evidence-based review of the literature on intrathecal delivery of pain medication
TRANSCRIPT

© U.S. Cancer Pain Relief Committee, 2000 0885-3924/00/$–see front matterPublished by Elsevier, New York, New York PII S0885-3924(00)00204-9
S12 Journal of Pain and Symptom Management Vol. 20 No. 2 August 2000
Original Article
Evidence-Based Review of the Literature on Intrathecal Delivery of Pain Medication
Gary Bennett, PhD, Mario Serafini, DO, Kim Burchiel, MD, Eric Buchser, MD,Ashley Classen, DO, Tim Deer, MD, Stuart Du Pen, MD, F. Michael Ferrante, MD,Samuel J. Hassenbusch, MD, PhD, Leland Lou, MD
,
Jan Maeyaert, MD,Richard Penn, MD, Russell K. Portenoy, MD, Richard Rauck, MD, K. Dean Willis, MD, and Tony Yaksh, PhD
Department of Neurology (G.B.), MCP Hahnemann University, Philadelphia, PA; Center for Pain Relief (M.S.), Clarksburg, WV; Department of Neurological Surgery (K.B.), Oregon Health Sciences University, Portland, OR ; Anesthesia and Pain Management Services (E.B.), Hôpital de zone de Morges, Morges, Switzerland; Trinity Pain Medicine Associates, P.A. (A.C.), Ft. Worth, TX; The Center for Pain Relief (T.D.), Charleston, WV; Department of Anesthesia (S.D.P.), Swedish Hospital, Seattle, WA; Pain Medicine Center (F.M.F), University of Pennsylvania Health System, Philadelphia, PA; Department of Neurosurgery (S.J.H.), M.D. Anderson Cancer Center, Houston, TX; Department of Anesthesiology (L.L.), Texas Tech University Health Science Center, Lubbock, TX; AZ St. Lucas (J.M.), Ghent, Belgium; Department of Neurosurgery (R.P.), Mt. Sinai Medical Center, New York, NY; Department of Pain Medicine and Palliative Care (R.K.P.), Beth Israel Medical Center, New York, NY; Pain Control Center (R.R.), Wake Forest University Baptist Medical Center, Winston-Salem, NC; Alabama Pain Center (K.D.W.), Huntsville, AL; and Department of Anesthesiology (T.Y.), University of California, San Diego, CA, USA
Abstract
Evidence-based medicine depends on the existence of controlled clinical trials that establish the safety and efficacy of specific therapeutic techniques. Many interventions in clinical practice have achieved widespread acceptance despite little evidence to support them in the scientific literature; the critical appraisal of these interventions based on accumulating experience is a goal of medicine. To clarify the current state of knowledge concerning the use of various drugs for intraspinal infusion in pain management, an expert panel conducted a thorough review of the published literature. The exhaustive review included 5 different groups of compounds, with morphine and bupivacaine yielding the most citations in the literature. The need for additional large published controlled studies was highlighted by this review, especially for promising agents that have been shown to be safe and efficacious in recent clinical studies.
J Pain Symptom Manage 2000;20:S12–S36.
© U.S. Cancer Pain Relief Committee, 2000.
Key Words
Evidence-based medicine, intraspinal infusion, pain management, intrathecal
Introduction
To effectively manage pain patients usinglong-term intrathecal infusions, it is importantto understand the strengths and weaknesses ofcurrent and upcoming therapies that havebeen reported in the literature. As part of a
Address reprint requests to:
Samuel J. Hassenbusch, MD,PhD, Department of Neurosurgery, C-9.075, The Uni-versity of Texas-Houston M.D. Anderson Cancer Cen-ter, 1515 Holcombe Blvd., Houston TX 77030, USA.
Accepted for publication: May 30, 2000

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S13
project to review the role of intrathecal in-fusions, an expert panel conducted a system-atic review of literature concerning the drugsthat have been used in long-term intrathecalinfusion.
Therapies were divided into five general cat-egories of compounds that have been utilized(or hypothesized to be effective) for intrathe-cal delivery of pain medication. The expertpanel then evaluated the safety and efficacy ofeach drug, as well as current clinical practicesand guidelines.
A major goal of the systematic review was tosearch for and evaluate reports of prospectivecontrolled studies examining the safety and ef-ficacy of existing and upcoming therapies—acrucial component of evidence-based medi-cine. Other important criteria in the literaturereview of intrathecal delivery included datafrom preclinical and toxicity studies in bothhumans and animals for the various com-pounds. By critically evaluating these pub-lished reports using widely accepted criteria,the panelists presented a case for the validity ofthe compounds for clinical use. In some cases,the panel suggested further research in ran-domized controlled clinical trials before thetherapy can be adopted for widespread clinicaluse; others, the panel suggested that theremight be no potential for clinical use based onsafety and efficacy considerations. In somecases, there was little or no evidence to supportthe use of specific drugs for intrathecal admin-istration in the treatment of chronic pain.
Methods
Computer literature searches were per-formed using the Medline database for 1966
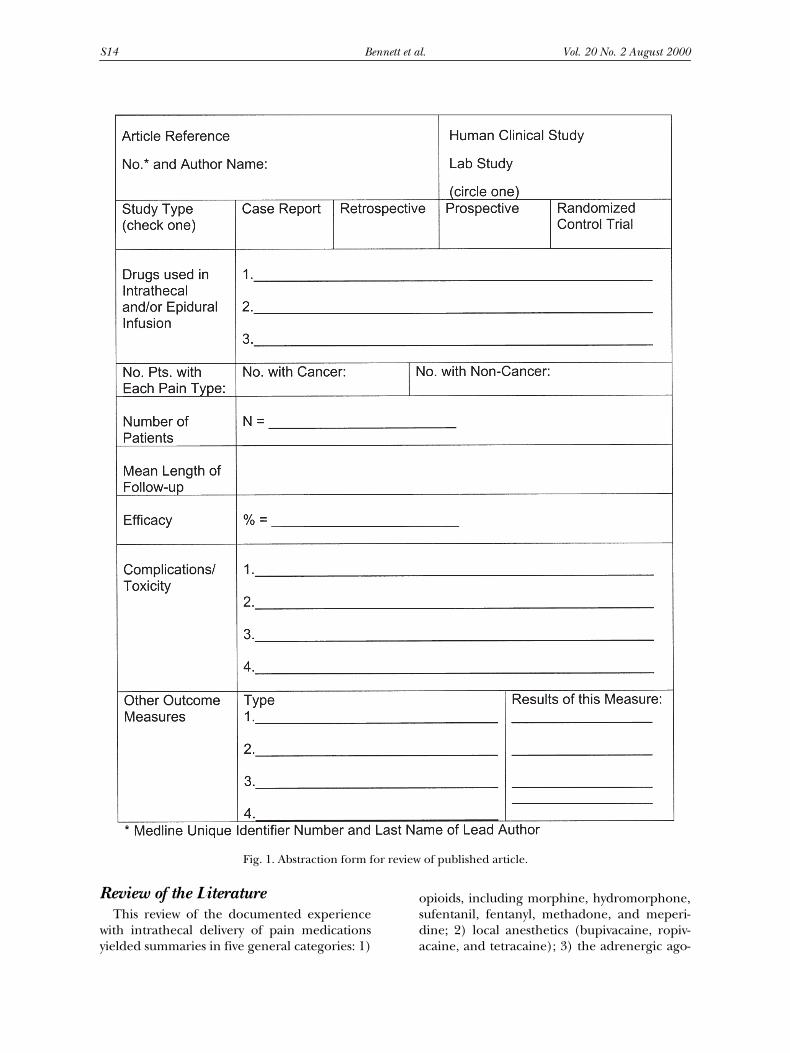
through October 1999. The searches groupedcitations into 12 groups, as outlined in Table 1.In addition, several specific drugs and drug/drug combination terms were searched (Table2). The panel members then manually scannedthe citation lists from these searches, and cita-tions were marked that potentially provideduseful information about long-term spinal infu-sions. Copies of the selected journal articleswere then obtained, analyzed, and abstracted.Figure 1 shows the abstraction form that wasused for each article to summarize useful infor-mation for reviewing and prioritizing the arti-cles (i.e., study type, drugs, patient type/num-ber, efficacy, and adverse effects).
Table 1
Categories According to Which Literature Search Was Carried Out
1. Drug & (intrathecal or subarachnoid) & (chronic or long-term)—limit to Human, review2. Drug & (intrathecal or subarachnoid) & (chronic or long-term)—limit to Human & (non-review)3. Drug & (intrathecal or subarachnoid) & (chronic or long-term)—limit to Non-human4. Drug & (intrathecal or subarachnoid) & Pain NOT (chronic or long-term)—limit to Human & review5. Drug & (intrathecal or subarachnoid) & Pain NOT (chronic or long-term)—limit to Human & non-review)6. Drug & (intrathecal or subarachnoid) & Pain NOT (chronic or long-term)—limit to Non-human7. Drug & (intrathecal or subarachnoid) NOT Pain NOT (chronic or long-term)—limit to Human8. Drug & (intrathecal or subarachnoid) NOT Pain NOT (chronic or long-term)—limit to Non-human9. Drug & (epidural or intraspinal) & (chronic or long-term)
10. Drug & (epidural or intraspinal) & Pain NOT (chronic or long-term)—limit to Human, English11. Drug & (epidural or intraspinal) & Pain NOT (chronic or long-term)—limit to Non-human, Non-English12. Drug & (epidural or intraspinal) NOT Pain NOT (chronic or long-term)
Table 2
Specific Drugs and Drug CombinationsThat Were Searched in the Database for
Literature Review
Aspirin or acetylsalicylic acid or ASA or salicylic acid or acetylsalicylate
(Baclofen or Lioresal) and painBupivacaine or MarcaineDemerol or Pethidine or Meperidine or DemeralDroperidol or InapsineFentanylClonidineHydromorphone or DilaudidMethadone or MethadonMidazolam or VersedMorphineNeostigmine or ProstigminDextrorphan or Dextromethorphan or MemantineKetamineMK-801Octreotide or VapreotideRopivacaine or Ropivicaine or NaropinSNX-111 or SNX111 or ZiconotideSufentanil or SufentaTetracaineTizanidine
S14 Bennett et al. Vol. 20 No. 2 August 2000
Review of the Literature
This review of the documented experiencewith intrathecal delivery of pain medicationsyielded summaries in five general categories: 1)
opioids, including morphine, hydromorphone,sufentanil, fentanyl, methadone, and meperi-dine; 2) local anesthetics (bupivacaine, ropiv-acaine, and tetracaine); 3) the adrenergic ago-
Fig. 1. Abstraction form for review of published article.
Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S15
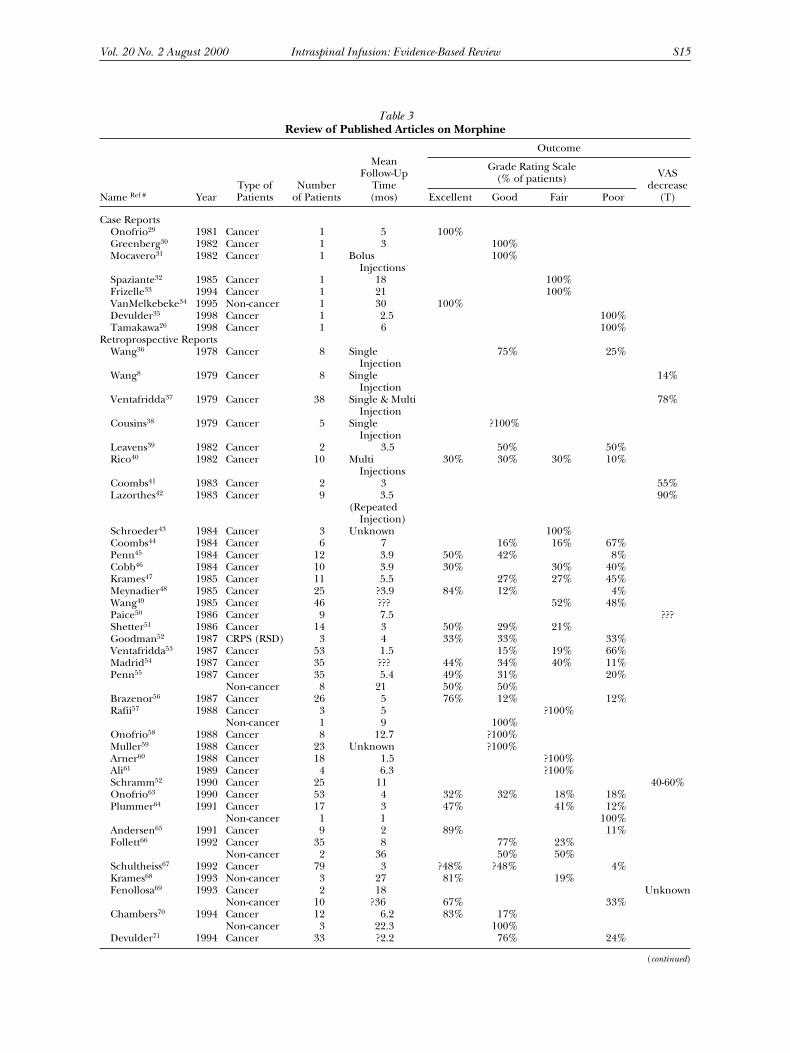
Table 3
Review of Published Articles on Morphine
Name
Ref #
YearType ofPatients
Numberof Patients
MeanFollow-Up
Time(mos)
Outcome
Grade Rating Scale(% of patients) VAS
decrease(T)Excellent Good Fair Poor
Case ReportsOnofrio
29
1981 Cancer 1 5 100%Greenberg
30
1982 Cancer 1 3 100%Mocavero
31
1982 Cancer 1 Bolus 100%Injections
Spaziante
32
1985 Cancer 1 18 100%Frizelle
33
1994 Cancer 1 21 100%VanMelkebeke
34
1995 Non-cancer 1 30 100%Devulder
35
1998 Cancer 1 2.5 100%Tamakawa
26
1998 Cancer 1 6 100%Retroprospective Reports
Wang
36
1978 Cancer 8 Single 75% 25%Injection
Wang
8
1979 Cancer 8 Single 14%Injection
Ventafridda
37
1979 Cancer 38 Single & Multi 78%Injection
Cousins
38
1979 Cancer 5 Single ?100%Injection
Leavens
39
1982 Cancer 2 3.5 50% 50%Rico
40
1982 Cancer 10 Multi 30% 30% 30% 10%Injections
Coombs
41
1983 Cancer 2 3 55%Lazorthes
42
1983 Cancer 9 3.5 90%(Repeated
Injection)Schroeder
43
1984 Cancer 3 Unknown 100%Coombs
44
1984 Cancer 6 7 16% 16% 67%Penn
45
1984 Cancer 12 3.9 50% 42% 8%Cobb
46
1984 Cancer 10 3.9 30% 30% 40%Krames
47
1985 Cancer 11 5.5 27% 27% 45%Meynadier
48
1985 Cancer 25 ?3.9 84% 12% 4%Wang
49
1985 Cancer 46 ??? 52% 48%Paice
50
1986 Cancer 9 7.5 ???Shetter
51
1986 Cancer 14 3 50% 29% 21%Goodman
52
1987 CRPS (RSD) 3 4 33% 33% 33%Ventafridda
53
1987 Cancer 53 1.5 15% 19% 66%Madrid
54
1987 Cancer 35 ??? 44% 34% 40% 11%Penn
55
1987 Cancer 35 5.4 49% 31% 20%Non-cancer 8 21 50% 50%
Brazenor
56
1987 Cancer 26 5 76% 12% 12%Rafii
57
1988 Cancer 3 5 ?100%Non-cancer 1 9 100%
Onofrio
58
1988 Cancer 8 12.7 ?100%Muller
59
1988 Cancer 23 Unknown ?100%Arner
60
1988 Cancer 18 1.5 ?100%Ali
61
1989 Cancer 4 6.3 ?100%Schramm
52
1990 Cancer 25 11 40-60%Onofrio
63
1990 Cancer 53 4 32% 32% 18% 18%Plummer
64
1991 Cancer 17 3 47% 41% 12%Non-cancer 1 1 100%
Andersen
65
1991 Cancer 9 2 89% 11%Follett
66
1992 Cancer 35 8 77% 23%Non-cancer 2 36 50% 50%
Schultheiss
67
1992 Cancer 79 3 ?48% ?48% 4%Krames
68
1993 Non-cancer 3 27 81% 19%Fenollosa
69
1993 Cancer 2 18 UnknownNon-cancer 10 ?36 67% 33%
Chambers
70
1994 Cancer 12 6.2 83% 17%Non-cancer 3 22.3 100%
Devulder
71
1994 Cancer 33 ?2.2 76% 24%
(
continued
)

