esthetic dentistry / dentisterie esthétique · esthetic dentistry / dentisterie esthétique...
TRANSCRIPT

PUBLICATIONS AGREEMENT # 40025049 • ISSN 1916-7520
www.andrewjohnpublishing.com
Esthetic Dentistry /Dentisterie esthétique
PEER-REVIEWED - JOURNAL - REVUE DES PAIRS
VOLUME 4 - 1Winter/Hiver 2011
Canadian Journal ofRestorative Dentistry & Prosthodontics
Publication officielle de l’Académie canadiennede dentisterie restauratrice et de prosthodontie
Journal canadien dedentisterie restauratrice et de prosthodontie
The official publication of the Canadian Academy ofRestorative Dentistry and Prosthodontics

CARDP OFFICERSPresident - Dr. Kim ParlettPresident-Elect - Dr. Maureen AndreaVice-President - Dr. Ashok VarmaSecretary-Treasurer - Dr. Les KallosPast-President - Dr. Vernon Shaffner
COUNCILLORS (YEARS LEFT IN TERM):Atlantic Provinces Dr. Scott Maclean (3)Quebec/Nunavut Dr. David Blair (1)Ontario Dr. Izchak Barzilay (3)Manitoba/Saskatchewan Dr. TerryKoltek(2)Alberta/NWT Dr. Richard Beauchamp (3)BC/Yukon Dr. Myrna Pearce ( 1)Vancouver, BC
PAST PRESIDENTS
Canadian Academy of RestorativeDentistry and ProsthodonticsL'Académie canadienne dedentisterie restauratrice et deprosthodontie
Vernon Shaffner ............................2010Stanley Blum ..................................2009Mike Racich....................................2008Dennis Nimchuk............................2007Gorman Doyle ..............................2006Allan Osborn..................................2005William H. Sehl ..............................2004Cary D.L. Letkemann ....................2003Brian N. Friesen ............................2002Hubert Gaucher ............................2001Bernard Linke ................................2000Robert J. David ..............................1999Michael R. Roda ............................1998Edward W. McIntyre......................1997Allan R. Mills..................................1996Graham G. Matheson ....................1995Anthony H. Sneazwell....................1994George K. Scott ............................1993
CANADIAN ACADEMY OFPROSTHODONTICS
Dennis P.A. Nimchuk ..................1992Carl J. Osadetz................................1991David H. Charles............................1990Nasser Dibai ..................................1989Bruce M. Jackson ..........................1988Harry L. Gelfant ............................1987Emmanuel J. Rajczak ....................1986Robert E. Hoar ..............................1985Andrew Tynio ................................1984Michael W. Balanko ......................1983Paul S. Sills......................................1982Paul Jean ........................................1981Leon A. Richardson........................1980Arthur H. Irvin ..............................1979Richard C. McLelland ....................1978Francoise Michaud ........................1977Herbert Ptack ................................1976Douglas V. Chaytor ........................1975Georges A. Zarb ............................1974W. Brock Love ................................1973Jacques Fiset ..................................1972A. Harris Crowson ........................1971
Donald Kepron ..............................1970Jean Nadeau ..................................1969Alan D. Fee ....................................1968William G. Woods..........................1967Kenneth M. Kerr* ..........................1966James E. McCutheon......................1965Wilfred D. Clark (charter meeting) ..1964Charles H. Moses ..........................1963R. Lawrence Twible ......................1962
CANADIAN ACADEMY OFRESTORATIVE DENTISTRY
Craig Naylor ..................................1992Ernest R. Ambrose ........................1991Leonard L. Kahane ........................1990Andrew Tynio ................................1989Stanley S. Kucey ............................1988Vernon B. Shaffner ........................1987Daniel C.T. MacIntosh ..................1986Edward J. Abrahams ......................1985
Berl L. Mendel ................................1984J. Ivan Johnston..............................1983B. Larry Pedlar................................1982Norman C. Ferguson ....................1981E.S. Morrison ................................1970Earl V. Gowda ................................1979George K. Scott ..............................1978Owen J. Yule ..................................1977Robert B. Telford............................1976Robert A. Clappison ......................1975Emmanuel J. Rajczak ....................1974Walter V. Grenkow ........................1973Douglas H. MacDougall ................1972D. Blake McAdam ..........................1971Sidney R. Katz ................................1970Jacques Fiset ..................................1969William R. Scott ............................1968James D. Purves..............................1967J. Rod Fraser ..................................1966Harry Rosen ..................................1965
2 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
CARDP EXECUTIVE

Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 3
MESSAGE FROM THE GUEST EDITOR
As each year passes it’s clear that change issomething we face each and every day in
our practices. We may go through each daywith the hope of some degree of predictabilityin our schedules, but being in health care, weknow that may not stay reliable for too long.People may react differently to the sameperiodontal therapy, or perhaps to the samerestoration type. So many factors play a role ininfluencing how our day takes shape and whatmay work or not for our patients. To makematters more complicated, our profession, as awhole is also very dynamic as material choices,treatment modalities and patient expectationscontinue to increase constantly.
Due to the fact that we constantly face changein our dental lives it’s not surprising for us tostart challenging some of what’s beingpresented and also look to fall back on thosethings that at least afford us some predictability.I’ve always subscribed to the fact that we needto think “outside the box,” but at what cost?This issue will focus on various new techniquesand materials while also challenging us to lookat some of the procedures many of us have beenquick to put aside even though they have servedas a solid foundation to our treatment successfor many years.
Dr. Greg Gillespie discusses common issues weface with indirect restorations, one of the mostimportant being that of patient comfort.Although our clinical success is measured bymany factors including longevity, function andesthetics, most patients look at their ultimatelong-term comfort as a true measure of oursuccess. Dr. Gillespie discusses the concept ofimmediate dentin sealing (IDS) as a protocol toassure “clinical success” for our indirectrestorations.
Dr. Gildo Santos Jr., and colleagues present aclinical case that transforms an unsightly smilewith newer generation all-ceramic restorations.Dental ceramics have developed rapidly overthe past decade to provide us with various all-
ceramic options for both anterior and posteriorteeth. The need for these materials andtechniques have been fuelled by the desire ofmany or our patients to find highly estheticoptions that will function well. The authorsdiscuss the use of a leucite-reinforced ceramicsystem for aesthetic anterior restorations.
Dr. Marc Mollot presents two clinical cases thatare designed to create some reflection in ourtreatment planning of more complex cases. Hepresents two multi-disciplinary anteriorrestorative cases that involve orthodontics,periodontics, surgery and prosthetics. Eachcase is carefully discussed in terms of treatmentoptions and material selection. One is treatedwith more contemporary ceramic restorationswhile the other falls back on the traditionalporcelain fused to metal option. He remindsus that both have a place in our treatmentarsenal and looking at the big picture and thepatient’s condition will hopefully guide us tomake appropriate choices.
Dr. Geoff Knight changes gears and takes thingsin a completely different direction bychallenging us to rethink the concept of“minimally invasive dentistry.” He reminds usthat the current model of restorative andesthetic dentistry is based on techniques thatcreate some degree of destruction to thedentition. He asks us to consider re-evaluatingtreatment modalities by consideringpharmacological management of dental diseaserather than the typical destructive nature ofmany of our current treatment choices. Hedemonstrates this with two clinical cases.
Finally I leave you with a clinical case todemonstrate how proper treatment planningand collaboration with a team of specialists canlead to success if it’s done in a structured andthoughtful manner. Many of us feel we arelistening to what our patients want when itcomes to more involved and complex therapies,and then make the assumption that eachspecialist is on the same page. Well times have
changed for both the restorative dentist andindividual specialties. We have a responsibilityto ourselves and our patients to assure we areon the same page when addressing their chiefcomplaint or desire.
So this brings me back to addressing thestatement – “think outside the box”. In orderfor us to grow and expand our horizons it isimperative that one look outside the box andstretch the mind to see what’s possible.Remember, we’re in a dynamic world andstanding still never gets you ahead. Sometimes,however, it’s not all that bad to stay “inside thebox” that has served as a solid foundation formany of our procedures and techniques formany years. This doesn’t imply that we have tostay stuck in our old set ways. This simplymeans we look at each individual case withsome thoroughness, scrutiny, humility, andopen-mindedness, when required. It’s nice toknow that we can leave the door open to thebox from time to time. I hope you’ll enjoy thisissue.
Thank you to all our authors for theircontributions to the education of ourreadership. Once again, I’d like to thank Dr.Hubert Gaucher for his tireless efforts as editor-in-chief. On behalf of our editorial team atCJRDP, thank you for your continued supportand happy reading!
Paresh Shah, DMD, MS, Cert. Esth. DentistryGuest Editor
Think Outside the Box ... Or Not!

4 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
Au fur et à mesure que le temps file, il estclair que le changement est omniprésent
dans notre pratique. Nous pouvons passerchaque jour en espérant une certaine constancedans notre horaire de travail, mais comme noustravaillons dans les soins de la santé, noussavons bien que la constance n’est pas de longuedurée. Les patients ne réagissent pas tous de lamême façon au même traitement parodontalou au même type de restauration. C’est ainsique plusieurs facteurs viennent influencer latournure de notre journée ou ce qui plaît ounon aux patients. Pour compliquer encore plusles choses, notre profession, en tant que telle esttrès dynamique quant au choix du matériau,des modalités de traitement, et les exigences despatients augmentent constamment.
Comme le changement fait partie intégrantede nos vies, il n’est pas surprenant pour nousde devoir remettre en question ce qui estprésenté et de se rabattre sur ce que nouscroyons avoir une certaine constance. J’aitoujours admis le fait que nous devons « sortir des sentiers battus »,mais à quel prix?Ce numéro traitera de diverses nouvellestechniques et divers matériaux tout en nousmettant au défi de revoir les procédures quenous avons mises de côté même si elles ontconstitué une base solide du succès destraitements pendant de nombreuses années.
Le Dr Greg Gillespie aborde les problèmescourants que nous avons avec les restaurationsindirectes, l’une des plus importantes étant leconfort du patient. Bien que notre succèsclinique soit mesuré par plusieurs facteurs, ycompris la longévité, la fonction et l’esthétique,la plupart des patients évaluent le confort à longterme comme mesure véritable de notre succès.Le DrGillespie discute du concept du scellementimmédiat de la dentine comme un protocolepour assurer le succès clinique de nosrestaurations indirectes.
Le DrGildo Santos Jr. et ses collègues présententun cas clinique qui transforme un sourireinesthétique en utilisant une nouvellegénération de restaurations en céramique. Lescéramiques ont évolué rapidement au cours desdix dernières années et nous ont permis d’offrirdiverses options pour les dents antérieures et
postérieures. Plusieurs de nos patients pousséspar le désir de trouver des options hautementesthétiques dont le fonctionnement est adéquatnous ont forcés à développer des matériaux etdes techniques pour répondre à leurs besoins.Les auteurs traitent de l’emploi de céramiquerenforcée à la leucite pour les restaurationsesthétiques des dents antérieures.
Le Dr Marc Mollot présente deux cas cliniquesqui sont conçus pour nous faire réfléchir à laplanification du traitement de cas pluscomplexes. Il présente deux cas de restaurationde dents antérieures en ayant recours à plusieursdisciplines soit : l’orthodontie, la parodontie, lachirurgie et la prosthodontie. Chaque cas estdiscuté en détail en termes d’optionsthérapeutiques et choix de matériau. Pour l’undes cas, une approche plus contemporaine derestauration en céramique a été utilisée, tandisque pour l’autre, il s’agissait d’une restaurationcéramo-métallique traditionnelle. Le DrMollotvient nous rappeler que ces deux restaurationsont une place dans l’arsenal thérapeutique etque le fait de voir la situation dans son ensembleet l’état du patient nous permettra de faire lesbons choix.
Le Dr Geoff Knight adopte une directioncomplètement différente en nous mettant audéfi de repenser au concept de la dentisterie peuinvasive. Il nous rappelle que le modèle courantde dentisterie restauratrice et esthétique estfondé sur des techniques qui engendrent uncertain degré de destruction de la dentition. Ilnous demande de considérer la réévaluation desmodalités de traitement en envisageant lagestion pharmacologique de la maladie dentaireplutôt que la nature destructive typique deplusieurs de nos choix de traitement courants.Il nous donne deux cas cliniques pour en fairela démonstration.
Finalement, je vous laisse avec un cas cliniquepour démontrer comment la planificationadéquate du traitement et la collaborationd’une équipe de spécialistes peuvent mener ausuccès si le tout est fait de manière structurée etréfléchie. Plusieurs d’entre nous ont conscienceque nous écoutons ce que nos patients désirentlorsqu’il s’agit de traitements plus élaborés etplus complexes et assumons que chaque
spécialiste comprend ou voit les choses de lamême façon. Bref, les temps ont changé pour ledentiste de dentisterie restauratrice et lesspécialités individuelles. Nous avons laresponsabilité envers nous-mêmes et envers nospatients de faire en sorte de parler des mêmeschoses lorsqu’il s’agit de prendre enconsidération leurs plaintes ou de combler leursdésirs.
Revenons à notre titre « sortir des sentiersbattus ». Afin de pouvoir grandir et d’élargirnos horizons, il est essentiel de sortir des sentiersbattus et de voir ce qu’il est possible de faire.N’oubliez pas que nous vivons dans un mondedynamique et que de rester inactif ne vousdonnera pas grand-chose. Parfois, ce n’est passi mauvais de ne pas sortir des sentiers battusavec plusieurs de nos procédures et techniquesque nous avons utilisées depuis plusieurs annéeset qui sont une base solide. Mais cela ne veut pasdire de s’enliser dans les vieilles coutumes. Nousdevons examiner chaque cas individuel avectoute la rigueur, l’humilité et l’ouverture d’espritlorsque cela est nécessaire. Il est agréable desavoir qu’il est parfois possible de sortir dessentiers battus de temps en temps. J’espère quevous apprécierez la lecture de ce numéro.
Je remercie tous les auteurs de leur contributionà l’éducation de nos lecteurs. Une fois de plus,je remercie le Dr Hubert Gaucher de sondévouement comme rédacteur en chef. Au nomde l’équipe éditoriale à JCDRP, je vous remerciede votre soutien continu et vous souhaite bonnelecture.
Paresh Shah, DMD, MS, Dentiste esthétiqueagrééRédacteur invité
Sortir des sentiers battus... peut-être pas !
MESSAGE DU RÉDACTEUR INVITÉ

