evaluation of a novel blood pressure scoring method and its association with clinical response in...
TRANSCRIPT

PHASE I STUDIES
Evaluation of a novel blood pressure scoring methodand its association with clinical response in cancer patients treatedwith anti-vascular endothelial growth factor therapy
Mehmet Asim Bilen & Jean-Bernard Durand & Lacey McQuinn & Kenneth R. Hess &Siqing Fu & Gerald S. Falchook & David S. Hong & Jennifer J. Wheler & Rabih Said &
Michael S. Ewer & Razelle Kurzrock & Aung Naing
Received: 19 February 2014 /Accepted: 15 April 2014# Springer Science+Business Media New York 2014
Summary Background The purposes of this study were toestablish a novel blood pressure (BP) scoring method and tocorrelate it with clinical response in advanced cancer patientstreated with anti-vascular endothelial growth factor (VEGF)therapies. Methods We retrospectively analyzed data for 368patients from 23 clinical trials that included at least one anti-VEGF agent. We determined BP scores using the traditionalCommon Terminology Criteria for Adverse Events (CTCAE)version 4.0 and our novel method that considers both BPreadings and number of anti-hypertensive medications the pa-tient received. BP scores were categorized at baseline and fourmonths. Logistic regression analysis correlated elevated scores
with clinical response. Agreement between the CTCAE and thenew method was assessed. Results Under the new BP scoringmethod, partial response rates were 20 % in patients with anelevated score at four months versus 6 % in patients withoutelevated score (P<0.001). When adjusted for tumor type, age,sex, history of anti-VEGF treatment, and number of anti-VEGFtreatments, elevated BP under the new scoring method had anodds ratio of 3.8 (95 % confidence interval [CI]: 1.8, 8.2;P<0.001). The kappa statistic for agreement between theCTCAE and new scoring methods was 0.57 (95 % CI: 0.47,0.67; P<0.001), indicating significant concordance.ConclusionUsing the novel scoring method, an increase in BP scores was amarker for favorable clinical response in patients who receivedanti-VEGF treatment. This new method ultimately providesinformation with regard to clinical tumor response over andabove that provided by the CTCAE scoring method.
Keywords Anti-VEGF therapy . Hypertension . Toxicity .
Clinical response . Scoringmethod
Introduction
Angiogenesis, the formation of new blood vessels, plays apivotal role in cancer progression [1, 2]. Several major signal-ing pathways play a role in tumor-induced angiogenesis, andof the molecules involved, vascular endothelial growth factor(VEGF) is the most common therapy target [3]. Severalmonoclonal antibodies and small molecules have been devel-oped to block VEGF [1, 3]. These anti-VEGF drugs arewidely used in treatment of various malignancies [4–6].
Hypertension is one of the most common side effectsassociated with anti VEGF agents [7]. Several studies havereported an increased incidence of hypertension with different
M. A. BilenDivision of CancerMedicine, The University of TexasMDAndersonCancer Center, Houston, TX, USA
J.<B. Durand :M. S. EwerDepartment of Cardiology, The University of Texas MD AndersonCancer Center, Houston, TX, USA
L. McQuinn : S. Fu :G. S. Falchook :D. S. Hong : J. J. Wheler :A. Naing (*)Department of Investigational Cancer Therapeutics, The Universityof Texas MD Anderson Cancer Center, 1515 Holcombe Blvd,Box 455, Houston, TX 77030, USAe-mail: [email protected]
K. R. HessDepartment of Biostatistics, The University of Texas MD AndersonCancer Center, Houston, TX, USA
R. SaidDivision of Internal Medicine-Oncology, The University of TexasHealth Science Center, Houston, TX, USA
R. KurzrockDivision of Hematology-Oncology, UC San Diego Moores CancerCenter, La Jolla, CA, USA
Invest New DrugsDOI 10.1007/s10637-014-0104-7

anti-VEGF agents [8–10]. Possible mechanisms, includingon-target and off-target effects, have been implicated in thepathogenesis of anti-VEGF therapy-induced hypertension;however, the exact mechanism has yet to be identified [7,11]. Interestingly, anti-VEGF therapy-induced hypertensionhas been suggested as not only a side effect of the treatmentbut also a biomarker of clinical tumor response; patients withhypertension had improved outcome [12–14]. However, therelationship between hypertension and response has not beenwell established.
