evolving technologies that can improve specialty patient outcomes april 3, 2013
TRANSCRIPT

Evolving Technologies that can Improve Specialty Patient
OutcomesApril 3, 2013
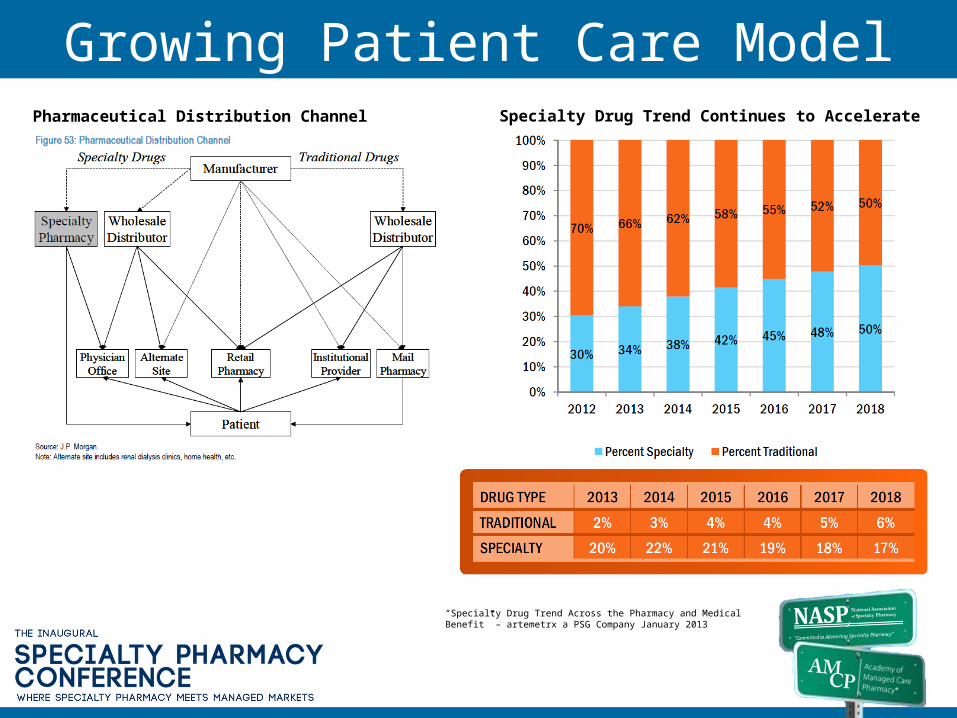
Growing Patient Care ModelPharmaceutical Distribution Channel Specialty Drug Trend Continues to Accelerate
“Specialty Drug Trend Across the Pharmacy and Medical Benefit” – artemetrx a PSG Company January 2013

TECHNOLOGY SUPPORT DEMAND

Enhanced Reporting Requirements Status Code PENDING Reason Codes
Status assigned to a patient who has been referred to the SP but has not yet received a shipment of product from that SP
P1 1 - New referral
Assigned to a patient immediately after receipt of the referral from Fingolimod® Support Center. Indicates that the SP just received the referral but has not yet determined whether or not the SP can service that patient referral (i.e., is a network provider).
P22 - Processing Benefit Investigation SP has determined that it can service the patient and is in the process of verifying benefits.
P3 3 - Processing Prior Authorization SP has determined that a prior authorization (PA) is required and the SP is working with the prescriber to complete the PA or is waiting to receive notification that the PA was approved.
P44 - Order Cleared - Ready to be shipped
SP has completed the benefit investigation (BI) and all required REMS activities (i.e., authorization number received, patient counseling) but has not yet shipped the product.
P5 5 - Patient Decision SP has completed the BI but progress has been stopped at the request of the patient or patient approval is required to move forward.
P6 6 - Prescriber Decision SP has completed the BI but progress has been stopped at the request of the prescriber or prescriber approval is required to move forward.
P7 7 - Clinical Reason
SP has completed the BI, but progress has been stopped due to a clinical reason (e.g., patient hospitalization). Treatment with the product is still under consideration. Note that if the patient has not received product from this SP, or any other SP, any clinical reason reported would not constitute an adverse event (AE). If, however, the SP is servicing the patient for the first time, but another SP had provided product, and the patient or the prescriber reports an AE, this AE must be reported per policy.
P8 8 - Unable to contact patient SP has not been able to contact the patient to relay critical information or conduct patient counseling but is continuing to attempt contact.
P99 - Processing waiting on inventory
SP has completed the BI, all required REMS activities and cleared the order but does not have sufficient product inventory.
P1010 - Processing - Foundation Review (Possible revision) SP is awaiting notification that the patient is approved for financial support.
P11 11 - Delay in Treatment Initiation SP has completed the BI and may have completed the required REMS activities, but the product will not be shipped because initiation of treatment will be/was delayed
P15 15 - Other To be used only when no other code adequately describes the PENDING status code.
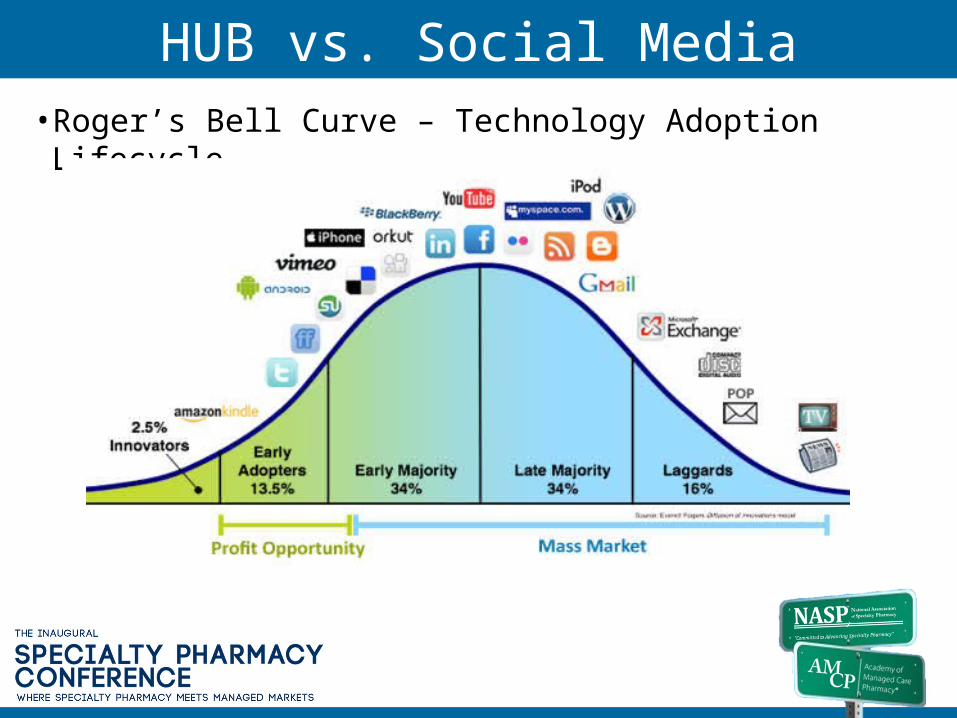
HUB vs. Social Media• Roger’s Bell Curve – Technology Adoption Lifecycle

