evaluation and integration of histology pattern...
TRANSCRIPT

Histology Pattern Recognition Software in Investigative Pathology
J. Webster, DVM, PhD, DACVP Laboratory of Cancer Biology and Genetics
National Cancer Institute, Bethesda, MD
Pathology Visions 2011 November 1, 2011

Outline
• Introduction – Pattern recognition image analysis
• Evaluation of pattern recognition image analysis – Tissue feature quantification
– Segmentation of morphologically complex tissues
– Observations and personal experiences
• Applications and Integration
• Conclusions
Whole Slide Digital Imaging: Revolutionary Transformation in Pathology
• Diagnostic pathology – Enhanced telepathology – Real-time consultations
• Education – Specimen preservation – Uniform lesion display – Conferencing
• Investigative pathology – Quantitative morphometric image analysis
Morphometric Image Analysis
• Quantify immunohistochemical reactions
• Quantify histochemical stains
• Quantify tissue feature areas
• Identify regions of interest
• Screen for histologic lesions
Morphometric Image Analysis
• Advantages – Increased data acquisition – Decreased subjectivity – Decreased observer variability – Whole-slide image analysis
• Limitations – Few well-developed protocols for applications – Sensitivity to processing and handling – Two-dimensional analysis
Pattern Recognition Image Analysis
• Advantages – Improved analysis throughput – Reproducible, quantitative analysis – Decreased intra-/ inter-observer bias
• Specific Applications – Quantifying metastatic lesions
• Pre-clinical therapeutic models • Tumor transplantation models
– Identifying regions of Interest • Immunohistochemistry quantification
– Diagnostic screening

Quantification of Metastatic Burden

Quantification of Metastatic Burden
23.57% Tumor

Identification of Regions of Interest: Immunohistochemistry Quantification

Pattern Recognition Image Analysis: Persistent Questions
• How accurate are PRIA measurements?
• How reproducible are PRIA measurements?
• Can PRIA software be used for diagnostic screening?
• How can we best employ PRIA software?
• How well does 2-D PRIA represent 3-D lesions?