VOL 4, NO.1 • Winter/Hiver , 2011
Official Publication of the CanadianAcademy of Restorative Dentistry and Prosthodontics
Publication officielle de L’Académie canadienne de dentisterie restauratrice et de prosthodontie
EDITOR-IN-CHIEF/RÉDACTEUR EN CHEFHubert Gaucher
Québec City, Québec | [email protected]
ASSOCIATE EDITORS/RÉDACTEURS ASSOCIÉSEmmanuel J. Rajczak
Hamilton, Ontario | [email protected] Andrea
Chester, Nova Scotia | [email protected] Nimchuk
Vancouver, British Columbia | [email protected]
SECTION EDITORS/RÉDACTEURS DE SECTIONOcclusion and Temporo-Mandibular Dysfunctions/Occlusion et dysfonctions temporo-mandibulaires
Kim ParlettBracebridge, Ontario | [email protected]
Implant Dentistry/Dentister ie implantaireRon Zokol
Vancouver, British Columbia | [email protected] Fortin
Québec City, Québec | [email protected] Dentistry / Dentister ie esthétique
Paresh ShahWinnipeg, Manitoba | [email protected]
Dental Technology / Technologie dentairePaul Rotsaert
Hamilton, Ontario | [email protected]
MANAGING EDITOR/DIRECTEUR DE LA RÉDACTION
Scott [email protected]
CONTRIBUTORS/CONTRIBUTEURS
ART DIRECTOR/DESIGN /DIRECTEUR ARTISTIQUE/DESIGN
Andrea [email protected]
SALES AND CIRCULATION COORDINATOR/COORDONATRICE DES VENTES ET DE LA DIFFUSION
Brenda [email protected]
TRANSLATION/TRADUCTION
ACCOUNTING / COMPTABILITÉSusan McClung
GROUP PUBLISHER / CHEF DE LA DIRECTIONJohn D. Birkby
CJRDP/JCDRP is published four times annually by Andrew JohnPublishing Inc. with offices at 115 King Street West, Dundas, On, CanadaL9H 1V1. We welcome editorial submissions but cannot assume respon-sibility or commitment for unsolicited material. Any editorial material,including photographs that are accepted from an unsolicited contributor,will become the property of Andrew John Publishing Inc.FeedbackWe welcome your views and comments. Please send them to Andrew JohnPublishing Inc., 115 King Street West, Dundas, On, Canada L9H 1V1.Copyright 2011 by Andrew John Publishing Inc. All rights reserved.Reprinting in part or in whole is forbidden without express written con-sent from the publisher.Individual CopiesIndividual copies may be purchased for a price of $19.95 Canadian. Bulkorders may be purchased at a discounted price with a minimum orderof 25 copies. Please contact Ms. Brenda Robinson at (905) 628-4309 orbrobinson@ andrewjohnpublishing.com for more information and specif-ic pricing.
Publications Agreement Number 40025049ISSN 1916-7520
Return Undeliverable Canadian Addresses to:
AJPI 115 King Street West, Suite 220Dundas Ontario L9H 1V1
Ian TesterSt. Catharines, Ontario | [email protected]
Gladys St. Louis
Gregory Gillespie, Parag Kachalia, Geo! Knight,Marc Mollot, Andrea Mota, John N. Nasedkin,
Gildo Coelho Santos Jr., Mariea Jacinta Moraes Coelho Santos,Paresh Shah
ACADEMY NEWS / NOUVELLES DE L’ACADÉMIE
Canadian Journal of Restorative Dentistry & Prosthodontics 5
At the Annual 2010 meeting in Calgary, we welcomed 10 new members to the academy. Theyinclude Dr. Denis Beauchesne from Georgetown, ON; Dr. David Bergen from St.
Catharines, ON; Heather Carr from Halifax, NS; Dr. David Fownes from Pointe Claire, QC; Dr.Bruce Mansbridge from Stoney Creek, ON; Dr. Anh Nguyen from Kingston, ON; Dr. Alexander Rosenczweig from Vancouver, BC; Dr. Joseph Rotondo from Montreal, QC; Dr.Peter Walford from Hornby Island, BC; and Dr. Wayne Wright from Guelph, ON.
Since October, Dr. Bruce Gardener and Dr. Patrick Pedlar both from Burlington, ON; Dr. BrianGoldenberg and Dr. Roxanna Saldarriaga both from Vancouver, BC; and Dr. Nick Seddon fromWest Vancouver, BC have been accepted as new members. These dentists will be introduced atthe Toronto 2011 meeting.
These are very healthy numbers. We have to continue to recruit new members to our greatorganization all the time. People often ask what exactly is the breakdown of the membership?Here are the numbers for you. As of the annual general meeting this year we had 57 Active, 70Fellows and 55 Life members for a total of 182.
The academy has streamlined the application procedure so that it is not nearly as onerous as itonce was. To become an Activemember the requirements are the following: 1. Attend a CARDPannual meeting as a guest. 2. Complete the application, which can be downloaded off our website at www.cardp.com Membership is by invitation so as members we need to encourage ourcolleagues to join. Friends from study clubs and dental societies would benefit from belongingto our outstanding organization. To share the wealth of talent and expertise I encourage allmembers to bring a guest to Toronto.
Also of note, after many years of hard work Life membership has been bestowed on Dr. Richard Baxter Rhodes and Dr. Gordon Bayes. Well done gentleman!
Dr. Mary Currie,Committee Chair / Présidente du comité
Message from the MembershipCommittee
Message du Comité des membres

High Strength and low water sorption assures a strong foundation for crowns and direct restoratives - cuts just like dentin
Non-Slumping and post cementation technique
Low Shrinkage properties allow it to be used effectively as a dentin replacement material
Excellent Flowability
CORE-FLO™ DCDual-Cured Flowable Core Build-Up/Dentin Replacement Material
New!
Etch & Rinse withUNI-ETCH
®
Bond withONE-STEP
®
PLUS
Cement withCORE-FLO™ DC
Seat Post Core Build-Up withCORE-FLO™ DC
Post Cementation and Core Build-up in One Single Step!
30 DaysMoney-back Guarantee
Buy 2 CORE-FLO™ DC Re�ll SyringesGet a Free Dispenser anda Free Double Taper LIGHT-POST™ Trial Kit Save
$149
CORE-FLO™ DC Intro Kit 30% o�Get 1 Additional Re�ll Syringe anda Free Double Taper LIGHT-POST™ Trial Kit Save
$138$174.30$249reg.
$69each $138 2 syringes
$925.00 Regular
Solaris™ LED headlight Solaris is the only portable headlight that has been given the top rating by not one, but two independent testing labs. Innovative features include economical replacement batteries and lamphead cable that can be replaced by the user. No more down time waiting for repairs or replacement.
RATED #1Rated #1 LED head light in 2009 by Reality!
Economical replacement cable
Solaris LED on Hogies frame
Solaris LED Headlight System
BISCO DENTAL PRODUCTS CANADA INC.w w w . b i s c o c a n a d a . c o m 1.800.667.8811 1.800.211.1200
Expires April 30, 2011
hDEL™siraloSSolaris po only the is
the given been has that independ two but one
thgildaehheadlight ortable
not by rating top labs testing dent
03 syaD
$9
independ two but one, inc features Innovative
batteries replacement replaced be can that cable
wait time down more No replacement.
925.00Regular
labs. testing dent economical clude
lamphead and . userthe by aced
or repairs for ting
htgnertShgiH woldna
kiltsujstuc-sevitarotser
gnipmulS-noNcetnoitatnemectsopdna
LF-EROCbawwaold F FlerreuCCu-aluD
New!
fgnortsaserussanoitprosretaw
nitnedek
euqinhc
OL ™ CDn i ttineD//Dpp/UUp-dliue Brre Boe C Colb
t ceriddnasnworcrofnoitadnuoffo
alirriettet Manemeceaplen R
0e
3 syaDetnarauGkcab-yenoM
cetnoitatnemectsopdna
egaknirhSwoL treporp
ytilibawolFtnellecxE
Post Cementation
euqinhc
aylevitceffffedesuebottiwollaseit
and Core Build-up in O
lairetamtnemecalpernitnedas
ne Single Step!
htiwesniR&hctEHCTE-INU
®
dnoBETS-ENO
htiwdPE
®
SULP
htiwtnemeCCD™OLF-EROC
OLLOF-EROC2y a eerF Dispenser ee aper LTTaper LIGHTouble D
96 hcae $ 831 s2
tsoPtaeS htiwpU-dliuBeroCCD™OLF-EROC
segnirySll�eRCD™O and
itial KrT-POST™ LIGHT -
segnirys
O BISCww
April 30, 201Expires
ICD™OLOF-EROdditional1 A e�l R
ee aper LTTaper LIGHTouble D
$ 471942 .ger
AS CTODUCAL PRO DENT TAL PRdanacocsib.w
1 1
�o%03tiKortnIinge andyrll S
itial KrT-POST™ LIGHT -
.4 03
A INC.ANADmoc.ad 1.800
DETAATRRated #1in 2009 by Reality!
0.667.8811 1.800.211.1200
1#D LED head light
by Reality!
1.800.211.1200

CJRDP Editorial Board/Le comité de rédaction JCDRP
Editor-in-Chief/Rédacteur en chefHUBERT GAUCHERQuébec City, Québec
Associate Editors/Rédacteurs associés
Section Editors/Section éditeurs
Occlusion andTemporo-MandibularDysfunctions/Occlusion et Dysfonctionstemporo-mandibulaireKIM PARLETTBracebridge, Ontario
Implant Dentistry/Dentisterie implantaireRON ZOKOLVancouver, British Columbia
Implant Dentistry/Dentisterie implantaireYVAN FORTINQuébec City, Québec
Esthetic Dentistry /Dentisterie esthétiquePARESH SHAHWinnipeg, Manitoba
Dental Technology /Technologie dentairePAUL ROTSAERTHamilton, Ontario
VOLUME 4 • I S SU E 1
Content/Sommaire
FEATUR ES/A RTICLES
3 Message from the Guest EditorMessage du rédacteur invité4
Academy News / Nouvel les de L 'académie
5
89
Message from the Membership CommitteeMessage du Comité de membresInstructions to AuthorsInstructions aux auteurs
14
20
INDICATES PEER REVIEWED/INDIQUE REVUE DES PAIRS
EMMANUELJ. RAJCZAKHamilton,Ontario
MAUREENANDREAChester,
Nova Scotia
DENNISNIMCHUKVancouver,
BritishColumbia
Immediate Dentin Sealing: Increasing Long-Term Predictability of Indirect RestorationsScellement immédiat de la dentine : augmentation de la constance à long terme des restaurations indirectesBy Dr. Gregory Gillespie
Minimal Intervention Esthetic DentistryIntervention minimale en dentisterie esthétique By Dr. Geoff Knight BDSc, MSc, MBA, PhD
IAN TESTERSt. Catharines, Ontario
Occlusion andTemporo-MandibularDysfunctions/Occlusion et Dysfonctionstemporo-mandibulaire
Esthetic Dentistry / Dentisterie esthétique
28 A Collaborative Approach to Patient Care: Keys to SuccessLes clés du succès : Une approche collaborative aux soins du patient By Dr. Paresh Shah, DMD, MS, Cert. Esthetic Dentistry
25 Mastering Clinical AdvancementsGérer les progrès cliniques By Dr. John N. Nasedkin, DDS, FRCD(C), FADM
34 Metal Free Ceramics: A Clinical CaseCéramique sans métal : Un cas clinique By Dr. Gildo Coelho Santos Jr., DDS, MSc, PhD; Dr. Andrea Mota, DDS; and Dr. Maria Jacinta Moraes Coelho Santos, DDS, MSc, PhD
39 Traditional versus Contemporary? A Comparative Multidisciplinary Case Report: Implant Fixed Prosthetic Treatment Traditionnel vs contemporain? Un rapport de cas multidisciplinaire comparatif : traitement prothétique implantaire #xeBy Dr. Marc Mollot, BSc, DMD
Cover image: View from Window of Ice Castle at Quebec City Carnaval
Photo couverture: vue d’une fenêtre du Château de glace, Canaval de Québec
Continuing Education in Dentistry / Éducation continue en dentisterie
Case Reports / Rapports des cas
47 Understanding Self-Adhesive Resin Cements (G-CEM by GC America)Compréhension des ciments résines auto-adhésifsBy Dr. Parag R. Kachalia
Product Profi le / Profi l de produit
Readers ' Corner / Coin des lecteurs49 Fall Occlusion Issue Well Received
Numéro Occlusion, automne, bien apprécié

8 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
The paper version of the Canadian Journal ofRestorative Dentistry and Prosthodonticspublishes papers, which are subject to peerreview. The Journal is primarily electronic withfull articles available online; in addition, a printversion of the abstracts from each article is alsosent to all members of CARDP, subscribers tothe print version, dental institutions, andassociations. The Journal considers articles oforiginal research, reviews, scholarly addresses,literature reviews, case reports, book reviews,historical interest, clinical tips, guidelines, lettersto the editor, and so on. Requirements are inaccordance with “Uniform requirements formanuscripts submitted to biomedical journals”(http://www.icmje.org). The editorial policies ofthe journal are in line with those of the Councilof Science Editors (http://www.councilscienceeditors.org/services/draft_approved.cfm). TheJournal endorses the CONSORT statement(www.consort-statement.org) relating toguidelines for improving the Evidence Basedquality reporting of Randomized Clinical Trials(RCTs).
Authors must disclose any commercial interestin the subject of study and the source of anysupport. A covering letter should state that thework is original and should include the addressfor correspondence, as well as the phone and faxnumbers and e-mail address to ensure rapidprocessing. Authors should identify theiraffiliation with a hospital or universitydepartment, and indicate if they are students ordentists. After acceptance of the manuscript, theauthor(s) must sign a copyright transferagreement.
The electronic version of the Canadian Journalof Restorative Dentistry and Prosthodontics willcontain all of the high-quality clinical researchand review articles and editorial material of thepaper version plus additional industry-drivenelements such as product profiles andannouncements. This electronic version ofCJRDP will be published in conjunction withthe paper version of the journal and will be
widely distributed to all CARDP members aswell as over 5,000 other dental professionalsacross the country.
The Journal reserves the right to editmanuscripts to ensure conformity with theJournal’s style. Such editing will not affect thescientific content.
Manuscript PreparationManuscripts should be double-spaced andbetween 1,000 and 4,000 words. The manuscriptmust be sent by e-mail attachment (Word orRich Text Format only). An abstract of up to 500words should be provided, and a statement thatthe study was approved by the relevant researchethics board should be included, where relevant.
The lead author should also provide a brief biosketch and high-resolution photo of himself orherself (see details regarding illustrationsbelow).
ReferencesReferences should be numbered consecutivelyin the text by superscript numerals.Corresponding references should be listed at theend of the text. Exhaustive lists of references arenot encouraged. Unpublished sources such aspersonal communications should be citedwithin the text and not included in the referencelist.
The sequence for journal references should beas follows: author(s); title of paper; journalname abbreviated as in the Index Medicus; yearof publication, volume number, first and lastpage numbers. When there are more than threeauthors, shorten to three and add “et al.”
Col NF, Eckman MH, Karas RH, et al. Patientspecific decisions about hormone replacementtherapy in postmenopausal women. JAMA1997;277:1140-7.
The sequence for chapters of a book should beas follows: author(s) of chapter, chapter title,
author(s) of book, book title, edition, place ofpublication, publisher, year of publication, pagenumbers.
Galloway AC, Colvin SB, Grossi EA, et al.Acquired heart disease. In: Schwartz SI, ShiresGT, Spencer FC, eds. Principles of Surgery, 6thedition. New York: McGraw-Hill; 1994:845-99.
Tables and illustrationsEach table should be typed on a separate page,and should have a legend at the top indicatingthe information contained.
Illustrations may be sent electronically as a TIFFor JPEG file on a disk or CD. Do not embedimages, etc., in text files. Note: Figurereproduction cannot improve on the quality of theoriginals.
Numbers, units, and abbreviationsMeasurements are to be metric. In scientific text,physical quantities and units of time should beexpressed in numerals, for example, 2 kg, 6mmol, 5 hours, 4°C. Use only standard abbreviations, and avoidusing abbreviations in the title. Define allabbreviations on their first mention.
PermissionsWritten permission must be obtained formaterial that has been published in copyrightedmaterial; this includes tables, figures, and quotedtext that exceeds 150 words. Signed patientrelease forms are required for photographs ofidentifiable persons. A copy of all permissionsand patient release forms must accompany themanuscript.
Please submit manuscripts to:Dr Hubert [email protected]
Only electronic submissions will be accepted.
Canadian Journal ofRestorative Dentistry & Prosthodontics
Publication officielle de l’Académie canadiennede dentisterie restauratrice et de prosthodontie
Journal canadien dedentisterie restauratrice et de prosthodontie
The official publication of the Canadian Academy ofRestorative Dentistry and Prosthodontics
INSTRUCTIONS TO AUTHORS
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 9
Le journal canadien de dentisterie restauratrice etde prosthodontie publie des articles revus par despairs. Le Journal est principalement électroniqueayant ses articles intégraux en ligne. De plus, uneversion papier des abstraits de chacun des articlesest envoyée à tous les membres de l'ACDRP, auxsouscripteurs à la version papier, ainsi qu'auxinstitutions et associations. Le Journal accepte lesarticles de recherche, les revues, les articlesscientifiques, les rapports de cas, les résumés delivre, les anecdotes historiques, les trucscliniques, les lignes directrices, les lettres àl’éditeur et ainsi de suite. Les conditionsessentielles correspondent aux « Exigencesuniformes pour les manuscrits soumis à desrevues médicales » (http://www.icmje.org). Lespolitiques en matière d’éditorial pour la revuesont celles adoptées par le Conseil des éditeurs en sciences (http://www.councilscienceeditors.org/services/draft_approved.cfm). LeJournal sanctionne l'énoncé CONSORT(www.consort-statement.org) ayant trait auxnormes pour l'amélioration de la qualité desrapports d'études sur les essais cliniquesaléatoires.
Les auteurs doivent déclarer tout intérêtcommercial dans l’étude et la source de toutecommandite. Une lettre d’accompagnementdevrait révéler que le travail est original etcomprendre une adresse pour toutecorrespondance, ainsi qu’un numéro detéléphone et de télécopieur et une adresseélectronique pour que la demande soit traitéerapidement. Les auteurs doivent mentionnerleur affiliation à un établissement hospitalier ouà une faculté de l’université et indiquer s’ils sontétudiants, résidents, chercheurs ou dentistestraitants. Une fois le manuscrit accepté, l’auteurou les auteurs doivent signer un contratd’exploitation des droits d’auteur.
Dans la version électronique du Journal canadiende dentisterie restauratrice et de prosthodontie yfigureront des rapports sur la recherche cliniquede haute qualité de même que des rapports desynthèse et les textes de fond de la version papieren plus des profils de produits et des annoncesconcernant l’industrie. Cette versionélectronique du JCDRP sera publiée en mêmetemps que la version papier du Journal et sera
distribuée à tous les membres de l’ACDRP ainsiqu’à plus de 5000 autres professionnels dentairesau pays.Les instructions pour la soumission de profils deproduit sont disponibles ici.
Le Journal se réserve le droit de réviser lesmanuscrits pour s’assurer de la conformité avecle style du Journal. Ces révisions n’affecterontpas le contenu scientifique.
Préparation du manuscritLes manuscrits doivent être rédigés à doubleinterligne et compter entre 1000 et 4000 mots.Le manuscrit doit être envoyé par courriel sousforme de pièce jointe (Word ou Rich TextFormat seulement). On exige un résumé d’unmaximum de 500 mots et un énoncé que l’étudea été approuvée par les comités d’éthique à larecherche lorsque cela est pertinent. L’auteurprincipal devrait préparer une courte biographieet fournir une photographie à haute définition(voir les détails ci-dessous concernant lesillustrations).
Références Les références doivent être numérotées demanière consécutive dans le texte sous formed’un exposant (indice supérieur). La liste desréférences correspondantes doit se trouver à lafin du texte. Les longues listes de références nesont pas encouragées. Les sources non publiéestelles que des communications personnellesdevraient être citées dans le texte même et nondans la liste des références.
La manière de présenter les références pour unerevue est la suivante : auteur(s); titre de l’article;nom de la revue abrégée comme dans IndexMedicus; année de publication, numéro duvolume, numéros de la première et de la dernièrepage. Lorsqu’il y plus de trois auteurs, limitez-vous à trois et ajoutez « et al. » Col NF, Eckman MH, Karas RH, et al. Patientspecific decisions about hormone replacementtherapy in postmenopausal women. JAMA1997;277:1140-7.
La séquence pour les chapitres d’un livre doitêtre la suivante : auteur(s) du chapitre, titre duchapitre, auteur(s) du livre, titre du livre, édition,
lieu de publication, éditeur, année depublication, numéros de page.
Galloway AC, Colvin SB, Grossi EA, et al.Acquired heart disease. In: Schwartz SI, ShiresGT, Spencer FC, eds. Principles of Surgery, 6eédition. New York: McGraw-Hill; 1994:845-99.
Tableaux et illustrationsChaque tableau doit être dactylographié sur unepage séparée et doit contenir une légende au baspour expliquer le contenu.
Les illustrations peuvent être envoyées parcourrier électronique sous forme de fichier TIFFou JPEG sur une disquette ou un CD. Veuillezne pas incorporer d’images, etc., dans le fichiertexte. Remarque : La reproduction des chiffres nepeut pas améliorer la qualité des originaux.
Chiffres, unités,et abréviationsToutes les mesures sont en système métrique. Dansun texte scientifique, les quantités et les unités detemps devraient être exprimées en chiffres, parexemple, 2 kg, 6 mmol, 5 heures, 4 °C.
N’utilisez que les abréviations standard et évitezd’utiliser des abréviations dans le titre. Définisseztoutes les abréviations la première fois qu’ellessont mentionnées.Permissions
Une permission écrite doit être obtenue pour lematériel qui a déjà été publié avec des droitsd’auteur. Ce matériel comprend des tableaux, desdiagrammes et du texte cité de plus de 150 mots.Les formulaires de consentement dûment signéspar les patients sont requis pour toutes lesphotographies de personnes pouvant êtreidentifiées. Une copie de toutes ces permissionset formulaires doit être envoyée avec lemanuscrit.
Veuillez soumettre votre manuscrit à :Dr Hubert [email protected]
Seulement les soumissions électroniques serontacceptées.
INSTRUCTIONS AUX AUTEURS