HUB Model: One Stop ShoppingNew Prescription Referral Management
SP Distribution Network Triage Management
Benefit Investigations
Prior Authorization Support & Re-Certifications
PAP Coordination Support
Copay Assistance
Claims Assistance
Clinical Services
Nurse Hotline Support
Telephonic & Home Injection Training
Persistency and Compliance Support
Web-portal for Providers & Patients
Big Data & Dynamic Reporting
Mobile Connectivity
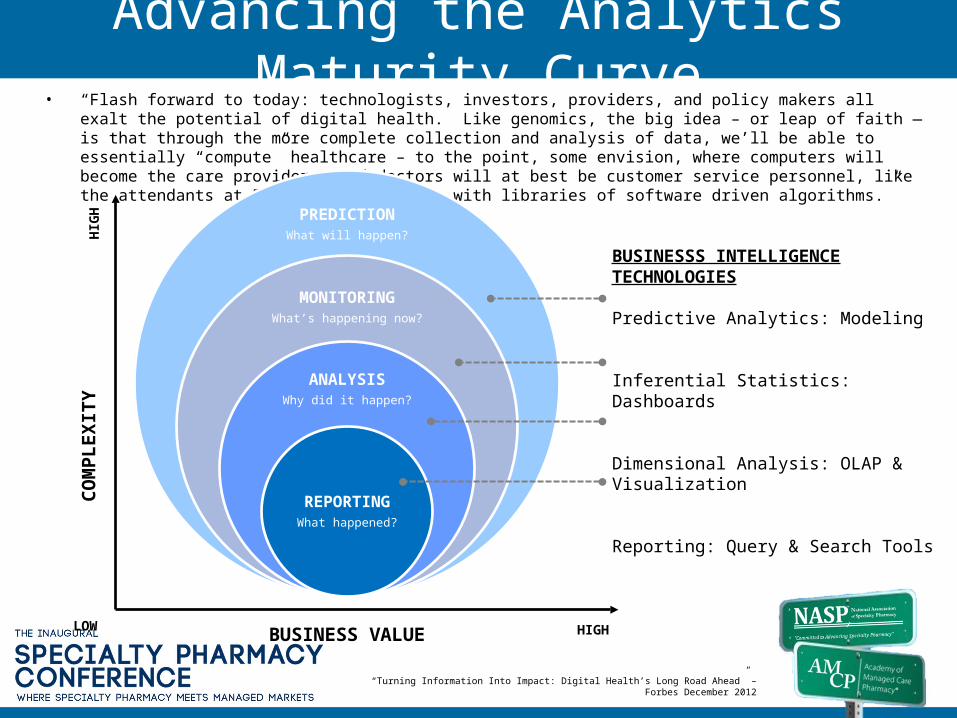
Advancing the Analytics Maturity Curve• “Flash forward to today: technologists, investors, providers, and policy makers all exalt the potential of digital health. Like
genomics, the big idea – or leap of faith — is that through the more complete collection and analysis of data, we’ll be able to essentially “compute” healthcare – to the point, some envision, where computers will become the care providers, and doctors will at best be customer service personnel, like the attendants at PepBoys, interfacing with libraries of software driven algorithms.”
PREDICTIONWhat will happen?
MONITORINGWhat’s happening
now?
ANALYSISWhy did it happen?
REPORTINGWhat happened?
BUSINESS VALUE
COM
PLEX
ITY
LOW
HIG
H
HIGH
BUSINESSS INTELLIGENCE TECHNOLOGIES
Predictive Analytics: Modeling
Inferential Statistics: Dashboards
Dimensional Analysis: OLAP & Visualization
Reporting: Query & Search Tools
“Turning Information Into Impact: Digital Health’s Long Road Ahead” – Forbes December 2012