Evaluation of Pattern Recognition Image Analysis (PRIA)
• Comparison to established morphometric measurements – Quantification of pulmonary metastatic tumor burden – PRIA vs. manual segmentation
• Assessment of performance during segmentation of morphologically complex tissues – Identification of 3 ontogenic germ layers in stem cell-
derived teratomas
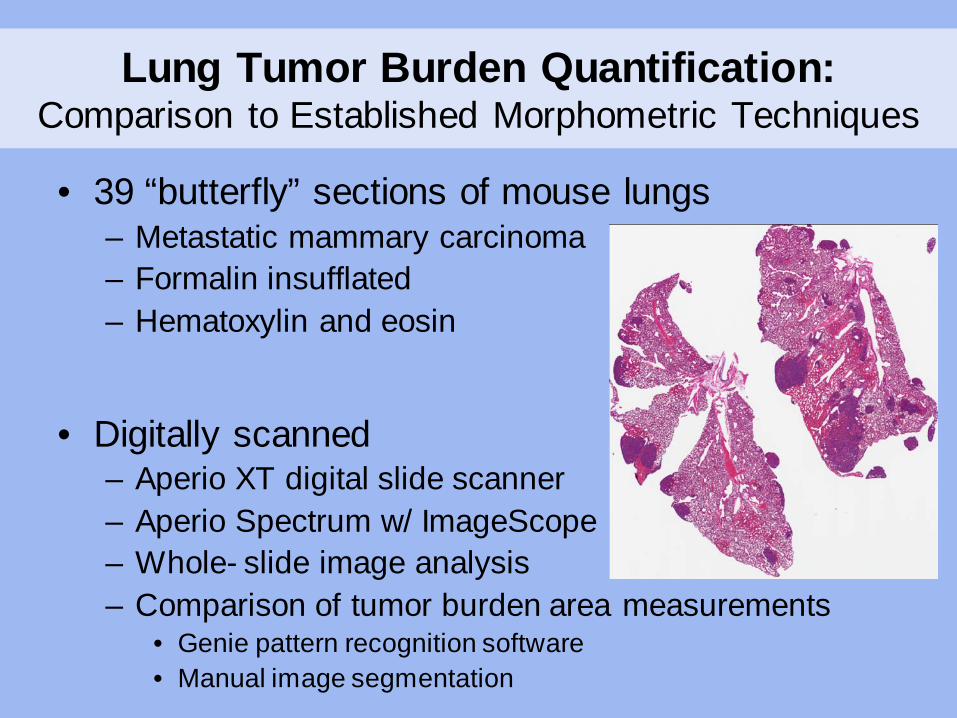
Lung Tumor Burden Quantification: Comparison to Established Morphometric Techniques
• 39 “butterfly” sections of mouse lungs – Metastatic mammary carcinoma – Formalin insufflated – Hematoxylin and eosin
• Digitally scanned
