nigg, Willcutt, Doyle, & Sonuga-Barke, 2005; Willcutt et al.,
2005). Given our understanding of frontal-subcortical circuit functioning, it is likely that circuit
dysfunction explains the cognitive and behavioural manifestations associated with ADHD
(Dickstein et al., 2006; Hale et al., 2009b; Lichter & Cummings, 2001; Volkow et al., 2001).
Expanding on the notion of “hot” versus “cool” EFs, Castellanos and colleagues (2006) suggest
that deficits in “cool” EF tasks may be implicated in inattentive symptomology and cognitive

6
tasks such as response inhibition and working memory, whereas “hot” EF deficits may be related
to hyperactive and impulsive symptoms and associated with more externalizing and risk-taking
behaviours. Further, “hot” EFs, including delay aversion and emotional regulation, tend to be
more associated with a broad range of ADHD behavioural characteristics, whereas “cool” EFs,
such as sustained attention and inhibitory control, appear to be more related to executive control
dimensions of ADHD (Solanto et al., 2001), This distinction suggests that “hot” and “cool” EFs
may be independent predictors of ADHD subtypes (Zelazo & Muller, 2011).
1.4 Methylphenidate treatment in ADHD
Although meta-analyses support the effectiveness of behavioural treatments for ADHD
(Fabiano et al., 2009), psychostimulant medications remain the most common and efficacious
treatment, with methylphenidate (MPH; Ritalin) being the most researched and prescribed form
of ADHD medication (Barkley, 2006b; Voeller, 2001). Extant treatment literature suggests that
MPH is effective in reducing symptoms of inattentiveness, impulsivity, and hyperactivity in
about 70% of children with ADHD while the child is on the medication (Engert & Pruessner,
2008; Van der Oord, Prins, Oosterlaan, & Emmelkamp, 2008). Psychostimulants directly
increase DA and indirectly increase NE availability in the prefrontal cortex and associated
circuits (Berridge et al., 2006). MPH is a DA agonist that increases the overall concentration of
this neurotransmitter in the prefrontal and associated subcortical areas by blocking the
transporter and hindering DA reuptake in the striatum (Hale et al., 2005).
MPH appears to have the most influence on DA and NE availability in the frontal-subcortical
circuits that control attention and executive functions (Lichter & Cummings, 2001), which are
consistently hypoactive in patients with ADHD (Dickstein et al., 2006; Li, Sham, Owen, & He,

7
2006). Increased availability of DA and NE has been shown to lead to both cognitive and
behavioural improvements in children with ADHD treated with MPH (Engert & Pruessner,
2008). For example, MPH helps to maintain adequate levels of DA in the striatum, enabling
children with ADHD to control their attention effectively (Hood et al., 2005). While MPH
enhances executive modulation of behaviour and cognition, emerging evidence suggests that
differences among DA receptors (Floresco & Magyar, 2006) may lead to differential MPH
effects, with low and clinically relevant doses (i.e., doses that produce clinically relevant plasma
concentrations) improving working memory and sustained attention and higher doses impairing
these cognitive-enhancing actions (Arnsten, 2006; Arnsten, 2009b; Berridge et al., 2006;
Berridge & Devilbiss, 2011). Low and clinically relevant MPH doses produce a preferential
elevation in extracellular DA and NE specific to the prefrontal cortex, whereas higher doses
potently increase extracellular doses of both neurotransmitters widely throughout the brain
(Kuczenski & Segel, 1992). Furthermore, lower doses of MPH improve behavioural and
cognitive processes mediated by the prefrontal cortex, without pronounced tolerance or
sensitization associated with extended treatment (Berridge & Devilbiss, 2011).
Consistent with these findings, higher MPH doses may be necessary for reducing
behavioural disruption and intensity in children and adolescents with ADHD, while lower MPH
doses may be more efficient at improving executive control of attention (Konrad, Gunther,
Hanisch, & Herpertz-Dahlmann, 2004). This could account for variable MPH response found in
children with behaviourally-diagnosed ADHD. Consistent with the hypothesis that varying
medication doses may differentially affect behaviour and cognition, differential MPH effects on
the “cool” (executive working memory; dorsolateral-dorsal cingulate) and “hot” (self-regulation;
orbital-ventral cingulate) frontal-subcortical circuits have been documented in the literature

8
(Castellanos et al., 2006; Kelly, Sonuga-Barke, Scheres, & Castellanos, 2007). Further,
numerous studies have found differential dose-response relationships for behaviour and
cognition in children with ADHD (Hale et al., 2011; Chacko et al., 2005; Pliszka et al., 2007),
suggesting that the best MPH dose for cognition may be lower than the best dose for behaviour,
and MPH may have a stronger linear effect on the “hot” circuit and a stronger curvilinear effect
on the “cool” circuit (Hale et al., 2011).
1.5 Methylphenidate effects on cognitive and neuropsychological functioning
Although an abundance of research documents the efficacy of MPH in reducing
noncompliant and disruptive behaviours in children with ADHD (Pearson et al., 2003; Van der
Oord et al., 2008; Waxmonsky et al., 2008), the effects of MPH on cognition and
neuropsychological functioning have been less consistent (Conners, 2002; Hale et al., 2011).
While some propose that improvements in cognitive and behavioural functioning follow a linear
pattern, with ADHD symptom improvement noted at successively higher stimulant doses
(Pearson et al., 2004; Rapport, Denney, DuPaul, & Gardner, 1994), others have found a
curvilinear response, whereby lower doses of stimulants resulted in initial improvements relative
to placebo, followed by deterioration at higher doses (Hale et al., 2011; Hoeppner et al., 1997;
Sprague & Sleator, 1976). A recent meta-analysis on the effects of MPH on various
neuropsychological tasks found that higher doses of MPH resulted in greater improvements than
lower doses for some tasks but provided no additional improvements on others (Pietrzak,
Mollica, Maruff, & Snyder, 2006). Thus, MPH dose response studies suggest that the optimal
dosing varies across individuals and is related to the functional domain – with high doses
producing greater enhancements in some areas (e.g. attention and vigilance) but providing no
additional improvements, or even resulting in deterioration, in other areas (e.g. planning and

9
cognitive flexibility) (Hale et al., 2011; Pietrzak et al., 2006; Swanson, Baler, & Volkow, 2011).
Inconsistent findings also emerge when investigating the effects of MPH on
neuropsychological functioning in children with ADHD. While some argue that MPH does not
result in any cognitive benefits (e.g., Kemner et al., 2004; Kobel et al., 2008), MPH related
improvements have been documented across a wide range of cognitive and neuropsychological
functions (Pietrzak et al., 2006; Swanson, et al., 2011). For instance, MPH improvements have
been documented for response inhibition and mental flexibility as measured by the Stroop Color-
Word Test (Stroop; Langleben et al., 2006), sustained attention as measured by the Test of
Everyday Attention for Children (TEA-CH; Hood et al., 2005), verbal working memory as
measured by the Clinical Evaluation of Language Fundamentals (CELF-3), ability to plan and
organize as measured by the writing subtest on the Wechsler Individual Achievement Test
(WIAT-II; Semrud-Clikeman, Pliszka, & Liotti, 2008), and visual memory and impulsivity as
measured by the Go-No Go, and Delayed-Matching-To-Sample tasks (Wilson, Cox, Merkel,
Moore, & Coghill, 2006). However, others have found mixed results, with improvement in some
areas but not others (DeVito et al., 2008; Rhodes, Coghill, & Matthews, 2006). Inconsistent
findings may be due to the monitoring of medication response in terms of their effects on
observed behaviour rather than on cognition (Hood et al., 2005). They may also be due to
differential MPH dose-response effects on cognitive and behavioural functioning (e.g., Hale et
al., 2005; Konrad et al., 2004; Pearson et al., 2004).
In addition to above optimal doses of MPH exacerbating cognitive dysfunction in some
individuals (e.g., Kuhle et al., 2007), some studies have found that high MPH doses may produce
“zombie effects” whereby in addition to poor cognitive functioning, children also become
unresponsive, hypoactive, and hyperfocused in the classroom (Tannock, Shachar, & Logan,

10
1995); however, others found no evidence to support this claim (Douglas, Barr, Desilets, &
Sherman, 1995). Due to response curve inconsistency across and within variables and individual
variability among children diagnosed with ADHD, Hoeppner and colleagues (1997) suggested
that careful examination of behavioural and cognitive MPH dose-response relationships is
warranted, especially for children who have been found to be poor responders to stimulant
treatment (e.g. Barkley, DuPaul, & McMurray, 1991).
1.6 Methylphenidate effects on academic functioning
Similar to cognitive and neuropsychological findings, studies exploring the long-term
effects of MPH on academic functioning and cognition have yielded mixed results (Advokat,
2009; Barbaresi, Katusic, Colligan, Weaver, & Jacobsen, 2007; Raggi & Chronis, 2006). While
some studies have found that MPH improves academic performance in children with ADHD
(Chacko et al., 2005; Powers, Marks, Miller, Newcorn, & Halperin, 2008), recent follow-up
studies have provided data that have generated speculations about the long-term cognitive effects
of MPH on academic functioning (Swanson et al., 2011). Although stimulant medication had a
positive impact on reading and math at the end of a 14-month study phase (MTA, 1999), follow-
up assessments revealed that after three years the initial relative benefits of treatment with
stimulant medication were no longer apparent (Jensen et al., 2007; Molina et al., 2009).
While the nature of the relationship between ADHD and academic underachievement
remains unclear, it is commonly believed that academic difficulties stem from the behavioural
manifestations of ADHD (e.g., inattention, hyperactivity, and impulsivity in the classroom)
(Corkum, McGonnell, & Schachar, 2010). An abundance of research demonstrates the efficacy
of MPH in reducing core symptoms of ADHD (Connor, 2006), in improving cognitive processes

11
considered important for learning (Rhodes et al., 2006), and in enhancing general classroom
functioning including academic accuracy and productivity (Evans et al., 2001). Many clinicians
believe that a reduction in core behaviour symptoms and improvements in underlying cognitive
processes, including attention, working memory, and response inhibition, may improve academic
performance over time by allowing children with ADHD to be more available to learn (Corkum
et al., 2010).
Although the long-term benefits of stimulant treatment have been equivocal (Swanson et
al., 2011), Volkow and colleagues (2009) have argued that MPH improves motivation for the
maintenance of academic tasks. Increased motivation may improve school performance by
increasing DA in the striatum and nucleus accumbens, thereby allowing for greater maintenance
of academic task performance. This hypothesis is consistent with Powers et al.’s (2008) report
that children and adolescents treated with psychostimulant medication achieved better
academically – as measured by standardized test and grades – than those not treated with
medication. Additionally, recent longitudinal research found positive associations between
medication use and standardized math and reading scores (Scheffler et al., 2009), with positive
long-term academic outcomes suggesting that MPH increases the availability for learning
through increased motivation, interest, and reward sensitivity (Volkow et al., 2009).
Despite evidence for increased motivation resulting from MPH treatment, differences in
cognitive and behavioural dose-response relationships may also explain the inconsistencies in
MPH effects on academic functioning (Hale et al., 2011). When differential MPH dose-response
relationships have been evaluated, higher doses often fail to offer additional benefit over lower
doses (Hale, et al., 2011). For example, Chacko et al. (2005) found academic and social
improvements for children following MPH treatment; however, few children showed significant

12
improvement with increased dosage. Similarly, a meta-analysis found that 63.5% of studies
showed improvement in cognitive functioning following MPH treatment with higher doses
producing no additional improvements over lower doses on various tasks (Pietrzak et al., 2006).
This pattern replicates earlier studies showing lower MPH doses leading to academic gains with
increasing dosage producing little additional cognitive and academic benefit (Greenhill et al.,
2001; Hale et al, 2011).
1.7 Purpose of Current Study
The present study builds upon previous research documenting cognitive and behavioural
dose-response relationships at single subject (Hale et al., 2011; Hale et al., 1998; Reddy & Hale,
2007) and group (Hale et al., 2005) levels of analyses. In this investigation, a double-blind
placebo controlled study of MPH response in children with ADHD was conducted. This research
examined whether differential MPH treatment effects emerged on various neuropsychological
measures when children with ADHD were grouped by level of “cool” executive working
memory (EWM) and “hot” self-regulation (SR) frontal-subcortical circuit impairment.
It was hypothesized that the level and pattern of baseline data obtained from the
EWM/SR neuropsychological measures described below would differentiate MPH responders
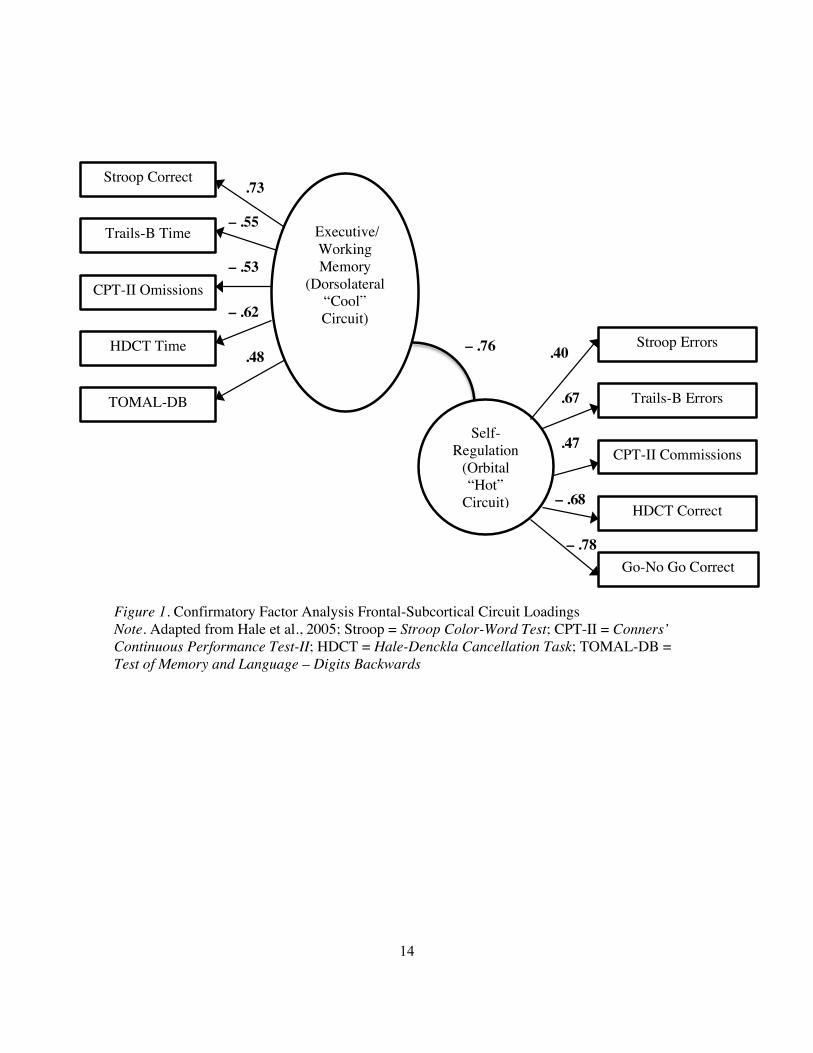
from nonresponders. In a previous study, Hale et al. (2005) used confirmatory factor analysis to
identify factor loadings and hypothesized relations to one of two frontal-subcortical circuits for a
number of different neuropsychological measures. The authors found that the number of correct
responses on the Stroop Color-Word Test (Stroop), the time on the Trail Making Test-Part B
(TMT-B), the number of omission errors on the Conners’ Continuous Performance Test-II (CPT-
II), the time on the Hale-Denckla Cancellation Test (HDCT), and the number of correct
responses on the Test of Memory and Learning-Digits Backwards (TOMAL-DB) were all related