19th Annual Scientific Meeting, September 22nd—24th, 2011 An Invitation Message from the CARDP President
I am honoured to start this New Year as President of the Canadian Academy of Restorative Dentistry and Prosthodontics. I was very lucky, early in my career, to be invited to my first CAP/CARD meetings. I felt from the outset that the members of these two academies had something unique to offer; a first-class dental education, engaging mentorship, and above all, enduring friendships from coast to coast. It is my heartfelt wish to con-tinue to build on that legacy during my term as President of CARDP. A great deal of work takes place behind the scenes in prepara-tion for your annual scientific meeting and for our Journal, as well as the day-to-day task of running our Academy. I want to extend a special recognition to Dr. Cary Letkemann, Convention Chair, to all the Committees, to Dr Hubert Gaucher, Editor-in-Chief of our Journal for his tireless efforts, as well as Alexander/Richardson for making each one of our events more memorable than the last. As with the dental field at large, our great organization is under-going transformations while we strive to produce the best meet-ing experiences in a very competitive market. That is why we need to help each other. Apathy is our only obstacle. I am ap-pealing to each and every one of you to attend this year’s To-ronto meeting September 22 – 24 and to invite a potential mem-ber as well. Don’t wait. Mark the dates on your calendar and call a colleague now! Working on a Committee, contributing an article for the Jour-nal, presenting a Table Clinic, are some of the ways to give back to your Academy. Your participation has never been more im-portant and without you, we will not progress. So plan now to “Attend and Bring a Friend”. See you in Toronto! Respectfully, Dr. Kim Parlett
A Message from the Conference Chair As Convention Chair, it is my great pleasure to invite you to our 19th Annual Scientific Meeting of the Canadian Academy of Restorative Dentistry and Prosthodontics taking place in Toronto September 22 – 24, 2011. This year’s Meeting will be held at the prestigious Fairmont Royal York Hotel. Being the only national dental organization dedicated to all aspects of restorative den-tistry and prosthodontics, our Academy will showcase an illustrious gathering of presenters and leading edge topics. It will also offer a wide array of social events to suit all palates. On Thursday, September 22, our optional, limited attendance Scientific Day will feature the emi-nent Dr. Terry Tanaka who will present a hands-on program titled “Esthetics and Occlusion”. For those who would prefer relaxation, 2 sporting activities are suggested: A golf tournament at Eagle’s Nest or Copper Creek, or sailing the Toronto Harbour on Lake Ontario. The day will culminate in a Welcoming Reception back at the hotel. Great food, cocktails, light entertainment and the opportunity to mingle with friends, colleagues and exhibitors make this a convivial occa-sion. On Friday, the heart of the Scientific Program will showcase 6 one-hour essayist presentations by Dr. Terry Tanaka, Dr. Jay Gibson, Dr. Terry Donovan, Dr. John Davies, Dr. Winston Chee and Dr. Daniel Melker. They will cover a variety of topics including mini implants for orthodontic anchorage, stem cell research, wear and erosion, occlusal factors relating to implant restorations, hazards to avoid in implant dentistry and the science of saving teeth. For those not attending the Meeting, a Partner’s Program will be designed to entertain and delight. Then the evening will be free to enjoy the incredible selection of restaurants and entertainment that Toronto offers. Saturday is usually the ‘meat and potatoes’ of the Meeting. The morning will headline 8 eighteen-minute clinical presentations where the speakers have just enough time to give you nothing but the facts. The afternoon is dedicated to table clinics with a wide range of hands-on presentations showing techniques that you can take back to the office on Monday. The entire Meeting will be capped with the President’s Gala, including a champagne reception, fine dining and dancing to the 905 Band, one of Canada’s foremost party bands. Plan on attending because you wouldn’t want your friends to tell you what a great time you missed. I look forward to seeing you there. Cary Letkemann Convention Chair
Friday, September 23rd, Essayists, 1 Hour Presentations Terry Tanaka D.D.S. Topic: Anatomical and Restora ve Complica ons in Implant Den stry Jay Gibson B.Sc., D.D.S. Topic: The Use of Mini-Implants for Orthodon c Anchorage in Pre- Prosthe c Movement John E. Davies Bds, PhD, Dsc Topic: Mesenchymal Stem Cells and Tissue Regenera on in the Craniofacial Complex Terry E. Donovan D.D.S Topic: Recogni on, Management and Preven on of Dental Erosion Winston W.L. Chee D.D.S. Topic: Occlusion as it relates to Implant Supported Structures
Daniel Melker D.D.S. Topic: The TEAM Approach to Comprehensive Periodontal and Restora ve Treatment
Saturday, September 24th, Clinics, 18 Minute Presentations Dr. Oliver C. Pin Harry Topic: Treatment of Atypical Dental Development using
contemporary Fixed Dental Prostheses
Dr. Peter Wolford Topic: Restoring Incisal A!ri on with Composite Resin Dr. Peter Fritz Topic: Periodontal Radiography Dr. Daniel Zeiter Topic: Periodontal Disease Classifica on and Accepted Treatment Dr. Alexandre Tache Topic: Ridge Preserva on: A key step for Implant Rehabilita on Dr. Michael Melkers Topic: Parafunc onal Analysis in Diagnos c and Restora ve Den stry Dr. Robert Margeas Topic: Immediate Extrac on, Implant Placement and Provisionaliza on
in the Anterior Maxilla Using the Pa ent’s Natural Tooth
Plus 15 Afternoon Table Clinics, are presented from 2:30 pm—5:30 pm More information on our Speakers and Thursday, Hands on Course coming in the Next Issue. Visit www.cardp.ca for program updates and registration coming soon!
Join us in Toronto this September!
Get Mee ng informa on & Register online soon @ www.cardp.ca
Toronto, Royal York Reserva ons 1 (800) 441-1414
Thursday, September 22nd, Full Day Hands on Course “Esthetics and Occlusion”
Dr Tanaka has published numerous articles and is widely recognized as a research anato-mist and for his teaching of advanced restora-tive procedures. He is highly sought after as a speaker throughout the world, and is known for his exciting presentations and outstanding clinical skills. His educational videotapes on TM Dysfunction, Anatomy and Implants are used in over 80 medical and dental schools and surgery programs throughout the world.
COURSE OBJECTIVES:
To gather, organize, interpret and apply important clinical infor-mation for comprehensive treatment planning
· To provide the most “comprehensive” treatment for the Patient
· Avoid esthetic and functional failures
· Learn interdisciplinary treatment guidelines
10 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011

A Recognized Provider
Date: ____________________________________ Date Received by Admissions Chair:________________________________ Applicant’s Complete Formal Name: Proposer’s Name: _________________________________________ _______________________________________________________________ Applicant’s Preferred Name: Secondary Proposers Name: _________________________________________ _______________________________________________________________ Year of Dental Graduation: __________________ Applicant’s Business Address: Applicant’s Bus. Phone: __________________________________________ _________________________________________ Applicant’s Home Phone:_________________________________________ _________________________________________ Applicant’s Fax No.: _____________________________________________ _________________________________________ Applicant’s E-Mail: ______________________________________________ Degree (s), School (s) and Year (s) Obtained: ___________________________________________________________________________ Number of Years in Practice: ________________ G.P. or Specialist (list specialty): ___________________ Other Memberships, Qualifications or History: _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Teaching Experience or Presentations Given: (list additional on reverse if more space required) _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Publications (list most pertinent if any): _________________________________________________________________________________________________________________ _________________________________________________________________________________________________________________ Number of CARDP Meetings Attended (indicate which years): ________________________________________ Proposer’s Signature: __________________________________________________________________________ Secondary Proposers Signature:_________________________________________________________________
PLEASE ALSO PROVIDE YOUR SPONSORS LETTER OF RECOMMENDATION WITH THIS APPLICATION!
APPLICATION FORM ALSO ONLINE @ www.cardp.ca
(MEMBERSHIP APPLICATION – Active Status)
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 11

Jeudi le 22 septembre: Cours pratique journée complète “Esthétique et occlusion”
Dr. Tanaka est un anatomiste réputé, auteur et enseignant de techniques restauratrices pointues dont les présentations et habiletés cliniques exceptionnelles sont reconnues internationalement. Ses vidéos instructifs sur la dysfonction TM, l’anatomie et les im-plants sont utilisés dans plus de 80 écoles dentaires et médicales et programmes chi-rurgicaux à travers le monde.
Obtenir, organiser, interpréter et appliquer l'information clinique pour un plan de traitement integral
• Donner au patient un traitement des plus complets
• Éviter les échecs esthétiques et de function
• Apprendre les directives de traitements interdisciplinaires
Une invitation du Président de l’ACDRP Je suis honoré de démarrer cette année en tant que Président de l’Académie canadi-enne de dentisterie restauratrice et de prosthodontie. Au tout début de ma carrière, j’ai eu la chance d’assister, comme invité, à des ren-contres de l’APC/ACDR. Dès lors j’ai eu l’impression que ces deux académies offraient quelque chose d’unique: une formation dentaire et un mentorat sans pareils, et surtout, des liens ami-caux durables d’un océan à l’autre. Je souhaite sincèrement renchérir sur cet héritage durant mon mandat. Une quantité considérable de travail est nécessaire dans la pré-paration des congrès annuels ainsi que le Journal de l’ACDRP, en plus de l’administration quotidienne de notre Académie. Je tiens à reconnaître tout spécialement Dr. Cary Letkemann, Président de notre Congrès cette année, tous les Comités, le Dr Hubert Gaucher, Rédacteur-en-chef de notre Journal pour son dévouement intarissable, et en dernier lieu, Alexander/Richardson qui rendent mémorable chacune de nos rencontres. Comme partout ailleurs dans le domaine dentaire, notre organ-isme subit certaines transformations tandis que nous nous ef-forçons de produire les meilleures expériences dans un marché extêmement concurrentiel. C’est pourquoi nous devons nous entraider. Notre seul obstacle, à vrai dire, c’est l’apathie. Je fais donc appel à chacun parmi vous d’assister au Congrès de cette année à Toronto, du 22 au 24 septembre, et de surcroît, d’inviter un membre potentiel. Ne tardez pas. Notez la date à votre agenda et appelez un collègue dès aujourd’hui. Plusieurs autres façons existent aussi pour venir en aide à votre Académie, par exemple: oeuvrer sur un comité, contribuer un article pour le Journal, présenter une démonstration clinique. Votre participation n’aura jamais eu autant de portée car, sans vous, nous cesserons de progresser. Alors “Assistez et Invitez”. On se voit à Toronto! Cordialement, Dr. Kim Parlett
Un message du Président du congrès En tant que Président du congrès, il me fait plaisir de vous convier à notre 19ième congrès annuel de l’Académie canadienne de dentisterie restauratrice et de prosthodontie qui aura lieu à Toronto du 22 au 24 septembre 2011. Cette année, l’événement se tiendra au prestigieux Fairmont Royal York Hotel. Étant donné que notre organisme est le seul au niveau national qui soit dédié à tous les aspects de la dentisterie restauratrice et de la prosthodontie, notre Académie présentera un illustre assemblage de conférenciers et de thèmes de fine pointe. Nous offrirons de plus in grande variété d’activités sociales pour plaire à tous les goûts. Jeudi le 22 septembre sera une journée scientifique optionnelle et contingentée, animée par le célèbre Dr. Terry Tanaka, qui offrira un programme pratique intitulé “L’esthétique et l’occlu-sion”. Pour ceux qui préfèrent la détente, 2 passe-temps sportifs seront à l’ordre du jour: Un tour-noi de golf au Eagle’s Nest ou à Copper Creek, ou bien de la voile dans le port du Lac Ontario. La journée se terminera à l’hôtel, pour une réception de bienvenue. La bonne chère, des appéros, de la musique et l’opportunité de rencontrer amis, collègues et exposants agrémenteront cette ren-contre conviviale. Le vendredi sera le coeur du programme scientifique. On y introduira 6 présentations d’une heure chacune, proposées par Dr. Terry Tanaka, Dr. Jay Gibson, Dr. Terry Donovan, Dr. John Davies, Dr. Winston Chee et Dr. Daniel Melker. Un assortiment de sujets seront discutés: les mini implants pour ancrage orthodontique, la recherche sur les cellules souches, l’usure et l’érosion, les facteurs occlusaux relatifs aux restorations implantaires, les dangers à éviter en dentisterie im-plantaire et la science de la sauvegarde des dents. Ceux et celles qui n’assisteront pas au congrès pourront profiter d’un programme agréable conçu pour vous enchanter. La soirée sera ensuite libre pour découvrir l’innombrable sélection de res-taurants et de divertissements qu’offre Toronto. Samedi matin, 8 présentations cliniques brèves de 18 minutes se succèderont durant lesquelles les conférenciers n’auront le temps que de vous fournir uniquement les faits. L’après-midi sera consacré aux démonstrations cliniques qui vous soumettront des techniques concrètes et pratiques. Le congrès sera couronné par le Bal du Prési-dent comportant la réception au champagne, une cuisine raffinée et de la danse au son du 905 Band, l’une des plus réputées au Canada. Soyez-y puisque vous ne voudriez pas regretter tous les plaisirs que vos amis auront goûtés! Au plaisir de vous voir, Dr. Cary Letkemann Président du congrès
Conférenciers du vendredi, Présentations d'une heure Terry Tanaka, D.D.S. Topic: Complica ons anatomiques et restauratrices en den sterie implantaire Jay Gibson, B.Sc., D.D.S. Topic: L’emploi de mini implants comme ancrage dans les mouvements pré-prothé ques John E. Davies, B.Ds., Ph.D., D.Sc. Topic: Les cellules souches mésenchymes et la regénéra on ssulaire du complexe craniofacial Terry E. Donovan, D.D.S. Topic: L’iden fica on, la ges on et la préven on de l’érosion dentaire Winston W.L. Chee, D.D.S. Topic: L’occlusion rela ve aux restaura ons implanto-portées Daniel Melker D.D.S. Topic: L'approche d'équipe vers un traitement d'ensemble parodontal et restaurateur
Cliniques du samedi, Présentations de 18 minutes Dr. Oliver C. Pin Harry Topic: Le traitement du développement dentaire atypique à l’aide d’une
prothèse dentaire télescopique fixe
Dr. Peter Walford Topic: La restaura on de l’a!ri on incisive avec la résine composite Dr. Peter Fritz Topic: La radiographie parodontale Dr. Daniel Zeiter Topic: La classifica on des maladies parodontales et leurs traitements Dr. Alex Tache Topic: Conserva on de la crête Dr. Michael Melkers Topic: Analyse parafonc onnelle en den sterie diagnos que et restau ratrice Dr. Robert Margeas Topic: Extrac on et placement immédiat d’un implant et temporisa on au maxillaire antérieur u lisant la dent naturelle du pa ent
De plus, 15 démonstrations cliniques seront présentées de 14h30 à 17h30 De l'information supplémentaire sur nos conférenciers et le cours pratique du jeudi
apparaîtra dans le prochain numéro. Pour des mises à jour des programmes et l'inscription, référez-vous à www.cardp.ca
Soyez des-nôtres en Septembre!
19ième Congrès annuel, 22 au 24 septembre 2011
Plus d’information sur le congrès et la possibilité de vous inscrire en ligne suivront bientôt @ www.cardp.ca
Réservations Royal York Hotel à Toronto: (800)441-1414
12 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011