Consumer Driven Ecosystem & mHealth
“Innovation – A Look at mHealth’s Moving Target” – Rick Krohn/David Metcalf HIMSS March 2013
Decision Support
Engagement
Care Coordination
Convenience
Retail Clinics
Individual
PCP
Transparency
Access
Content
Worksite Clinics
PHR/EHR/HRA Dataflow
Price/Quality Information
Remote Monitoring
DiagnosticsCare Gaps
Wellness/ Coaching/ Incentives
Care Management
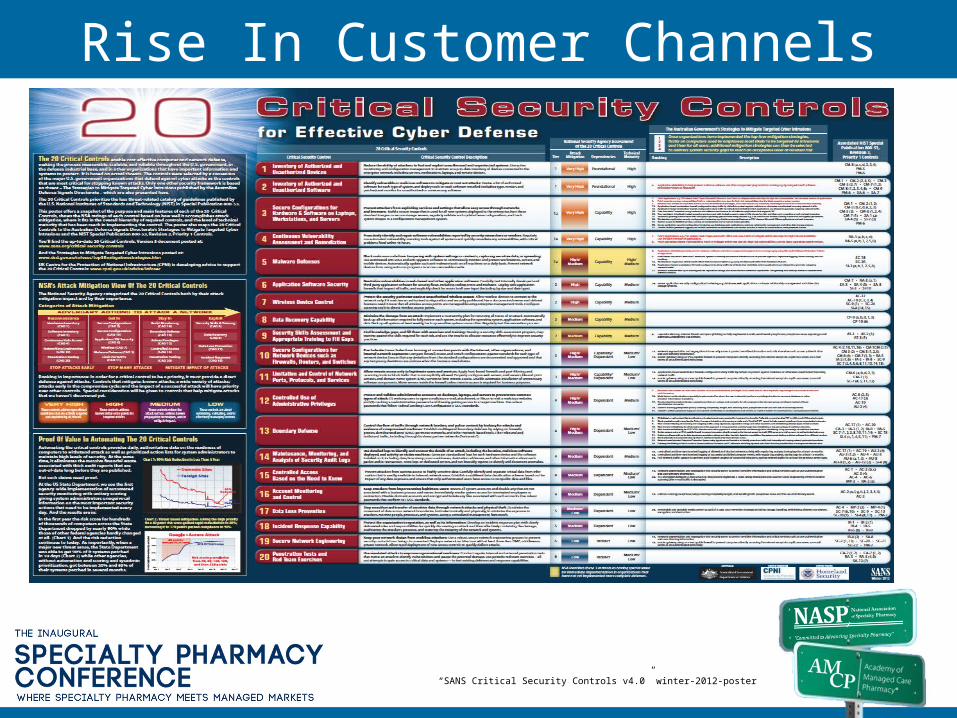
Rise In Customer Channels
“SANS Critical Security Controls v4.0” winter-2012-poster
EVOLVING TECHNOLOGIES THAT CAN IMPROVE SPECIALTY PATIENT OUTCOMES
4:15 – 5:30
Sean CreehanPresidentcreehan & company

© creehan & company
EnterprisePartner
Collaboration
Analytics MyShare
Technology Portfolio Technology-Enabled Services
Infrastructure
interchange

Evidence Quality Cost
Coordination Engagement Reporting
6 Critical Success Factors Driving Technology Needs … and Opportunities
© creehan & company

Protocol Development
Data Collection
Protocol Execution
Data Access Challenges
Applying the Data
Patient Care Story
Decision Support
Data Interoperability
Transactional & Trend Data
Supporting Technology Initiatives
Care Management
Evidence
© creehan & company
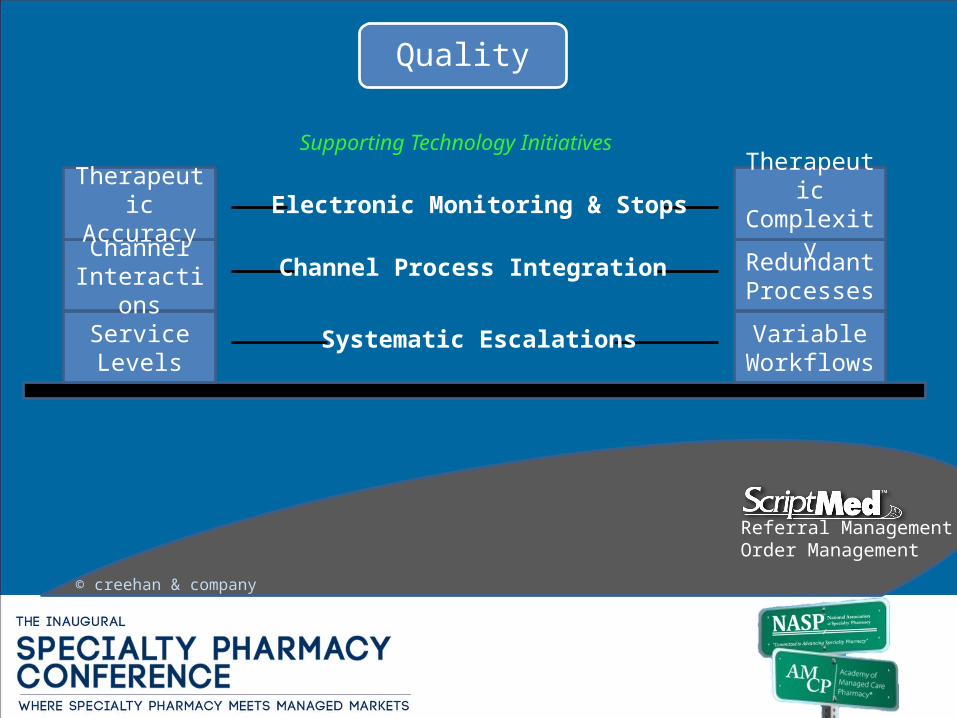
Service Levels
Channel Interactions
Variable Workflows
Redundant Processes
TherapeuticComplexity
TherapeuticAccuracy
Systematic Escalations
Channel Process Integration
Electronic Monitoring & Stops
Referral ManagementOrder Management
Quality
© creehan & company
Supporting Technology Initiatives

