evaluation of vch-759 monotherapy in hepatitis c infection
TRANSCRIPT

www.elsevier.com/locate/jhep
Journal of Hepatology 51 (2009) 39–46
Evaluation of VCH-759 monotherapy in hepatitis C infectionq
Curtis Cooper1,*, Eric J. Lawitz2, Peter Ghali3, Maribel Rodriguez-Torres4,Frank H. Anderson5, Samuel S. Lee6, Jean Bedard7, Nathalie Chauret7, Roch Thibert7,
Isabel Boivin7, Olivier Nicolas7, Louise Proulx7
1The Ottawa Hospital, Division of Infectious Disease, Ottawa, ON, Canada K1H 8L62Alamo Medical Research, San Antonio, TX, USA
3Department of Gastroenterology and Hepatology, McGill University Health Center, Royal Victoria Hospital, Montreal, QC, Canada4Fundacion de Investigacion de Diego, San Juan, PR, USA
5Liver and Intestinal Research Center, Vancouver, BC, Canada6Liver Unit, University of Calgary, Calgary, AB, Canada
7ViroChem Pharma Inc., Laval, QC, Canada
Background/Aims: VCH-759 is a non-nucleoside inhibitor of HCV RNA-dependent polymerase with sub-micromolar
IC50 values versus genotype 1a /1b replicons.
Methods: The antiviral activity, pharmacokinetics and tolerability of VCH-759 administered as monotherapy for 10
days with a 14 day follow-up period were evaluated in 31 treatment-naıve genotype 1 participants. Three cohorts received:
400 mg thrice (t.i.d.), 800 mg twice (b.i.d.), 800 mg t.i.d or placebo.
Results: VCH-759 was well tolerated with the most frequent adverse event being gastrointestinal upset in both the active
and placebo groups attributable, in part, to the dosing vehicle. VCH-759 was rapidly absorbed and trough plasma levels wereat or above the IC90 (non protein-adjusted) for all dosing regimens. The mean maximal decrease in HCV RNA log10 (IU/mL)
was 1.97, 2.30 and 2.46 for 400 mg t.i.d., 800 mg b.i.d. and 800 mg t.i.d. doses. Viral polymerase genotypic sequencing
revealed emergence of HCV variants in a majority of participants that coincided with on-treatment viral rebound.
Conclusions: VCH-759 was well tolerated and achieved a P 2 log10 decline in HCV RNA with 800 mg b.i.d. and t.i.d
doses. In a subset of participants, viral rebound was observed and associated with resistant variants. This data supports
further evaluation of VCH-759 in combination with interferon–ribavirin treatment.
� 2009 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Keywords: Non-nucleoside NS5b inhibitor; Proof-of-concept study; Antiviral activity; Safety and tolerability;
Pharmacokinetics; Variant identification
0168-8278/$36.00 � 2009 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.jhep.2009.03.015
Received 16 October 2008; received in revised form 17 February 2009; accepted 19 March 2009; available online 23 April 2009
Associate Editor: M.P. Mannsq The authors have declared that this study was funded by ViroChem Pharma Inc. J.B., N.C., R.T., I.B., O.N., and L.P. are employees of
ViroChem PharmaInc. The other authors have also declared a relationship with the manufacturers of the drugs involved.* Corresponding author. Tel.: +1 613 7378924; fax: +1 613 7378164.
E-mail address: [email protected] (C. Cooper).Abbreviations: HCV, hepatitis C virus; RNA, ribonucleic acid; IC50, 50% inhibitory concentration; t.i.d., three times daily; b.i.d., twice daily; IC90,
90% inhibitory concentration; DNA, deoxyribonucleic acid; TI, therapeutic index; CC50, 50% cytotoxic concentration; PK, pharmacokinetic; PIB,powder-in-bottle; RV, reconstitution vehicle; BMI, body mass index; ALT, alanine aminotransferase; PP, per-protocol; Cmax, maximum concent-ration; Tmax, time at maximum concentration; AUC, area-under-the-curve; t1/2, half-life; LC/MS/MS, liquid chromatography/mass spectrometer/mass spectrometer; AE, adverse event; GI, gastro-intestinal; AST, aspartate aminotransferase; SD, standard deviation; SVR, sustained virologicalresponse; RVR, rapid virological response; STAT-C, specifically targeted antiviral therapy for Hepatitis C.

40 C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46
1. Introduction
The hepatitis C virus (HCV) is a 9.6 kb positivestrand ribonucleic acid (RNA) virus of the flaviviridaefamily, genus hepacivirus. The genome comprises a sin-gle open-reading frame coding for a �3000 amino acidpolypeptide which is further processed into individualstructural (core, E1 and E2) and non-structural (NS2,NS3, NS4A, NS4B, NS5A and NS5B) proteins by hostand viral NS2 (zinc-dependent) and NS3 (chymotryp-sin-like) proteases [1]. The non-structural proteins func-tion as enzymes or accessory factors involved ingenomic replication. The viral replication strategy issimilar to that of other positive strand viruses, withthe initial synthesis of a replicative intermediate nega-tive strand RNA by the NS5B RNA-dependent RNApolymerase. This negative strand RNA then serves asa template for genomic RNA production. The NS3and the NS5B enzymes are key targets for anti-HCVtherapy, as they are essential for HCV replicationand infectivity [2–5]. The NS5B enzyme has the charac-teristic right-handed ‘‘fingers-palm-thumb” domain ofpolymerases [4]. The active site, which resides in thepalm region, contains the conserved GDD motif ofpolymerases and is partially enclosed by the fingerand thumb domains.