Fournisseur reconnu
Date _____________________________________ Date reçue par le comité d’admission________________________________ Nom complet du candidat Président du comité _________________________________________ ____________________________________________________________ Nom usuel du candidat Nom du second commanditaire _________________________________________ ____________________________________________________________ Année de sa promotion ____________________ Adresse d’affaires Téléphone au bureau __________________________________________
_________________________________________ Adresse au domicile___________________________________________ _________________________________________ Télécopieur __________________________________________________
_________________________________________ Courriel ______________________________________________________
Diplômes, institutions d’enseignement et années d’obtention___________________________________________________________ ________________________________________________________________________________________________________________ Nombre d’années en pratique____________ Omnipraticien ou spécialiste_______________(nommer spécialité) Autres organismes et/ou qualifications ________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________ Expérience en enseignement ou conférences présentées (utiliser le verso si faute d’espace) ________________________________________________________________________________________________________________ ________________________________________________________________________________________________________________ Publications (les plus pertinentes s’il y a lieu) ________________________________________________________________________________________________________________ Nombre de congrès de ACDRP assistés (indiquer les années)________________________________________ Signature du commanditaire:___________________________________________________________________ Signature du second commanditaire:_____________________________________________________________
Veuillez inclure la lettre de recommandation de votre
commanditaire avec cette demande
Demande d’adhésion aussi en ligne @ www.cardp.ca
(Demande d’adhésion – membre actif)
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 13

ESTHETIC DENTISTRY / DENTISTERIE ESTHÉTIQUE
ABSTRACTLong-term “clinical success” of indirect restorations is categorized in many ways: In addition to a patient’scomfort, the practitioner must also ensure the longevity of the restoration, functionality, and esthetics. Doneproperly, immediate dentin sealing (IDS) is one technique that accomplishes these goals. In this article, theauthor explains what IDS is, discusses its beneficial factors, and outlines the procedural steps involved ineffective IDS.
RÉSUMÉLe succès clinique à long terme des restaurations indirectes est catégorisé de plusieurs manières : en plus depenser au confort du patient, le praticien doit aussi assurer la longévité de la restauration, sa fonctionnalitéet son esthétique. Lorsqu’il est fait de manière adéquate, le scellement immédiat de la dentine est unetechnique qui atteint les objectifs mentionnés auparavant. Dans cet article, l’auteur définit le scellementimmédiat de la dentine, énonce les facteurs bénéfiques et donne les étapes à suivre pour réussir ce scellement.
14 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
Immediate Dentin Sealing: Increasing Long-TermPredictability of Indirect Restorations
Scellement immédiat de la dentine : augmentation dela constance à long terme des restaurations indirectes
By Dr. Gregory Gillespie
About the Author
Dr. Gillespie received his dental degree from the University of Washington School of Dentistry andmaintains a full time practice in Vancouver, WA focusing on general dentistry with an emphasis onimplant dentistry. His vision of comprehensive dentistry focuses on effective treatment planning andutilizing the best dental materials available. Dr. Gillespie lectures nationally and is associated withCatapult Elite. As a member of this select group of clinicians, he is involved in ongoing evaluations ofthe latest materials and techniques in dentistry.
GILLESPIE
Long-term clinical success of indirectrestorations is categorized in many ways.
The patient’s satisfaction with the restorationover the immediate term and long-termlargely determines whether the outcome is a“clinical success.” From the patient’sperspective, satisfaction for the entireprocedure rests in comfort – from thepreparation stage, weeks of temporization,cementation, and finally to function.Maintaining comfort consistently remains alofty goal for the practitioner, but is the mostbasic of expectations from the patient. Yetcomfort comprises only a portion of what thepractitioner would consider “clinical success.”In addition to the patient’s comfort, thepractitioner must also ensure the longevity ofthe restoration, including no catastrophicfailures, marginal ridge or cuspal fractures,microleakage, delamination or debonding, theminimization of microfractures, andprotection of the pulp. Such specificationssimply address functionality withoutconsideration of the esthetic result. Given theenormity of factors qualifying “clinicalsuccess,” fulfillment of patient’s comfort,functionality, and esthetics are difficult tosimultaneously achieve, yet should stillroutinely be met regardless of the indirectmaterial of choice. Simple reason suggests theneed for techniques to improve chances of“clinical success” for the patient andpractitioner alike. Done properly, immediatedentin sealing (IDS) is one technique thataccomplishes this goal.
What Is IDS?Immediate dentin sealing (IDS), also knownas “resin coating,” consists of sealing freshlycut dentin at the time of preparation with adentin bonding agent. The clean,uncontaminated dentin surface optimizes thebonding procedure, allowing deeper resinpenetration into dentinal tubules. A resincoated preparation preserves dentin bonds forcementation and greatly decreases bacterialcontamination during temporization.1–3
After the preparation is completed, a 3-stepetch-rinse or 2-step self-etch adhesive systemis layered and light cured. Currently, 2- and 3-step adhesive systems are preferred over 1-stepadhesive systems (all-in-one or 7th generationbonding) due to the increased hydrophobicsurface formed during the adhesive process.4
The formation of theresin hybrid layerreinforces collagenprone to collapseduring the impressionand cementationphases.5–7 Additionally,sealing the dentinprior to theimpression accountsfor film thickness ofthe adhesive system,and removes concernof an imperfect fit ofthe permanentrestoration.4,8 Pre-polymerization of thebonding agent allowsmaturation of the bond during temporizationwithout the stress associated with thecementation, or luting, process.9
At the final seating appointment thetemporary is removed, the preparationcleansed, and an additional layer of thebonding resin is light-cured in conjunctionwith the resin-luting agent. Ultimately, sealingthe dentin at the time of preparation preservesthe adhesive layer and significantly increasesbond strengths of the permanentrestoration,4,8,10–12 regardless of the type ofluting agent chosen.13
Beneficial Factors of IDSImmediately sealing the dentin followingtooth preparation for indirect restorations(inlay, onlay, veneer, or crown) increases thelikelihood of long-term “clinical success.” Thefollowing four specific beneficial factors areoutlined further below.
Factor 1: Decreased SensitivityHydrodynamic theory suggests fluidmovement through dentinal tubules highlycontributes to patient’s sensitivity.14,15 Physicalobstruction of the tubules with a filled resindramatically diminishes sensitivity during thetemporization phase and immediately post-cementation.16,17 Studies indicate that sealingthe dentin decreases sensitivity even up to one-month post-cementation,18 thereby decreasingrisk of erroneous continual treatmentrecommendations such as root canal therapy.Anecdotally, the author reports increasedpatient comfort and decreased sensitivity
when immediate dentin sealing is performed.
Factor 2: Reduced Bacterial ContaminationProvisional restorations are fabricated in amanner to facilitate removal after a shortinterval. Hence, bacterial contamination dueto microleakage often develops during thetemporization phase.1 Contamination frombacteria and temporary cements greatlydecrease the bonding efficacy of luting agents.
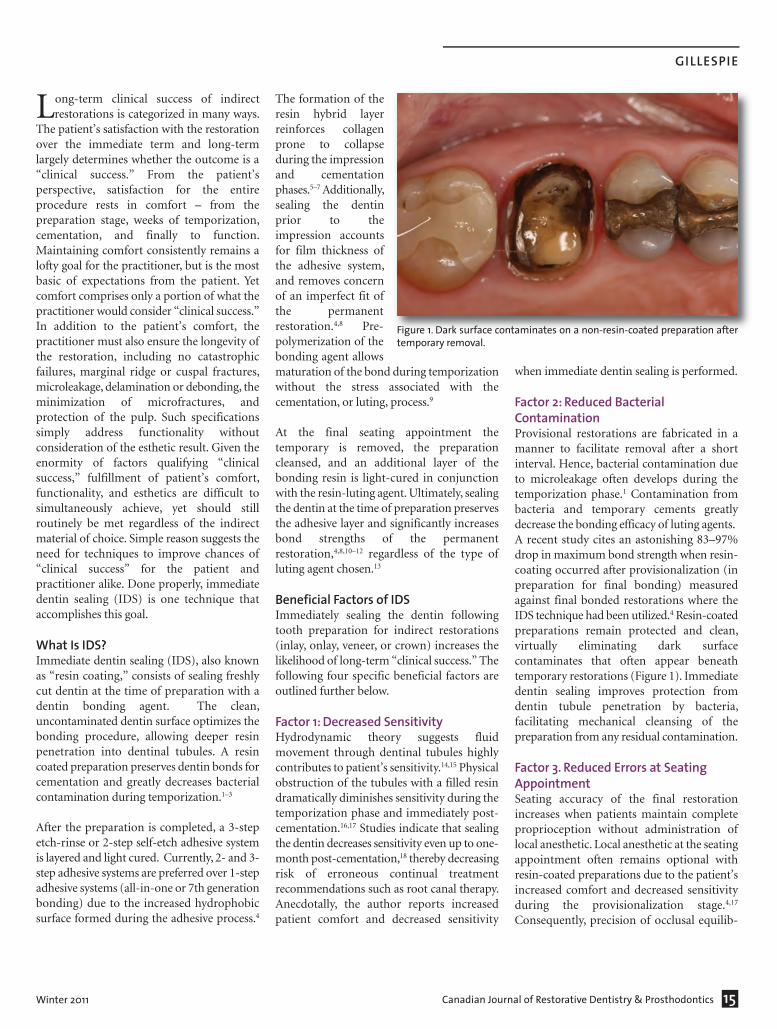
A recent study cites an astonishing 83–97%drop in maximum bond strength when resin-coating occurred after provisionalization (inpreparation for final bonding) measuredagainst final bonded restorations where theIDS technique had been utilized.4 Resin-coatedpreparations remain protected and clean,virtually eliminating dark surfacecontaminates that often appear beneathtemporary restorations (Figure 1). Immediatedentin sealing improves protection fromdentin tubule penetration by bacteria,facilitating mechanical cleansing of thepreparation from any residual contamination.
Factor 3. Reduced Errors at Seating AppointmentSeating accuracy of the final restorationincreases when patients maintain completeproprioception without administration oflocal anesthetic. Local anesthetic at the seatingappointment often remains optional withresin-coated preparations due to the patient’sincreased comfort and decreased sensitivityduring the provisionalization stage.4,17
Consequently, precision of occlusal equilib-
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 15
Figure 1. Dark surface contaminates on a non-resin-coated preparation aftertemporary removal.
16 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
IMMEDIATE DENTIN SEALING: INCREASING LONG-TERM PREDICTABILITY OF INDIRECT RESTORATIONS
ration and adjustment increases leading togreater initial patient satisfaction.
Factor 4. Increased Bond StrengthsPerhaps most compelling, current researchdemonstrates immediate dentin sealing maysignificantly improve shear bond strength.4,8,10–12, 21 Remarkably, no statistically significantdifferences in bond strengths were recordedwith direct immediate bonding (i.e., directbonding with composite resin) versus delayedbonding with resin-coated preparations seatedafter 2,7, and 12 weeks of provisionalization.4
Increased shear bond strengths were foundwhen IDS was used with all luting agents;including resin-modified glass ionomer(RMGI), total-etch adhesives, and self-adhesive luting cements.13
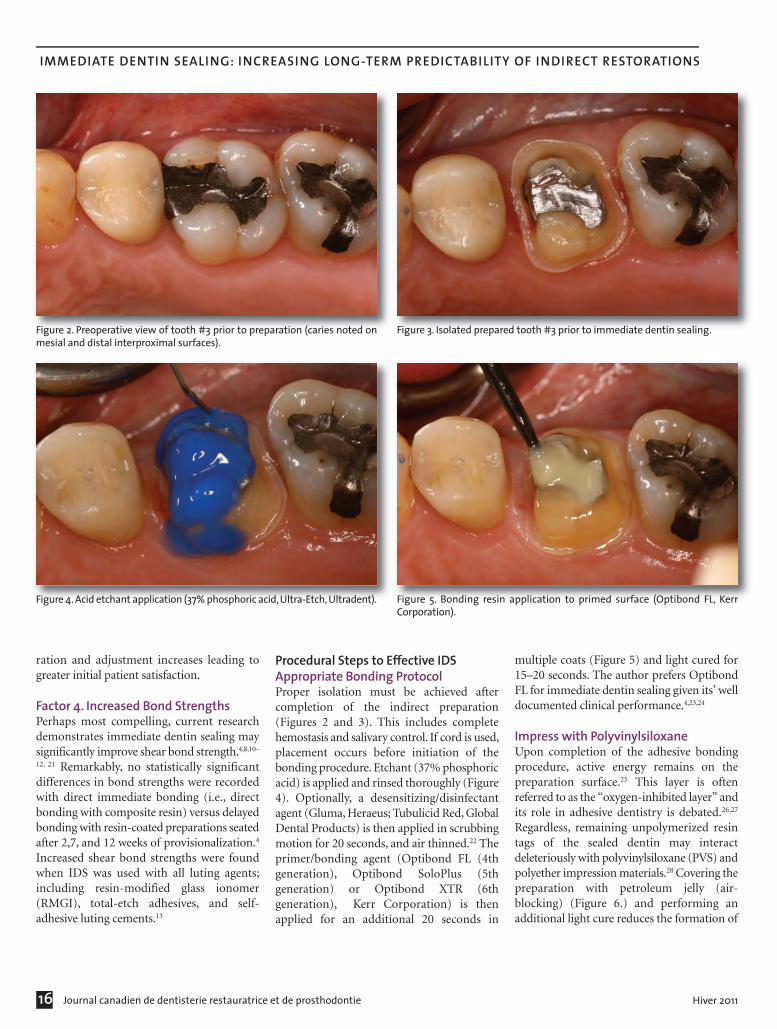
Procedural Steps to Effective IDSAppropriate Bonding ProtocolProper isolation must be achieved aftercompletion of the indirect preparation(Figures 2 and 3). This includes completehemostasis and salivary control. If cord is used,placement occurs before initiation of thebonding procedure. Etchant (37% phosphoricacid) is applied and rinsed thoroughly (Figure4). Optionally, a desensitizing/disinfectantagent (Gluma, Heraeus; Tubulicid Red, GlobalDental Products) is then applied in scrubbingmotion for 20 seconds, and air thinned.22 Theprimer/bonding agent (Optibond FL (4thgeneration), Optibond SoloPlus (5thgeneration) or Optibond XTR (6thgeneration), Kerr Corporation) is thenapplied for an additional 20 seconds in
multiple coats (Figure 5) and light cured for15–20 seconds. The author prefers OptibondFL for immediate dentin sealing given its’ welldocumented clinical performance.4,23,24
Impress with PolyvinylsiloxaneUpon completion of the adhesive bondingprocedure, active energy remains on thepreparation surface.25 This layer is oftenreferred to as the “oxygen-inhibited layer” andits role in adhesive dentistry is debated.26,27
Regardless, remaining unpolymerized resintags of the sealed dentin may interactdeleteriously with polyvinylsiloxane (PVS) andpolyether impression materials.28 Covering thepreparation with petroleum jelly (air-blocking) (Figure 6.) and performing anadditional light cure reduces the formation of
Figure 2. Preoperative view of tooth #3 prior to preparation (caries noted onmesial and distal interproximal surfaces).
Figure 3. Isolated prepared tooth #3 prior to immediate dentin sealing.
Figure 4. Acid etchant application (37% phosphoric acid, Ultra-Etch, Ultradent). Figure 5. Bonding resin application to primed surface (Optibond FL, KerrCorporation).

