evidence-based nursing (ebn) and diagnostic accuracy in
TRANSCRIPT
M. Lunney, October 2008 1
Evidence-Based NursingEvidence-Based Nursing(EBN) and Diagnostic(EBN) and DiagnosticAccuracy in ElectronicAccuracy in ElectronicHealth RecordsHealth Records (EHR)(EHR)
Margaret Lunney, RN, PhDMargaret Lunney, RN, PhDCollege of Staten Island, TheCollege of Staten Island, TheCity University of New YorkCity University of New York
[email protected]@si.rr.com
My topic this morning is accuracy ofnurses’ diagnoses and its relation toEvidenced-based nursing (EBN) andelectronic health records.
With the reality of the electronic healthrecord worldwide, nurse leaders mustaddress the accuracy of nurses’ datainterpretations in order to achieve EBNpractice.
M. Lunney, October 2008 2
The purposes of this paperThe purposes of this paperare to:are to:1) describe the research1) describe the researchevidence related to diagnosticevidence related to diagnosticaccuracy;accuracy;2) explain the impact of2) explain the impact ofdiagnostic accuracy in an EHR;diagnostic accuracy in an EHR;3) Propose strategies to improve3) Propose strategies to improvediagnostic accuracy.diagnostic accuracy.
The purposes of this paper areto:1) Describe the research evidencerelated to diagnostic accuracy;
2) Explain the impact ofdiagnostic accuracy in an EHR;
3) Propose strategies to improvediagnostic accuracy.
M. Lunney, October 2008 3
Assumption: NursingAssumption: Nursinginterventions to help people areinterventions to help people arebased on data interpretations.based on data interpretations.
-A basic assumption is that all nursing interventionsare based on data interpretations. For example, evenif a nurse decides to help a patient change positionsin bed, it is based on the nurse’s interpretation ofpatient data that the patient needs to move.- Every data interpretation, however, has thepotential to be less accurate than it should be toactually help patients. I became interested in theconcept of accuracy, for example, when I was ahome care nurse. When other nurses visited mypatients, they tried to teach them about what theyalready knew. Patients later complained to me thatthe nurses’ teachings confused them, rather thanhelped them. I started to realize that nurses caneasily misinterpret patients’ problems and needs,thus providing interventions that are not helpful.

M. Lunney, October 2008 4
Data interpretations may not beData interpretations may not beaccurate enough to guide the selectionaccurate enough to guide the selection
of interventions.of interventions.
Research findings have substantiated that datainterpretations may not be accurate enough to guide theselection of interventions.
The goal for nurses is to match data interpretations withthe individual, family or community’s experiences orresponses to health problems and life processes.
But, people are unique and their responses to theirenvironment are unique.
We do not know other people, so it is complex anddifficult to interpret other people’s responses.
M. Lunney, October 2008 5
Nursing diagnoses are dataNursing diagnoses are datainterpretations of human responses,interpretations of human responses,
e.g., Carlson-Catalano, 1997e.g., Carlson-Catalano, 1997 Disturbed ThoughtDisturbed Thought
ProcessesProcesses Stress OverloadStress Overload Social IsolationSocial Isolation Sleep DeprivationSleep Deprivation Chronic Low SelfChronic Low Self
EsteemEsteem Ineffective CopingIneffective Coping
FatigueFatigue Ineffective DenialIneffective Denial HopelessnessHopelessness Ineffective RoleIneffective Role
PerformancePerformance PowerlessnessPowerlessness Ineffective ParentingIneffective Parenting Decisional ConflictDecisional Conflict
This list is an example of some of the humanresponses that are nursing diagnoses in the NANDA-International classification. This is also a list from a qualitative research study ofthe responses of 8 women who had been battered in thepast by their husbands. The researcher spent about 3hours with each woman to identify their responses tobattering and their health problems. Each of these women were already being treated forthe medical diagnoses of broken bones, headaches, andgastrointestinal problems, but this list of their responsesadds significantly more information about their healthstatus. Don’t you think so? In this study, these women also identified how nursescould help them with interventions.

M. Lunney, October 2008 6
Accuracy is a raterAccuracy is a rater’’s judgment of thes judgment of thedegree to which a diagnosticdegree to which a diagnostic
statement matches the cues in astatement matches the cues in apatient situationpatient situation (Lunney, 1990).(Lunney, 1990).
+ 5 Highly accurate, a priority & precise match+ 5 Highly accurate, a priority & precise match+ 4 Close to accurate+ 4 Close to accurate+ 3 Represent the general idea+ 3 Represent the general idea+ 2 Reflects some cues but not highly relevant cues+ 2 Reflects some cues but not highly relevant cues+1 Reflects only one or a few cues+1 Reflects only one or a few cues 0 Not supported by the evidence 0 Not supported by the evidence-1 Evidence says it is not accurate-1 Evidence says it is not accurate
The concept of accuracy of nurses’ diagnoses ofhuman responses was first described by me for my doctoralresearch; concept development was published in 1990. Idescribed accuracy as a continuous variable from high tolow because the phenomena that nurses diagnose overlapwith one another. For example, anxiety and fearsignificantly overlap and they require differentinterventions, so if the best diagnosis is fear, anxiety wouldbe close but not right on target. If the best diagnosis was fear, a general diagnosissuch as ineffective coping might be scored at level 3. Level 2 on the 7 point scale is for diagnoses that havesufficient evidence but they are not the priority at this time. Level 1, 0 and -1At least 5 studies have substantiated that nurses’ diagnosesof clinical cases can be scored on these 7 levels.