VCH-759 is a novel substituted thiophene-2-carbox-ylic acid derivative non-nucleoside inhibitor of HCVNS5B polymerase genotype 1a and 1b. This com-pound inhibits the NS5B (IC50 1a = 0.41 lM andIC50 1b = 0.38 lM) by binding to an allosteric sitein the ‘thumb’ domain situated �35 A from the activesite. X-ray crystallography studies suggest that inhibi-tion of RNA synthesis initiation may result fromenzyme conformational changes induced by occupancyof the compound binding site [6]. VCH-759 is activeagainst HCV sub-genomic replicon in Huh-7 cells(IC50 � 0.3 lM for both 1a and 1b genotypes). Thecompound is also selective for the HCV NS5B poly-merase relative to human DNA polymerases a, band c (IC50 > 100 lM). VCH-759 has a good in vitro
therapeutic index (TI) (CC50/IC50) > 600 and non-clin-ical safety profile.
Given an estimated 170 million people worldwideinfected by HCV and limitations of currently avail-able interferon-based therapies, there is an importantunmet need for novel, more effective, more conve-nient, and better tolerated anti-HCV treatments [7].Hence, we evaluated the antiviral activity, safety, tol-erability and HCV variant selection of VCH-759administered as monotherapy for 10 days in HCVgenotype 1a or 1b-infected treatment-naıve partici-pants. Pharmacokinetic (PK) profile, plasma HCVRNA kinetics and correlation between VCH-759plasma trough levels and HCV RNA reduction werealso assessed.
2. Patients and methods
2.1. Study design
This was a randomized, double-blinded, placebo-controlled studyconducted following research ethics review/institutional review boardand approval at all participating sites. Consenting participants wereassigned to VCH-759 doses (400 mg t.i.d., 800 mg b.i.d. and 800 mgt.i.d.) or corresponding placebo in a 3:1 ratio (n = 12 for 400 and800 mg t.i.d. cohorts; n = 8 for 800 mg b.i.d cohort). Dosing occurreddaily under direct supervision for 10 days at 7h:00, 13h:00 and 21h:00for t.i.d. dosing, and at 7h:00 and 19h:00 for b.i.d. dosing. Beforedosing, participants were required to consume a light meal. VCH-759 was supplied as an oral solution formulation in individual120 mL clear glass bottles. The oral solution was reconstituted bycombining the appropriate VCH-759 powder-in-bottle (PIB) dose ina 30% polyethylene glycol 400/15% Solutol� HS15 aqueous reconsti-tution vehicle (RV) (20 and 40 mL for the 400 and 800 mg doses,respectively).
2.2. Participants
Treatment-naıve, genotype 1-infected male or female participantsbetween 18 and 60 years of age with a body mass index (BMI)633 kg/m2 were recruited. Baseline plasma HCV RNA greater than100,000 IU/mL, alanine aminotransaminase (ALT) values less thanfive times the upper limit of normal and a Metavir liver fibrosis stagebetween 0 and 3 were required.
2.3. Endpoint measures
The primary endpoint was defined as the absolute change in plasmaHCV RNA levels between baseline to nadir measured with the COBASAmplicor� HCV Monitor v.2 kit (Roche Diagnostics, Laval, QC).Blood samples for evaluation of the plasma HCV RNA viral load werecollected at screening, before the first dose on Days 1–10 and at follow-up visits (Days 11, 17 and 24). Blood samples for NS5B polymerasesequencing were collected before the first dose on Day 1 and on Days11, 17 and 24. Sequence analyses were performed at ViroChemPharma.
The complete PK profile was obtained on Days 1 and 10 for thefirst daily dose. Approximately 6 mL of blood were collected at the fol-lowing time points: for the t.i.d. cohorts, at 10 min before dosing (nom-inal time 0) and at 0.5, 1, 1.5, 2, 3, 4, 5 and 6 h after administration ofstudy medication and for the b.i.d. cohort, 10 min before the morningdose (nominal time 0), at 0.5, 1, 1.5, 2, 3, 4, 5, 6, 8 and 10 h afteradministration of the study medication, and at 5 min before the even-ing dose (nominal time 12 h). For determination of pre-dose VCH-759trough levels, blood was drawn within 10 min before the first dose onDays 2, 3, 4, 5, 6, 7, 8 and 9. On Day 11, blood sampling for VCH-759plasma trough level quantification was collected at the same time as theDay 9 blood draw. A validated liquid chromatography/mass spectrom-eter/mass spectrometer bio-analytical method for the evaluation ofVCH-759 plasma concentration was used [unpublished internal report;Anapharm, Quebec, Canada].