There are three widely used grading methods for hyperten-sion: the National Cancer Institute’s Common TerminologyCriteria for Adverse Events (CTCAE) [15], which mainlyreflect therapeutic interventions, and the European Societyof Hypertension (ESH) [16] and Joint National Committee(JNC) [17] guidelines, which both utilize BP measurements.The disadvantage of these single-parameter methods is illus-trated by the following example. Per CTCAE version 4.0, theadverse event of hypertension is defined as grade 3 if apatient’s BP is greater than 160/100 mmHg or the patient isreceiving intensifiedmedical intervention (more than one drugor more intensive therapy than was indicated before the clin-ical trial) [15]. Thus, a patient taking two BP medicationswould be considered to have grade 3 toxicity whether theBP was 120/80 or 160/100 mmHg. In other words, theCTCAE method does not distinguish whether BP is wellcontrolled. To address this problem, we developed a multi-parameter-based BP scoring method. This novel method con-siders both BP measurements and the use of anti-hypertensivemedication to control BP.
The primary objective of this study was to investigate thevalidity of the new BP scoring method. Additionally, weretrospectively examined the correlation of BP score to clin-ical tumor response in patients with treated with anti-VEGFtherapy.
Materials and methods
Study design
We conducted a retrospective chart review of 368 patientswith advanced cancers who had been treated on 23 differentphase I clinical trials from January 1, 2006, until February 1,2012. All the clinical trials included a regimen that consistedof at least one anti-VEGF agent. This data review and analysiswere approved by the Institutional Review Board.
Treatment of hypertension
Treatment of elevated BP (systolic blood pressure[SBP]>140 mmHg) was managed by increasing the dose ofone anti-hypertensive agent to the maximum tolerated dose; if
the BP was still elevated, a second agent was added and esca-lated to its maximum dose. Diuretics were not typically utilizedbecause of concern for potential renal dysfunction.
Hypertension scoring method
We developed a novel multi-parameter-based BP scoringmethod to independently capture two hypertension-relatedparameters: BP measurement and number of anti-hypertensive medications being taken to control blood pres-sure. In this new scoring method, the mean SBP and meandiastolic blood pressure (DBP) are scored separately, and thehigher of these is added to a score for BP medication to equalthe total BP score (Table 1). For example, if a patient had anaverage mean SBP of 145 and a DBP of 95 and was receivingtwo anti-hypertensive medications (no diuretics), the scorewould be 4 (1+3).
The baseline BP was defined as the mean of the last threeBP measurements before the initiation of the anti-VEGF clin-ical trial. The 4-month BP was defined as the mean of all BPreadings recorded from the first day until the last day oftreatment since we are interested in durable response. The 4-month score was compared to the baseline score and catego-rized as: 1) elevated or 2) decreased or stable. BP was alsograded using CTCAE version 4.0. To validate our novelscoring method, we compared the findings for our scoringmethod and for the CTCAE.
Clinical tumor response
Clinical tumor response was determined by ResponseEvaluation Criteria in Solid Tumors (RECIST) 1.0 accordingto the patient’s medical record [18]. Patients underwentrestaging at the end of two cycles of anti-VEGF treatment(6–8 weeks), but we opted for a 4-month follow-up period toallow inclusion of more BP readings in our comparison ofscoring methods and to enable assessment of more persistentstable disease.
Statistical analysis
Descriptive statistics were used to summarize the patients’characteristics: demographic measures (age, sex), tumor type,history of anti-VEGF therapy, and clinical response.
To determine the association of elevated BP and clinicaltumor response four months after initiation of therapy, sepa-rate univariate logistic regression models for the novel scoringmethod, and the CTCAE method were performed to estimateodds ratios (ORs) and 95 % confidence intervals (CIs).Multivariate logistic regression models were also performedto adjust for the potential confounders of age, sex, tumor type,history of anti-VEGF treatment, and number of anti-VEGFagents in a trial.
Invest New Drugs

To determine whether the new scoring method was con-cordant with the CTCAE method, a kappa statistic was calcu-lated for assessing the level of agreement beyond chance.
Results
Patient demographics
A total of 368 patients were included in this data review. Theircharacteristics are shown in Table 2. Patient age ranged from
12 to 89 years, with a median of 57 years. The most commontumor type was gastrointestinal (29.1 %). Prior use of anti-VEGF therapy before our Phase I trials was recorded in20.9 % of patients (N=77). Twelve percent of these patients(N=45) had participated in a trial that included two or moreanti-VEGF agents, and 9.0% of patients (N=33) achieved PR.