M. Lunney, October 2008 7
Example: Case study by CavendishExample: Case study by Cavendish
I am now going to use the writtencase study of Craig C to illustrate thevarious diagnoses that might bemade by nurses and how they wouldbe scored for accuracy using thisscale.
M. Lunney, October 2008 8
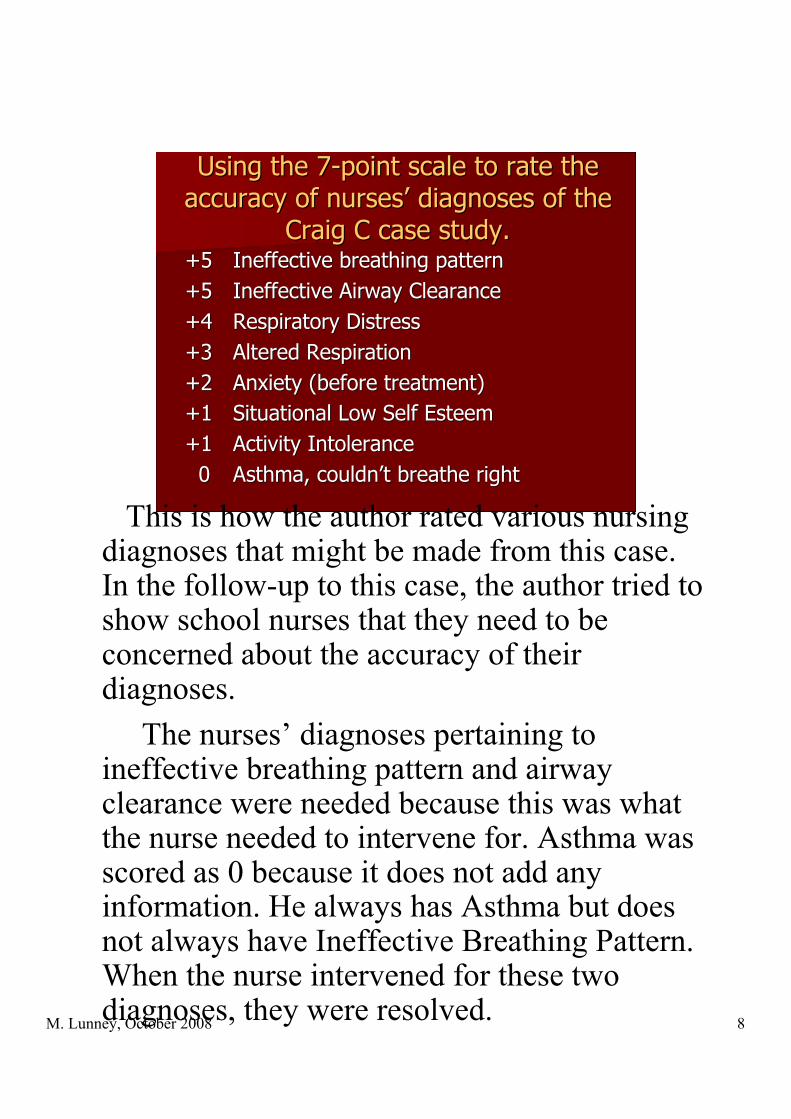
Using the 7-point scale to rate theUsing the 7-point scale to rate theaccuracy of nursesaccuracy of nurses’’ diagnoses of the diagnoses of the
Craig C case study.Craig C case study.+5+5 Ineffective breathing patternIneffective breathing pattern+5+5 Ineffective Airway ClearanceIneffective Airway Clearance+4+4 Respiratory DistressRespiratory Distress+3+3 Altered RespirationAltered Respiration+2 +2 Anxiety (before treatment)Anxiety (before treatment)+1 +1 Situational Low Self EsteemSituational Low Self Esteem+1 +1 Activity IntoleranceActivity Intolerance 0 0 Asthma, couldnAsthma, couldn’’t breathe rightt breathe right
This is how the author rated various nursingdiagnoses that might be made from this case.In the follow-up to this case, the author tried toshow school nurses that they need to beconcerned about the accuracy of theirdiagnoses. The nurses’ diagnoses pertaining toineffective breathing pattern and airwayclearance were needed because this was whatthe nurse needed to intervene for. Asthma wasscored as 0 because it does not add anyinformation. He always has Asthma but doesnot always have Ineffective Breathing Pattern.When the nurse intervened for these twodiagnoses, they were resolved.
M. Lunney, October 2008 9
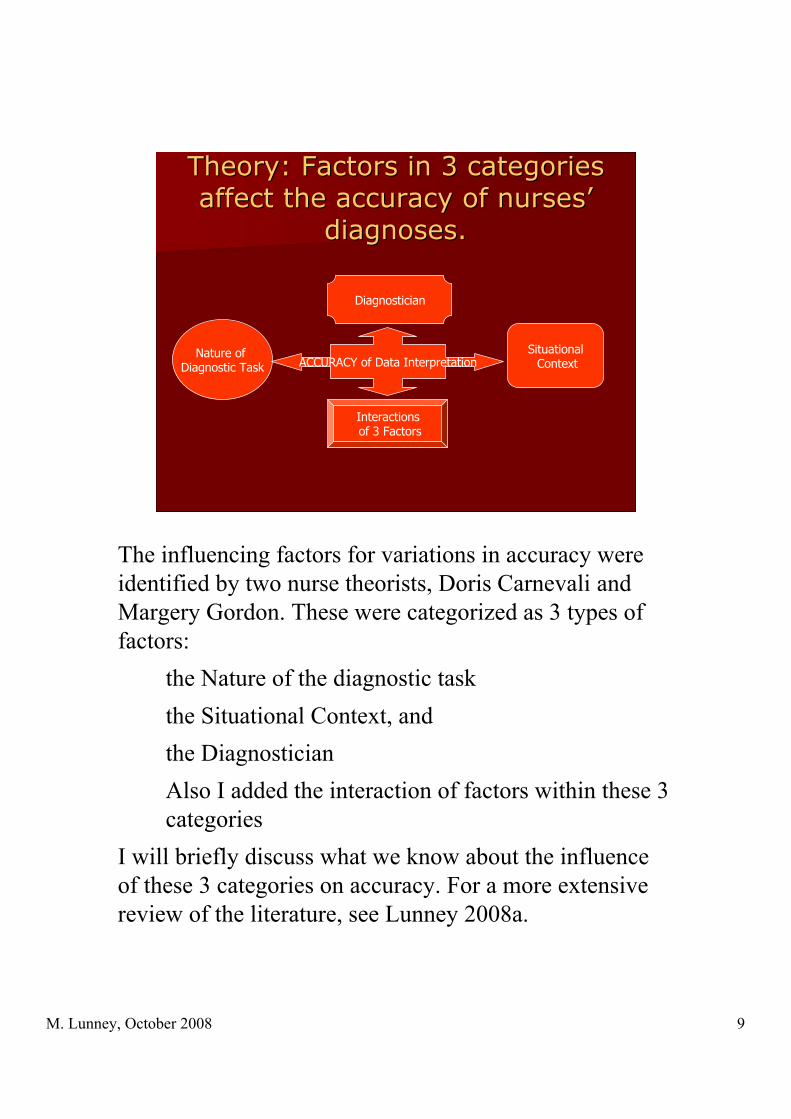
Theory: Factors in 3 categoriesTheory: Factors in 3 categoriesaffect the accuracy of nursesaffect the accuracy of nurses’’
diagnoses.diagnoses.
ACCURACYNature of Diagnostic Task
Situational Context
Diagnostician
ACCURACY of Data Interpretation
Interactions of 3 Factors
The influencing factors for variations in accuracy wereidentified by two nurse theorists, Doris Carnevali andMargery Gordon. These were categorized as 3 types offactors:
the Nature of the diagnostic taskthe Situational Context, andthe DiagnosticianAlso I added the interaction of factors within these 3categories
I will briefly discuss what we know about the influenceof these 3 categories on accuracy. For a more extensivereview of the literature, see Lunney 2008a.
M. Lunney, October 2008 10
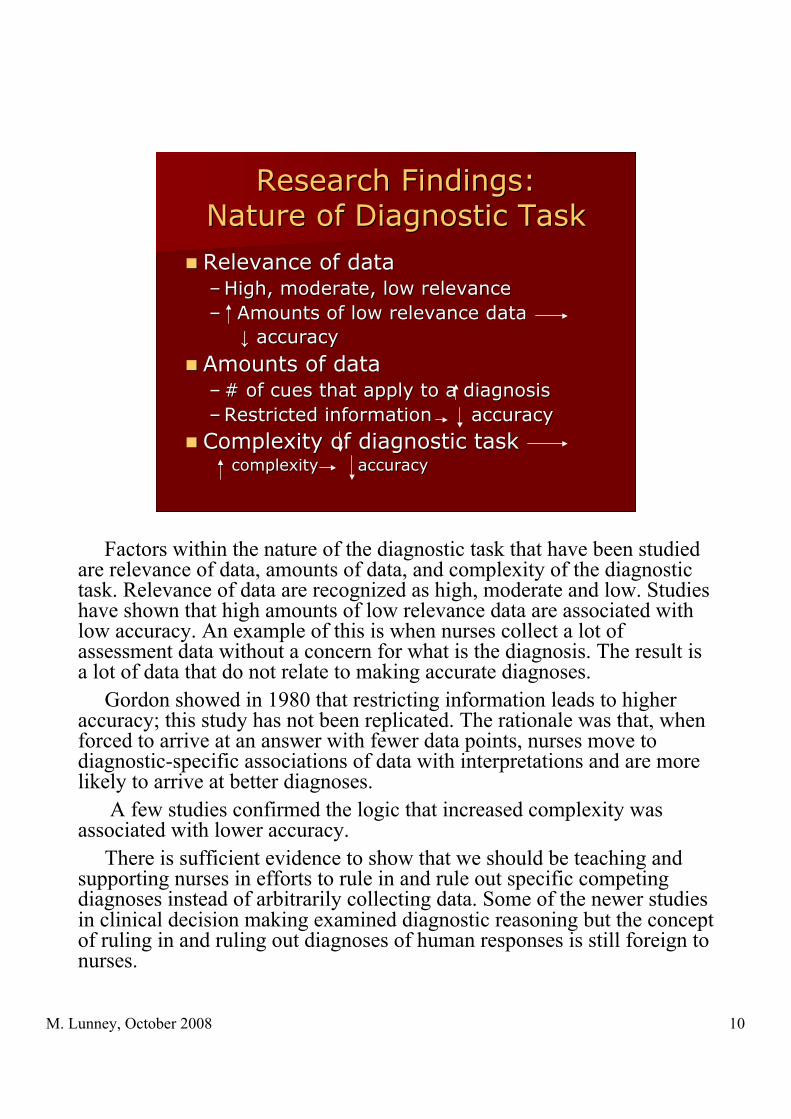
Research Findings:Research Findings:Nature of Diagnostic TaskNature of Diagnostic Task
Relevance of dataRelevance of data–– High, moderate, low relevanceHigh, moderate, low relevance–– Amounts of low relevance data Amounts of low relevance data
↓↓ accuracy accuracy
Amounts of dataAmounts of data–– # of cues that apply to a diagnosis# of cues that apply to a diagnosis–– Restricted information accuracyRestricted information accuracy
Complexity of diagnostic taskComplexity of diagnostic task complexity accuracy complexity accuracy