2.4. Statistical methods
The data were summarized using descriptive statistics. Change inplasma HCV RNA from baseline to subsequent time points was eval-uated by a two-sample t-test. Comparisons between dosing groups andtheir respective placebo group were performed. Analyses of antiviralactivity were based on per protocol (PP) participant population. A ser-ies of PK parameters (e.g., Cmax, Tmax, AUC, t1/2) were determinedfrom blood samples collected at pre-specified time points. Correlationsbetween VCH-759 trough plasma levels and plasma HCV RNA fromDay 2 through end of treatment were analyzed by Pearson’s correla-tion coefficient.

C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46 41
2.5. Genotypic analysis of HCV variants
The HCV RNA was isolated from patients’ sera using the QIA-amp� Viral Minikit (Qiagen, Mississauga, ON). The cDNAs were syn-thesized using random hexamers (Invitrogen, Burlington, ON) and theSuperScript� III reverse transcriptase (RT) (Invitrogen) for 1 h at50 �C. For population sequencing, a series of specific primers for geno-type 1a and genotype 1b were designed based on the comparison of 92HCV NS5A and NS5B sequences retrieved from the Hepatitis C Data-base (www.hcvdb.org). Primers designed by Yao et al. were also uti-lized [8]. Briefly, aliquots of the cDNA reactions were subjected toamplification by PCR using combinations of upstream primers anddownstream primers in order to obtain overlapping products ofapproximately 700–1200 bp to cover the entire NS5B region. ThePCR reactions of 50 ll consisted of the high fidelity buffer, 2 mMMgCl2, 3% DMSO, 200 lM dNTP, 0.5 lM each primer and 1 unitof the Phusion Hot start DNA polymerase (Finnzymes Oy, Epsoo,Finland). The following conditions were used for all PCRs: initialdenaturation of 2 min at 98 �C, followed by 42 cycles with 10 s at98 �C, 15 s at 55 �C, 70 s at 72 �C, and a final elongation step of10 min at 72 �C. For the clonal analysis, PCR products, encompassingthe VCH-759-binding pocket (amino acids 340–539), were producedusing two generated primers (50 ACG GAG GCY ATG ACY AGRTAY TC and 50 AT YGG AGT GAG YTT RAG YTT KGT) for bothgenotypes 1a and 1b. The appropriate sized product (599 bp) was thengel-purified (QIAXII� gel purification kit, Qiagen) and cloned usingthe Zero Blunt� TOPO� PCR cloning kit (Invitrogen) and trans-formed TOP10 E. coli cells were plated on kanamycin LB agar plates.Alternatively, PCR fragments were treated with the Taq DNA poly-merase and cloned using the TA cloning� kit (Invitrogen). Colonieswere randomly picked and a variable number (6–30) of clones per par-ticipant and per time point were sent for sequencing at Genome Que-bec (Montreal, QC).
2.6. Phenotypic analysis of HCV variants
2.6.1. Generation of stable HCV replicon cellsWith the exception of V494A, all variations were introduced into
the pFKI389/NS3-30/adapt vector [2,9] obtained from Dr. Ralf Bart-enschlager (ReBLikon GmbH, Gau-Odernheim, Germany) or into agenotype 1a sub-genomic replicon that was shown to be sensitive toVCH-759 by PCR-based site-directed mutagenesis and standardrecombinant DNA technologies. In vitro produced transcripts (Ambi-on, Austin, TX) were electroporated into Huh-7 derived cells asdescribed by Lohmann et al. [2] and selected colonies were expandedand sequence of the progeny RNA was confirmed by direct sequencingof the RT-PCR products.
2.6.2. Drug sensitivity assay using real-time PCRThe 9–13 replicon cells and the stable recombinant replicon cells
were seeded in complete DMEM media plus 10% FBS. After anincubation period of 3–4 h, VCH-759 was added at various concen-
Table 1
Characteristics of participants at Day 1 (or Baseline) with evaluable efficacy d
Placebo (n = 9)
Average Age (±SD) (range) (yr) 45.2 ± 1.92 (41–52)Average BMI (±SD) (kg/m2) 26.7 ± 3.48Male/Female (n) 7/2Genotype 1a/1b (n) 8/1Race (n)
White 5Black 1Hispanic 3Other –Average viral RNA concentration (log10 IU/mL) 6.3Median ALT (U/L) (range) 73 (20–186)
trations. Cells were then further incubated for 4 days at 37 �C with5% CO2. Thereafter, total RNA was extracted using the RNeasy�
kit (Qiagen) according to the manufacturer’s protocol and thecDNA synthesis was performed using the MMLV reverse transcrip-tase and random hexamer primer (Invitrogen). The inhibitory effectof drugs against the wild-type replicon cells, resistant colonies orrecombinant replicons cells was determined by monitoring the levelsof HCV RNA normalized to the 18S ribosomal RNA by real-timePCR using the ABI PRISM� 7700 Sequence Detection System(Applied Biosystems, Foster City, CA). To investigate the potentialeffects of VCH-759 on 9–13 replicon cells proliferation, a [3H] thy-midine incorporation assay was performed. Briefly, replicon cellswere seeded at sub-confluence density for 96-h incubation in thepresence of VCH-759, then 10 lCi/mL solution of [3H] methyl thy-midine was added in culture medium. The plates were incubated foran additional 18 h at 37 �C and the accumulation of [3H] methylthymidine, representing viable replicating cells, was measured usinga liquid scintillation counter.