– Aperio XT digital slide scanner – Aperio Spectrum w/ ImageScope – Whole- slide image analysis – Comparison of tumor burden area measurements
• Genie pattern recognition software • Manual image segmentation
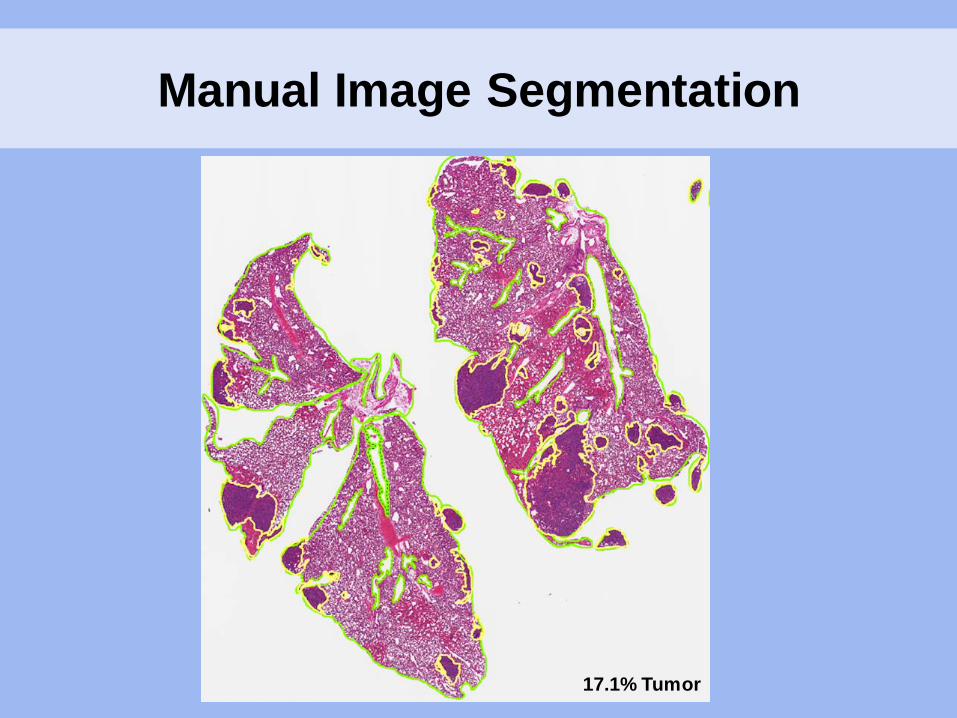
Manual Image Segmentation
17.1% Tumor
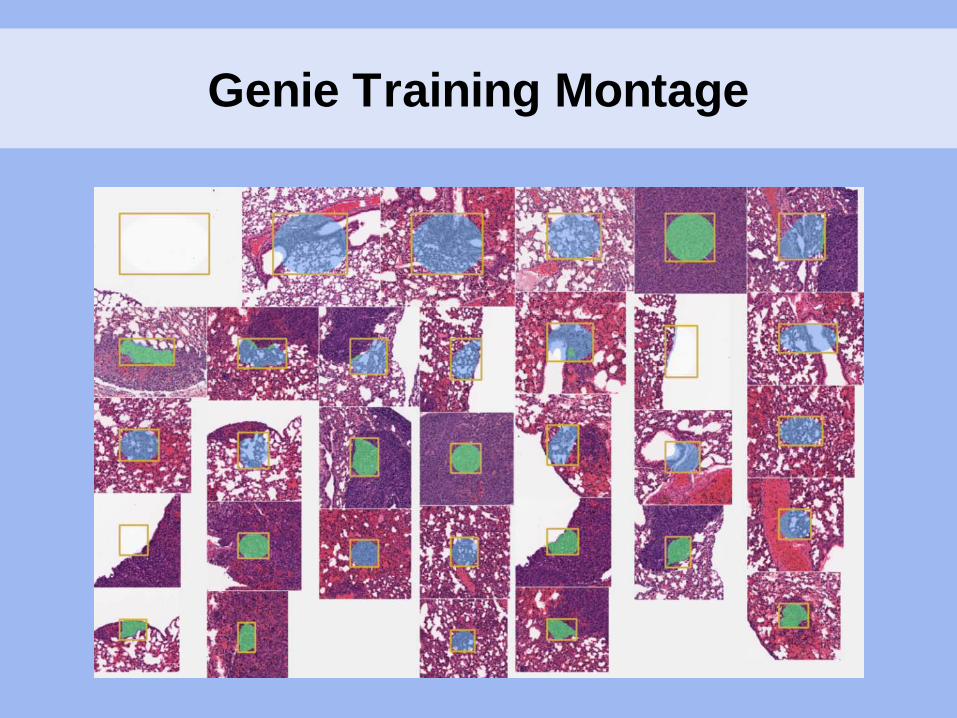
Genie Training Montage
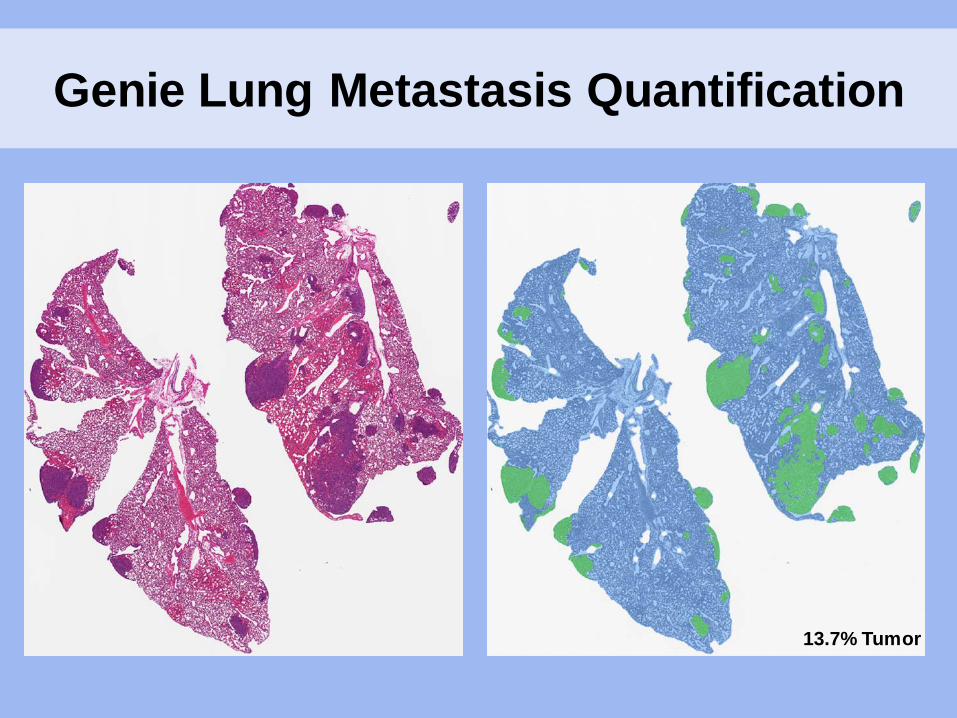
Genie Lung Metastasis Quantification
13.7% Tumor
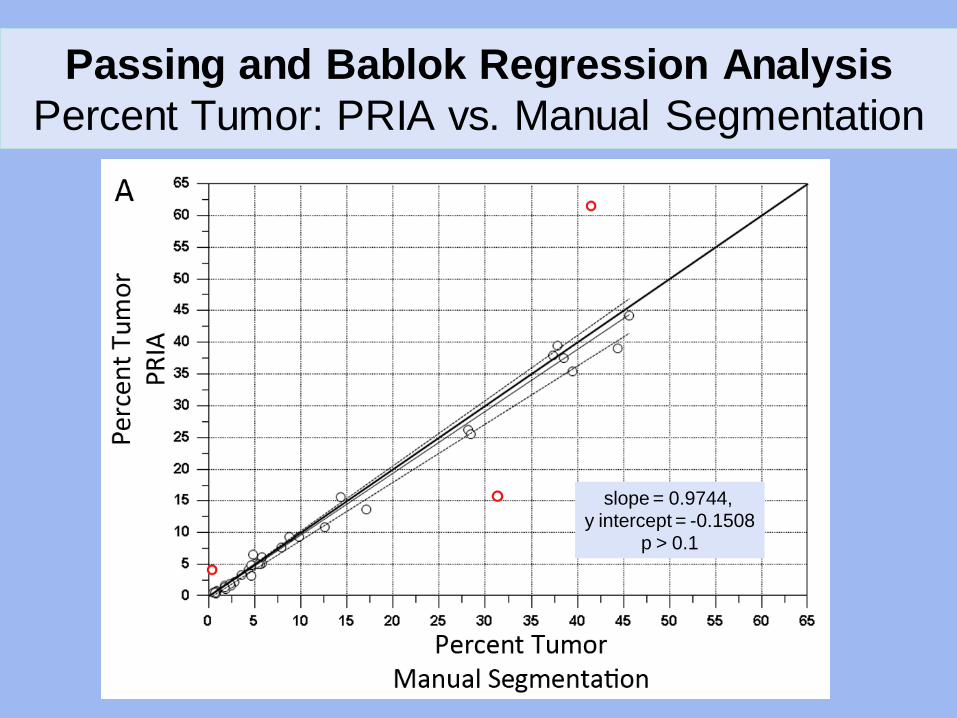
Passing and Bablok Regression Analysis Percent Tumor: PRIA vs. Manual Segmentation
slope = 0.9744, y intercept = -0.1508
p > 0.1
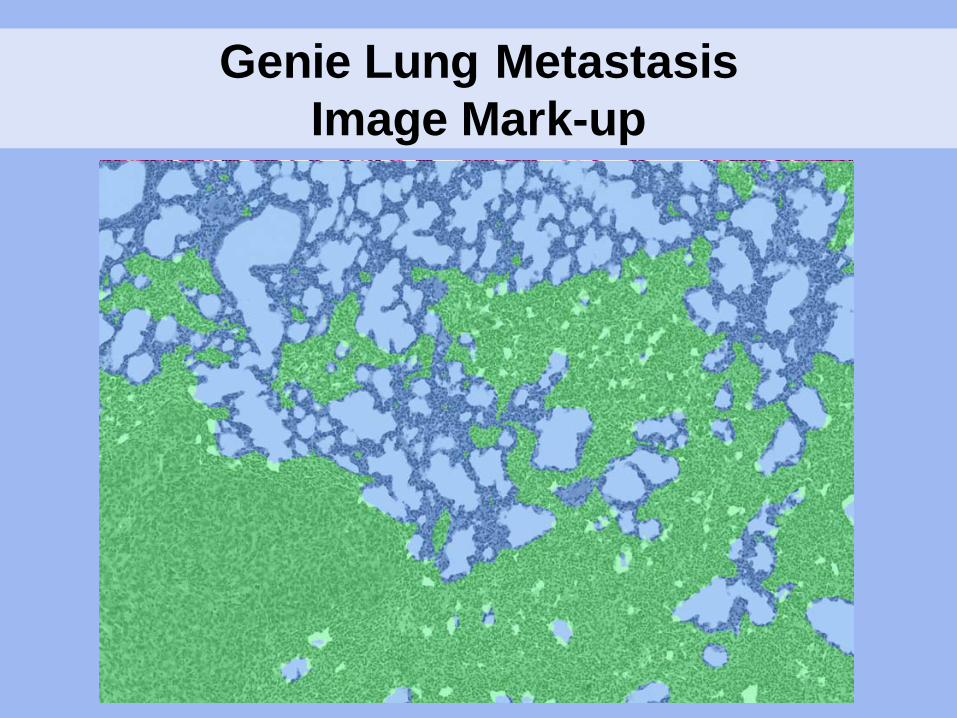
Genie Lung Metastasis Image Mark-up