Factors within the nature of the diagnostic task that have been studiedare relevance of data, amounts of data, and complexity of the diagnostictask. Relevance of data are recognized as high, moderate and low. Studieshave shown that high amounts of low relevance data are associated withlow accuracy. An example of this is when nurses collect a lot ofassessment data without a concern for what is the diagnosis. The result isa lot of data that do not relate to making accurate diagnoses. Gordon showed in 1980 that restricting information leads to higheraccuracy; this study has not been replicated. The rationale was that, whenforced to arrive at an answer with fewer data points, nurses move todiagnostic-specific associations of data with interpretations and are morelikely to arrive at better diagnoses. A few studies confirmed the logic that increased complexity wasassociated with lower accuracy. There is sufficient evidence to show that we should be teaching andsupporting nurses in efforts to rule in and rule out specific competingdiagnoses instead of arbitrarily collecting data. Some of the newer studiesin clinical decision making examined diagnostic reasoning but the conceptof ruling in and ruling out diagnoses of human responses is still foreign tonurses.
M. Lunney, October 2008 11
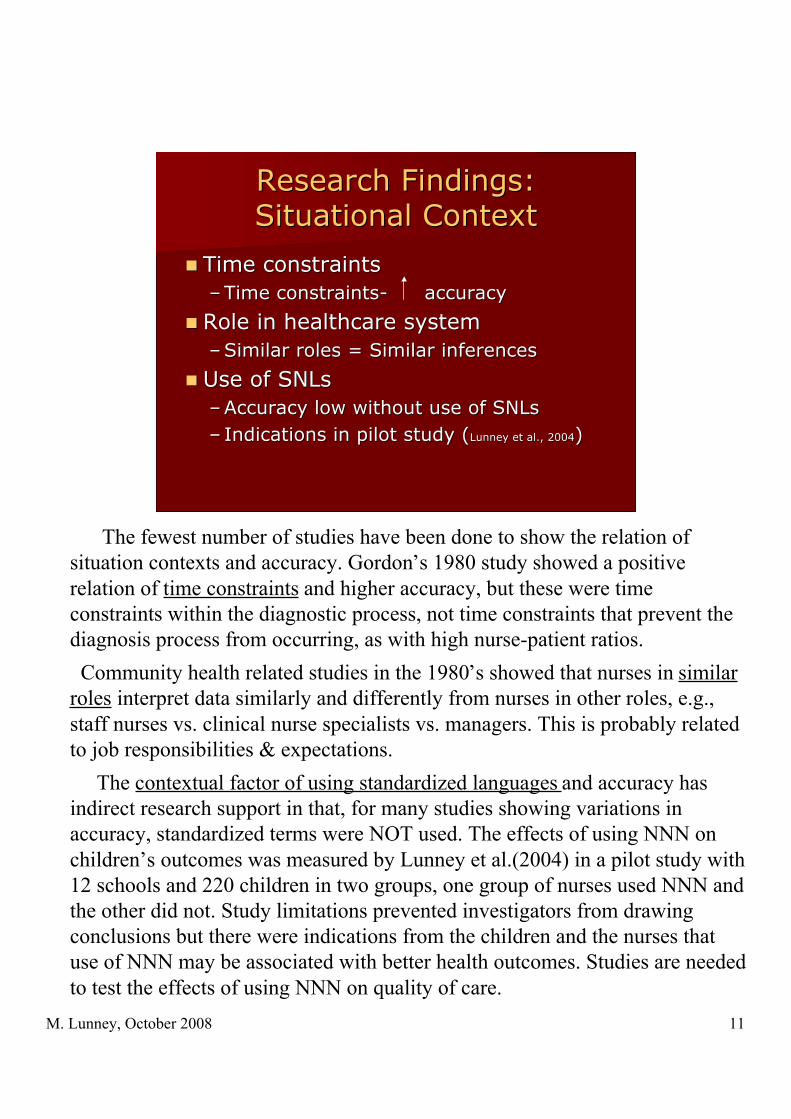
Research Findings:Research Findings:Situational ContextSituational Context
Time constraintsTime constraints–– Time constraints- Time constraints- accuracyaccuracy
Role in healthcare systemRole in healthcare system–– Similar roles = Similar inferencesSimilar roles = Similar inferences
Use of SNLsUse of SNLs–– Accuracy low without use of SNLsAccuracy low without use of SNLs–– Indications in pilot study (Indications in pilot study (Lunney et al., 2004Lunney et al., 2004))
The fewest number of studies have been done to show the relation ofsituation contexts and accuracy. Gordon’s 1980 study showed a positiverelation of time constraints and higher accuracy, but these were timeconstraints within the diagnostic process, not time constraints that prevent thediagnosis process from occurring, as with high nurse-patient ratios. Community health related studies in the 1980’s showed that nurses in similarroles interpret data similarly and differently from nurses in other roles, e.g.,staff nurses vs. clinical nurse specialists vs. managers. This is probably relatedto job responsibilities & expectations. The contextual factor of using standardized languages and accuracy hasindirect research support in that, for many studies showing variations inaccuracy, standardized terms were NOT used. The effects of using NNN onchildren’s outcomes was measured by Lunney et al.(2004) in a pilot study with12 schools and 220 children in two groups, one group of nurses used NNN andthe other did not. Study limitations prevented investigators from drawingconclusions but there were indications from the children and the nurses thatuse of NNN may be associated with better health outcomes. Studies are neededto test the effects of using NNN on quality of care.