GILLESPIE
that layer4,28. The preparation is furtherscrubbed with alcohol, or hand-piecemanipulation with pumice to ensure nointeraction of surface energy with impressionmaterials. PVS impression materials setproperly and record accurate impressions afteraltering the active surface (Figures 7 and 8),whereas polyether impression materials stilldemonstrated incomplete setting reactionsunder similar conditions.28
Excess resin at the margin impedes subgingivalpenetration of the impression material. Thisis eliminated through the removal of the topcord (when using a double cord technique) orby carefully moving an explorer around theboarder of the margin while maintaininghemostatsis.
Temporary FabricationResin based temporaries bond to sealedpreparations unless a separating agent isapplied. Petroleum jelly or Pro-V coat (Bisco)must be liberally applied before fabrication ofthe temporary.4,17 Additionally, utilization ofnon-resin temporary cements (TempbondNE, Kerr Corporation) diminish chances ofbonding a temporary restoration to resin-coated preparations4 (Figure 9).
Cementation ProtocolThe practitioner will notice the absence ofdark bacterial contamination upon temporaryremoval (Figure 10). Mechanical mani-pulation with pumice and chlorhexidine scrubensures a clean surface for bonding the lutingagent (Figure 11). The practitioner chooses an
appropriate luting agent; all types arecompatible with immediate dentin sealing.13
The priming step may be omitted but a freshlayer of bonding agent is applied then light-cured in conjunction with the resin lutingcement when utilizing a total-etch bondingtechnique for cementation (NX3, KerrCorporation) (Figure 12 to 14). Thecementation procedure is unchanged with aprimed resin cement (Multilink Automix,Ivoclar Vivadent) or self-adhesive resin cement(Maxcem Elite, Kerr Corporation).
ConclusionsImmediate dentin sealing enhances long-term“clinical success” for both the patient andpractitioner. The extra steps required overtraditional preparation and provisionalization
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 17
Figure 6. Petroleum jelly application prior to additional light cure (air-blocking). Figure 7. Extrusion of low-viscosity polyvinylsiloxane impression material (Take1 Advance, Kerr Corporation).
Figure 8. Final impression of resin-coated preparation (note proper set of PVSmaterial).
Figure 9. Seating of temporary restoration with non-resin temporary cement(Tempbond NE, Kerr Corporation).

18 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
IMMEDIATE DENTIN SEALING: INCREASING LONG-TERM PREDICTABILITY OF INDIRECT RESTORATIONS
techniques more than recuperate time lost with the positive advantagesgained. The patient’s comfort is enhanced with decreased sensitivityand increased seating accuracy, while the practitioner’s confidence isreinforced through reduced bacterial contamination and improvedbond strengths.
ConflictsDr. Gillespie has received financial support from Kerr Corporation.
References1. Paul SJ, Schärer P. The dual bonding technique: a modified
method to improve adhesive luting procedures. Int J PeriodonticsRestorative Dent 1997;17:536–45.
2. Cagidiaco MC, Ferrari M, Garberoglio R, et al. Dentin contamination protection after mechanical preparation for veneering. Am J Dent 1996;9(2):57–60.
3. Pashley EL, Comer RW, Simpson MD, et al. Dentin permeability: sealing the dentin in crown preparations. Oper Dent 1992;17(1):13–20.
Figure 10. Clean preparation immediately following temporary removal (noteabsence of bacterial contamination).
Figure 11. Mechanical cleansing of preparation with 2% chlorhexidine.
Figure 12. Luting final restoration (E.Max, Ivoclar Vivadent) with total-etch resincement (NX3, Kerr Corporation).
Figure 13. Easy clean up of gel phase following tack cure of resin luting agent(NX3, Kerr Corporation).
Figure 14. Final buccal view of bonded restoration (note natural transition fromrestoration to natural tooth structure).

GILLESPIE
4. Magne P, So WS, Cascione D. Immediatedentin sealing supports delayed restoration placement. J ProsthetDent 2007;98(3):166–74.
5. Dietschi D, Magne P, Holz J. Bonded to tooth ceramic restorations: in vitro evaluation of the efficiency and failure mode of two modern adhesives. SchweizMonatsschr Zahnmed 1995;105(3):299–305.
6. Dietschi D, Herzfeld D. In vitro evaluation of marginal and internal adaptation of class II resin composite restorations after thermal and occlusal stressing. Eur J Oral Sci 1998;106(6):1033–42.
7. Frankenberger R, Sindel J, Krämer N, et al. Dentin bond strength and marginal adaptation: direct composite resins vs ceramic inlays. Oper Dent 1999;24(3):147–55.
8. Magne P, Kim TH, Cascione D, DonovanTE. Immediate dentin sealing improves bond strength of indirect restorations. J Prosthet Dent 2005;94(6):511–9.
9. Dietschi D, Monasevic M, Krejci I. Marginal and internal adaptation of classII restorations after immediate or delayedcomposite placement. J Dent 2002;30(5-6):259–69.
10. Jayasooriya PR, Pereira PN, Nikaido T. Efficacy of a resin coating on bond strengths of resin cement to dentin. J Esthet Restor Dent 2003;15(2):105–13.
11. Ozturk N, Aykent F. Dentin bond strengths of two ceramic inlay systems after cementation with three different techniques and one bonding system. J
Prosthet Dent 2003;89(3):275–81.12. Okuda M, Nikaido T, Maruoka R.
Microtensile bond strengths to cavity floor dentin in indirect composite restorations using resin coating. J Esthet Restor Dent 2007;19(1):38–46
13. Johnson GH, Hazelton LR, Bales DJ, et al.The effect of a resin-based sealer on crown retention for three types of cement.J Prosthet Dent 2004;91(5):428–35.
14. Al-Sabbagh M, Andreana S, Ciancio SG.Dentinal hypersensitivity: review of aetiology, differential diagnosis, prevalence, and mechanism. J Int Acad Periodontol 2004;6(1):8–12.
15. Brännström M, Aström A. The hydrodynamics of the dentine; its possiblerelationship to dentinal pain. Int Dent J 1972;22(2):219–27.
16. Trowbridge HO, Silver DR. A review of current approaches to in-office management of tooth hypersensitivity. Dent Clin North Am 1990;34(3):561–81.
17. Morgan MJ, Brown DJ, Suh BI. Immediate Dentin Sealing (IDS). Inside Dentistry 2010;3:84–87.
18. Hu J, Zhu Q. Effect of immediate dentinsealing on preventive treatment for postcementation hypersensitivity. Int J Prosthodont 2010;23(1):49–52.
19. Frankenberger R, Lohbauer U, TaschnerM, et al. Adhesive luting revisited: influence of adhesive, temporary cement,cavity cleaning, and curing mode on internal dentin bond strength. J Adhes Dent 2007;9 Suppl 2:269–73.
20. Bagis B, Bagis YH, Hasanreisoglu U. Bonding Effectiveness of a Self-adhesive
Resin-based Luting Cement to Dentin After Provisional Cement Contamination. J Adhes Dent 2010. doi: 10.3290/j.jad.a19811.
21. Islam MR, Takada T, Weerasinghe DS, etal. Effect of resin coating on adhesion of composite crown restoration. Dent MaterJ 2006;25(2):272–9.
22. Saraç D, Bulucu B, Saraç YS, Kulunk S. The effect of dentin-cleaning agents on resin cement bond strength to dentin. J Am Dent Assoc 2008;139(6):751–8.
23. Poitevin A, De Munck J, Cardoso MV, etal. Dynamic versus static bond-strength testing of adhesive interfaces. Dent Mater2010;26(11):1068–76.
24. Stavridakis MM, Krejci I, Magne P. Immediate dentin sealing of onlay preparations: thickness of pre-cured Dentin Bonding Agent and effect of surface cleaning. Oper Dent 2005;30(6):747–57.
25. Tsujimoto A, Iwasa M, Shimamura Y, et al. Enamel bonding of single-step self-etch adhesives: influence of surface energycharacteristics. J Dent 2010;38(2):123–30.
26. Ghivari S, Chandak M, Manvar N. Role of oxygen inhibited layer on shear bond strength of composites. J Conserv Dent 2010;13(1):39–41.
27. Suh BI. Oxygen-inhibited layer in adhesion dentistry. J Esthet Restor Dent 2004;16(5):316–23.
28. Magne P, Nielsen B. Interactions betweenimpression materials and immediate dentin sealing. J Prosthet Dent 2009;102(5):298–305.
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 19

The current clinical model ofrestorative and esthetic dentistry
is founded upon highly invasiverestorative techniques. The long-termeffects of this over-preparation arechronic destruction of the dentition,resulting in the high-end care that isso often promoted at seminars todental practitioners.
Minimal intervention esthetic
dentistry is not about drilling smallercavities or conservative crownpreparations, but the re-evaluation oftreatment modalities based on thepharmacological management ofdental disease and changes to thecurrent amputation model of clinicalcare. Since the late 1990s it has beenacknowledged that caries infecteddentine will stabilize beneath arestoration1 and that creating a
biological seal at the cavo margin(isolating the lesion from the overlyingbiofilm) reduces the viability ofbacteria remaining within the lesionand prevents further cariesprogression.2
Despite this, many dentists strive toremove caries-infected dentine duringcavity preparation and leave behindthe slightly demineralized caries
20 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
ESTHETIC DENTISTRY / DENTISTERIE ESTHÉTIQUE
ABSTRACTThe current clinical model of restorative and esthetic dentistry is founded upon highly invasive restorativetechniques. These lead to the chronic destruction of dentition, resulting in a need for high-end care.Enlightened restorative dentistry should be based upon mineralization rather than mutilation, and estheticdentistry should be based upon augmentation rather than amputation. This article discusses several optionsin minimally invasive dentristry.
RÉSUMÉLe modèle clinique courant de dentisterie restauratrice et esthétique est fondé sur des techniquesrestauratrices très invasives. Ce qui entraîne la destruction chronique de la dentition et le besoin de soins dehaut de gamme. La dentisterie restauratrice éclairée devrait être fondée sur la minéralisation plutôt que surla mutilation, tandis que la dentisterie esthétique devrait être fondée sur la mise en valeur plutôt que surl’amputation. Cet article traite des diverses options de dentisterie peu invasive.
Minimal Intervention Esthetic Dentistry
Intervention minimale en dentisterie esthétique
By Dr. Geoff Knight BDSc, MSc, MBA, PhD
About the Author
Geoff Knight is a general dentist and internationally noted dental speaker with special interests inminimal intervention esthetic dentistry.
He has pioneered a number of innovative clinical procedures in esthetic dentistry and thepharmacological management of caries. He has consulted widely across the dental industry and isnamed on several patents.
He has been published in Quintessence International, Australian Dental Journal, and Journal ofPeriodontal Research. He has produced a series of clinical videos and written numerous articles onesthetic and adhesive dentistry that have been translated and published internationally in a numberof languages

KNIGHT
affected dentine believing it to remineralizeinto sound dentine. This is based upon thewidely held notion that bacterially infecteddentine is irreversibly decomposed, unable toremineralize, and should be removed prior torestoration placement.
The removal of carious dentine prior tocompleting cavity preparation infers that thedentine pulp complex is the only vital tissue inthe body that lacks a front-line physiologicalresponse to bacterial invasion creating a singlepoint of tissue vulnerability in the bodyagainst infection. It has been shown3 thatdemineralized dentine is more effective inreducing the viability of streptococcus mutansthan dentine treated with an antibacterialsubstance (silver fluoride and potassiumiodide) This raises the hypothesis that there aresubstances released by carious dentine thatmay inhibit bacteria viability. Furthermore,when silver fluoride and potassium iodide areapplied to the surface of demineralizeddentine there is a substantial reduction inbacterial viability3 suggesting an anti bacterialsynergism between silver fluoride andpotassium iodide with demineralized dentine. Arrested root caries demonstrates the abilityof a tooth to self heal by remineralization ofcarious tooth structure. Figure 1. Arrestedcaries are inevitably black as sulphur saltsbecome incorporated into the remineralizingtissues. Remineralized lesions remain resistantto further caries attack unless there aredramatic changes in the oral environment.This is partly due to the remineralizationprocess that transforms carbonated apatite
with a demineralization pH of around 5.5 intoa complex of hydroxyl and fluorapatite4 thatresists demineralization to a pH of around 4.5.Preventing biofilm formation prevents cariesprogression.2 Both the application of ozone5
and silver fluoride/ potassium iodide6 todentine prevents biofilm formation and mayplay a role in caries management.
Glass Ionomer Cements Glass ionomer cements pharmacologicallyassist with the remineralization of cariousdentine by providing a source of fluoride,calcium, or strontium ions (depending uponthe glass ionomer used) that can penetrateover 100 microns into dentine to assist withthe formation of hydroxyl and fluorapatite inthe demineralized tissue.7,8 Glass ionomercements have further benefits when treatingcaries as they prevent demineralization at theperimeter of the restoration unlike compositeresin that offers no such protection.
The Pharmacological Management ofDental Caries Following is an approach for thepharmacological management of a cariouslesion using silver fluoride/potassium iodideand glass ionomer cement:
• Figure 2 shows occlusal caries on an upper second molar.
• Enamel was removed and a moat was prepared in sound dentine with a #3 slow-speed round bur at the dentino-enamel junction around the perimeter ofthe caries (Figure 3).
• The preparation was etched with 37% phosphoric acid for 5 seconds, washed with water, and dried with oil free air (Figure 4).
• Silver fluoride was applied to the preparation, with a microbrush (Figure 5).
• This was followed by potassium iodide until the precipitation turned from cloudy white to clear (Figure 6).
• The cavity was then washed and dried with oil free air (Figure 7).
• After isolating the preparation from moisture with cotton rolls, an auto-cure glass ionomer cement was placed into thepreparation to slightly overfill the cavity.Silver fluoride/potassium iodide enhances the bond strength between autocure glass ionomer and dentine10
(Figure 8). • A 3 cm square piece of freezer bag was
placed over the unset glass ionomer andthe patient asked to occlude into centric occlusion for 4 minutes until the glass ionomer had cured (Figure 9).
• As the freezer bag acted as an occlusal matrix, once the glass ionomer had set, minimal contouring was required to complete the restoration (Figure 10).
Cosmetic Dentistry Dental implants have unquestionablyimproved the well-being of millions of peopleover the past 30 years and dentists areconstantly invited either by mail or theInternet to attend courses that will improvetheir skills in this particular facet of dentistry.
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 21
Figure 1. Arrested caries. Figure 2. Occlusal cavity in upper second molar.

22 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
MINIMAL INTERVENTION ESTHETIC DENTISTRY
Figure 3. Open lesion through enamel to expose caries. Figure 4. Etch with phosphoric acid for 5 seconds, wash and dry.
Figure 5. Apply Riva Star Solution 1 (silver fluoride). Figure 6. Apply Riva Star Solution 2 (potassium iodide). Apply solution untilwhite precipitate clears.
Figure 7. Wash and dry cavity prior to glass ionomer placement. Figure 8. Apply auto-cure glass ionomer cement into cavity.