Findings using the new BP scoring method
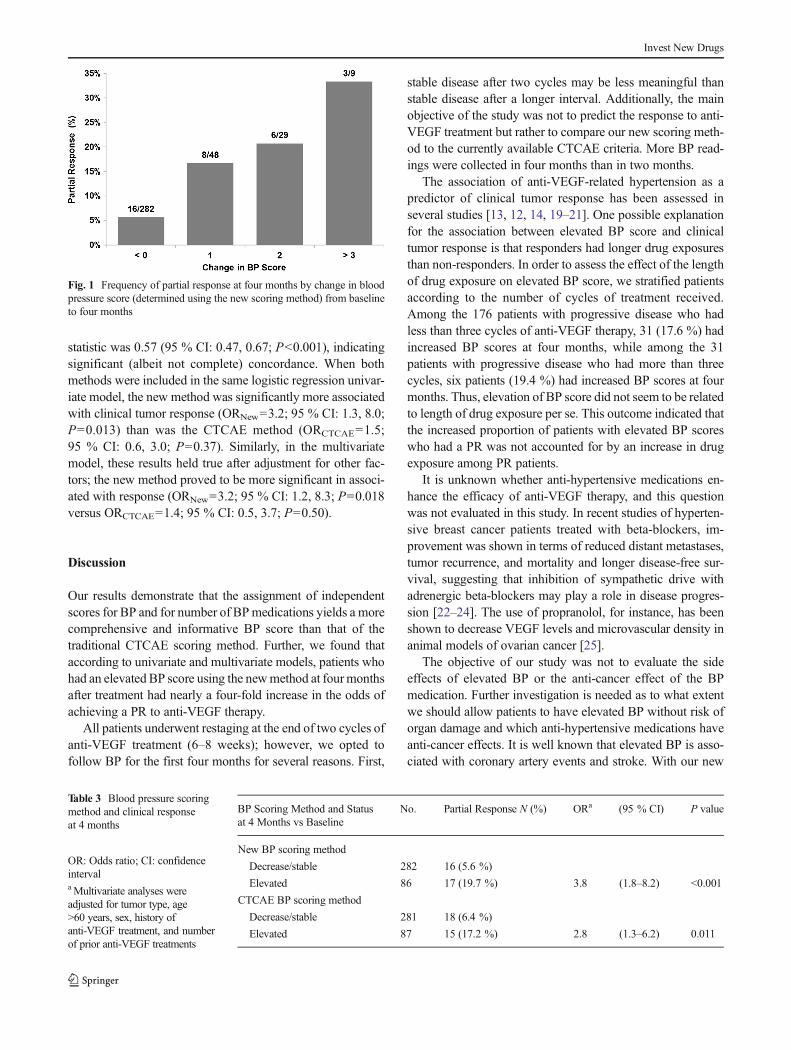
At four months after receiving anti-VEGF therapy, 23 % ofpatients (86/368) had elevated BP based on the new BPscoring method. There was a 19.7 % PR rate (17/86) inpatients with elevated BP at four months, versus a 5.6 % PRrate (16/282) in patients without elevated BP (Fig. 1; Table 3).In the univariate model, the OR for patients who had elevatedBP at four months based on the newmethodwas 4.1 (95%CI:2.0, 8.5; P<0.001), suggesting they were four times morelikely to have a PR than were patients with stable or decreasedBP. When adjusted for tumor type, age (>60 years), sex,history of anti-VEGF treatment, and number of anti-VEGFtreatments, the OR was 3.8 (95 % CI: 1.8, 8.2; P<0.001)(Table 3).
Findings using the CTCAE BP scoring method
Based on the CTCAE scoring method, 24 % of patients (87/368) had elevated BP at four months. There was a 17.2 % PRrate (15/87) in patients with elevated BP based on the CTCAEmethod at four months, versus a 6.4 % PR rate (18/281) inpatients without elevated BP (Table 3). In the univariatemodel, the OR was 3.0 (95 % CI: 1.5, 6.3; P=0.004), sug-gesting that patients with elevated BP according to CTCAEcriteria were three times more likely to achieve PR at fourmonths than were those without elevated BP. When adjustedin the multivariate model for tumor type, age (>60 years), sex,history of anti-VEGF treatment, and number of anti-VEGFtreatments, the OR was 2.8 (95 % CI: 1.3, 6.2; P=0.011)(Table 3).