M. Lunney, October 2008 12
Research Findings:Research Findings:DiagnosticianDiagnostician
Nursing education:Nursing education:–– Mixed resultsMixed results–– Level of education may not be asLevel of education may not be as
important as education related to important as education related to NDxNDx–– Positive association withPositive association with
Teaching aidsTeaching aids Continuing education on Continuing education on NDxNDx
Nursing experience:Nursing experience:–– Mixed resultsMixed results–– Experience related to types of casesExperience related to types of cases
Most of the studies related to accuracy have focused onnurses as diagnosticians. There is some evidence thatimproved accuracy is associated with higher levels ofeducation. The evidence is stronger that higher accuracy isassociated with education on nursing diagnoses and thediagnostic process, e.g., Muller Staub et al, 2007. Use ofteaching aids such as decision trees and courses on nursingdiagnosis were significantly related to higher levels ofaccuracy. For nursing experience, too, it seems that it is not years ofexperience in nursing that is important but the experience ofworking with the same types of patients represented in theresearch studies. Studies of the decision making of criticalcare nurses further support this relationship, see Redden &Wotton (2001), and Reischman & Yarandi (2002). .
M. Lunney, October 2008 13
Clinical study showing that accuracyClinical study showing that accuracyof data interpretations varies widelyof data interpretations varies widely
(Lunney et al., 1997)(Lunney et al., 1997)
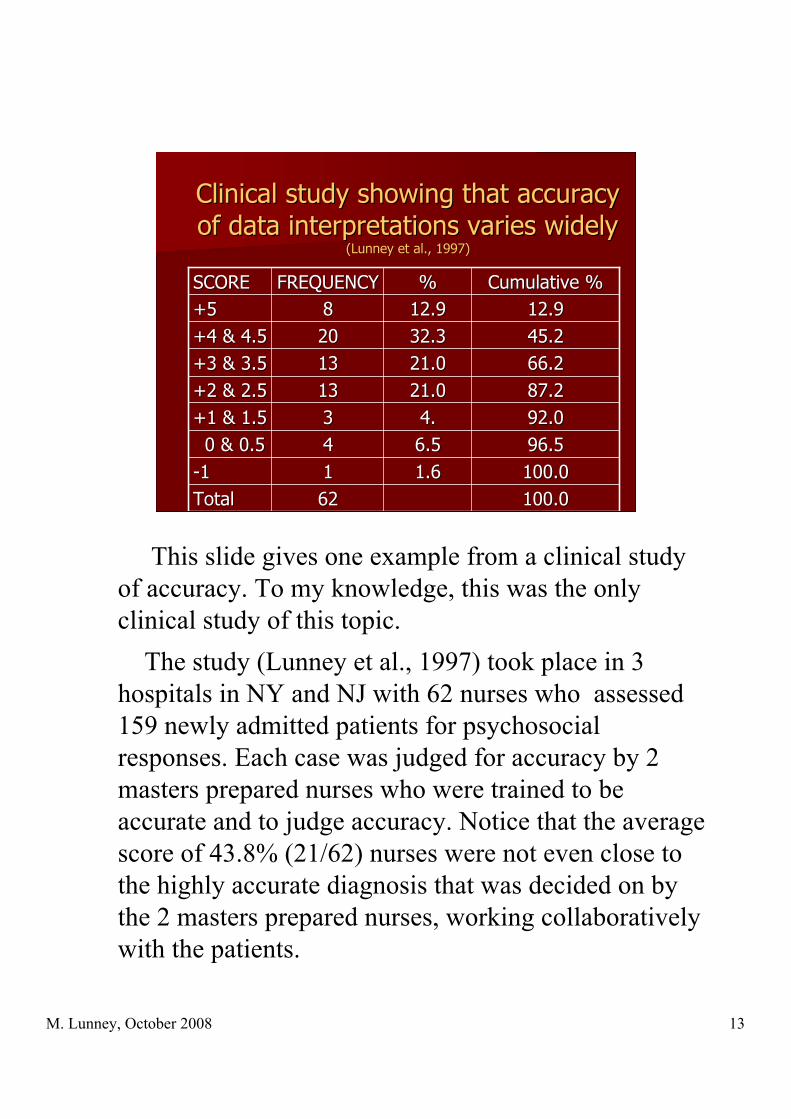
100.0100.06262TotalTotal100.0100.01.61.611-1-196.596.56.56.544 0 & 0.5 0 & 0.592.092.04.4.33+1 & 1.5+1 & 1.587.287.221.021.01313+2 & 2.5+2 & 2.566.266.221.021.01313+3 & 3.5+3 & 3.545.245.232.332.32020+4 & 4.5+4 & 4.512.912.912.912.988+5+5
Cumulative %Cumulative %%%FREQUENCYFREQUENCYSCORESCORE
This slide gives one example from a clinical studyof accuracy. To my knowledge, this was the onlyclinical study of this topic. The study (Lunney et al., 1997) took place in 3hospitals in NY and NJ with 62 nurses who assessed159 newly admitted patients for psychosocialresponses. Each case was judged for accuracy by 2masters prepared nurses who were trained to beaccurate and to judge accuracy. Notice that the averagescore of 43.8% (21/62) nurses were not even close tothe highly accurate diagnosis that was decided on bythe 2 masters prepared nurses, working collaborativelywith the patients.

