evaluation of febrile thrombocytopenia cases in a south indian … · b. direct effect on...
TRANSCRIPT
Journal of The Association of Physicians of India ■ Vol. 66 ■ May 2018 61
Mechanism of thrombocytopenia in febrile patients1 – a. Decreased platelet production b. Direct effect on progenitor cellsc. Hemophagocytosis d. Antibody mediated destruction e. Circulating platelet destruction
In our study we have used novel platelet indices like MPV and PDW to predict the risk of outcome.
Materials and Methods
This is a prospective study of 100 continuous adult patients who were admitted during the period of January 2016 to February 2016. Already known thrombocytopenia patients with other diseases were excluded from the study. This study was approved by the hospital ethical committee and informed consent was obtained from each pat ients . Laboratory investigations like complete blood count (3 part different cell count, Impedance principle {SYSMEX} was used), l iver function test , dengue serology (IgM ELISA) were done. Blood counts were periodically monitored till resolution and discharge of patients.
Results
In our study out of 100 patients 34 patients were dengue positive and 66 were dengue negative (Tables 1, 2).
Our s tudy showed tha t about 58.88% of patients who were dengue positive had dengue specific general symptoms like (myalgia and retro orbital pain) as against 10.60% of dengue negative patients. Apart from the general constitutional symptoms Gastro intestinal symptoms (abdominal
Evaluation of Febrile Thrombocytopenia Cases in a South Indian Tertiary Care HospitalP Vishnuram1*, Kumar Natarajan2, N Karuppusamy3, Srinivasan Karthikeyan4, J Kiruthika5, A Muruganathan6
1Assistant Professor, 2Professor and HOD, Department of General Medicine, Coimbatore Medical College Hospital, 3Assistant Professor, 6Emeritus Professor, The Tamil Nadu Dr. MGR Medical University, 4Post Graduate, 5Post Graduate, Department of General Medicine, Coimbatore Medical College Hospital, Coimbatore, Tamil Nadu; *Corresponding AuthorReceived: 01.06.2016; Accepted: 08.01.2018
O R I G I N A L A R T I C L E
AbstractObjective: This study is aimed at analyzing the clinical symptomatology and hematological evaluation with an emphasis on platelet indices in relation to predicting the outcome of the febrile thrombocytopenic patients admitted in Coimbatore medical college hospital.
Methods: This is a prospective study involving 100 adult patients who presented to our hospital with fever and thrombocytopenia (platelet <1,50,000). This study excluded patients with known causes of thrombocytopenia like ITP and patients on chemotherapy etc.
Results: Out of 100 patients 34 were dengue positive, 66 were dengue negative. Dengue specific symptoms like myalgia and retro-orbital pain were present in 58.88% of dengue positive and 10.60% of dengue negative patients. Laboratory evaluation revealed sharp rise in hematocrit with fall in platelet count in both the groups more significant in dengue positive group. Bleeding manifestation and rashes were 29.4% and 26.4% in dengue positive, 12.12% and 7.57% in dengue negative group respectively. MPV was significantly lower in patients with bleeding manifestations irrespective of platelet count in both the groups. Mortality in our study was 2%.
Conclusion: MPV is an independent predictor of bleeding manifestation and poor outcome. Dengue virus may suppress the bone marrow as evidenced by alteration in MPV in addition to other mechanisms of thrombocytopenia.
Introduction
Pu r p u r a wa s r e c o g n i z e d a s a manifestation of pestilential fever
2000 years ago, 1 though purpura may be thrombocytopenic or non thrombocytopenic.
Pla te le t s are a -nuc lea ted ce l l s with c irculat ing l i fe span of 8-10 days and vital for hemostasis.2 Often physicians are perplexed of febrile thrombocytopenia with definite or indefinite etiology which influence the treatment modality. We aimed at a study of 100 adult patients with febrile thrombocytopenia with the criteria of platelet count < 1,50,000.
Causes of febrile thrombocytopenia-1
1. Infection – dengue virus, parvo virus, rubella, mumps, varicella, h e p a t i t i s , E B V, C M V, H I V, leptospirosis, malaria, rickettsial infections, gram – negative sepsis.