13
to the EWM or “cool” dorsolateral-dorsal cingulate circuits, while the number of errors on the
Stroop, the number of errors on the TMT-B, the number of commission errors on the CPT-II, the
number of correct responses on the HDCT, and the number of correct responses on the Go No-
Go Test were related to the SR or “hot” orbital-ventral cingulate circuits (Hale et al., 2005; See
Figure 1 and Appendices 1 and 2 for breakdown). In this study, participants were administered
the same neuropsychological measures described above during the baseline unmedicated week.
Children’s raw scores from the baseline week were then multiplied by a factor loading obtained
by Hale and colleagues in 2005, with resultant z-scores used to determine individual baseline
executive impairment. It was predicted that neuropsychological test performance on the
measures indicated above would vary based on the level of baseline executive impairment.
Specifically, it was hypothesized that the lower medication doses would produce better
neuropsychological performance than the higher medication doses for children with moderate to
high baseline cognitive impairment, since previous research has shown that cognition begins to
deteriorate at higher medication doses (Hale et al., 2011).
!
14
.73
– .55
– .53
– .62
.48 – .76 .40
.67
.47
– .68
– .78
!!! ! ! !!!!!!!!!!!!!!!!!!!!!!
Figure 1. Confirmatory Factor Analysis Frontal-Subcortical Circuit Loadings Note. Adapted from Hale et al., 2005; Stroop = Stroop Color-Word Test; CPT-II = Conners’ Continuous Performance Test-II; HDCT = Hale-Denckla Cancellation Task; TOMAL-DB = Test of Memory and Language – Digits Backwards
Executive/ Working Memory
(Dorsolateral “Cool” Circuit)
Stroop Correct
Trails-B Time
CPT-II Omissions
HDCT Time
TOMAL-DB
Self-Regulation
(Orbital “Hot”
Circuit)
Stroop Errors
Trails-B Errors
CPT-II Commissions
HDCT Correct
Go-No Go Correct

15
Chapter 2: Method
2.1 Participants
Participants were drawn from a sample of 65 elementary and high school students that
were diagnosed by pediatricians with ADHD. Pediatricians used a semi-structured interview,
Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition–Text Revision (DSM-IV-
TR; APA, 2000) criteria, and parent and teacher behaviour rating scales to diagnose ADHD-
Inattentive Type (IT), ADHD-Hyperactive-Impulsive Type (HIT), and ADHD-Combined Type
(CT) subtypes. DSM-IV-TR diagnoses were independently confirmed by a licensed psychologist
through a semi-structured interview with parent, child, and/or teacher and review of medical,
developmental, social, and academic histories. Included participants also exhibited significant
inattention, hyperactivity, and/or impulsivity difficulties that interfered with adaptive functioning
at home and school, as conveyed by parent and/or teacher informant reports. Additionally,
participant behaviour ratings were at least 1.5 standard deviations (SDs) above the mean (M =
50; SD = 10) on one or more of the following subscales: Attention Problems of the Achenbach
(1991) Child Behavior Checklist (CBCL) or Teacher Report Form (TRF), or the DSM-IV-TR
Inattention and/or Hyperactive-Impulsive subscales of the Conners’ Parent Rating Scales–
Revised: Long Form (CPRS-R:L) or Conners’ Teacher Rating Scales–Revised: Long Form
(CTRS-R:L; Conners, 1997). Participants with more than one secondary diagnosis or those with
a diagnosis of intellectual disability, seizure disorder, brain injury, or other medical condition
affecting neuropsychological performance were excluded.
The final sample included 53 participants ranging in age from 74 to 200 months (M =
119.72 months, SD = 29.97); the majority were in grades one through five (n = 39; 74%). There
were 37 male and 16 female participants. Congruent with epidemiological studies (Barkley,

16
2006b), children diagnosed with ADHD-CT (n = 35) comprised the largest group, followed by
IT (n = 18). Common comorbid diagnoses of LD (n = 13), oppositional defiant disorder/conduct
disorder (ODD/CD; n = 9), and anxiety/depression (n = 5) were noted. Similar to other research
on the comorbidity of ADHD and internalizing disorders (Biederman, Faraone, & Lapey, 1992),
all children diagnosed with anxiety/depression were in the IT group (n = 5). Participants were all
either medication naïve, or they received a wash-out period of two days prior to beginning the
medication trial.
2.2 Procedure
Following pediatrician diagnosis, parents were referred to the Principal Investigator (PI;
last author) for a MPH medication trial. After receiving information regarding the medication,
potential side effects, and medication trial protocol, interested parents saw a licensed
psychologist. The licensed psychologist proceeded to conduct a semi-structured interview,
obtaining informed consent as well as confirming DSM-IV-TR and parent behaviour rating scale
inclusion criteria. During a teacher meeting, the treatment protocol and classroom observation
were described and scheduled. At baseline assessment only, the TRF (Achenbach, 1991) was
used for classroom behaviour assessment. Classroom behaviour assessment at baseline and
treatment follow up included four other forms: the Academic Performance Rating Scale (APRS;
DuPaul, Rapport, & Perriello, 1991) the Conners’ Teacher Rating Scales–Revised: Long Form
(CTRS-R:L; Conners, 1997), the School Situations Questionnaire-Revised (SSQ-R; DuPaul &
Barkley, 1992), and the Side Effects Rating Scale (SERS; Barkley, 1990). After the initial parent
and teaching meetings, participants received a 45-minute classroom observation and a one-hour
17
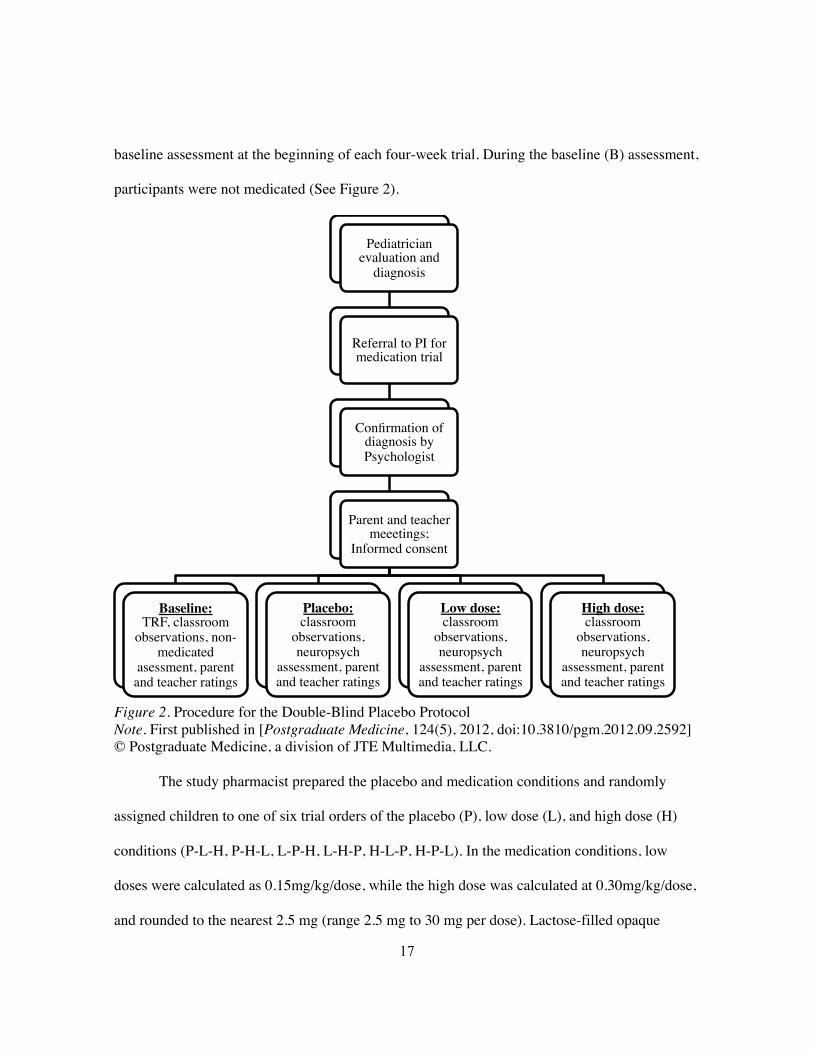
baseline assessment at the beginning of each four-week trial. During the baseline (B) assessment,
participants were not medicated (See Figure 2).
Figure 2. Procedure for the Double-Blind Placebo Protocol Note. First published in [Postgraduate Medicine, 124(5), 2012, doi:10.3810/pgm.2012.09.2592] © Postgraduate Medicine, a division of JTE Multimedia, LLC. The study pharmacist prepared the placebo and medication conditions and randomly
assigned children to one of six trial orders of the placebo (P), low dose (L), and high dose (H)
conditions (P-L-H, P-H-L, L-P-H, L-H-P, H-L-P, H-P-L). In the medication conditions, low
doses were calculated as 0.15mg/kg/dose, while the high dose was calculated at 0.30mg/kg/dose,
and rounded to the nearest 2.5 mg (range 2.5 mg to 30 mg per dose). Lactose-filled opaque
Pediatrician evaluation and
diagnosis!
Referral to PI for medication trial !
Confirmation of diagnosis by Psychologist!
Parent and teacher meeetings;
Informed consent!
!Baseline: !
TRF, classroom observations, non-
medicated asessment, parent and teacher ratings !
!
Placebo:!classroom
observations, neuropsych
assessment, parent and teacher ratings !
Low dose: classroom
observations, neuropsych
assessment, parent and teacher ratings !
High dose: classroom
observations, neuropsych
assessment, parent and teacher ratings !

18
tablets were administered for the placebo condition, while in the active drug conditions the
lactose-filled opaque capsules contained a ground MPH tablet. Both placebo and active drug
conditions were delivered twice per day. To ensure the safety of the patient and to monitor
quality control, the physician, pharmacist, and PI were not blind to the order of conditions.
However, the research assistants, teachers, parents, and participants were all unaware of the
order of conditions.
A series of neuropsychological instruments were used to assess attention, working
memory, inhibition, and self-regulation through auditory, visual, verbal, and motor domains.
Graduate students, trained and supervised by the PI, administered the tests in the same order on
the last day of each condition. The neuropsychological assessments occurred within one to two
hours after medication was administered to the children. Classroom observations took place on
the same day as the assessments, within one to two hours of the second daily dose of medication.
Off-task, fidgeting, vocalizing, playing with objects, and out of seat observable behaviours were
determined using an adaptation of the Restricted Academic Task (RAT; Barkley, 1990). During
the observational period of classroom instructional activities, a 20-second momentary time
sampling technique was utilized. In order to ensure inter-rater reliability of observational
methods, videotaped classroom recordings were used for training purposes prior to data
collection, with inter-rater reliability measured at .90 or higher for all graduate students after
receiving training in the observational procedures.
To determine MPH dose-response patterns, the ordinal data was subjected to a non-
parametric randomization test for ranks (NPStat; May, Mason, Hunter, & Wells, 1990) used to
approximate repeated measures of a multivariate analysis of variance (MANOVA) in the absence
of normal data. At the conclusion of the study, the order of conditions was revealed and brief

19
reports were provided to parents and pediatricians for subsequent clinical decision-making.
In 2005, Hale and colleagues used Structural Equation Modeling (SEM) to develop a
model of the Executive/Working Memory (EWM) and Self-Regulation (SR) factors, which were
hypothesized to reflect dorsolateral-dorsal cingulate and orbital-ventral cingulate frontal-
subcortical circuit functioning. This model was based on non-medicated, neuropsychological test
performance of children with ADHD and included the same neuropsychological measures that
were used in this study, including the: Go-No Go Test, Stroop-Color Word Test, Trails-B,
Conner’s Continuous Performance Test-II, Hale-Denckla Cancellation Task, Wisconsin
Selective Reminding Test, and Test of Memory and Language – Digits Backwards as well as the
Wisconsin Card Sorting Test and the Controlled Oral Word Association Test at baseline only.
See Figure 1 for a breakdown of the SEM derived factor scores for each of the
neuropsychological measures analyzed in this study.
In the current sample, raw scores from baseline (non-medicated) neuropsychological test
performance were multiplied by the Hale et al. (2005) derived factor scores for the same
neuropsychological measures to produce EWM dorsolateral “cool” and SR orbital “hot” scores.
Although Hale and colleagues (2005) hypothesized that EWM factors would be correlated with
DSM-IV-TR inattentive symptoms and the SR factors would be correlated with DSM-IV-TR
hyperactive/impulsive symptoms, they found that both the EWM (r = .502, p = .001) and SR (r =
.327. p = .034) correlated only with the hyperactive/impulsive symptoms. In addition, the EWM
and SR scores were highly correlated (r = -.76, p < .001). As such, the regression-based saved
EWM and SR factor scores were added to produce a combined EWM/SR impairment score.
This impairment score was then converted to a z-score for each participant. It was assumed that
positive z-scores reflected low levels of impairment and negative z-scores reflected higher levels

20
of impairment since the original Hale et al. (2005) analyses with the entire ADHD sample
yielded only moderate differences between the standardization sample and the total ADHD one.
As a result, z-scores were used to calculate no apparent (N/A; +1.01 or higher; n = 8), low (0.01
to +1.00; n = 20), moderate (0.00 to –1.00; n = 15), and high (–1.01 or lower; n = 10) executive
impairment groups.
2.3 Instrumentation
A variety of neuropsychological measures were used over the course of four-week trial to
identify medication effects on test performance over time. The utility of these reliable and valid
instruments when diagnosing ADHD and determining treatments effects is well documented in
the literature (Hale & Fiorello, 2004; Pennington & Ozonoff, 1996; Sergeant, Geurts, &
Oosterlaan, 2002; Willcutt et al., 2005), and previous studies have shown no significant practice
effects during medication trials (Hale et al., 2005, 2006; Hoeppner et al., 1997).
2.3.1 Go No-Go Test (Trommer, Hoeppner, & Zecker, 1991).
The Go No-Go test is a clinical tool with a long history of use in neuropsychological
assessments. It is used as a measure of motor inhibition, and has been used to measure
inattention and impulsivity in individuals with ADHD (Trommer et al., 1991). In this audiotaped
version, children raise and lower their index finger following a single beep sound or “Go” signal
and refrain from movement when presented with the double beep sound or “No-Go” signal. The
number of correct responses out of a total possible of 30 is recorded and used as a measure of
“hot” SR functioning. Research suggests that consistent group differences in performances are
found between controls and children with ADHD on measures of motor response inhibition,
including the Go No-Go (Pennington & Ozonoff, 1996), with consistent replicated evidence