Clinical Success
Spend and Trend Mgt
Labor Activity Costs
Lower Fee More Service
Consolidated Channel
Restricted Networks
Risk Share Management
Stakeholder Facing Tools
Improved Contract Administration
Cost
AnalyticsA/R Management
© creehan & company
Supporting Technology Initiatives
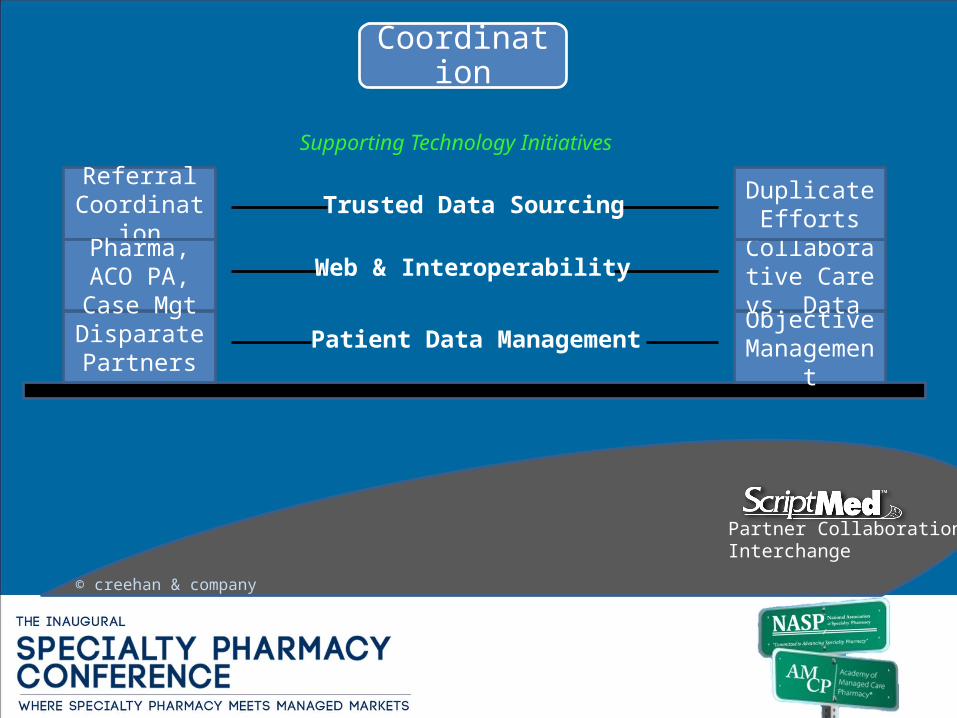
Disparate Partners
Objective Management
Collaborative Care vs. Data
Duplicate Efforts
Referral Coordination
Patient Data Management
Web & Interoperability
Trusted Data Sourcing
Pharma, ACO PA, Case Mgt
Partner CollaborationInterchange
Coordination
© creehan & company
Supporting Technology Initiatives

Channel Synergy
Systems Integration
Consistent Data Capture
Care Standards
Cost & Convenience
Channel Partner Integration
Web & Mobile
Multi-Method Engagement
Patient Preference
MyShareTelephony Enablement
Engagement
© creehan & company
Supporting Technology Initiatives
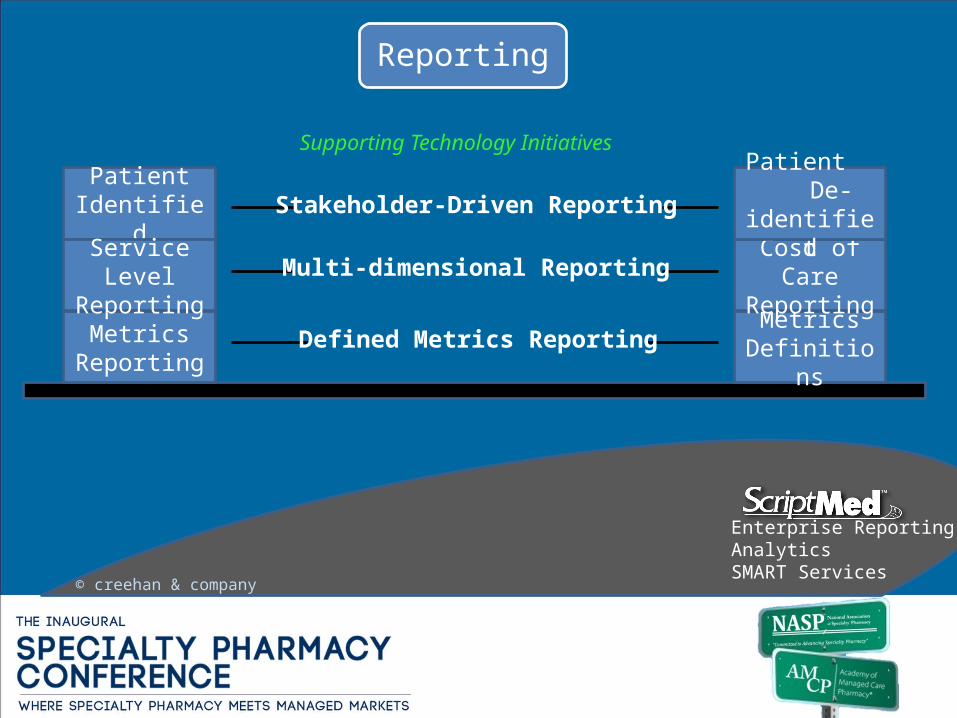
MetricsReporting
Metrics Definitions
Cost of Care Reporting
Patient De-identified
Patient Identified
Defined Metrics Reporting
Multi-dimensional Reporting
Stakeholder-Driven Reporting
Service Level Reporting
Enterprise ReportingAnalyticsSMART Services
Reporting
© creehan & company
Supporting Technology Initiatives

An integrated technology portfolio is paramount for the next generation of Specialty Pharmacy.
© creehan & company
Evidence Quality Cost
Coordination Engagement Reporting

Evolving Technologies That Can Improve Specialty Patient Outcomes
Cardinal HealthSpecialty Solutions
PathWare™ Demonstration
Bruce Feinberg, DOVP/CMO, Cardinal Health
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