Bland-Altman Limits of Agreement Plot: Percent Tumor Difference vs. Tumor Burden
Lung Tumor Burden Quantification: Conclusions
• Commensurate percent tumor measures – PRIA tended to be < 9% less than Manual
• Differences between methods are uniform across samples
• Consistent inaccuracies – Mostly tolerable – Tangential bronchioles and atelectasis
• Algorithms are sensitive to variations in – Tissue handling – Processing – Staining

Segmentation of Morphologically Complex Tissues: Stem Cell-derived Teratomas
Teratomas: • Neoplasm derived from
pluripotent cells capable of recapitulating the spectrum of embryonic development
• Tissues representing 3 ontogenic germ layers
• In vivo evidence of stem cell pluipotency
Stem Cell Derived Teratomas
• Samples: – 26 Teratomas
• Mouse – 10 Embryonic stem cell/ 2 induced pluripotent stem cell
• Human – 8 Embryonic stem cell/ 6 induced pluripotent stem cell
• 10 more differentiated
• 16 less differentiated
• Formalin fixed, hematoxylin and eosin stained

Genie Training Montage
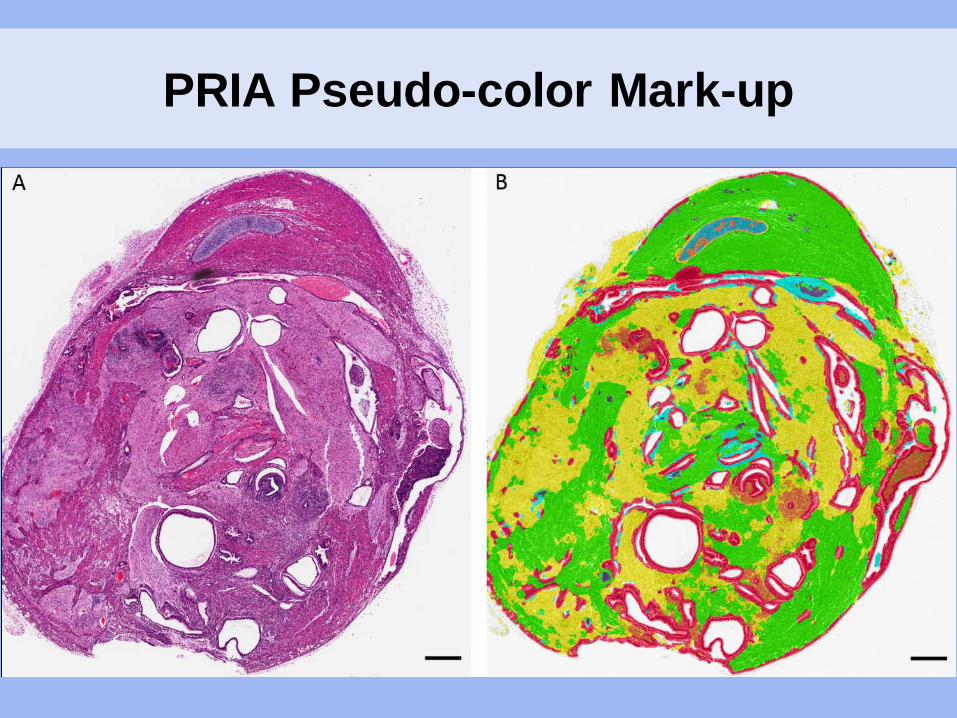
PRIA Pseudo-color Mark-up