KNIGHT
While before and after photographs areimpressive, the astute observer would like tosee pictures of the same prosthesis beyond 10years for while there is more than 30 years ofclinical experience with dental implants long-term clinical photographs do not seem to bepart of the promotional literature.
A recent study measuring the success of dentalimplants of 10 years and beyond confirms thehigh retention rate. However, when theincidence of peri-implantitis and mechanicalproblems with the prosthetics are factored in,the percentage of implants free ofcomplications was less than 50%. 11,12 This maywell be less successful than other prostheticprocedures dentists apply to the dentition andis a timely reminder that there is a continual
maintenance factor that has to be taken intoaccount with implant use. The rigidity of animplant in a flexing dentition would suggestan increased propensity for porcelain tofracture in this environment. A porcelaincrown on a root filled tooth may be less proneto fracturing than an implant supportedcrown in the same location. Non-invasive Management of a Missing Upper Incisor The following clinical case is presented to showthere are conservative options that provide afunctional and esthetic alternative to replacinga missing tooth.
• Figure 11 shows a patient with a fracturedroot on an upper right central incisor thatrequired extraction.
• The clinical situation was managed by placement of a direct resin bridge without tissue preparation. Figure 12 shows the prosthesis 16 years after placement.
• Lingual view of direct resin bridge showing conservative preparation (Figure 13).
Conclusions The current clinical model of restorative andesthetic dentistry leads to the chronicdestruction of the dentition. Enlightenedrestorative dentistry should be based uponmineralization rather than mutilation andesthetic dentistry should be based uponaugmentation rather than amputation.
Silver fluoride has been used to arrest caries,
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 23
Figure 10. Minimal contouring required to complete the restoration.
Figure 11. Fractured root of upper central incisor. Figure 12. Direct composite resin bridge 16 years after initial placement.
Figure 9. Place a freezer bag over the occlusal surface of the cavity and ask thepatient to close in retruded occlusion for 4 minutes until the restoration sets.
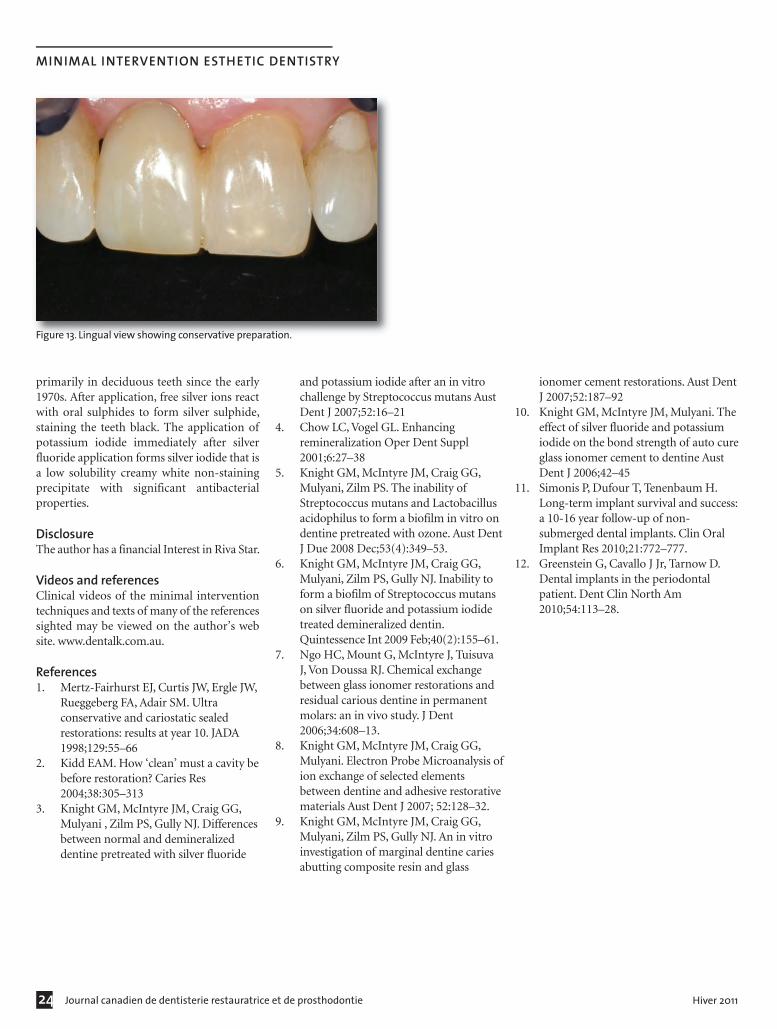
24 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
MINIMAL INTERVENTION ESTHETIC DENTISTRY
primarily in deciduous teeth since the early1970s. After application, free silver ions reactwith oral sulphides to form silver sulphide,staining the teeth black. The application ofpotassium iodide immediately after silverfluoride application forms silver iodide that isa low solubility creamy white non-stainingprecipitate with significant antibacterialproperties.
Disclosure The author has a financial Interest in Riva Star.
Videos and references Clinical videos of the minimal interventiontechniques and texts of many of the referencessighted may be viewed on the author’s website. www.dentalk.com.au.
References 1. Mertz-Fairhurst EJ, Curtis JW, Ergle JW,
Rueggeberg FA, Adair SM. Ultra conservative and cariostatic sealed restorations: results at year 10. JADA 1998;129:55–66
2. Kidd EAM. How ‘clean’ must a cavity bebefore restoration? Caries Res 2004;38:305–313
3. Knight GM, McIntyre JM, Craig GG, Mulyani , Zilm PS, Gully NJ. Differencesbetween normal and demineralized dentine pretreated with silver fluoride
and potassium iodide after an in vitro challenge by Streptococcus mutans AustDent J 2007;52:16–21
4. Chow LC, Vogel GL. Enhancing remineralization Oper Dent Suppl 2001;6:27–38
5. Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS. The inability of Streptococcus mutans and Lactobacillusacidophilus to form a biofilm in vitro ondentine pretreated with ozone. Aust DentJ Due 2008 Dec;53(4):349–53.
6. Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. Inability to form a biofilm of Streptococcus mutans on silver fluoride and potassium iodide treated demineralized dentin. Quintessence Int 2009 Feb;40(2):155–61.
7. Ngo HC, Mount G, McIntyre J, Tuisuva J, Von Doussa RJ. Chemical exchange between glass ionomer restorations and residual carious dentine in permanent molars: an in vivo study. J Dent 2006;34:608–13.
8. Knight GM, McIntyre JM, Craig GG, Mulyani. Electron Probe Microanalysis ofion exchange of selected elements between dentine and adhesive restorativematerials Aust Dent J 2007; 52:128–32.
9. Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. An in vitro investigation of marginal dentine caries abutting composite resin and glass
ionomer cement restorations. Aust DentJ 2007;52:187–92
10. Knight GM, McIntyre JM, Mulyani. Theeffect of silver fluoride and potassium iodide on the bond strength of auto cureglass ionomer cement to dentine Aust Dent J 2006;42–45
11. Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success:a 10-16 year follow-up of non-submerged dental implants. Clin Oral Implant Res 2010;21:772–777.
12. Greenstein G, Cavallo J Jr, Tarnow D. Dental implants in the periodontal patient. Dent Clin North Am 2010;54:113–28.
Figure 13. Lingual view showing conservative preparation.

CONTINUING EDUCATION IN DENTISTRY /ÉDUCATION CONTINUE EN DENTISTERIE
Dentists are inundated withadvertisements and promises of
new materials and technologies atevery turn. Keeping up has become afull-time job with the difficulty ofdetermining which of these so-calledpromises merit introduction into one’sregular practice activity. There is nobetter place to make these decisionsthan a study club.
Dentistry has long followed thementorial model where an expert in a
specific subject shares knowledge withdentists who become his students.Study club activities vary fromprovince to province and country tocountry, but some noticeable trendsare apparent. Evening sessions or studyclubs generally follow the format of amentor lecture followed by discussionand perhaps case presentations. Someliterature reviews can occur but theseactivities are short and sweet and onlyuseful to a degree. Frequently thegroup will have dinner in association
with the activity and this can, onoccasion and unfortunately, becomethe principal reason for attending.
In Ontario the lecture methodpredominates as the learningexperience. Centers like The DentalLearning Centres in Oakville offer alecture room with adjacent clinicaldemonstration suite www.tdlc.ca formore information). In Toronto theCentre for Continuing DentalEducation of the University of
Mastering Clinical Advancements
Gérer les progrès cliniques
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 25
ABSTRACTThe learning process leading to changes in the way dentists provide clinical services for their clients can be aslow and arduous journey. Changes suggested by advertisements, journal articles, technician suggestions andlectures attended, require effort for us to implement in our practices. The mentor/clinical application modelwhich is a principal method in British Columbia is encouraged for greater application across Canada.
RÉSUMÉLe processus d’apprentissage menant aux changements dans la façon dont les dentistes fournissent desservices cliniques à leurs clients peut être un parcours lent et ardu. Les changements suggérés par lesannonces, les articles de journaux, les techniciens et la participation à des conférences exigent un certaineffort de notre part pour mettre ces changements en pratique. Le modèle d’application clinique/mentor,principale méthode en Colombie-Britannique, est encouragé partout au Canada.
By Dr. John N. Nasedkin, DDS, FRCD(C), FADM
About the Author
Dr. Nasedkin is a consultant prosthodontist in Vancouver Canada, who has taught occlusion/TMJ andesthetics on every continent. He is a past-president of the American Equilibration Society and a memberof the Pacific Coast Society of Prosthodontists, CARDP, the American Academy of Cosmetic Dentistry,and other many prestigious organizations. He is the co-editor of the book, Occlusion: The State of theArt. He is the mentor of the first esthetic study club in Canada and a clinical assistant professor at theUniversity of British Columbia. He can be contacted at: [email protected] or www.drnasedkin.com.

Toronto, is a beautifully equipped lecture roomin a central setting (visit www:utoronto.ca/cdefor more details). Various other groups withspecific interests have established programswhich sometimes use the operatories ofdentist’s offices for clinical learning programson weekends. Interestingly the predominantclinical programs in Ontario are almostexclusively related to implant surgicaltreatments.
In BC we have a long tradition of clinicalrestorative study clubs dating back nearly 100years. The original groups were the foil studyclubs which have morphed into the AmericanAcademy of Gold Foil Operators. Several of thegold foil study club mentors became theformative instructional staff when theUniversity of Washington dental school wasbegun in the post-war period.
For more than 25 years, we had a clinicalteaching facility at the College of DentalSurgeons of BC in Vancouver. This was recentlyrevitalized by the Study Club Alliance of BCand re-opened as the Sirona Learning Centre.Here we have a 30-seat lecture room, anadjacent glassed demonstration operatory, and
12 fully equipped dental chairs. The prevailingstudy club model is a half day per month inwhich a lecture is followed by clinicalexperience on the dentist’s patient to convertknowledge at a challenge level into clinicalexperience. We also have a complete clinic forcontinuing dental education at UBC. There isa complete webcasting camera set-up so thedemonstrations and lectures can betransmitted on-line across the province(www.sironalearningcentre.org).
My own study club is known as TEST – TheEsthetic Study Team – meeting for 26 years.The accompanying photos were taken at ourJanuary session where Corrie Paulsen of 3MEspe conducted a Digital Impressioningclinical workshop on the Lava Chairside OralScanner. Our current theme is CAD/CAMrestorations and we will next meet withrepresentatives of CEREC and use the ACBluecam for digitally scanning then designingand completing restorations using the In-Labmilling machine. In September of 2008 we hada clinical demonstration of the iTero scanner.Our objective is for each member or our groupto develop personal experience with the use ofdigital technology.
Dental assistants and staff members areencouraged to participate in the clinicalteaching sessions since it is their understandingand commitment to a process which insures itssuccessful application. Study club members areprovided with teaching aids to assist in thisimplementation for use in staff meetings andin the essential training sessions required for allfor staff members.
Dentistry’s challenges are minimized by first-hand experience. The objective of clinicalworkshops and study clubs is to directlytransfer new information into everydayskillsets.
Even when assisting a colleague, a dentist addsto his/her memory bank of case history andsome experience which is useful in one’s ownoffice. In Canada the learning experience variesfrom province to province and within theprovinces themselves. We encourage the use ofthe mentor/clinical model for your esthetic andrestorative advancement in continuing dentaleducation.
26 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
MASTERING CLINICAL ADVANCEMENTS
2011 Annual Scientific Meeting
September 22-24, Toronto, Ontario
Dr. David Monaghan prepares a crown with the microscope.
Dr. Monaghan scans his tooth preparation. Dr. Ed Lowe, Dr. Baird, and Corrie Paulsen prepare data for transmission to theLAVA milling facility.
Dr. Brian Baird scans his preparation watched by members of TEST and CorriePaulsen in the white coat.
NASEDKIN
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 27
Congrès annuel 201122 au 24 Septembre, Toronto, Ontario

28 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
A Collaborative Approach to Patient Care: Keys to Success
Les clés du succès : Une approche collaborative aux soins du patient
CASE REPORT / RAPPORT DE CAS
ABSTRACTToday dentists are challenged with an increased complexity in esthetic challenges and demands. We are facedwith an ever-changing selection of materials, procedures and requests from patients. Furthermore, manypeople present with aesthetic, functional, and occlusal problems that require extensive treatment. At theheart of all this is what is best for our patients to achieve their treatment goals. Communication with thepatient and the entire team of dentists and specialists is important to achieve treatment success. Thefollowing clinical case will review the concept of true interdisciplinary dentistry and how the restorativedentist working harmoniously with specialists can achieve more predictable and stable results for theirpatients.
RÉSUMÉDe nos jours, les dentistes doivent savoir répondre aux besoins de plus en plus complexes des patients enmatière de dentisterie esthétique. Le choix des matériaux, des procédures et les demandes de la part despatients changent constamment. De plus, de nombreux patients présentent des problèmes esthétiques,fonctionnels et occlusaux qui requièrent un traitement parfois très long. Ce qui en ressort en bout de lignec’est la satisfaction des patients qui ont obtenu ce qu’ils désiraient. La communication avec le patient etl’équipe de dentistes et de spécialistes est importante à la réussite du traitement. Le cas clinique suivantpassera en revue le concept de la vraie dentisterie interdisciplinaire et la façon dont les praticiens en dentisterierestauratrice travaillant en harmonie avec les spécialistes peuvent obtenir des résultats prévisibles etsouhaités.
By Dr. Paresh Shah, DMD, MS, Cert. Esthetic Dentistry
About the Author
Dr. Paresh Shah has been in private practice in Winnipeg since 1992. His post-secondary education atthe University of Manitoba includes a BSc (microbiology) in 1983, a MSc. (physiology) in 1987, and a DMD.in 1991. Dr. Shah’s interests and expertise lie in cosmetic, restorative, and implant dentistry. He has takenover 1,000 hours of advanced education from programs all over North America.
Besides serving as a past board member for the Manitoba Dental Association, Dr. Shah is currently onthe executive of the Canadian Academy of Esthetic Dentistry as a founding member. Dr. Shah is also in-volved in organized dentistry, clinical teaching, and serves as a clinical consultant for several dentalmanufacturers.

SHAH
Esthetic dentistry in today’s termsencompasses much more than having a
straight, white smile. Our patient’s not onlywant to look better and feel younger, theirexpectations are far greater. What’s estheticallypleasing to one person may not be for the next.Ideal esthetics should not only deal withappearance, but also provide optimal functionand stability. There’s little point of havingbrighter teeth if the restorations last for only ayear or don’t allow you eat or speak properly?Furthermore, dentistry is not only far moresophisticated today, but the expectations ofour patients quite often transcend the “usualand customary” of basic general dentistry andinvolves many aspects of the specialtydisciplines. It has become more common tofind orthodontists, periodontists, and oralsurgeons working as a team to help coordinatea healthy, stable, and optimally esthetic result.To achieve these results it is imperative for thespecialists involved to have a workingunderstanding of the restorative challengesand goals from the outset. To that end, it isequally imperative that the restorative dentistalso has a good working knowledge of otherrelated disciplines. We all know that restorativedentistry, periodontal health, materialselection, and occlusion are the foundation of
an average general practice. However, intoday’s climate that may not be enough toprovide the most optimal treatment for manyof our patients. The restorative dentist has anobligation to integrate and facilitate thedisciplines necessary to create the mostfunctionally stable and esthetic result whenrequired. A variety of disciplines may benecessary to achieve successful completion ofthe patient’s treatment goals. These mayinclude any of the following: orthodontics,oral surgery, periodontal therapy/surgery, andperhaps orthognathic surgery.
The concept of interdisciplinary dentistry isnot a new one. Many dentists may believe theypractice interdisciplinary dentistry, but it’show the process is managed and carried outthat is most important. This requires a changein how we approach our patients in everydaygeneral practice.1 It also requires gaining theextra knowledge to be able to treat these casesproperly. Peter Dawson has said: “to have anaccurate starting point, every problem to longterm health must be recognized … planningthe complete process to a visualized end pointshould come first.”2 Richard Roblee separatesthe various levels of dentofacial therapy intothree main categories: unidisciplinary therapy,
multidisciplinary therapy, and inter-disciplinary therapy.3,4 Each approach varies intheir degree of sophistication and similarly intheir degree of success. Interdisciplinarydentistry involves a structured collaborationbetween the restorative dentist and thespecialists involved in the patient treatment.Furthermore, there is a common workingknowledge between all parties. The providerswork together, think alike, and have commongoals for the patient’s complete treatmentplan. The following case provides an exampleof how treatment can get side-tracked withoutadequate communication and provides somesolutions on how to perhaps avoid similarconsequences when a group workscollaboratively during treatment.
Case ReportA 20-year-old female patient presented withnumerous congenitally missing teeth that shewished to have replaced with dental implants.She was happy with her appearance andcurrent smile (Figure 1) but wasn’t thrilledwith having to indefinitely wear retainers toreplace her missing teeth (Figure 2). On initialexamination, it was apparent that some of hertooth proportions and tissue heights were outof balance (Figure 3), but she stated that this
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 29
Figure 1. Smile (unretracted) initial presentation. Figure 2. Smile (retracted) initial presentation with retainers to replace missingteeth.
Figure 3. Smile (retracted) initial presentation without retainers.