PathWare™ DemonstrationPathWare™ Decision Support Tool
• MACRO and client specific such as IDN
• PathWare ™ is a decision support tool not EMR
• End to end transaction support tool
• Enables communication between IDN, PBM, MD and CardinalHealth
• Evidence based (deep Evidence based literature such as: NCCN, ASCO, Compendia, FDA labeling, Global Literature)
• Clinical Content Management in real time
• Measures physician compliance to pathways in real time
• Cost of regimens
• Contains patient education materials, consent forms and chemotherapy orders
EMR • MICRO and patient specific
• Day-to-Day operational tool for management of patient information and flow such as frequency of use, data input and output, encounter time, encounter frequency
• Definitive record keeper patient of encounter information
• Billing and claims information
• Daily documentation and ordering
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
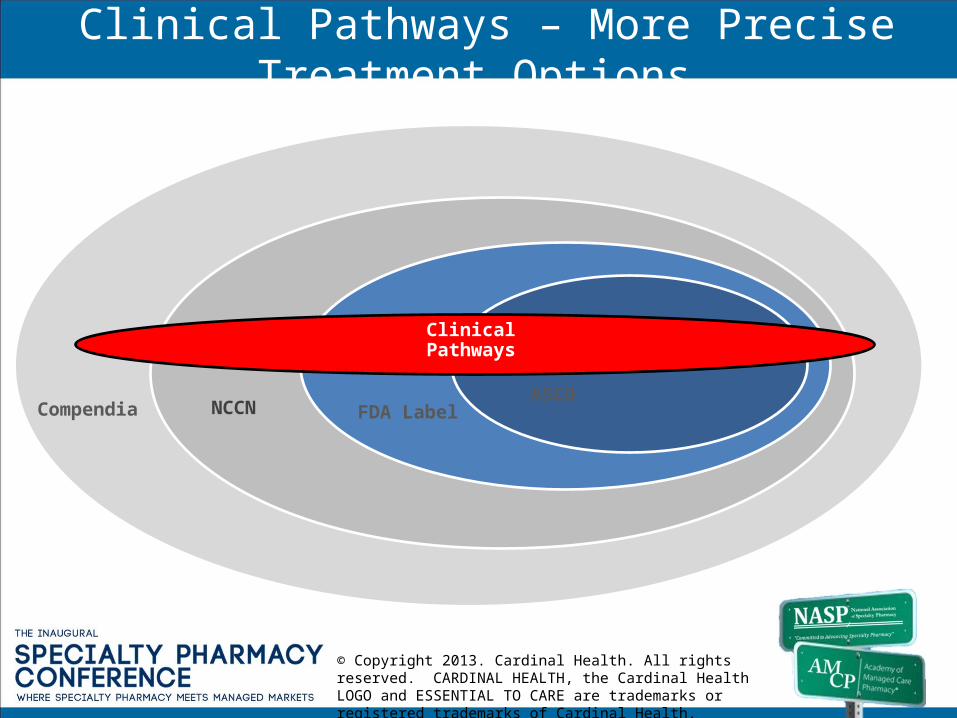
Clinical Pathways – More Precise Treatment Options
Clinical Pathways
ASCOFDA LabelNCCN Compendia
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

Poonacha T K , Go R S JCO 2011;29:186-191
NCCN Distribution of Evidence
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