2.6.3. Replication capacity of HCV recombinant repliconclones
A transient replicon system was used for this study. Briefly, tran-scripts (10–20 lg) derived from recombinant pFK I389luc/NS3-30/5.1constructs were electroporated in Huh-7 derived cells [9]. Cells wereimmediately transferred to 40 mL of complete DMEM and seededin 96-well plates, with one plate per each time point (4 and 96 h).Cells were then further incubated for 4 h up to 96 h at 37 �C in a5% CO2 incubator. For each time point post-transfection, the culturemedia from each corresponding plate was removed and cells werelysed by the addition of a luciferase buffer (luciferin substrate in buf-fered detergent). Plates were then read for luciferase counts using aluminometer (Wallac MicroBeta TriluxTM, Perkin-Elmer, MA). Repli-cation capacity of all recombinant variants were determined as theratio of the luciferase signal at day 4 post-electroporation dividedby the luciferase signal at 4 h post-transfection to normalize for thetransfection efficiency.
3. Results
Of 34 randomized participants, 32 completed thestudy and were evaluated for compound safety. Twoparticipants dropped out before receiving any treatment:one participant no longer met the inclusion/exclusioncriteria and one subject withdrew consent. As a singlegenotype 6-infected participant was erroneouslyenrolled, 31 were ‘efficacy-evaluable’. Table 1 presentsthe principal key demographic characteristics of theparticipants.
ata.
400 mg t.i.d. (n = 8) 800 mg b.i.d. (n = 5) 800 mg t.i.d. (n = 9)
46.5 ± 5.35 (39–54) 35.2 ± 9.85 (25–47) 45.0 ± 13.10 (20–61)23.2 ± 1.67 25.1 ± 4.91 26.6 ± 4.996/2 2/3 6/37/1 4/1 6/3
6 2 5– – –– 3 22 – 26.4 5.8 6.448 (27–203) 71 (43–192) 62 (31–177)

42 C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46
3.1. Safety and tolerability
The compound was well tolerated without severeadverse events. The overall incidence of adverse events(AE) was similar across treatment groups (Table 2).There were no discontinuations due to AEs or death.Adverse events were experienced by 30 (88%) partici-pants. Mild and moderate AEs occurred in 27 (79%)and 12 (35%) participants, respectively. The most fre-quent treatment-emergent AEs in active and placeborecipients, respectively, included diarrhea (79% vs56%), headache (30% vs 22%), flatulence (24% vs11%), dyspepsia (19% vs 11%) and fatigue (22% vs0%). We believe that the formulation vehicle (an aque-ous mixture of polyethylene glycol 400 and Solutol�
HS15) likely contributed to the gastrointestinal (GI)adverse events observed in this study. Of note, GIadverse events did not negatively impede daily activities.All AEs were resolved by the end of follow-up. No QTprolongation or other electrocardiographic abnormali-ties were observed.
Clinical laboratory evaluations revealed no clinicallysignificant effect of VCH-759 treatment on complete
Table 2
Summary of safety data for all cohorts and placebo.
Placebon = 9
400 mgt.i.d.n = 9
800 mgb.i.d.n = 5
800 mgt.i.d.n = 9
Any adverse events(number of subjects)
6 7 4 9
Gastrointestinal
disorders
6 7 4 9
Diarrhea 5 5 4 9Flatulence 1 2 2 1Dyspepsia 1 1 0 4Nausea 1 1 2 0Abdominal pain 0 2 0 1Vomiting 0 0 1 3General disorders 0 4 1 5Fatigue 0 2 1 2Chills 0 1 0 0Nervous system disorders 2 4 0 5Headache 2 3 0 5Somnolence 1 0 0 1Vascular disorders 0 0 0 2Flushing 0 0 0 2
Table 3
Pharmacokinetic parameters (±SD) of VCH-759 after administration of differ
Day 1 D
Cmax
(ng/mL)Tmax (h) AUC0�6 h
a
(ng � h/mL)t1/2 (h) C
(
400 mg t.i.d. 1857 ± 773 1.62 ± 0.65 6553 ± 2518 2.65 ± 0.99 2800 mg b.i.d. 4627 ± 1689 1.90 ± 1.02 20706 ± 13395 2.76 ± 0.75 4800 mg t.i.d. 4857 ± 4107 2.77 ± 2.06 19286 ± 17173 3.02 ± 1.29 5
a Corresponds to AUC0�12 h for b.i.d. cohort.
blood count, blood chemistry or urinalysis. There wereno clinical signs or symptoms of liver toxicity in any par-ticipants during dosing or in the post-dosing period. Onaverage, ALT levels decreased with VCH-759 adminis-tration in all cohorts. Increased total blood bilirubinoccurring after VCH-759 dosing was observed in oneparticipant (3%) in the 800 mg t.i.d. cohort. In this case,the total bilirubin was slightly above the upper limit ofnormal at baseline (i.e., before dosing). The bilirubindoubled from Day 1 (1.2 mg/dL) to Day 2 (2.4 mg/dL)of dosing but subsequently returned to pretreatment lev-els by Day 7 despite continued dosing of VCH-759. Theincreased bilirubin was predominantly unconjugated.This increase in bilirubin was accompanied by anincrease in ALT from 113 U/L at screening and Day 1to a maximum of 231 U/L on Day 6. The ALT valuereturned to baseline levels by Day 17. In another recipi-ent of 800 mg t.i.d. dosing, a single ALT elevation (154U/L) on Day 4 was observed, however, ALT on Days 3and 5 were 80 and 81, respectively. All ALT values forthis patient were in the normal range (range of 60–90U/L), both at baseline and during the dosing period.No change in bilirubin was observed in this patient.