30 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
A COLLABORATIVE APPROACH TO PATIENT CARE: KEYS TO SUCCESS
was never a concern of hers and that shesimply wanted to have her missing teethreplaced with dental implants. When thesubject of orthodontics was suggested thepatient explained that she had alreadycompleted 4.5 years of orthodontic treatmentand has been wearing retainers for almost 9months. She had already seen some otherspecialists but her treatment had not beenfollowed up by anyone and thecommunication between the providers wasnot consistent.
We received permission to update someradiographs and contact her orthodontist toobtain some history on her treatment. It was
evident from the panoramic radiograph andintraoral views (Figures 4 and 5) that therewere missing permanent teeth, retainedprimary teeth, and inadequate root alignmentsto facilitate ideal implant placement. Herorthodontist explained that there was little tono communication between the variousdentists and specialists involved so no idealgoals regarding implant therapy werediscussed initially. He was happy to retreat thepatient once a comprehensive treatment wasdeveloped if she so chose. At this stage, Isuggested a consultation with the orthodontistand oral surgeon would be helpful anddeveloped a diagnostic wax-up of ourtreatment goals in consultation with the
patient (Figure 6).
At the interdisciplinary consultation visit thetreatment goals of the patient were reviewedwith the oral surgeon and orthodontist. Themounted diagnostic wax-up gave all providersa “road map” of treatment objectives. The oralsurgeon asked that he be kept apprised of theroot positioning as orthodontics continued sothat he would have adequate room for implantplacement. The patient was also informed thatbone grafting would be required afterorthodontics. The patient resumedorthodontics once again (Figure 7) andprogress was monitored closely from arestorative and surgical point of view by all
Figure 7. Orthodontic retreatment to correct alignment.
Figure 4. Panoramic radiograph displaying missing permanent dentition andinadequate root spacing for implants.
Figure 5. Periapical radiographs (maxillary anteriors) on initial presentationdisplaying inadequate spacing and root alignments for implants.
Figure 8. Periapical radiographs to monitor progress of root alignment andspacing. Root alignments are approaching a more favourable position forimplant placement.
Figure 9. Diagnostic waxup to final contour to assess for bone grafting andimplant placements.
Figure 6. Mounted diagnostic casts (wax-up) to visual and discuss idealizedgoals.

SHAH
three providers. Progressive periapicalradiographs were taken throughout theorthodontic treatment and shared with theoral surgeon (Figure 8). We also tookmeasurements of the coronal spacing to assurethe widths of the prosthetic teeth would bebalanced. The patient wasn’t concerned abouttissue heights as her smile didn’t reveal thosefeatures. She had already now reached over 5years of orthodontics and wished to achieveher goal of receiving implants rather thanperfecting every detail of her smile.
Once adequate space appropriation5 wasachieved and the root alignments deemedsuitable by the surgeon, another mounted
diagnostic wax-up was made to allowfabrication of surgical guides for bone graftingand subsequent implant placements (Figures9 and 10). The patient continued to wearretainers, which we modified to fit over thefollowing year while her bone grafting (iliaccrest) healed and implants were finally placedby the surgeon. A total of 9 implants wereplaced and once integration was confirmed bythe surgeon, impressions were made to beginthe restorative phase of treatment (Figure 11).We had discussed esthetics from the outset oftreatment with the patient and advised herthat in order to make her smile as pleasing aspossible we had to address the shapes of her ofexisting teeth. Her original central incisors
were narrow and their root forms weredivergent prior to retreatment withorthodontics (see Figures 2 and 3). Hercanines were also quite square on the incisaledge. She once again reiterated that she wasnot concerned about her gingival heights andso the team as a whole did not spend too muchtime focusing on those issues, but rather onthe primary goal of achieving adequatespacing for prosthetics with implants andocclusal harmony. To that end, the laboratoryfabricated custom zirconia abutments for theimplants (Figures 12 and 13). The abutmentswere seated in the mouth to verify adaptationand positioning. (Figure 14). The final designof the restorations was completed after taking
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 31
Figure 10. Surgical guides are provided to the implant surgeon to facilitateappropriate placement.
Figure 11. VPS impression of maxillary implants with impression copings inplace.
Figure 12. Custom zirconia abutments (mandible) with soft tissue.
Figure: 13. Custom zirconia abutments (maxilla) with soft tissue.

32 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
A COLLABORATIVE APPROACH TO PATIENT CARE: KEYS TO SUCCESS
into account the changes in contour required to make the patient’sexisting teeth more symmetrical. This was done using a diagnostic wax-up on the final master cast and approved by the patient (Figures 15 and16). The patient had already committed to extensive treatment withthe implants and restorations that she wasn’t ready to do indirectveneers on her existing teeth at this time. For this reason, we used thediagnostic wax-up as a guide to improve the shape of her existing teethto balance with the implant restorations. This transitional bondingwith a nano-composite using a multiple shade layering techniqueallows for a highly aesthetic result.6,7 The finish and polish retention ofthe composite allowed for a nice match to the ceramic crowns (Figure17). Furthermore because the patient’s occlusion was harmonized andspaces made symmetrical, she is now able to change over hertransitional bonding one unit at a time (or more) depending on herfinancial situation. Her final smile wasn’t altered significantly fromher initial (Figure 18) but we were able to achieve her goals of replacingher missing teeth with dental implants and allowing her not to wearretainers anymore. She now has control over how she will proceed withthe remaining restorations as she sees fit.
SummaryAlthough we could have chosen several other treatment options, thefinal result was deemed a success based on the treatment objectives of
Figure 17. Retracted smile with implant crowns and transitionally bondedcomposite restorations.
Figure 14. Custom abutments seated intra-orally to verify position and fit.
Figure 16. Diagnostic wax-up (mandible) of existing teeth allows finalrestorations to be created in a balanced manner.
Figure 18. Final smile (unretracted) post treatment.
Figure 15. Diagnostic wax-up (maxilla) of existing teeth allows finalrestorations to be created in a balanced manner.

SHAH
the patient. Her primary goal from thebeginning was to have her missing teethreplaced with dental implants. However,somewhere along the way this was not initiallydiscussed in a collaborative fashion among thedentists and specialists involved. By the timethe patient had completed almost 5 years oftreatment, the case had to be reassessed andthe treatment objectives collaborativelyfocused upon by the treating practitioners.Granted, due to her age, it would have beenbest to wait for implant placement until her20s, but she could at least have had lessorthodontic treatment and perhaps someconservative fixed appliances rather than theretainers she didn’t feel comfortable with.
Many practitioners choose to treat all aspectsof a case, sometimes oblivious of thechallenges that lie ahead. If the restorativedentist is not comfortable to perform some ofthe treatment, specialists should be consulted.It is equally important to assemble aninterdisciplinary team of specialists thatunderstand how to work together in astructured manner. The restorative dentist hasan obligation to visualize the end point to
completion and then coordinate the team tomake sure the desired outcome is achieved. Aninterdisciplinary approach allows one toprovide comprehensive treatment to allpatients and provides the ability to stagetreatment for those who cannot afford to doall of it at once. It is critical for all members ofthe team to have a working knowledge of whatthe others are doing and provide structuredcollaboration to achieve the occlusion,function and aesthetics the patient desires.
AcknowledgementsThe author would like to acknowledge thefollowing for their contribution to thetreatment: Dr. D. Sullivan for the orthodontics,Dr. M. Cohen for the implant surgery, and Mr.L. Benga for his lab work.
ConflictsNone declared.
References1. Shah, P. Optimizing esthetics and
function through interdisciplinary dentistry. General Dentistry – Special Esthetics Issue. 2008: 268–72.
2. Dawson, PE. Functional occlusion: FromTMJ to smile design. New York: Elsevier Publishing Inc. 2007.
3. Roblee, RD. Interdisciplinary Dentofacialdentistry: A comprehensive approach to optimal patient care. Chicago: Quintessence Publishing Co. Inc., 1994.
4. Roblee, RD. Interdisciplinary dentistry: 20 Years of evolution. Presented at the AAO Interdisciplinary Conference: Multiple Disciplines, One Focus. February 9-11, 2007 in Palm Springs, CA.
5. Smalley, WM. Comprehensive Interdisciplinary management of Patientswith Missing and/or Abnormally Proportioned Teeth. In: Cohen, M, editor.Interdisciplinary Treatment Planning. Chicago: Quintessence Inc., 2008.
6. Margeas, RC. Keys to success in creating esthetic class iv restorations. In: Journal Compilation. Wilmington, DE: Wiley Periodicals Inc., 2010. 66–71.
7. Rinn LA. Applied theory of color. In: Rinn LA, editor. The polychromatic layering technique—a practical manual for ceramics and acrylic resins. Chicago, IL: Quintessence Publishing; 1990, 11–30.
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 33

34 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
Metal Free Ceramics: A Clinical Case
Céramique sans métal : Un cas clinique
CASE REPORT / RAPPORT DE CAS
ABSTRACTAll-ceramic restorations have been an option largely utilized to restore anterior and posterior teeth due totheir excellent esthetic and several ceramic systems are available in the market to fabricate partial restorationsand crowns. The improvement of the resin cements and adhesive systems has allowed an effective adhesionbetween these materials and the dental structure.
This paper reports the use of an all-ceramic system, IPS Empress from Ivoclar/Vivadent. The background ofthe case is discussed and the clinical diagnosis and treatment plan of a patient are outlined. This clinical reportdescribes the procedures used for the restoration of maxillary anterior teeth and mandibular incisors with aleucite-reinforced system. This case illustrates that ceramic coping with the latest ceramic layering systemsare a highly aesthetic alternative to metal-ceramic restorations.
RÉSUMÉLes restaurations en céramique sont une option largement utilisée pour réparer les dents antérieures etpostérieures en raison de leur excellent caractère esthétique et de la disponibilité sur le marché de plusieurssystèmes pour les restaurations partielles et les couronnes. L’amélioration des résines-ciments et des adhésifsa permis une meilleure adhésion entre ces matériaux et la structure dentaire.
Cet article traite de l’utilisation d’un matériau en céramique, IPS Empress de Ivoclar/Vivadent. L’historique ducas est mentionné et le diagnostic et le plan de traitement ont été schématisés. Ce rapport clinique décrit lesprocédures utilisées pour la restauration des dents antérieures du maxillaire et des incisives de la mandibuleen utilisant une céramique renforcée à la leucite. Ce cas illustre que les couronnes en céramique réalisées avecles derniers systèmes céramo-céramiques sont des options très esthétiques aux couronnes céramo-métalliques.
By Dr. Gildo Coelho Santos Jr., DDS, MSc, PhD; Dr. Andrea Mota, DDS; and Dr. Maria Jacinta Moraes Coelho Santos, DDS, MSc, PhD
About the Authors
Gildo Coelho Santos Jr., DDS, MSc,PhD, is an assistant professor thethe University of Western Ontario,Schulich School of Medicine andDentistry in London, ON. He can bereached at: [email protected].
Maria Jacinta Moraes Coelho Santos,DDS, MSc, PhD is an adjunct professorat the University of Western Ontario,Schulich School of Medicine andDentistry in London, ON.
Andrea Mota, DDS is in clinical practice in Salvador, Bahia, Brazil.

SANTOS ET AL.
While metal-ceramic systems stillrepresent a high-strength mode of
treatment associated with positive long-termsuccess rates, there are a number ofdisadvantages, mainly aesthetics and bio-compatibility. The past decade has seen theemergence of a number of novel all-ceramiccrown and bridge systems with the capabilityof restoring anterior, posterior and multipleunits. The search for new methods has beendriven in part by patients who haveincreasingly high expectations in aestheticdentistry and who also have concerns aboutthe biocompatibility of metals intra-orally.1
Recent developments in dental materials haveled to the introduction of a large number ofall-ceramic systems for full-coveragerestorations. Some systems were developed asa single-layer glass-ceramic (Dicor, Dentisply/
Caulk; IPS Empress, Ivoclar/Vivadent), whileothers with a bi-layer design (In-Ceram,Vident, Procera, Nobel Biocare).2
Clinical evaluations of all ceramic crowns arepromising, and success rates of 98.4% over aperiod of 2–3.5 years have been reported.3 Ina recent study,4 the success rate for singlecrowns on the anterior dentition after a 5-yearperiod of evaluation was reported as 100%.The following report describes the restorationof six anterior maxillary teeth and fouranterior mandibular teeth and utilizing the IPSEmpress (Ivoclar/Vivadent) all-ceramicsystem.
Case ReportA 25-year old female in excellent health cameto our office with the chief complain being theappearance of her anterior upper and lower
dentition teeth that had been restored with fullgold (Figures 1–4). The patient disclosed thather appearance was causing problems on hersocial life and it was difficult to find a job.During the treatment planning session, thepatient was given the option of PFM(porcelain fused to metal) or metal-freerestorations. The patient chose to have all theteeth restored with the metal-free IPSEmpress. Initial impressions were taken forstudy models and laboratory-madeprovisionals (Figure 5).
The occlusion was analyzed pre-operatively,clinically, and with the aid of mounted studymodels on a semi-adjustable articulator. Adiagnostic wax-up was completed and thefinal outline form of the new restorations weredeemed to be aesthetically satisfactory andapproved by the patient.
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 35
Figure 2. Closer view of full gold crowns.
Figure 3. Occlusal view of maxillary teeth. Figure 4. Occlusal view of mandibular teeth.
Figure 1. Maxillary and mandibular anterior teeth presenting full gold crowns.

36 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
METAL FREE CERAMICS: A CLINICAL CASE
Figure 6. Initial cut with carbide bur in order to remove full gold crown.
Figure 7. Full gold crown sectioned.
Figure 5. Provisional restorations made at the laboratory
Figure 10. Right side view of the crowns. Note the proper contour andalignment obtained with the final restorations.
Figure 9. Upper and lower set of provisionals in place.
Figure 8. Teeth preparation. (Note the modified shoulder finish line, necessaryfor all-ceramic crowns.)

SANTOS ET AL.
At the tooth preparation/registration stage, allfull-gold crowns were cut using a 1/4” roundcarbide burr (Figures 6 and 7) and theabutment teeth were refined using modifiedshoulder diamond burrs with coarse andsuperfine grit (Figure 8). After refinishing themargins, a small unimpregnated retractioncord was placed (Ultrapack #000, Ultradent)followed by a second cord (Ultrapack #00,Ultradent) impregnated with haemostaticsolution (Hemodent, Ultradent). The finalfull-arch impression was made with acombination of a heavy and light viscositypolyvinyl siloxane (Take 1, Kerr) for the upperand lower arch. The provisionals were adaptedto the teeth preparations (Figure 9) and theocclusion was checked and adjusted. Beforethe cementation of the provisionals, aninterocclusal record at the patient’s maximum
intercuspidation position and a face bowtransfer were obtained. After the cementationof the provisionals with non-eugenoltemporary cement (TempBond NE, Kerr)another impression of the upper arch wasmade with irreversible hydrocolloid (Jeltrate,Dentsply/Caulk) in order to replicate theincisal guidance on the articulator. The shadewas determined with a shade guide (Vitapan3D Master, Vita)
During the final appointment all abutmentteeth were cleaned of temporary cement, thecrowns were inserted and the length, contour,and shades were inspected (Figures 10 and 11).All restorations were cemented with resinluting cement (Variolink II, Ivoclar/Vivadent).The patient received post-operative careinstructions, and a recall appointment was
scheduled for one week later. At the recallappointment the occlusion was checked. Themargins were inspected to ensure that therewas perfect integration of the soft tissuearound the crowns (Figure 12). The patientwas extremely happy with the final result(Figures 13 and 14).
Discussion / ConclusionAll ceramic systems indicated excellentesthetics, biocompatibility, and short-termclinical evaluations and have demonstratedhigh success rates.5,6 The IPS Empress was firstintroduced almost 20 years ago. In a processcomposed of several stages, controlledcrystallization is used to produce leucitecrystals, measuring a few microns, in the glassmatrix. The semi-finished product of leucite-reinforced ceramic powder is pressed into
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 37
Figure 13. Final result. There is excellent colour-matching with the rest of theteeth and superior lifelike esthetics.
Figure 14. Close-up of the Empress crowns after cementation.
Figure 11. Left side view of the crowns. Figure 12. One week follow-up. Close-up of gingival margins of the crowns onteeth #11 and #21, note the health of the tissue margins.