Comparison of CTCAE and new method
We assessed agreement on elevated BP between the CTCAEscoring method and the new scoring method. The kappa
Table 1 Novel hypertension scoring method
Total Score = Higher Score for Mean SBP or Mean DBPa + Score for BP Medication
SBP (mm Hg) DBP (mm Hg) 0=No medication
0=SBP<140 0=DBP<90 1=One medication
1=SBP 140–159 1=DBP 90–99 2=Increasing dose of same medication or adding diuretics
2=SBP 160–179 2=DBP 100–109 3=Two medications other than diuretics
3=SBP≥180 3=DBP≥110 4=Three or more medications
a Either mean systolic blood pressure (SBP) or mean diastolic blood pressure (DBP) is scored, whichever would result in a higher score (0–3)
Table 2 Characteristics of patients
Characteristic No. %
Age, years
<60 218 59.2 %
≥60 150 40.8 %
Median (range) 57 (12–89)
Sex
Female 170 46.2 %
Male 198 53.8 %
Tumor type
Gastrointestinal 107 29.1 %
Endocrine 62 16.8 %
Thoracic 54 14.7 %
Genitourinary 41 11.1 %
Gynecologic 30 8.2 %
Melanoma 22 5.9 %
Breast 20 5.4 %
Othera 32 8.7 %
History of anti-VEGF therapy
Yes 77 20.9 %
No 291 79.1 %
≥2 previous anti-VEGF regimens
Yes 45 12.2 %
No 323 87.8 %
Tumor response
PR 33 9.0 %
aOther tumor types were squamous or basal cell carcinoma (9), eye andorbit (3), sarcoma (11), neuroendocrine (2), hematological (1), and un-known primary (6)
Invest New Drugs
statistic was 0.57 (95 % CI: 0.47, 0.67; P<0.001), indicatingsignificant (albeit not complete) concordance. When bothmethods were included in the same logistic regression univar-iate model, the new method was significantly more associatedwith clinical tumor response (ORNew=3.2; 95 % CI: 1.3, 8.0;P=0.013) than was the CTCAE method (ORCTCAE=1.5;95 % CI: 0.6, 3.0; P=0.37). Similarly, in the multivariatemodel, these results held true after adjustment for other fac-tors; the new method proved to be more significant in associ-ated with response (ORNew=3.2; 95 % CI: 1.2, 8.3; P=0.018versus ORCTCAE=1.4; 95 % CI: 0.5, 3.7; P=0.50).
Discussion
Our results demonstrate that the assignment of independentscores for BP and for number of BPmedications yields a morecomprehensive and informative BP score than that of thetraditional CTCAE scoring method. Further, we found thataccording to univariate and multivariate models, patients whohad an elevated BP score using the newmethod at fourmonthsafter treatment had nearly a four-fold increase in the odds ofachieving a PR to anti-VEGF therapy.
All patients underwent restaging at the end of two cycles ofanti-VEGF treatment (6–8 weeks); however, we opted tofollow BP for the first four months for several reasons. First,
stable disease after two cycles may be less meaningful thanstable disease after a longer interval. Additionally, the mainobjective of the study was not to predict the response to anti-VEGF treatment but rather to compare our new scoring meth-od to the currently available CTCAE criteria. More BP read-ings were collected in four months than in two months.
The association of anti-VEGF-related hypertension as apredictor of clinical tumor response has been assessed inseveral studies [13, 12, 14, 19–21]. One possible explanationfor the association between elevated BP score and clinicaltumor response is that responders had longer drug exposuresthan non-responders. In order to assess the effect of the lengthof drug exposure on elevated BP score, we stratified patientsaccording to the number of cycles of treatment received.Among the 176 patients with progressive disease who hadless than three cycles of anti-VEGF therapy, 31 (17.6 %) hadincreased BP scores at four months, while among the 31patients with progressive disease who had more than threecycles, six patients (19.4 %) had increased BP scores at fourmonths. Thus, elevation of BP score did not seem to be relatedto length of drug exposure per se. This outcome indicated thatthe increased proportion of patients with elevated BP scoreswho had a PR was not accounted for by an increase in drugexposure among PR patients.
