evaluation of testicular disorders richard e. freeman md mph 2013 lock haven university
TRANSCRIPT

Evaluation of Testicular Disorders
Richard E. Freeman MD MPH
2013
Lock Haven University

TESTICULAR EVALUATIONSection 1
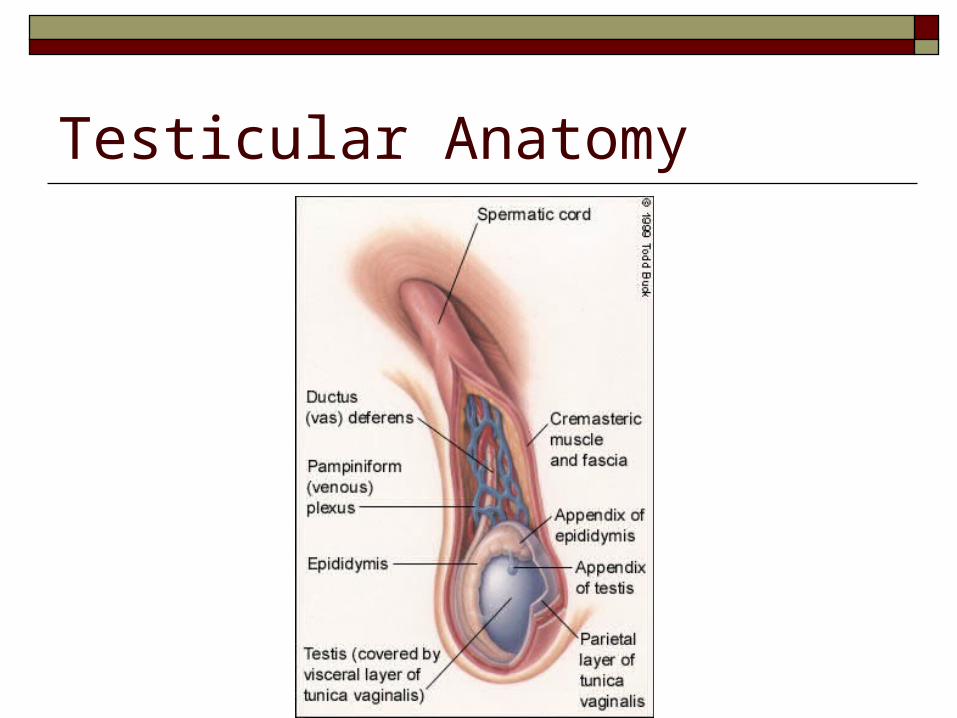
Testicular Anatomy

History Age of Patient helpful in limiting differential and determining responsible
organisms : Nature of Pain:
Severity Quality Radiation Alleviating/Aggravating factors
Sexual History Associated constitutional symptoms Associated urinary symptoms
Dysuria, frequency, hesitancy Discharge- etc Other
Activities involved with: Sports-lifting, trauma