M. Lunney, October 2008 14
The difficulty is that (1)humanThe difficulty is that (1)humanexperiences are complex; (2)experiences are complex; (2)we do not know other people.we do not know other people.
You might be asking yourself at this point: WHY?Why do nurses have difficulty interpretinghuman responses to health problems and lifeprocesses.
The two main reasons are:1)Human beings are unique and complex. Nurses
are interested in the whole person, not just in anobjective part of the person.
2)We do not know other people. Sometimes, we actas if we do know them, but essentially we do notknow them. Thus, we have to listen carefully, usecritical thinking, and conduct really goodassessments in order to understand the needs ofother people.
M. Lunney, October 2008 15
This is an example of theThis is an example of thecomplexity of selecting the bestcomplexity of selecting the bestnursing diagnosis to guide care.nursing diagnosis to guide care.
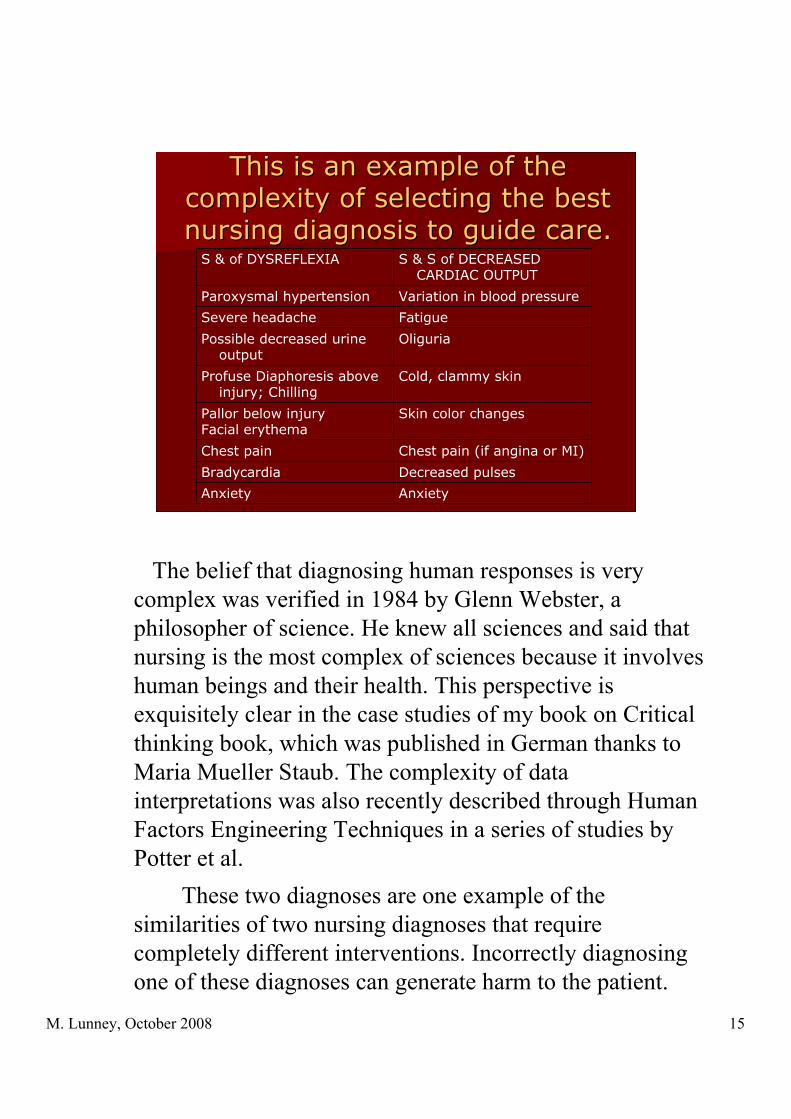
AnxietyAnxiety
Decreased pulsesBradycardia
Chest pain (if angina or MI)Chest pain
Skin color changesPallor below injuryFacial erythema
Cold, clammy skinProfuse Diaphoresis aboveinjury; Chilling
OliguriaPossible decreased urineoutput
FatigueSevere headache
Variation in blood pressureParoxysmal hypertension
S & S of DECREASEDCARDIAC OUTPUT
S & of DYSREFLEXIA
The belief that diagnosing human responses is verycomplex was verified in 1984 by Glenn Webster, aphilosopher of science. He knew all sciences and said thatnursing is the most complex of sciences because it involveshuman beings and their health. This perspective isexquisitely clear in the case studies of my book on Criticalthinking book, which was published in German thanks toMaria Mueller Staub. The complexity of datainterpretations was also recently described through HumanFactors Engineering Techniques in a series of studies byPotter et al. These two diagnoses are one example of thesimilarities of two nursing diagnoses that requirecompletely different interventions. Incorrectly diagnosingone of these diagnoses can generate harm to the patient.

