everything - ahcsa.org.au · 2 everything goes great until there’s a problem – corporate...
TRANSCRIPT
Corporate Governance in Aboriginal Community ControlledHealth Services in NSW: The Theory and The Practice
Everything
Aboriginal Health & Medical Research Council of NSWThis project was funded by the Commonwealth Department of Health and Ageing
May 2011
Until There’s a Problem
Goes Great


Everything
Until There’s a Problem
Goes Great
Corporate Governance in Aboriginal Community Controlled Health Services in NSW: The Theory and The Practice
A report for the Aboriginal Health & Medical Research Council of NSW
May 2011

2 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Author: Kirsty McEwin
Aboriginal Health & Medical Research Council of NSW
PO Box 1565Strawberry HillsNSW 2012
Ph: 02 9212 4777
www.ahmrc.org.au
©AH&MRC May 2011
Acknowledgements
The author would like to acknowledge the contributions of many people including the representatives of the five participating Aboriginal Community Controlled Health Services, the three auspicing organisations and the members of the AH&MRC Corporate Governance Reference Group.
Artwork
Cover art by Connie Ah See, a Wiradjuri migay (woman) from Wellington NSW.
Printed on ecoStar – a Carbon Neutral, FSC 100% post consumer recycled paper product using vegetable oil-based inks and an environmentally friendly alcohol-free printing process. ecoDesign ecoPrint FSC chain of custody No. QMI-COC-001113
Cert no. QMI-COC-001113

3Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Acknowledgements ........................................................................................................................................... 2
Acronyms ............................................................................................................................................................... 4
Preface ................................................................................................................................................................... 4
Executive Summary ........................................................................................................................................... 5
Recommendations ............................................................................................................................................ 7
1: AH&MRC Corporate Governance Project ....................................................................................10
1.1 Introduction .................................................................................................................................101.2 Project Methodology .................................................................................................................10
2: The Theory ...............................................................................................................................................11
2.1 Governance ................................................................................................................................112.2 Corporate Governance .............................................................................................................112.3 Aboriginal Corporate Governance .........................................................................................112.4 Indigenous Corporate Governance Project.........................................................................112.5 Support Systems for Indigenous Primary Healthcare Services Project ......................122.6 Literature Review on Aboriginal Corporate Governance .................................................12
3: The Practice ..............................................................................................................................................19
3.1 Aboriginal Community Controlled Health Services ...........................................................193.2 Regulatory Arrangements in NSW ACCHSs .....................................................................203.3 ACCHSs Participating in the AH&MRC Corporate Governance Project ....................20 3.4 Changing Landscape and Political Environment ...............................................................23 3.5 Tensions, Practice and a Proviso ...........................................................................................25
4: Recommendations .................................................................................................................................29
4.1 Framework for Good Governance for NSW ACCHSs .....................................................29 4.2 Training in Corporate Governance and Strategic Planning ............................................31 4.3 AH&MRC Governance Symposium ......................................................................................32 4.4 Board Membership ....................................................................................................................33 4.5 CEO Meetings and Support ....................................................................................................34 4.6 AH&MRC Governance Support Team..................................................................................34 4.7 Corporate Governance Resources for ACCHSs ...............................................................36
References ........................................................................................................................................................38
Appendix A: List of People Consulted ..........................................................................................................44
Tables and Flowchart
Table 1: Regulatory Arrangements in NSW ACCHSs (March 2011) ........................................20Table 2: Framework for Good Governance for ACCHS ....................................................... 7 & 30Flowchart 1: AH&MRC Corporate Governance Recommendations .......................................... 9 & 37
Contents

4 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Acronyms
ACCH Aboriginal Community Controlled Health
ACCHS Aboriginal Community Controlled Health Service
ACCHO Aboriginal Community Controlled Health Organisation
AGPAL Australian General Practice Accreditation Limited
AH&MRC Aboriginal Health and Medical Research Council
ANU Australian National University
ASIC Australian Securities and Investments Commission
CAEPR Centre for Aboriginal Economic Policy Research
CATSI Corporations Aboriginal and Torres Strait Islander
COAG Council of Australian Governments
ICGP Indigenous Community Governance Project
NACCHO National Aboriginal Community Controlled Health Organisation
NHHR National Health and Hospitals Reform
OATSIH Office of Aboriginal and Torres Strait Islander Health
ORIC Officer of the Registrar of Indigenous Corporations
WIPO Workforce Initiatives and Programs Officer
Preface
“Good intentions don’t run organisations.” (Mr Jamie Newman, CEO Orange Aboriginal Health Service, June 2010)
“It is only when effective governance is in place that communities and regions will have a solid foundation for making sound decisions about their overall goals and objectives, what kind of life they want to try to build, what assets they have or require, what things they want to retain, protect or change, the kind of development they want to promote or reject, and what actions they need to take to achieve those goals.” (Dodson and Smith, 2003)

5Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
The Aboriginal Health and Medical Research Council of NSW (AH&MRC) Corporate Governance Project was funded by the Office of Aboriginal and Torres Strait Islander Health (OATSIH) to examine governance arrangements in different models of Aboriginal Community Controlled Health Services (ACCHSs) in NSW. Five ACCHSs from across NSW and with different corporate structures participated in the project and representatives from many other services and organisations were also consulted. The objectives of the project were: to build on the corporate governance capacities of the participating ACCHSs; to enable the AH&MRC to further engage in the area of corporate governance support as part of its broader member services support role; and to encourage the exploration of opportunities to further develop the corporate governance models for the Aboriginal Community Controlled Health Sector in NSW.
The project had three stages: reviewing the literature on Aboriginal Corporate Governance; establishing a Reference Group and identifying five ACCHSs willing to participate in the project; and consulting the participating ACCHSs and other stakeholders to identify how best the AH&MRC and ACCHSs could support corporate governance capacity by (i) identifying the issues impacting on corporate governance effectiveness and (ii) making recommendations for future actions.
The findings from the project confirmed that there are many examples of good governance practice in NSW ACCHSs. The findings also revealed that ‘good practice’ is consistent
with the literature on Aboriginal Corporate Governance. While no one size fits all, there are principles of good practice that can be observed in the services that have the most effective governance arrangements. The principles include the appointment of boards that are demographically representative of their communities and have diversity in board membership and an appropriate skills mix; that have strong links back to their communities and mechanisms to engage with the communities; that understand the roles and responsibilities of board members; that have strong CEOs who are effective communicators; that have mechanisms in place to monitor performance and to ensure internal accountability; that have long term visions for their services which are shared by management and the community; that are engaged in strategic planning and monitoring activities linked to board meeting processes and planning cycles; and that have two or three year staggered board terms to facilitate a balance between continuity and board renewal.
There are many challenges facing ACCHS board directors and CEOs, not least of which is how to best run an organisation that must compete for funds in a rapidly changing political landscape and in a climate of increasing funding contestability. As well, inherent tensions may exist between Aboriginal culture and values and mainstream concepts of corporate governance and funding compliance requirements. Aboriginal values may include obligations based on kinship relationships and putting family
Executive Summary

6 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
needs before business goals. ACCHS board directors have the challenging role of balancing cultural and community expectations with their legal and fiscal obligations. Board members may see the imposition of ‘white’ governance values and compliance requirements as foreign and unwanted and older members may feel the need to abandon their own values and beliefs about leadership and traditional governance in order to comply with funding agreements. The services that work best are those that manage the potential conflicts between the two ‘belief systems’ and those that have boards that are not too involved in the day to day activities of their services and yet at the same time are well equipped to effectively monitor their organisations.
The report makes a number of recommendations, which if accepted and funded, will see the AH&MRC becoming more active in supporting good governance practice across the Aboriginal Community Controlled Health (ACCH) sector in NSW.
7Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
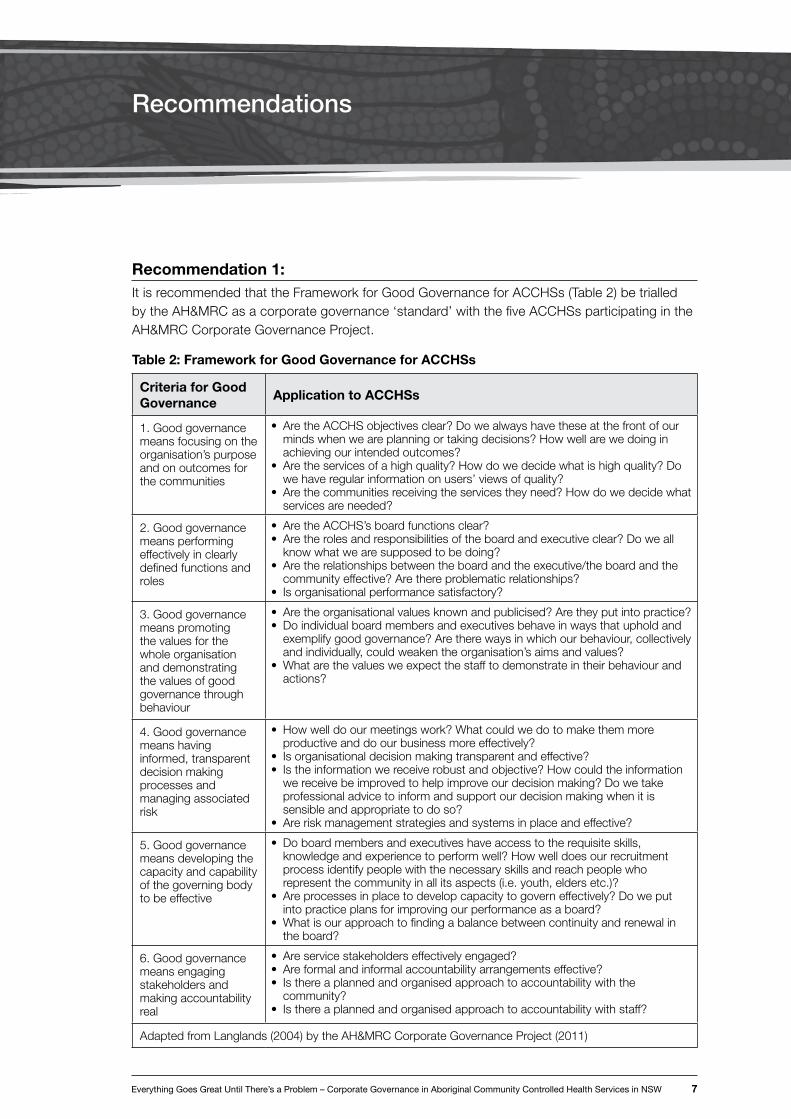
Recommendation 1:It is recommended that the Framework for Good Governance for ACCHSs (Table 2) be trialled by the AH&MRC as a corporate governance ‘standard’ with the five ACCHSs participating in the AH&MRC Corporate Governance Project.
Table 2: Framework for Good Governance for ACCHSs
Criteria for Good Governance
Application to ACCHSs
1. Good governance means focusing on the organisation’s purpose and on outcomes for the communities
• AretheACCHSobjectivesclear?Dowealwayshavetheseatthefrontofourmindswhenweareplanningortakingdecisions?Howwellarewedoinginachievingourintendedoutcomes?
• Aretheservicesofahighquality?Howdowedecidewhatishighquality?Dowehaveregularinformationonusers’viewsofquality?
• Arethecommunitiesreceivingtheservicestheyneed?Howdowedecidewhatservicesareneeded?
2. Good governance means performing effectively in clearly defined functions and roles
• AretheACCHS’sboardfunctionsclear?• Aretherolesandresponsibilitiesoftheboardandexecutiveclear?Doweall
knowwhatwearesupposedtobedoing?• Aretherelationshipsbetweentheboardandtheexecutive/theboardandthe
communityeffective?Arethereproblematicrelationships?• Isorganisationalperformancesatisfactory?
3. Good governance means promoting the values for the whole organisation and demonstrating the values of good governance through behaviour
• Aretheorganisationalvaluesknownandpublicised?Aretheyputintopractice?• Doindividualboardmembersandexecutivesbehaveinwaysthatupholdand
exemplifygoodgovernance?Aretherewaysinwhichourbehaviour,collectivelyandindividually,couldweakentheorganisation’saimsandvalues?
• Whatarethevaluesweexpectthestafftodemonstrateintheirbehaviourandactions?
4. Good governance means having informed, transparent decision making processes and managing associated risk
• Howwelldoourmeetingswork?Whatcouldwedotomakethemmoreproductiveanddoourbusinessmoreeffectively?
• Isorganisationaldecisionmakingtransparentandeffective?• Istheinformationwereceiverobustandobjective?Howcouldtheinformation
wereceivebeimprovedtohelpimproveourdecisionmaking?Dowetakeprofessional advice to inform and support our decision making when it is sensibleandappropriatetodoso?
• Areriskmanagementstrategiesandsystemsinplaceandeffective?
5. Good governance means developing the capacity and capability of the governing body to be effective
• Doboardmembersandexecutiveshaveaccesstotherequisiteskills,knowledgeandexperiencetoperformwell?Howwelldoesourrecruitmentprocess identify people with the necessary skills and reach people who representthecommunityinallitsaspects(i.e.youth,eldersetc.)?
• Areprocessesinplacetodevelopcapacitytogoverneffectively?Doweputintopracticeplansforimprovingourperformanceasaboard?
• Whatisourapproachtofindingabalancebetweencontinuityandrenewalintheboard?
6. Good governance means engaging stakeholders and making accountability real
• Areservicestakeholderseffectivelyengaged?• Areformalandinformalaccountabilityarrangementseffective?• Isthereaplannedandorganisedapproachtoaccountabilitywiththe
community?• Isthereaplannedandorganisedapproachtoaccountabilitywithstaff?
Adapted from Langlands (2004) by the AH&MRC Corporate Governance Project (2011)
Recommendations