Physical Exam Always complete GU: - be systematic Inspection- entire perineum- over, under, and beside
Skin- cysts, ulcers, erythema/rash, parasites Masses-
Palpation Inguinal- hernias, masses, nodes
Scrotum- Cord, Epididymis, Testes Penile shaft – palpate from bulbous to tip- masses tenderness ulcers Milk the shaft – discharge- Examine urethral meatus Rectal Hemorrhoids Prostate Masses Occult blood
Abdominal Exam - Complete ?? Parotids
Diagnostic Studies Urinalysis Urethral Discharge
Gram Stain Culture PCR (Chlamydia/GC)
Ultrasound Doppler Ultrasound Testicular Scan
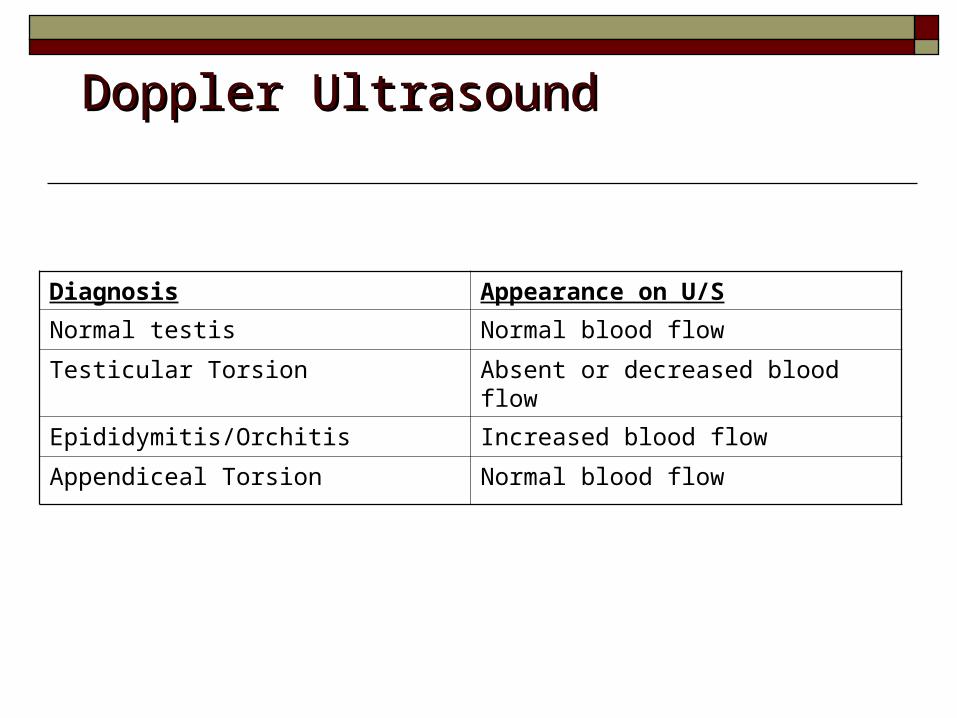
Diagnosis Appearance on U/S
Normal testis Normal blood flow
Testicular Torsion Absent or decreased blood flow
Epididymitis/Orchitis Increased blood flow
Appendiceal Torsion Normal blood flow
Doppler UltrasoundDoppler Ultrasound
THE PAINFUL TESTICALSection 2
Case 1 A ten year old male presents to your clinic
complaining of acute testicular pain while playing outside this afternoon. There is no history of trauma. He is afebrile and denies any recent symptoms of viral illness. On physical exam you note a tender right testicle that has a transverse lie in the scrotal sac. Elevating the testicle exacerbates symptoms.
TESTICULAR PAIN: Differential Diagnosis Epididymitis/Epididymo-Orchitis Orchitis Testicular Torsion Torsion Torsion of Testicular appendix

Torsion Testicle Severe pain - abrupt onset
Possibly previous history of similar episode that resolved
Absence of cremasteric reflex on affected side suggestive of torsion
High riding testicle with transverse lie of testicle- suggests torsion
Prehn’s sign- lack of pain relief with testicle elevation

Torsion Testicle Occurs due to anatomic defect in scrotal
development- Tunica Vaginalis compltely surrounds the testes and possibly the cord.
No attachment of the Tunica vaginalis to the wall of the scrotum.
Allows Testes to “swing freely “Bell-Clapper deformity” Two variations
Intravaginal Torsion Extravaginal Torsion-Exclusively in neonates

Torsion Testicle Incidence- 1:4000 males before age 25

TESTICULAR TORSION DIAGNOSIS: High degree of suspicion CLINICAL DIAGNOSIS Blood Flow:
ULTRASOUND - color doppler Radionucleotide
Torsion Testicle
REPRESENTS SURGICAL EMERGENCY
Requires immediate orchidopexy Contralateral side should be repaired at the
same time

Testicular Salvage rates < 6 hours – 90-100% salvage rate 12-24 hours – 20-50% > 24 hours – 0-10%

Torsion Testicle
Differential includes Appendiceal torsion Orchitis Epididymitis

Appendiceal Torsion Onset of Symptoms:
Subacute Age
Prepubertal Tenderness
Localized to upper pole UA
Negative Cremasteric reflex
Positive Treatment
Bed rest/scrotal evalvation Surgical
Torsion of Testicular appendix Appendix Testes
Remnant of Mullerian duct (92%) “Blue dot” sign More common in children than testicular torsion
Appendix Epididymis Remnant of Wolffian duct (23%)
Present as Subacute pain Absence of systemic/Urinary tract symptoms