S16 Bennett et al. Vol. 20 No. 2 August 2000
nists clonidine and tizanidine; 4) N-methyl-D-aspartate (NMDA) antagonists, such as dextror-phan, dextromethorphan, memantine, and ket-amine; and 5) other agents, including soma-tostatin analogs (octreotide and valpreotide);baclofen, ziconotide, midazolam, neostigmine,aspirin, and droperidol.
Opioids
Morphine
During the 1970s, the discovery of spinal opi-oid receptors aroused interest in intrathecaladministration of morphine.
1–28
Three majortypes of opioid receptors (mu-, kappa-, anddelta-) have been identified.
4
The mu-recep-tors mediate the major effects of morphine,such as analgesia and respiratory depression.
5
Though subtypes of the mu-receptors havebeen proposed,
6
no useful drugs have arisenthus far from the hypothesized classification.Other studies have found a high concentrationof these receptors in the substantial gelatinosaof the dorsal horn, a major site for early inte-gration of nociceptive input.
7,8
There are no data on either efficacy or safetyfrom controlled clinical trials investigating in-trathecal morphine. There are, however, numer-ous published case reports and retrospectivestudies with a smaller number of published pro-spective and multicenter studies. In these articles,over 2,000 patients, with chronic cancer and non-cancer pain, are reported to have received in-trathecal morphine (Table 3).
8,26,29–87
Intrathecal morphine is considered to be ap-proximately ten times more potent than thesame amount administered epidurally (i.e., 0.5mg intrathecal morphine produces equivalentanalgesia of 5 mg epidural). Because of thesmall volume of distribution (approximately 70mL), the intrathecal morphine dose yields acerebrospinal fluid (CSF) concentration muchhigher than that which occurs with vascular ab-sorption following epidural administration.
11
Also, since the rate of elimination from the CSFmorphine is similar to the rate of eliminationfrom plasma, the duration of action is relativelylong (apparently due to the high concentrationfound in CSF).
12
Following intrathecal adminis-tration, morphine is not detected in the plasmafor the first 2 hours after injection.
10
Slow rostral
Table 3 (continued)
Name
Ref #
YearType ofPatients
Numberof Patients
MeanFollow-Up
Time(mos)
Outcome
Grade Rating Scale(% of patients) VAS
decrease(T)Excellent Good Fair Poor
Cherny
72
1995 Cancer 4 Unknown UnknownBecker
73
1995 CRPS (RSD)
2 57 50% 50%
Bloomfield
74
1995 Non-cancer 50 39 78% ?11% ?11%Paice
75
1996 Cancer 200 ?14.6 ?52% ?43% ?5%Non-cancer 100 ?14.6 ?52% ?43% ?5%
Winkelmuller
76
1996 Non-cancer 112 40.8 23% 23% 26% 28%Tutak
77
1996 Non-cancer 26 23 50% 27% 19% 4%Gestin
78
1997 Cancer 50 5 ?50% ?50%Sallerin-Caute
79
1998 Cancer 159 3 ?40% ?40% 17% 3%Gilmer-Hill
80
1999 Cancer 9 4.5 ?50% ?50%Prospective Reports
Hassenbusch
81
1995 Non-cancer 18 29 33% 28% 39%Angel
82
1998 Non-cancer 11 27 45% 27% 27%Anderson
83
1999 Non-cancer 30 24 20%Multicenter Reports
Rawal
84
1987 Cancer 70% Unknown UnknownSwedenAnesthDepts.
Yaksh
85
1987 Cancer 133 13 Unknown(130),
Non-cancer(3)
Ballantyne
85
1996 Cancer 186 Unknown 58% Unknown Unknown 6.3%Dahm
87
1998 Non-cancer 323 19.5 Unknown ?88% Unknown Unknown

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S17
spread is thought to be responsible for “delayed”respiratory depression.
13–16
This rostral redistri-bution of morphine is one factor associated withthe clearance of morphine from the CSF.
17
Elimination also occurs by vascular absorp-tion via the blood supply to the spinal cord.
18
The similarity between the duration of actionand the rate of morphine recompartmentaliza-tion from the CSF to plasma indicates limitedmetabolism in the spinal cord.
19
In the chronicinfusion situation, the metabolite morphine-6-glucuronide (M-6-G) is thought to play alarger role. M-6-G to morphine ratios varygreatly.
20
In two animal studies, the potency ofM-6-G given intrathecally was 10–45 times thatof morphine.
21–23
The metabolites were foundto enter the CSF from the plasma as well as be-ing created in situ by the brain following in-tracerebroventricular injections.
24
There have been no large-scale, randomizedcontrolled trials investigating intrathecal mor-phine. Anecdotal reports suggest the potentialfor good to excellent pain relief, taking into ac-count morphine’s dose characteristics (Table 4).
Hydromorphone
Few studies of intrathecal hydromorphonefor pain have been performed, and there havebeen no controlled trials. It is likely that in-trathecal hydromorphone is widely used be-cause it is more potent than morphine andtherefore allows longer periods of time be-tween without refills, and causes fewer side ef-fects. Hydromorphone’s potency appears to beabout five times that of morphine, but the side-effect profile is equivalent to or better than thatof morphine.
83
There have not been any spe-cific reports of unexpected side effects in theanecdotal reports that have been published.
Sufentanil
There has been a substantial amount of bothhuman and animal research investigating the
use of sufentanil in the management ofpain.
88–102
Sufentanil is a selective mu-receptoropioid analgesic, the thienyl analog of the4-anilinopiperidine, fentanyl,
88
and is highly li-pophilic.
89
Most of intrathecally administeredsufentanil is cleared from the CSF by diffusionvia the epidural space into the epidural fat,systemic circulation, and diffusion into the spi-nal cord.
Animal data on neurotoxicity are conflictingand warrant caution with intrathecal use ofhigh doses of sufentanil. Intrathecal sufentanilhas been studied in cats, sheep, and dogs forinfusions ranging from 1–28 days.
93–96
No drug-related neurotoxicity was found with low tomoderate repeated doses.
95
Large doses (7.5
m
g/kg) of intrathecal sufentanil in sheep wereassociated with moderate behavioral responses(i.e., agitation, rigidity, vocalization), hind limbweakness, and histologic neuronal changes (e.g.,spongiosis, chromatolysis).
In humans, short-term use of small doses ofepidural or intrathecal sufentanil for postoper-ative or labor pain control has been associatedwith no obvious neurotoxicity. Sufentanil, whendelivered by epidural or intrathecal routes inthese clinical settings, showed comparable paincontrol and similar plasma concentrations re-gardless of the administration route. Side ef-fects consisted of rare early respiratory de-pression, nausea, vomiting, somnolence, andrare urinary retention. However, compared tomorphine, these side effects seemed less fre-quent.
91,97–99
The limited data on long-termepidural or intrathecal use in the treatment ofchronic malignant and non-malignant painsuggest that this drug can be infused withoutclinical signs of neurotoxicity.
During long-term follow-up, intrathecal infu-sion of sufentanil was found to be effective inthe treatment of pain. Side effects were rareand not significantly different from those thatoccur with long-term morphine infusion. Onepossible exception is that there appears to be alower incidence of peripheral edema withsufentanil. Pain control was comparable to pre-vious reports with morphine long-term infu-sion.
100,101,103
Fentanyl
The use of intraspinal fentanyl has been ex-tensively reported.
103–131
However, there are no
Table 4
Morphine: Summary of Dose Characteristics
• Dose may stabilize for long periods• Dose escalation commonly occurs• Dose escalation may have multiple causes (i.e., tolerance
progressive disease)

S18 Bennett et al. Vol. 20 No. 2 August 2000
randomized controlled clinical trials on theuse of epidural or intrathecal fentanyl. Thereare three non-controlled retrospective studiesof the efficacy of “long-term” intraspinal fenta-nyl, and a small study in cancer patients receiv-ing intrathecal fentanyl.
Fentanyl is a highly potent mu-receptor opi-oid agonist with a high degree of lipid solubility.Rapid clearance following intraspinal adminis-tration to the circulation results in clinically rel-evant plasma levels. Even after an epidural bolusor short-term (
,
24 hour) epidural infusion, itis likely that systemic redistribution contributesto fentanyl analgesia.
107,113–116,127,130
Moreover,because of the marked inter-individual differ-ences in concentrations of epidural fentanyl ap-pearing in plasma,
118
results from small studiesthat measure leakage in plasma are difficult tointerpret.
There are three retrospective studies evalu-ating the efficacy of intraspinal fentanyl. Themost extensive study
104
described 551 patientstreated for non-malignant lower-back pain withcontinuous epidural infusion of bupivacaine/fentanyl/droperidol. Most were treated via apump and some via an implanted pump. Mostreceived an infusion of 2 mL/hr containingfentanyl 5 mcg/mL, bupivacaine 9 mg/mL,and droperidol 0.05 mcg/mL. The infusionwas repeated 2–9 times (mean: 6.9) for a totalof 3,108 treatments, over a mean duration of19.8 days (range: 2–81 days). Time between in-fusions ranged from 6 to 184 days (mean: 12days). Pain relief was reported to be “excel-lent” in 73% and “good” in 26.5% of patients;no serious side effects were noted.
Another study
120
described the treatment of40 terminal cancer patients who received in-trathecal fentanyl via an external portablepump up to eleven months. The dose of fenta-nyl was not specified, but no serious complica-tions were observed; supraspinal side effectswere only seen during the first week.
Methadone
There are no randomized, controlled clini-cal trials of methadone given by long-term epi-dural or intrathecal infusion. There are nostudies of any kind of the effects of long-termintrathecal methadone infusions.
Interpretation of the literature on metha-done’s effects
17,124,132–151
is greatly complicated
by the recent discovery that the d-isomer ofmethadone is a moderately potent antagonistof the NMDA receptor (with no significant ac-tivity at the mu-receptor). The l-isomer has triv-ial activity at the NMDA receptor; its analgesiceffects are completely reversible by naloxoneand thus ascribable to the mu-receptor alone.The clinically available methadone in theUnited States (Roxane Laboratories) is the ra-cemic mixture. But the methadone used inGermany,
142
and perhaps elsewhere in Europe,Israel, and other countries, may be the l-iso-mer. Reports in the literature often fail to spec-ify the source of drug, and whether it is thel-isomer or the racemic. The NMDA-blockingaction contributed by the d-isomer in a typicaldose of the racemate is very likely to be clini-cally relevant.
133,146
Meperidine
There has been little information publishedon the use of intraspinal meperidine in thetreatment of pain.
153–158
Meperidine is a syn-thetic phenylpiperidine structure with local an-esthetic-like effects. It is capable of both sensoryand motor blockade, and its local anesthetic-likeeffect is not blocked or reversed by naloxone.There is some evidence that the local anestheticeffect occurs not in the dorsal horn of the spinalcord, but at the actual nerve root levels.
The stability data on meperidine show thatcompared to morphine, it is rapidly eliminatedfrom the CSF. This is due to its higher lipid solu-bility. Following intrathecal delivery, morphineis found to have much higher CSF concentra-tions as compared to plasma concentrations. Be-cause meperidine is more lipid soluble thanmorphine, there is also less cephalad spreadcompared to morphine, owing to its higherlipid solubility.
157
There are no published dataavailable on the compound’s stability for long-term intrathecal use (i.e., within a pump reser-voir at 37
8
C). Anecdotal data indicate it to bestable at 37
8
C for 90 days.Toxicity data are also limited and question-
able. There is one case report of the intrathecalinfusion of meperidine that showed no evidenceof toxicity or adverse effects long term.
158
Potential advantages of meperidine includeits combined opioid and local anesthetic prop-erties, intermediate lipid solubility, and stabil-ity at 100 and 200 mg/cc concentrations. In

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S19
limited cases, there has been no overt toxicity,and use of meperidine having a pH near 4.0did not appear to affect pump performance.Anecdotal experience might indicate that a pH
$
4.0 might lessen the likelihood of pump fail-ure. Additional study of this drug is warranted.
Local Anesthetics
Bupivacaine
Bupivacaine is a local anesthetic agent of theamide class. The use of bupivacaine by contin-uous infusion via the epidural or intrathecalroute has gained interest over the past fewyears. At this point, there is a great deal of epi-dural data regarding efficacy, side effects, toxic-ity, stability, and cost-effectiveness when deliv-ered by this method (Table 5). The neuraxialuse of this agent has been primarily in the post-operative patient for pain reduction and in theobstetrical patient to aid in comfort during deliv-ery. The use of bupivacaine by continuous infu-sion in the intrathecal space is becoming morecommon.
159–194
There have been no long-termrandomized prospective studies examiningthe efficacy of bupivacaine in intrathecal ad-ministration.
Neurotoxicity studies suggest bupivacaine issafe in humans at clinically relevant doses forintrathecal use. Toxicity data in animals alsoappear favorable at clinically relevant doses.Studies in dog, cat, and sheep models haveshown no toxicity in concentrations well abovethose used in humans.
174–176
Pharmacokinetic
evaluations
177,178
indicate that the systemic ab-sorption of bupivacaine by neuraxial infusiondoes not appear to be affected by age, coexistingdisease, or gender. Renal disease does not ap-pear to have an effect short term, but no long-term studies are available. Pharmacokinetic andpharmacodynamic properties of bupivacaineare well defined and used to determine appro-priate intraspinal dosing and effect.
195,196
In epidural dosing, studies suggest that thetotal dose is more important than the volumeadministered. Epidural bupivacaine has beenshown to be synergistic with epidural opioids. An-ecdotally, the combination of these two drugs ap-pears to be helpful in reducing rapid sensitiza-tion, reducing side effects, and improving overallpain relief.
197–199
The published opioids adminis-tered with bupivacaine include morphine, fenta-nyl, sufentanil, hydromorphone, methadone, andmeperidine.
199–203
Based on the currently available literature, itappears that intrathecal bupivacaine is a safeand acceptable method for providing pain re-lief in both cancer and non-cancer patients. Atthis point, intrathecal bupivacaine appears tobe a clinically efficacious addition to intrathe-cal opioids. Toxicity studies primarily in cancerpatients appear to show no intrathecal toxicityat clinically significant doses. In a small pro-spective study, Sjoberg and co-workers
172
failedto find neurological deficits associated with in-trathecal bupivacaine and morphine. This wascorroborated in other studies that failed to findclinically significant neurohistologic effects.171
Larger studies indicated that there was rare tox-icity when systemic complaints were analyzed.170
Retrospective analysis185 also indicated lack ofsignificant side-effect risks, directly attributableto bupivacaine.
In another small study with non-cancer pa-tients, addition of bupivacaine to intrathecal opi-oids was more effective than opioids alone.68
Also, Sjoberg and co-workers192 reported in astudy of 53 cancer patients that a bupivacaineand morphine combination was more effectivethan high doses of bupivacaine alone (withlower complication rates than bupivacainealone). In a prospective study of 47 non-cancerpatients, Anderson and Burchiel83 observed a50% response rate after 2 years (i.e., visual ana-log scale, McGill pain questionnaire, chronic ill-ness problem inventory) following intrathecaltreatment of morphine/bupivacaine or hydro-
Table 5Bupivacaine Efficacy Summary Based on
Epidural Experience
• Improved visual analogue scale (VAS), McGill, Chronic Illness Inventory
• Significantly higher patient satisfaction with intrathecal dosing than with epidural, less complications than with epidural infusion
• Bupivacaine spares morphine dosing, oral and intrathecal• Improved sleep, gait, and daily activities• Failure higher with personality disorders, narcotic
dependence, neurotic disturbances, widespread pain patterns, social problems
• Intrathecal treatment provides better relief than epidural infusion: sleeping and walking patterns improved with intrathecal infusion
• Decreased need for opioids and decreased VAS• Improved outcome combined with intrathecal opioids