21
demonstrating a deficit in executive motor inhibition in ADHD (Nigg, 2001). In a meta-analysis
conducted in 2005, signification differences between groups with and without ADHD were
obtained most consistently for response inhibition tasks similar to the Go No-Go (Willcutt et al.,
2005). The Go No-Go test has also been shown to be sensitive to medication effects in children
with ADHD, with even modest doses improving performance by decreasing the tendency to
make impulsive commission errors (failure to inhibit response to the No-Go signal) (Trommer et
al., 1991). It is also one of the measures used in studies that show changes in ADHD brain
functioning following stimulant treatment (see Vaidya et al., 1998). Neuroimaging research
suggests that children with ADHD do not activate frontostriatal regions in the same manner as
control participants, and tend to rely on a more diffuse network of regions, including more
dorsolateral and posterior brain regions (Durston et al., 2003; Tamm et al., 2004). Imaging
research pinpoints the right inferior prefrontal cortex as a crucial region for the ability to stop a
prepotent motor response (Rubia et al., 2005), and several studies report greater activation in the
dorsolateral and orbital prefrontal cortices during the inhibitory trials of the Go No-Go task
(Casey et al., 1997; Schulz et al., 2005). Imaging research also suggests that lower than normal
activation of the inferior prefrontal cortex may be responsible for the poor inhibitory control
often displayed by individuals with ADHD (Rubia et al., 1999).
2.3.2 Stroop Color-Word Test (Stroop; Golden, 1978).
Children are presented with colour words (e.g. “red”) that are printed in non-matching
coloured ink (e.g. blue ink). Participants name the colour of the ink rather than read the word that
is printed. Scoring consists of the number of correct word responses, used as a measure of “cool”
EWM functioning, and the number of errors (i.e., reading word instead of naming ink), used as a

22
measure of “hot” SR functioning, completed in 45 seconds. Test-retest reliability was found to be
.91, and some practice effects have been shown in college students (Spreen & Strauss, 1998).
However, the researchers suggest that increases in performance may not affect interpretation of
results if interpretation is based on the pattern rather than the level of performance. Results from
several meta-analysis indicate that children and adolescents with ADHD consistently exhibit
pooper performance on the Stroop task when compared to individuals without clinical diagnoses
(Homack & Riccio, 2004; Van Mourik et al., 2005), and neuroimaging studies have reported
greater activation in the lateral prefrontal cortex in ADHD patients during trials requiring
inhibitory control in the Stroop task (Bush et al., 1999).
2.3.3 Test of Memory and Learning-Digits Backwards (TOMAL-DB; Reynolds & Bigler, 1994).
This digit span task requires children to listen to orally presented numbers with spans
increasing in length and to repeat the digits in reverse order. The number of correct digits
recalled in the correct reverse order is used for scoring purposes. The Digit Span test is a
commonly used working memory measure, and the backward version has been found to sensitive
to ADHD neuropsychological and behavioural impairment (Hale, Hoeppner, & Fiorello, 2002).
Meta-analyses suggest that significant differences between groups with and without ADHD
emerge in the majority (55%) of studies that include verbal working memory tasks (Willcutt et
al., 2005). In another comprehensive meta-analysis of the relation between ADHD and working
memory, Martinussen et al. (2005) suggest that children with ADHD exhibit deficits in multiple
component of working memory, including verbal storage (effect size = 0.47) and verbal working
memory requiring manipulation (effect size = 0.43). Neuroimaging research has also
demonstrated that during task conditions requiring and increase in working memory, children

23
and adolescents with ADHD exhibit greater and more varied prefrontal cortex activation
compared to age-matched control participants (Rypma & D’Esposito, 2000; Sheridan, Hinshaw,
& D’Esposito, 2007).
2.3.4 Wisconsin Selective Reminding Test of Memory (WSRTM; Newby, 1999).
The examiner reads a word list, and children repeat all words remembered. The examiner
then repeats only the words missed on the previous trial and asks participants to repeat all words
recalled, including words recalled on the previous trial. This selective reminding continues until
the word list is completely recalled for two consecutive trials or until all ten trials are completed.
Words that are recalled without immediate reminding for two or more trials are assumed to have
entered long-term memory storage. The consistency of retrieval of words that have entered long-
term storage is also measured over successive trials. Four equivalent alternate forms were used,
and long-term storage and consistent long-term retrieval were analyzed in this study. The
alternate lists were found to be equivalent on frequency of occurrence in written English,
imagery, concreteness, and meaningfulness (all overall F-ratios and all pairwise t-tests > .05)
(Newby, 1999). Literature on similar selective reminding tests suggests minimal practice effects,
and increasing performance with age, especially in children (Spreen & Strauss, 1998). The
SRTM has been used in previous research on ADHD (Barkley, Anastopoulos, Guevremont, &
Fletcher, 1991), with equivocal effects of stimulants on SRTM noted in some studies (Barkley,
DuPaul, & McMurray, 1991; Hoeppner et al., 1997), but in others MPH response has been
positive for long-term storage and consistent long-term retrieval (Barkley, McMurray,
Edelbrock, & Robbins, 1989; Evans, Gualtieri, & Amara, 1986).

24
2.3.5 Trail Making Test–Part B (TMT-B; Reitan & Wolfson, 1985).
The Trail Making Test (TMT) is one of the most popular neuropsychological tests,
providing information on visual search, scanning, processing speed, and mental flexibility
(Tombaugh, 2004). Part B requires participants to shift between numbers and letters in ascending
order (i.e. 1-A-2-B). With Part A and Part B correlating only .49 with each other, research
suggests that the two alternate forms measure different functions, with Part B including more
visual interference and requiring more visual-perceptual processing ability than Part A
(Heilbronner et al., 1991).With alternate forms constructed by Hale (1997), only Part B was
utilized for the purposes of this study, as it has been found to be closely related to other tests of
timed executive function, suggesting that it measures frontal lobe dysfunction (Libon et al.,
1994). Both completion time and errors are recorded, with completion time used as a measure of
“cool” EWM functioning, and errors used as a measure of “hot” SR functioning. Meta-analyses
have found that TMT-B completion time can discriminate between children with ADHD and
controls (effect size range 0.55 to 0.75) (Pennington & Ozonoff, 1996; Willcutt et al., 2005), and
research suggests that TMT-B errors are sensitive to frontal-executive impairment (Hale et al.,
2009; Stuss et al., 2001). Interrater reliability for TMT-B has been reported as .90 (Fals-Stewart,
1991), and although some practice effects have been noted, these were found only for Part A,
and not for Part B (Lezak, 1995).
2.3.6 Conners’ Continuous Performance Test–II (CPT-II; Conners & MHS Staff, 2004).
This computerized continuous performance test requires sustained attention to visually
presented stimuli on a computer screen. The child watches the screen and responds each time a
letter appears (non-target stimulus) with the exception of one letter (target stimulus) for which no

25
response is required. Omissions were used as a measure of “cool” EWM functioning, and
commissions were used as a measure of “hot” SR functioning. Split-half reliability is .83 for
commission, and .94 for omissions, whereas test-retest reliability was found to be .65 (p < .01)
for commissions and .84 (p < .01) for omissions. The test-retest data suggests that the CPT-II is
relatively unaffected by practice effects, and all of the CPT measures used in this study yielded
non-significant p-values in a pre-post analysis designed to measure systematic improvement or
decline in performance over repeated administrations (Conners & MHS Staff, 2004). Meta-
analyses have found that stimulant medication improves CPT performance for both control
subjects and ADHD populations (Riccio et al., 2001), with CPT Omission errors consistently
producing the most significant differences between groups with and without ADHD (Willcutt et
al., 2005). Computerized CPT Omission measures have also been found to be sensitive to ADHD
medication response (Hale et al., 2005; Willcutt et al., 2005). A recent meta-analytic review
revealed large effect sizes for number of commissions (0.98), omissions (1.34), and variability in
response times (0.61) between children with ADHD and controls, suggesting that children with
ADHD committed more errors and had slower and/or more variable reaction times than controls
without ADHD. Performance over time effects were more moderate for all variables and the
authors suggested that these differences could be attributed entirely to sampling errors (Huang-
Pollock et al., 2012). Thus, for the purposes of this study we decided to focus on the most
consistent findings with CPT use in the ADHD population, and focus on commission and
omission errors.

26
2.3.7 Hale-Denckla Cancellation Test (HDCT; Hale, 1997).
This paper and pencil continuous performance test requires participants to cross out the
target stimulus embedded in a group of distractor stimuli. It is a measure of visual attention,
discrimination, scanning, tracking, memory, and graphomotor speed. Completion time and
number correct out of 30 is recorded. The HDCT is an adaptation and extension of the
Cancellation of Rapidly Reoccurring Target Figures Test (Rudel, Denckla, & Broman, 1978).
The HDCT has been found to discriminate children with ADHD from controls and children with
SLD, and was found to be sensitive to medication dose-response relationships in previous
ADHD research (Hale et al., 1998, 2005, 2006, Hoeppner et al., 1997). Previous research also
suggests that children with ADHD make more omission and commission errors on cancellation
tasks, suggesting that cancellation tasks measure aspects of executive attention (Fischer, Barkley,
Smallish, & Fletcher, 2005; Woods & Mark, 2007).

27
Chapter 3: Results
3.1 Overview
A repeated-measures MANOVA was computed for each of the seven neuropsychological
variables to determine individual response, with Drug Condition (B, P, L, H) serving as the
within-subjects factor and Impairment Level (N/A, Low, Moderate, High), based on Hale et al.
(2005), serving as the between-subjects factor. The results for each of the variables are presented
in Table 1 and graphically depicted in Figure 2. A summary of means, standard deviations, and
dose-response relationships for the individual tests can be found in Appendices 1 and 2.
Table 1 provides a breakdown of the frontal-subcortical circuit (dorsolateral-dorsal
cingulate [“cool”] and orbital-ventral cingulate [“hot]) that each of the neuropsychological tests
used in this study are hypothesized to reflect, according to the model developed by Hale at al.
(2005). The F-statistic and p-value associated with the repeated-measures MANOVAs for test
performance was broken down into each of the four Impairment groups (N/A, Low, Moderate,
and High). The post-hoc column specifically identifies the test scores that differed significantly
from one another across Drug conditions (B, P, L, H) at each Impairment group level. For
example, looking at the TOMAL-DB test, children with no apparent (N/A) baseline impairment
showed no significant test performance differences across the four drug conditions. However,
children with Low baseline executive impairment had Baseline (identified with a “1”) test
performances that were significantly lower than both the Placebo (identified with a superscripted
“b”) and the High dose (identified with a superscripted “d”) Drug Conditions.

28
Table 1. MPH Dose-Response Relationships for EWM/SR Impairment Groups for Individual Tests “Cool” Circuit Tests
“Hot” Circuit Tests F
F
p
p
Post-Hoc
Post-Hoc
F p
p
Post-Hoc
Post-Hoc TOMAL-DB
TOMAL-DB
Go No-Go
Go No-Go N/A 1.79 .266 N/S N/A 2.09 .220 N/S Low 6.04 .004 1bd Low 12.05 <.001 1bcd;2d Moderate 4.68 .022 1c Moderate 19.33 <.001 1bcd High 4.21 .029 1c;2cd High 10.32 .006 1bcd;2cd
Stroop Word Stroop Errors N/A 6.19 .039 1bcd
N/A 1.03 .453 N/S Low 8.94 <.001 1bcd;2d;3d Low 13.89 <.001 3a;4abc Moderate 19.93 <.001 1bcd Moderate 6.81 .006 3ab;4ab High 3.30 .088 1cd High 4.26 .035 3ab;4a
Trails Time Trails Errors N/A 1.48 .266 N/S N/A .64 .624 N/S Low 9.39 <.001 2a;3a;4a Low 3.97 .026 3b;4b Moderate 14.85 <.001 2a;3a;4a Moderate 6.86 .006 3a;4a High 3.14 .105 3bd High 9.18 .008 3ab;4ab
CPT Omissions CPT Commissions N/A 3.13 .126 4ab N/A .483 .708 N/S Low 6.61 .001 2a;3ab;4a Low 4.45 .018 3a;4a Moderate 6.64 .007 2a;3ab;4ab Moderate 2.49 .111 3ab;4c High 4.16 .065 3a High 1.83 .229 3a;4a
WSRTM HDCT N/A 1.59 .243 N/S N/A .725 .579 N/S Low 4.30 .015 1cd Low 1.61 .207 N/S Moderate 4.94 .019 1bcd Moderate 5.75 .011 1bcd High 8.82 .009 1bcd High 14.78 .002 1bcd;2cd Note. First published in [Postgraduate Medicine, 124(5), 2012, doi:10.3810/pgm.2012.09.2592]
© Postgraduate Medicine, a division of JTE Multimedia, LLC. N/S = not significant; N/A = no apparent baseline executive impairment (n = 8); Low = low baseline executive impairment (n = 20); Moderate = moderate baseline executive impairment (n = 15); High = high baseline executive impairment (n = 10); 1 = Baseline; 2 = Placebo; 3 = Low dose; 4 = High dose aLess than Baseline; bLess than Placebo; cLess than Low dose; dLess than High dose. Means and standard deviations of test performance for all measures across all conditions can be found in Appendices 1 and 2. CPT Commissions was not displayed in a graph as no relevant significant differences emerged.

29
Figure 3. Dose-Response Relationships for Neuropsychological Tests by Impairment Group. Note. First published in [Postgraduate Medicine, 124(5), 2012, doi:10.3810/pgm.2012.09.2592] © Postgraduate Medicine, a division of JTE Multimedia, LLC. No Apparent = No apparent baseline executive impairment (n = 8); Low = low baseline executive impairment (n = 20); Moderate = moderate baseline executive impairment (n = 15); High = high baseline executive impairment (n = 10). CPT Commissions was not displayed in a graph as no significant differences emerged.