3.2. Pharmacokinetics
VCH-759 was rapidly absorbed with a time at whichplasma concentration was maximal of 1.62, 1.90 and2.77 h and peak plasma levels of 1857, 4627 and4857 ng/mL at Day 1 for the 400 mg t.i.d., 800 mgb.i.d. and 800 mg t.i.d. doses, respectively (Table 3).VCH-759 did not accumulate significantly following 10days of twice- or thrice-daily administrations as shownby the ratio of approximately 1 when comparing AUC-
Day10 to AUCDay1. Rate (Cmax) and extent of exposure(AUC) were variable and appeared to be more than pro-portional between 400 and 800 mg administered thrice-daily. Tmax was delayed by approximately 1 h with the800 mg dose compared to the 400 mg dose. Eliminationhalf-life, clearance and volume of distribution appearedto be similar between the three cohorts.
VCH-759 plasma trough concentrations betweenDays 2 and 11 were at or above the replicon IC90
(420 ng/mL, 0.85 lM non protein-adjusted) for theduration of treatment for each dosing regimen. There
ent dosing regimens on Days 1 and 10 of treatment.
ay 10 AUCDay10/AUCDay1
max
ng/mL)Tmax (h) AUC0�6 h
a
(ng � h/mL)t1/2 (h)
130 ± 1185 1.16 ± 0.37 7181 ± 3799 2.87 ± 0.59 1.10351 ± 2468 2.20 ± 1.79 21806 ± 19926 2.95 ± 0.40 1.05740 ± 5917 2.31 ± 1.66 22706 ± 26035 2.80 ± 0.66 1.18

C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46 43
was no clear correlation between baseline HCV RNAlevels and viral load decline during the dosing periodin active compound recipients. However, this analysiswas limited by the small sample size.
3.3. Antiviral activity
All participants who received VCH-759 achieved arapid initial decline of approximately 1.5 log10 in plasmaHCV RNA level during the first two days of dosing asshown in Fig. 1B–D. The change from baseline inplasma HCV RNA to nadir was 2 log10 or greater inthe three active treatment groups. The 800 mg t.i.d doseproduced the greatest change in viral load (mean: �2.46log10, range: �1.2 to �3.4) followed by the 800 mg b.i.d.(mean: �2.30 log10, range �1.5 to �2.9) and 400 mgt.i.d. (mean: �1.97 log10, range: �1.4 to �2.6) dosedcohorts (Fig. 1B–D). The change from baseline to nadirwas statistically significant in all groups (400 mg t.i.d.,p = 0.0002; 800 mg b.i.d., p = 0.0021; 800 mg t.i.d.,p = 0.0004). Viral rebound, defined as >0.75 log10
increase from nadir before Day 11, was observed in 5of 8 (63%), 5 of 5 (100%) and 6 of 9 (67%) participantsin the 400 mg t.i.d., 800 mg b.i.d. and 800 mg t.i.d.cohorts, respectively. There was no apparent differencein HCV RNA decline between subtypes 1a and 1b.However, low numbers of 1b (n = 6) limited our abilityto fully investigate this issue.
3.4. Genotypic analysis of HCV variants
Initially, the entire NS5B gene was sequenced (popu-lation sequencing of overlapping PCR fragments) atbaseline (Day 1), end of dosing (Day 11), and follow-up days (Days 17 and 24) of the study for each partici-pant treated with VCH-759. Amino acids 419, 423, 482and 494 within the NS5B gene were consistently foundto present more amino acid variations since mixednucleotide populations were found at these positions.Amino acid changes outside the VCH-759 bindingpocket were sporadic and not considered potential resis-tance variations. In order to obtain a quantitative eval-uation of the HCV variants selected during VCH-759dosing, a clonal sequencing analysis method of theVCH-759 binding pocket (amino acids 340–539) wasdeveloped and validated using mixes of known amountsof recombinant RNAs. An average of 30 clones perpost-treatment timepoint, per participant, were analyzedwhich theoretically allows a 75% probability of detectinga minority clone present at a frequency of 5% within apopulation [10]. Amino acid changes at specific posi-tions within the VCH-759 binding pocket, other thanL419, M423, I482 and V494, with an increase of lessthan 5% frequency from baseline (Day 1) to end of study(Day 24) were regarded as non significant (data notshown). Genotypic analysis of all samples from patients
treated with VCH-759 collected at Days 1, 11, 17 and 24revealed the most prevalent changes at position 423(M423T/V/I) (Table 4). The number of sequencedclones with any variation at position L419, M423,I482 or V494 was found to be 1.4% at the baseline,67.5% at the end of treatment, 60.4% at Day 17 and53.1% at the end of the study (Day 24). Increase ofamino acid changes up to 6.4%, 50.4% and 6.2% frombaseline was observed at positions 419, 423 and 482,respectively, at the end of treatment (Table 4).