S20 Bennett et al. Vol. 20 No. 2 August 2000
morphone/bupivacaine. Most reported compli-cations in animal studies suggest problems atplasma levels that would not be seen at clinicallyrelevant doses of intrathecal bupivacaine. Avail-able studies indicate stability in both in vitro andin vivo analysis.
Additional studies are needed to documentstability in an intrathecal pump at body tem-perature. The bacteriostatic properties appearto be favorable as well. This is based on bupi-vacaine being bacteriostatic at clinical concen-trations on multiple bacteriological organ-isms.204–206 Further studies are also needed todefine future use of intrathecal bupivacaine.Studies should include long-term toxicity,long-term neuropathology, and compatibilitystudies when used in combination with otheragents. Further studies are needed also to dif-ferentiate types of pain syndromes for whichbupivacaine is most effective.
RopivacaineRopivacaine is an amide-type local anes-
thetic. The relative affinity of this drug for theA-delta and C fibers over A-beta fibers makes itan excellent choice for analgesia without motorloss. Studies demonstrate that it has less affinityfor motor blockade with effective sensory block-ade when compared to bupivacaine.207,208 Withlower lipid solubility than bupivacaine, it is a bitmore available for spread within the intrathecalspace.209
There is no literature on the safety and effi-cacy of long-term intrathecal use of ropi-vacaine. Most of the reported experience hasbeen with short-term epidural use for postop-erative pain.207–216
There is a fairly large amount of toxicity datain the literature on ropivacaine, in which it ap-pears to be approximately 25% less toxic to theCNS and especially to the cardiovascular systemthan bupivacaine (i.e., comparing epidural in-fusions of either drug at a rate of 10 mg/min,to a maximum dose of 150 to 250 mg).207,210 Ad-verse effects of ropivacaine are similar to that ofbupivacaine and the other local anesthetics.The major advantages of ropivacaine in com-parison to bupivacaine are that it is somewhatless toxic; it is more selective for sensory versusmotor nerves between the sensory and motorblockade, and it has lower lipid solubility re-sulting in greater spinal segmental spread. Itsdisadvantages are that it is less potent than
bupivacaine; it has a shorter duration of ac-tion; it has biphasic time-dependent pharma-cokinetics, with gradually increasing totalplasma concentrations and decreasing totalclearance.
Human data on short-term epidural ropi-vacaine use for postoperative pain (2 mg/mLbegun at a rate of 6 mL/h for 63 to 72 hours ofinfusion in 10 patients) suggests doses some-what higher than bupivacaine would have agreater therapeutic window.208 When it was ti-trated to achieve a stable sensory block, therewas a low incidence of motor block, and ropi-vacaine levels in plasma were well below thetoxic range.
TetracaineTetracaine is an ester-linkage-type local anes-
thetic, similar in structure to procaine. It is re-constituted from commercially available pow-der form, and therefore can be tailored tospecific concentrations from low to ultra-highconcentrations due to its very high solubility inaqueous solutions. Little research has beendone on the long-term intrathecal delivery ofthis drug, but there is some significant re-search on short-term delivery of intrathecal tet-racaine.152
Toxicity from intrathecal tetracaine was sug-gested by several cases of cauda equina syndromeresulting from continuous spinal anesthesia inhumans and animals with tetracaine.152,217,218 Astudy using a rat model to assess maldistributionand sustained concentration suggested that thetoxicity was caused by maldistribution of thedrug, which overwhelmed the buffering capabil-ity of the CNS. Tetracaine’s low pH may increasethe chances of toxicity. Despite its potential ad-vantages, long-term intrathecal use is not sup-ported.
Adrenergic AgonistsClonidine and Tizanidine
Although the a-2–adrenergic agonists tizani-dine and clonidine have been extensively stud-ied in animal models; there are few clinicalstudies.170,219–225,235–258,260 For example, publishedsafety studies with 28-day epidural infusions ofclonidine in dogs revealed no safety issues.238
Controlled trials of epidural use in cancer pa-tients as well as normal adult volunteers exists in

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S21
the literature, as does an analgesia study in can-cer patients.225,249,255,256
The predominant side effects reported inthe animal and human reports for both drugsare supraspinal, spinal, and peripheral cardio-vascular effects resulting in a dose-dependentbradycardia and blood pressure changes. Sur-veys and case reports indicated both safety andefficacy, but most were not controlled stud-ies.170,226–233
Tizanidine is not available in the UnitedStates as an injectable agent.234 The animalstudies seem to show a dose-related hypoten-sion, but to a degree less than that ascribed toclonidine. No spinal cord changes were ob-served at doses ten times greater than thera-peutic doses.234–236
Leiphart and co-workers and Levy et al., in arat sciatic nerve model, showed that both intra-thecal morphine and tizanidine were (equally)effective for neuropathic pain,235,257 but Ono andcolleagues, working with a similar model, showedthat clonidine and tizanidine were both superiorto opioids in control of neuropathic pain.258 Inneuropathic models, thermal hyperalgesia andtactile allodynia was reversed by intrathecal a-2–adrenergic agents, including clonidine and tiza-nidine.259
In human volunteers, Eisenach and co-workers249 described the positive results of acontrolled trial of epidural titaridine deliveryfor thermal- or capsaicin-induced pain and hy-peralgesia. Clonidine was also found to be effec-tive in the control of complex neuropathic painstates in a randomized double-blind study of 85cancer patients with morphine rescue (56% suc-cessful response for the clonidine arm vs 5% forplacebo),225 and also by Mercadante and Tum-ber in another report, who proposed a role forclonidine in a cancer pain algorithm.255,256
Those studies that looked at pain character andspecifically at neuropathic pain showed thegreater effect of clonidine in this patient popu-lation. Based on results from controlled studies,additional investigation is warranted.
NMDA AntagonistsGlutamate is the most abundant excitatory
transmitter in the central nervous system. It ex-erts its action principally through the AMPA(adenosine monophosphate) receptor and the
NMDA receptor. The release of glutamate andoccupancy of the NMDA receptor serves to de-polarize the membrane and increase intracel-lular calcium. The opening of the channel maybe prevented by 1) competitively antagonizingthe occupancy by glutamate of the receptor(i.e., drugs AP5 or CPP CGS19755.); 2) block-ing the channel (ketamine, memantine, MK801,or CNS5161); or 3) blocking the allostericallycoupled glycine site (i.e., 7 Cl-kynurenic acidor the drug ACEA 1021).
A wide variety of drugs have been synthesizedthat interfere with NMDA receptor function.The majority of these agents are noncompeti-tive, use-dependent antagonists that block theNMDA ionophore channel.96,146,237,261–314
NMDA delivery by the spinal (epidural or in-trathecal) route has been limited principally tothe use of ketamine. A single case study re-ported using intrathecal administration of thedrug CPP, a receptor antagonist.
Aside from analgesic effects, the spinal deliv-ery of NMDA receptor antagonists has uni-formly produced a dose-dependent incidenceof motor dysfunction characterized by weak-ness and hypotension. Preclinical safety studieshave shown little, if any, spinal toxicity in ratmodels, but extended intrathecal infusionstudies carried out in well-characterized dogand sheep models with MK801, ketamine, dex-tromethorphan, dextrorphan, memantine,and the drug AP-5 revealed certain signs of spi-nal cord parenchymal inflammation and in-jury. It is not clear whether the pathology re-sults from a blockade of the NMDA receptor orwhether it represents an effect of these drugsat other molecular targets. These effects arelikely mediated at the spinal level (interme-diolateral cell column neurons) and reflect theexcitatory role of glutamatergic receptors.237
Lower doses in dogs resulted in minimaleffect289 on motor neuron excitation gener-ated by spinopetal cells and interneurons.
Nonspinal effects resulting from redistribu-tion of intrathecal agent to the vascular poolinclude all of the signs typically observed aftersystemic delivery. These include sedation and ageneral behavioral dysfunction including hy-permobility.
Combined with the results obtained fromone study using intrathecal CPP, the resultswith ketamine emphasize the likelihood thatNMDA receptor blockade can reduce pain.

S22 Bennett et al. Vol. 20 No. 2 August 2000
However, these studies do not adequately dis-sociate the spinal action from the systemic ef-fects of low doses of ketamine. In addition, it isdifficult to determine the role played by possi-ble “local anesthetic-like” action.277,315
Spinal NMDA receptors play an importantrole in post-tissue and nerve injury pain pro-cessing, and in the development of tolerance,but currently available drugs must be consid-ered to have a suspect safety profile. Moreover,redistribution of these agents may result in su-praspinal side effects at therapeutic dose.
Octreotide and VapreotideVery little research has been done on the use
of the somatostatin analogue octreotide in-trathecally for pain, and none has been per-formed for vapreotide.316,317 In anecdotal re-ports, an intrathecal dose of 15 to 20 mg/hrproduced a marked decrease in patient pain.
The preclinical literature on pain mecha-nisms suggests that somatostatin or its analoguescould be useful in the intrathecal treatment ofpain. However, the considerable literature re-lated to the spinal actions of spinal somatostatin(beyond the scope of this review) raises safetyquestions. Additional studies are warranted.
Other AgentsBaclofen
Intrathecal baclofen is a standard therapyfor spasticity. A number of animal experimentshave suggested that gamma amino bulyric acid-A (GABA-B) agonists may be helpful in decreas-ing nociceptive responses. Since safety studiesdemonstrated that intrathecal infusion of ba-clofen posed no direct toxicity issues, these haveled to a number of clinical studies using intra-thecal baclofen for nociceptive pain.318–320 Theintrathecal infusion of baclofen has been rarelyreported to be effective for chronic pain fromcauses other than spasticity. However, a recentreport of 5 patients, followed for 6–20 months,showed an average 76% reduction in pain fromphantom pain, arachnoiditis/epidural scarring,lumbar plexopathy, and sciatic neuropathy.321
ZiconotideZiconotide, or SNX 111, an omega-conopep-
tide, is a 25 amino acid peptide from thevenom of the Conus magus, a piscivorous ma-
rine snail. There is a small but important bodyof literature describing ziconotide.322–328 It is ahighly selective N-type voltage-sensitive cal-cium channel antagonist. These N-type volt-age-sensitive calcium channels (VSCCs) arefound at the presynaptic nerve terminals in thespinal dorsal horn. The presumed mechanismof action of SNX 111 in analgesia is the block-ade of neurotransmitter release at the primaryafferent nerve terminal. There is some evi-dence that opioid receptors are connected tothe N-type VSCC, through a G-protein, and it ispossible that some of the acute effects pro-duced by opioids are mediated by inhibition ofN-type calcium channels.322–324
No data are available on the long-term in-trathecal use of SNX 111 either in humans orin animals. Penn and co-workers described nu-merous adverse effects in 3 patients with in-trathecal infusions of ziconotide, includingnystagmus, dysmetria, ataxia, sedation, agita-tion, hallucinations, and coma. Many of thechanges appeared to require days or weeks toclear after stopping or reducing the dose ofthe drug.330
In animal models of acute and neuropathicpain, ziconotide has been found to be consis-tently effective without the development of tol-erance during seven days of infusion.325,326 Theanalgesic effect and the side effects appear tobe dose-related. Recently, Ridgeway and col-leagues reported that ziconotide was useful inthe treatment of severe spasticity after spinalcord injury.329
MidazolamHuman safety studies have not been done.
Analgesia has been observed in postoperativepatients when midazolam is combined with lo-cal anesthetics or opiates, but only anecdotalreports with subarachnoid administration ofmidazolam and morphine are available onlong-term use.331
Preclinical studies suggest concerns aboutthe safety of midazolam during intrathecal in-fusion.331–334 In one study, Erdine and col-leagues gave rabbits 0.3 mg midazolam (pH3.3) intrathecally for 5 days.332 On light andfluorescent microscopy of transverse spinalcord sections, midazolam was found to causesignificant histologic and spinal cord toxicity.They observed histologic and vascular lesions,fibrosis, and actual cell death associated with

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S23
administration of midazolam. Svensson andcolleagues at Uppsala University in Swedenalso showed significant changes in dorsal hornand microglial cells in the animals that weretreated with midazolam.333 Schoeffler and co-workers331 and Edwards et al.334 observed nodifference compared to control when assessingsubarachnoid administration in rats. In theirarticle describing their preclinical data withrats, Schoeffler and co-workers also reportedthat in 2 patients with chronic neoplastic painresistant to morphine, addition of midazolamwas effective in controlling pain.331
These neurotoxicity studies raise seriousconcerns about the use of this drug. Muchmore work needs to be completed prior to rec-ommending midazolam for standard use in in-trathecal pain management.
NeostigmineNeostigmine is an acetylcholinesterase inhibi-
tor and appears to produce consistently effectiveanalgesia in the postoperative setting.335–339 Inrandomized controlled trials, neostigmine causeslittle or no neurotoxicity340,341 although nauseaand vomiting, particularly at higher doses (50–200 mg) have been seen in perioperative and vol-unteer settings.
In sheep, rat, and dog models, neostigmineappears to be a safe compound with no histo-logic or spinal cord toxicity. In the mid 1990s,the preservative-free form of neostigmine wasdiscontinued, leaving only the methyl-propylpa-raben form. Gürün and collaborators342 studiedneostigmine with a methyl preservative formu-lation and found that the chronic intrathecal ad-ministration of neostigmine was safe in ratsand sheep.
Although efficacy and safety trials in peri-and postoperative settings (orthopedics, volun-teer, oncology, and obstetrics) have shownconsistently good outcome with effective anal-gesia, there are, however, no data on long-termuse. Neostigmine may also show promise foruse in adjuvant or co-analgesic therapy.
AspirinThe use of aspirin in the intrathecal manage-
ment of pain has become a focus of attentionrecently.343–354 The mechanism of action for theintrathecal injection of aspirin, which probablyexists at the spinal level, is inhibition of pro-staglandin synthesis, causing dose-dependent
hypoalgesia. Previous studies have shown thatprostaglandins can block endogenous pain con-trol mechanisms by inhibiting the bulbospinalnoradrenergic component of the descending an-tinociceptive system.343
In the human, there have been two retro-spective studies involving a total of 5 cancer pa-tients and 67 non-cancer patients. All patientswere treated with a single intrathecal bolusthat provided pain relief from 1–30 days. It isdifficult to determine if there were any long-term neurologic examinations or side effects ofthese patients after the single injection. The ef-ficacy was 57%, 78%, and 100%.
Human toxicity appeared to be short-termand consisted of generalized fatigue and hallu-cinations at night. More detailed studies involv-ing other patients with long-term follow-up, es-pecially during and after long-term continuousintrathecal infusion, are not available in the lit-erature. Examination of this drug in other ani-mal species for safety has likewise not beendocumented.
DroperidolClinical studies, including two randomized
controlled trials, a retrospective study, and onecase report, have shown that a low dose of dro-peridol given epidurally can potentiate the anti-nociceptive effect of epidural morphine.355–359
Grip and co-workers demonstrated that dro-peridol itself or in combination with morphinehad no antinociceptive effects. They also ex-erted no histopathologic effect on the ratspinal cord.355 This discrepancy between previ-ous clinical findings and experimental painstudies suggests different modes of action ofdroperidol in humans and rat models. Re-search is needed to determine whether epidu-ral administration of the dopamine antagonistdroperidol may be beneficial as supplementarymedication to epidural opioids when tolerancedevelops.
DiscussionClearly, further research in the intrathecal de-
livery of pain medication is warranted. Clinical ef-ficacy in large-scale randomized controlled trialsutilizing intrathecal delivery of most compoundshas not been demonstrated, and variations be-tween study designs make useful comparisons ofexisting studies difficult. Generally, the scientific