Patient Selection
DiagnosisBenefits
Verification
Supporting Literature
Treatment Summary
ClinicalData
Capture
Protocol SelectionAuthorization
and Alerts
PathWare™ Decision Support Tool
Drug Shortages
PathWareTM
Solutions
Specialty Pharmacy
Site of
Care
PathWareTM is the end to end decision support
tool connecting the Payer, Provider, PBM, Specialty Pharmacy and Cardinal in the
treatment ecosystem. (consider removing)
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
ANSI-EDI
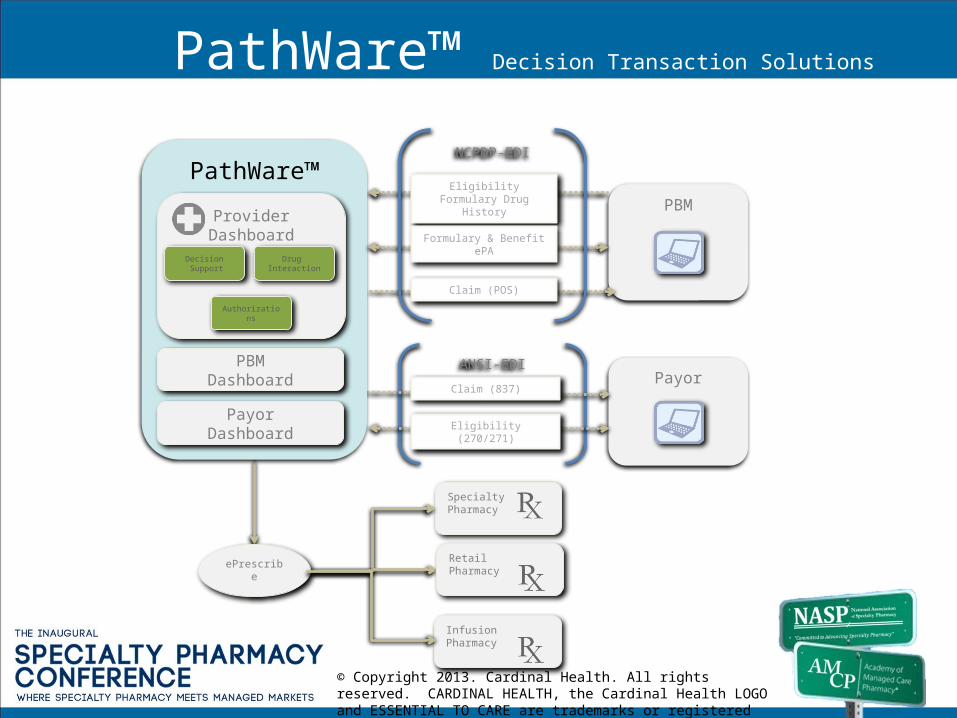
PathWare™ Decision Transaction Solutions
Specialty Pharmacy
PBM
Payor
Claim (POS)
Claim (837)
RetailPharmacy
ePrescribe
PathWare™
ProviderDashboard
PayorDashboard
PBMDashboard
Decision Support
Drug Interaction
Authorizations
Eligibility Formulary Drug History
Eligibility (270/271)
Formulary & Benefit ePA
NCPDP-EDI
InfusionPharmacy
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
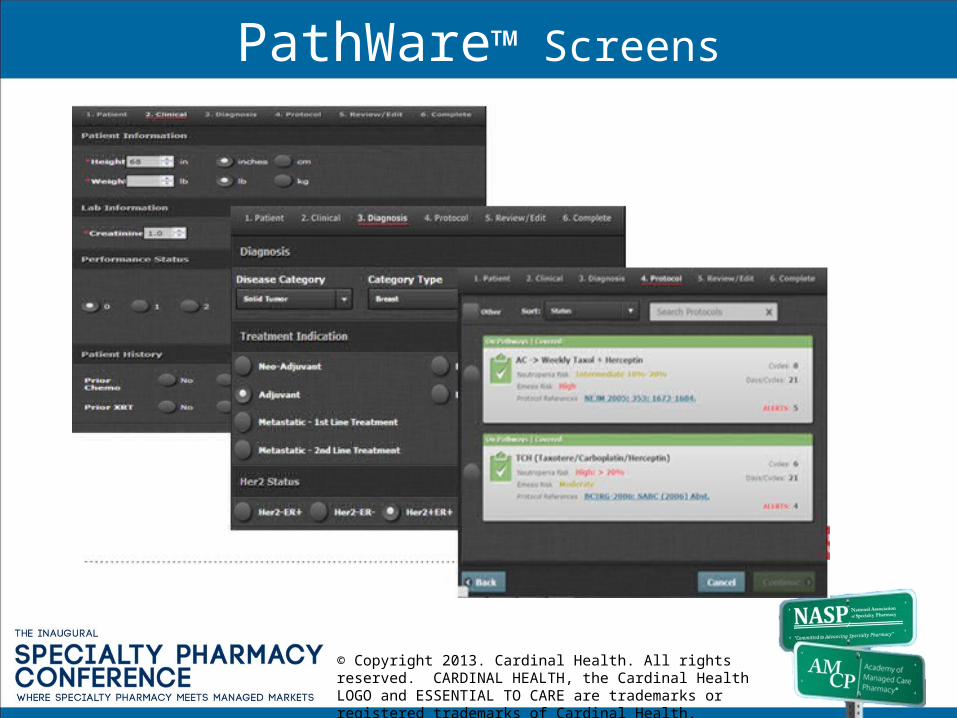
PathWare™ Screens
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
Pathway Guiding Principles• Our pathway programs are independent from our
commercial relationships
• Our pathways are collaboratively developed with the participating physicians
• Our pathways are designed to deliver the best clinical outcome for the patient
• Our pathways incorporate quality indicators developed in cooperation with participating physicians
IndependenceIndependence
CollaborativeCollaborative
Best Patient Outcome
Best Patient Outcome
We believe properly designed pathway programs will create sustainable reimbursement that rewards innovation based on clinical data while delivering excellent
clinical care
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

Program Patient Inclusion Ramp
Per 1MM lives commercial plan (<65 years), treatment naïve patients
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