Teratoma Algorithm 1: Well-differentiated Teratoma
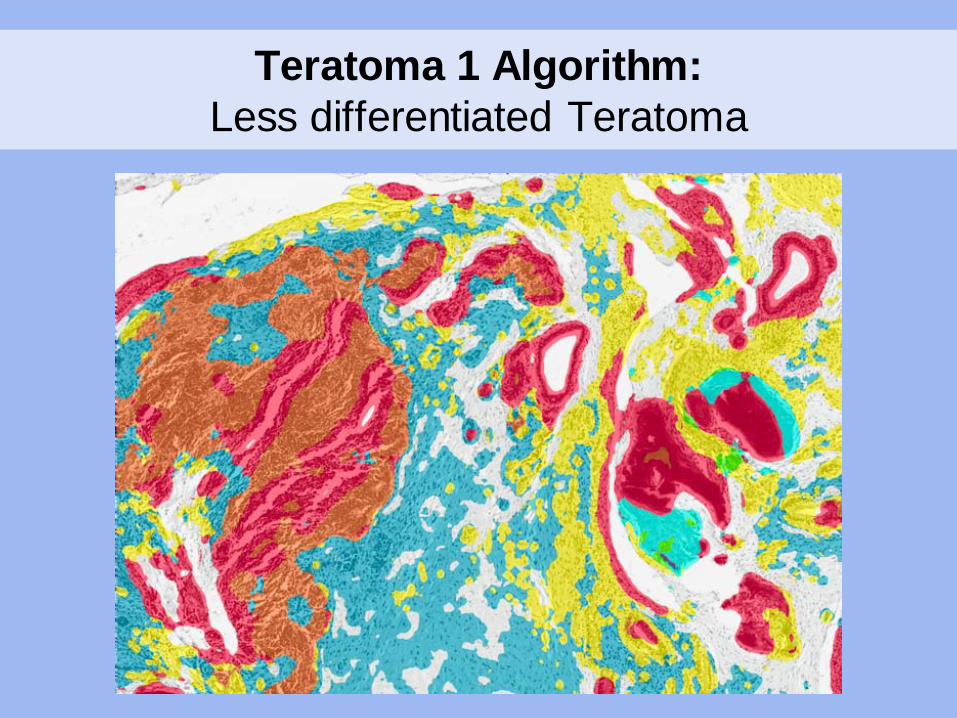
Teratoma 1 Algorithm: Less differentiated Teratoma
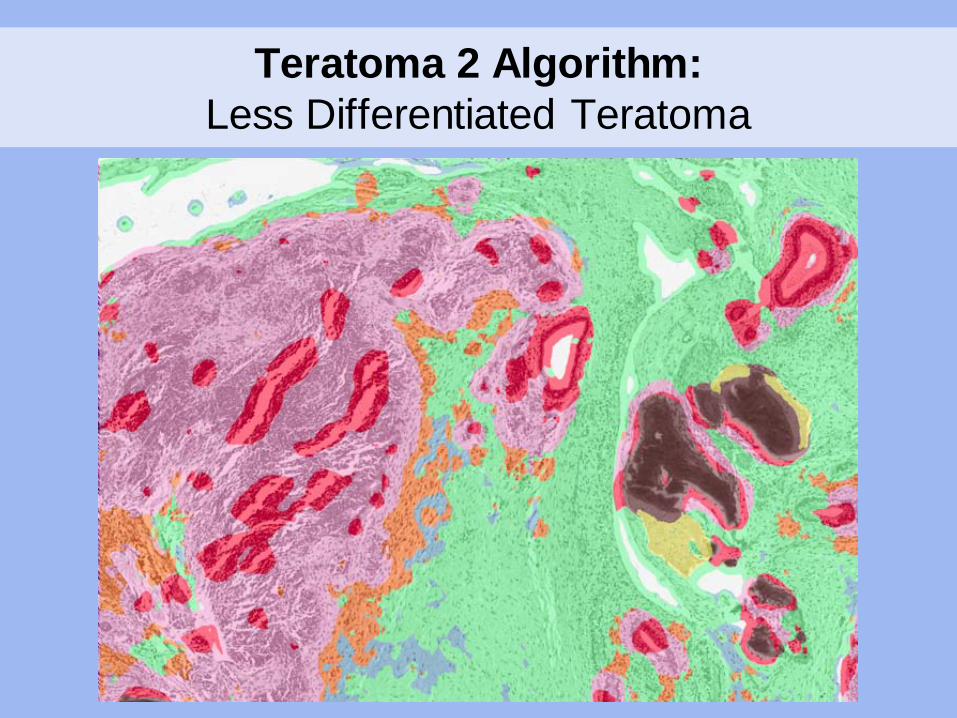
Teratoma 2 Algorithm: Less Differentiated Teratoma