M. Lunney, October 2008 16
Summary of Evidence: ResearchSummary of Evidence: Researchfindings over 4 decades showfindings over 4 decades showthat there is wide variation inthat there is wide variation inthe accuracy of nursesthe accuracy of nurses’’ data data
interpretations.interpretations.
In the Lunney, 2008a article, I summarized the evidence.All evidence over 4 decades verifies that there is widevariation in the accuracy of nurses’ data interpretations. This is a picture of the standard model ofEvidenced-Based Practice. Note in the black box on thebottom, it says we need to use the best availableevidence. We have sufficient evidence now to expectthat nurses accuracy will vary. And, when datainterpretations vary, it means that some interpretationsare not accurate enough to guide care.

M. Lunney, October 2008 17
Thus, the accuracy of nursesThus, the accuracy of nurses’’data interpretations should be adata interpretations should be a
serious concernserious concern..
With formal use ofWith formal use ofnursing diagnosisnursing diagnosis
OROR
Without formal use ofWithout formal use ofnursing diagnosisnursing diagnosis
-Does not communicate interpretations-Communicates “problems”
Thus, the accuracy of nurses’ diagnoses should be aserious concern of nurses worldwide, especially nurseleaders. This concern is relevant whether or not the healthcare system is using the language of nurses diagnoses.Nurses interpret data, regardless of whether they use alanguage system or not. In systems that are not usingnursing diagnoses, nurses either do not state theirinterpretations (they just act them and say what they did)or, nurses call their interpretations “problems,” orwhatever label is usually used in that system.
M. Lunney, October 2008 18
Nurses Nurses who do not usewho do not usestandardized nursing languages arestandardized nursing languages are
probably less accurate.probably less accurate. Extensional meaningExtensional meaning
IsIsbetter to use thanbetter to use than
IntensionalIntensional meaning meaning
I believe that nurses who do not use standardizednursing languages are probably less accurate than nurseswho use nursing classifications such as NANDA-I. This is because there are two kinds of meanings ofconcepts, extensional, or the meaning that is shared withother people based on classifications and other language-related tools, and intensional, the personal meaning thatwe attach to a concept. In nursing science, it is better touse the extensional meaning because it is important forthe quality of care to communicate our words to others.It is better if the meanings of words are shared withothers.

M. Lunney, October 2008 19
This picture shows how use of aThis picture shows how use of anursing diagnosis classification helpsnursing diagnosis classification helpsnurses to achieve more accurate datanurses to achieve more accurate data
interpretations interpretations (Lunney, 2008b).(Lunney, 2008b).
This picture shows how use of a nursing diagnosisclassification helps nurses to achieve more accurate datainterpretations (Lunney, 2008b). Having the namesavailable for human responses enables nurses to thinkabout these phenomena and to discern what is happeningwith individuals and families using names from theclassification, with definitions and descriptions. Becausewe have these names, it gives us the words tocommunicate and collaborate with other providers andpatients themselves in deciding what is the bestdiagnosis. Human beings can best work together when they havewords with which to communicate about what they think.We also think with words, so if we do not have words forsomething, we cannot even see that thing, e.g.,powerlessness.

M. Lunney, October 2008 20
The degree of accuracy isThe degree of accuracy isprobably not acceptable forprobably not acceptable for
quality care; needs to be studied.quality care; needs to be studied.
Going back to the English-languageresearch evidence, it suggests that thedegree of accuracy is probably lowerthan it should be for high quality care. Applying this model of results-drivenhealth care, it says that we shouldexpect the best care, i.e., highdiagnostic accuracy, we should measurethe factors that influence accuracy andthe outcomes of accuracy, we shoulddisclose the results of measurement, andwe should reward and support those whocontribute to high accuracy and betterresults.
M. Lunney, October 2008 21
Lack of attention to accuracyLack of attention to accuracycompounds the problem.compounds the problem.
The current lack of attention to the issue ofaccuracy compounds the problem of low accuracy. If we do not talk about it or even recognize itas a problem, we cannot achieve higher levels ofaccuracy.