S24 Bennett et al. Vol. 20 No. 2 August 2000
quality of the published studies is variable, withresults obtained from limited numbers of pro-spective controlled studies (many with inade-quate patient group size), uncontrolled clinicalstudies, case reports, retrospective studies, andanecdotes. However, clinical use of the agentshas less rigid aims, criteria, and endpoints thanacademic/clinical research. Data on drug inter-actions, toxicity, and long-term safety for severalcompounds is also incomplete. Preliminary re-sults with several promising agents warrant fur-ther study in randomized controlled trials—animportant criterion for evidence-based medicineas well as acceptance into widespread clinicalpractice.
Periodic surveys of the preclinical and clini-cal literature are important in comparing thesediverse data. For example, in their recent,thorough review, Wallace and Yaksh360 dis-cussed classes of spinally delivered analgesicagents (including clinical experience), toler-ance, safety evaluation, drug delivery tech-niques, morbidity and economics of chronicspinal delivery, and patient screening. The ex-pert panel hopes that the evidence-based re-view presented here will also provide a criticaltool that other investigators may use while ac-cumulating clinical experience with promisingcompounds and studying them in randomizedtrials.
Based on this review of the literature, in-trathecal morphine appears to be safe at clini-cal concentrations, and has favorable efficacydata. Limited information on the other opioidclasses also appears favorable from both a toxi-cology and efficacy standpoint, although pub-lished literature supporting this is very limited.Ongoing research and evaluation is needed todefine the best clinical settings in which to utilizethese compounds as an alternative to morphine.While some studies support the clinical use ofmethadone and meperidine, other studies reportpossible concerns with human use on a long-term, continuous infusion basis, and possible in-compatibility with intrathecal infusion pumps.
Bupivacaine is the only local anesthetic thatcurrently has favorable data for both clinical ef-ficacy and toxicology. Other local anestheticsare being used clinically at this time, but re-search is incomplete regarding this practice.Based on the currently available literature,both clinical efficacy and toxicology for cloni-dine appear favorable. Many anecdotal reports
indicate markedly improved outcomes in pa-tients who previously failed opioid infusions assole agents. Combinations of different drugclasses such as opioids/local anesthetics, opio-ids/clonidine, and opioids/local anesthetics/clonidine are currently being used in clinicalpractice. The efficacy reports appear favorable,but are based largely on case studies and retro-spective analysis. No information is availableon the long-term compatibility of these combi-nations.
Several new agents appear to have the inter-est of both practitioners and researchers forthe future treatment of intractable pain disor-ders. Research on gabapentin, aspirin, NMDAantagonists, naloxone, calcium channel block-ers, midazolam, and cyclooxygenase-2 inhibi-tors appear to be on the horizon, and mayeventually lead to the discovery of clinically rel-evant treatments.
Further research is needed to determine thebest clinical application for many of the com-pounds currently used in clinical practice. Dataare limited on the compatibility of drug combi-nations, dose ranges, and long-term safety formany agents currently identified as clinicallyrelevant. Information is also incomplete re-garding the long-term effects of drug combina-tions on intrathecal catheters and infusion de-vices. Hopefully, the information that thepanelists have provided in this critical reviewwill provide a basis and rationale for future evi-dence-based research in the safety and efficacyof promising agents, either singly or in combi-nation, used in long-term intrathecal infusionsfor pain relief.
References1. Boerner U, Abbott S, Roe RL. The metabolism
of morphine and heroin in man. Drug Metab Rev1975;4:39–73.
2. Mather L. Opioid pharmacokinetics and phar-macodynamic factors. Clin Anesthesiol 1983;1:17–40.
3. Yaksh TL, Rudy TA. Analgesia mediated by adirect spinal action of narcotics. Science 1976;192:1357–1358.
4. Pasternak GW. Basic pharmacology of opioids.In: Bowdle T, Horita A, Kharasch E, eds. The phar-macologic basis of anesthesiology. New York:Churchill Livingstone, 1994:19–36.
5. Bowdle TA. Adverse effects of opioid agonists

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S25
and agonist-antagonists in anesthesia. Drug Safety1998;19:173–189.
6. Moskowitz AS, Goodman RR. Autoradio-graphic distribution of mu1- and mu2-opioid bind-ing in the mouse central nervous system. Brain Res1985;360:117–129.
7. Herkenham M, Pert CB. Light microscopic lo-calization of brain opiate receptors: a general auto-radiographic method which preserves tissue quality.J Neurosci 1982;2:1120–1149.
8. Wang JK, Nauss LA, Thomas TE. Pain relief byintrathecally applied morphine in man. Anesthesiol-ogy 1979;50:149–151.
9. Weddel SJ, Ritter RR. Epidural morphine: se-rum levels and pain relief. Anesthesiology 1981;54:210–214.
10. Jorgensen BC, Anderson HB, Engquist A. CSFand plasma morphine after epidural and intrathecalapplication. Anesthesiology 1981;55:714–715.
11. Nordberg G. Pharmacokinetic aspects of spinalmorphine analgesia. Acta Anaesthesiol Scand 1984;28(Suppl 79):2–38.
12. Nordberg G, Hedner T, Mellstrand T, Dahl-strom B. Pharmacokinetic aspects of intrathecal mor-phine analgesia. Anesthesiology 1984;60:448–454.
13. Gustafsson LL, Post C, Edvardsen B, RamsayCH. Distribution of morphine and meperidine afterintrathecal administration in rat and mouse. Anes-thesiology 1985;64:483–498.
14. Gregory MA, Brock-Utne JG, Bux S, DowningJW. Morphine concentration in brain and spinalcord after subarachnoid morphine injection in ba-boons. Anesth Analg 1985;64:929–932.
15. Gourlay GK, Cherry DA, Cousins MJ. Cephaladmigration of morphine in CSF following lumbar epi-dural administration in patients with cancer pain.Pain 1985;23:317–326.
16. Downing JW, Williams V, Hascke R, et al. Ros-tral spread of epidural morphine. Anesth Analg1984;63:371–376.
17. Payne R, Inturrisi CE. CSF distribution of mor-phine, methadone, and sucrose after intrathecal in-jection. Life Sci 1985;37:1137–1144.
18. Moore A, Bullingham R, McQuay H, Allen M,Baldwin D, Cole A. Spinal fluid kinetics of morphineand heroin. Clin Pharmacol 1984;35:40–45.
19. Sandouk P, Scherrmann JM, Chauvin M. Rate-limiting diffusion processes following intrathecal ad-ministration of morphine. Eur J Clin Pharmacol1986;30:575–579.
20. Faura CC, Collins SL, Moore RA, McQuay HJ.Systematic review of factors affecting the ratios ofmorphine and its major metabolites. Pain 1998;74:43–53.
21. Shimomura K, Karmata O, Ueki S, et al. Anal-gesic effect of morphine glucuronides. J Exp Med1971;105:45–52.
22. Pasternak GW, Bodnar RJ, Clarke JA, InturrisiCE. Morphine-6-glucuronide, a potent mu agonist.Life Sci 1987;41:2845–2849.
23. Sullivan ARF, McQuay HJ, Bailey D, DickensonAH. The spinal antinociceptive actions of morphinemetabolites: morphine-6-glucuronide and normor-phine in the rat. Brain Res 1989;482:219–224.
24. Sandouk P, Serrie A, Scherrmann JM, Lang-lade A, Bourre, JM. Presence of morphine metabo-lites in human cerebrospinal fluid after intracere-broventricular administration of morphine. Eur JDrug Metab Pharmacokinet 1991;3:166–171.
25. Tanelian DL, Cousins MJ. Failure of epiduralopioid to control cancer pain in a patient previouslytreated with massive doses of intravenous opioid.Pain 1989;36:359–362.
26. Tamakawa S, Iwanami Y, Ogawa H. High doseintrathecal morphine to control cancer pain—acase report. J Pain Symptom Manage 1998;15:70–72.
27. Suzuki R, Chapman V, Dickenson AH. The ef-fectiveness of spinal and systemic morphine on ratdorsal horn neuronal responses in the spinal nerveligation model of neuropathic pain. Pain 1999;80:215–228.
28. Kamei J, Iwamoto Y, Hitosugi H, Misawa M, Na-gase H, Kasuya Y. Streptozotocin-induced diabetesselectively reduces antinociception mediated bymu1-opioid receptors, but not mediated by mu2-opi-oid receptors. Neurosci Lett 1994;165:141–143.
29. Onofrio BM, Yaksh TL, Arnold PG. Continu-ous low-dose intrathecal morphine administrationin the treatment of chronic pain of malignant ori-gin. Mayo Clinic Proc 1981;56:516–520.
30. Greenberg HS, Taren J, Ensminger WD, EoanK. Benefit from and tolerance to continuous intra-thecal infusion of morphine for intractable cancerpain. J Neurosurg 1982;57:360–364.
31. Mocavero G. Perineural, epidural and sub-arachnoid morphine for the relief of chronic pain.Anaesthesia 1982;37:471–472.
32. Spaziante R, Cappabiana P, Ferone A, CrausW, de’ Santi MS, deDivitiis E. Treatment of chroniccancer pain by means of continuous intrathecal lowdose morphine administration with a totally im-plantable subcutaneous pump. J Neurosurg Sci1985;29:143–151.
33. Frizelle H, Hannon V, McNicholas M. Intrathe-cal narcotics in cancer pain—a case report. Ir J MedSci 1994;163:328–330.
34. Van Melkebeke S, Wostyn L, Gellens P, CamuF. Continuous cervical intrathecal administration ofmorphine with a new infusion pump, the AnschutzIP 35.1: a case report. Acta Anaesthesiol Belg 1995;46:87–91.
35. Devulder JE. Subcutaneous morphine is supe-rior to intrathecal morphine for pain control in apatient with hypernephroma. J Clin Anesth 1998;10:163–165.

S26 Bennett et al. Vol. 20 No. 2 August 2000
36. Wang JF. Soulagement de la douleur par injec-tion intrathecale de serontonine ou de morphine.Ann Anesth Franc 1978;19:371–372.37. Ventafridda V, Figliuzzi M, Tamburini M, Gori
G, Parolaro D, Sala M. Clinical observation on anal-gesia elicited by intrathecal morphine in cancer pa-tients. Adv Pain Res Ther 1979;3:559–565.38. Cousins MJ, Mather LE, Glynn CJ, Wilson PR,
Graham JR. Selective spinal analgesia. Lancet 1979;1:1141–1142.39. Leavens M, Stratton-Hill C, Cech D, Weyland J,
Weston J. Intrathecal and intraventricular morphinefor pain in cancer patients: initial study. Neurosur-gery 1982;56:241–245.40. Rico RC, Hobika GH, Avellanosa AM, Trud-
nowski RJ, Rempel J, West CR. Use of intrathecaland epidural morphine for pain relief in patientswith malignant diseases: a preliminary report. J Med1982;13:223–231.41. Coombs DW, Saunders RL, Gaylor MS, et al.
Relief of continuous chronic pain by intraspinal nar-cotics infusion via an implanted reservoir. JAMA1983;250:2336–2339.42. Lazorthes Y, Siegfraied J, Gouarderes C, Bas-
tide R, Cros J, Verdie JC. Periventricular gray matterstimulation versus chronic intrathecal morphine incancer pain. Adv Pain Res Ther 1983;5:467–475.
43. Schroeder KA, Taren JA, Greenberg HS, Lay-ton P. Continuous intrathecal morphine for intracta-ble cancer pain: preliminary report of a method forcase selection. Surg Forum 1984;35:498–499.44. Coombs DW, Maurer LH, Saunders RL, Gaylor
M. Outcomes and complications of continuous in-traspinal narcotic analgesia for cancer pain control.J Clin Oncol 1984;2:1414–1420.45. Penn RD, Paice JA, Gottschalk W, Ivankovich
AD. Cancer pain relief using chronic morphine in-fusion. Early experience with a programmable im-planted drug pump. J Neurosurg 1984;61:302–306.46. Cobb CA III, French BN, Smith KA. Intrathe-
cal morphine for pelvic and sacral pain caused bycancer. Surg Neurol 1984;22:63–68.47. Krames ES, Gershow J, Glassberg A, et al. Con-
tinuous infusion of spinally administered narcoticsfor the relief of pain due to malignant disorders.Cancer 1985;56:696–702.48. Meynadier J, Dubar M, Blond S, Combelles-
Pruvot M. Intrathecal morphine in treatment ofintractable pain in cancer patients. In: ErdmannW, Oyama T, Pernak MJ, eds. The Pain Clinic I.Proceedings of the First International Symposium.Utrecht, Netherlands: VNU Science Press, 1985:87–91.49. Wang JK. Intrathecal morphine for intractable
pain secondary to cancer of pelvic organs. Pain1985;21:99–102.50. Paice JA. Intrathecal morphine infusion for in-
tractable cancer pain: a new use for implantedpumps. Oncol Nurs Forum 1986;13:41–47.
51. Shetter AG, Hadley MN, Wilkinson E. Adminis-tration of intraspinal morphine sulfate for the treat-ment of intractable cancer pain. Neurosurgery 1986;18:740–747.
52. Goodman RR, Brisman R. Treatment of lowerextremity reflex sympathetic dystrophy with contin-uous intrathecal morphine infusion. Appl Neuro-physiol 1987;50:425–426.
53. Ventafridda V, Spoldi E, Caraceni A, DeConno F. Intraspinal morphine for cancer pain.Acta Anaesthesiol Scand Suppl 1987;85:47–53.
54. Madrid JL, Fatela LV, Lobato RD, Gozalo A. In-trathecal therapy: rationale, technique, clinical re-sults. Acta Anaesthesiol Scand Suppl 1987;85:60–67.
55. Penn RD, Paice JA. Chronic intrathecal mor-phine for intractable pain. J Neurosurg 1987;67:182–186.
56. Brazenor GA. Long term intrathecal adminis-tration of morphine: a comparison of bolus injec-tion via reservoir with continuous infusion by im-planted pump. Neurosurgery 1987;21:484–491.
57. Rafii A, Singh K, Allen KC, Allen AD. Continu-ous intraspinal morphine administration for man-agement of cancer pain. J Pain Symptom Manage1988;3:S11[abstr].
58. Onofrio BM. Treatment of chronic pain of ma-lignant origin with intrathecal opiates. Clin Neuro-surg 1983;31:304–315.
59. Muller H, Luben V, Bierski J, et al. Long-termspinal opiate treatment. Acta Anaesth Belg 1988;39(Suppl 2):83–86.
60. Arner S, Rawal N, Gustafsson LL. Clinical ex-perience of long-term treatment with epidural andintrathecal opioids—a nationwide survey. Acta Ana-esthesiol Scand 1988;32:253–259.
61. Ali NM, Hoffman JS. Tolerance during long-term administration of intrathecal morphine. ConnMed 1989;53:266–268.
62. Schramm J, Neidhardt J, Vahle-Hinz C. Long-term pain relief and dosage pattern development incancer pain treated by intrathecal morphine via asubcutaneous reservoir [abstr]. Pain 1990;(Supp 5):S497, Special Issue.
63. Onofrio BM, Yaksh TL. Long-term pain reliefproduced by intrathecal morphine infusion in 53patients. J Neurosurg 1990;72:200–209.
64. Plummer JL, Cherry DA, Cousins MJ, et al.Long-term spinal administration of morphine incancer and non-cancer pain: a retrospective study.Pain 1991;44:215–220.
65. Anderson PE, Cohen JI, Everts EC, et al. In-trathecal narcotics for relief of pain from head andneck cancer. Arch Otolaryngol Head Neck Surg1991;117:1277–1280.
66. Follett KA, Hitchon PW, Piper J, et al. Responseof intractable pain to continuous intrathecal mor-phine: a retrospective study. Pain 1992;49:21–25.