2. M a l i g n a n c i e s – l e u k e m i a , lymphoma
3. Others like – aplastic anemia / SLE/ HUS / TTP/ITP/DIC
Table 1: Number of dengue positive and negative cases
Male FemaleDengue +ve 24 10Dengue –ve 26 40
Table 2: Age-wise distribution
Age Dengue positive Dengue negative 12 2 3
12-40 25 4240-60 5 11> 60 2 4

Journal of The Association of Physicians of India ■ Vol. 66 ■ May 201862
0
20
40
60
80
100
120
140
160
1 4 7 10131619222528313437404346495255586164
Coun
ts in
Tho
usan
ds
Patients (Dengue negative)
Platelets
MPV
0
20
40
60
80
100
120
140
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33
Coun
ts in
thou
sand
s
Patients (Dengue positive)
Platelets
MPV
Group (MPV) Mean ± SDDengue positive 9.82 ± 0.93Dengue negative 10.37±1.13P value (t test) 0.02
Fig. 2: Comparing patient groups with mean platelet volume (MPV)
Fig. 1: Comparing patient groups with platelet count and hematocrit
Table 3: Clinical manifestations
Symptoms Dengue positive patients
Dengue Negative patients
General 32 59Dengue specific 20 7Bleeding 10 8Rashes 9 5CVS - -RS 7 16CNS 17 16GIT 28 41
Table 4: Duration for fever to subside
Days at which patient became afebrile
Dengue + ve patients
Dengue –ve patients
2-5d 24 475-10d 7 18>10d 3 1
Table 5: Platelet count among patients
Platelet Dengue + ve Dengue - ve<20000 7 520-40 9 1740-60 8 1760-80 3 1580-1 lac 3 31 – 1.5lac 4 10
Table 6: Hematocrit value among patients
HCT Dengue +ve Dengue -ve15-25 - 125-30 2 1030-35 4 2235-40 6 1940-45 13 1445-50 5 ->50 4 -Total 34 66
FIGURE-1
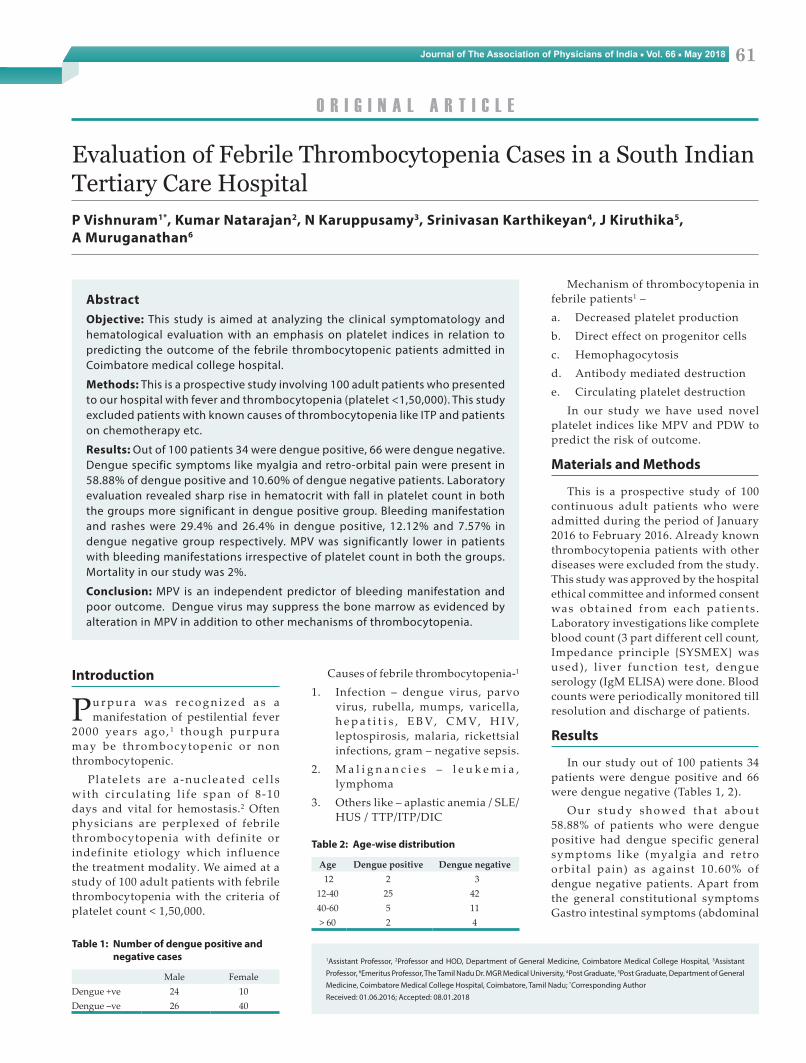
While comparing other platelet indices it showed that patients with dengue had low MPV compared to dengue negative patients and it was more important predictor of bleeding manifestation compared to platelet count. Comparison of platelet count with PDW did not show significant correlation.(fig-2)(fig-3)