30
3.2 Individual neuropsychological assessment measure results
The data were subjected to repeated measures MANOVA using Pillai’s Trace to
determine treatment effects. Mauchly Sphericity tests were used to determine whether a
multivariate or univariate approach to the data was warranted. Mauchly’s Test of Sphericity
assesses the null hypothesis that the error covariance matrix of the orthonormalized transformed
neuropsychological test performance was proportional to an identity matrix. Box’s M test for the
equality of covariance matrices was used to test the homogeneity of variance assumption, and
Levine’s Test of Equality of Error Variances was used to assess the null hypothesis that the error
variance of the neuropsychological test performance was equal across groups.
3.2.1 Go No-Go Test
Although Mauchly’s test of sphericity assumption for Drug was met (χ2(5) = 7.39, p =
.193), as was Levene’s test for the equality of error variances (p range .088 to .600), a
multivariate approach could not be completed due to an equality of covariance matrices violation
as determined by Box’s M test (F(30, 2,905.05) = 2.02, p = .001). Huynh-Feldt univariate tests
of within-subjects effects showed a highly significant Drug effect (F(3, 147) = 42.51, p < .001,
η2 = .47, power = 1.00), and Drug by Impairment Group interaction (F(9, 147) = 3.70, p < .001,
η2 = .19, power = .99). Tests of within-subjects orthogonal/polynomial contrasts revealed linear
and quadratic effects for both Drug and the Drug by Impairment interaction, suggesting that
dose-response curves were not uniform across conditions and impairment levels. A main effect
for the Impairment group (F(3, 49) = 4.59, p = .007, η2 = .22) was also observed, suggesting
significant group differences when collapsed across drug conditions.
31
With MANOVA results suggesting that test performance varied based on the level of
EWM/SR impairment, repeated-measures MANOVAs were then computed for each of the four
impairment groups separately. As indicated in Table 1, and depicted in Figure 2, post-hoc tests
revealed a significant medication response for the Low, Moderate, and High impairment groups,
with performance improving across Drug conditions.
3.2.2 Stroop Color-Word Test (Stroop)
For the Stroop test, we evaluated both the overall word score and the number of errors
made. For the overall word score, while Mauchly’s test of sphericity assumption for Drug was
met (χ2(5) = 7.40, p = .193), as was Levene’s test for the equality of error variances (p range
.211 to .979), a multivariate approach to the data could not be completed due to a violation of the
equality of covariance matrices as determined by Box’s M test (F(30, 2,905.05) = 1.56, p =
.028). While Huynh-Feldt univariate tests of within-subjects effects showed a highly significant
effect for Drug (F(3, 147) = 30.31, p < .001, η2 = .38, power = 1.00), the Drug by Impairment
Group interaction was not significant. Tests of within-subjects orthogonal/polynomial contrasts
revealed a quadratic effect for the Drug condition, suggesting that dose-response curves were not
uniform across conditions. There was also a main effect for Impairment group, (F(3, 49) = 12.91,
p < .001, η2 = .44), suggesting that there were group differences regardless of medication
condition. Post-hoc analyses presented in Table 1 revealed significant differences between Drug
conditions in all four Impairment conditions.
For Stroop errors, there were no violations of MANOVA assumptions, with Box’s M test
(F(30, 2,905.05) = 1.23, p = .183), Mauchly’s test of sphericity (χ2(5) = 10.60, p = .060), and
Levene’s test for the equality of error variances (p range .07 to .70) all nonsignificant. Using the

32
multivariate approach, Pillai’s Trace revealed a highly significant Drug effect (F(3, 47) = 17.14,
p < .001, η2 = .52, power = 1.00), and a significant Drug by Impairment Group interaction (F(9,
147) = 2.07, p = .036, η2 = .11, power = .85). Tests of within-subjects orthogonal/polynomial
contrasts revealed a linear effect for Drug and a cubic effect for the Drug by Impairment Group
Interaction indicating different response curves for different levels of impairment. However, no
main effect was found for Impairment Group. Post-hoc analyses reported in Table 1 revealed
significant Drug effects for the Low, Moderate, and High Impairment groups.
3.2.3 Test of Memory and Learning-Digits Backwards (TOMAL-DB)
For the TOMAL-DB test, a multivariate approach to the data could not be used as
Mauchly’s test of sphericity assumption for drug was violated (χ2(5) = 15.54, p = .008), as was
Levene’s test for the equality of error variances (p range .035 to .091), and the equality of
covariance matrices as determined by Box’s M test (F(30, 2,905.05) = 1.90, p = .002). Huynh-
Feldt univariate tests of within-subjects effects showed a highly significant effect for Drug (F(3,
147) = 10.46, p < .001, η2 = .18, power = 1.00), with the Drug by Impairment Group interaction
not reaching significance. Tests of within-subjects orthogonal/polynomial contrasts revealed a
linear and quadratic effect for Drug indicating that dose-response curves were not uniform across
conditions, which could suggest individual response curve differences. However, no main effect
was found for Impairment suggesting that there was no defining overall drug trial performance
pattern between impairment groups. As revealed in Table 1, post-hoc analyses revealed a
significant performance differences across Drug Conditions for the Low, Moderate, and High
Impairment groups.

33
3.2.4 Wisconsin Selective Reminding Test of Memory (WSRTM)
For the WSRTM, we looked at the storage-consistent retrieval ratio of task performance.
A multivariate approach to the data could not be used as Mauchly’s test of sphericity assumption
for drug was violated (χ2(5) = 15.20, p = .010), as was Levene’s test for the equality of error
variances (p range .025 to .855), and there was also a violation of the equality of covariance
matrices as determined by Box’s M test (F(30, 2,905.05) = 2.27, p < .001). Huynh-Feldt
univariate tests of within-subjects effects showed a highly significant effect for Drug (F(2.84,
139) = 16.24, p < .001, η2 = .25, power = 1.00); however, the Drug by Impairment group effect
was not significant. Tests of within-subjects orthogonal/polynomial contrasts revealed linear and
quadratic effects for Drug, suggesting that dose-response curves were not uniform across
conditions. However, no main effect for Impairment group (F(3, 49) = 0.55, p = .653, η2 = .03)
was found. Post-hoc analyses revealed a significant Drug effect for the Low, Moderate, and High
Impairment as depicted in Table 1.
3.2.5 Trail Making Test Part B (TMT-B)
For the TMT-B, analyses were conducted for the number of errors made and for total
completion time. Looking first at errors, while Mauchly’s test of sphericity assumption for drug
was not violated (χ2(5) = 7.31, p = .199) and there was also no violation of the equality of
covariance matrices (Box’s M test, F(30, 2,905.05) = 1.13, p = .291), a univariate approach was
required because of a violation in the equality of error variances according to Levene’s test (p
range .025 to .715). Huynh-Feldt univariate tests of within-subjects effects showed highly
significant Drug (F(3, 147) = 15.58, p < .001, η2 = .24, power = 1.00), and Drug by Impairment
interaction effects (F(9, 147) = 6.07, p < .001, η2 = .27, power = 1.00). Tests of within-subjects

34
orthogonal/polynomial contrasts revealed linear and cubic effects for Drug, and the Drug by
Impairment interaction, suggesting non-uniform dose-response curves across conditions.
Analyses also revealed a main effect for Impairment (F(3, 49) = 12.30, p < .001, η2 = .43).
Referring to Table 1, post-hoc analyses revealed a significant Drug effect for the Low, Moderate,
and High Impairment groups.
For TMT-B time, a multivariate approach to the data could not be used as Mauchly’s test
of sphericity assumption for drug was violated (χ2(5) = 132.95 p < .001) as was Levene’s test for
the equality of error variances (p range < .001 to .172), and there was also a violation of the
equality of covariance matrices as determined by Box’s M test (F(30, 2,905.05) = 5.35, p <
.001). Huynh-Feldt univariate tests of within-subjects effects showed a highly significant effect
for Drug (F(1.34, 147) = 10.89, p = .001, η2 = .18, power = .95). The Drug by Impairment group
interaction was also significant (F(4, 147) = 2.79, p = .034, η2 = .15, power = .73). Tests of
within-subjects orthogonal/polynomial contrasts revealed a linear and quadratic effect for Drug,
suggesting that dose-response curves were not uniform across conditions. There was also a main
effect for Impairment group (F(3, 49) = 6.93 p = .001, η2 = .30). Significant differences in
performance time were noted across Drug conditions for the Low, Moderate, and High
Impairment Groups during post-hoc analysis, as shown in Table 1.
3.2.6 Conners’ Continuous Performance Test-II (CPT-II)
For the CPT-II task we looked at both omission and commission errors made. Looking
first at omission errors, a multivariate approach to the data could not be used as Mauchly’s test of
sphericity assumption for drug was violated (χ2(5) = 84.62, p < .001) as was Levene’s test for the
equality of error variances (p range .006 to .205), and there was also a violation of the equality of

35
covariance matrices as determined by Box’s M test (F(30, 2,905.05) = 3.53, p < .001). Huynh-
Feldt univariate tests of within-subjects effects showed a highly significant effect for Drug
(F(1.61, 79) = 14.84, p < .001, η2 = .23, power = 1.00) and the Drug by Impairment group
interaction (F(4.83, 79) = 2.70, p = .028, η2 = .14, power = .78). For the Drug condition,
orthogonal/polynomial contrasts revealed both linear and quadratic effects suggesting varying
dose-response curves across conditions and groups. There was also a main effect for Impairment
group (F(3, 49) = 3.49, p = .023, η2 = .18). Post-hoc analyses revealed significant performance
differences across Drug conditions for each of the four Impairment levels, as indicated in Table
1.
For CPT-II commission errors, a multivariate approach to the data was used as Mauchly’s
test of sphericity assumption for drug was not violated (χ2(5) = 8.03, p = .155) neither was
Levene’s test for the equality of error variances (p range .060 to .126), and there was also no
violation of the equality of covariance matrices as determined by Box’s M test (F(30, 2,905.05)
= .88, p = .662). Although Pillai’s Trace multivariate tests showed a highly significant effect for
Drug (F(3, 47) = 6.21, p < .001, η2 = .28, power = .95), the interaction between Drug and
Impairment group was not significant. While tests of within-subjects orthogonal/polynomial
contrasts revealed a linear effect for Drug, suggesting that dose-response curves were not
uniform across conditions, no main effect for Impairment group was found. As outlined in Table
1, post-hoc analyses revealed a significant Drug effect for the Low, Moderate, and High
Impairment groups.

36
3.2.7 Hale–Denckla Cancellation Test (HDCT)
For the HDCT number of correct responses, although the equality of covariance matrices
assumption was not violated (Box’s M F(30, 2,905.05) = 1.25, p = .167), a multivariate approach
to the data could not be used as Mauchly’s test of sphericity assumption for Drug was violated
(χ2(5) = 23.37, p < .001) as was Levene’s test for the equality of error variances (p range < .001
to .677). Huynh-Feldt univariate tests of within-subjects effects showed a highly significant
effect for Drug (F(2.60, 147) = 27.89, p < .001, η2 = .36, power = 1.00) and for the interaction of
Drug and Impairment group (F(7.80, 147) = 6.14, p < .001, η2 = .27, power = 1.00). Tests of
within-subjects orthogonal/polynomial contrasts revealed a linear and quadratic effect for both
the Drug and the Drug by Impairment level interaction, suggesting that dose-response curves
were not uniform across conditions and impairment levels. A main effect for Impairment group
(F(3, 49) = 8.54, p < .001, η2 = .34), was also found, suggesting that there was a performance
pattern between impairment groups. Post-hoc analyses revealed a significant Drug effect for the
Moderate and High Impairment groups as outlined in Table 1.

37
Chapter 4: Discussion
4.1 Overview of findings
In the present study, children with behaviourally diagnosed ADHD underwent double-
blind placebo controlled MPH trials with cognitive/neuropsychological, data collected during
four different conditions (B, P, L, H) throughout the randomized controlled trial (RCT). Results
revealed highly significant MPH treatment effects with differences in performance emerging for
children based upon the structural equation modeling (SEM)-determined level of EWM/SR
impairment on a number of the cognitive/neuropsychological measures as depicted in Figure 3,
and summarized in Table 1 and Appendices 1 and 2. Orthogonal polynomial within-subjects
contrasts for Drug revealed that not all individuals had a uniform linear MPH response across
variables, with quadratic and cubic effects found. For those with no apparent (N/A) and low
baseline EWM/SR impairment, MPH response was often poor; while for those with moderate or
high baseline impairment, MPH response was often dramatic. In addition, differential cognitive
MPH response patterns emerged for those with moderate and high baseline impairment with
performance deteriorating on some measures at the higher medication dose.
Although statistically significant performance differences did not emerge between the
low dose and high dose Drug conditions for all of the tests, the graphs presented in Figure 2
suggest that performance began to deteriorate at the higher dosage for the Go No-Go, Stroop
errors, TOMAL-DB, HDCT errors, and the TMT-B errors and time, a trend that was especially
salient at Moderate and High levels of impairment. Furthermore, test performance for children
with N/A and Low baseline executive impairment showed minimal improvement across the Drug
conditions for the Go No-Go, Stroop word, TOMAL-DB, HDCT correct, and TMT-B time,
suggesting that children with minimal baseline executive impairment may not respond well to

38
stimulant medication – at least as measured by performance on these neuropsychological
measures.
4.2 Implications for “hot” and “cool” circuit executive functions
While a neurophysiological explanation for the differential cognitive MPH dose-response
relationships is beyond the scope and evidence provided here, some speculation appears to be
warranted given similar empirical findings (Arnsten, 2006; Berridge et al., 2006; Konrad et al.,
2004). As suggested earlier, it is possible that MPH has a differential effect on the “hot” (e.g.,
SR; orbital-ventral cingulate) and “cool” (e.g., EWM; dorsolateral-dorsal cingulate) frontal-
striatal-thalamic circuits (Castellanos et al., 2006; Kelly et al., 2007). The phylogenetically
younger “cool” dorsal circuits, necessary for deliberative executive processing, working
memory, and attention control, may respond best to low dose stimulants; while the
phylogenetically older “hot” ventral circuits, necessary for affective decision making, self-
regulation, and behavioural control, may respond best to high dose stimulants (Figner,
Mackinlay, Wilkening, & Weber, 2009; Roiser et al., 2009; Steinberg, 2008).
In this study, while most of the children with moderate to high baseline impairment
responded cognitively to stimulant medication, quadratic and/or cubic effects were observed with
the high MPH dose often resulting in deteriorating test performance. For example, inspection of
Go No-Go, TOMAL-DB, HDCT, and TMT-B test means (See Appendices 1 and 2) revealed
better performance on the lower MPH dosage. Additionally, the Stroop and TMT-B errors were
greater on the higher dosage, especially in the high impairment group. For those with ADHD and
high baseline impairment, the “cool” neuropsychological circuits appear to be optimized with
low dose stimulants with deterioration occurring with increased medication. With clinician focus