8 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Recommendation 2:It is recommended that the AH&MRC seeks funding to provide an ‘Introduction to Corporate Governance Board Training’ program that would be offered to all new ACCHS board members on a state-wide basis at the beginning of each calendar year (after the school holidays). CEOs and serving board members could be invited to participate as well. A Board Induction Kit would be provided to assist with and complement the introductory board training. The training could be organised through the Aboriginal Health College.
Recommendation 3:It is recommended that the AH&MRC seeks funding to provide governance training to ACCHSs on a regional level that is tailored to suit the ACCHSs involved and is pitched ‘higher’ than an ‘Introduction to Corporate Governance’ program (in recognition of board experience and prior learning). The training could lead to Certificate IV in Business (Governance) qualifications. The training could be organised through the Aboriginal Health College.
Recommendation 4:It is recommended that the AH&MRC seeks funding to provide training in strategic planning for ACCHS boards which could be offered regionally and include discussions about contextual issues impacting on ACCHSs such as the Council of Australian Governments (COAG) initiatives e.g. Closing the Gap and National Health and Hospitals Reform.
Recommendation 5:It is recommended that the AH&MRC holds a Corporate Governance Symposium in 2011 for ACCHS CEOs and board chairs. The program would include sessions on the principles of good governance in the ACCH sector, discussions on the strategic issues that impact on good governance and opportunities to showcase examples of good governance practices in ACCHSs. CEOs and board chairs could meet separately in pre or post workshop meetings.
Recommendation 6:It is recommended that the AH&MRC, at its Governance Symposium (Recommendation 5), showcases the strategies that ACCHSs employ, consistent with the principles of good governance, to ensure that their boards are demographically representative of their communities and balance community and cultural drivers with specialist skill sets. Such strategies include proactively encouraging young people onto boards; holding pre AGM workshops to increase the level of awareness of the roles and responsibilities of directors; and co-opting experts onto boards as ex-officio directors where those skill sets aren’t available on the board.
Recommendation 7:It is recommended that, consistent with the principles of good governance, the AH&MRC works with those ACCHSs that have not yet moved away from annual board appointments to enable the services to introduce constitutional changes that will give board directors terms of either two or three years (or a combination thereof) with the directors appointed on a staggered basis.

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 9
Recommendation 8:It is recommended that the AH&MRC Workforce Initiatives and Programs Officer (WIPO) be supported by the AH&MRC in (i) working with ACCHS CEOs to develop CEO training, networking and peer support opportunities; (ii) facilitating annual CEO workshops; and (iii) extending the training and development programs to middle managers in the future.
Recommendation 9:It is recommended that the AH&MRC considers the feasibility of establishing a Governance Support Team to assist
and promote governance capacity in the NSW ACCHS sector. Consideration would need to be given to the development of a communication protocol between the AH&MRC and Member Services that would enable the AH&MRC to be involved with an ACCHS while protecting the principles of autonomy and self determination of the service.
Recommendation 10:It is recommended that the AH&MRC include a list of useful governance resources on its website and that the website be updated regularly to ensure currency of the materials.
Flowchart 1: AH&MRC Corporate Governance Recommendations
Recommendation 1
Trial ACCHS Framework for Good Governance with 5
ACCHSs as AH&MRC corporate governance
‘standard’
Recommendation 2
Introductory level governance training for all ACCHS Board members. Development of
Board Induction Kit
Recommendation 3
Regionally based higher level governance training tailored
to services
Recommendation 5
AH&MRC host a Corporate Governance Symposium in 2011
for CEOs and Chairpersons
Recommendation 8
AH&MRC WIPO role be supported to include
development of CEO training and peer support opportunities
Recommendation 10
AH&MRC to provide governance resources on
its website
Recommendation 7
Constitutional changes to ACCHSs for 2 or 3 year staggered board
appointments
Recommendation 6
Showcase best practice including strategies aimed at ensuring demographic
representation skills mix on ACCHS Boards
Recommendation 9Establish Governance
Support Team
Recommendation 4
Regionally based strategic planning training

10 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
1 AH&MRC Corporate Governance Project
1.1 Introduction The Aboriginal Health and Medical Research Council of NSW Corporate Governance Project was funded by the Office of Aboriginal and Torres Strait Islander Health to examine governance arrangements in different models of Aboriginal Community Controlled Health Services in NSW. Five ACCHSs, representing a range of different localities and corporate structures, were invited to participate in the project. These were Armajun Aboriginal Health Service (auspiced by Bulgarr Ngaru Medical Aboriginal Corporation), Bullinah Aboriginal Health Service (previously auspiced by North Coast General Practice Network), Coomealla Aboriginal Health Corporation, Illawarra Aboriginal Medical Service Corporation and Tamworth Aboriginal Medical Service (auspiced by North West Slopes Division of General Practice).
The objectives of the project were:
• to build on the corporate governance capacities of the participating ACCHSs;
• to enable the AH&MRC to further engage in the area of corporate governance support as part of its broader member services support role; and
• to encourage the exploration of opportunities to further develop the corporate governance models for the Aboriginal Community Controlled Health Sector in NSW.
A Reference Group was established to guide the project comprising representatives of the AH&MRC (Ms Melinda Bell – Chair); OATSIH (Mr Nathan Jones); ACCHS CEOs (Mr Darren Ah See, Wellington Aboriginal Corporation Health Service; Mr David Kennedy, Galambila Aboriginal Health Service; Ms Cathie Sinclair,
Yerin Aboriginal Health Services); Aboriginal Health College (Mr Terry Smith); and an independent member (Mr Wayne Munster, NSW Aboriginal Land Council). Ms Kirsty McEwin was appointed to manage the project.
The project had three stages:
• reviewing the literature on Aboriginal Corporate Governance;
• establishing a Reference Group and identifying five ACCHSs willing to participate in the project; and
• consulting the participating ACCHSs and other stakeholders to identify how best the AH&MRC and ACCHSs could support corporate governance capacity by (i) identifying the issues impacting on corporate governance effectiveness and (ii) making recommendations for future actions.
1.2 Project Methodology Kirsty McEwin was contracted by the AH&MRC to undertake the AH&MRC Governance Project. The published and unpublished literature was interrogated and a review of the literature was prepared. A Reference Group was established to guide the project and met by teleconference five times. Five ACCHSs were invited to participate in the project, three of which were under auspice (with one achieving independence during the course of the project) and the views of the auspicing organisations were also sought. Many other people were consulted including CEOs and board members from other ACCHSs and individuals from a number of other organisations. A list of all those consulted is included in Appendix A.

11Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
2.1 Governance Governance is a broad term for how an organisation or a group of people operates or governs itself. Governance is made up of processes (how things are done), structures (the ways people organise themselves and relate to each other) and institutions (the rules for how things should be done) (Reconciliation Australia, 2007, p 8). Governance is about power, relationships and accountability, i.e. who has influence, who decides, and how decision-makers are held accountable (Plumptre and Graham, 1999). The function of governance is to ensure that an organisation or partnership fulfils its overall purpose, achieves its intended outcomes and operates in an effective, efficient and ethical manner (Langlands, 2004, p 7).
2.2 Corporate GovernanceThe term corporate governance is a more specific term than governance in that it refers to the type of governance that is specific to a corporation (or a company or an association). “Corporate governance refers to the framework of rules, relationships, systems and processes within and by which authority is exercised and controlled in corporations” (Owen, 2003 quoted in ORIC Research Paper, 2010, p 9). Or to put it simply, corporate governance is the “system of control and accountability for an organisation” (Dwyer et al, 2007, p 8). It influences how the objectives of a corporation are set and achieved, how risks are monitored and assessed and how performance is optimised (Moriarty, 2010).
The key elements of good corporate governance include honesty, trust and integrity, openness, performance orientation, responsibility and accountability, mutual respect, and commitment to the organisation
(http://en.wikopedia.org/wiki/Corporate_governance accessed 14th May 2010).
2.3 Aboriginal Corporate Governance
The term Aboriginal corporate governance refers to corporate governance as it applies to Aboriginal community controlled organisations. The term recognises that Aboriginal community organisations have their own specific issues. Good Aboriginal governance “develops community capacity, fosters leadership, models success and influences policy. Where communities are supported in building stable, capable and legitimate governing institutions improvements in other aspects of community life will follow” (Reconciliation Australia, 2008, p 5).
The concept of Aboriginal corporate governance is relatively new and draws on international research, particularly the findings of the Harvard Project on American Indian Economic Development (see 2.6 below).
2.4 Indigenous Community Governance Project
The Indigenous Community Governance Project (ICGP) was the first national project to research Indigenous governance in Australia and to assess the extent to which lessons from overseas had relevance in this country. It was a joint project between the Centre for Aboriginal Economic Policy Research (CAEPR) at the Australian National University (ANU) and Reconciliation Australia. It was funded by an Australian Research Council linkage grant and ran for five years from 2003 to 2008. The chief investigators were Professor Mick Dodson (Institute of Indigenous Studies at ANU) and Dr Diane Smith and Dr Will Saunders (CAEPR).
2 The Theory

12 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
The ICGP set out to understand the nature of Indigenous community governance to determine what works, what doesn’t work and why. It examined different models of governance, the factors influencing culturally legitimate governance arrangements in Indigenous communities, the shortfalls in governance skills and capacities as well as governance strengths, and the wider governance environments and policy networks including the role and impact of State, Territory and Federal Government policy and service delivery on the effectiveness of community governance. (http://www.reconciliation.org.au/home/projects/indigenous-governance-research-project, accessed 30th April 2010). The ICGP research looked closely at 13 Aboriginal and Torres Strait Islander community organisations including one in NSW (in Newcastle). The ICGP produced a large number of useful research papers and a detailed bibliography.
2.5 Support Systems for Indigenous Primary Healthcare Services Project
The first national research project looking specifically at governance in Aboriginal Community Controlled Health Organisations (ACCHOs) is the Support Systems for Indigenous Primary Healthcare Services Project (the Support Systems Project). The project was identified as a priority project by the Board of the Cooperative Research Centre in Aboriginal Health after consultation with Aboriginal Community Controlled Health Organisations and the sector and aims to develop knowledge about how to support the corporate functions of ACCHOs and therefore to contribute to improving the viability and sustainability of ACCHOs across Australia
(http:// www.crcah.org.au/research/support_systems_phc.html accessed 31st May 2010).
The project received three year funding from 2008. It was led by Professor Ian Anderson (Director of Onemda VicHealth Koori Health Unit, Melbourne University) and conducted by Kate Silburn (Australian Institute of Primary Care, La Trobe University) and Alister Thorpe (Onemda VicHealth Koori Health Unit, Melbourne University). The project aimed to improve the quality and sustainability of ACCHOs as corporate entities through improved knowledge of how to strengthen organisational capacity to access and take up appropriate corporate support required for optimum organisational functioning, including sound governance and management practices and the provision of high quality comprehensive primary health care services. The final report of the project was released in December 2010 (Silburn, Thorpe and Anderson, 2010).
2.6 Literature Review on Aboriginal Corporate Governance
This literature review on Aboriginal Corporate Governance builds on the work of the Indigenous Community Governance Project and the Support Systems for Indigenous Primary Healthcare Services Project (see 2.4 and 2.5 above) as well as the work of other State/TerritoryAffiliatesandNACCHO,theNSW Aboriginal Lands Council and the Office of the Registrar of Indigenous Corporations. Searches for relevant articles were also made on the PubMed and Google Scholar websites. The literature is summarised under a number of different headings.