Group Mean ± Std Deviation Dengue negative 34.57±8.2 Dengue positive 42.43±6.16 P value (t test) < 0.005
pain, vomiting, loose stools) were p r e d o m i n a n t , 8 2 . 3 5 % i n d e n g u e positive and 62.12% in dengue negative patients, may be influenced by outside drug intake which the patient revealed poorly. Bleeding manifestations and rashes were more common in dengue positive patients around 29.4% and 2 6 . 4 % r e s p e c t i ve l y . W h e r e a s i n dengue negative patients bleeding manifestation was seen in 12.12% and
rashes in 7.57% (Table 3).Around 70.58% of dengue positive
patients became afebrile after 2- 5 days. However 8.82 % of dengue positive patients had prolonged fever of more than 10 days. Whereas in dengue negat ive pat ients 71 .21% became afebrile after 2-5 days and 1.51 % had prolonged fever (Table 4).
Regarding platelet count 20.58% of
dengue positive patients had severe thrombocytopenia (<20,000) whereas only 7.57 % of dengue negative patients had such low platelet counts.(table-5) While comparing the platelet count with the hematocrit, our data revealed that lower the platelet count with a significant increase in the hematocrit which had significant p value (<0.005) (Table 6) (Figure 1).
While comparing other platelet indices it showed that patients with dengue had low MPV compared to dengue negative patients and it was more important predictor of bleeding manifestation compared to platelet count. Comparison of platelet count with PDW did not show significant correlation (Figures 2, 3).
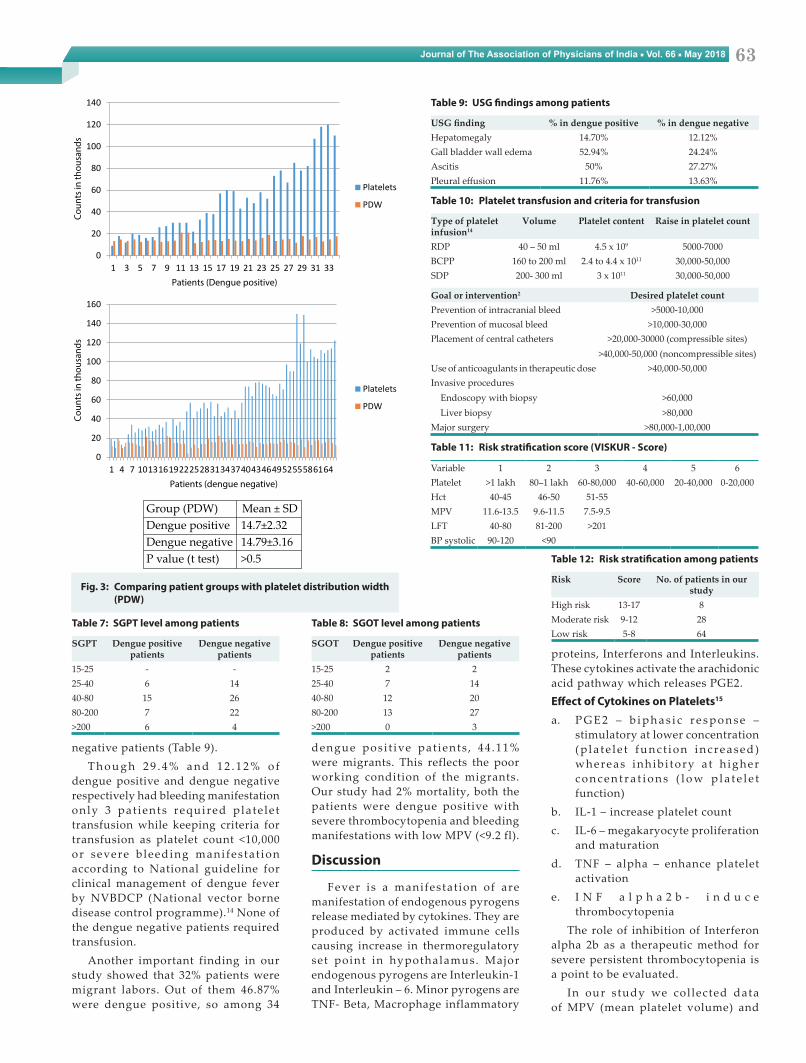
W h e n l i v e r p a r a m e t e r s w e r e obtained it showed a greater rise of SGPT compared to SGOT as like other studies (Tables 7, 8).