The M423T variant was the predominant variantfound at Days 11, 17 and 24 (Table 4) but decreasedover time (e.g., Day 11 (32.1%) vs Day 24 (19.6%)).The frequency of M423V and L419M variations was rel-atively stable during the study: 15.9% and 17.7% forM423V and 6.4% and 6.0% for L419M at Days 11and 24, respectively (Table 4). Some double variantswere also detected at very low frequency. M423T/I482L, M423I/I482L, L419M/I482T and L419M/V494I variants were detected at 0.5% and 0.6%, 0.2%and 0.2%, 0% and 0.2% and 3.2% and 1.4% frequencyat Days 11 and 17, respectively (Table 4). No doublevariants were detected at Day 24.
3.5. Phenotypic analysis of HCV variants
Since amino acids L419, M423, I482 and V494 werefound to be enriched in about two-thirds of allsequenced clones at the end of treatment, their actualrole in conferring resistance to VCH-759 was investi-gated. Recombinant replicons with single variation atpositions L419, M423, I482 and V494 as well as variouscombinations of the two simultaneous variations weregenerated and stable replicon cell lines were obtainedfor each one of these variations.
The activity of VCH-759 against the wild-type repli-con cells (genotype 1a or 1b) was compared to the var-iant replicon. A 1.6- to 54-fold increase of thecompound’s IC50 was recorded for the replicons harbor-ing single variations at positions L419, M423, I482 orV494 whereas up to 462-fold reduction in susceptibility(IC50) to the compound was noticed for the repliconharboring the M423I/I482L double variation. In themajority of participants who experienced a viralrebound, variants were found to remain present up to13 days despite an in vivo high HCV replication rate.Some of the variations found in participants treatedwith VCH-759 were not previously selected in vitro usingthe replicon system (e.g., V494A). However, it should benoted that the 1a genotype was over-represented in trea-ted patients (17 treated patients) compared to genotype1b (5 treated patients) and all the in vitro studies wereperformed with the 1b sub-genomic replicon.
A transient replicon assay using variants (L419M,M423I, M423T, M423V, I482L, I482T, I482V, V494A,L419M/I482T, M423I/I482L, M423T/I482L) engineered

Fig. 1. Individual plasma HCV RNA reduction profiles following the administration of placebo (A) or VCH-759 400 mg t.i.d. (B), 800 mg b.i.d. (C) and
800 mg t.i.d. (D). (note: shaded area represents treatment period; solid lines are patients with HCV genotype 1a; dotted lines are patients with HCV
genotype 1b).
44 C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46
into the wild-type sub-genomic replicon 1b was chosenfor characterization of their replication capacities. Allvariants were associated with in vitro reduced replication
fitness when compared to the parental wild-type repliconin the absence of VCH-759. The degree of reduced fit-ness ranged broadly depending on the specific mutation.
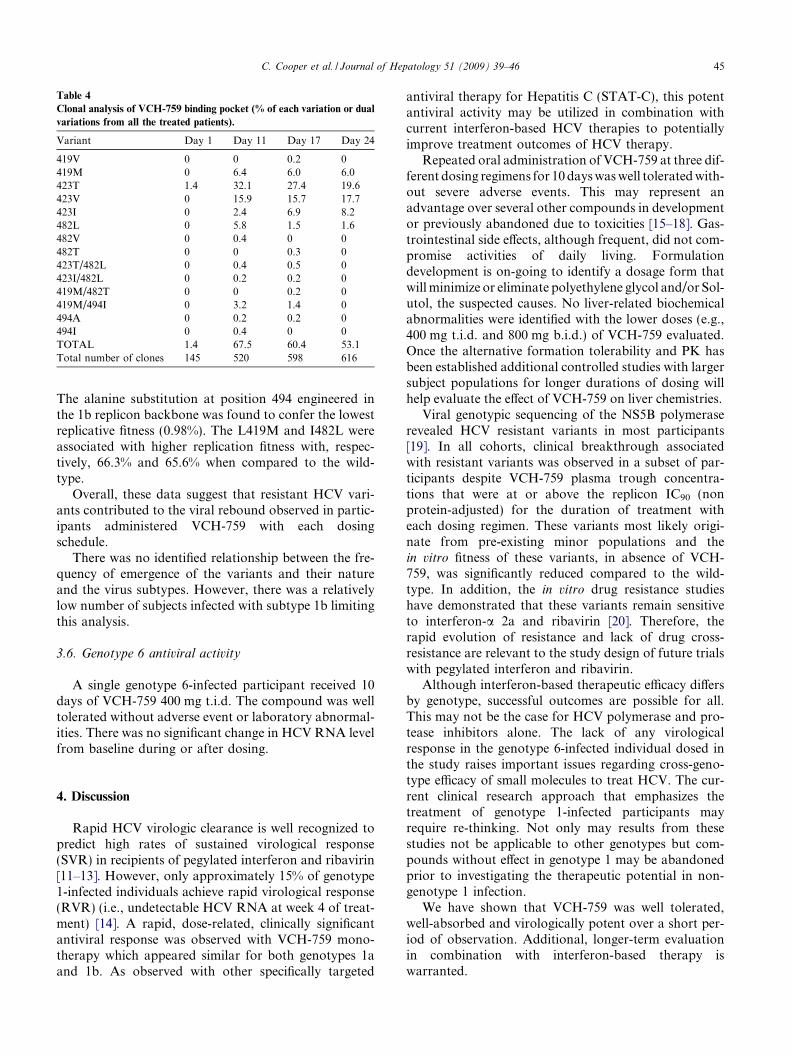
Table 4
Clonal analysis of VCH-759 binding pocket (% of each variation or dual
variations from all the treated patients).