39
on behavioural criteria for ADHD diagnosis and for judging treatment response, affected
children may be receiving the correct dose for behavioural and self-regulatory control, but this in
turn may limit “cool” executive functions necessary for effective problem-solving and academic
learning.
4.3 Implications for academic achievement in ADHD
Using MPH to alleviate overt ADHD behavioural problems may be the preeminent
concern of parents and teachers, but the MPH RCT results presented here are consistent with the
cognitive and academic achievement MPH literature, suggesting that the best dose for cognition,
neuropsychological functioning, and academic achievement may be lower than the best dose for
behavioural control (Chacko et al., 2005; Hale et al., 2011; Pliszka et al., 2007; Teicher, Polcari,
& McGreenery, 2008). Although behaviour was not directly assessed for the purposes of this
study, previous research has found that MPH has a linear effect on behaviour – as measured by
behaviour rating scales – suggesting that increasing medication doses reduces problematic
behaviours (Hale et al., 2005; Hale et al., 2011). The differential dose-response relationships
reported here could explain why long-term treatment MPH efficacy remains limited in ADHD
(Jensen et al., 2007) and the inconsistent findings of MPH effects on academic achievement
(Langberg & Becker, 2012; Van der Oord et al., 2008). It is possible that by focusing our clinical
attention on the “hot” behavioural/self-regulation circuit for diagnosis and MPH titration, we are
limiting the long-term academic gains in many children with ADHD because higher medication
doses may result in deleterious cognitive and neuropsychological effects. If the optimal dose is
chosen solely on behavioural criteria, children will likely struggle with learning and academic

40
achievement because their “cool” dorsal executive and attention control/working memory
functions may be impaired as a result of (Berridge et al., 2006).
“Cool” dorsolateral-dorsal cingulate executive functions such as sustained attention,
flexible problem solving, fluid reasoning, and working memory are important predictors of
academic areas such as math reasoning, reading comprehension, written expression, higher level
implicit language, and reading, math, and writing fluency (Biederman et al., 2004; Decker, Hill,
& Dean, 2007; Denckla, 1996; Goldstein & Naglieri, 2008; Hale & Fiorello, 2004; Loe &
Feldman, 2007). However, concerns over whether measurement of these executive functions is
useful in ADHD diagnosis (Brown & LaRosa, 2002) has led to few protocols addressing these
neuropsychological-academic relationships in ADHD, especially in relation to judging MPH
treatment efficacy.
MPH titration that focuses on overt behaviour could increase short-term academic
compliance and performance gains (DuPaul & Stoner, 2004), but it is unlikely to produce long-
term academic treatment efficacy because neuropsychological functioning may be impaired in
children who appear to be receiving optimal titration given their behavioural concerns. However,
if medication titration was based on maximizing neuropsychological and academic functioning,
with concurrent behaviour therapy offered to reduce remaining problematic behaviours, perhaps
both academic and behavioural long-term improvements would be realized in children with
ADHD (Hale et al., 2009b; Hale et al., 2012).
4.4 Limitations
These findings should be evaluated in the context of several study limitations. Although
the sample largely consisted of children in grades one through five, children aged six to 16 were

41
included. Since ADHD developmental differences in neuropsychological and cognitive
functioning are well established (Barkley, 1997), future research should examine MPH effects on
test performance across age ranges. The sample size in this study was small, which likely limited
the reliability and power of results. Although baseline and placebo conditions partially guarded
against intelligence differences, future research should consider including a cognitive screening
of all children. Finally, the ratio of males to females is approximately 3-to-1 in community
ADHD samples, and as high as 9-to-1 in clinical ADHD samples (APA, 2000), so the current
sample is atypical for a clinical population.
4.5 Future research
Future research is needed to examine the long-term MPH effects on cognition and
academic performance in relation to levels of executive impairment and how these important
relationships are affected by differing medication dosages. Research examining
neuropsychological and behavioural MPH response over time will allow researchers to evaluate
how dosage and length of MPH treatment affects outcomes. Additionally, functional magnetic
resonance imaging (fMRI) and diffusor tensor imaging (DTI) research is needed to explore MPH
response in the different “hot” orbital-ventral cingulate and “cool” dorsolateral-dorsal cingulate
circuits and how this impacts SR and EWM respectively. This future empirical work may benefit
the field in determining whether MPH dose response curves differ for the circuits and ultimately
lead to better titration practices and outcomes for children with ADHD (Hale et al., 2011).
Future studies should consider the underlying differences between MPH treatment
responders and non-responders. A valuable question that arises from the present study is whether
children who are MPH non-responders truly have ADHD or if the symptoms of ADHD are the

42
result of other diagnoses (e.g., depression). Further increasing the heterogeneity of the disorder,
some research suggests that the current DSM-IV-TR diagnostic subtypes of ADHD miss a
constellation of symptoms described as “sluggish cognitive tempo” (SCT; Carlson, 1986). SCT
symptoms include hypoactivity, daydreaming, lethargy, limited alertness, and mental confusion,
with many researchers arguing that SCT is a distinct disorder of inattention (Garner, Marceaux,
Mrug, Patterson, & Hodgens, 2010; Harrington & Waldman, 2010; Jacobson et al., 2012) with
fewer EF deficits but higher rates of depression than DSM-IV-TR identified ADHD subgroups
(Barkley, 2012). Thus, future research should examine medication response across the different
ADHD subtypes, as some subtypes may be less responsive to medication than others (Hale et al.,
2009).

43
Chapter 5: Conclusion
Although the neurobiological basis of ADHD is well established, and ADHD is known to
affect the frontal-subcortical circuits responsible for executive function and self-regulation,
(Dickstein et al., 2006; Lichter & Cummings, 2001), it continues to be diagnosed primarily on
the basis of overt behaviour and indirect summative informant reports. Making diagnoses and
judging treatment efficacy on the basis of overt behavioural symptoms is problematic as ADHD
may also interfere with cognitive, neuropsychological, academic and social functioning across
multiple environments (Hale et al., 2009b; Hale et al., 2012). Further, most frontal-subcortical
circuit disorders lead to impaired attention (Lichter & Cummings, 2001), making differential
diagnosis difficult if only behavioural criteria are used (Hale et al., 2005).
Current behavioural diagnostic practices cannot address the neuropsychological
heterogeneity found in children diagnosed with ADHD, because behaviour ratings are based on
subjective interpretation of an individual’s behaviour rather than brain-behaviour relationships
(Hale et al., 2012). Although positive MPH treatment effects on behaviour are well established
(Abikoff et al., 2004; Pearson et al., 2004; Van der Oord et al., 2008, Waxmonsky et al., 2008)
and MPH can improve a child’s readiness for classroom learning (DuPaul & Stoner, 2004),
long-term MPH treatment efficacy remains elusive (Jensen et al., 2007). Although research
supporting the association between long-term ADHD medication use and improved standardized
achievement scores is emerging (Langberg & Becker, 2012), the clinical and educational utility
of these statistically significant achievement gains remains unclear. The relationship between
long-term medication use and school grades is also inconclusive with attenuated treatment
outcomes found in some ADHD samples and minimal, equivocal, or even untoward response in
certain individuals (Hale et al., 2011).

44
It is unclear how MPH ameliorates the EWM/SR deficits experienced in this
heterogeneous population because medication use and titration are typically based solely on
behavioural criteria. Focusing on overt behaviour rather than underlying executive deficits
experienced by children with ADHD may explain why MPH produces equivocal effects on long-
term academic success (Van der Oord, 2008), and the reason that long-term treatment efficacy of
stimulants remains limited in all areas (Jensen et al., 2007), especially since the best medication
dose for cognition may be lower than the best dose for behaviour (Goldstein & Naglierli, 2008;
Hale, Mulligan, & Simmerman, 2006; Hale et al., 1998, 2005, 2011; Hoeppner et al., 1997;
Reddy & Hale, 2007). Thus, a new clinical orientation and alternative training approach is
needed for physicians and other practitioners working with children with attention problems and
ADHD. Education is needed to help practitioners attend to the neuropsychological, academic,
and behavioural characteristics of affected children for differential diagnosis and optimization of
treatment outcomes.
The results from this study suggest that the current use of indirect and subjective
behavioural approaches for ADHD differential diagnosis and judgment of MPH treatment
efficacy need to be re-examined. Rather than focusing solely on behavioural criteria, future
research and clinical practice should include direct assessment of cognitive, neuropsychological,
academic, and behavioural functioning to ensure children referred for attention problems indeed
have “true” ADHD – at least the kind that responds to medication (Hale et al., 2009a). The RCT
results presented here not only have direct implications for ADHD differential diagnosis but also
for understanding MPH dose-response relationships in ADHD. As a result, children with ADHD
and other attention problems would benefit from interdisciplinary coordination of service
delivery (Hale & Fiorello, 2004) using multimodal, multi-method approaches to address their

45
diverse needs (DuPaul & Stoner, 2004). Physicians, psychologists, teachers, and parents can
enhance treatment outcomes through regular communication and coordination of service delivery
to determine the child’s response to MPH and other interventions. By examining MPH response
in relation to, and in combination with other interventions, interdisciplinary teams can optimize
the neuropsychological, academic, and behavioural functioning of children with ADHD.

46
References
Achenbach, T. M. (1991). Integrative guide for the 1991 CBCL/4–18, YSR, and TRF profiles.
Burlington, VT: University of Vermont, Department of Psychiatry.
Advokat, C. (2009). What exactly are the benefits of stimulants for ADHD? Journal of Attention
Disorders, 12(6), 495–498. doi:10.1177/1087054708329781
American Academy of Pediatrics, Subcommittee on Attention-Deficit/Hyperactivity Disorder,
Steering Committee on Quality Improvement and Management. (2011). ADHD: Clinical
practice guideline for the diagnosis, evaluation, and treatment of attention-
deficit/hyperactivity disorder in children and adolescents. Pediatrics, 128(5), 1–16.
doi:10.1542/peds.2011-2654
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders
(4th ed., Text Rev.). Washington, DC: Author.
Arnsten, A. F. (2006). Stimulants: Therapeutic actions in ADHD. Neuropsychopharmacology,
31, 2367–2383. doi:10.1038/sj.npp.1301164
Arnsten, A. F. T. (2009a). The emerging neurobiology of attention deficit hyperactivity disorder:
The key role of the prefrontal association cortex. Journal of Pediatrics, 154(5), I–S43.
doi:10.1016/j.jpeds.2009.01.018.
Arnsten, A. F. T. (2009b). Toward a new understanding of attention-deficit hyperactivity
disorder pathophysiology. CNS Drugs, 23(1, Supplement), 33–41. doi:1172-
7047/09/0001-0033
Arnsten, A. F. T., & Li, B. (2005). Neurobiology of executive functions: Catecholamine
influences on prefrontal cortical functions. Biological Psychiatry, 57(11), 1377–1384.
doi:10.1016/j.biopsych.2004.08.019

47
Arnsten, A. F. T., & Pliszka, S. R. (2011). Catecholamine influences on prefrontal cortical
function: Relevance to treatment of attention deficit/hyperactivity disorder and related
disorders. Pharmacology Biochemistry and Behavior, 99(2), 211–216.
doi:10.1016/j.pbb.2011.01.020
Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Weaver, A. L., & Jacobsen, S. J. (2007).
Modifiers of long-term school outcomes for children with attention-deficit/hyperactivity
disorder: Does treatment with stimulant medication make a difference? Results from a
population-based study. Journal of Developmental & Behavioral Pediatrics, 28(4), 274–
287. doi:10.1097/DBP.0b013e3180cabc28
Barkley, R. A. (1990). Attention-deficit hyperactivity disorder: A handbook for diagnosis and
treatment. New York, NY: Guilford.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions:
Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65–94.
doi:10.1037/0033-2909.121.1.65
Barkley, R. A. (2006a). Attention-deficit/hyperactivity disorder: A handbook for diagnosis and
treatment (3rd ed.). New York, NY: Guilford Press.
Barkley, R. A. (2006b). Attention-deficit/hyperactivity disorder. In D. A. Wolfe & E. J. Mash
(Eds.), Behavioral and emotional disorders in adolescents: Nature, assessment, and
treatment (pp. 91–152). New York, NY: Guilford Press.
Barkley, R. A. (2012). Distinguishing sluggish cognitive tempo from ADHD in children and
adolescents: Executive functioning, impairment, and comorbidity. Journal of Clinical
Child & Adolescent Psychology, 42(2), 161–173. doi:10.1080/15374416.2012.734259

48
Barkley, R. A., Anastopoulos, A. D., Guevremont, D. C., & Fletcher, K. E. (1991). Adolescents
with ADHD: patterns of behavioral adjustment, academic functioning, and treatment
utilization. Journal of the American Academy of Child & Adolescent Psychiatry, 30(5),
752-761.
Barkley, R. A., DuPaul, G. J., & McMurray, M. B. (1991). Attention deficit disorder with and
without hyperactivity: Clinical response to three dose levels of methylphenidate.
Pediatrics, 87, 519–531.
Barkley, R. A., McMurray, M. B., Edelbrock, C. S., & Robbins, K. (1989). The response of
aggressive and nonaggressive ADHD children to two doses of methylphenidate. Journal
of the American Academy of Child and Adolescent Psychiatry, 28(6), 873.
Berridge, C. W., & Devilbiss, D. M. (2011). Psychostimulants as cognitive enhancers: The
prefrontal cortex, catecholamines, and attention-deficit/hyperactivity disorder. Biological
Psychiatry, 69(12), e101–e111. doi:10.1016/j.biopsych.2010.06.023
Berridge, C. W., Devilbiss, D. M., Andrzejewski, M. E., Arnsten, A. F., Kelley, A. E.,
Schmeichel, . . . Spencer, R. C. (2006). Methylphenidate preferentially increases
catecholamine neurotransmission within prefrontal cortex at low doses that enhance
cognitive function. Biological Psychiatry, 60, 1111–1120.
doi:10.1016/j.biopsych.2006.04.022
Biederman, J., Faraone, S. V., & Lapey, K. (1992). Comorbidity of diagnosis in attention-deficit
hyperactivity disorder. In G. Weiss (Ed.), Child and adolescent psychiatry clinics of
North America: Attention deficit hyperactivity disorder (pp. 335–360). Philadelphia, PA:
Saunders.