When USG abdomen and pelvis was done 35 out of 100 had positive findings. Gall bladder wall edema was more seen in dengue patient. 52.94 % with dengue had gall bladder wall edema as against 24.24 % of dengue
Journal of The Association of Physicians of India ■ Vol. 66 ■ May 2018 63
proteins, Interferons and Interleukins. These cytokines activate the arachidonic acid pathway which releases PGE2.Effect of Cytokines on Platelets15
a. P G E 2 – b i p h a s i c r e s p o n s e – stimulatory at lower concentration ( p l a t e l e t f u n c t i o n i n c r e a s e d ) whereas inhib i tory a t h igher c o n c e n t r a t i o n s ( l o w p l a t e l e t function)
b. IL-1 – increase platelet countc. IL-6 – megakaryocyte proliferation
and maturationd. TNF – alpha – enhance platelet
activatione. I N F a l p h a 2 b - i n d u c e
thrombocytopeniaThe role of inhibition of Interferon
alpha 2b as a therapeutic method for severe persistent thrombocytopenia is a point to be evaluated.
In our study we col lected data of MPV (mean platelet volume) and
negative patients (Table 9).T h o u g h 2 9 . 4 % a n d 1 2 . 1 2 % o f
dengue positive and dengue negative respectively had bleeding manifestation only 3 pat ients required plate le t transfusion while keeping criteria for transfusion as platelet count <10,000 or severe b leeding manifes tat ion according to National guideline for clinical management of dengue fever by NVBDCP (National vector borne disease control programme).14 None of the dengue negative patients required transfusion.
Another important finding in our study showed that 32% patients were migrant labors. Out of them 46.87% were dengue positive, so among 34
dengue posi t ive pat ients , 44 .11% were migrants. This reflects the poor working condition of the migrants. Our study had 2% mortality, both the patients were dengue positive with severe thrombocytopenia and bleeding manifestations with low MPV (<9.2 fl).