M. Lunney, October 2008 22
Low accuracy contributes toLow accuracy contributes to- Harm to patients & families- Harm to patients & families- Wasted time and energy- Wasted time and energy- Absence of positive outcomes- Absence of positive outcomes- Patient dissatisfaction- Patient dissatisfaction- Higher costs- Higher costs
This is a serious problem because low accuracycontributes to:
- Harm to patients- Wasted time & energy treating diagnoses,e.g., knowledge deficit- Absence of positive outcomes, and-Patient and family dissatisfaction, and-Higher costs (from wasted time and energy)
M. Lunney, October 2008 23
The status of this predictionThe status of this predictionfrom 1963 is that from 1963 is that we are notwe are not
there yetthere yet..
““I envision the day whenI envision the day whennurses will spend timenurses will spend timediscussing discussing ‘‘what is thewhat is the
diagnosis?diagnosis?’’
KomoritaKomorita, N.I. (1963). Nursing diagnosis., N.I. (1963). Nursing diagnosis.
American Journal of Nursing, 63 American Journal of Nursing, 63 (12), 83-86 83-86..
In 1963, Komorita said“I envision the day when nurses will spend time
discussing ‘what is the diagnosis?’Komorita, N.I. (1963). Nursing diagnosis.
American Journal of Nursing, 63 (12), 83-86.We are not there yet but we need to work on getting there.
M. Lunney, October 2008 24
The EHR is being implementedThe EHR is being implementedworldwide.worldwide.
The EHR is being implemented worldwide. This meansthat the impact of low accuracy data interpretations will bemore dramatic than it has been in the past with paper records. All data will be used more efficiently and will beavailable for aggregation and comparison to know how wellwe are doing with health outcomes. The data interpretations of nurses will be visible toeveryone. Besides the nurse who made the diagnosis,everyone else will be expected to address this phenomena aswell. The negative effects of low accuracy, e.g., wasted timeand money, will be even greater with an EHR than it is now.
M. Lunney, October 2008 25
With the EHR, nursesWith the EHR, nurses’’ data datainterpretations will be visible andinterpretations will be visible and
used by others.used by others.
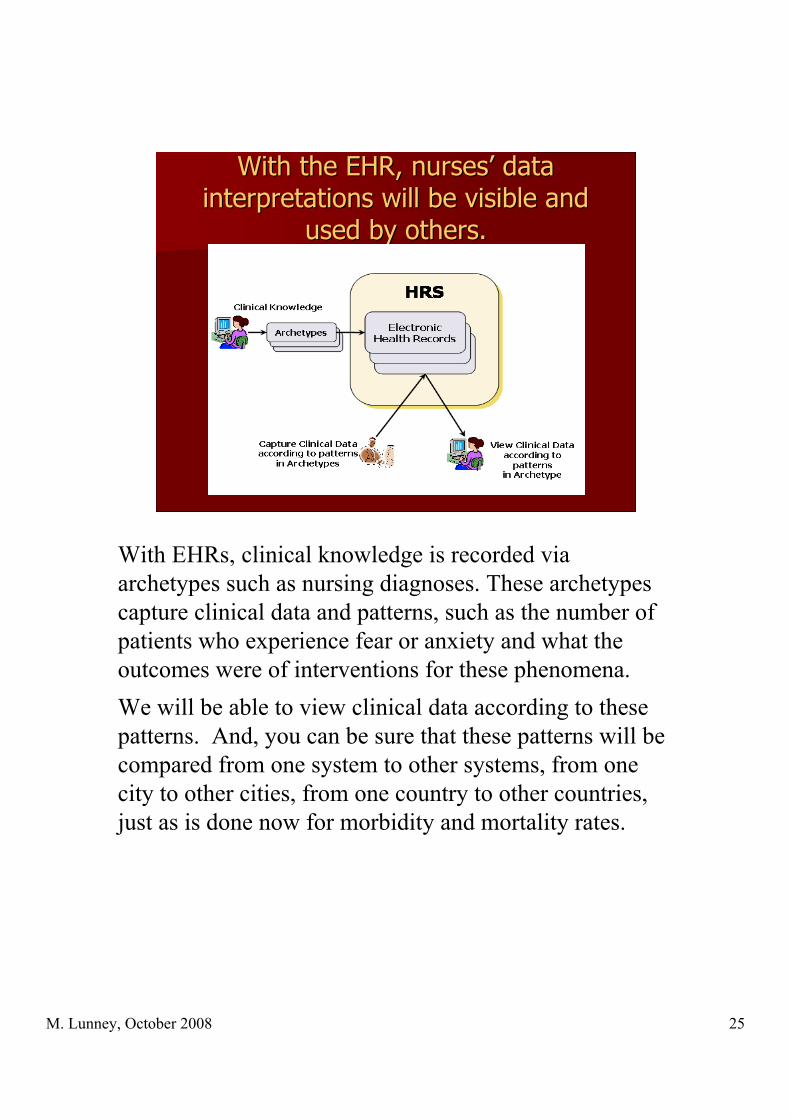
With EHRs, clinical knowledge is recorded viaarchetypes such as nursing diagnoses. These archetypescapture clinical data and patterns, such as the number ofpatients who experience fear or anxiety and what theoutcomes were of interventions for these phenomena.We will be able to view clinical data according to thesepatterns. And, you can be sure that these patterns will becompared from one system to other systems, from onecity to other cities, from one country to other countries,just as is done now for morbidity and mortality rates.

M. Lunney, October 2008 26
Data, diagnoses, interventions &Data, diagnoses, interventions &outcomes will be transported locally,outcomes will be transported locally,
regionally, nationally andregionally, nationally andinternationally.internationally.
We will be required to pass on certain kinds of data, e.g.,the nursing care elements of the nursing minimum dataset (nurses’ diagnoses, interventions, outcomes andintensity), to our national statistical centers.In the U.S., this will be the CDC in Atlanta, Georgia. TheSwiss will probably send their data to Geneva. Is thatright?

M. Lunney, October 2008 27
The impact of diagnostic accuracy willThe impact of diagnostic accuracy willbe exquisitely clear to everyone.be exquisitely clear to everyone.
Thus, the impact of diagnostic accuracy will becomeexquisitely clear to everyone. The outcomes of nursingcare that are influenced by diagnostic accuracy may be asgood as others, better than others, or worse than others.

M. Lunney, October 2008 28
It is It is time nowtime now to attend to to attend todiagnostic accuracy.diagnostic accuracy.
To conclude this part of the paper, it is time now to attendto or address diagnostic accuracy. In this cartoon, the catowner says, “As time passes you get fatter and fatter.And the cat says, “ah yes, the age old dilemma, how tostop time.”
Well, we cannot stop time, so it is time to address thisissue so that it gets better, not worse.