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S27
67. Schultheiss R, Schramm J, Neidhardt J. Dosechanges in long- and medium-term intrathecal mor-phine therapy of cancer pain. Neurosurgery 1992;31:664–669 [discussion 669–670].
68. Krames ES, Lanning RM. Intrathecal infu-sional analgesia for nonmalignant pain: analgesic ef-ficacy of intrathecal opioid with or without bupiv-acaine. J Pain Symptom Manage 1993;8:539–548.
69. Fenollosa P, Pallares J, Cervera J, et al. Chronicpain in the spinal cord injured: statistical approachand pharmacological treatment. Paraplegia 1993;31:722–729.
70. Chambers FA, MacSullivan R. Intrathecal mor-phine in the treatment of chronic intractable pain.Ir J Med Sci 1994;163:318–321.
71. Devulder J, Ghys L, Dhondt W, Rolly G. Spinalanalgesia in terminal care: risk versus benefit. J PainSymptom Manage 1994;9:75–81.
72. Cheryn NJ, Chang V, Frager G, et al. Opioidpharmacotherapy in the management of cancerpain: a survey of strategies used by pain physiciansfor the selection of analgesic drugs and routes of ad-ministration. Cancer 1995;76:1283–1293.
73. Becker WJ, Ablett DP, Harris CJ, Dold ON.Long-term treatment of intractable reflex sympa-thetic dystrophy with intrathecal morphine. Can JNeurolog Sci 1995;22:153–159.
74. Bloomfield S, Hogg J, Ortiz O, Gross R. Analy-sis of breakthrough pain in 50 patients treated withintrathecal morphine infusion therapy. Develop-ment of tolerance or infusion system malfunction.Stereotact Funct Neurosurg 1995;65:142–146.
75. Paice JA, Penn RD, Shott S. Intraspinal mor-phine for chronic pain: a retrospective, multicenterstudy. J Pain Symptom Manage 1996;11:71–80.
76. Winkelmuller M, Winkelmuller W. Long-termeffects of continuous intrathecal opioid treatmentin chronic pain of nonmalignant etiology. J Neuro-surg 1996;85:458–467.
77. Tutak U, Doleys DM. Intrathecal infusion sys-tems for treatment of chronic low back and leg painof noncancer origin. South Med J 1996;89:295–300.
78. Gestin Y, Vainio A, Pegurier AM. Long-term in-trathecal infusion of morphine in the home care ofpatients with advanced cancer. Acta AnaesthesiolScand 1997;41:12–17.
79. Sallerin-Caute B, Lazorthes Y, Deguine O, et al.Does intrathecal morphine in the treatment of can-cer pain induce the development of tolerance? Neu-rosurg 1998;42:44–49 [discussion 49–50].
80. Gilmer-Hill HS, Boggan JE, Smith KA, et al. In-trathecal morphine delivered via subcutaneouspump for intractable pain in pancreatic cancer.Surg Neurol 1999;51:6–11.
81. Hassenbusch SJ, Stanton-Hicks M, CovingtonEC, Walsh JG, Guthrey DS. Long-term intraspinal in-fusions of opioids in the treatment of neuropathicpain. J Pain Symptom Manage 1995;10:527–543.
82. Angel IF, Gould HJ Jr, Carey ME. Intrathecalmorphine pump as a treatment option in chronic painof nonmalignant origin. Surg Neurol 1998;49:92–98.
83. Anderson VC, Burchiel KJ. A prospective studyof long-term intrathecal morphine in the manage-ment of chronic nonmalignant pain. Neurosurgery1999;44:289–300 [discussion 300–301].
84. Rawal N, Arner S, Gustafsson LL, Allvin R.Present state of extradural and intrathecal opioidanalgesia in Sweden. A nationwide follow-up survey.Br J Anaesth 1987;59:791–799.
85. Yaksh TL, Onofrio BM. Retrospective consider-ation of the doses of morphine given intrathecallyby chronic infusion in 163 patients by 19 physicians.Pain 1987;31:211–223.
86. Ballantyne JC, Carr DB, Berkey CS, et al. Com-parative efficacy of epidural, subarachnoid, and in-tracerebroventricular opioids in patients with paindue to cancer. Reg Anesth 1996;21:542–556.
87. Dahm P, Nitescu P, Appelgren L, Curelaru I.Efficacy and technical complications of long-termcontinuous intraspinal infusions of opioid and/orbupivacaine in refractory nonmalignant pain: acomparison between epidural and intrathecal ap-proach with externalized or implanted cathetersand infusion pumps. Clin J Pain 1998;14:4–16.
88. Monk JP, Beresford R, Ward A. Sufentanil. Areview of its pharmacologic properties and thera-peutic use. Drugs 1988;36:286–313.
89. Bernards C, Hill H. Physical and chemicalproperties of drug molecules governing their diffu-sion through the spinal meninges. Anesthesiology1992;77:750–756.
90. Bernards C. Epidural and intrathecal opioids:which drugs should we choose and how should theybe used. Am J Anesthesiol 1999;27:13–30.
91. Hansdottir V, Hedner T, Woestenborghs R,Nordberg G. The CSF and plasma pharmacokineticsof Sufentanil after intrathecal administration. Anes-thesiology 1991;74:264–269.
92. Stevens CW, Yaksh TL. Potency of infused anti-nociceptive agents is inversely related to magnitudeof tolerance after continuous infusion. J PharmacolExp Ther 1989;250:1–8.
93. Stevens CW, Yaksh TL. Time course character-istics of tolerance development to continuously in-fused antinociceptive agents in rat spinal cord. JPharmacol Exp Ther 1989;251:216–223.
94. Yaksh TL, Noueihed RY, Durant PAC. Studiesof the pharmacology and pathology of intrathecallyadministered 4-anilinopiperidine analogues andmorphine in the rat and cat. Anesthesiology 1986;64:54–66.
95. Rawal N, Nuutinen L, Raj PP, et al. Behavioraland histopathology effect following intrathecal ad-ministration of butorphanol, sufentanil, and nalbu-phine in sheep. Anesthesiology 1991;75:1025–1034.

S28 Bennett et al. Vol. 20 No. 2 August 2000
96. Sabbe MB, Grafe MR, Mjanger E, et al. Spinaldelivery of sufentanil, alfentanil, and morphine indogs. Physiologic toxicologic investigations. Anes-thesiology 1994;81:899–920.97. Barlow MR, Monrell M, et al. A prospective,
randomized, double-blind comparison of epiduraland intravenous sufentanil infusions. Anesthesiol-ogy 1994;81:346–352.98. Ionesco TI, Taverne HT, Houveling PL, et al.
Pharmacokinetic study of extradural and intrathecalSufentanil anesthesia for major surgery. Br J Anesth1991;40:634–638.99. Blackburn C. Respiratory arrest after epidural
sufentanil. Anesthesia 1987;42:665–666.100. Boersma FP, Noorduin H, Vanden Bussche G.Epidural sufentanil for cancer pain control in out-patients. Presented at the VIII Annual Meeting ofthe ESRA, Lisbon, Portugal, May 1989.101. Hassenbusch SJ, Stanton-Hicks MD, Soukup J,et al. Sufentanil citrate and morphine/bupivacaineas alternative agents in chronic epidural infusionsfor intractable non-cancer pain. Neurosurgery 1991;29:76–82.102. Hassenbusch SJ, Stanton-Hicks M, CovingtonEC, et al. Long-term intraspinal infusions of opioidsin the treatment of neuropathic pain. J Pain Symp-tom Manage 1995;10:527–543.103. Aldrete JA, Brown CA, Yharcho KL. Cervical ra-diculopathy treated by infusion of epidural analgesicsin homebound patients. J Clin Anesth 1994;6:33–36.104. Aldrete JA. Extended epidural catheter infu-sion with analgesics for patients with noncancerpain at their homes. Reg Anesth 1997;22:35–42.105. Badner NH, Reimer EJ, Komar WE, et al. Low-dose bupivacaine does not improve postoperativeepidural fentanyl analgesia in orthopedic patients.Anesth Analg 1991;72:337–341.106. 1Baron CM, Kowalski SE, Greengrass R, et al.Epinephrine decreases postoperative requirementsfor continuous thoracic epidural fentanyl infusions.Anesth Analg 1996;82:670–675.107. Bergstrom KA, Hokkonen J, Kuikka JT, et al.Fentanyl decreases beta-CIT binding to the dopa-mine transporter. Synapse 1998;29:13–15.108. Cascio M, Pygon B, Bernett C, et al. Labor an-algesia with intrathecal fentanyl decreases maternalstress. Can J Anaesth 1997;44:605–609.109. Chilvers CR, Vaghadia H, Mitchell GW, et al.Small-dose hypobaric lidocaine-fentanyl spinal anes-thesia for short duration outpatient laparoscopy. II.Optimal fentanyl dose. Anesth Analg 1996;84:65–70.110. Chu CC, Shu SS, Lin SM, et al. The effect ofintrathecal bupivacaine with combined fentanyl incesarean section. Acta Anaesthesiol Sin 1995;33:149–154.111. Collis RE, Davies DW, Aveling W. Randomizedcomparison of combined spinal-epidural and stan-dard epidural analgesia in labor. Lancet 1995;345:1413–1416.
112. Cook TM, Eaton JM, Goodwin AP. Epidural anal-gesia following upper abdominal surgery: United King-dom practice. Acta Anesthesiol Scand 1997;41:18–24.
113. Ellis DJ, Millar WL, Reisner LS. A randomizeddouble-blind comparison of epidural versus intrave-nous fentanyl infusion for analgesia after cesareansection. Anesthesiology 1990;72:981–986.
114. Glass PS, Estok P, Ginsberg B, et al. Use of pa-tient-controlled analgesia to compare the efficacy ofepidural to intravenous fentanyl. Anesth Analg1992;74:345–351.
115. Grass JA. Fentanyl: clinical use as postoperativeanalgesic–epidural/intrathecal route. J Pain Symp-tom Manage 1992;7:419–430.
116. Guinard JP, Carpenter RL, Chassot PG. Epiduraland intravenous fentanyl produce equivalent effectsduring major surgery. Anesthesiology 1995;82:377–382.
117. Herman NL, Choi KC, Afflect PJ, et al. Analge-sia, pruritus, and ventilation exhibit a dose-responserelationship in patients receiving intrathecal fenta-nyl. Anesth Anal 1999;89:3778–3783.
118. Justins DM, Knott C, Luthman J, et al. Epiduralversus intramuscular fentanyl. Analgesia and pharma-cokinetics in labor. Anaesthesia 1983;38:937–942.
119. McBride WJ, Dicker R, Abajian JC, et al. Con-tinuous thoracic epidural infusions for postopera-tive analgesia after pectus deformity repair. J RadiatSurg 1996;31:105–107.
120. Motsch J, Bleser W, Ismaily AJ, et al. Continu-ous intrathecal opiate therapy with a portable drugpump in cancer pain. Anasth Intensivther Noft Med1988;23:271–275.
121. Paech MJ, Westmore MD, Speirs HM. A dou-ble-blind comparison of epidural bupivacaine andbupivacaine-fentanyl for caesarean section. AnaesthIntensive Care 1990;18:22–30.
122. Palmer CM, Cork RC, Hays R, et al. The dose-response relation of intrathecal fentanyl for laboranesthesia. Anesthesiology 1998;88:355–361.
123. Palmer CM, Voulgaropoulos D, Alves D. Sub-arachnoid fentanyl augments lidocaine spinal anes-thesia for cesarean delivery. Reg Anesth Pain Med1995;20:389–394.
124. Preito-Alvarez MP, Fuentes-Bellido JG, Lopez-Cebollada J, et al. Comparative study of postopera-tive analgesia with methadone and fentanyl in con-tinuous peridural perfusion. Rev Esp Anestesiol Re-anim 1997;44:305–309.
125. Rawal N, Allvin R. Epidural and intrathecalopioids for postoperative pain management in Eu-rope–a 17-national questionnaire study. Acta Anes-thesiol Scand 1996;40:1119–1126.
126. Robertson K, Doublas MJ, McMorland GH.Epidural fentanyl, with and without epinephrine forpost-Caesarean section analgesia. Can Anaest Soc J1985;32:502–505.