Discussion
Fever is a manifestat ion of are manifestation of endogenous pyrogens release mediated by cytokines. They are produced by activated immune cells causing increase in thermoregulatory set point in hypothalamus. Major endogenous pyrogens are Interleukin-1 and Interleukin – 6. Minor pyrogens are TNF- Beta, Macrophage inflammatory
0
20
40
60
80
100
120
140
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33
Coun
ts in
thou
sand
s
Patients (Dengue positive)
Platelets
PDW
0
20
40
60
80
100
120
140
160
1 4 7 10131619222528313437404346495255586164
Coun
ts in
thou
sand
s
Patients (dengue negative)
Platelets
PDW
Group (PDW) Mean ± SDDengue positive 14.7±2.32Dengue negative 14.79±3.16P value (t test) >0.5
Fig. 3: Comparing patient groups with platelet distribution width (PDW)
Table 10: Platelet transfusion and criteria for transfusion
Type of platelet infusion14
Volume Platelet content Raise in platelet count
RDP 40 – 50 ml 4.5 x 109 5000-7000 BCPP 160 to 200 ml 2.4 to 4.4 x 1011 30,000-50,000SDP 200- 300 ml 3 x 1011 30,000-50,000
Goal or intervention2 Desired platelet countPrevention of intracranial bleed >5000-10,000Prevention of mucosal bleed >10,000-30,000Placement of central catheters >20,000-30000 (compressible sites)
>40,000-50,000 (noncompressible sites)Use of anticoagulants in therapeutic dose >40,000-50,000Invasive procedures
Endoscopy with biopsyLiver biopsy
>60,000>80,000
Major surgery >80,000-1,00,000
Table 11: Risk stratification score (VISKUR - Score)
Variable 1 2 3 4 5 6Platelet >1 lakh 80–1 lakh 60-80,000 40-60,000 20-40,000 0-20,000Hct 40-45 46-50 51-55MPV 11.6-13.5 9.6-11.5 7.5-9.5LFT 40-80 81-200 >201BP systolic 90-120 <90
Table 7: SGPT level among patients
SGPT Dengue positive patients
Dengue negative patients
15-25 - -25-40 6 1440-80 15 2680-200 7 22>200 6 4
Table 8: SGOT level among patients
SGOT Dengue positive patients
Dengue negative patients
15-25 2 225-40 7 1440-80 12 2080-200 13 27>200 0 3
Table 9: USG findings among patients
USG finding % in dengue positive % in dengue negative Hepatomegaly 14.70% 12.12%Gall bladder wall edema 52.94% 24.24%Ascitis 50% 27.27%Pleural effusion 11.76% 13.63%
Table 12: Risk stratification among patients
Risk Score No. of patients in our study
High risk 13-17 8Moderate risk 9-12 28Low risk 5-8 64

Journal of The Association of Physicians of India ■ Vol. 66 ■ May 201864
e t i o l o g i c a l e va l u a t i o n o f f e b r i l e thrombocytopenic patients other than dengue serology may not be necessary unless warranted in specific situations. MPV is an independent predictor of bleeding manifestation and poor outcome. Dengue virus may suppress the bone marrow as evidenced by alteration in MPV in addition to other mechanisms of thrombocytopenia.
References1. Wintrobe MM. Clinical hematology. 13th ed. Philadelphia:
Lea and Febiger
2. Rodgers GP, Young NS. Bethesda handbook of clinical hematology. Philadelphia: Lippincott Williams and Wilkins; 2013; 9:422
3. Dr. Tejinder Singh, Atlas and Text of Hematology. 3rd ed:56-57
4. Handbook of clinical management of dengue. WHO 2012:1.3;16
5. Lewis SM, Bain BJ, Bates I, Dacie JV, Dacie JV. Dacie and Lewis practical haematology. Philadelphia: Churchill Livingstone/Elsevier; 2006.
6. Kottke ME, Bavis B. Laboratory Hemtological Clinical Practice 1st ed. 2012.
7. Vincent F.la russa, Innis BL. Baillieres’s Clinical Hematology 1995; 8:249-270.
8. Bashir AB, Saeed OK, Mohammed BA, Ageep AK, Role of platelet indices in patients with dengue infection in red sea state sudan. International J science and Research 2011.
9. Katti TV, et al, How far are the platelet indices mirror image of mechanism of thrombocytopenia mystery still remains?. International J of Advance in Medicine 2014; 1;200-205.
10. Deshwal R, et al. Clinical and laboratory profile of dengue fever. J Association of Physicians of India 2015; 63:30-33.
11. Guidelines for the use of platelet transfusions. British J of Haematology 2003; 122:10–23.
12. Xu, Rui-Long et al. Platelet Volume Indices Have Low Diagnostic Efficiency for Predicting Bone Marrow Failure in Thrombocytopenic Patients. Experimental and Therapeutic Medicine 5.1 (2013): 209–214. PMC. Web. 1 June 2016.