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 13
The Harvard Project
The Harvard Project on Indian Economic Development has been operating for more than twenty years and is based in the John F Kennedy School of Government in USA. Its work is concerned with relationships between economic development, governance principles and social well being within Indigenous communities. Representatives of the project have toured Australia several times and presented summaries of their work at Indigenous governance conferences (Sullivan, 2006, p 4). In the absence of Australian literature on best practice in Indigenous organisations researchers looked to the Harvard Project for direction. “In Australia the Harvard studies are generally interpreted as offering a solution to a widespread concern of post-colonial development: How to implement Indigenous governance that is respectful of cultural norms, responsive to local wisdom and at the same time delivers practical outcomes that reassure institutional investors” (Sullivan, 2006, p 8). The project found that: Indigenous tribes that made their own decisions perform better than those that included outside decision makers; culture strengthens governance; successful tribal governments share several institutional attributes, such as fairness in dispute resolution, the separation of the functions of elected representation and business management, and successful implementation of tribal policies that advance tribal strategic goals; and good governance in Indigenous organisations is consistent with standard public administration principles (Support Systems Project Draft Literature Review, 2008, p 5).
Why Aboriginal Governance Matters
The concept of Aboriginal corporate governance is important because the principles and practices of corporate governance can not be separated from their political, institutional, ideological and cultural contexts. As Hunt and Smith write “(there is) a growing recognition that governance, and evaluations of its effectiveness, are the products of culturally-based systems” (Hunt and Smith, 2006, p3). In other words what is good governance in one cultural context, for example, the for-profit business community, may not translate to good governance in a not-for-profit Aboriginal community controlled organisation. This had led to the development of the concept of the ‘governance environment’.
Governance Environment
The governance environment refers to the cultural context within which an organisation operates. Governance does not exist in isolation. It is located in the wider governance environment and therefore needs to be cognisant of elements in that environment. This includes the particular values of the Aboriginal community or communities, funding body requirements, government policy frameworks and so on. It also recognises that Aboriginal peoples have had their own ways of practising governance for tens of thousands of years which may be at odds with the dominant cultural values brought to Australia by the British colonisers (Reconciliation Australia, 2007, p 5 & p 9). Acknowledging the governance environment according to the Harvard Project, means having governance arrangements that “embody values that Indigenous peoples feel are important; reflect their contemporary conceptions of how authority should be organised and exercised;

14 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
are generated through Indigenous efforts; and therefore have the support of those they govern” (as quoted in Reconciliation Australia, 2007, p 24). Aboriginal and Torres Strait Islander values may include obligations based on kinship relationships and putting family needs before business needs (ORIC Research Paper, 2010, p 7).
Cultural Match
The notion of cultural match refers to governance arrangements that embody and reinforce the organisation’s preferred contemporary values, norms and conceptions of how authority should be organised and leadership exercised. Aboriginal organisational governance arrangements need to be informed by local cultural standards if they are to be regarded as legitimate by community members and yet at the same time need to work in the contemporary policy and funding environment (Dodson and Smith, 2003).
One Size Does Not Fit All
Effective governance recognises the governance environment and is based on local realities. No single model will be suitable for all community corporate governance. In other words no one size fits all. Hunt and Smith write “a key hurdle for government policy makers, in particular, is the fact that the issues involved (in corporate governance) are complex, conceptually challenging, multi-layered and do not lend themselves to straightforward or instant solutions. The findings… reflect the maxim that an imposed or ‘one size fits all’ policy approach to addressing many of the issues will likely prove to be both unworkable and unsustainable” (Hunt and Smith, 2007, p v).
Enabling Policy Frameworks
The work undertaken by the Queensland Aboriginal and Islander Health Council as part of its Investing in Community Control Project stresses the importance of governments providing enabling policy frameworks (and program guidelines) which will promote Indigenous capacity and authority. “At a minimum, governance needs to meet broader standards of corporate governance as well as ensuring cultural legitimacy and that organisations are run productively and in a way that reflects local priorities.” (Queensland Aboriginal and Islander Health Council, 2008, p 7). An enabling environment needs top-level political support and advocacy within government, an integrated approach to funding and a clear program focus located within a lead agency with a mandate and a lead Minister. “Anything less puts the government in the position of reproducing a disabling environment for Indigenous governance” (Smith, 2005, p 9).
Community Control
The Indigenous Community Governance Project defines community as a network of people and organisations linked together by a web of personal relationships, cultural and political connections and identities, networks of support, traditions and institutions, shared socioeconomic conditions, or common understandings and interests. Communities may therefore include not only geographically discrete settlements, but also dispersed communities of shared identity, voluntary communities of interest, and the policy and bureaucratic communities of government (Hunt and Smith, 2007). Community control is the ability, for the people who are going to use health services, to determine the nature of those services and then participate in the

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 15
planning, implementation and evaluation of those services. (Queensland Aboriginal and Islander Health Council Papers on Governance, http://www.qaihc.com.au/index.php?page=community-control-in-qld accessed on 30th March 2010). It means that Aboriginal communities have the right to make decisions that affect their health and well being.
Aboriginal Community Controlled Health Services
Aboriginal Community Controlled Health Services are based on the philosophy of self-determination and the principle of community control. ACCHSs are services initiated by and based in the Aboriginal community and governed by an Aboriginal body which is elected by the local Aboriginal community. They deliver a holistic and culturally appropriate health service to the communities that control them. The principle of community control requires that ownership and management is vested in the local Aboriginal community, generally through a board of management. “Decision making authority over healthcare (within the constraints of funding and regulation) is devolved to the community level. The model is based on the central role of the community and its delegation of decision making responsibilities in health to the ACCHS board” (Dwyer et al, 2007, p 2). Under this model good governance requires that organisations have genuine decision-making powers.
Challenges
Dwyer et al, (2007, p 6) examined previous studies into management issues in ACCHSs and reported limited work specifically examining these issues. Nonetheless there are some findings that are relevant to the AH&MRC Governance Project. A study by Wakerman et al (2000) reported that managers in ACCHSs will sometimes make a distinction between Aboriginal and non-Indigenous domains in order to minimise conflict or confusion. This may apply, for example, in the case of family obligations when a manager must make a distinction between respecting one’s senior family members and arguing with a senior member in the work place, failing to employ family members or being in the situation where board members have family members on staff. The need to make this distinction is one that a person working in mainstream health services is not generally required to make.
Dwyer et al (2007) also refer to articles by Wilson (2001) and Armstrong (2003) which impact on the governance of ACCHSs. Wilson identified the three key management issues that managers face as reconciling client and staff expectations with resources and practice constraints; reconciling community control ideology with the need for technical knowledge and hence a skilled and expert workforce; and reconciling the complexities of health status determinants with a clear organisational vision. Armstrong identified two different types of barriers to effective financial management: internal barriers which include the lack of understanding of the role of the board; and external barriers which are conflicts between the cultural values and financial accountability. Dwyer et

16 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
al conclude that the challenge for ACCHS boards and CEOs is to be able to deliver good governance as defined by funding bodies and regulators and at the same time to be able to find ways to give expression to the priorities and goals of the communities as determined by the community members.
Principles of Good Governance
Dalton (2008, p 4) believes that the basic principles of effective corporate governance can be encapsulated in three principles: transparency, accountability and corporate control. Other researchers have, however, been more expansive in their lists of principles. A collated list is provided below:
• the need for transparency;
• certainty of sufficient resources;
• equity and fairness – all people have opportunities to improve their well being;
• flexibility and choice;
• internal and external accountability – an organisation is accountable to its members, legislation, those affected by the decisions or actions and the public;
• responsiveness i.e. serving people’s needs, doing what is right and good for the organisation, the members and the broader community;
• acting in good faith and honesty;
• having clear procedures for appeal and redress;
• efficiency and effectiveness;
• legitimacy and mandate;
• recognising the rule of law – an organisation must respect legal frameworks;
• participation – all have a voice in decision making, either directly or through representative groups;
• consensus orientation;
• high level leadership skills;
• strategic vision – traditional owners to play a central role in identifying strategic directions and joint operational planning, monitoring and evaluation procedures;
• clearly identifying and developing the capacity of all parties involved;
• placing an emphasis on Indigenous youth;
• importance of interpersonal transactions.
(Support Systems Literature Review, 2008, pp 5 & 6; Sullivan, 2006; Dodson and Smith, 2003; Burdon and Torzillo, 2008)
Leadership
Professor Mick Dodson has said “the three key elements of good governance … are leadership, leadership and leadership” (Reconciliation Australia, 2007, p 51). Leaders are the foundation stone for community governance, for better or worse, depending on how leadership is exercised (Smith, 2005, p 11). A good leader works with people and motivates them to achieve a positive outcome towards a shared vision. Younger and emerging leaders should be supported and mentored.

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 17
Building Governance
Good governance can be actively built and strengthened through certain processes. These include establishing shared goals, agreed procedures, constitutions, policies and so on. “Building effective governance is a task which is achieved over time and is maintained with vigilance” (ORIC Research Paper, 2010 p 25). Sonnenfeld (2002), as quoted in ORIC Research Paper (2010, p 26) recommends that building governance is enhanced by:
• creating a climate of trust and candour, including rotating members through small groups to develop familiarity but avoid factions;
• fostering a culture of open dissent – distinguishing constructive professional conflict from disloyalty;
• using fluid portfolios to avoid typecasting individuals and to continue to challenge roles and assumptions;
• ensuring individual accountability, including explicit task completion by directors; and by
• evaluating the board’s performance, including full governing body evaluation, individuals’ self-assessment and peer reviews.
ICGP research also highlights several important lessons for building good governance. It states that effective and legitimate institutions (rules) are the foundation stones for exercising effective, legitimate governance. It takes hard work, time and commitment and, once achieved, should be protected by enshrining the elements of good
governance into constitutions, rules, policies, strategies, agreements and so on (Indigenous Community Governance Project, Indigenous Governance Matters, February 2008, p 6).
Governance Procedures
Bauman and Smyth (2007) as quoted in the Support Systems Literature Review (2008, pp 15-17) propose that competent and effective governance procedures involve:
• a degree of flexibility;
• consistently high level leadership skills;
• traditional owners playing a central role in identifying strategic directions and joint operational planning, monitoring and evaluation procedures which are matched against the emotional, procedural and substantive rights, needs and interests of parties;
• allocating sufficient resources and planning to participatory community development approaches;
• getting appropriate technical advice;
• clearly identifying and developing the capacity of all parties involved;
• integrating training activities across all the joint management partner organisations;
• placing an emphasis on Indigenous youth;
• having innovative pathways of employment, research partnerships and approaches to traditional owners undertaking contract work.