Reduction in Treatment Variability
1. Clinical Pathways has been effective in reducing treatment variability.
2. The cost of therapies utilized before, but not after pathways represents a 4% savings
Nu
mb
er o
f d
isti
nct
co
mb
inat
ion
% of Patients
After implementation annual spend
$54,080,164
Saving of Pre-pathways regimens no longer used
$ 2,279,267
Percent Savings 4%
*Analysis used patient line of therapy starts during each period. “Pre-pathways” contains the 12 mo prior to Aug 2008, and “after implementation” contains the 12 mo ending Jul 2010. #Limited to anti-neoplastics for Breast, Colon and Lung Cancer in “after implementation” period.@Categories are not distinct and total will sum to >100%
Reduced Variability Has Been Observed in the Participating Physician Population
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
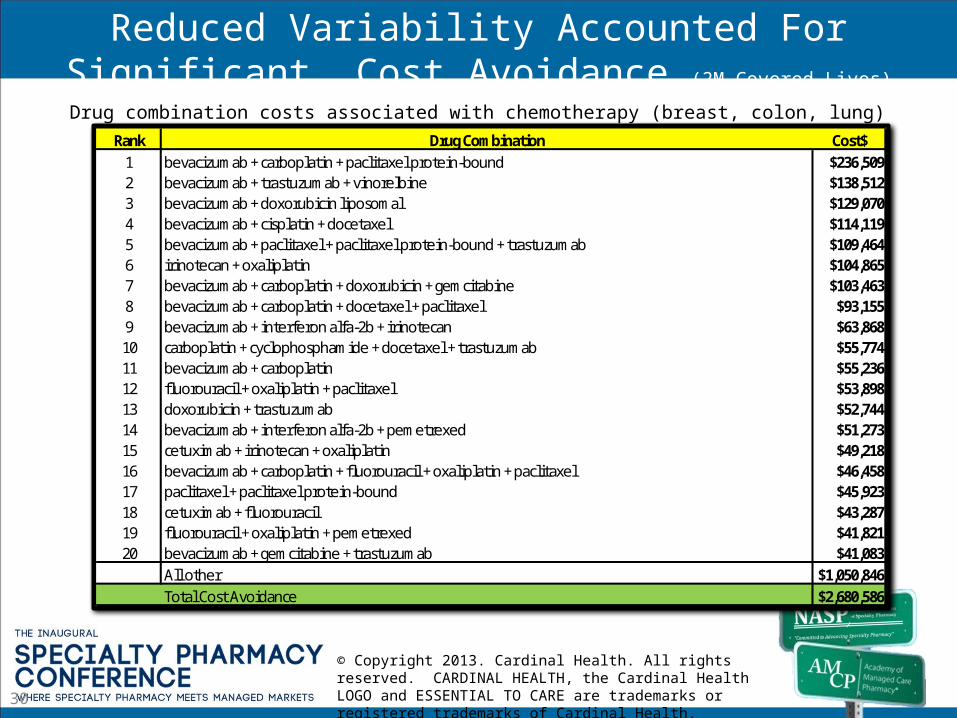
Rank Drug Combination Cost$1 bevacizumab + carboplatin + paclitaxel protein-bound $236,5092 bevacizumab + trastuzumab + vinorelbine $138,5123 bevacizumab + doxorubicin liposomal $129,0704 bevacizumab + cisplatin + docetaxel $114,1195 bevacizumab + paclitaxel + paclitaxel protein-bound + trastuzumab $109,4646 irinotecan + oxaliplatin $104,8657 bevacizumab + carboplatin + doxorubicin + gemcitabine $103,4638 bevacizumab + carboplatin + docetaxel + paclitaxel $93,1559 bevacizumab + interferon alfa-2b + irinotecan $63,86810 carboplatin + cyclophosphamide + docetaxel + trastuzumab $55,77411 bevacizumab + carboplatin $55,23612 fluorouracil + oxaliplatin + paclitaxel $53,89813 doxorubicin + trastuzumab $52,74414 bevacizumab + interferon alfa-2b + pemetrexed $51,27315 cetuximab + irinotecan + oxaliplatin $49,21816 bevacizumab + carboplatin + fluorouracil + oxaliplatin + paclitaxel $46,45817 paclitaxel + paclitaxel protein-bound $45,92318 cetuximab + fluorouracil $43,28719 fluorouracil + oxaliplatin + pemetrexed $41,82120 bevacizumab + gemcitabine + trastuzumab $41,083
All other $1,050,846Total Cost Avoidance $2,680,586
30
Reduced Variability Accounted For Significant Cost Avoidance (2M Covered Lives)
Drug combination costs associated with chemotherapy (breast, colon, lung)
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.
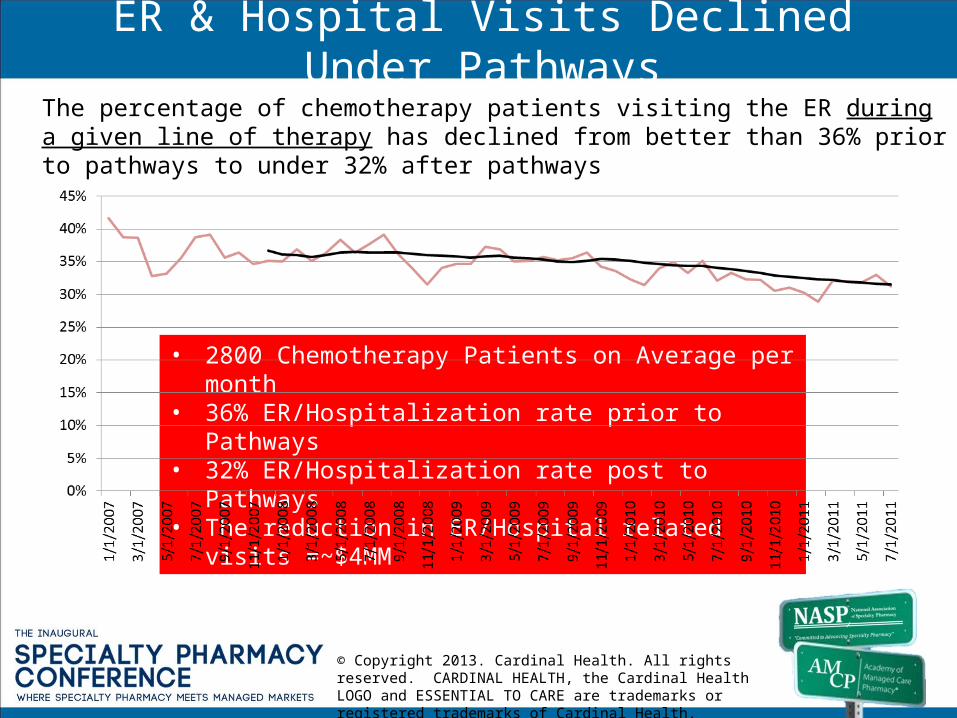
ER & Hospital Visits Declined Under PathwaysThe percentage of chemotherapy patients visiting the ER during a given line of therapy has declined from better than 36% prior to pathways to under 32% after pathways
• 2800 Chemotherapy Patients on Average per month• 36% ER/Hospitalization rate prior to Pathways• 32% ER/Hospitalization rate post to Pathways• The reduction in ER/Hospital related visits =~$4MM
© Copyright 2013. Cardinal Health. All rights reserved. CARDINAL HEALTH, the Cardinal Health LOGO and ESSENTIAL TO CARE are trademarks or registered trademarks of Cardinal Health.