49
Biederman, J., Monuteaux, M. C., Doyle, A. E., Seidman, L. J., Wilens, T. E., Ferraro, F., . . .
Faraone, S. V. (2004). Impact of executive function deficits and attention-
deficit/hyperactivity disorder (ADHD) on academic outcomes in children. Journal of
Consulting and Clinical Psychology, 72(5), 757–766. doi:10.1037/0022-006X.72.5.757
Brown, R. T., & La Rosa, A. (2002). Recent developments in the pharmacotherapy of attention-
deficit/hyperactivity disorder (ADHD). Professional Psychology, Research and Practice,
33(6), 591–595. doi:10.1037/0735-7028.33.6.591
Bush, G., Frazier, J. A., Rauch, S. L., Seidman, L. J., Whalen, P. J., Jenike, M. A., ... &
Biederman, J. (1999). Anterior cingulate cortex dysfunction in attention-
deficit/hyperactivity disorder revealed by fMRI and the Counting Stroop. Biological
psychiatry, 45(12), 1542–1552.
Carlson, C. L. (1986). Attention deficit disorder with and without hyperactivity: A review of
preliminary experimental evidence. In B. B. Lahey & A. E. Kazdin (Eds.), Advances in
clinical child psychology (Vol. 9, pp. 153–175). New York, NY: Plenum.
Casey, B. J., Trainor, R. J., Orendi, J. L., Schubert, A. B., Nystrom, L. E., Giedd, J. N., ... &
Rapoport, J. L. (1997). A developmental functional MRI study of prefrontal activation
during performance of a go-no-go task. Journal of Cognitive Neuroscience, 9(6), 835–
847.
Castellanos, F.X., & Tannock, R. (2002). Neuroscience of attention-deficit/hyperactivity
disorder: The search for endophenotypes. Nature Reviews Neuroscience, 3, 617–628.
doi:10.1038/nrn896

50
Castellanos, F. X., Patti, P. L., Sharp, W., Jeffries, N. O., Greestein, D. K., Clasen, L. S., . . .
Rapoport, J. L. (2002). Developmental trajectories of brain volume abnormalities in
children and adolescents with attention-deficit/hyperactivity disorder. Journal of the
American Medical Association, 288(14), 1740–1748. doi:10.1001/jama.288.14.1740.
Castellanos, F. X., Sonuga-Barke, E. J. S., Milham, M. P., & Tannock, R. (2006). Characterizing
cognition in ADHD: Beyond executive dysfunction. Trends in Cognitive Sciences, 10(3),
117–123. doi:10.1016/j.tics.2006.01.011
Chacko, A., Pelham, W. E., Gnagy, E. M., Greiner, A., Vallano, G., Bukstein, O., & Rancurello,
M. (2005). Stimulant medication effects in a summer treatment program among young
children with attention-deficit/hyperactivity disorder. Journal of the American Academy
of Child and Adolescent Psychiatry, 44(3), 249–257. doi:10.1097/00004583-200503000-
00009
Conners, C. K. (1997). Conners’ Rating Scales–Revised: Long Form. North Tonawanda, NY:
Multi-Heath Systems.
Conners, C. K. (2002). Forty years of methylphenidate treatment in attention-
deficit/hyperactivity disorder. Journal of Attention Disorders, 6, S17–S30.
Conners, K., & MHS Staff. (2004). Conners’ Continuous Performance Test–II user’s manual.
Toronto, Canada: Multi-Health Systems.
Connor, D. F. (2006). Stimulants. In R. A. Barkley (Ed.), Attention deficit hyperactivity disorder:
A handbook for diagnosis and treatment (3rd ed, pp. 608–648). New York, NY: Guilford
Press.
Corkum, P., McGonnell, M., & Schachar, R. (2010). Factors affecting academic achievement in
children with ADHD. Journal of Applied Research on Learning, 3(Article 9), 1–14.

51
Decker, S. L., Hill, S. K., & Dean, R. S. (2007). Evidence of construct similarity in executive
functions and fluid reasoning abilities. International Journal of Neuroscience, 117(6),
735–748. doi:10.1080/00207450600910085
Denckla, M. B. (1996). Biological correlates of learning and attention: what is relevant to
learning disability and attention-deficit hyperactivity disorder? Journal of Developmental
& Behavioral Pediatrics, 17(2), 114–119.
DeVito, E. E., Blackwell, A. D., Kent, L., Ersche, K. D., Clark, L., Salmond, C. H., . . .
Sahakian, B. J. (2008). The effects of methylphenidate on decision making in attention-
deficit/hyperactivity disorder. Biological Psychiatry, 64, 636–639.
doi:10.1016/j.biopsych.2008.04.017
Dickstein, S. G., Bannon, K., Castellanos, F. X., & Milham, M. P. (2006). The neural correlates
of attention deficit hyperactivity disorder: An ALE meta-analysis. Journal of Child
Psychology and Psychiatry, 47(10), 1051–1062. doi:10.1111/j.1469-7610.2006.01671.x
Douglas, V. I., Barr, R. G., Desilets, J., & Sherman, E. (1995). Do high doses of stimulants
impair flexible thinking in attention-deficit hyperactivity disorder? Journal of the
American Academy of Child and Adolescent Psychiatry, 34(7), 879–885.
DuPaul, G. J., & Barkley, R. A. (1992). Situational variability of attention problems:
Psychometric properties of the Revised Home and School Situations Questionnaires.
Journal of Clinical Child Psychology, 21, 178–188. doi:10.1207/s15374424jccp2102_10
DuPaul, G. J., Rapport, M. D., & Perriello, L. M. (1991). Teacher ratings of academic skills: The
development of the Academic Performance Rating Scale. School Psychology Review,
20(2), 284–300.

52
DuPaul, G. J., & Stoner, G. (2004). ADHD in the schools: Assessment and intervention
strategies (2nd ed.). New York, NY: Guilford.
Durston, S., Tottenham, N. T., Thomas, K. M., Davidson, M. C., Eigsti, I., Yang, Y., . . . Casey,
B. J. (2003). Differential patterns of striatal activation in young children with and without
ADHD. Biological Psychiatry, 53(10), 871–878.
Engert, V., & Pruessner, J. C. (2008). Dopaminergic and noradrenergic contributions to
functionality in ADHD: The role of methylphenidate. Current Neuropharmacology, 6(4),
322–328. doi:10.2174/157015908787386069
Evans, R. W., Gualtieri, C. T., & Amara, I. (1986). Methylphenidate and memory: dissociated
effects in hyperactive children. Psychopharmacology, 90(2), 211–216.
Evans, S. W., Pelham, W. E., Smith, B. H., Bukstein, O., Gnagy, E. M., Greiner, A. R., . . .
Baron-Myak, C. (2001). Does-response effects of methylphenidate on ecologically valid
measures of academic performance and classroom behavior in adolescents with ADHD.
Experimental and Clinical Psychopharmacology, 9, 163–175. doi:10.1037//1064-
1297.9.2.163
Fabiano, G. A., Pelham, Jr., W. E., Coles, E. K., Gnagy, E. M., Chronis-Tuscano, A., &
O’Connor, B. C. (2009). A meta-analysis of behavioural treatments for attention-deficit/
hyperactivity disorder. Clinical Psychology Review, 29, 129–140.
doi:10.1016/j.cpr.2008.11.001
Figner, B., Mackinlay, R., Wilkening, F., & Weber, E. (2009). Affective and deliberative
processes in risky choice: Age differences in risk taking in the Columbia Card Task.
Journal of Experimental Psychology: Learning, Memory, and Cognition, 35(3), 709–
730. doi:10.1037/a0014983

53
Fischer, M., Barkley, R. A., Smallish, L., & Fletcher, K. (2005). Executive functioning in
hyperactive children as young adults: attention, inhibition, response perseveration, and
the impact of comorbidity. Developmental Neuropsychology, 27(1), 107–133.
Floresco, S. B., & Magyar, O. (2006). Mesocortical dopamine modulation of executive
functions: Beyond working memory. Psychopharmacology, 188, 567–585.
doi:10.1007/s00213-006-0404-5
Garner, A. A., Marceaux, J. C., Mrug, S., Patterson, C., & Hodgens, B. (2010). Dimensions and
correlates of attention deficit/hyperactivity disorder and sluggish cognitive tempo.
Journal of Abnormal Child Psychology, 38, 1097–1107. doi:10.1007/s10802-010-943-8
Golden, J. C. (1978). Stroop Color and Word Test. Chicago, IL: Stoelting.
Goldstein, S., & Naglieri, J. (2008). The school neuropsychology of ADHD: Theory, assessment,
and intervention. Psychology in the Schools, 45(9), 859-874.
Greenhill, L. L., Swanson, J. M., Vitiello, B., Davies, M., Clevenger, W., Wu, M., . . . Wigal, T.
(2001). Impairment and deportment responses to different methylphenidate doses in
children with ADHD: The MTA titration trial. Journal of the American Academy of Child
and Adolescent Psychiatry, 40, 180–187. doi:10.1097/00004583-200102000-00012
Evans, R. W., Gualtieri, C. T., & Amara, I. (1986). Methylphenidate and memory: Dissociated
effects in hyperactive children. Psychopharmacology, 90, 211-216.
Hale, J. B. (1997). Development of alternate forms of the Hale Cancellation Task and Trail-
Making Test for use in ADHD medication trials. Unpublished manuscript, Rochester
Institute of Technology.
Hale, J. B., & Fiorello, C. A. (2004). School neuropsychology: A practitioner’s handbook. New
York, NY: Guilford.

54
Hale, J. B., Fiorello, C. A., & Brown, L. (2005). Determining medication treatment effects using
teacher ratings and classroom observations of children with ADHD: Does
neuropsychological impairment matter? Educational and Child Psychology, 22, 39–61.
Hale, J. B., Hoeppner, J. B., DeWitt, M. B., Coury, D. L., Ritacco, D. G., & Trommer, B. (1998).
Evaluating medication response in ADHD. Journal of Learning Disabilities, 31(6), 595–
607. doi:10.1177/002221949803100610
Hale, J. B., Mulligan, C. A., & Simmerman, K. L. (2006, February). Quantifying medication
response in ADHD: Does neuropsychological impairment matter? Poster presentation at
the 34th Annual Meeting of the International Neuropsychological Society, Boston, MA.
Hale, J. B., Reddy, L. A., Decker, S. L., Thompson, R., Henzel, J., Teodori, A., . . . Denckla, M.
B. (2009a). Development and validation of an executive function and behavior rating
screening battery sensitive to ADHD. Journal of Clinical and Experimental
Neuropsychology, 1, 1–16. doi:10.1080/13803390802687423
Hale, J. B., Reddy, L. A., Semrud-Clikeman, M., Hain, L. A., Whitaker, J., Morely, J., . . . Jones,
N. (2011). Executive impairment determines ADHD medication response: Implications
for academic achievement. Journal of Learning Disabilities, 44(2), 196–212.
doi:10.1177/0022219410391191
Hale, J. B., Reddy, L. A., Wilcox, G., McLaughlin, A., Hain, L., Stern, A., . . . Eusebio, E.
(2009b). Assessment and intervention for children with ADHD and other frontal-striatal
circuit disorders. In D. C. Miller (Ed.), Best practices in school neuropsychology:
Guidelines for effective practice, assessment and evidence-based interventions (pp. 225–
280). New York, NY: John Wiley.

55
Hale, J. B., Yim, M., Schneider, A. N., Wilcox, G., Henzel, J. N., & Dixon, S. G. (2012).
Cognitive and neuropsychological assessment of ADHD: Redefining a disruptive
behavior disorder. In D. P. Flanagan & P. Harrison (Eds.), Contemporary intellectual
assessment: Theories, tests, and issues (3rd ed., pp. 687–707). New York, NY: Guilford
Press.
Hansen, D. L., & Hansen, E. H. (2006). Caught in a balancing act: Parents’ dilemmas regarding
their ADHD child’s treatment with stimulant medication. Qualitative Health Research,
16, 1267–1285. doi:10.1177/1049732306292543
Harrington, K. M. & Waldman, I. D. (2010). Evaluating the utility of sluggish cognitive tempo
in discriminating among DSM-IV ADHD subtypes. Journal of Abnormal Child
Psychology, 38, 173–185. doi:10.1007/s10802-009-9355-8
Heilbronner, R. L., Henry, G. K., Buck, P., Adams, R. L., & Fogle, T. (1991). Lateralized brain
damage and performance on trail making A and B, digit span forward and backward, and
TPT memory and location. Archives of Clinical Neuropsychology, 6(4), 251–258.
Hoeppner, J. B., Hale, J. B., Bradley, A. M., Byrnes, M., Coury, D. L., Lennie, L., & Trommer,
B. L. (1997). A clinical protocol for determining methylphenidate dosage levels in
ADHD. Journal of Attention Disorders, 2, 19–30. doi:10.1177/108705479700200102
Homack, S., & Riccio, C. A. (2004). A meta-analysis of the sensitivity and specificity of the
Stroop Color and Word Test with children. Archives of Clinical Neuropsychology, 19(6),
725–743.

56
Hood, J., Baird, G., Rankin, P. M., & Isaacs, E. (2005). Immediate effects of methylphenidate on
cognitive attention skills of children with attention-deficit/hyperactivity disorder.
Developmental Medicine & Child Neurology, 47(6), 408–414. doi:10.1111/j.1469-
8749.2005.tb01162.x
Huang-Pollock, C. L., Karalunas, S. L., Tam, H., & Moore, A. N. (2012). Evaluating vigilance
deficits in ADHD: A meta-analysis of CPT performance. Journal of Abnormal
Psychology, 121(2), 360–371.
Isles, A. R., & Humby, T. (2006). Modes of imprinted gene action in learning disability. Journal
of Intellectual Disability Research, 50(5), 318–325. doi:10.1111/j.1365-
2788.2006.00843.x
Jacobson, L. A., Murphy-Bowman, S. C., Pritchard, A. E., Tart-Zelvin, A., Zabel, T. A., &
Mahone, E. M. (2012). Factor structure of a sluggish cognitive tempo scale in clinically-
referred children. Journal of Abnormal Child Psychology, 40(8), 1327–1337.
doi:10.1007=s10802-012-9643-6
Jensen, P. S., Arnold, L. E., Swanson, J. M., Vitiello, B., Abikoff, H. B., Greenhill, L. L. . . .
Hur, K. (2007). 3-year follow up of the NIMH MTA study. Journal of the American
Academy of Child and Adolescent Psychiatry, 46, 989–1002.
doi:10.I097lchi.0b0r3e3I80686d48
Kelly, C., Sonuga-Barke, E. J. S., Scheres, A., & Castellanos, F. X. (2007). Functional
neuroimaging of the reward and motivational pathway in ADHD. In M. Fitzgerald, M.
Bellgrove, & M. Gill (Eds.), Handbook of attention deficit hyperactivity disorder (pp.
209–235). Hoboken, NJ: John Wiley & Sons.