18 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Enhancing Good Governance
In addition to having appropriate procedures in place, good governance is enhanced by paying attention to the factors that Edwards and Clough describe as the “intangible governance factors” (quoted in ORIC Research paper, 2010, pp 24, 25). By “intangible” they mean that the factors can’t be quantified. Sonnenfeld refers to these as the “chemistry that works” (quoted in ORIC Research Paper, 2010, p 25). These factors include:
• clarity in roles, responsibilities, and relationships between the CEO and the board chair and the directors and management;
• ahealthyboardchair/CEOinterface;
• directors working as a team;
• culture, trust and open dissent;
• a mix of the right skills, competencies and characteristics;
• a good induction process and ongoing access to training;
• good leadership skills of the board chair;
• clear information flows; and
• regular evaluation of the board performance.
(Edwards and Clough (2005) quoted in ORIC Research Paper, 2010, pp 24 & 25)

19Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
3.1 Aboriginal Community Controlled Health Services
The first Aboriginal Community Controlled Health Service in Australia was established in Redfern in 1971 in response to concern about Aboriginal people’s access to mainstream health services, which were perceived as racist, discriminatory and expensive (where they existed at all)1. There are approximately 50 ACCHSs in NSW and while they vary considerably in size and scope, the underlying philosophy common to all is that of self-determination. Most operate as autonomous organisations but some are auspiced by other ACCHSs or Divisions of General Practice. Many ACCHSs provide outreach services to smaller surrounding communities. One of the strengths of ACCHSs is that their roots are in the community. As a result of this local knowledge they are in a position, not only to provide good individual health care, but also to undertake community development and to respond flexibly to local needs.
1 The Australian Medical Association has reported evidence of ongoing inherent discrimination in the Australian health system. It found that Aboriginal and Torres Strait Islanders do not benefit from mainstream health services to the same extent as other Australians because they either are located out of the reach of Aboriginal communities or the medical attention they receive is culturally intolerant and unwelcoming (Australian Medical Association, 2007).
There is good evidence that increased funding for the Aboriginal Community Controlled Health sector has had a positive impact on health outcomes (Dwyer, 2010). Additionally, “the greater number of problems managed per consultation in ACCHSs, compared with Indigenous patients in mainstream general practice, supports the assertion that ACCHSs fill an important role in the health system by providing care for their largely Indigenous patients with complex care needs” (Larkins, Geia and Panaretto, 2006, p2). There are many examples of community controlled health care leading to demonstrably better health outcomes. Studies published in the Medical Journal of Australia, for example, reported that patients attending Aboriginal Medical Services were more likely than patients attending mainstream general practices to get necessary treatments for risk factors such as high blood pressure, diabetes or cholesterol (Peiris at al, 2009) (Webster et al, 2009)2.
2 Findings overseas also report that transferring health care to community control is yielding results. Research in Canada, for example, has revealed striking evidence “that First Nations control of health care leads to better health” (Canadian Medical Association Journal, 2009, pE249).
3 The Practice

20 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
3.2 Regulatory Arrangements in NSW ACCHSsThe AH&MRC has 44 ACCHS Member Services and some additional Associate Members (March 2011). The Member Services are incorporated organisations under one of the following four regulatory bodies:
Table 1: Regulatory Arrangements in NSW ACCHSs (March 2011)
Regulatory Body Number of Member Services
Office of the Registrar of Indigenous Corporations (ORIC) under the Corporations (Aboriginal and Torres Strait Islander) (or CATSI) Act 2006
19
NSW Fair Trading through the NSW Associations Incorporation Act 2009
20
NSW Fair Trading through the NSW Co-operatives Act 1992 4
Australian Securities and Investments Commission (ASIC) as a public company limited by guarantee under the Federal Corporations Act 2001
1
3.3 ACCHSs Participating in the AH&MRC Corporate Governance Project
Five ACCHSs participated in the AH&MRC Corporate Governance Project in order to examine governance issues as they ‘play out’ in individual services. The services were selected as they are from different geographic localities, vary in scope and size and have different legal structures (auspiced and stand alone). During consultations with the CEOs and board members of the five services, a number of governance issues and challenges were discussed and many examples of good practice were showcased. The AH&MRC will continue to work with the services on their specific governance requirements but these
discussions are beyond the scope of this report.
The five services are:
i. Armajun Aboriginal Health Service (auspiced by Bulgarr Ngaru Medical Aboriginal Corporation)
The Armajun Aboriginal Health Service is an Aboriginal Community Controlled Health Service registered as an Incorporated Association with NSW Fair Trading. It provides culturally appropriate primary health care services to the Aboriginal communities in Inverell and surrounding areas. Armajun offers a range of primary care services and has 1.0 FTE GPs employed in the service as well as a number of visiting specialists and allied health providers.

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 21
Armajun has AGPAL accreditation. When Armajun AHS opened in September 2005, it did so with OATSIH funding directed through Armidale and District Aboriginal Medical Service. In November 2007 the auspicing of Armajun AHS was transferred to Bulgarr Ngaru Medical Aboriginal Corporation in Grafton (almost three hours drive from Inverell). The Armajun Executive Officer reports directly to the Bulgarr Ngaru Chief Executive Officer and all staff employed at Armajun are employees of Bulgarr Ngaru.
Bulgarr Ngaru and Armajun have a signed Memorandum of Understanding in which both Boards of Directors have agreed to focus on the broader strategic issues associated with governance rather than the day to day management activities of the organisation. Day to day matters are the responsibilities of the Bulgarr Ngaru CEO in consultation with the Armajun Executive Officer. The Armajun Board operates as an Advisory Committee to the Bulgarr Ngaru Board. Under this arrangement all issues regarding the operation or development of Armajun AHS requiring board deliberation are initially considered by the Armajun Board, which then makes recommendations to the Bulgarr Ngaru Board. The expectation under the auspicing arrangement is that Armajun AHS will move towards independence as a fully autonomous and independent legal entity under a staged process with Bulgarr Ngaru assisting the process through the development of the necessary operational, financial management and governance capacities in Armajun.
The auspicing model assumes that there is a move towards independence and hence the arrangement is short term. But the process can be slow as it can be hard for the auspiced service to demonstrate it is ready
for financial and legal independence when under auspice it is not required to manage its own finances etc. The CEO and senior staff are often the first to leave an organisation when administrative arrangements change. At Armajun the Executive Officer position had been vacant for over 12 months when the current EO took the job in February 2010. Administrative processes had consequently lapsed and new staff needed to be appointed (e.g. the practice manager). The transition process requires careful management to ensure that the auspiced service (board, staff and members) does not feel disempowered in the process. The local communities often still assume that the ACCHS board has more power that it does under auspice. There is potential for conflict between community expectations and what is realistic in terms of funding and capacity.
Bulgarr Ngaru has previous experience in auspicing other services and since July 2010 has also been auspicing the Casino Aboriginal Medical Service.
ii. Bullinah Aboriginal Health Service (previously auspiced by North Coast General Practice Network)
Bullinah Aboriginal Health Service is an Aboriginal Community Controlled Health Service that was initiated by the local Aboriginal community to deliver holistic and culturally appropriate health care to people within the Ballina and surrounding region. It is registered through the Office of the Registrar of Indigenous Corporations under the Corporations (Aboriginal and Torres Strait Islander) Act 2006.
OATSIH provided funds to the Northern Rivers General Practice Network (NRGPN) in 2006 for a scoping study and following this, funds

22 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
fortheservicein2007/2008.Theservicewas auspiced by NRGPN, which is located in Lismore about a half hour drive from Ballina. Bullinah AHS opened in March 2008 and achieved independence from the Division on 1st October 2010. It provides services to the Aboriginal communities in Ballina, Cabbage Tree Island, Evans Head, Wollongbar and Byron Bay and has AGPAL accreditation. While under auspice the Bullinah AHS Board acted in an advisory capacity to the NRGPN. The board comprised community elders who undertook governance training. The current CEO commenced in July 2010. The AH&MRC provided some assistance with policies and procedures.
As at March 2011 Bullinah AHS had the following staff: 5 Contracted Medical Officers (1.2 FTE); 1 FTE VR Registrar; 1 Medical Student (2 days a week); 2 Permanent Part timeR/Ns(1.4FTE);1PermanentParttime Aboriginal Health Worker (0.8 FTE); 1 FTE Permanent Medical Receptionist; 1 FTE Permanent Practice Manager; 1 Permanent Part time Counsellor (0.2 FTE); 1 FTE Permanent CEO; and other Visiting Contracted Specialists and Allied Health staff (Paediatrician, Child Psychologist, Podiatrist, Psychologist, Optometrist and Dietician). In addition Bullinah has recently been approved for Mothers and Babies Program Funding and the following staff will be employed in this: 1 ParttimeGP(0.1FTE);1PartTimeR/N(0.45FTE); 1Part time Medical Receptionist (0.3 FTE); and 1 Aboriginal Health Worker (0.6 FTE).
iii. Coomealla Aboriginal Health Corporation
Coomealla Aboriginal Health Corporation is an Aboriginal Community Controlled Health Service located in Dareton in western New South Wales. It is an independent organisation which provides a wide range of clinical and health promotion services to Aboriginal communities in the Wentworth Shire. The service has 1.5 FTE GPs. Other services offered include population health programs in the areas of child and maternal health, nutrition, immunisation, substance use, and sexual health. Coomealla was registered with the Office of the Registrar of Indigenous Corporations under the Corporations (Aboriginal and Torres Strait Islander) Act in 1992. The current CEO commenced in February 2006 and, with the board, has been able to expand the range of services offered. Coomealla has AGPAL accreditation.
iv. Illawarra Aboriginal Medical Service Corporation
Illawarra Aboriginal Medical Service Corporation (IAMS) was established in 1984 and has always been a stand-alone organisation. It is registered with the Office of the Registrar of Indigenous Corporations as a corporation under the Corporations (Aboriginal and Torres Strait Islander) Act. The service has 42 staff over two sites – Wollongong and Dapto – and draws its members from the coastal area bordered by the escarpment that stretches from Helensburg to Gerroa. Both sites have AGPAL accreditation and GP registrars as well as GPs. University of Wollongong medical students also undertake placements with the service. The organisation is working towards Quality Improvement Council accreditation. As well as medical and

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 23
dental services, the IAMS provides regular allied health clinics in diabetes management, podiatry, endocrinology, hearing, physiotherapy, and speech therapy. Public health, drug and alcohol, maternal health, child health, men’s health, sexual health and welfare programs are also provided. The current CEO has been a board member and also had an earlier period as CEO.
v. Tamworth Aboriginal Medical Service (auspiced by North West Slopes Division of General Practice)
Tamworth Aboriginal Medical Service (TAMS) is an Aboriginal Community Controlled Health Service registered as an Incorporated Association with NSW Fair Trading. It was established in 2005 with OATSIH funding provided through an auspicing arrangement with Pius X Aboriginal Corporation in Moree. In November 2007 the North West Slopes Division of General Practice (NWSDGP) took over auspicing TAMS. The close proximity of auspiced body and auspicer (in the same town) is recognised as a positive feature of the arrangement. TAMS offers a range of primary care services and has the equivalent of 1.7 FTE GPs employed in the service as well as a number of visiting specialists.
The TAMS Board acts as an advisory group (Tamworth Aboriginal Medical Service Incorporated or TAMS Inc) for the NWSDGP Board. The Division has one board director acting as the liaison between the two boards and he also attends meetings of TAMS Inc. The Division has always regarded the auspicing arrangement as temporary and has been working with TAMS to move to independence as soon as possible. The service has had four CEOs with the most recent starting mid 2010. The CEO prior to
that was employed in the Division and was seconded in an acting capacity to TAMS. TAMS will be moving to new and larger premises in 2011 adjacent to the NWSDGP.
TAMS Inc Board members have ‘portfolios’ and have recently developed a Tamworth Transition Action Plan to guide the move to independence. The TAMS CEO feels that they are reasonably close to independence. He found it useful to have had advice from the CEO of Bullinah Aboriginal Health Service. Like Armajan, the TAMS CEO expressed frustration with the “Catch 22” situation of needing to be able to demonstrate that it has the financial management capacity required of an autonomous service while all financial matters are currently managed by NWSDG. The Division has funding through to 30th June 2012 and is confident that TAMS will achieve independence prior to that. The last six months under auspice will inevitably be taken up with the nuts and bolts of the handover (transfer of staff, finances and so on). The TAMS Board is largely made up of directors employed in other positions who receive governance training through their full time jobs or as directors of other boards (e.g. the Aboriginal Lands Council). The TAMS Chairperson believes that prior governance training should be recognised and that it would be helpful if the AH&MRC could organise training which recognised this.