Evolving Technologies That Can Improve Specialty Patient
Outcomes
Chad Malone, MDVice President, Medical Affairs
Remedy Informatics

Basic Research
Preclinical Res Clinical Res
Health Care
Outcomes ResComparative Res
Outcomes and comparative effectiveness
informed basic research
Genomics informed biomarker
discovery and drug
development
Genomics informed
clinical trials
Genomics- and outcomes-informed patient
stratification
Outcomes informed preclinical research
Outcomes informed cost-benefit analysis
Evidence-Based Research & Healthcare Delivery

Ontologically Driven Data Harmonization
‘Omics Data
Reports/Dashboards
Biospecimen Data
Clinical Trials Management
Quality Improvement
Pedigree Charts
Disease Associations
National Registries
Claims Data
Cohort Selection
University Partners
PI Study Data
Imaging
Clinical Trials
Longitudinal PatientReported Data
Epic Data
Principal Investigators
Query & Reporting
Aggregate,
Map,Harm
onize
Workfl
ow
Mgt
Data
visualization
Patient
PortalStudy Management
EDC
Web
Serv
ices
Biospecim
en
man
agem
en
t
MosaicRepository
MosaicOntology
ACO Data
Mosaic Repository

Learning Products Lead to Patient Specific Care
• All about continuous learning
• More data, better results lead to competitive advantage
• Must be customizable to each specialty
• Cross specialty and cross institution collaboration is the home run here

Thomas Morrow MDAuthor of
Tomorrow’s MedicineManaged Care
Evolving Technologies That Can Improve Specialty Patient Outcomes
Personal Health Assistant in Specialty Pharmacy
Disclaimer
Dr. Morrow: • is a full time employee of of a Genentech but no company products will be
discussed during this presentation. The opinions expressed during this discussion are his alone and do not reflect the opinions of his full time employer.
• has created this talk from his research concerning VHA for an article published Managed Care and Forbes
http://www.forbes.com/sites/ciocentral/2013/03/13/how-virtual-health-assistants-can-reshape-healthcare/
http://managedcaremag.com/archives/1202/1202.biotech.html


The Maasai Warrior in Kenya has better access to data and communication than President Reagan!
Natural Language Processing and the Conversational Interface:
Keys to Artificial Intelligence
• Artificial Intelligence– The ability of a computer or other machine to perform actions
thought to require intelligence.
• Natural Language• Human written or spoken language as opposed to a
computer language. Top Companies:
– Next IT: focusing on the patient interaction– Nuance/VirtuOz: focusing on medical records– Creative Virtual: no obvious medical focus– IBM Watson:
• No commercially available products• Oncology/Cardiac physician decision support

Medical Decisions Occur in a Minute by Minute Basis,
• Patients spend a few hours per year with their physician for a “specialty pharmacy” disorder.
• They spend 5000 hours per year making literally thousands of decisions that affect their health
• They need day to day decision support and guideline/algorithm driven
• Natural Language Equipped Intelligent Agents can full this need

Characteristic Traditional IVR Traditional Web Chatbot Next IT’s Multimodal Virtual Assistant
Input Voice and DTMF tones input via keypad
Text Text, Talk, Tap
Language Processing Decision Tree with limited FAQ based interactions
Searchable FAQ Stochastic NLP engine with an intent based language model
Logic Model Linear with branchesTypically 4x4 or 5x4 model
Silo singular answer based Human Emulation – The model is a combination of decision tree, FAQ and intent model which also incorporates context like a human does.
Channels Phone Web Phone, web, SMS Text, mobile, kiosk, social mediaOutput Voice Text and sometimes voice Voice, Text, Navigation often simultaneously based on channel
Contextual Awareness Minimal: Based upon account, user profile
Minimal Based upon account, user profile
or General Answers
Page AwarenessConversational Awareness
User ProfileEvery question is taken in the context of the entire conversation as well
as other data sources
Proactive Engagement None None Multiple options, dynamic, personalized
language model size 4x4 to 5x4 200-300 in a basic FAQ mode 10s of thousands of intents in a single model
Where placed in organization
IVR’s can be set up to support specific tasks in an organization
Usually isolated to a section of a web site, not the entire site.
Across the entire web site/portal and across multiple channels as well.
Breadth/ Depth minimal on both since a human listening to the phone can only
remember a small number of options
Typically limited to either broad OR deep but not both
Able to cover a very broad domain of knowledge while also having a great deal of depth where applicable.
End Point Simple task General Answer to simple questions Truly conversational
Cost to Build $$ $$ $$$How built Voice Recognition Search Based Chat Recognition
Future enhancements Limits reached Limits almost reached Virtually infinite
Overall Long Term Value $ $$ $$$$$
Monthly Operational Cost to Organization
$$$$$(based on need to divert calls to Live
Agent)
$$$$$(based on need to divert calls to Live
Agent)
$(Virtually all calls can be handled by Virtual Agent limiting the number
of live agents needed)
Automated system choices available to an organization

The Virtual Health Assistant: a disruptive technology
• A New Definition of High Touch• Fulfillment Needs• Patient Education• Disease Treatment Management Programs• A New Level of Data Collection: Treatment Optimization

Evolving Technologies that can Improve Patient Outcomes
David Schaefer – AxelaCare
Home Based, Patient Outcomes, Data Capture and Management

Clinical Outcomes Data for True Managed Care

Home Infusion Therapy Monitoring
Physical AssessmentsDisability / Activities of Daily Living
(ADL)Quality of Life (QOL)
ValidatedOutcomesMeasures
IVIg PatientData Collection
CIDP/GBS/Peripheral Neuropathy Myasthenia Gravis
Primary Immunodeficiency
Outcomes vs.
Dose Over Time
CareatorsCare Support
PhysicianData Review
AdministratorsCoordinatorsResearchers
Dose, Side Effect, ClinicalMonitoring
PharmacistData Review
Patient Assessments

Physical Assessments Nurse Driven Data Collection…
Grip Strength (Jamar Dynamometer) TUGS (Timed Up and Go) Spirometry (FEV, PEF, FVC, Flow Volume Loop) NIF (Negative Inspiratory Force) Double Vision

Clinical Example – IVIG Neuropathy

IVIG Est. Cost Savings - Strategies Comparison
Est. 50% of
Improving, New, and Unstable
13
11
20
44%
Cure(>5 years)
Remission(<5 years)
IVIG - Neuropathy

Evolving Technologies that can Improve Specialty Patient
OutcomesApril 3, 2013