It is unknown whether anti-hypertensive medications en-hance the efficacy of anti-VEGF therapy, and this questionwas not evaluated in this study. In recent studies of hyperten-sive breast cancer patients treated with beta-blockers, im-provement was shown in terms of reduced distant metastases,tumor recurrence, and mortality and longer disease-free sur-vival, suggesting that inhibition of sympathetic drive withadrenergic beta-blockers may play a role in disease progres-sion [22–24]. The use of propranolol, for instance, has beenshown to decrease VEGF levels and microvascular density inanimal models of ovarian cancer [25].
The objective of our study was not to evaluate the sideeffects of elevated BP or the anti-cancer effect of the BPmedication. Further investigation is needed as to what extentwe should allow patients to have elevated BP without risk oforgan damage and which anti-hypertensive medications haveanti-cancer effects. It is well known that elevated BP is asso-ciated with coronary artery events and stroke. With our new
Fig. 1 Frequency of partial response at four months by change in bloodpressure score (determined using the new scoring method) from baselineto four months
Table 3 Blood pressure scoringmethod and clinical responseat 4 months
OR: Odds ratio; CI: confidenceintervalaMultivariate analyses wereadjusted for tumor type, age>60 years, sex, history ofanti-VEGF treatment, and numberof prior anti-VEGF treatments
BP Scoring Method and Statusat 4 Months vs Baseline
No. Partial Response N (%) ORa (95 % CI) P value
New BP scoring method
Decrease/stable 282 16 (5.6 %)
Elevated 86 17 (19.7 %) 3.8 (1.8–8.2) <0.001
CTCAE BP scoring method
Decrease/stable 281 18 (6.4 %)
Elevated 87 15 (17.2 %) 2.8 (1.3–6.2) 0.011
Invest New Drugs

scoring method, early elevation of BP score at the 4-monthinterval had several clinical implications. Treatment with ad-ditional anti-hypertensive therapy to lower BP did not reducethe efficacy of Phase I drugs. In fact, overcoming the seriousadverse event (hypertension) allowed our patients to continueaggressive anti-cancer therapy rather than being removedfrom the clinical study, and so rendered some indirect benefitin terms of anti-cancer effect. Additionally, prehypertension isa revision of the definition of normal or borderline hyperten-sion. A new category was added to the Seventh Report of theJoint National Committee on Prevention, Detection,Evaluation, and treatment of High Blood Pressure (JNC-7)[26]. Treatment of the prehypertension patient prepared toundergo chemotherapy is especially challenging given thatcancer patients have poor oral intake, are anorexic and donot usually tolerate first line therapy for hypertension [27].The current recommendations of lifestyle modifications aresuited in some cancer patients such as reduced salt intake,cessation of smoking, the DASH diet and exercise [27].
The novel scoring method used in this study incorporatesmore information than the scoring methods in current use.Returning to the example above, using the CTCAE method,patients taking two medications would be considered to havegrade 3 toxicity regardless of their BP measurements.However, in our new scoring method, the patient with a meanBP of 120/80 mmHg would be given a BP score of 3 (0+3),while the patient with a mean BP of 160/100 mmHg would begiven a score of 5 (2+3). Although both patients are takingtwo BP medications, Patient A’s BP is well controlled butPatient B’s BP is not, suggesting that Patient B is morehypertensive than Patient A. Giving these patients differentscores could better predict differences in clinical response.
Indeed, we found that this new method ultimately providesinformation with regard to clinical tumor response over andabove that provided by the CTCAE scoring method. Ourmethod had a better association with clinical response, dem-onstrating 14 % PR, versus the 7 % PR rate for CTCAE. Ourkappa statistic analysis suggested that there was significantbut not complete concordance between the two methods. Inboth univariate and multivariate logistic regression models,the new scoring method was significantly more associatedwith clinical tumor response than was the CTCAE method.Such results indicate that our method was strongly associatedwith response even when controlling for the association be-tween the CTCAE method and clinical tumor response. Theimpact of hypertension on PFS and OSwas not analyzed sincethe heterogeneity of patients and treatment characteristics wasthe major limitation for this.
In conclusion, we found an association between elevatedBP and clinical response in patients treated with anti-VEGFtherapy. The implementation of a novel BP scoring methodthat incorporates parameters of both BP measurement and BPmedication use provided more value than the CTCAEmethod
in determining the clinical tumor response to anti-VEGFtherapy. The results need to be validated in a prospectivemulti-center clinical trial.