24 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
3.4 Changing Landscape and Policy Environment
The environment in which ACCHSs operate is complex. The political landscape is rapidly changing and there is increasing competition to access funding for the provision of Aboriginal health services. Governments have moved towards contestability and tendering of services, outcomes based funding and quality assurance (Effective Change Executive Summary 2007 – p ii).
Recent major changes impacting on the Aboriginal Community Controlled Health sector include the following:
• The Council of Australian Governments (COAG) National Partnership Agreement on Closing the Gap in Indigenous Health Outcomes. This has committed $1.57 million over four years to improve Indigenous health. New financial incentives (e.g. the expanded Practice Incentive Program) and funding for new positions (e.g. Indigenous Outreach Workers) are encouraging mainstream general practices and Divisions of General Practice to provide more targeted services to Aboriginal patients. The programs are designed “to encourage better care, particularly from mainstream general practices, of Aboriginal people with chronic disease to help ‘close the gap’ by reducing Aboriginal health disparity” (Couzos and Delaney Thiele, 2009).
• The Federal Government’s National Health and Hospitals Reform (NHHR). The reforms, which were developed under the Rudd Labor Government, were accepted by COAG (with the exception of Western Australia) in April 2010 and initially focus on improving hospital services. At the COAG
meeting in February 2011 Prime Minister Gillard won agreement from COAG for a 50:50 Commonwealth:State funding split and in-principle agreement from the premiers to her new (single pool) national health funding model.
• Local Hospital Networks. As part of the National Health and Hospitals Reform process Local Hospital Networks are being established across Australia. In NSW eighteen new Local Health Districts were established on January 1, 2011, replacing eight Area Health Services.
• Medicare Locals (Primary Health Care Organisations). Medicare Locals will replace Divisions of General Practice. The first Medicare Locals (fifteen nationally) will be established in July 2011 with a further 15 in January 2011 and the remainder commencing in mid 2012. Medicare Locals will identify and respond to local health needs and expand the functions and activities currently undertaken by Divisions.
• GP Super Clinics. Over sixty clinics are being funded by the Federal Government to bring together general practitioners, nurses, visiting medical specialists, allied health and other health care professionals to provide health care tailored to the needs and priorities of the local community “including the needs of Aboriginal and Torres Strait Islander peoples” (http://www.health.gov.au/internet/main/publishing.nsf/Content/pacd-gpsuperclinic-about#intro accessed 11th January 2011).
How the health reforms will impact on the ACCH sector in NSW remains to be seen. Overall funding for Aboriginal health has increased but so too have the number of

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 25
organisations competing for these funds. Organisational structures in some ACCHSs haven’t necessarily kept up with the requirements of the increasingly competitive environment.
3.5 Tensions, Practice and a Proviso
Discussions with representatives of the five participating ACCHSs and conversations with other CEOs and stakeholders have led to a number of observations about corporate governance practices in NSW ACCHSs. In summary these observations can be divided into two major themes: firstly, that there are inherent tensions between mainstream concepts of governance and Aboriginal culture; and secondly that in general governance practice in ACCHSs supports the theory as espoused in Part 2 of this report.
Tensions between mainstream concepts of governance and Aboriginal culture3
Aboriginal values may include obligations based on kinship relationships, an importance on consensus decision making and putting family needs before business goals (ORIC Research Paper, 2010, p 7). ACCHSs board directors have the challenging role of balancing cultural and community expectations with their legal and fiscal obligations. Board members may see the imposition of ‘white’ governance values and compliance requirements as foreign and unwanted and older members may feel the need to abandon their own values and beliefs about leadership and traditional governance in
3 It is noted that two members of the AH&MRC Corporate Governance Project Reference Group believe that the tensions between the community controlled model and the requirements of running ACCHSs as businesses in a rapidly changing and increasingly competitive landscape will become irreconcilable.
order to comply with funding agreements. The services that work best are those that manage the potential conflicts between the two ‘belief systems’ and those that have boards that are not too involved in the day to day activities of their services and yet at the same time are well equipped to effectively monitor their organisations.
Effective governance in ACCHSs acknowledges the differences in the ‘white fella’ governance and the traditional or historical values that have underpinned the establishment of the services, and works through these differences. Getting this right means that the boards can ‘govern’ and have their say in the community focused operations and decision making that impacts upon their communities (ensuring their communities have services, setting the strategic directions, developing the shared vision and so on) while the ‘business’ side of the services and day to day operations can be managed and run by the CEOs and staff who have the necessary training and skills to meet the corporate governance requirements of the mainstream funders and government. “This kind of model is one of ‘functionality’. It recognises the differences in the role and functions of the boards compared with the role and functions of the operating side of the services. It can free community elders up from the pressures and complex demands of the newer imposed governance requirements that they may often not believe in, while at the same time utilises the depth of knowledge, wisdom and experience embodied in the community elders” (Wayne Munster, email 22 November 2010). This model will also work for younger community members who may otherwise be put off going onto boards because of the potential tensions between ‘white’ governance

26 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
requirements and traditional Aboriginal values and culture.
The practice reflects the theory
The practices observed during the AH&MRC Corporate Governance Project are consistent with the literature on corporate governance in Aboriginal Community Controlled Services (discussed in Part 2 of this report). Services that have the most effective corporate governance arrangements are those with boards:
• that are demographically representative of their community (or communities) (i.e. have elders, youth and appropriate gender representation) and have diversity in board membership;
• where community and culture remain the primary drivers but are complemented by other relevant skill sets (expertise in law, health, IT, HR, finance etc.) i.e. have a good skills mix that reflects the needs of the organisation;
• that have strong links back to the community and mechanisms to engage and communicate with the community;
• that have strategies in place to ensure that the best possible members stand for board election (e.g. hold Pre AGM Workshops; have consistent and clear mechanisms in place for board elections; publicise the date of the AGM well in advance and don’t change the date);
• that have two or three year staggered board terms to facilitate a balance between continuity and board renewal;
• that invest in training (to ensure, among other things, that the boards know the questions to ask so that they can fully understand the business and therefore make informed decisions);
• that understand their roles and responsibilities as board members and have these clearly defined;
• that have mechanisms in place to monitor performance and ensure internal accountability;
• that have strong CEOs who are effective communicators and provide information to the board clearly and concisely in a number of different ways including graphic representation of financial information;
• that value, promote and respect leadership qualities in the CEO and the board office bearers (where leaders are visionary, consistent, transparent, accountable and have autonomy within the role delineation guidelines);
• that have a long term vision for where they want the organisation to go which is shared by management and the community;
• that have meeting and clear decision making processes in place; and
• that are engaged in strategic planning and monitoring activities and link these into board meeting processes and planning cycles.
The major challenges for good governance in community controlled organisations include:
• running organisations that value community and culture while being efficient, effective, accountable and successful businesses;

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 27
• supporting boards to manage the expectations of their communities and to balance their cultural values with their legal and fiscal obligations in a business setting;
• establishing and maintaining clear delineation between the role of the board and the role of the CEO and management so the board does the ‘governing’ and management does the ‘operating’;
• increasing the pool of community members interested in nominating for boards and equipping these members with the requisite skills and understanding of what board membership involves;
• moving board member terms from annual appointments to two or three year terms where this hasn’t already occurred;
• developing strategies to bring specialist financial, legal, IT, IR etc. skills onto the boards where they aren’t currently available by co-opting ex-officio members onto the boards;
• encouraging young people onto boards and mentoring these people as future leaders;
• developing strategies to support CEOs and senior management (staff development, peer support);
• introducing change management skills in board members to equip them to respond to the rapidly changing policy environment and the need to oversee what are now sometimes multi million dollar businesses.
The findings from the consultations also support the literature that ‘no one size fits all’. While there is a body of agreed principles of good governance, the effective realisation (or implementation) of these principles will vary
from service to service in response to their different arrangements and circumstances. Community control and the tensions inherent in the model add complexities to standard governance theories. Best practice does operate in ACCHSs and where it works really well it has evolved from within the service and community to suit the particular circumstances of the service. It has not been imposed upon the organisation. As one ACCHS CEO put it “you can take a horse to water but you can’t make it drink”. Careful planning around introducing best corporate governance practice is critical and all ACCHS stakeholders (the board and management, staff and community) should be involved in the process. This is best linked to the planning cycle of the organisation (i.e. developing the shared vision, the strategic planning, the business and financial planning, AGM planning and so on). Orange Aboriginal Health Service does this well, as does Coomealla. Orange developed a five-year strategic plan with input from the board, the staff and the community. It is very clear and enables the CEO to make management decisions based on the shared strategic directions for the service. The board sets the direction, the community members are involved and consulted and the CEO can make his management decisions with the confidence of the board and the community without always having to go back to them. The Coomealla AHC CEO suggests a six year planning cycle which is reviewed every three years to coincide with three yearly board appointments.
Good corporate governance requires a constitution that supports a functional board. The AH&MRC Policy and Legal Officer has worked with many NSW ACCHSs to introduce constitutional changes, including moving

28 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
away from annual board appointments and appointing ex-officio directors when this is appropriate. Good corporate governance also requires strong leadership: “leadership, leadership and leadership” as Professor Mick Dodson stated “are the three key elements of good governance” (Reconciliation Australia, 2007, p 51). There are many examples of good leadership in NSW ACCHSs with CEOs and board members working to achieve positive health outcomes within the context of good governance frameworks. Professor Ian Anderson refers to the governance framework as the legal architecture of the organisation (Ian Anderson at the Support Systems National Roundtable, Melbourne, 20th June 2010).
Postscript Proviso – A final comment on the theory
What is not fully explored in the literature and is absolutely contextual is the issue of ‘relationships’ and how these are managed, particularly in the current environment that requires services to adapt historical ways of operating to meet the new challenges. Even with best practice, with the clear separation of the role and functions of the board and management, with fiscal and legal accountability mechanisms in place and so on, risks remain around managing relationships in the organisation (managing kinship relationships and managing relationships between the board and CEO, within the board, within the communities, between the CEO and the communities etc.). Unresolved relationship issues might lead, for example, to the resignation of a CEO who has been driving the good governance process or key board members resigning or not being re-elected.
29Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
The AH&MRC Corporate Governance Project has highlighted many examples of good governance practice in NSW ACCHSs. It has also revealed that many ACCHSs would like the AH&MRC to be more active in supporting governance capacity across the ACCH sector. The following recommendations, if accepted, are directed at the AH&MRC and the funding bodies with the aim of focussing and enhancing corporate governance in the NSW ACCH sector.
4.1 Framework for Good Governance for NSW ACCHSs
Fully effective organisations have processes in place to continuously improve corporate governance systems. The processes involve identifying improvements, implementing improvements, evaluating the effect of improvements, and going back to identify more improvements (OATSIH Accreditation Manual, 2010, p12).
To participate in continuous quality improvement organisations need to have a shared view about what constitutes good governance practice and a standard towards which to work. A useful governance framework for NSW ACCHSs is an adaptation of a governance framework developed by Langlands (2004)4. The framework has been adapted by the AH&MRC Corporate Governance Project and is provided in
4 Pope (2007) has developed the PHO Governance Self Assessment Tool for Health Care Aotaeroa and Te Wana which is an alternate model which could be adapted for NSW ACCHSs.
Table 2. It comprises six elements (guiding principles) of good governance, each of which has three or four supporting principles. It has been developed to assist board directors to not only apply principles of good governance to their services but also to assess the strengths and weaknesses of their current governance practices and to improve them, where necessary. The principles, when taken together, form a ‘standard’ towards which ACCHSs can strive. The questions that ACCHSs would ask themselves to test how far they live up to the standard, and to develop actions plans for making any necessary improvements are contained in the framework. It is designed to be sufficiently flexible to reflect the various capacities and circumstances of local services. It may be, for example, that a particular ACCHS board will prefer to reduce the number of questions and this can be done without compromising the integrity of the standard. Other boards may wish to ask all the questions.
4 Recommendations