Variant Day 1 Day 11 Day 17 Day 24
419V 0 0 0.2 0419M 0 6.4 6.0 6.0423T 1.4 32.1 27.4 19.6423V 0 15.9 15.7 17.7423I 0 2.4 6.9 8.2482L 0 5.8 1.5 1.6482V 0 0.4 0 0482T 0 0 0.3 0423T/482L 0 0.4 0.5 0423I/482L 0 0.2 0.2 0419M/482T 0 0 0.2 0419M/494I 0 3.2 1.4 0494A 0 0.2 0.2 0494I 0 0.4 0 0TOTAL 1.4 67.5 60.4 53.1Total number of clones 145 520 598 616
C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46 45
The alanine substitution at position 494 engineered inthe 1b replicon backbone was found to confer the lowestreplicative fitness (0.98%). The L419M and I482L wereassociated with higher replication fitness with, respec-tively, 66.3% and 65.6% when compared to the wild-type.
Overall, these data suggest that resistant HCV vari-ants contributed to the viral rebound observed in partic-ipants administered VCH-759 with each dosingschedule.
There was no identified relationship between the fre-quency of emergence of the variants and their natureand the virus subtypes. However, there was a relativelylow number of subjects infected with subtype 1b limitingthis analysis.
3.6. Genotype 6 antiviral activity
A single genotype 6-infected participant received 10days of VCH-759 400 mg t.i.d. The compound was welltolerated without adverse event or laboratory abnormal-ities. There was no significant change in HCV RNA levelfrom baseline during or after dosing.
4. Discussion
Rapid HCV virologic clearance is well recognized topredict high rates of sustained virological response(SVR) in recipients of pegylated interferon and ribavirin[11–13]. However, only approximately 15% of genotype1-infected individuals achieve rapid virological response(RVR) (i.e., undetectable HCV RNA at week 4 of treat-ment) [14]. A rapid, dose-related, clinically significantantiviral response was observed with VCH-759 mono-therapy which appeared similar for both genotypes 1aand 1b. As observed with other specifically targeted
antiviral therapy for Hepatitis C (STAT-C), this potentantiviral activity may be utilized in combination withcurrent interferon-based HCV therapies to potentiallyimprove treatment outcomes of HCV therapy.
Repeated oral administration of VCH-759 at three dif-ferent dosing regimens for 10 days was well tolerated with-out severe adverse events. This may represent anadvantage over several other compounds in developmentor previously abandoned due to toxicities [15–18]. Gas-trointestinal side effects, although frequent, did not com-promise activities of daily living. Formulationdevelopment is on-going to identify a dosage form thatwill minimize or eliminate polyethylene glycol and/or Sol-utol, the suspected causes. No liver-related biochemicalabnormalities were identified with the lower doses (e.g.,400 mg t.i.d. and 800 mg b.i.d.) of VCH-759 evaluated.Once the alternative formation tolerability and PK hasbeen established additional controlled studies with largersubject populations for longer durations of dosing willhelp evaluate the effect of VCH-759 on liver chemistries.
Viral genotypic sequencing of the NS5B polymeraserevealed HCV resistant variants in most participants[19]. In all cohorts, clinical breakthrough associatedwith resistant variants was observed in a subset of par-ticipants despite VCH-759 plasma trough concentra-tions that were at or above the replicon IC90 (nonprotein-adjusted) for the duration of treatment witheach dosing regimen. These variants most likely origi-nate from pre-existing minor populations and thein vitro fitness of these variants, in absence of VCH-759, was significantly reduced compared to the wild-type. In addition, the in vitro drug resistance studieshave demonstrated that these variants remain sensitiveto interferon-a 2a and ribavirin [20]. Therefore, therapid evolution of resistance and lack of drug cross-resistance are relevant to the study design of future trialswith pegylated interferon and ribavirin.
Although interferon-based therapeutic efficacy differsby genotype, successful outcomes are possible for all.This may not be the case for HCV polymerase and pro-tease inhibitors alone. The lack of any virologicalresponse in the genotype 6-infected individual dosed inthe study raises important issues regarding cross-geno-type efficacy of small molecules to treat HCV. The cur-rent clinical research approach that emphasizes thetreatment of genotype 1-infected participants mayrequire re-thinking. Not only may results from thesestudies not be applicable to other genotypes but com-pounds without effect in genotype 1 may be abandonedprior to investigating the therapeutic potential in non-genotype 1 infection.
We have shown that VCH-759 was well tolerated,well-absorbed and virologically potent over a short per-iod of observation. Additional, longer-term evaluationin combination with interferon-based therapy iswarranted.

46 C. Cooper et al. / Journal of Hepatology 51 (2009) 39–46
Acknowledgement
Bernard Bourgault of ViroChem Pharma is acknowl-edged for the management of this clinical study.