Acknowledgments We acknowledge Sunita Patterson for scientificediting of the manuscript.
Disclosures The authors have declared no conflicts of interest.
References
1. Ichihara E, Kiura K, Tanimoto M (2011) Targeting angiogenesis incancer therapy. Acta Med Okayama 65(6):353–362
2. Folkman J (2006) Antiangiogenesis in cancer therapy–endostatin andits mechanisms of action. Exp Cell Res 312(5):594–607. doi:10.1016/j.yexcr.2005.11.015
3. Linkous AG, Yazlovitskaya EM (2012) Novel therapeuticapproaches for targeting tumor angiogenesis. Anticancer Res 32(1):1–12
4. Kabbinavar F, Hurwitz HI, Fehrenbacher L, Meropol NJ, NovotnyWF, Lieberman G, Griffing S, Bergsland E (2003) Phase II, random-ized trial comparing bevacizumab plus fluorouracil (FU)/leucovorin(LV) with FU/LValone in patients with metastatic colorectal cancer. JClin Oncol 21(1):60–65
5. Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Siebels M,Negrier S, Chevreau C, Solska E, Desai AA, Rolland F, Demkow T,Hutson TE, Gore M, Freeman S, Schwartz B, Shan M, Simantov R,Bukowski RM (2007) Sorafenib in advanced clear-cell renal-cellcarcinoma. N Engl J Med 356(2):125–134. doi:10.1056/NEJMoa060655
6. Motzer RJ, Hutson TE, Tomczak P, MichaelsonMD, Bukowski RM,Rixe O, Oudard S, Negrier S, Szczylik C, Kim ST, Chen I, BycottPW, Baum CM, Figlin RA (2007) Sunitinib versus interferon alfa inmetastatic renal-cell carcinoma. N Engl J Med 356(2):115–124. doi:10.1056/NEJMoa065044
7. Chen HX, Cleck JN (2009) Adverse effects of anticancer agents thattarget the VEGF pathway. Nat Rev Clin Oncol 6(8):465–477. doi:10.1038/nrclinonc.2009.94
8. Wu S, Chen JJ, Kudelka A, Lu J, Zhu X (2008) Incidence and risk ofhypertension with sorafenib in patients with cancer: a systematicreview and meta-analysis. Lancet Oncol 9(2):117–123. doi:10.1016/S1470-2045(08)70003-2
9. Le Tourneau C, Raymond E, Faivre S (2007) Sunitinib: a noveltyrosine kinase inhibitor. A brief review of its therapeutic potentialin the treatment of renal carcinoma and gastrointestinal stromaltumors (GIST). Ther Clin Risk Manag 3(2):341–348
10. Bergsland E, Dickler MN (2004) Maximizing the potential ofbevacizumab in cancer treatment. Oncologist 9(Suppl 1):36–42
11. Sunshine SB, Dallabrida SM, Durand E, Ismail NS, Bazinet L,Birsner AE, Sohn R, Ikeda S, Pu WT, Kulke MH, Javaherian K,Zurakowski D, Folkman JM, Rupnick M (2012) Endostatin lowersblood pressure via nitric oxide and prevents hypertension associatedwith VEGF inhibition. Proc Natl Acad Sci U S A 109(28):11306–11311. doi:10.1073/pnas.1203275109
12. Scartozzi M, Galizia E, Chiorrini S, Giampieri R, Berardi R,Pierantoni C, Cascinu S (2009) Arterial hypertension correlates withclinical outcome in colorectal cancer patients treated with first-linebevacizumab. Ann Oncol 20(2):227–230. doi:10.1093/annonc/mdn637
13. De Stefano A, Carlomagno C, Pepe S, Bianco R, De Placido S (2011)Bevacizumab-related arterial hypertension as a predictive marker in
Invest New Drugs

metastatic colorectal cancer patients. Cancer Chemother Pharmacol68(5):1207–1213. doi:10.1007/s00280-011-1604-1
14. Rini BI, Cohen DP, Lu DR, Chen I, Hariharan S, Gore ME, Figlin RA,BaumMS, Motzer RJ (2011) Hypertension as a biomarker of efficacyin patients with metastatic renal cell carcinoma treated with sunitinib. JNatl Cancer Inst 103(9):763–773. doi:10.1093/jnci/djr128
15. Institute NC (2009) Common terminology criteria for adverse eventsv4.0 In Edition 2009