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S29
127. Salomaki TE, Laitinen JO, Nuutinen LS. A ran-domized double-blind comparison of epidural ver-sus fentanyl infusion for analgesia after thoracot-omy. Anesthesiology 1991;75:90–95.
128. Sattler A, Jage J, Kramer I. Physico-chemical sta-bility of infusion solutions for epidural administrationcontaining fentanyl. Pharmazie 1998;53:386–391.
129. Singh H, Yang J, Thornton K, et al. Intrathecalfentanyl prolongs sensory bupivacaine spinal block.Can J Anaesth 1995;42:987–991.
130. Varrassi G, Celleno D, Capogna G, et al. Venti-latory effects of subarachnoid fentanyl in the eld-erly. Anaesthesia 1992;47:558–562.
131. Wang C, Chakrabarti MK, Whitwam JG. Spe-cific enhancement by fentanyl of the effects of in-trathecal bupivacaine on nociceptive afferent butnot on sympathetic efferent pathways in dogs. Anes-thesiology 1993;79:766–773.
132. Beeby D, MacIntosh KC, Bailey M, et al. Post-operative analgesia for caesarean section using epi-dural methadone. Anaesthesia 1984;39:61–63.
133. Davis AM, Inturrisi CE. d-Methadone blocksmorphine tolerance and N-methyl-D-aspartate-induced hyperalgesia. J Pharmacol Exp Ther 1999;289:1048–1053.
134. Eimerl D, Shir Y, Ureski G, et al. Continuouspostoperative epidural pump infusion of metha-done. Harefuah 1987;112:275–277.
135. Evron S, Samueloff A, Simon A, et al. Urinaryfunction during epidural analgesia with methadoneand morphine in post-cesarean section patients.Pain 1985;23:135–144.
136. Gedney JA, Liu EH. Side-effects of epidural in-fusions of opioid bupivacaine mixtures. Anaesthesia1998;53:1148–1155.
137. Haminsky G, Shir Y, Zagzag D, et al. Continu-ous self-administered epidural methadone andMarcaine for low-back and sciatic pain. Harefuah1987;112:10–11.
138. Haynes SR, Davidson I, Allsop JR, et al. Com-parison of epidural methadone with epidural di-amorphine for analgesia following caesarean sec-tion. Acta Anesthesiol Scand 1993;37:375–380.
139. Hernancez-Palazon J, Tortosa-Serrano JA,Sanchez-Ortega JL, et al. Postoperative analgesiawith epidural methadone in patients operated forhernia of the lumbar disc. Rev Esp Anestesiol Re-anim 1997;44:182–185.
140. Jacobson L, Chabla C, Brody MC, et al. Intra-thecal methadone: a dose-response study and com-parison with intrathecal morphine 0.5 mg. Pain1990;43:141–148.
141. Jacobson L, Chabla C, Brody MC, et al. Intra-thecal methadone and morphine for postoperativeanalgesia: a comparison of the efficacy, duration,and side effects. Anesthesiology 1990;70:742–746.
142. Jage J. Methadone—pharmacokinetics and
pharmacodynamics of an opiate. Anaesthesist 1989;38:159–166.
143. Nyska M, Shapira Y, Klin B, et al. Epiduralmethadone for analgesic management of patientswith conservatively treated proximal femoral frac-ture. J Am Geriatr Soc 1989;37:980–982.
144. Payne R, Gradert TL, Inturrisi CE. Cerebrospi-nal fluid distribution of opioids after intraventricu-lar and lumbar subarachnoid administration insheep. Life Sci 1996;59:1307–1321.
145. Samuelsson H, Malmberg F, Eriksson M, et al.Outcomes of epidural morphine treatment in can-cer pain: nine years of clinical experience. J PainSymptom Manage 1995;10:105–112.
146. Shimomaya N, Simomaya M, Elliot KJ, et al.D-Methadone is antinociceptive in the rat formalintest. J Pharmacol Exp Ther 1997;283:648–652.
147. Shir Y, Shapira SS, Shenkman Z, et al. Continu-ous epidural methadone for treatment of cancerpain. Clin J Pain 1991;7:339–341.
148. Tung AS, Yaksh TL. The antinociceptive ef-fects of epidural opiates in the cat: studies of thepharmacology and the effects of lipophilicity in spi-nal analgesia. Pain 1982;12:343–356.
149. Villalonga A, Gomar C, Nalda MA. Effect of theperidural methadone concentration in postopera-tive analgesia. Rev Esp Anesthesiol Reanim 1989;36:260–263.
150. Wang JM, Knarr DC, Raj PP, et al. Continuousepidural methadone for the management of postop-erative pain after lower abdominal surgery. RegAnesth 1992;17:26–28.
151. Welch DB, Hrynaszkeiwicz A. Postoperative an-algesia using epidural methadone. Administrationby the lumbar route for thoracic pain relief. Anaes-thesia 1981;36:1051–1054.
152. Sumi M, Sakura S, Kosaka Y. Intrathecal hyper-baric 0.5% tetracaine as a possible cause of transientneurologic toxicity. Anesth Analg 1996;82:1076–1077.
153. Ngan Kee WD. Epidural pethidine: pharmacol-ogy and clinical experience. Anaesth Intensive Care1998;26:247–255.
154. Ngan Kee WD. Epidural pethidine: pharmacol-ogy and clinical applications. Anaesth IntensiveCare 1998;26:137–146 [comments 594, 707].
155. Bostrom MA, Pakiz AM, Melnyk DL et al. Spinalanesthesia with meperidine: will epinephrine pro-long its duration? AANAJ 1994;62:267–272.
156. St-Onge S, Fugere F, Girard M. Bupivacainedecreases epidural meperidine requirements afterabdominal surgery. Can J Anaesth 1997;44:360–366.
157. Sjostrom S, Tamsen A, Perrson MP, Hartvig P.Pharmacokinetics of intrathecal morphine and mep-eridine in humans. Anesthesiology 1987;67:889–895.
158. Harvey SC, O’Neil MG, Hope CA, et al. Contin-uous intrathecal meperidine via an implantable in-

S30 Bennett et al. Vol. 20 No. 2 August 2000
fusion pump for chronic, nonmalignant pain. AnnPharmacother 1997;31:1306–1308.
159. Wulf H, Gleim M, Mignat C. The stability ofmixtures of morphine hydrochloride, bupivacainehydrochloride, and clonidine hydrochloride in por-table pump reservoirs for the management ofchronic pain syndromes. J Pain Symptom Manage1994;9:308–311.
160. Adams HA, Pawlik D, Bauer H, Mautgreve W.Stability of local anesthetics in heparinized blood,plasma and sulfuric acid. Acta Anaesthes Scand1998;42:783–785.
161. Sattler A, Jage J, Kramer I. Physico-chemicalstability of infusion solutions for epidural adminis-tration containing fentanyl and bupivacaine orlidocaine. Pharmazie 1998;53:386–391.
162. Roos PJ, Glerum HJ, Schroeders MJ. Effect ofglucose 5% solution and bupivacaine hydrochlorideon absorption of sufentanil citrate in a portable pumpreservoir during storage and simulated infusion by anepidural catheter. Pharm World Sci 1993;15:269–275.
163. Christen C, Johnson CE, Walters JR. Stability ofbupivacaine hydrochloride and hydromorphone hy-drochloride during simulated epidural coadminis-tration. Am J Health Syst Pharm 1996;53:170–713.
164. Barnes AR, Nash S. Stability of bupivacaine hy-drochloride with diamorphine hydrochloride in anepidural infusion. Pharm World Sci 1995;17:87–92.
165. Cook TM, James PA, Stannard CF. Diamor-phine and bupivacaine mixtures: an in vitro study ofmirobiological safety. Pain 1998;76:259–263.
166. Sakuragi T, Ishino H, Dan K. Bacterial activityof clinically used local anesthetics on Staphylococ-cus aureus. Reg Anesth 1996;21:239–242.
167. Grimmond TR, Brownridge P. Antimicrobialactivity of bupivacaine and pethidine. Anaesth In-tensive Care 1986;14:418–420.
168. Hotvedt R, Refsum H, Helgesen KG. Cardiacelectrophysiologic and hemodynamic effects relatedto plasma levels of bupivacaine in the dog. AnesthAnalg 1985;64:388–394.
169. Kaukinen S, Ojanen R, Kaukinen L, et al.Plasma thromboxane B2 levels and thromboxaneB2 production by platelets are increased in patientsduring spinal and epidural anesthesia. Prostaglan-dins Leukot Essent Fatty Acids 1989;37:83–88.
170. Mercadante S. Neuraxial techniques for cancerpain: an opinion about unresolved therapeutic di-lemmas. Reg Anesth Pain Med 1999;24:74–83.
171. Wagemans MF, Van der Valk P, Spoelder EM,et al. Neurohistopathological findings after continu-ous intrathecal administration of morphine or amorphine/bupivacaine mixture in cancer pain pa-tients. Acta Anaesth Scand 1997;41:1033–1038.
172. Sjoberg M, Karlsson PA, Nordborg C, et al.Neuropathologic findings after long term intrathe-cal infusion of morphine and bupivacaine for pain
treatment in cancer patients. Anesthesiology 1992;76:173–186.173. Karlsson PA, Nordberg C, Sjoberg M, et al.Neuropathological findings after long-term intrath-ecal infusion of buprenorphine and bupivacaine ofpain treatment in cancer patients. Eur J Pain 1994;15:68–76.174. Li DF, Bahar M, Cole G, Rosen M. Neurologi-cal toxicity of the subarachnoid infusion of bupi-vacaine, lignocaine or 2-chlorprocaine in the rat.Brit J Anesth 1985;57:424–429.175. Evans KR, Carrie LE. Continuous epidural in-fusion of bupivacine in labour—a simple method.Anaesthesia 1979;34:310.176. Ready LB, Plumber MH, Fink BR, Sumi SM. In-trathecal local anesthetic toxicity in rabbits. Anes-thesiology 1983;59:A187.177. Burm AG, Vermeulen NP, Van Kleef JW, et al.Pharmacokinetics of lignocaine and bupivacaine insurgical patients following epidural administration.Simultaneous investigation of absorption and dispo-sition kinetics using stable isotopes. Clin Pharma-cokinet 1987;13:191–203.178. Veering BT, Bum AG, Vletter AA, et al. The ef-fect of age on the systemic absorption, dispositionand pharmacodynamics of bupivacaine after epiduraladministration. Clin Pharmacokinet 1992;22:75–84.179. Penning JP, Yaksh TL. Interaction of intrathe-cal morphine, bupivacaine, lidocaine in the rat. An-esthesiology 1992;77:1186–1200.180. Kroin JS, McCarthy RJ, Penn RD, et al. The ef-fect of chronic subarachnoid bupivacaine infusionin dogs. Anesthesiology 1987;66:737–742.181. Pan HL, Song HK, Eisenach JC. Effects of in-trathecal neostigmine, bupivacaine, and their com-bination on sympathetic nerve activity in rats. Anes-thesiology 1998;88:481–486.182. Carp H, Jayaram A, Morrow D. Intrathecal cho-linergic agonists lessen bupivacaine spinal block in-ducted hypotension in rats. Anesth Analg 1994;79:112–116.183. Nitescu P, Hultman E, Appelgran L, et al. Bac-teriology, drug stability and exchange of percutane-ous delivery systems. Clin J Pain 1992;8:324–337.184. Nitescu P, Sjoberg M, Appelgren L, Curelaru I.Complications of intrathecal opioids and bupi-vacaine in the treatment of “refractory” cancer pain.Clin J Pain 1995;11:45–62.185. Van Dongen RT, Crul BJ, DeBock M. Long-term intrathecal infusion of morphine and mor-phine/pubicaine mixtures in the treatment of can-cer pain: a retrospective analysis of 51 cases. Pain1993;55:119–123.186. Van Dongen RT, van Ee R, Crul BJ. Neurologi-cal impairment during long-term intrathecal infu-sion of bupivacaine in cancer patients: a sign of spi-nal cord compression. Pain 1997;69:205–209.187. Orko R, Pitkanen M, Rosenberg PH. Subarach-noid anaesthesia with 0.75% bupivacine in patients
Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S31
with chronic renal failure. Brit J Anaesth 1986;58:605–609.
188. Appelgren L, Nordborg C, Sjoberg M, et al.Spinal epidural metastasis: implications of spinal an-algesia to treat “refractory” cancer pain. J PainSymptom Manage 1997;13:25–42.
189. Sjoberg M, Appelgren L, Einarsson S, et al.Long-term intrathecal morphine and bupivacine in“refractory” cancer pain. I. Results from the first se-ries of 52 patients. Acta Anaesthes Scand 1991;35:30–43.
190. Krames ES, Lanning RM. Intrathecal infu-sional analgesia for nonmalignant pain; analgesic ef-ficacy of intrathecal opioid with or without bupiv-acaine. J Pain Symptom Manage 1993;8:539–548.
191. Nitescu P, Dahm P, Appelgren L, Curelaru I.Continuous infusion of opioid and bupivacaine byexternalized intrathecal catheters in long-term treat-ment of “refractory” nonmalignant pain. Clin J Pain1998;14:17–28.
192. Sjoberg M, Nitescu P, Appelgren L, Curelaru I.Long-term intrathecal morphine and bupivacaine inpatients with refractory cancer pain. Results from amorphine:bupivacaine dose regimen of 0.5:4.75mg/ml. Anesthesiology 1994;80:284–297.
193. Dahm P, Nitescu P, Appelgren L, Curelaru I.Efficacy and technical complications of long-termcontinuous intraspinal infusions of opioid and/orbupivacaine in refractory nonmalignant pain: acomparison between the epidural and the intrathe-cal approach with externalized or implanted cathe-ters and infusion pumps. Clin J Pain 1998;14:4–16.
194. Nitescu P, Appelgren L, Linder, et al. Epiduralversus intrathecal morphine-bupivacaine: assess-ment of consecutive treatments in advanced cancerpain. J Pain Symptom Manage 1990;5:18–26.
195. Brennum J, Nielsen PT, Horn A, et al. Quanti-tative sensory examination of epidural anaesthesiaand analgesia in man; dose-response effect of bupiv-acaine. Pain 1994;56:315–326.
196. Curatolo M, Kaufmann R, Petersen-Felix S, etal. Block of pinprick and cold sensation poorly cor-relate with relief of postoperative pain during epidu-ral analgesia. Clin J Pain 1999;15:6–12.
197. Lund C, Mogensen T, Hjortso NC, Kehlet H.Systemic morphine enhances spread of sensory anal-gesia during postoperative epidural bupivacaine in-fusion. Lancet 1985;2:1156–1157.
198. Dahl JB, Rosenberg J, Hansen BL, et al. Differ-ential analgesic effects of low-dose epidural mor-phine and morphine-bupivacaine at rest and duringmobilization after major abdominal surgery. AnesthAnalg 1992;74:362–365.
199. Etches RC, Gammer TL, Comish R. Patient-controlled epidural analgesia after thoracotomy: acomparison of meperidine with and without bupi-vacaine. Anesth Analg 1996;83:81–86.
200. Rankin AP, Comber RE. Management of fiftycases of chest injury with a regimen of epiduralbupivacaine and morphine. Anaesth Intensive Care1984;12:311–314.
201. Ragni J, Guillen JC, Aug A, et al. Prolongedepidural analgesia following thoracotomy. Clinicalstudy and serum levels over five days. Ann Chir1991;45:167–176.
202. Wiebalck A, Brodner G, Van Aken H. The ef-fects of adding sufentanil to bupivacaine for postop-erative patient-controlled epidural analgesia. AnesthAnalg 1997;85:124–129.
203. Coppe E, Willaert J. Postoperative analgesia formajor abdominal surgery with continuous thoracicepidural infusion of bupivacaine with sufentanil, ver-sus bupivacaine with morphine. A randomized doubleblind study. Acta Anaesthesiol Belg 1992;43:131–137.
204. Sakuragi T, Ishino H, Dan K. Bactericidal activ-ity of clinically used local anesthetics on Staphylo-coccus aureus. Reg Anesth 1996;19:43–47.
205. Feldman JM, Chapin-Roberson K, Turner J. Doagents used to epidural analgesia have antimicrobialproperties? Reg Anesth 1994;19:43–47.
206. Grimmond TR, Brownridge P. Antimicrobialactivity of bupivacaine and pethidine. Anaesth In-tensive Care 1986;14:418–420.
207. Markham A, Faulds D. Ropivacaine: a review ofits pharmacology and therapeutic use in regionalanesthesia. Drugs 1996;52:429–449.
208. Scott DA, Emanuelsson BM, Mooney PH, et al.Pharmacokinetics and efficacy of long-term epiduralropivacaine infusion for postoperative analgesia.Anesth Analg 1997;85:1322–1330.
209. Naropin® (ropivacaine HCl Injection). ASTRAProduct Safety Information Sheet.
210. Cederholm I. Preliminary risk-benefit analysisof ropivacaine in labour and following surgery.Drug Safety 1997;16:391–402.
211. Erichsen CJ, Sjovall J, et al. Pharmacokineticsand analgesic effect of ropivacaine during continu-ous epidural infusion for postoperative pain relief.Anesthesiology 1996;84:834–842.
212. Kampe S, Weigand C, et al. Postoperative anal-gesia with no motor block by continuous epiduralinfusion of ropivacaine 0.1% and sufentanil after to-tal hip replacement. Anesth Analg 1999;89:395–398.
213. Cascio MG, Gaiser RR, et al. Comparative eval-uation of four different infusion rates of ropivacaine(2 mg/mL) for epidural labor analgesia. RegAnesth Pain Med 1998;23:548–553.
214. Zaric D, Nydahl PA, et al. The effect of contin-uous lumbar epidural infusion of ropivacaine(0.1%, 2%, and 3%) and 0.25% bupivacaine on sen-sory and motor block in volunteers: a double-blindstudy. Reg Anesth Pain Med 1996;21:14–25.
215. Irestedt L, Ekbolm A, et al. Pharmacokinetics