30 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Table 2: Framework for Good Governance for ACCHSs
Criteria for Good Governance
Application to ACCHSs
1. Good governance means focusing on the organisation’s purpose and on outcomes for the communities
• AretheACCHSobjectivesclear?Dowealwayshavetheseatthefrontofourmindswhenweareplanningortakingdecisions?Howwellarewedoinginachievingourintendedoutcomes?
• Aretheservicesofahighquality?Howdowedecidewhatishighquality?Dowehaveregularinformationonusers’viewsofquality?
• Arethecommunitiesreceivingtheservicestheyneed?Howdowedecidewhatservicesareneeded?
2. Good governance means performing effectively in clearly defined functions and roles
• AretheACCHS’sboardfunctionsclear?• Aretherolesandresponsibilitiesoftheboardandexecutiveclear?Doweall
knowwhatwearesupposedtobedoing?• Aretherelationshipsbetweentheboardandtheexecutive/theboardandthe
communityeffective?Arethereproblematicrelationships?• Isorganisationalperformancesatisfactory?
3. Good governance means promoting the values for the whole organisation and demonstrating the values of good governance through behaviour
• Aretheorganisationalvaluesknownandpublicised?Aretheyputintopractice?• Doindividualboardmembersandexecutivesbehaveinwaysthatupholdand
exemplifygoodgovernance?Aretherewaysinwhichourbehaviour,collectivelyandindividually,couldweakentheorganisation’saimsandvalues?
• Whatarethevaluesweexpectthestafftodemonstrateintheirbehaviourandactions?
4. Good governance means having informed, transparent decision making processes and managing associated risk
• Howwelldoourmeetingswork?Whatcouldwedotomakethemmoreproductiveanddoourbusinessmoreeffectively?
• Isorganisationaldecisionmakingtransparentandeffective?• Istheinformationwereceiverobustandobjective?Howcouldtheinformation
wereceivebeimprovedtohelpimproveourdecisionmaking?Dowetakeprofessional advice to inform and support our decision making when it is sensibleandappropriatetodoso?
• Areriskmanagementstrategiesandsystemsinplaceandeffective?
5. Good governance means developing the capacity and capability of the governing body to be effective
• Doboardmembersandexecutiveshaveaccesstotherequisiteskills,knowledgeandexperiencetoperformwell?Howwelldoesourrecruitmentprocess identify people with the necessary skills and reach people who representthecommunityinallitsaspects(i.e.youth,eldersetc.)?
• Areprocessesinplacetodevelopcapacitytogoverneffectively?Doweputintopracticeplansforimprovingourperformanceasaboard?
• Whatisourapproachtofindingabalancebetweencontinuityandrenewalintheboard?
6. Good governance means engaging stakeholders and making accountability real
• Areservicestakeholderseffectivelyengaged?• Areformalandinformalaccountabilityarrangementseffective?• Isthereaplannedandorganisedapproachtoaccountabilitywiththe
community?• Isthereaplannedandorganisedapproachtoaccountabilitywithstaff?
Adapted from Langlands (2004) by the AH&MRC Corporate Governance Project (2011)

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 31
As discussed in 3.3 of the report, five ACCHSs agreed to participate in the AH&MRC Corporate Governance Project in order to examine governance issues as they ‘play out’ in individual services. Consultations with the services have informed the project. The AH&MRC is currently working with these services on their specific governance requirements and developing ‘Governance Action Plans’ for the services. This work is not documented in this report but does provide an opportunity to trial the governance framework to test its usefulness and to fine tune it to suit individual board requirements.
Recommendation 1:
It is recommended that the Framework for Good Governance for ACCHSs (Table 2) be trialled by the AH&MRC as a corporate governance ‘standard’ with the five ACCHSs participating in the AH&MRC Corporate Governance Project.
4.2 Training in Corporate Governance and Strategic Planning
The OATSIH Risk Assessment Protocol requires that more than 50% of current board members have completed governance training in the last 12 months5 although OATSIH does not specifically fund ACCHSs to do so. Good models of community controlled corporate governance training exist including that offered by the NSW Land Council and ORIC, which offers training free of charge. (Nineteen of 44 Member Services are incorporated under ORIC6). CEOs and board members have, however, stated that they prefer training
5 Or requires that resources for governance training for board members have been allocated and training has been scheduled.
6 As at March 2011
that is specifically tailored to the community controlled health sector and to their services’ particular issues. Training needs to reflect the corporate regulatory arrangements covering the services, whether this be under NSW Fair Trading, ORIC or ASIC. The more successful training programs are those that are structured around case studies and practical examples that are relevant to the ACCH sector.
ACCHSs currently organise governance training through a variety of providers including the Aboriginal Health College. Some ACCHSs have developed their own very successful training programs with experienced consultants who work in the sector. A number of CEOs and board members, however, expressed the wish that the AH&MRC would organise board governance training rather than each service organising its own. They also expressed the view that there is value in bringing together board members from different ACCHSs to share ideas, knowledge, stories and experiences. There may be economies of scale in the AH&MRC organising high quality governance training on behalf of its Member Services. There is also value in offering governance training to new directors early in their board terms to introduce governance concepts as they apply to the ACCH sector.
Recommendation 2:
It is recommended that the AH&MRC seeks funding to provide an ‘Introduction to Corporate Governance Board Training’ program that would be offered to all new ACCHS board members on a state-wide basis at the beginning of each calendar year (after the school holidays). CEOs and serving board members could be invited to participate

32 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
as well. A Board Induction Kit would be provided to assist with and complement the introductory board training. The training could be organised through the Aboriginal Health College.
In addition to the introductory governance training there is merit in offering governance training that is a step up from this level and which recognises prior learning and experience. It could be offered as Certificate IV in Business (Governance) training and could be offered regionally, bringing together different ACCHSs, some of which will have different governance capacities. This would assist in capacity building by exposing board members to what is happening in other services as well as honouring the existing regional groups. Courses designed for board office bearers could also be offered.
Recommendation 3:
It is recommended that the AH&MRC seeks funding to provide governance training to ACCHSs on a regional level that is tailored to suit the ACCHSs involved and is pitched ‘higher’ than an ‘Introduction to Corporate Governance’ program (in recognition of board experience and prior learning). The training could lead to Certificate IV in Business (Governance) qualifications. The training could be organised through the Aboriginal Health College.
ACCHSs with the most effective corporate governance arrangements are those with a long term vision for where they want the organisation to go which is shared by management and the community. Strategic planning is an organisation’s process of defining its strategy, or direction (for realising its vision), and making decisions about allocating its resources to pursue this strategy,
including its capital and people. The process also helps to clarify the different roles and responsibilities of boards and management.
Recommendation 4:
It is recommended that the AH&MRC seeks funding to provide training in strategic planning for ACCHS boards which could be offered regionally and include discussions about contextual issues impacting on ACCHSs such as the Council of Australian Governments (COAG) initiatives e.g. Closing the Gap and National Health and Hospitals Reform.
4.3 AH&MRC Governance Symposium
CEOs and board chairs consulted during this project wanted the opportunity to meet to show case examples of good governance practice, to discuss issues of concern around governance including the big picture strategic issues that impact on governance (COAG, health reform etc.) and opportunities for professional development sessions (change management, leadership etc.). CEOs and board chairs could meet separately in pre or post workshop meetings.
Recommendation 5:
It is recommended that the AH&MRC holds a Corporate Governance Symposium in 2011 for ACCHS CEOs and board chairs. The program would include sessions on the principles of good governance in the ACCH sector, discussions on the strategic issues that impact on good governance and opportunities to showcase examples of good governance practices in ACCHSs. CEOs and board chairs could meet separately in pre or post workshop meetings.

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 33
4.4 Board MembershipGenerally boards that work most cohesively and effectively are those that attract board members who are representative of the community and with a skills mix appropriate to the needs of the service.
ACCHS board members currently include elders, community leaders and people employed in a range of occupations including public servants and staff of other Aboriginal community controlled services. They bring a range of expertise and experiences to their boards. Their educational levels vary from basic literacy and numeracy skills to professional qualifications and doctorates. ACCHS board members are not paid for being on the boards (other than being reimbursed for any out of pocket expenses).
CEOs utilise a range of strategies to attract good board members. Some (e.g. Yerin Aboriginal Health Service) encourage members with experience in education, housing or health to stand for the board and report that this has contributed to better functioning boards. Other CEOs (e.g. Wellington Aboriginal Corporation Health) hold pre AGM workshops where the roles and responsibilities of board directors are discussed, funding bodies are invited to attend and those interested in standing for the board participate in an ‘Expression of Interest’ process. Galambila Aboriginal Health Service identified the skills mix it wanted on the board and then actively encouraged community members with those skills to apply for positions on the board.
In smaller communities, however, it is not always easy to include directors with the requisite specialist skills, (that are increasingly important as ACCHSs meet their business
commitments) such as financial, legal, IT andindustrialrelations/HRexpertiseontheirboards. Individuals with experience working in the health system also make valuable board members. People with these requisite skills and experiences can be co-opted onto boards as ex-officio non-voting members. These arrangements can work well, as evidenced in Orange Aboriginal Health Service. Some CEOs stated that they actively encourage young people to participate in order to ‘refresh’ the potential pool of board members and to bring new skills and ideas onto the board to complement the skills and experiences of the older members. For example, Walgett Aboriginal Medical Service has a designated youth position on its board and Durri Aboriginal Medical Service holds specific functions to encourage their younger members to be involved with the service.
Recommendation 6:
It is recommended that the AH&MRC, at its Governance Symposium (Recommendation 5), showcases the strategies that ACCHSs employ, consistent with the principles of good governance, to ensure that their boards are demographically representative of their communities and balance community and cultural drivers with specialist skill sets. Such strategies include proactively encouraging young people onto boards; holding pre AGM workshops to increase the level of awareness of the roles and responsibilities of directors; and co-opting experts onto boards as ex-officio directors where those skill sets aren’t available on the board.
Most ACCHSs are now moving away from annual board appointments and appointing directors for two or three years (or a combination thereof) on a rotating basis. More

34 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
than one board member commented that under annual terms there were times when his board members “got up to scratch” only to be replaced by those without experience, or as one CEO stated “you have a five year strategic plan but with board members changing annually there’s no ownership”. A balance is required between having continuity on the boards and renewal. Staggered terms allow for this.
Recommendation 7:
It is recommended that, consistent with the principles of good governance, the AH&MRC works with those ACCHSs that have not yet moved away from annual board appointments to enable the services to introduce constitutional changes that will give board directors terms of either two or three years (or a combination thereof) with the directors appointed on a staggered basis.
4.5 CEO Meetings and SupportMany organisations provide regular opportunities for their senior managers (or CEOs) to get together to share information and ideas and to discuss matters of concern (e.g. in the guise of ‘senior officers meetings’). There are currently no state-wide CEOs meetings and few formalised professional development opportunities for ACCHS CEOs and middle managers. The AH&MRC Workforce Initiatives and Programs Officer (WIPO) is currently working with ACCHS CEOs to develop opportunities for CEO training, networking and peer support, including a CEOs workshop. The workshop could, for example, include discussion around CEO support mechanisms and mentoring; CEO appraisal processes; ideas or suggestions around where to obtain advice for operational issues and tasks including planning, HR etc.
(Darren Ah See, CEO, Wellington Aboriginal Health Corporation, email 8th December 2010).
Recommendation 8:
It is recommended that the AH&MRC Workforce Initiatives and Programs Officer (WIPO) be supported by the AH&MRC in (i) working with ACCHS CEOs to develop CEO training, networking and peer support opportunities; (ii) facilitating annual CEO workshops; and (iii) extending the training and development programs to middle managers in the future.
4.6 AH&MRC Governance Support Team
Many stakeholders consulted during the AH&MRC Corporate Governance Project wanted the AH&MRC to be more actively engaged in assisting ACCHSs with corporate governance. The AH&MRC provides support which includes legal and administrative advice as well as how to best manage risk in certain circumstances, but it does not provide corporate governance support as a matter of course. It is not funded to do so and any assistance it does provide is funded through existing resources or, at times, on a fee for service basis. The stakeholders consulted saw value in extending and formalising the support they receive from the AH&MRC by establishing a governance team in the AH&MRC. They felt that this would add value to the existing governance activities in the ACCHS sector and would also facilitate sharing and promoting a range of good governance practices between services in a systematic and cohesive fashion. The NACCHO Governance Scoping Study Report (February 2011) has also recommended that eachState/TerritoryAffiliatehasagovernance