16. Cifkova R, Erdine S, Fagard R, Farsang C, Heagerty AM, KiowskiW, Kjeldsen S, Luscher T, Mallion JM, Mancia G, Poulter N, RahnKH, Rodicio JL, Ruilope LM, van Zwieten P, Waeber B,Williams B,Zanchetti A (2003) Practice guidelines for primary care physicians:2003 ESH/ESC hypertension guidelines. J Hypertens 21(10):1779–1786. doi:10.1097/01.hjh.0000084773.37215.1b
17. CuddyML (2005) Treatment of hypertension: guidelines from JNC 7(the seventh report of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High Blood Pressure 1). JPract Nurs 55(4):17–21, quiz 22–13
18. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS,Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT,Christian MC, Gwyther SG (2000) New guidelines to evaluate theresponse to treatment in solid tumors. European Organization forResearch and Treatment of Cancer, National Cancer Institute of theUnited States, National Cancer Institute of Canada. J Natl Cancer Inst92(3):205–216
19. Mir O, Coriat R, Cabanes L, Ropert S, Billemont B, Alexandre J,Durand JP, Treluyer JM, Knebelmann B, Goldwasser F (2011) Anobservational study of bevacizumab-induced hypertension as a clin-ical biomarker of antitumor activity. Oncologist 16(9):1325–1332.doi:10.1634/theoncologist.2010-0002
20. George S, Reichardt P, Lechner T, Li S, Cohen DP, Demetri GD(2012) Hypertension as a potential biomarker of efficacy in patientswith gastrointestinal stromal tumor treated with sunitinib. Ann Oncol23(12):3180–3187. doi:10.1093/annonc/mds179
21. Gallagher DJ, Al-Ahmadie H, Ostrovnaya I, Gerst SR, Regazzi A,Garcia-Grossman I, Riches J, Gounder SK, Flaherty AM, Trout A,
Milowsky MI, Bajorin DF (2011) Sunitinib in urothelial cancer:clinical, pharmacokinetic, and immunohistochemical study of pre-dictors of response. Eur Urol 60(2):344–349. doi:10.1016/j.eururo.2011.05.034
22. Powe DG, Voss MJ, Zanker KS, Habashy HO, Green AR, Ellis IO,Entschladen F (2010) Beta-blocker drug therapy reduces secondarycancer formation in breast cancer and improves cancer specificsurvival. Oncotarget 1(7):628–638
23. Powe DG, Entschladen F (2011) Targeted therapies: using beta-blockers to inhibit breast cancer progression. Nat Rev Clin Oncol8(9):511–512. doi:10.1038/nrclinonc.2011.123
24. Melhem-Bertrandt A, Chavez-Macgregor M, Lei X, Brown EN, LeeRT, Meric-Bernstam F, Sood AK, Conzen SD, Hortobagyi GN,Gonzalez-Angulo AM (2011) Beta-blocker use is associated with im-proved relapse-free survival in patients with triple-negative breast can-cer. J Clin Oncol 29(19):2645–2652. doi:10.1200/JCO.2010.33.4441
25. Thaker PH, Han LY, Kamat AA, Arevalo JM, Takahashi R, Lu C,Jennings NB, Armaiz-Pena G, Bankson JA, Ravoori M,Merritt WM,Lin YG, Mangala LS, Kim TJ, Coleman RL, Landen CN, LiY, Felix E, Sanguino AM, Newman RA, Lloyd M, GershensonDM, Kundra V, Lopez-Berestein G, Lutgendorf SK, Cole SW, SoodAK (2006) Chronic stress promotes tumor growth and angio-genesis in a mouse model of ovarian carcinoma. Nat Med12(8):939–944
26. ChobanianAV, Bakris GL, BlackHR, CushmanWC,Green LA, IzzoJL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ,National Heart L, Blood Institute Joint National Committee onPrevention DE, Treatment of High Blood P, National High BloodPressure Education Program Coordinating C (2003) The SeventhReport of the Joint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure: the JNC 7 report.JAMA : J Am Med Assoc 289(19):2560–2572. doi:10.1001/jama.289.19.2560
27. Zhang W, Li N (2011) Prevalence, risk factors, and management ofprehypertension. Int J Hypertens 2011:605359. doi:10.4061/2011/605359
Invest New Drugs