Segmentation of Complex Tissues: Conclusions
• Challenging to account for all tissue classes in a single montage – Montage size limits – Broad spectrum of spatial-spectral features – Overlapping spatial-spectral features
• Overcoming some challenges – Development of multiple algorithms – Consider limitations – Ask appropriate questions

Perceived Limitations Based on Experience
• Preferential reliance on spectral features
• Sensitivity to specimen handling, processing, staining
• Limited contextual understanding – Restriction to a single magnification
• Repetitive difficulties in segmenting necrosis
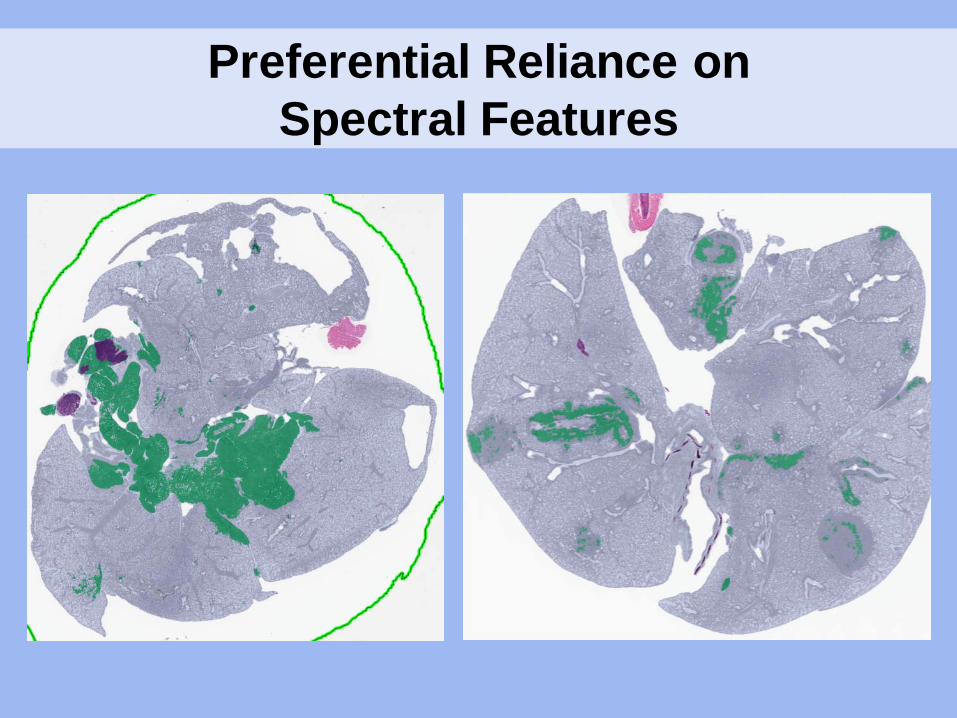
Preferential Reliance on Spectral Features