57
Kemner, C., Jonkman, L. M., Kenemans, J. L., Bocker, K. B., Verbaten, M. N., & Engeland, H.
(2004). Sources of auditory selective attention and the effects of methylphenidate in
children with attention-deficit/hyperactivity disorder. Biological Psychiatry, 55, 776–778.
doi:10.1016/j.biopsych.2003.12.007
Kobel, M., Bechtel, N., Weber, P., Specht, K., Klarhofer, M., Scheffler, K., . . . Penner, I. K.
(2008). Effects of methylphenidate on working memory functioning in children with
attention deficit/hyperactivity disorder. European Journal of Paediatric Neurology, 13,
516–523. doi:10.1016/j.ejpn.2008.10.008
Konrad, K., Gunther, T., Hanisch, C., & Herpertz-Dahlmann, B. (2004). Differential effects of
methylphenidate on attentional functions in children with attention-deficit/hyperactivity
disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 43(2),
191–198. doi:10.1097/00004583-200402000-00015
Kuczenski, R., & Segal, D. S. (1992). Regional norepinephrine response to amphetamine using
dialysis: comparison with caudate dopamine. Synapse, 11(2), 164–169.
Kuhle, H., Kinkebur, J., Andes, K., Heidorn, F., Zeyer, S., Rautzenberg, P., . . . Jansen, F.
(2007). Self-regulation of visual attention and facial expression of emotions in ADHD
children. Journal of Attention Disorders, 10(4), 350–358.
doi:10.1177/1087054706289944
Langberg, J. M., & Becker, S. P. (2012). Does long-term medication use improve the academic
outcomes of youth with attention-deficit/hyperactivity disorder? Clinical Child and
Family Psychology Review, 15(3), 215–233. doi:10.1007/s10567-012-0117-8

58
Langleben, D. D., Monterosso, L., Elman, I., Ash, B., Krikorian, G., & Austin, G. (2006).
Effects of methylphenidate on Stroop Color-Word task performance in children with
attention-deficit/ hyperactivity disorder. Psychiatry Research, 141, 315–320.
doi:10.1016/j.psychres.2005.09.007
Lezak, M. D. (Ed.). (1995). Neuropsychological assessment (3rd ed.). New York, NY: Oxford
University Press.
Li, D., Sham, P. K., Owen, M. J., & He, L. (2006). Meta-analysis shows significant association
between dopamine system genes and attention deficit hyperactivity disorder (ADHD).
Human Molecular Genetics, 15(14), 2276–2284. doi:10.1093/hmg/ddl152
Libon, D. J., Glosser, G., Malamut, B. L., Kaplan, E., Goldberg, E., Swenson, R., & Prouty
Sands, L. (1994). Age, executive functions, and visuospatial functioning in healthy older
adults. Neuropsychology, 8(1), 38–43. doi:10.1037/0894-4105.8.1.38
Lichter, D. G., & Cummings, J. L. (Eds.). (2001). Frontal-subcortical circuits in psychiatric and
neurological disorders. New York, NY: Guilford.
Loe, I. M., & Feldman, H. M. (2007). Academic and educational outcomes of children with
ADHD. Ambulatory Pediatrics, 7, 82–90. doi:10.1093/jpepsy/jsl054
Manor, I., Meidad, S. Zalsman, G., Zemishlany, Z., Tyano, S., & Weizman, A. (2008). Objective
versus subjective assessment of methylphenidate response. Child Psychiatry and Human
Development, 39, 273–282. doi:10.1007/s10578-007-0087-0
Martinussen, R., Hayden, J., Hogg-Johnson, S., & Tannock, R. (2005). A meta-analysis of
working memory impairments in children with attention-deficit/hyperactive disorder.
Journal of the American Academy of Child and Adolescent Psychiatry, 44, 377–384.
doi:10.1097/01.chi.0000153228.72591.73

59
May, R. B., Masson, M. E. J., Hunter, M. A., & Wells, J. (1990). NPStat 3.01 [Computer
software]. Victoria, Canada: University of Victoria.
Molina, B. S. G., Hinshaw, S. P., Swanson, J. M., Arnold, L. E., Vitiello, B., Jensen, P. S., . . .
Houck, P. R. (2009). The MTA at 8 years: Prospective follow-up of children treated for
combined-type ADHD in a multisite study. Journal of the American Academy of Child &
Adolescent Psychiatry, 48(5), 484–500. doi:10.1097/CHI.0b013e31819c23d0
The MTA Cooperative Group. (1999). A 14-month randomized clinical trial of treatment
strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry,
56(12), 1073–1086. doi:10.1001/archpsyc.56.12.1073
Newby, R. F. (1999). Wisconsin Selective Reminding Test. Milwaukee, WI: Medical College of
Wisconsin.
Nigg, J. T. (2001). Is ADHD a disinhibitory disorder? Psychological Bulletin, 127(5), 571–598. Nigg, J. T., Willcutt, E. G., Doyle, A. E., & Sonuga-Barke, E. J. S. (2005). Causal heterogeneity
in attention-deficit/hyperactivity disorder: Do we need neuropsychologically impaired
subtypes? Biological Psychiatry, 57(11), 1224–1230.
doi:10.1016/j.biopsych.2004.08.025
Pearson, D. A., Santos, C. W., Casat, C. D., Lane, D. M., Jerger, S. W., Roache, J. D., . . .
Cleveland, L. A. (2004). Treatment effects of methylphenidate on cognitive functioning
in children with mental retardation and ADHD. Journal of the American Academy of
Child & Adolescent Psychiatry, 43(6), 677–685.
doi:10.1097/01.chi.0000124461.81324.13

60
Pearson, D. A., Santos, C. W., Roache, J. D., Casat, C. D., Loveland, K. A., Lachar, D., . . .
Cleveland, L. A. (2003). Treatment effects of methylphenidate on behavioral adjustment
in children with mental retardation and ADHD. Journal of the American Academy of
Child and Adolescent Psychiatry, 42, 209–216.
doi:10.1097/01.CHI.0000037009.34553.36
Pelham, W. E., Gnagy, E. M., Burrows-Maclean, L., Williams, A., Fabiano, G. A., Morrisey, S.
M., . . . Morse, G. D. (2001). Once-a-day Concerta methylphenidate versus three-times-
daily methylphenidate in laboratory and natural settings. Pediatrics, 107, e105.
doi:10.1542/peds.107.6.e105
Pennington, B. F., & Ozonoff, S. (1996). Executive functions and developmental
psychopathology. Journal of Child Psychology and Psychiatry, 37, 51–87.
doi:10.1111/j.1469-7610.1996.tb01380.x
Pietrzak, R. H., Mollica, C. M., Maruff, P., & Snyder, P. J. (2006). Cognitive effects of
immediate-release methylphenidate in children with attention-deficit/hyperactivity
disorder. Neuroscience and Behavioral Reviews, 30(8), 1225–1245.
doi:10.1016/j.neubiorev.2006.10.002
Pliszka, S. R., Liotti, M., Bailey, B. Y., Perez, R., Glahn, D., & Semrud-Clikeman, M. (2007).
Electrophysiological effects of stimulant treatment on inhibitory control in children with
attention-deficit/hyperactivity disorder. Journal of Child and Adolescent
Psychopharmacology, 17, 356–366. doi:10.1089/cap.2006.0081
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The
worldwide prevalence of ADHD: A systematic review and metaregression analysis. The
American Journal of Psychiatry, 164, 942–948.

61
Powers, R. L., Marks, D. J., Miller, C. J., Newcorn, J. H., & Halperin, J. M. (2008). Stimulant
treatment in children with attention-deficit/hyperactivity disorder moderates adolescent
academic outcome. Journal of Child and Adolescent Psychopharmacology, 18(5), 449–
459. doi:10.1089/cap.2008.021
Raggi, V. L. & Chronis, A. M. (2006). Interventions to address the academic impairment of
children and adolescents with ADHD. Clinical Child and Family Psychology Review, 9,
85–111. doi:10.1007/s10567-006-0006-0
Rapport, M. D., Denney, C., DuPaul, G. J., & Gardner, M. J. (1994). Attention deficit disorder
and methylphenidate: Normalization rates, clinical effectiveness, and response prediction
in 76 children. Journal of the American Academy of Child & Adolescent Psychiatry,
33(6), 882–893. doi:10.1097/00004583-199407000-00015
Reddy, L. A., & Hale, J. B. (2007). Inattentiveness. In A. R. Eisen (Ed.), Treating childhood
behavioral and emotional disorders: A step-by-step evidence-based approach (pp. 156–
211). New York, NY: Guilford.
Reitan, R. M., & Wolfson, D. (1985). Neuroanatomy and neuropathology: A guide for
neuropsychologists. Tucson, AZ: Neuropsychology Press.
Reynolds, C. R., & Bigler, E. D. (1994). Test of memory and learning. Austin, TX: Pro-Ed.
Rhee, S. H., Willcutt, E. G., Hartman, C. A., Pennington, B. F., & DeFries, J. C. (2008) Test of
alternative hypotheses explaining the comorbidity between attention-deficit/hyperactivity
disorder and conduct disorder. Journal of Abnormal Child Psychology, 36, 29–40.
doi:10.1007/s10802-007-9157-9

62
Rhodes, S. M., Coghill, D. R., & Matthews, K. (2006). Acute neuropsychological effects of
methylphenidate in stimulant drug-naïve boys with ADHD II – broader executive and
non-executive domains. Journal of Child Psychology and Psychiatry, 47(11), 1184–1194.
doi:11 11/j.1469-7610.2006.01633.x.
Riccio, C. A., Waldrop, J. J., Reynolds, C. R., & Lowe, P. (2001). Effects of Stimulants on the
Continuous Performance Test (CPT) Implications for CPT Use and Interpretation. The
Journal of neuropsychiatry and clinical neurosciences, 13(3), 326–335.
Roiser, J. P., Cannon, D. M., Gandhi, S. K., Tavares, J. T., Erickson, K., Wood, S., . . . &
Drevets, W. C. (2009). Hot and cold cognition in unmedicated depressed subjects with
bipolar disorder. BipolarDdisorders, 11(2), 178–189. doi:10.1111/j.1399-
5618.2009.00669.x
Roth, R. M., & Saykin, A. J. (2004). Executive dysfunction in attention-deficit/hyperactivity
disorder: cognitive and neuroimaging findings. The Psychiatric Clinics of North America,
27(1), 83–96. doi:10.1016/S0193-953X(03)00112-6
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C., Simmons, A., & Bullmore,
E. T. (1999). Hypofrontality in attention deficit hyperactivity disorder during higher-
order motor control: a study with functional MRI. American Journal of Psychiatry,
156(6), 891–896.
Rubia, K., Smith, A. B., Brammer, M. J., Toone, B., & Taylor, E. (2005). Abnormal brain
activation during inhibition and error detection in medication-naive adolescents with
ADHD. American Journal of Psychiatry, 162(6), 1067–1075.
Rudel, R. G., Denckla, M. B., & Broman, M. (1978). Rapid silent response to repeated target
symbols by dyslexic and nondyslexic children. Brain and language, 6(1), 52–62.

63
Rypma, B., & D'Esposito, M. (2000). Isolating the neural mechanisms of age-related changes in
human working memory. Nature Neuroscience, 3(5), 509–515.
Scheffler, R. M., Brown, T. T., Fulton, B. D., Hinshaw, S. P., Levine, P., & Stone, S. (2009).
Positive association between attention-deficit/ hyperactivity disorder medication use and
academic achievement during elementary school. Pediatrics, 123, 1273–1279.
doi:10.1542/peds.2008-1597
Schulz, K. P., Fan, J., Magidina, O., Marks, D. J., Hahn, B., & Halperin, J. M. (2007). Does the
emotional go/no-go task really measure behavioral inhibition?: Convergence with
measures on a non-emotional analog. Archives of Clinical Neuropsychology, 22(2), 151–
160.
Semrud-Clikeman, M. (2005). Neuropsychological aspects for evaluating learning disabilities.
Journal of Learning Disabilities, 38(6), 563–568. doi:10.1177/00222194050380061301
Semrud-Clikeman, M., Pliszka, S., & Liotto, M. (2008). Executive functioning in children with
attention-deficit hyperactivity disorder: Combined type with and without a stimulant
medication history. Neuropsychology, 22(3), 329–340. doi:10.1037/0894-4105.22.3.329
Sergeant, J. A., Geurts, H., & Oosterlaan, J. (2002). How specific is a deficit of executive
functioning for attention-deficit/hyperactivity disorder? Behavioural Brain Research,
130, 3–28. doi:10.1016/S0166-4328(01)00430-2
Sheridan, M. A., Hinshaw, S., & D'ESPOSITO, M. A. R. K. (2007). Efficiency of the prefrontal
cortex during working memory in attention-deficit/hyperactivity disorder. Journal of the
American Academy of Child & Adolescent Psychiatry, 46(10), 1357–1366.