S32 Bennett et al. Vol. 20 No. 2 August 2000
and clinical effect during continuous epidural infu-sion with ropivacaine 2.5 mg/mL or bupivacaine 2.5mg/mL for labour pain relief. Acta Aneasth Scand1998;42:890–896.
216. Gaiser RR, Venkateswaren P, et al. Comparisonof 0.025% ropivacaine and bupivacaine for epiduralanalgesia for labor and vaginal delivery. J ClinAnesth 1997;9:564–568.
217. Drasner K, Sakura S, Chan VW, et al. Persistentsacral sensory deficit induced by intrathecal localanesthetic infusion in the rat. Anesthesiology 1994;80:847–852.
218. Ready LB, Plumer MH, Haschke RH, et al.Neurotoxicity of intrathecal local anesthetic in rab-bits. Anesthesiology 1985;63:364–370.
219. Ferrante FM, Fanciullo GJ, Grichnik KP, et al.Regression of sensory anesthesia during continuousepidural infusions of bupivacaine and opioid for totalknee replacement. Anesth Analg 1993;77:1179–1184.
220. Bohme K, Tryba M. Paraspinal opioids andpump systems. Z Arztl Fortbuild Qualitatssich 1998;92:47–52.
221. Zenz M, Schappler-Scheele B, Neuhaus R, etal. Long-term peridural morphine analgesia in can-cer pain [letter]. Lancet 1981;1:91.
222. Du Pen SL, Du Pen A. Tunneled epidural cath-eters: practical considerations and implantationtechniques. In: Waldman S, Winnie A, eds. Interven-tional Pain Management. Philadelphia, PA: WBSaunders Company, 1996.
223. Cousins MJ, Plummer JL. Spinal opioids inacute and chronic pain. Adv Pain Res Ther 1991;18:457–473.
224. Du Pen SL, Du Pen AR, Polissar N, et al. Imple-menting guidelines for cancer pain management:results of a randomized controlled clinical trial. JClin Oncol 1999;17:361–370.
225. Eisenach JC, Du Pen S, Dubois M, et al. Epidu-ral clonidine analgesia for intractable cancer pain.The Epidural Clonidine Study Group. Pain 1995;61:391–399.
226. Gautier PE, De Kock M, Fanard L, et al. In-trathecal clonidine combined with sufentanil for la-bor analgesia. Anesthesiology 1998;88:651–656.
227. Mercier FR, Dounas M, Bouaziz H, et al. Theeffect of adding a minidose of clonidine to intrathe-cal sufentanil for labor analgesia. Anesthesiology1998;89:594–601.
228. De Kock M, Gauthier P, Pavlopoulou A, et al.Epidural clonidine or bupivacaine as the sole anal-gesic agent during and after abdominal surgery: acomparative study. Anesthesiology 1999;90:1354–1362.
229. Claes B, Soetens M, Van Zundert A, Datta S.Clonidine added to bupivacaine-epinephrine-sufen-tanil improves epidural analgesia during childbirth.Reg Anesthes Pain Med 1998;23:540–547.
230. Rauck RL, Eisenach JC, Jackson K, et al. Epidu-ral clonidine treatment for refractory reflex sympa-thetic dystrophy. Anesthesiology 1993;79:1163–1169.
231. Mogensen T, Eliasen K, Ejlersen E, et al. Epi-dural clonidine enhances postoperative analgesiafrom a combined low-dose epidural bupivacaineand morphine regimen. Anaesthes Analg 1992;75:607–610.
232. Motsch J, Graber E, Ludwig K. The addition ofclonidine enhances postoperative analgesia fromepidural morphine: a double-blind study. Anesthesi-ology 1990;73:1067–1073.
233. De Kock M, Crochet B, Morimont C, ScholtesJL. Intravenous or epidural clonidine for intra- andpostoperative analgesia. Anesthesiology 1993;79:525–531.
234. Gracies JM, Nance P, Elovic E, Simpson DM.Traditional pharmacological treatments for spastic-ity. Part II: General and regional treatments [Re-view]. Muscle Nerve 1997;6(Suppl):S92–S120.
235. Leiphart JW, Dills CV, Zikel OM, et al. A com-parison of intrathecal administered narcotic andnonnarcotic analgesics for experimental chronicneuropathic pain. J Neurosurg 1995;82:595–599.
236. Ochs G, Loew M, Tonn J, Toyka K. Distribu-tion, tolerability and tissue compatibility of intrathe-cal tizanidine in the sheep. Acta Anaestheiol Scand1998;42:786–793.
237. Kawamata T, Omote K, Kawamata M, et al. An-tinociceptive interaction of intrathecal alpha 2-adr-energic agonists, tizanidine and clonidine, withlidocaine in rats. Anesthesiology 1997;87:1027.
238. Yaksh TL, Rathbun M, Jage J, et al. Pharmacol-ogy and toxicology of chronically infused epiduralclonidine HCl in dogs. Fundam Appl Toxicol 1994;23:319–335.
239. Tallariada RJ, Stone DJ, Raffa RB. Efficient de-signs for studying synergistic drug combinations.Life Sci 1997;61:PL417–425.
240. Eisenach JC, Castro MI, Dewan DM, Rose JC.Epidural clonidine analgesia in obstetrics: sheepstudy. Anesthesiology 1989;70:51–56.
241. Danzebrick RM, Gebhart GF. Antinociceptiveeffects of intrathecal adrenoceptor agonists in a ratmodel of visceral nociception. J Pharmacol ExpTher 1990;253:698–705.
242. Pan HL, Chan SR, Eisenach JC. Intrathecalclonidine alleviates allodynia in neuropathic rats: in-teraction with spinal muscarinic and nicotinic re-ceptors. Anesthesiol 1999;90:509–514.
243. Meert TR, De Kock M. Interactions betweenthe lipophilic opioid sufentanil and clonidine in ratsafter spinal application. Acta Anesthesiol Scand1995;89:527–534.
244. Eisenach JC, Grice SC. Epidural clonidine doesnot decrease blood pressure or spinal cord bloodflow in awake sheep. Anesthesiology 1988;68:335–340.

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S33
245. De Kock M, Le Polain B, Henin D, et al. Cloni-dine pretreatment reduces the systemic toxicity ofintravenous bupivacaine in rats. Anesthesiology1993;79:282–289.
246. Klimscha W, Tong C, Eisenach JC. Intrathecalalpha 2-adrenergic agonists stimulate acetylcholineand norepinephrine release from the spinal corddorsal horn in sheep. An in vivo microdialysis study.Anesthesiology 1997;87:110–116.
247. De Kock M, Eisenach J, Tong C, et al. Analge-sic doses of intrathecal but not intravenous cloni-dine increase acetylcholine in cerebrospinal fluid inhumans. Anesth Analg 1997;84:800–803.
248. Wulf H, Gleim M, Mignat C. The stability ofmixtures of morphine hydrochloride, bupivacainehydrochloride, and clonidine hydrochloride in por-table pump reservoirs for the management ofchronic pain syndromes. J Pain Symptom Manage1994;9:308–311.
249. Eisenach JC, Hood DD, Curry R. Intrathecal, butnot intravenous, clonidine reduces experimental ther-mal or capsaicin-induced pain and hyperalgesia innormal volunteers. Anesthes Analg 1998;87:591–596.
250. Fitzgibbon D, Rapp S, Butler S, et al. Reboundhypertension and withdrawal associated with discon-tinuation of an infusion of epidural clonidine. Anes-thesiology 1996;94:729–731.
251. Brunschwiler M, Van Gessel E, Forester A,Bruce A. Gamulin comparison of clonidine. Mor-phine or placebo mixed with bupivacaine duringcontinuous spinal anaesthesia. Can J Anaesth 1998;45:735–740.
252. Klimscha W, Chiari A, Krafft P, et al. Hemody-namic and analgesic effects of clonidine added re-petitively to continuous epidural and spinal blocks.Anesth Analg 1995;80:322–327.
253. Sia S, Lepri A. Clonidine administered as anauxiliary block does not affect postoperative painwhen given as the sole analgesic. Anesth Analg 1999;88:1109–1112.
254. Chiari A, Lorber C, Eisenach JC, et al. Analge-sic and hemodynamic effects of intrathecal cloni-dine as the sole analgesic agent during first stage oflabor: a dose-response study. Anesthesiology 1999;91:388–396.
255. Mercadante S, Serretta R, Sapio M, et al. Whenall else fails: stepwise multiple solutions for a com-plex cancer pain syndrome. Support Care Cancer1999;7:45–50.
256. Tumber PS, Fitzgibbon DR. The control of se-vere cancer pain by continuous intrathecal infusionand patient controlled intrathecal analgesia with mor-phine, bupivacaine and clonidine. Pain 1998;78:217–220.
257. Levy R, Leiphart J, Dills C. Analgesic action ofacute and chronic intraspinally administered opiateand alpha 2-adrenergic agonists in chronic neuro-pathic pain. Stereotact Funct Neurosurg 1994;62:279–289.
258. Ono N, Kroin JS, Penn RD, Paice J. Effects ofintrathecal nonnarcotic analgesics on chronic tac-tile allodynia in rats: alpha 2-agonists versus soma-tostatin analog. Neurol Med Chir 1997;37:6–10.
259. Yaksh TL, Pogrel JW, Lee YW, Chaplan SR. Re-versal of nerve ligation-induced allodynia by spinalalpha-2 adrenoceptor agonists. J Pharmacol ExperTher 1995;272:207–214.
260. Kroin JS, McCarthy RJ, Penn RD, et al. Intrath-ecal clonidine and tizanidine in conscious dogs:comparison of analgesic and hemodynamic effects.Anesthes Analg 1996;83:891.
261. Bazil MK, Gordon FJ. Spinal NMDA receptorsmediate pressor responses evoked from the rostralven-trolateral medulla. Am J Physiol 1991;260:H267–275.
262. Bennett GJ, Xie YK. A peripheral mononeur-opathy in rat that produces disorders of pain sensa-tion like those seen in man. Pain 1988;33:87–107.
263. Bion JF. Intrathecal ketamine for war surgery.A preliminary study under field conditions. Anaes-thesia 1984;39:1023–1028.
264. Bormann J. Memantine is a potent blocker ofN-methyl-d aspartate (NMDA) receptor channels.Eur J Pharmacol 1989;166:591–592.
265. Brock-Utne JG, Kallichurum S, Mankowitz E,et al. Intrathecal ketamine with preservative—histo-logical effects on spinal nerve roots of baboons. SAfr Med J 1982;61:40–41.
266. Brock-Utne JG, Mankowitz E, Kallichurum S,Downing JW. Effects of intrathecal saline and ket-amine with and without preservative on the spinalnerve roots of monkeys. S Afr Med J 1982;61:360–361.
267. Burton AW, Lee DH, Saab C, Chung JM. Pre-emptive intrathecal ketamine injection produces along-lasting decrease in neuropathic pain behaviors ina rat model. Reg Anesth Pain Med 1999;24:208–213.
268. Chaplan SR, Malmberg AB, Yaksh TL. Efficacyof spinal NMDA receptor antagonism in formalinhyperalgesia and nerve injury evoked allodynia inthe rat. J Pharm Exper Ther 1997;280:829–838.
269. Chen H-SV, Pellegrini J, Aggarwal S, et al.Open channel block of N-methyl d-aspartate(NMDA) responses by memantine: therapeutic ad-vantage against NMDA receptor-mediated toxicity. JNeurosci 1992;12:4427–4436.
270. Coderre TJ, Melzack R. The contribution ofexcitatory amino acids to central sensitization andpersistent nociception after formalin-induced tissueinjury. J Neurosci 1992;12:3665–3670.
271. Dunbar SA, Pulai IJ. Repetitive opioid absti-nence causes progressive hyperalgesia sensitive toN-methyl-D-aspartate receptor blockade in the rat. JPharmacol Exp Ther 1998;284:678–686.
272. Dunbar SA, Yaksh TL. Concurrent spinal infu-sion of MK801 blocks spinal tolerance and depen-dence induced by chronic intrathecal morphine inthe rat. Anesthesiology 1996;84:1177–1188.