13. Noris P, Klersy C, Gresele P, et al. Platelet size for distinguishing between inherited thrombocytopenias and immune thrombocytopenia: a multicentric, real life study. British Journal of Haematology 2013; 162:112-119. doi:10.1111/bjh.12349.
14. NVBDCP. National guidelines for managent of dengue fever. http://nvbdcp.gov.in/Doc/Dengue-National-Guidelines-2014.pdf
15. Norol F, Vitrat N, Cramer E, Guichard J, Burstein SA, Vainchenker W, Debili N. Effects of Cytokines on Platelet Production From Blood and Marrow CD34+ Cells. Blood 1998; 91.
16. Kshirsagar P, Chauhan S, Samel D. Towards Developing a Scoring System for Febrile Thrombocytopenia. Journal of The Association of Physicians of India 2016; 64.
PDW(platelet distribution width). MPV indicates the average volume of platelets, calculated by platelecrit divided by number of platelets6 and it is a surrogate marker of bone marrow activity with normal value of 8-12 fl whereas PDW shows how uniform the platelets are in size and it is a measure of platelet activation with normal value of 9-14fl.4 Low MPV a more important predictor of bleeding manifestation.9
In dengue, development of IgM antibody coincides with disappearance of viraemia3. Detection of IgM at 3-5 days of fever is seen in 50% of patients whereas 95-98% of patients will be positive for IgM antibody during 6-10 days of fever. It can persist for about for about 3 months. At 9-10 days IgG starts appearing3
Platelet transfusion for treatment of thrombocytopenia may be deferred till platelet count is <10,000. In our study only 3 patients required transfusion all had platelet count of <10,000 and severe hemorrhagic manifestations (Table 10). Prophylactic platelet transfusion is avoided to prevent allo-immunisation and platelet refractoriness11. If needed Platelet transfusion can be done either using Random donor platelets (RDP), Buffy coat pooled platelets (BCPP), Single donor apheresis (SDP).The standard dosage is 5- 6 units of RDP or one unit of BCPP or SDP.14 Packed cell transfusion/Fresh frozen plasma can also be used along with platelet transfusion in severe bleeding with coagulopathy. However whole blood transfusion has no role.14
Analyzing our study we found out that patients with dengue had more dengue specific symptoms 58.88% compared to others (10.60% in dengue negative) and also had more bleeding mani fes ta t ion (29 .4%) . Moreover severe thrombocytopenia was more common in dengue (20.58%) compared to non dengue patients (7.57%). While considering HCT, hemoconcentration
was more in dengue patients (mean HCT 42.43±6.16) and low platelet count had higher HCT with p value<0.005 which is significant.
The mean MPV in dengue was 9.82 ± 0.93 whereas in dengue negative it was 10.37±1.13 with a p value of <0.02 which is significant. Patients with low MPV had higher risk of bleeding.9 Thus it can be used an important predictor for risk of bleeding. PDW results didn’t show any significance in dengue positive and dengue negative patients with or without bleeding manifestation.
U S G a l s o r e v e a l e d t h a t g a l l bladder wall edema and ascites was more common in dengue (52 .94% and 50% respectively) compared to dengue negative (24.24 % and 27.27% respectively).
There have been studies to show that dengue causes bone marrow suppression.7 Low MPV is an indicator for bone marrow activity.12,13 Our study showed relationship between low MPV and very low platelet, thus proving that dengue virus directly suppress bone marrow.6
Thus with our data we formulated a risk stratification scoring system (VISKUR- named after the first two authors) (Tables 11, 12).
Same journal had published clinical scoring system earlier which was a useful guideline. Applying within our clinic-laboratory scoring system along with the previous scoring system may predict the outcome of disease on admission. Apart from the study, in our clinical experience we have seen two patients of AML with positive dengue serology. The relationship between dengue and leukemia needs further studies.Conclusion
I n o u r s t u d y o u t o f 1 0 0 thrombocytopenic patients only 3 received platelet transfusion. Extensive

Journal of The Association of Physicians of India ■ Vol. 66 ■ May 2018 65