Blue Dot sign
Epididymitis
DEFINITION: Inflammation, Pain, Swelling of epididymis Acute: Symptoms usually lasting < 6 weeks Chronic: Symptoms usually lasting > 6 weeks
May be acute sub-acute chronic
EPIDEMIOLOGY: Most common cause of acute scrotal pain Age: 16-30 y/o & 51-70 y/o Incidence parallels incidence of Chlamydia & GC

Epididymitis ETIOLOGY:
Retrograde infection from the urinary tract.Sexually active – Chlamydia, Gonorrhea, E.coliOlder men and children- E.coliNon-infectious – post surgery, drugs
SIGNS/SYMPTOMS:Scrotal pain- slow onset+- Dysuria, frequency, Discharge, FeverTenderness and swelling epididymis
Epididymitis Natural History/Complications
Abscess Epididymis and testicular infarction Chronic inflammation/disability

EPIDYDIMITISDiagnostic Studies
Urinalysis May reveal pyuria
Urine Culture Responsible organisms
Urethral Swab Gram Stain Culture PCR-Gonorrhea/Chlamydia
Epididymitis Treatment
< 35 y/o Ceftriaxone 250 mg IM Doxycyxline 100 BID x 14 days
> 50 y/o Treat responsible organism Ciprofloxin/Quinilones TMP/SMZ
Orchitis DEFINITION:
Inflammation or infection of the testicles may be related to epididymitis Extension to testes
Etiology: bacterial (E. coli, K. pneumoniae, P. aeruginosa,
Staph. or Strep) viral (EBV, coxsackievirus, arbovirus,
enterovirus, MUMPS VIRUS)

ORCHITIS & MUMPS Most common cause of orchitis Approximately 20% of prepubertal patients with mumps
develop orchitis. 4 out of 5 cases occur in prepubertal males(younger than 10
years). Mumps orchitis follows the development of parotitis by 4-7
days. Mumps orchitis presents unilaterally in 70% of cases (fertility
usually maintained) In 30% of cases, contralateral testicular involvement follows by 1-9
days.

ORCHITIS SIGNS & SYMPTOMS:
similar to epididymitis, hematuria, ejaculation of blood Pain, entire testes swollen- exquisitely tender Systemic- fever chills, malaise

Orchitis - Treatment GENERAL: BED REST, SCROTAL SUPPORT ANALGESICS,
ANTIEMETICs
VIRAL etiology- Supportive care
Orchitis- Treatment
BACTERIAL etiology: <35 y/o and sexually active,
antibiotic coverage for sexually transmitted pathogens (particularly gonorrhea and chlamydia)
Ceftriaxone and either doxycycline or azithromycin is appropriate.
>35 y/o with bacterial etiology require additional coverage for other
gram-negative bacteria fluoroquinolone ( not for gonorrhea) TMP-SMX
Painless scrotal massesSection 3

PAIN LESS SCROTAL MASSES Varicocele Hydrocele Hernia Testicular Tumors Spermatocele Scrotal Edema

Varicocele•Patient presents with mass of scrotum that feels like “bag of worms”
•Most commonly left sided due to drainage of L gonadal vein into the left renal vein at an acute angle and anatomic variants which cause back pressure
•Clinically benign Except in the setting of infertility
•40% of men with infertility have varicocele.
•Surgical removal may be necessary
• Why might this cause infertility?