Repetitive Challenge: Necrosis Segmentation Teratoma Algorithm 1

PRIA Application: Tissue Biobank Quality Assurance
• Tissue biobanking – Essential for translational biomedical research – Reliant on high-quality, well-annotated specimens
• Need for quality assurance pathology review
• Traditional quality assurance pathology review – Confirmation of disease – Subjective assessment of percent tumor – Single or multiple staff pathologists
• Goal: – Utilize PRIA to reproducibly and consistently quantify
tumor percentages in biobank specimens
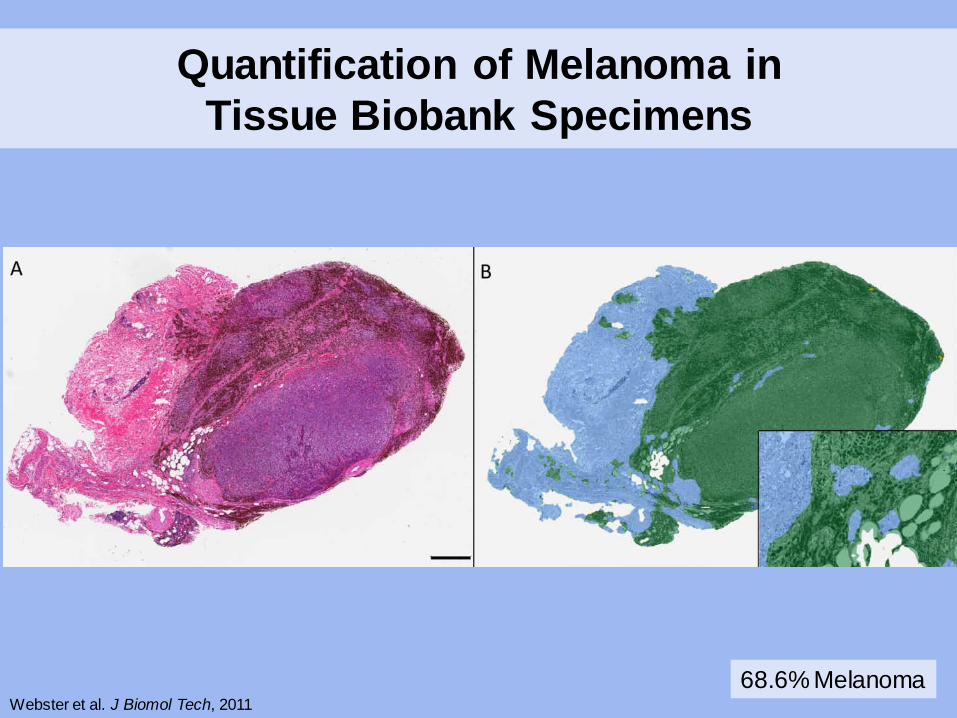
Quantification of Melanoma in Tissue Biobank Specimens
68.6% Melanoma Webster et al. J Biomol Tech, 2011
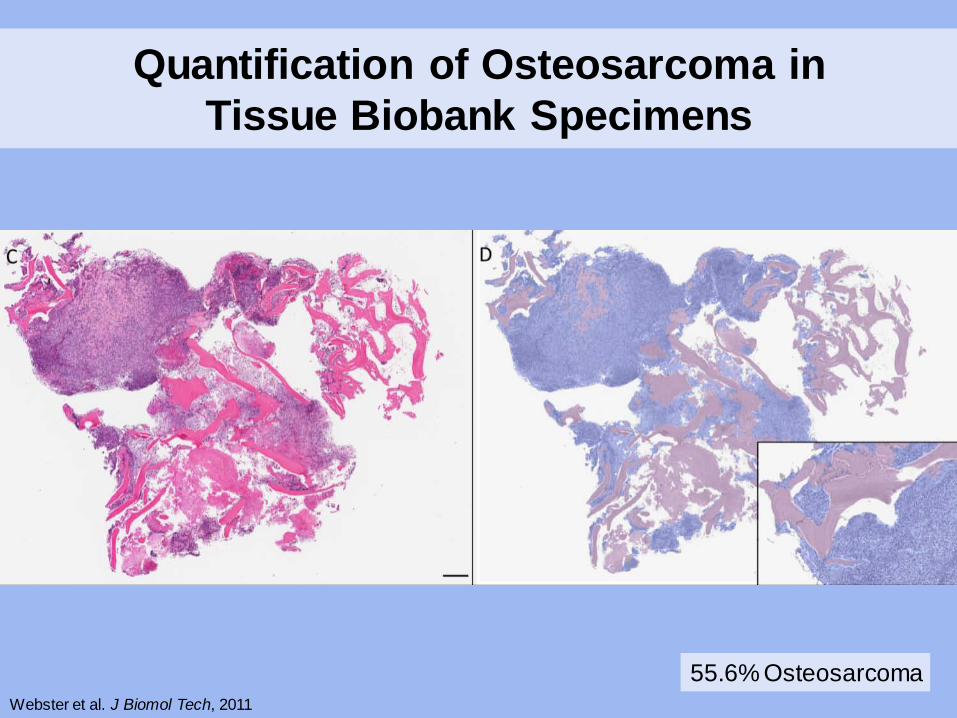
Quantification of Osteosarcoma in Tissue Biobank Specimens
55.6% Osteosarcoma Webster et al. J Biomol Tech, 2011
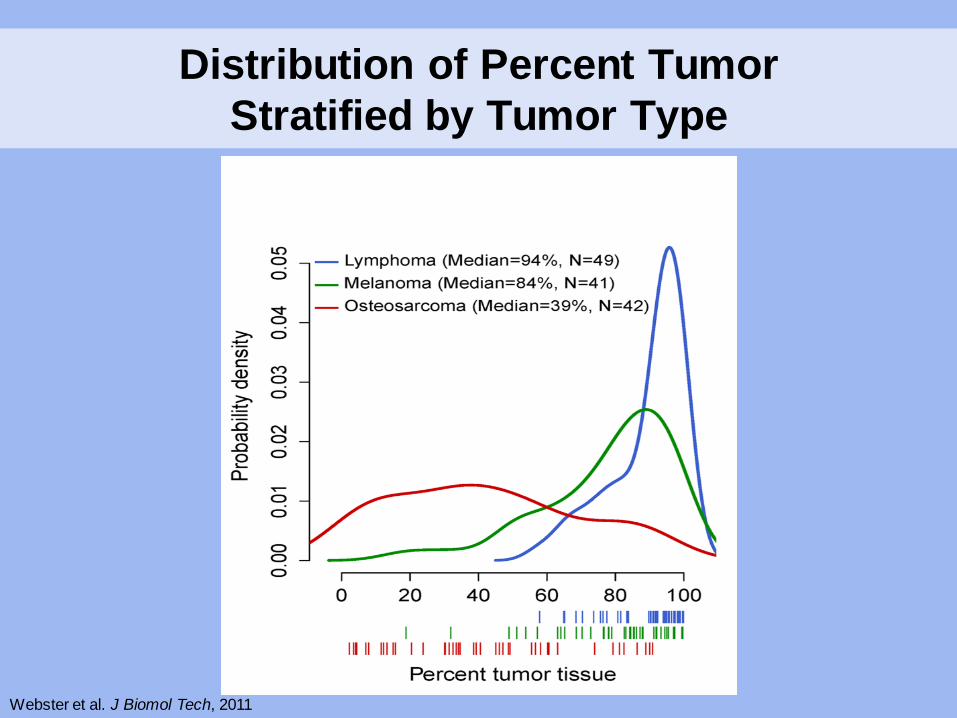
Distribution of Percent Tumor Stratified by Tumor Type
Webster et al. J Biomol Tech, 2011