M. Lunney, October 2008 29
Strategies can be developed atStrategies can be developed atthe system-wide level.the system-wide level.
ProfessionalismProfessionalism AutonomyAutonomy Complex decision-makingComplex decision-making Collaborative practiceCollaborative practice Patient-nurse partnershipsPatient-nurse partnerships Time to think & reflectTime to think & reflect Evidence-based practiceEvidence-based practice
Studies of system-wide policies and procedures need to beconducted to identify factors that impact on accuracy, e.g.,the support that is necessary for nurses to be more professional,be make autonomous decisions, to be able to achieve complexdecision-making, to work collaboratively with other nurses andwith patients and families, to establish patient-nursepartnerships, and to achieve evidence-based practice. Some ofthese system-wide factors are currently being studied but not inrelation to accuracy. Studies of the effects of nurse-patient ratios and quality ofcare are relevant to accuracy as well as studies of nurses’abilities to implement evidence-based practice.

M. Lunney, October 2008 30
Promote nursesPromote nurses’’ image as image asdiagnosticians.diagnosticians.
From day 1 of nursing education programs, students need to startthinking of themselves as developing diagnosticians. This image can bereinforced and supported throughout education and practice experiences. Based on the complexity of decision making in nursing, we need to helpnurses develop tolerance for ambiguity. Students and nurses can bereminded that they are helping people with complex responses to healthproblems and life processes and that errors in diagnosing are consistentlypossible. They can be taught to recognize ambiguity and ways to deal withit, e.g., seek consultations, obtain research evidence, validate impressions. Nurse-patient partnerships are probably essential to obtain valid andreliable data from patients. The need for critical thinking skills is self evident. More is written about this in the articles on the bibliography. EBN can be fostered by helping nurses to develop competencies forseeking and using research evidence.

M. Lunney, October 2008 31
Develop and test decisionDevelop and test decisionsupport tools, e.g., standardssupport tools, e.g., standards
of care for specific populations.of care for specific populations.
problemproblem
Action
Research Plan
Action
Research Plan
DataData
ResultsResults
Action
Research
problemproblem
Action
Research Plan
Action
Research Plan
DataData
ResultsResults
Action
Research
Recently, I have been using action research methods toidentify the standards of care that apply to specific populations.This is a detailed method for experienced nurses to sit downtogether and decide what nursing diagnoses and associatedoutcomes and interventions generally apply to the people theyserve. We have had very good results with this method. I amwaiting for Judy Carlson, the founder of this research method topublish an article on how to do it. If you are interested inconducting this type of consensus validation study, write to meand I will help. It is also possible to use decision support tools, such asalgorithms, decision support trees, & practice protocols andguidelines. Some good references on this topic were cited in theLunney 2008a article.
M. Lunney, October 2008 32
Provide resources that containProvide resources that containEBN knowledge.EBN knowledge.http://www.nanda.orghttp://www.nanda.orghttp://www.nursing.uiowa.edu/excellence/nursinhttp://www.nursing.uiowa.edu/excellence/nursing_knowledge/clinical_effectiveness/index.htmg_knowledge/clinical_effectiveness/index.htm
Sophisticated knowledge resources are essential to achievehigh rates of accuracy. These include the latest books ondiagnosis development, clinical experts that can function asconsultants, and access to research evidence through theInternet, Cochrane reviews, and other sources. The new NANDA-I Book is coming out in December of thisyear. The new NOC and NIC books were just published in 2008.The next editions are expected in 2012, so this is a good time topurchase them. If you use them in courses, you can ask theInternational Mosby representative for desk copies.NOC is a research-based classification of patient outcomes thatare sensitive to the quality of nursing care. NIC is a research-based classification of nursing interventions.

M. Lunney, October 2008 33
Study the effects of high and lowStudy the effects of high and lowaccuracy on health outcomes.accuracy on health outcomes.
In a recently published study, Welton & Halloran (2005) substantiatedthat use of nursing diagnoses explains a significant amount of variance inpatient outcomes such as length of stay and disposition to nursing homes.Similar studies need to be done to show the relation of high vs. lowaccuracy of nurses’ diagnoses and patient outcomes. EHRs need to bedesigned so that accuracy can be systematically and regularly examined.For example, the findings from assessment screens should be separatefrom diagnostic screens so data support for diagnoses can beretrospectively examined for the adequacy of data support. One thing to consider is a request for patient and family signatures onthe diagnoses that they validate and for which they agree to treatment,i.e., contracts between nurses and patients re: which diagnoses will beaddressed.

M. Lunney, October 2008 34
Develop rewards for accuracy, e.g.,Develop rewards for accuracy, e.g.,acknowledgement, feedback.acknowledgement, feedback.
Remember the model for results-driven health care, itincluded rewards such as acknowledgement and feedback forhigh quality care. Since nurses do not follow specific patients to other unitsand disposition to home or other health care agencies, it wouldbe helpful to create feedback systems so nurses could know theoutcomes of their diagnoses and be able to have evidence ofindividual patient outcomes. If the public knew that nurses’ diagnose human responses,it would promote accountability for accuracy. This could bedone through agency newsletters, local newspapers, and byacknowledging diagnostic processes and outcomes with patients& families.

M. Lunney, October 2008 35
Encourage nurses to collaborateEncourage nurses to collaboratetoward the achievement of diagnostictoward the achievement of diagnostic
accuracy.accuracy.
For accuracy, it is very important for nurses collaboratewith each other and with patients and families. If wework together, we will be able to accurately identify theresponses that should be treated.Isn’t this a cute cartoon showing the value of workingtogether and sharing the task instead of trying to go italone.
M. Lunney, October 2008 36
Work together toward theWork together toward theprofessional goal of diagnosticprofessional goal of diagnostic
accuracy and treatment ofaccuracy and treatment ofhuman responses.human responses.
Nurse leaders in Switzerland, the U.S., and othercountries can also work together toward the professionalgoal of diagnostic accuracy and the associatedinterventions and outcomes.

M. Lunney, October 2008 37
Excellence in nursing is achieved whenExcellence in nursing is achieved whenwe provide the best possible care forwe provide the best possible care forpatients and families. The quality ofpatients and families. The quality of
care depends on diagnostic accuracy.care depends on diagnostic accuracy.
Excellence in nursing is achieved when we provide thebest possible care for patients and families.And the quality of care will depend on diagnosticaccuracy.

M. Lunney, October 2008 38
Comments or QuestionsComments or Questions