Varicocele
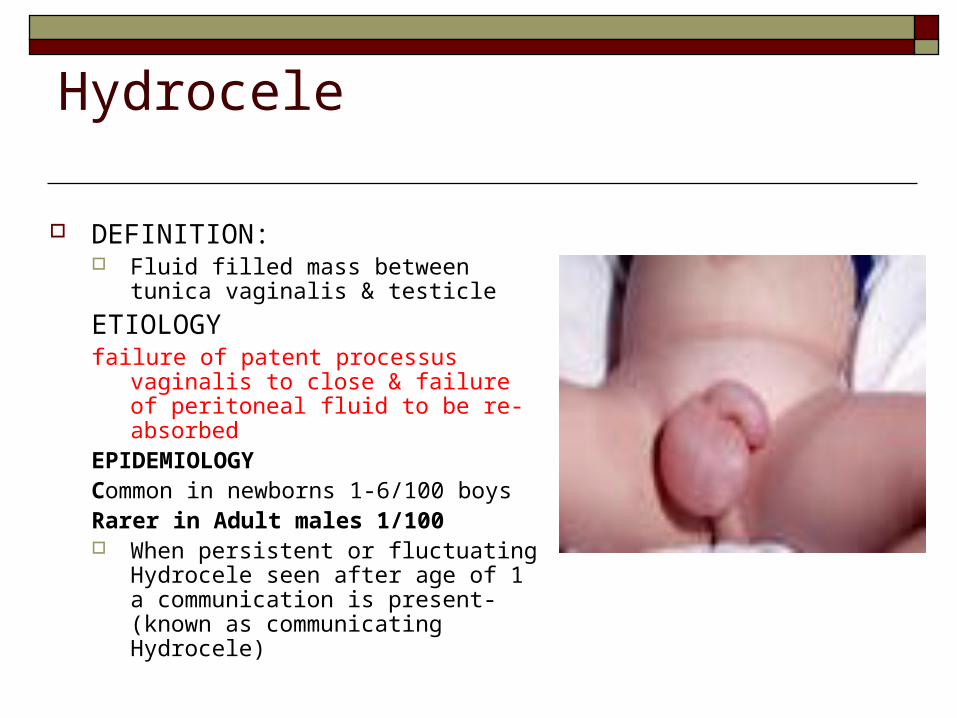
Hydrocele
DEFINITION: Fluid filled mass between tunica
vaginalis & testicle
ETIOLOGYfailure of patent processus vaginalis to
close & failure of peritoneal fluid to be re-absorbed
EPIDEMIOLOGYCommon in newborns 1-6/100 boysRarer in Adult males 1/100 When persistent or fluctuating
Hydrocele seen after age of 1 a communication is present- (known as communicating Hydrocele)

HYDROCELE RISK FACTORS Premature and low-birth-weight infants Indirect inguinal hernia Primary testicular/intrascrotal pathology Trauma Surgery Increased intra-abdominal pressure Lymphatic obstruction Ventriculoperitoneal shunt Peritoneal dialysis Ehlers-Danlos syndrome Non communicating forms may result from trauma, infection or neoplasm

Hydrocele Physical Exam
Transilluminating mass-waxes and wanes May associated with a indirect hernia Consider ultrasound due to possibility of
neoplasm causing Hydrocele Management
Expectant- watch and wait Surgical resection

Hydrocele C
NORMALCOMMUNICATING
NON-COMMUNICATING

HERNIA: DEFINITION: ETIOLOGY: EPIDEMIOLOGY:

HERNIA:RISK FACTORSBeing male.
Family history.
Certain medical conditions: cystic fibrosis
Chronic cough..
Chronic constipation. Straining during bowel movements
Excess weight: moderately to severely overweight puts extra pressure on abdomen.
Pregnancy: This can both weaken the abdominal muscles and cause increased pressure inside your abdomen.
Certain occupations: Having a job that requires standing for long periods or doing heavy physical labor increases risk of developing an inguinal hernia.
Premature birth: Infants who are born early are more likely to have inguinal hernias.
History of hernias: one inguinal hernia, it's much more likely develop another — usually on the opposite side.

Hernias: EXAM

Hernias

Hernias

Hernias

Hernias CLINICAL COURSE: NORMAL: REDUCIBLE Complications:
INCARCERATION Not easily manually reduced
STRANGULATION Surgical Emergency- herniorrhaphy Blood supply to hernial contents (omentum/intestines)
is compromised tissue death

Spermatocele
DEFINITION: Usually asymptomatic, small mass of
the epididymis Equivalent of a Berry aneurysm of the
epididymis
Benign DIAGNOSIS:
normally confirmed with ultrasound however only (definitive diagnosis is made through biopsy or aspiration returning spermatozoa- not necessary)
TREATMENT: Surgical excision reserved for chronic
pain or extensive enlargement