Within Patient Variability of Percent Tumor in Tissue Sections
Webster et al. J Biomol Tech, 2011

2-Dimensional Analysis of 3-Dimensional Lesions
• Questions: – Are single sections representative? – How many step sections are representative?
• What thicknesses?
• Evaluations: – Comparison to in vivo bioluminescence imaging – Comparison to advanced imaging modalities
• MRI • CT scan
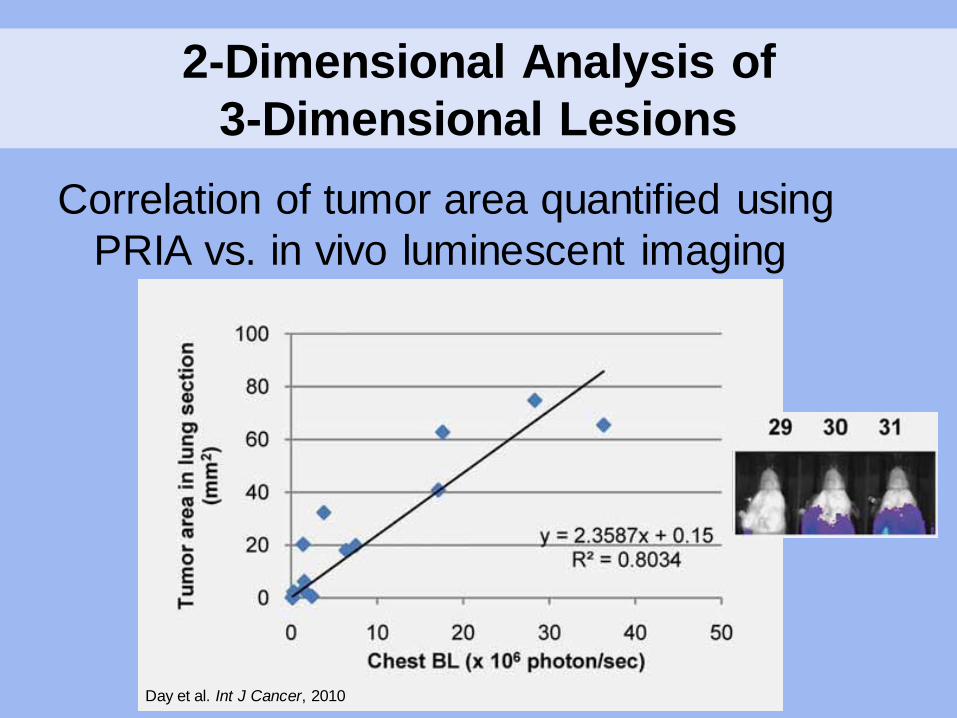
2-Dimensional Analysis of 3-Dimensional Lesions
Correlation of tumor area quantified using PRIA vs. in vivo luminescent imaging
Day et al. Int J Cancer, 2010

Conclusions
• Histologic PRIA software allows for – Reproducible tissue quantification – Decreased intra-/ inter-observer variability – Decreased subjectivity – Increased throughput
• Limitations must be considered – Difficulty segmenting complex tissues – Sensitivity to variations in tissue processing – Preferential reliance on spectral features
Conclusions
• PRIA is optimally utilized when – Tissues are uniformly handled/ processed
– Algorithms are simplified
– Application to appropriate questions
– Quality assurance is uniformly applied
– Pathologist oversight is included in PRIA applications
Acknowledgments • NCI Molecular Pathology Unit
– Mark Simpson – Jennifer Dwyer – Kara Corps – Shelley Hoover – Bih-Rong Wei – John Hickerson
• NCI Laboratory of Cancer
Biology and Genetics – Lalage Wakefield – Yu-an Yang – Christie Tomlinson – Jeff Green – Jing Huang
• National Institute of Aging – Minoru Ko – Yuhki Nakatake
• Johns Hopkins University
– Tarja Juopperi – Hongjun Song