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 35
support unit for its Member Services to provide “a consistent point of contact ... (to offer) within the sector specialist expertise in governance ... and a co-ordinated approach”. NACCHO noted that this function is not resourced (or adequately and sustainably resourced) at present (NACCHO, 2011, p 9).
A Governance Support Team in the AH&MRC would support all Member Services including those in transition to independence and the more vulnerable services (vulnerabilities are generally the result of poor governance practice or poor management – ORIC Research Paper, 2010, p 6). Consideration would need to be given to the development of a communication protocol between the AH&MRC and Member Services that would enable the AH&MRC to be involved with an ACCHS while protecting the principles of autonomy and self determination of the organisation. Consideration would also need to be given to whether the team provides ‘front end’ support only or whether it is also staffed to provide ‘back end’ governance support (assisting organisations struggling on the brink of, or already under administration). The scope and range of services provided would depend on the availability of funding and/orestimatedrevenue.(Servicescouldbe offered on a fee for service basis and new start up funding could also be sought).
Responsibilities could include providing:
• governance workshops for CEOs and board members (as per Recommendation 5) ;
• general advice on good governance principles and practice;
• information and advice regarding the impact of the big picture strategic issues and how they impact on governance;
• assisting with or facilitating strategic planning;
• governance training and board support that is tailored to the ACCHS context, i.e. training that includes the standard issues around separation of powers, financial accountability and so on but which also addresses the contextual issues arising from the tensions between community control and ‘white fella’ corporate law or the ‘relationship’ issues discussed earlier in the report (Recommendations 2 and 3);
• ‘one stop shop’ and clearing house function for governance advice and for information on resources with links provided on the AH&MRC website (Recommendation 10). There are useful resources in the public domain but the ACCHSs are not always aware that these resources exist;
• templates for employment contracts, position statements, board financial statements, policies and procedures and so on;
• advice on administrative issues related to OH&Smatters,HR/IRrequirementsetc.;
• CEO relief – ACCHS CEOs face huge challenges and work incredibly hard. Some CEOs felt that they are not able to take the leave owing to them because of the pressures of work. This in itself becomes a risk to the organisation. Some CEOs have said that because of the flat management structures of their services there is not always someone who can step up to the acting CEO role. There are ‘elder statesmen and women’ among the ACCHS CEOs, a couple of whom have expressed interest in helping other services on a secondment or fee for service basis. A ‘floating

36 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
CEO’ position could be included in the Governance Support Team;
• assistance with constitutional and organisational change in ACCHSs;
• assistance with managing and mediating conflict.
Recommendation 9:
It is recommended that the AH&MRC considers the feasibility of establishing a Governance Support Team to assist and promote governance capacity in the NSW ACCHS sector. Consideration would need to be given to the development of a communication protocol between the AH&MRC and Member Services that would enable the AH&MRC to be involved with an ACCHS while protecting the principles of autonomy and self determination of the service.
4.7 Corporate Governance Resources for ACCHSs
While it would be possible to drown under the weight of the articles published on corporate governance most refer to the for profit sector. There is, however, a body of published and unpublished articles on governance in the Indigenous community controlled sector, although many of these are academic articles rather than practical hands-on resources for ACCHSs. Some useful hands-on resources for ACCHSs are as follows:
• Reconciliation Australia – Indigenous Governance Toolkit (2010)
The Indigenous Governance Toolkit is available on line at http://www.reconciliation.org.au/governance/home. It is a comprehensive resource introducing Indigenous community governance concepts, examples of good
practice, signs of problems and diagnostic checklists. It builds upon Reconciliation Australia’s workshops in the field, the findings from the Indigenous Community Governance Research Project and analysis of the Indigenous Governance Award applications.
• Office of the Registrar of Indigenous Corporations – Healthy Corporation Checklist (2010)
This 21 page checklist was released in June 2010 to assist organisations registered with ORIC to keep track of their compliance requirements. It refers to membership matters, AGM and general meeting issues, directors’ meetings, appointments and removal of directors, roles and responsibilities of directors and officers, financial management and administration and ethical issues. It is available on line at http://www.oric.gov.au
• NSW Rural Doctors Network & AH&MRC updated Administration Manual for ACCHSs in Rural NSW (2010)
The manual, updated in 2010, is designed to enable ACCHSs to develop or revise their policies and procedures and to assist those services moving through the accreditation process. It includes accreditation specific copyrightmaterialprovidedbyQIP/AGPALaswell as materials specific to Aboriginal Medical Services. The original 2007 version was piloted by five ACCHSs (both urban and rural) and their feedback was incorporated into the final 2010 version. It is available at http://www.nswrdn.com.au under GP Resources and Support.
• Aboriginal Health College
The Aboriginal Health College offers the Certificate IV in Business (Governance) to ACCHSs. It is based upon the ORIC Two

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 37
Worlds model but customised for the specific AMS context. Contact the AHC on phone: 02 9019 0730 or email: [email protected].
• OATSIH Risk Assessment Protocol
Whilst designed for OATSIH to ensure that processes and procedures are in place within the governance structures and systems of an ACCHS to appropriately manage key risks, this resource can also be used as a self assessment tool by organisations.
• Our Community Best Practice Principles/Guidelines
The Boards, Committees and Governance Centre of Our Community provides governance training (up to and including Cert
IV in Business Governance) and resources to the community sector. Available at http://www.ourcomunity.com.au
• NCOSS Management Support Unit
Q&A on the Associations Incorporation Act 2009 as well as the Information Sheet on Conflict of Interest is available at http://www.ncoss.org.au/projects/msu/downloads/resources/
Recommendation 10:
It is recommended that the AH&MRC include a list of useful governance resources on its website and that the website be updated regularly to ensure currency of the materials.
Flowchart 1: AH&MRC Corporate Governance Recommendations
Recommendation 1
Trial ACCHS Framework for Good Governance with 5
ACCHSs as AH&MRC corporate governance
‘standard’
Recommendation 2
Introductory level governance training for all ACCHS Board members. Development of
Board Induction Kit
Recommendation 3
Regionally based higher level governance training tailored
to services
Recommendation 5
AH&MRC host a Corporate Governance Symposium in 2011
for CEOs and Chairpersons
Recommendation 8
AH&MRC WIPO role be supported to include
development of CEO training and peer support opportunities
Recommendation 10
AH&MRC to provide governance resources on
its website
Recommendation 7
Constitutional changes to ACCHSs for 2 or 3 year staggered board
appointments
Recommendation 6
Showcase best practice including strategies aimed at ensuring demographic
representation skills mix on ACCHS Boards
Recommendation 9Establish Governance
Support Team
Recommendation 4
Regionally based strategic planning training

38 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Aboriginal Health and Medical Research Council of NSW. Collation of the Documented Achievements of Aboriginal Community Controlled Health Services in NSW (unpublished). August 2009
Aboriginal Health Council of South Australia. Comments on the Discussion Paper Towards a National Primary Health Care Strategy. February 2009
Aboriginal Health Council of Western Australia. Management Framework: A Guide to Improve Organisational Governance. 2006
Armstrong L. Financial Management and Business Systems: The Backbone of an Effectively Resourced Capacity for Governance. Paper delivered at the Building Effective Indigenous Governance Conference, Jabiru Northern Territory. November 2003
Bauman T and Smyth D. Indigenous Partnerships in Protected Area Management in Australia: Three Case Studies. Australian Institute of Aboriginal and Torres Strait Islander Studies and Australian Collaboration. Canberra. 2007
Burdon Torzillo and Associates. Empower Good Governance for Local Aboriginal Land Councils. Governance Kit developed for the NSW Aboriginal Land Council. January 2008
Canadian Medical Association Journal. 2009; 181(11), pE249
Centre for Aboriginal Economic Policy Research and Reconciliation Australia. Final Report: Indigenous Community Governance Project. CAEPR, Canberra. 2008
Cooperative Research Centre for Aboriginal Health. Support Systems for Indigenous Primary Health Care Services Project. http://www.crcah.org.au/research/support_systems_phc.html (accessed 4th May 2010)
Couzos Sophie and Delaney Thiele Dea. Closing the Gap Depends on ACCHSs. Medical Journal of Australia. 2009; 190 (10)
Dalton Jason. Corporate Governance Directors Duties. Notes provided for AH&MRC of NSW Corporate Governance Training held in Sydney from 19th – 21st February 2008
Department of Health and Ageing. Aboriginal and Torres Strait Islander Health Performance Framework. Commonwealth of Australia. Canberra. 2008
Department of Health and Ageing. Medicare Locals – Discussion Paper on Governance and Functions. 2010. http://www.yourhealth.gov.au (accessed 30th October 2010)
Dodson M and Smith DE. Governance for Sustainable Development: Strategic Issues and Principles for Indigenous Australian Communities. Centre for Aboriginal Economic Policy Research Discussion Paper No. 250. 2003
Dwyer Judith. Why Constitutional Recognition for Indigenous Australians is a Health Issue. Crikey. 22 November 2010. http://www.crikey.com (accessed 23rd November 2010)
Dwyer Judith, Shannon Cindy and Godwin Shirley. Learning from Action: Management of Aboriginal and Torres Strait Islander Health Services. Cooperative Research Centre for Aboriginal Health. Darwin. 2007
References

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 39
Dwyer Judith, Silburn Kate and Wilson Gai. National Strategies for Improving Indigenous Health and Health Care. Aboriginal and Torres Strait Islander Primary Health Care Review: Consultant Report No. 1. Commonwealth of Australia. Canberra. 2004
Edwards M and Clough R. Corporate Governance and Performance: An Exploration of the Connection in a Public Sector Context. Issues Series Paper No. 1. University of Canberra. 2005
Effective Change Pty Ltd. Positioning Aboriginal Services for the Future. April 2007. http://www.health.vic.gov.au/__data/assets/pdf_file/0005/270986/posfuturereport.pdf (accessed 23rd August 2010)
Governance and Business Improvement Conference Proceedings. Queensland Aboriginal and Islander Health Council. 2007 http://www.qaihc.com.au/uploads/Governance%20and%20Business%20Improvement%20Conference%20Report.pdf (accessed 23rd August 2010)
Griew Robert, Tilton Edward, Cox Nick, Thomas David. The Link Between Primary Health Care and Health Outcomes for Aboriginal and Torres Strait Islander Australians. A Report for the Office of Aboriginal and Torres Strait Islander Health, Department of Health and Ageing. Canberra. June 2008
Hunt Janet. Capacity Building for Indigenous Governance: International Development Experience of Capacity Development: ImplicationsforIndigenousAustralia?Centrefor Aboriginal Economic Policy Research. December 2005
Hunt Janet and Garling Stephanie (Editors). Community Governance Research Update No. 6, Indigenous Community Governance Project. Australian National University. Canberra. September 2007. http://www.anu.edu.au/caepr-old/Projects (accessed 11th May 2010)
Hunt Janet and Garling Stephanie (Editors). Community Governance Research Update No. 5, Indigenous Community Governance Project. Australian National University. Canberra. July 2007. http://www.anu.edu.au/caepr-old/Projects (accessed 11th May 2010)
Hunt Janet and Garling Stephanie (Editors). Community Governance Research Update No. 4, Indigenous Community Governance Project. Australian National University. Canberra. March 2007. http://www.anu.edu.au/caepr-old/Projects (accessed 11th May 2010)
Hunt Janet and Garling Stephanie (Editors). Community Governance Research Update No. 3, Indigenous Community Governance Project. Australian National University. Canberra. October 2006. http://www.anu.edu.au/caepr-old/Projects (accessed 11th May 2010)
Hunt Janet and May Katherine (Editors). Community Governance Research Update No. 7, Indigenous Community Governance Project. Australian National University. Canberra. October 2008. http://www.anu.edu.au/caepr-old/Projects (accessed 11th May 2010)
Hunt J and Smith D. Indigenous Community Governance Project: Year Two Research Findings. Centre for Aboriginal Economic Policy Research Working Paper No. 36. Australian National University. Canberra. April 2007