CRYPTORCHIDISM DEFINITION:
Undescended or“Hidden testis”
EPIDEMIOLOGY: Incidence- 0.7-1% at age 1.
ETIOLOGY: Uncertain
COMPLICATIONS: Can lead to infertility and
has a higher incidence of malignancy .
Tx- Orchiopexy

TESTICULAR TUMORS
EPIDEMIOLOGY: Incidence low: 4/100,000 Prevalence: 3.7/100,000
Most common cancer in men between ages of 15-35
Excellent prognosis with early detection

Who gets testicular cancer? Men who are more likely to get testicular cancer:
Are white Have a father or brother who had testicular cancer Have a testicle that did not come down into the scrotum
even if surgery was done to remove the testicle or bring it down
Have small testicles or testicles that aren't shaped right (most testicles are round, smooth and firm)
Have Klinefelter's syndrome

What are the signs of testicular cancer?
A hard, painless lump in the testicle (this is the most common sign)
Pain or a dull ache in the scrotum A scrotum that feels heavy or swollen Bigger or more tender breasts
Back Pain Dyspnea

Testicular Cancer
Histology: 2 groups
Nongerminal (5%) Leydig or sertoli cells
GERMINAL (95%) Seminoma, Embryonal,
tertatoma, choriocarcinoma, yolk sac tumors
Testicular Cancer Germinal tumors usually metastasize thru
lymph system except for choricocarcinoma which metastasize thru the vascular system.
TREATMENT AND PROGNOSIS varies with type of tumor. The earlier its found the better the outcome! Virtually 100% CURE if found before metastasis >80% if metastasized
chemotherapy

Testicular Self Examination Check your testicles
one at a time. Use one or both hands.
Cup your scrotum with one hand to see if there is any change.
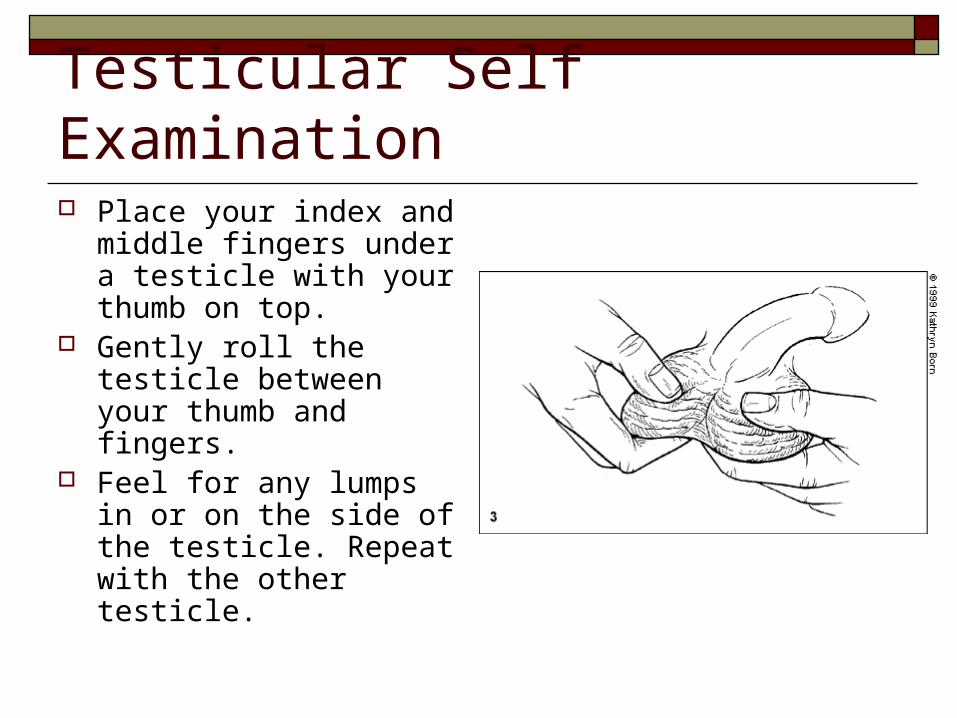
Testicular Self Examination Place your index and
middle fingers under a testicle with your thumb on top.
Gently roll the testicle between your thumb and fingers.
Feel for any lumps in or on the side of the testicle. Repeat with the other testicle.

Testicular Self Examination Feel along the
epididymis for swelling