64
Solanto, M. V., Abikoff, H., Sonuga-Barke, E., Schachar, R., Logan, G., Wigal, T., . . . Turkel,
E. (2001). The ecological validity of delay aversion and response inhibition as measures
of impulsivity in AD/HD: A supplement to the NIMH Multi-Modal Treatment Study of
AD/HD. Journal of Abnormal Child Psychology, 29, 215–228.
doi:10.1023/A:1010329714819
Sonuga-Barke, E. J. S., Sergeant, J. A., Nigg, J., & Willcutt, E. (2008). Executive dysfunction
and delay aversion in attention deficit hyperactivity disorder: Nosologic and diagnostic
implications. Child and Adolescent Psychiatric Clinics of North America, 17(2), 367–
384. doi:10.1016/j.chc.2007.11.008
Van Mourik, R., Oosterlaan, J., & Sergeant, J. A. (2005). The Stroop revisited: A meta!analysis
of interference control in AD/HD. Journal of Child Psychology and Psychiatry, 46(2),
150–165.
Sprague, R. L., & Sleator, E. K. (1977). Methylphenidate in hyperkinetic children: Differences in
dose effects on learning and social behavior. Science, 198, 1274–1276.
doi:10.1126/science.337493
Steinberg, L. (2008). A social neuroscience perspective on adolescent risk-taking.
Developmental Review, 28(1), 78–106. doi:10.1016/j.dr.2007.08.002
Stuss, D. T., Bisschop, S. M., Alexander, M. P., Levine, B., Katz, D., & Izukawa, D. (2001). The
Trail Making Test: a study in focal lesion patients. Psychological Assessment, 13(2),
230–239. doi:10.1037/1040-3590.13.2.230
Swanson, J., Baler, R. D., & Volkow, N. D. (2011). Understanding the effects of stimulant
medications on cognition in individuals with attention-deficit hyperactivity disorder: A
decade of progress. Neuropsychopharmacology, 36, 207–226. doi:10.1038/npp.2010.160

65
Tamm, L., Menon, V., Ringel, J., & Reiss, A. L. (2004). Event-related FMRI evidence of
frontotemporal involvement in aberrant response inhibition and task switching in
attention-deficit/hyperactivity disorder. Journal of the American Academy of Child &
Adolescent Psychiatry, 43(11), 1430–1440.
Tannock, R., Schachar, R., & Logan, G. (1995). Methylphenidate and cognitive flexibility:
Dissociated dose effects in hyperactive children. Journal of Abnormal Child Psychology,
23(2), 235–266. doi:10.1007/BF01447091
Taylor, E. (2011). Antecedents of ADHD: A historical account of diagnostic concepts. Attention
Deficit and Hyperactivity Disorders, 3, 69–75. doi:10.1007/s12402-010-0051-x
Teicher, M. H., Polcari, A., & McGreenery, C. E. (2008). Utility of objective measures of
activity and attention in the assessment of therapeutic response to stimulants in children
with attention-deficit/hyperactivity disorder. Journal of Child and Adolescent
Psychopharmacology, 18(3), 265–270. doi:10.1089/cap.2007.0090
Thapar, A., Cooper, M., Eyre, O., & Langley, K. (2013). Practitioner Review: What have we
learnt about the causes of ADHD? Journal of Child Psychology and Psychiatry, 54(1), 3–
16. doi:10.1111/j.1469-7610.2012.02611.x
Tombaugh, T. N. (2004). Trail Making Test A and B: Normative data stratified by age and
education. Archives of Clinical Neuropsychology, 19(2), 203–214.
Trommer, B. L., Hoeppner, J. B., & Zecker, S. G. (1991). The go-no go test in attention deficit
disorder is sensitive to methylphenidate. Journal of Child Neurology, 6(Suppl.), S128–
S131. doi:10.1177/0883073891006001131

66
Vaidya, C. J. & Stollstroff, M. (2008). Cognitive neuroscience of attention deficit hyperactivity
disorder: Current status and working hypotheses. Developmental Disabilities Research
Reviews, 14, 261–267. doi:10.1002/ddrr.40
Vaidya, C. J., Austin, G., Kirkorian, G., Ridlehuber, H. W., Desmond, J. E., Glover, G. H., &
Gabrieli, J. D. (1998). Selective effects of methylphenidate in attention deficit
hyperactivity disorder: a functional magnetic resonance study. Proceedings of the
National Academy of Sciences, 95(24), 14494–14499.
Valera, E. M., Faraone, S. V., Murray, K. E., & Seidman, L. J. (2007). Meta-analysis of
structural imaging findings in attention-deficit/hyperactivity disorder. Biological
Psychiatry, 61(12), 1361–1369. doi:10.1016/j.biopsych.2006.06.011
Van der Oord, S., Prins, P. J., Oosterlaan, J., & Emmelkamp, P. M. (2008). Efficacy of
methylphenidate, psychosocial treatments and their combination in school-aged children
with ADHD: A meta-analysis. Clinical Psychology Review, 28, 783–800.
doi:10.1016/j.cpr.2007.10.007
Voeller, K. K. S. (2001). Attention-deficit/hyperactivity disorder as a frontal-subcortical
disorder. In D. G. Lichter & J. L. Cummings (Eds.), Frontal-subcortical circuits in
psychiatric and neurological disorders (pp. 334–371). New York, NY: Guilford Press.
Volkow, N. D., Wang, G-J., Fowler, J. S., Logan, J., Gerasimov, M., Maynard, . . . Franceschi,
D. (2001). Therapeutic doses of oral methylphenidate significantly increase extracellular
dopamine in the human brain. The Journal of Neuroscience, 21(2), 1–5.
Volkow, N. D., Wang, G., Kollins, S. H., Wigal, T. L., Newcorn, J. H., Telang, F., . . . Swanson,
J. M. (2009). Evaluating dopamine reward pathway in ADHD. JAMA: The Journal of the
American Medical Association, 302(10), 1084–1091. doi:10.1001/jama.2009.1308

67
Waxmonsky, J., Pelham, W. E., Gnagy, E., Cummings, M. R., O’Connor, B., Majumdar, A., . . .
Robb, J. A. (2008). The efficacy and tolerability of methylphenidate and behavior
modification in children with attention-deficit/hyperactivity disorder and severe mood
dysregulation. Journal of Child and Adolescent Psychopharmacology, 18(6), 573–588.
doi:10.1089/cap.2008.065
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of
the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic
review. Biological Psychiatry, 57(11), 1336–1346. doi:10.1016/j.biopsych.2005.02.006
Willcutt, E .G., Nigg, J., Pennington, B. F., Solanto, M. V., Rohde, L. A., Tannock, R., . . .
Lahey, B. B. (2012). Validity of DSM-IV attention deficit/hyperactivity disorder
symptom dimensions and subtypes. Journal of Abnormal Psychology, 121(4), 991–1010.
doi:10.1037/a0027347
Wilson, H. K., Cox, D. J., Merkel, R. L., Moore, M., & Coghill, D. (2006). Effect of extended
release stimulant-based medications on neuropsychological functioning among
adolescents with attention-deficit/hyperactivity disorder. Archives of Clinical
Neuropsychology, 21, 797–807. doi:10.1016/j.acn.2006.06.016
Woods, A. J., & Mark, V. W. (2007). Convergent validity of executive organization measures on
cancellation. Journal of Clinical and Experimental Neuropsychology, 29(7), 719–723.
Zelazo, P. D., & Muller, U. (2011). Executive function in typical and atypical development. In
U. Goswami (Ed.), The Wiley-Blackwell handbook of childhood cognitive development
(2nd ed.) (pp. 574–603). Malden, MA: Blackwell Publishing.

68
Zwick, R., & Sklar, J. C. (2005). Predicting college grades and degree completion using high
school grades and SAT scores: The role of student ethnicity and first language. American
Educational Research Journal, 42, 439–464. doi:10.3102/00028312042003439

69
Note. TO
MA
L DB
= Test of Mem
ory and Learning – Digits Backw
ard; Stroop = Stroop Color W
ord Test; TMT-B
= Trail Making Test
Part B; CPT-II = C
onners’ Continuous Perform
ance Test-II; WSR
TM = W
isconsin Selective Reminding Test of M
emory; N
/S = not significant; N
/A = no apparent baseline executive im
pairment (n = 8); Low
= low baseline executive im
pairment (n = 20); M
oderate = m
oderate baseline executive impairm
ent (n = 15); High = high baseline executive im
pairment (n = 10); 1 = B
aseline; 2 = Placebo; 3 = Low
dose; 4 = High dose; aLess than B
aseline; bLess than Placebo; cLess than Low dose; dLess than H
igh dose.
Appendix A
. Summ
ary of Means, Standard D
eviations, and MPH
Dose-Response Relationships for Executive W
orking Mem
ory “Cool”
Circuit N
europsychological Measures Across Im
pairment G
roups
Baseline Placebo
Low D
ose H
igh Dose
“Cool” Circuit Tests M
SD
M
SD
M
SD
M
SD
F
p Post-H
oc !TO
MA
L-DB
!N
/A
17.13 8.27
23.50 14.38
22.38 14.62
22.63 14.60
1.79 .266
N/S
Low
15.50 8.45
21.75 12.03
21.50 12.77
24.65 13.91
6.04 .004
1bd
Moderate
11.20 4.96
13.47 5.84
16.87 4.63
14.13 6.64
4.68 .022
1c
High
9.50 5.48
12.70 11.64
17.30 12.76
15.00 11.89
4.21 .029
1c;2
cd Stroop
N/A
34.88
9.36 42.38
8.25 44.38
9.15 45.75
12.23 6.19
.039 1
bcd Low
25.90
6.49 31.30
8.14 29.75
7.77 34.30
8.29 8.94
<.001 1
bcd;2d;3
d M
oderate 19.20
5.10 24.27
7.34 26.67
6.32 26.07
5.39 19.93
<.001 1
bcd H
igh 20.10
6.21 24.90
9.41 27.30
11.86 28.00
9.90 3.30
.088 1
cd TM
T-B Time
N/A
46.00
51.65 43.88
48.92 32.63
26.10 39.75
33.97 1.48
.266 N
/S Low
55.15
19.04 37.90
14.50 40.40
14.04 37.85
16.77 9.39
<.001 2
a;3a;4
a M
oderate 77.87
28.33 50.07
21.63 47.27
27.42 55.13
21.40 14.85
<.001 2
a;3a;4
a H
igh 161.40
165.64 88.90
56.57 60.50
29.57 75.20
42.17 3.14
.105 3
bd CPT-II O
missions
N/A
51.50
5.66 50.38
8.09 46.88
7.51 45.75
6.18 3.13
.126 4
ab Low
62.50
18.06 55.90
13.72 49.85
8.62 51.25
14.92 6.61
.001 2
a;3ab;4
a M
oderate 68.53
14.74 62.27
10.27 56.33
10.70 52.07
9.52 6.64
.007 2
a;3ab;4
ab H
igh 100.00
72.20 68.30
24.71 67.00
37.38 54.20
8.73 4.16
.065 3
a W
SRTM
N/A
76.73
20.97 85.27
30.35 91.01
12.64 81.92
34.97 1.59
.243 N
/S Low
74.21
12.22 81.75
22.25 88.36
13.68 88.42
20.10 4.30
.015 1
cd M
oderate 64.91
16.16 80.33
22.26 89.09
16.96 83.20
21.13 4.94
.019 1
bcd H
igh 55.53
25.52 74.73
30.83 86.72
15.28 90.19
9.74 8.82
.009 1
bcd

70
Note. Stroop = Stroop C
olor Word Test; TM
T-B = Trail M
aking Test Part B; CPT-II = C
onners’ Continuous Perform
ance Test-II; HD
CT
= Hale-D
enckla Cancellation Test; N
/S = not significant; N/A
= no apparent baseline executive impairm
ent (n = 8); Low = low
baseline executive im
pairment (n = 20); M
oderate = moderate baseline executive im
pairment (n = 15); H
igh = high baseline executive impairm
ent (n = 10); 1 = B
aseline; 2 = Placebo; 3 = Low dose; 4 = H
igh dose; aLess than Baseline; bLess than Placebo; cLess than Low
dose; dLess than H
igh dose.
Appendix B. Sum
mary of M
eans, Standard Deviations, and M
PH D
ose-Response Relationships for Self-Regulation “Hot” C
ircuit N
europsychological Measures Across Im
pairment G
roups
Baseline Placebo
Low D
ose H
igh Dose
“Hot Circuit Tests”
M
SD
M
SD
M
SD
M
SD
F p
Post-Hoc
Go N
o-Go
N/A
26.13
3.44 27.00
4.93 27.00
4.93 27.63
5.13 2.09
.220 N
/S Low
25.30
2.39 27.70
1.75 27.80
1.32 28.70
1.72 12.05
<.001 1
bcd;2d
Moderate
22.87 2.90
27.13 2.33
27.53 2.20
27.20 2.54
19.33 <.001
1bcd
High
20.40
3.13 23.40
3.57 26.40
2.37 25.90
3.57 10.32
.006 1
bcd;2cd
Stroop Errors N
/A
2.13 .99
2.38 1.60
2.38 .92
1.63 1.06
1.03 .453
N/S
Low
3.15 1.50
2.50 1.79
1.95 1.61
1.20 1.28
13.89 <.001
3a;4
abc M
oderate 3.60
1.72 2.87
1.73 1.67
1.50 1.67
1.54 6.81
.006 3
ab;4ab
High
3.70 1.16
4.10 3.41
1.60 1.58
1.90 1.73
4.26 .035
3ab;4
a TM
T-B Errors N
/A
.88 .83
1.25 1.67
1.13 .64
1.63 1.19
.64 .624
N/S
Low
1.00 1.03
1.60 1.31
.80 .95
.65 1.14
3.97 .026
3b;4
b M
oderate 2.47
1.51 1.67
1.11 .87
1.13 .93
.70 6.86
.006 3
a;4a
High
4.50 1.78
3.70 1.25
1.20 .92
1.70 1.42
9.18 .008
3ab;4
ab CPT-II Com
missions
N/A
50.25
11.89 51.88
15.11 50.13
17.10 48.50
16.57 .483
.708 N
/S Low
51.25
11.78 47.00
11.77 45.90
11.69 43.55
12.43 4.45
.018 3
a;4a
Moderate
51.53 7.97
49.47 9.33
45.27 9.92
48.60 8.06
2.49 .111
3ab;4
c H
igh
55.20 7.90
48.60 9.40
45.50 13.43
43.80 15.09
1.83 .229
3a;4
a H
DCT Correct
N/A
27.13
3.04 28.50
1.51 28.38
3.46 27.88
3.18 .725
.579 N
/S Low
26.55
2.78 27.65
2.25 27.90
3.37 27.95
2.21 1.61
.207 N
/S M
oderate 22.00
4.04 26.60
2.47 27.60
1.99 26.80
2.91 5.75
.011 1
bcd H
igh 17.80
5.07 24.00
4.78 27.80
1.62 27.50
2.42 14.78
.002 1
bcd;2cd

71
Appendix C: Copyright Permission Letter
Global Multimedia Partners, Inc Permission Letter
Permission #: 127021 Date: 22 May 2013
Hanna Kubas ! 5212 32 Avenue NW Calgary, Alberta, T3B-0J6! Canada [email protected]
Reference to material to be used: Kubas, H. A., Backenson, E. M., Wilcox, G., Piercy, J. C., & Hale, J. B. (2012). The effects of methylphenidate on cognitive functions in children with attention-deficit/hyperactivity disorder. Postgraduate Medicine 124(5): 33-48.! Table 1. MPH Dose-Response Relationships for EWM/SR Impairment Groups for Individual Tests; Figure 1. Procedure for the double-blind placebo controlled protocol; and! Figure 2. Dose response relationships for neuropsychological tests by impairment group.
Proposed use: Author will be using Figure 1 &2, Table 1, as well as data presented in the Results of the article in thesis.
We hereby grant you permission to republish the material mentioned above for the purpose you have indicated only, subject to the following conditions:
1. Receipt of a copyright fee of [WAIVED] due upon receipt of our permission letter and invoice. All applicable taxes will be presented on the invoice.
2. If any part of the material to be used (for example, figures) has appeared in our publication with credit or acknowledgement to another source, permission must also be sought from that source. If such permission is not obtained then that material may not be included in your publication/copies.
3. Reproduction of this material is confined to the purpose for which permission is hereby given. 4. Suitable acknowledgement to the source must be made, either as a footnote or in a reference
list at the end of your publication, as follows: Reprinted from Publication title, Volume number, Author(s). Title of Article, Page No., Copyright (Year), with permission from JTE Multimedia.
5. This permission is for one time use and is granted for non-exclusive English world rights only. For other languages, please reapply for permission separately. Permission EXCLUDES use in any electronic form other than as specified.
Reprints/Permissions Manager! For and on behalf of JTE Multimedia! Agreed Global Multimedia Partners, Inc ________________________________ _____________________________