40 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Hunt J and Smith D. Building Indigenous Community Governance in Australia. Preliminary Research Findings. Centre for Aboriginal Economic Policy Research Working Paper No. 31. Australian National University. Canberra. 2006
Hunt J and Smith D. Ten Key Messages from the Preliminary Findings of the Indigenous Community Governance Project, 2005. Centre for Aboriginal Economic Policy Research. Australian National University. Canberra. 2005
Hunt Janet, Smith Diane, Garling Stephanie and Sanders Will (Editors). Contested Governance – Culture, Power and Institutions in Indigenous Australia. Centre for Aboriginal Economic Policy Research Monogram No. 29. Australian National University. Canberra. 2008
Indigenous Community Governance Project http://www.anu.edu.au/caepr-old/ICGP_history.php (accessed 4th May 2010)http://www.anu.edu.au/caepr-old/ICGP_concepts.php (accessed 4th May 2010)http://www.anu.edu.au/caepr-old/ICGP_research_aims.php (accessed 4th May 2010)
Indigenous Community Governance Project Annotated Bibliography (undated). http://www.anu.edu.au/caepr/ICGP_publications.php#biblio (accessed 4th May 2010)
Indigenous Community Governance Project. Community Governance. Vol 4, No. 1, October 2008
Indigenous Community Governance Project. Indigenous Governance Matters. No. 2, February 2008
Indigenous Community Governance Project. Indigenous Governance Matters. No. 1, January 2008
Langlands Alan. The Good Governance Standard for Public Services. The Independent Commission on Good Governance in Public Services. London. 2004
Larkins SL, Geia LK and Panaretto KS. Consultations in General Practice at an Aboriginal Community Controlled Health Service:DoTheyDiffer?RemoteandRuralHealth 2006; 6: 560
Maari Ma Health Aboriginal Corporation. Aboriginal Community Governance Resource Kit. A Resource Guide for Effective Communities. September 2002
McEwin,Kirsty.GPs–DealorNoDeal?General Practitioners in Aboriginal Community Controlled Health Services in NSW. Report prepared for the Aboriginal Health and Medical Council of NSW. Sydney. March 2010
Moriarty Patrick. Secrets of Successful Boards. Power Point Presentation. August 2010 http://www.ourcommunity.com.au (accessed 10th November 2010)
NACCHO. Report of the NACCHO Governance Scoping Study. Canberra. February 2011
National Aboriginal Health Strategy Working Party. A National Aboriginal Health Strategy. Canberra. Department of Aboriginal Affairs. 1989
Northern Territory Aboriginal Health Forum. Pathways to Community Control – An Agenda to Further Promote Aboriginal Community Control in the Provision of Primary Health Care Services. Undated. http://www.nt.gov.au/health (accessed 4th May 2010)

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 41
NSW Aboriginal Land Council Training and Development Unit. On-Line Governance Training Take Home Notes. February 2010
NSW Health. Corporate Governance and Accountability Compendium for NSW Health. North Sydney. December 2005
NSW Rural Doctors Network and Aboriginal Health and Medical Research Council of NSW. ACCHS Policy and Procedures Manual. 2010. http://www.nswrdn.com.au/site/index.cfm?display=76666 (accessed 10th November 2010)
Office of the Registrar of Indigenous Corporations. Research Paper. Analysing Key Characteristics in Indigenous Corporate Failure. Australian Government. Canberra. March 2010
Office of the Registrar of Indigenous Corporations. The ORIC Oracle. May 2010
Office of the Registrar of Indigenous Corporations. Healthy Corporation Checklist. 2010 http://www.oric.gov.au (accessed 7th October 2010)
OATSIH. Review of Reporting Requirements for OATSIH Funded Organisations. September 2008
OATSIH. Risk Assessment Profile Report (5th edition). Canberra. 2009
OATSIH. Accreditation Manual – A Handbook for Aboriginal and Torres Strait Islander Community Controlled Health Organisations. Canberra. 2010
Peiris David P, Patel Anushka A, Cass Alan, Howard Michael P, Tchan Maria L, Brady John P, De Vries Joanne, Rickards Bernadette A, Yarnold Della J, Hayman Noel E and
Brown Alex D. Cardiovascular Disease Risk Management for Aboriginal and Torres Strait Islander Peoples in Primary Health Care Settings: Findings from the Kanyini Audit. Medical Journal of Australia. 2009; 191 (6) pp304-309
Plumptre T and Graham J. Governance and Good Governance: International and Aboriginal Perspectives. Institute on Governance. Ottawa, Canada. 1999 http://iog.ca/sites/iog/files/govgoodgov.pdf (accessed 12th October 2010)
Pope Stephanie. PHO Governance Self Assessment Tool in Support of the Realisation of the Primary Health Care Strategy. District Health Board New Zealand, Health Care Aotearoa and Te Wana. 2007
Quality Improvement Council. Interpretive Guide for Aboriginal and Torres Strait Islander Health Services – QIC Health and Community Services Standards (6th edition). La Trobe University. 2010
Quality Improvement Council. QIC Standards and Accreditation Program. Organisational Analysis Tool. March 2010
Queensland Aboriginal and Islander Health Council. Why the Nation Needs More Indigenous Community Controlled Health Organisations. http://www.qaihc.com.au/index.php?page=community-control-in-qld (accessed 30th March 2010)
Queensland Aboriginal and Islander Health Council. Community Control Around the World. http://www.qaihc.com.au/index.php?page=community-control-in-qld (accessed 9th February 2010)

42 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
Queensland Aboriginal and Islander Health Council. Governance Framework and the Role of the Board. http://www.qaihc.com.au/index.php?page=qaihc-governance (accessed 30th March 2010)
Queensland Aboriginal and Islander Health Council. Investing in Community Control – A New Community Controlled Model for Long Term Reform. Power Point Presentation. August 2009
Queensland Aboriginal and Islander Health Council. A New Beginning, Charting a Better Way in Primary Health Care for Aboriginal and Torres Strait Islander Peoples. Submission to the National Health and Hospital Reform Commission. July 2008 http://www.qaihc.com.au/iploads/news/id42/QAIHC%20submission
Reconciliation Australia. Indigenous Governance Toolkit. September 2010 http://www.reconcialition.org.au/governance/tools-and-templates (accessed 7th October 2010)
Reconciliation Australia. Kalgoorlie Sharing More Success Governance Workshop. February 2010 http://www.reconciliation.org.au/home/projects/indigenous-governance-research-project (accessed 11th October 2010)
Reconciliation Australia. Celebrating Indigenous Governance – Success Stories of the 2008 Indigenous Governance Awards. Canberra. 2008 http://www.reconciliation.org.au/home/projects/indigenous-governance-research-project (accessed 4th May 2010)
Reconciliation Australia. Mt Isa Sharing Success Governance Workshop. September 2007. http://www.reconciliation.org.au/igawards/media/Workbook_Mt_Isa.pdf (accessed 4th May 2010)
Reconciliation Australia. Summary of Year Two Research Findings. Indigenous Community Governance Project. July 2007 http://www.reconciliation.org.au/home/projects/indigenous-governance-research-project (accessed 4th May 2010)
Reconciliation Australia. Summary of Preliminary Research Findings. Indigenous Community Governance Project. June 2006 http://www.reconciliation.org.au/home/projects/indigenous-governance-research-project (accessed 4th May 2010)
Royal Australian College of General Practitioners. Interpretive Guide of the RACGPP Standards for General Practices for Aboriginal and Torres Strait Islander Health Services (3rd edition). South Melbourne. April 2010
Sanders W. Being a Good Senior Manager in Indigenous Community Governance: Working with Public Purpose and Private Benefit. Centre for Aboriginal Economic Policy Research.DiscussionPaperNo.280/2006.Canberra 2006
Silburn Kate, Thorpe Alister and Anderson Ian. Taking Care of Business: Corporate Services for Indigenous Primary Healthcare Services. Support Systems for Indigenous Primary Health Care Services. 2010
Shannon Cindy and Longbottom Helen. Capacity Development in Aboriginal and Torres Strait Islander Health Service Delivery – Case Studies. Aboriginal and Torres Strait Islander Primary Health Care Review: Consultant Report No. 4. Commonwealth of Australia. Canberra. 2004

Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW 43
Smith Diane. Capacity Development for Indigenous Governance: Emerging Issues and Lessons from the Indigenous Community Governance Project. Centre for Aboriginal Economic Policy Research. October 2005
Sonnenfeld JA. What makes Great Boards Great. Harvard Business Review. 2002; 80 (9) pp 106-113
Stuart Adam. An Overview of the National Health and Hospitals Reform Policy Environment. AH&MRC Background Paper (unpublished). July 2010
Support Systems for Indigenous Primary Health Care Services Project. Report on the Second National Roundtable in Melbourne. 21st and 22nd June 2010
Support Systems for Indigenous Primary Health Care Services Project. Discussion Paper No. 2. June 2010
Support Systems for Indigenous Primary Health Care Services. Project Update. December 2009
Support Systems for Indigenous Primary Health Care Services. Draft Literature Review. Australian Institute for Primary Care (unpublished). May 2008
Sullivan Patrick. Indigenous Governance – The Harvard Project on Native American Economic Development and Appropriate Principles of Governance for Aboriginal Australia. Australian Institute of Aboriginal and Torres Strait Islander Studies Research Discussion Paper No. 17. Canberra. February 2006
Taylor John. Capacity Building for Indigenous Governance: Social Indicators for Indigenous Governance. Centre for Aboriginal Economic Policy Research. October 2005
Thorpe Alister, Silburn Kate and Anderson Ian. Support Systems for Indigenous Primary Health Care Services Project. Discussion Paper No. 1. November 2008
Wakerman J, Matthews S, Hill P and Gibson O. Beyond Charcoal Lane, Aboriginal and Torres Strait Islander Health Managers: Issues and Strategies to Assist Recruitment, Retention and Professional Development. 2000
Webster Ruth J, Heeley Emma L, Peiris David P, Bayram Clare, Cass Alan and Patel Anushka A. Gaps in Cardiovascular Disease Risk Management in Australian General Practice. Medical Journal of Australia. 2009; 191 (6) pp324-329
Wilson J. Remote Area Aboriginal Health Service Managers: Key Practice Challenges. Australian Journal of Rural Health. 2001; Vol 9, pp 138-140

44 Everything Goes Great Until There’s a Problem – Corporate Governance in Aboriginal Community Controlled Health Services in NSW
List of people consulted in the AH&MRC Corporate Governance Project
Ms Connie Ah See AH&MRC (until January 2011)Mr Darren Ah See Wellington Aboriginal Health CorporationMs Sandra Bailey AH&MRCDr Liz Barrett NSW Rural Doctors Network Ms Melinda Bell AH&MRC Ms Julie Booker Illawarra Aboriginal Medical ServiceMs Trish Bullen Wellington Aboriginal Health CorporationMr Selwyn Button Queensland Aboriginal and Islander Health CorporationDr Ian Cameron NSW Rural Doctors Network Mr Scott Campbell OATSIHMr Chris Clarke Northern Rivers General Practice Network Ms Kerry Cole OATSIHMr Harry Cutmore Tamworth Aboriginal Health ServiceMr Michael Cutmore Tamworth Aboriginal Health ServiceMr Peter Davidson OATSIHMr Berlos Davis AH&MRCDr Rose Ellis NSW Rural Doctors Network Ms Louise Fearnley NSW Rural Doctors NetworkMr Warren Frost AH&MRCMr Lyndon Gray Coomealla Aboriginal Health CorporationMs Kaylie Harrison AH&MRCMs Kristie Harrison AH&MRCMr John Hendry AH&MRCDr Jenny Hunt AH&MRC Ms Jessica Jeeves Reconciliation AustraliaMr Nathan Jones OATSIHDr Kath Keenan AH&MRC (until January 2011) Mr David Kennedy Galambila Aboriginal Health CorporationMr Graham Kershaw North West Slopes Division of General PracticeMr Mike Kirby AH&MRC Ms Debbie McGowan Armajun Aboriginal Health ServiceMr Scott Monaghan Bulgarr Ngaru Medical Aboriginal CorporationMr Mark Moore Bullinah Aboriginal Health ServiceDr Richard Nelson Aboriginal Health Council of South Australia Mr Jamie Newman Orange Aboriginal Health ServiceMs Stephanie Pope ConsultantMr James Porter AH&MRC Ms Mary Porter Tamworth Aboriginal Health ServiceMrs Leona Quinnell Armajun Aboriginal Health ServiceDr Kate Silburn Institute of Primary Healthcare, La Trobe UniversityMr Terry Smith Aboriginal Health CollegeMr Adam Stuart AH&MRC Ms Davina Thomas Reconciliation AustraliaMr Ben Thompson AH&MRCMs Margaret Tuema OATSIHMr Rodger Williams AH&MRCMs Colleen Wykes Wellington Aboriginal Health Corporation
APPENDIX A


Aboriginal Health & Medical Research Council of NSW
PO Box 1565Strawberry Hills NSW 2012