S34 Bennett et al. Vol. 20 No. 2 August 2000
273. Dunbar SA, Yaksh TL. Spinal infusion ofN-methyl-D-aspartate antagonist MK801 induces hy-persensitivity to the spinal alpha-2 agonist ST91 inthe rat. J Pharm Exp Ther 1997;281:1219–1225.
274. Ebert B, Andersen S, Krogsgaard-Larsen P. Ke-tobemidone, methadone and pethidine are non-competitive N-methyl-D-aspartate (NMDA) antago-nists in the rat cortex and spinal cord. Neurosci Lett1995;187:165–168.
275. Eisenach JC, Gebhart GF. Intrathecal amitrip-tyline acts as an N-methyl-D-aspartate receptor an-tagonist in the presence of inflammatory hyperalge-sia in rats. Anesthesiology 1995;83:1046–1054.
276. Franklin PH, Murray TF. High affinity[3H]Dextrorphan binding in rat brain is localized toa noncompetitive antagonist site of the activatedN-methyl-D-aspartate receptor-cation channel. MolPharmacol 1991;41:134–146.
277. Gorman AL, Elliott KJ, Inturrisi CE. The d- andl-isomers of methadone bind to the non-competitivesite on the N-methyl-D-aspartate (NMDA) receptorin rat forebrain and spinal cord. Neurosci Lett 1997;223:5–8.
278. Iida H Dohi S, Tanahashi T, et al. Spinal con-duction block by intrathecal ketamine in dogs.Anesth Analg 1997;85:106–110.
279. Islas JA, Astorga J, Laredo M. Epidural ket-amine for control of postoperative pain. Anesth An-alg 1985;64:1161–1162.
280. Karpinski N, Dunn J, Hansen L, Masliah E.Subpial vacuolar myelopathy after intrathecal ket-amine: report of a case. Pain 1997;73:103–105.
281. Kim SH, Chung JM. An experimental modelfor peripheral neuropathy produced by segmentalspinal nerve ligation in the rat. Pain 1992;50:355–363.
282. Klimscha W, Horvath G, Szikszay M, et al. Anti-nociceptive effect of the S(1)-enantiomer of ket-amine on carrageenan hyperalgesia after intrathecaladministration in rats. Anesth Analg 1998;86:561–565.
283. Kristensen JD, Karlsten R, Gordh T Jr, Holtz A.Spinal cord blood flow after intrathecal injection ofa N-methyl-D-aspartate receptor antagonist or an ad-enosine receptor agonist in rats. Anesth Analg 1993;76:1279–1283.
284. Kristensen JD, Svensson B, Gordh T, Jr. TheNMDA-receptor antagonist CPP abolishes neuro-genic ‘wind-up pain’ after intrathecal administra-tion in humans. Pain 1992;51:249–253.
285. Malinovsky JM, Cozian A, Lepage JY, et al. Ket-amine and midazolam neurotoxicity in the rabbit.Anesthesiology 1991;75:91–97.
286. Malinovsky JM, Lepage JY, Cozian A, et al. Is ket-amine or its preservative responsible for neurotoxic-ity in the rabbit? Anesthesiology 1993;78:109–115.
287. Mankowitz E, Brock-Utne JG, Cosnett JE,Green-Thompson R. Epidural ketamine. A prelimi-nary report. S Afr Med J 1982;61:441–442.
288. Mao J, Price DD, Hayes RL, et al. Intrathecaltreatment with dextrorphan or ketamine potently re-duces pain-related behaviors in a rat model of periph-eral mononeuropathy. Brain Res 1993;605:164–168.
289. Martin DD, Tranquilli WJ, Olson WA, et al. He-modynamic effects of epidural ketamine in isoflu-rane-anesthetized dogs. Vet Surg 1997;26:505.
290. Olney JW, Labruyere J, Price, MT. Pathologicalchanges in cerebrocortical neurons by phencylidineand related drugs. Science 1989;244:1360–1362.
291. Olney JW, Labruyere J, Wang G, et al. NMDAantagonist neurotoxicity: mechanism and preven-tion. Science 1991;254:1515–1518.
292. Peat SJ, Bras P, Hanna MH. A double-blindcomparison of epidural ketamine and diamorphinefor postoperative analgesia. Anaesthesia 1989;44:555–558.
293. Pedraz JL, Calvo MB, Gascon AR, et al. Phar-macokinetics and distribution of ketamine after ex-tradural administration to dogs. Br J Anaesth 1991;67:310–316.
294. Ravat F, Dorne R, Baechle JP, et al. Epiduralketamine or morphine for postoperative analgesia.Anesthesiology 1987;66:819–822.
295. Ren K, Williams GM, Hylden JL, et al. The in-trathecal administration of excitatory amino acid re-ceptor antagonists selectively attenuated carra-geenan-induced behavioral hyperalgesia in rats. EurJ Pharmacol 1992;219:235–243.
296. Eisenberg E, LaCross S, Strassman AM. The ef-fects of the clinically tested NMDA receptor antago-nist memantine on carrageenan-induced thermal hy-peralgesia in rats. Eur J Pharmacol 1994;255:123–129.
297. Sharif NA, Nunes JL, Whiting RL. Pharmaco-logical characterization of the N-methyl-D-aspartate(NMDA) receptor-channel in rodent and dog brainand rat spinal cord using [3H]MK–801 binding.Neurochem Res 1991;16:563–569.
298. Sonoda H, Omote K. Suppressive effects of ket-amine on neuropathic pain. Masui 1998;47:136–144.
299. Stevens CW, Yaksh TL. Potency of infused spi-nal antinociceptive agents is inversely related tomagnitude of tolerance after continuous infusion. JPharmacol Exp Ther 1989;250:1–8.
300. Sucher NJ, Awobuluyi M, Choi YB, Lipton SA.NMDA receptors: from genes to channels. TrendsPharmacol Sci 1996;17:348–55.
301. Takahashi H, Miyazaki M, Nanbu T, et al. TheNMDA-receptor antagonist ketamine abolishes neu-ropathic pain after epidural administration in a clin-ical case. Pain 1998;75:391–394.
302. Tal M, Bennett GJ. Dextrorphan relieves neu-ropathic heat-evoked hyperalgesia in the rat. Neuro-sci Lett 1993;151:107–110.
303. Tiseo PJ, Yaksh TL. The spinal pharmacologyof urinary function: studies on urinary continence

Vol. 20 No. 2 August 2000 Intraspinal Infusion: Evidence-Based Review S35
in the unanaesthetized rat. In: Neurobiology of In-continence (Ciba Foundation Symposium 151).Chichester: John Wiley & Sons. 1990;91–109.
304. Tung AS, Yaksh TL. Analgesic effect of intra-thecal ketamine in the rat. Reg Anesth 1981;6:91–94.
305. Wong CS, Liaw WJ, Tung CS, et al. Ketaminepotentiates analgesic effect of morphine in postop-erative epidural pain control. Reg Anesth 1996;21:534–541.
306. Yaksh TL. Behavioral and autonomic corre-lates of the tactile evoked allodynia produced by spi-nal glycine inhibition: effects of modulatory recep-tor systems and excitatory amino acid antagonists.Pain 1989;37:111–123.
307. Yaksh TL. Preclinical models of nociception.In: Yaksh TL, Lynch C III, Zapol WM, Maze M, Bie-buyck JF, Saidman LJ, eds. Anesthesia: BiologicFoundations. Philadelphia, PA: Lippincott-Raven1997:685–718.
308. Yaksh TL, Harty GJ. Pharmacology of the allo-dynia in rats evoked by high dose intrathecal mor-phine. J Pharmacol Exp Ther 1988;244:501–507.
309. Yaksh TL, Reddy SVR. Studies in the primateon the analgesic effects associated with intrathecalactions of opiate, a-adrenergic agonists and ba-clofen. Anesthesiology 1981;54:451–467.
310. Yaksh TL (unpublished).
311. Yamamoto T, Yaksh TL. Comparison of the an-tinociceptive effects of pre- and post treatment withintrathecal morphine and MK801, an NMDA antag-onist, on the formalin test in the rat. Anesthesiology1992;77:757–763.
312. Yamamoto T, Yaksh TL. Spinal pharmacologyof thermal hyperesthesia induced by incomplete li-gation of sciatic nerve. I. Opioid and nonopioid re-ceptors. Anesthesiology 1991;75:817–826.
313. Yamamoto T, Yaksh TL. Spinal pharmacologyof thermal hyperesthesia induced by constriction in-jury of sciatic nerve. Excitatory amino acid antago-nists. Pain 1992;49:121–128.
314. Yang CY, Wong CS, Chang JY, Ho ST. Intrathe-cal ketamine reduces morphine requirements in pa-tients with terminal cancer pain. Can J Anaesth1996;43:379–383.
315. Zahn PK, Brennan TJ. Lack of effect of intra-thecally administered N-methyl-D-aspartate receptorantagonists in a rat model for postoperative pain.Anesthesiology 1998;88:143–156.
316. Penn RD, Paice JA, Kroen JS. Octreotide: a po-tent new non-opiate analgesic for intrathecal infu-sion. Pain 1992;49:13–19.
317. Paice JA, Penn RD, Kroen JS. Intrathecal oc-treotide for relief of intractable non-malignant pain:5-year experience with two cases. Neurosurgery1996;38:203–207.
318. Taira T, Kawamura H, Tanikawa T, et al. A newapproach to control central deafferentation pain:
spinal intrathecal baclofen. Stereotact Funct Neuro-surg 1995;65:101–105.
319. Herman RN, D’Luzansky SC, Ippolito R. In-trathecal baclofen suppresses central pain in pa-tients with spinal lesions: a pilot study. Clin J Pain1992;8:338–345.
320. Loubser PG, Akman NM. Effects of intrathecalbaclofen on chronic spinal cord pain. J Pain Symp-tom Manage 1996;12:241–247.
321. Zuniga RE, Schlict CR, Abram SE. Intrathecalbaclofen is analgesic in patients with chronic pain.Anesthesiology 2000;92:876–880.
322. Bean BP. Classes of calcium channels in verte-brate cells. Ann Rev Physiol 1989;S1:367–384.
323. Anwyl R. Modulation of vertebrate neuronalcalcium channels by transmitters. Brain Res Rev1991;16:265–281.
324. Schroeder JE, Fischbach PS, Zheng D, McCler-key EW. Activation of m-opioid receptors inhibitstransient high and low threshold Ca11 currents, butspares a sustained current. Neuron 1991;6:13–20.
325. Chaplan SR, Pogrel JW, Yaksh TL. Role of volt-age-dependent calcium channel. Subtypes in experi-mental tactile allodynia. J Pharm Exp Ther 1994;269:1117–1123.
326. Malmberg AB, Yaksh TL. Effect of continuousintrathecal infusion of w-conopeptides, N-type cal-cium-channel blockers, on behavior and antinoci-ception in the formalin and hot-plate test in rats.Pain 1995;60:83–90.
327. Brose WG, Cutlove DP, Luther RR, et al. Use ofintrathecal SNX-111, a novel, N-type voltage-sensitive,calcium channel blocker, in the management of in-tractable brachial plexus avulsion pain. Clin J Pain1997;13:256–259.
328. Investigators Post-Study meeting 95-001 & 96-002,Philadelphia. May 7–8, 1999. Elan Pharmaceuticals.
329. Ridgeway B, Wallace M, Gerayli A. Ziconotidefor the treatment of severe spasticity after spinalcord injury. Pain 2000;85:287–289.
330. Penn RD, Paice JA. Adverse effects associatedwith the intrathecal administration of ziconotide.Pain 2000;85:291–296.
331. Schoeffler P, Auroy P, Bazin JE, et al. Sub-arachnoid midazolam: histologic study in rats andreport of its effect of chronic pain in humans. RegAnesth 1991;16:329–332.
332. Erdine S, Yucel A, Ozalcin S, et al. Neurotoxicityof midazolam in the rabbit. Pain 1999;80:419–423.
333. Svensson BA, Welin M, Gordh T Jr, Westman J.Chronic subarachnoid midazolam (dormicum) inthe rat. Morphologic evidence of spinal cord neuro-toxicity. Reg Anesth 1995;20:426–434.
334. Edwards M, Serrao JM, Gent JP, Goodchild CS.On the mechanisms by which midazolam causes spi-nally mediated analgesia. Anesthesiology 1990;73:273–277.

S36 Bennett et al. Vol. 20 No. 2 August 2000
335. Krukowsky JA, Hood DD, Eisenach JC, et al. In-trathecal neostigmine for post-cesarean section analge-sia: dose response. Anesth Analg 1997;84:1269–1275.336. Lauretti GR, Mattos AL, Gomes JM, PereiraNL. Postoperative analgesia and antiemetic efficacyafter intrathecal neostigmine in patients undergo-ing abdominal hysterectomy during spinal anesthe-sia. Reg Anesth 1997;22:527–533.337. Lauretti GR, Hood DD, Eisenach JC, PfeiferBL. A multi-center study of intrathecal neostigminefor analgesia following vaginal hysterectomy. Anes-thesiol 1998;89:913–918.338. Lauretti GR, Oliveira R, Reis MP, et al. Study ofthree different doses of epidural neostigmine coad-ministered with lidocaine for postoperative analge-sia. Anesthesiology 1999;90:1534–1538.339. Chung CJ, Kim JS, Park HS, Chin YJ. The effi-cacy of intrathecal neostigmine, intrathecal mor-phine, and their combination for post-cesarean sec-tion analgesia. Anesth Analg 1998;87:341–346.340. Lauretti GR, Reis MP, Prado WA, Klamt JG.Dose-response study of intrathecal morphine versusintrathecal neostigmine, their combination, or pla-cebo for postoperative analgesia in patients under-going anterior and posterior vaginoplasty. AnesthAnalg 1996;82:1182–1187.341. Hood DD, Mallak KA, Eisenach JC, Tong C. In-teraction between intrathecal neostigmine and epi-dural clonidine in human volunteers. Anesthesiol1996;85:315–325.342. Gürün MS, Leinbach R, Moore L, et al. Studieson the safety of glucose and paraben-containingneostigmine for intrathecal administration. AnesthAnalg 1997;85:317–323.343. Taiwo YO, Levine JD. Prostaglandins inhibitendogenous pain control mechanisms by blockingtransmission at spinal noradrenergic synapses. JNeurosci 1988;8:1346–349.344. Malmberg AB, Yaksh TL. Pharmacology of thespinal auction of ketorolac, morphine, ST-91,U50488H, and L-PIA on the formalin test and anisobolographic analysis of the NSAID interaction.Anesthesiol 1993;79:270–281.345. . Eisenach JC. Aspirin, the miracle drug: spi-nally, too? Anesthesiology 1993;79:211–213.346. Jurna I, Spohrer B, Bock R. Intrathecal injec-tion of acetylsalicylic acid, salicylic acid and in-domethacin depresses C fibre-evoked activity in therat thalamus and spinal cord. Pain 1992;49:249–257.347. Malmberg AB, Yaksh TL. Antinociceptive ac-
tions of spinal nonsteroidal anti-inflammatory agentson the formalin test in the rat. J Pharmacol Exp Ther1992;263:136–146.348. Bustamante D, Paeile C, Willer JC, Le Bars D.Effects of intrathecal or intracerebroventricular ad-ministration of nonsteroidal anti-inflammatorydrugs on a C-fiber reflex in rats. J Pharm Exp Ther1997;281:1381–1391.349. Antognini JF. Intrathecal acetylsalicylic acidand indomethacin are not analgesic for a supramax-imal stimulus. Anesth Analg 1993;76:1079–1082.350. Amiot JF, Palacci JH, Vedrenne C, et al. Spinaltoxicity of lysine acetylsalicylate and ketamine hy-drochloride given by the intrathecal route in the rat.Ann Fr Anesth Reanim 1986;5:462.351. Svensson BA, Karlsten R, Kristensen JD, et al.Intrathecal injection of lysine acetylsalicylic acid inthe rat: a neurotoxicological study. Acta Anaesthe-siol Scand 1993;37:799–805.352. Devoghel JC. Small intrathecal doses of lysine-acetylsalicylate relieve intractable pain in man. J IntMed Res 1983;11:90–91.353. Pellerin M, Hardy F, Abergel A, et al. Chronicrefractory pain in cancer patients. Usefulness of in-trathecal lysine acetylsalicylate in 60 cases. PresseMed 1987;16:1465–1468.354. Yamamura H. Remarks on some analgesicsused in the pain clinic. Masui 1989;38:152–156.355. Grip G, Svensson BA, Gordh T, Hartvig P. His-topathology and evaluation of potentiation of mor-phine-induced antinociception by intrathecal dro-peridol in the rat. Acta Anaesthesiol Scand 1992;36:145–152.356. Bach V, Carll P, Ravlo O, et al. Potentiation ofepidural opioids with epidural droperidol—a one-year retrospective study. Anaesthesia 1986;41:1116–1119.357. Naji P, Farschtschain M, Wilder-Smith O, et al.Epidural droperidol and morphine for postopera-tive pain. Anesthes Analg 1990;70:583–588.358. . Wilder-Smith CH, Wilder-Smith OHG, Far-schtschian M, Naji P. Epidural droperidol reducesthe side effects and duration of analgesia of epiduralsufentanil. Anesth Analg 1994;79:98–104.359. Athanassaiadis C, Karamanis A. Akathisia afterlonger-term epidural use of droperidol: a case re-port. Pain 1992;50:203–204.360. Wallace M, Yaksh T. Long-term spinal analge-sic delivery: a review of the preclinical and clinicalliterature. Reg Anesth Pain Med 2000;25:117–157.