References
[1] Rice C. Flaviviridae: the viruses and their applications. In: FieldsBN, Knipe DM, Howley PM, editors. Field virology. Philadel-phia: Lippincott-Raven Publishers; 1996. p. 931–960.
[2] Lohmann V, Korner F, Koch J, Herian U, Theilmann L,Bartenschlager R. Replication of subgenomic hepatitis C virusRNAs in a hepatoma cell line. Science 1999;285:110–113.
[3] Bartenschlager R. Hepatitis C virus replicons: potential role fordrug development. Nat Rev Drug Discov 2002;1:911–916.
[4] De Francesco R, Tomei L, Altamura S, Summa V, Migliaccio G.Approaching a new era for hepatitis C virus therapy: inhibitors ofthe NS3-4A serine protease and the NS5B RNA-dependent RNApolymerase. Antiviral Res 2003;58:1–16.
[5] Kolykhalov AA, Mihalik K, Feinstone SM, Rice CM. Hepatitis Cvirus-encoded enzymatic activities and conserved RNA elementsin the 30 nontranslated region are essential for virus replicationin vivo. J Virol 2000;74:2046–2051.
[6] Biswal BK, Cherney MM, Wang M, Chan L, Yannopoulos CG,Bilimoria D, et al. Crystal structures of the RNA-dependent RNApolymerase genotype 2a of hepatitis C virus reveal two confor-mations and suggest mechanisms of inhibition by non-nucleosideinhibitors. J Biol Chem 2005;280:18202–18210.
[7] Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med2001;345:41–52.
[8] Yao E, Tavis JE. A general method for nested RT-PCRamplification and sequencing the complete HCV genotype 1 openreading frame. Virol J 2005;2:88.
[9] Krieger N, Lohmann V, Bartenschlager R. Enhancement ofhepatitis C virus RNA replication by cell culture-adaptivemutations. J Virol 2001;75:4614–4624.
[10] McHutchison J. STAT-C: role in HCV treatment algorithm in2008. In: Hep DART 2007.
[11] Ferenci P, Fried MW, Shiffman ML, Smith CI, Marinos G,Goncales Jr FL, et al. Predicting sustained virological responses inchronic hepatitis C patients treated with peginterferon alfa-2a (40KD)/ribavirin. J Hepatol 2005;43:425–433.
[12] Jensen DM, Morgan TR, Marcellin P, Pockros PJ, Reddy KR,Hadziyannis SJ, et al. Early identification of HCV genotype 1patients responding to 24 weeks peginterferon alpha-2a (40 kd)/ribavirin therapy. Hepatology 2006;43:954–960.
[13] Zeuzem S, Buti M, Ferenci P, Sperl J, Horsmans Y, Cianciara J,et al. Efficacy of 24 weeks treatment with peginterferon alfa-2bplus ribavirin in patients with chronic hepatitis C infected withgenotype 1 and low pretreatment viremia. J Hepatol2006;44:97–103.
[14] Sulkowski MS, Lawitz E, Schiffman ML, Muir AJ, Galler G,McCone J, et al. Final results of the IDEAL (IndividualizedDosing Efficacy versus Flat Dosing to Assess Optimal PegylatedInterferon Therapy) Phase IIIb study. J Hepatol2008;48:S370–S371.
[15] Kwo P, Lawitz E, McCone J, Schiff ER, Vierling J, Pound D,et al. Interim results from HCV SPRINT-1: RVR/EVR fromphase 2 study of boceprevir plus PegIntron (Peginterferon alpha-2b)/ribavirin in treatment naive subjects with genotype-1 CHC. JHepatol 2008;48:S372.
[16] Jacobson IM, Everson G, Gordon SC, Kauffmann RH, McNairL, Muir A, et al. Interim analysis results from a phase 2 studyof telaprevir with peginterferon alfa-2a and ribavirin in treat-ment-naiive subjects with hepatptis C. Hepatology 2007;46:315A–316A.
[17] Lawitz E, Nguyen T, Younes Z, Santoro J, Gitlin N, McEniry D,et al. Valopicitabine (NM283) plus peg-interferon in treatment-naive hepatitis C participants with HCV genotype-1 infection:HCV RNA clearance during 24 weeks of treatment. Hepatology2006;44:223A.
[18] Jacobson IM, Ghalib R, Lawitz E, Freilich B, Gordon SC,Kwo P. Early viral response and on treatment response toCPG 10101 (Actilon), in combination with pegylated inter-feron and/or ribavirin, in chronic HCV genotype 1 infectedparticipants with prior relapse response. Hepatology 2006;44:224A–225A.
[19] Nicolas O, Boivin G, St-Denis C, Bedard J. Genotypic analysis ofHCV NS5B variants from participants treated with VCH-759. JHepatol 2008;48:S317.
[20] David M, Nicolas O, Fex P, Billimoria D, L’Heureux L, Bedard J.Combination studies of VCH-916, a novel allosteric inhibitor ofHCV NS5B polymerase, with interferon-a2a. In: 15th Interna-tional Symposium on Hepatitis C Virus and Related Viruses; 2008October 5–9, 2008; San Antonio, TX, USA; 2008.