38 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
METAL FREE CERAMICS: A CLINICAL CASE
ingots and sintered. These ingots are the basiccomponents from which restorations arepressed. According to the manufacturer, IPSEmpress Esthetic is the material of choicewhen it comes to the fabrication of pressed,highly-esthetic single tooth restorations. Inaddition to the excellent strength values, theleucite glass-ceramic ingots are alsodistinguished for their exceptional esthetics.
Marquardt and Strub (2006)4 found that thesurvival rate of 27 single crowns made withIPS Empress 2 after a 5-year period ofobservation was 100%. They also observedthat the level of accuracy of fit (crownretention, marginal quality, and marginaladaptation) and esthetics accomplished wasdeemed very satisfying. Walia (2009)7presented a similar case restored with Proceracrowns, the authors also reinforced thesuperior esthetics achieved with an all-ceramicsystem and highlighted the excellent marginalfit.
For the purpose of this case report, it may beconcluded that the IPS Empress providedrestorations exhibiting excellent marginal fitand aesthetics.
ConflictsNone declared.
References1. Barnfather KDP, Brunton PA. Restoration
of the upper dental arch using Lava all-ceramic crown and bridgework. Br DentJ 2007;202(12):731–5.
2. Polack MA. Restoration of maxillary incisors with a zirconia all-ceramic system: a case report. Quintessence Int 2006;37(5):375–80.
3. Zitzmann NU, Galindo ML, Hagmann E,Marinello CP. Clinical evaluation of Procera AllCeram crowns in the anteriorand posterior regions. Int J Prosthodont 2007;20(3):239–41.
4. Marquardt P, Strub JR. Survival rates of
IPS Empress 2 all-ceramic crowns and fixed partial dentures: Results of a 5-yearprospective clinical study. Quint Int 2006;37:253–9.
5. Lopes GC, Baratieri LN, Caldeira de Andrada MA, Maia HP. All-ceramic postcore, and crown: technique and case report. J Esthet Restor Dent 2001;13(5):285–95.
6. Oden A, Andersson M, Krystek-OndracekI, Magnusson D. Five-year clinical evaluation of Procera All Ceram crowns.J Prosthet Dent 1998;80:450–6.
7. Walia S, Mathew P, Sandhu H, Santos Jr.GC, Restoring Esthetics with Metal-Free Ceramics: A Case Report. J Can Dent Assoc 2009;75(5):357–9.
Whether you are using implants from:Astra TechNobel Biocare StraumannBiomet 3i Zimmer Dental
Patient-specific abutments for all major implant systems
—Atlantis™ is the best solution for cement-retained implant prosthetics.
orBioHorizonsDenstply FriadentKeystone DentalSybron Implant Solutions
Visit www.atlantisabutment.com
For more information
mationFor more infor

Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 39
CASE REPORT / RAPPORT DE CAS
Traditional versus Contemporary? A ComparativeMultidisciplinary Case Report: Implant Fixed Prosthetic
Treatment
Traditionnel vs contemporain? Un rapport de casmultidisciplinaire comparatif : traitement prothétique
implantaire fixe
ABSTRACTIn virtually every industry, rapid changes are occurring as a result of technological innovation. In dentistry,changes in materials and techniques have provided patients and practitioners with many contemporaryoptions. With that in mind, many proven traditional techniques have continued to be employed with muchsuccess. As restorative dentists, we must consider all available options in order to help deliver the best possibletreatment to each patient on a case by case basis.
This article will feature the treatment plans, techniques, and materials for two multidisciplinary fixedrestorative reconstructions – one employing a more traditional approach, the other a more contemporary one.
By Dr. Marc Mollot, BSc, DMD
About the Author
Dr. Marc Mollot maintains a private practise in Winnipeg, Canada offering all aspects of family dentistrywith a particular interest in implant and fixed prosthetic dentistry.After completing a bachelor of science, Dr. Mollot obtained his DMD degree from the University ofManitoba in 1997.
He has served the profession both locally and nationally including as a clinical instructor at theUniversity of Manitoba, Faculty of Dentistry and on multiple provincial committees. He was awarded aCertificate of Merit for service in 2001 for work on both the Ethics and Dental Materials and Devicesadvisories for the Canadian Dental Association in Ottawa.
Dr. Mollot is a graduate of the Misch International Implant Institute and a Fellow of the InternationalCongress of Oral Implantologists. In 2005 he became a Fellow of the Pierre Fauchard Academy.Dr. Mollot is also a member of the Canadian Academy of Esthetic Dentistry, the Canadian DentalAssociation, the Manitoba Dental Association, Winnipeg Progressive Dental Study Club, and theWinnipeg Dental Society, among others.
To contact Dr. Mollot directly please e-mail at [email protected].

40 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
TRADITIONAL VERSUS CONTEMPORARY? IMPLANT FIXED PROSTHETIC TREATMENT
Case Report 1: Traditional ApproachInitial PresentationA 43-year-old man presented at his regularlyscheduled recare appointment. He indicatedthat he wanted to pursue having his “frontteeth fixed.” He indicated a desire to “closegaps, have straighter and whiter teeth” as wellas have “more even upper front teeth.”
In profile, the patient was skeletal class I with3 mm overjet and 30% overbite. He exhibitedan average height maxillary lip line and hisfacial and maxillary dental midlines werecoincident. He was, however, obviouslyfacially asymmetrical. As well, he wasbrachecephalic and had very well developedmuscles of mastication.
Intraoral ExaminationUpon intraoral examination, the followingobservations were noted (Figures 1–6):
• Uneven maxillary teeth – inverted smileline
• Crowded mandibular anterior teeth• Missing #12 from childhood, #13 in
position of #12 • Failing bridge #14 - #12 fixed partial
dentures (FPD) – porcelain fracture onall three abutments
• #13 endodontically treated. #14 apical radiolucency secondary to pulpal necrosis
• #11 lost in 1982 hockey accident – replaced with endosseous root form dental implant
• #11 Implant retained porcelain-fused-to-metal (PFM) crown – colour, angulation, and contour undesirable
• #21 Severe discoloration• #22 Pegged lateral incisor – rotated• Flat occlusal plane• Signs of wear and bruxism
Restorative Treatment OptionsIt was immediately evident that in order toaddress all of the patients concerns,restorative treatment would have to beundertaken on a minimum of six teeth (#14through #22 inclusive). A contemporaryapproach to restoring this particular casewould likely involve use of all-ceramicrestorations. All-ceramic restorations arehighly esthetic, primarily due to their relativetranslucency as compared to PFMs. If all-ceramic restorations were deemed to be therestorations of choice in this case, a zirconiaimplant abutment would be required in the#11 position. There would be little senseplacing a metal abutment under an allceramic crown; the #11 restoration wouldalways appear “grey” as compared to theadjacent teeth. Even if an aggressive opaquelayer were used, the optical qualities of onerestoration would be difficult to impossibleto reproduce on the others.
In consideration of the above, the followingwould be a contemporary restorative optionfor this case:
• All-ceramic bridge with zirconia framework #14– #12
• New zirconia implant abutment #11• All-ceramic crown (alumina or zircona
coping) #11• All-ceramic crowns or veneers #21 and
#22• Optional: consideration of #13 implant
declined
A more traditional approach would involvethe use of a metal abutment and PFMrestorations. Although with special care anddesign PFMs can be made to be very esthetic,they can have limitations in their opticalqualities. They are, however, very durable and
carry with them many years of research andclinical success.1 The following would be atraditional restorative option for this case:
• Metal titanium or cast UCLA abutment#11
• PFM bridge #12 – #14• PFM crowns # 11, #21, and #22
Final Treatment PlanRationale for recommending a moretraditional approach to restorative treatmentwas based upon the results of the initialintraoral and extraoral examination. In thiscase, it was determined that the patientexhibited high force factors. As well,consideration was given to the fact that thepatient had a moderate lip line and anaverage expectation for esthetics, yetunderstood that strength was an importantfactor in determining the long-termoutcome. Finally, because this case requiredmultiple crowns and a bridge, supported byboth teeth and by implants, a single commonrestorative system (i.e., PFM or all ceramic)would lead to a more consistent visualoutcome. For these reasons, the followingfinal treatment plan outlined below wasproposed and accepted.
Orthodontics• Idealize crowding and expand arches• Set up for new maxillary anterior
restoration
Restorative• Maxillary and mandibular take-home
whitening• Lengthen maxillary anterior teeth.
Correct reverse smile line. • Achieve a consistent shade across
maxillary anterior• Achieve bi-lateral symmetry of
RÉSUMÉDans presque que toutes les industries, les innovations technologiques engendrent des changements rapides.En dentisterie, les changements dans les matériaux et les techniques ont donné aux cliniciens et aux patientsplusieurs options contemporaines. Il ne faut pas oublier que plusieurs techniques traditionnelles éprouvéescontinuent d’être utilisées avec grand succès. En tant que dentistes en médecine dentaire restauratrice, nousdevons retenir toutes les options disponibles afin de traiter du mieux possible chaque patient en fonction dechaque cas.
Cet article traitera des plans de traitement, des techniques et des matériaux utilisés pour deux reconstructionsprothétiques multidisciplinaires fixes – la première utilisant une approche plus traditionnelle tandis que ladeuxième une approche plus contemporaine.

MOLLOT
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 41
Figure 1. Pre-treatment smiling. Figure 2. Pre-treatment centric view. Figure 3. Pre-treatment maxillary view.
Figure 4. Pre-treatment mandibular view. Figure 5. Pre-treatment panoramic radiograph. Figure 6. Pre-treatment panoramic radiograph.
maxillary anterior sextant• Treat #14 endodontically• Traditional restorations (PFM bridge
#14–#12; maintain metal UCLA abutment #11) Abutment level impression (PFM #11, #21, and #22)
• Occlusion goals (group function right side; cuspid guided left side)
He was referred for full-mouth fixedorthodontic treatment. Orthodontictreatment time elapsed was 21 months. Oncein retention, endodontic treatment of #14was completed. After 6 months of retention(to ensure a stable occlusion) the teeth wereprepared ensuring a shoulder margin to helphide and potentially grey margins. Afterseveral weeks of temporization, a dual cordtechnique for retraction was employed(Ultrapak, Ultradent) and a final abutmentlevel impression of tooth #11 as well as theother C and B units was made. PFMrestorations were fabricated, adjusted, and
custom stained and glazed. Restorationswere sandblasted and luted using a resin-modified glass ionomer (Rely-X, LutingPlus3M). A maxillary night-guard andmandibular retainer were fabricated (Figures7–14).
Case Report 1: TraditionalDiscussionWhen undertaking an anteriorreconstruction, mixing FPD restorativesystems within a particular case is lessdesirable. Blending PFM with all ceramic, oreven blending one all-ceramic system withanother can lead to a compromised estheticresult. Practitioners can expect a far morehomogeneous final outcome if they employthe use of a common FPD system wheneverpossible for all restorations employed in acase. For obvious reasons, placing highlytranslucent restorations directly beside non-translucent restorations should be avoided,especially in the maxillary anterior.
In this case specifically, an argument couldbe made that simply veneering #21 and #22would be a more conservative solution toaddressing their colour and contour issues.With that in mind, being placed directly nextto PFMs on #11, #12, #13, and #14, therewould be an obvious visual difference toeven the untrained eye. Once the decisionwas made to use a metal implant abutmentand PFM bridge on one side of the maxillaryanterior, this determined the need for thesame FPD technology (PFM crowns) on theother side. As displayed with this particularcase, when careful attention is given tofactors such as margin design, adequatetooth reduction, and careful laboratorytechnique, PFM restorations can provide fora very esthetic outcome. Furthermore, PFMcrowns continue to be a dependable long-term restoration. Bond strengths ofporcelain to semi-precious alloys continue tobe high and reliable (Figures 15–18).2

42 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
TRADITIONAL VERSUS CONTEMPORARY? IMPLANT FIXED PROSTHETIC TREATMENT
Figure 7. Post-orthodontic centric view. Figure 8. Post-orthodontic maxillary view. Figure 9. Post-orthodontic mandibular view.
Figure 10. Non-surgical root canal therapy #14. Figure 11. Preparation day. Figure 12. Abutment-level polyether impression.
Figure 16. Before. Figure 17. After. Figure 18. Post-treatment smiling.
Figure 13. Abutment-level final cast. Figure 14. Porcelain-fused-to-metal crowns. Figure15. Post-treatment occlusal view.

MOLLOT
Case Report 2: ContemporaryInitial Presentation This 29-year-old single male presented byreferral from another practitioner. His chiefcomplaint was that he had “crooked lowerteeth and three of his front teeth wereknocked out in a sports accident.” Heindicated a clear desire to better his overallappearance and improve his teeth esthetically.
In profile, the patient was skeletal class II with5 mm overjet and 50% overbite. He had aretruded mandible and exhibited a highmaxillary lip line. He was facially symmetricalbut his facial and dental midlines were non-coincident.
Intraoral Examination Upon intraoral examination, the followingobservations were noted (Figures 19–23).
• Missing #21 and # 22 – avulsed monthsearlier
• Teeth #11 and #12 tilted into edentulousspace
• M/D width of edentulous space less thanM/D width of #11 and #12 combined.
• Tooth #31 fractured and unrestorable
• Satisfactory colour and contour of remaining natural teeth
• Crowded mandibular anterior teeth• Little to no signs of bruxism
Restorative Treatment OptionsA contemporary approach to restoring thisparticular case would involve use of allceramic restorations. The following would bea contemporary restorative option for thiscase:
• Zirconia abutments #21 and #22• All-ceramic crowns #21 and #22
A more traditional approach would involvePFM restorations. The following would be atraditional restorative option for this case:
• Metal titanium or case UCLA abutments#21 and #22
• PFM crowns #21 and #22
Final Treatment PlanRationale for recommending a morecontemporary approach to restorativetreatment was based upon the results of theinitial intraoral and extraoral examination. In
this case, unlike case report 1, it wasdetermined that the patient exhibited low tomoderate force factors. Furthermore,consideration was given to the fact that thepatient had a high smile line and an aboveaverage expectation for a highly estheticoutcome. Finally, because the case requiredmaxillary anterior dental implantrestorations directly adjacent to unrestorednatural teeth, a high level of translucency andesthetics was required to achieve a bilaterallyhomogeneous outcome.3
For these reasons, the following finaltreatment plan was proposed and accepted:
Orthodontics• Remove #31 – to treat orthodontically to
three lower incisors• Idealize mandibular crowding• Set up for new maxillary anterior
restoration
Restorative• Achieve bi-lateral symmetry of
maxillary anterior sextant• Contemporary restorations: zirconia
abutments #21 and #22 – custom
Winter 2011
Figure 22. Pre-treatment mandibular view. Figure 23. Pre-treatment panoramic radiograph.
Canadian Journal of Restorative Dentistry & Prosthodontics 43
Figure 19. Preoperative smiling. Figure 20. Pre-treatment centric view. Figure 21. Pre-treatment maxillary view.

44 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
TRADITIONAL VERSUS CONTEMPORARY? IMPLANT FIXED PROSTHETIC TREATMENT
fabricated (fixture implant) level impression). All-ceramic crowns (alumina copings) #21 and #22
• Occlusion goals (cuspid guided bilaterally)
Tooth # 31 was extracted. The patient wasreferred for full-mouth fixed orthodontictreatment. Treatment time elapsed was 12months. Once orthodontics was completed,but before debanding, a surgical guide wasfabricated and he was referred to theperiodontist to have two root form dentalimplants (Nobel Biocare) placed in the #21and #22 positions. After successfulosseointegration of the implants wasconfirmed, temporary abutments wereplaced and adapted to help developemergence profile and tissue contours. At 6months post-orthodontics (to ensure a stableocclusion), an implant-level final impressionwas made. Zirconia abutments and alumina-reinforced all-ceramic crowns (Procera AllCeram, Nobel Biocare) were fabricated.Abutments were torqued to 35 N/cm. Final
crowns were luted using a resin-modifiedglass ionomer (Rely-X Luting Plus, 3M). Amaxillary nightguard and mandibularretainer were also fabricated (Figures 24–28).
Case Report 2: ContemporaryDiscussionThere is little debate that all-ceramic crownsare highly esthetic restorations. However,when optimal esthetics are required fordental implant restorations, considerationmust be given to the translucency of theabutment underneath.4 As previouslydiscussed, there would be little advantage toplacing an all-ceramic crown with a metalabutment underneath.
In this case specifically, it would have beendifficult to achieve anything better than anaverage result by placing metal abutmentsand PFMs on #21 and # 22 directly adjacentto natural, unrestored teeth #11 and #12. Nomatter what level of attention to detail, therewould have always been a visible difference inopacity and an underlying “greyness” to the
restored teeth. As well, given the patients’high smile line, there would be an increasedrisk of discoloration of the vestibular peri-implant tissues.4,5
Today, zirconia abutments are widelyavailable commercially for use with mostdental implant systems. Zirconia abutmentsoffer a reliable alternative to titanium or castabutments.6 They can withstand clinical loadsabove those expected during mastication.7
Although not the same translucency asnatural teeth, zirconia abutments still offer arelative translucency and the opportunity toemploy all ceramic crowns as finalrestorations. They also offer an excellentsolution for patients with thin periodontalbiotype where there is a fear of greying or“purple” gingivae overlying an implantrestoration site.5,8
As with titanium, zirconia abutments can becustom designed or purchased as stockcomponents. What is not well known,however, is that unlike titanium, zirconia is a
Figure 24. Post-orthodontic maxillary view. Figure 25. Post-orthodontic mandibular view.
Figure 27. Implant-level polyether impression. Figure 28. Implant-level master cast. Figure 26. Implant placement of tooth #21 and tooth#22.
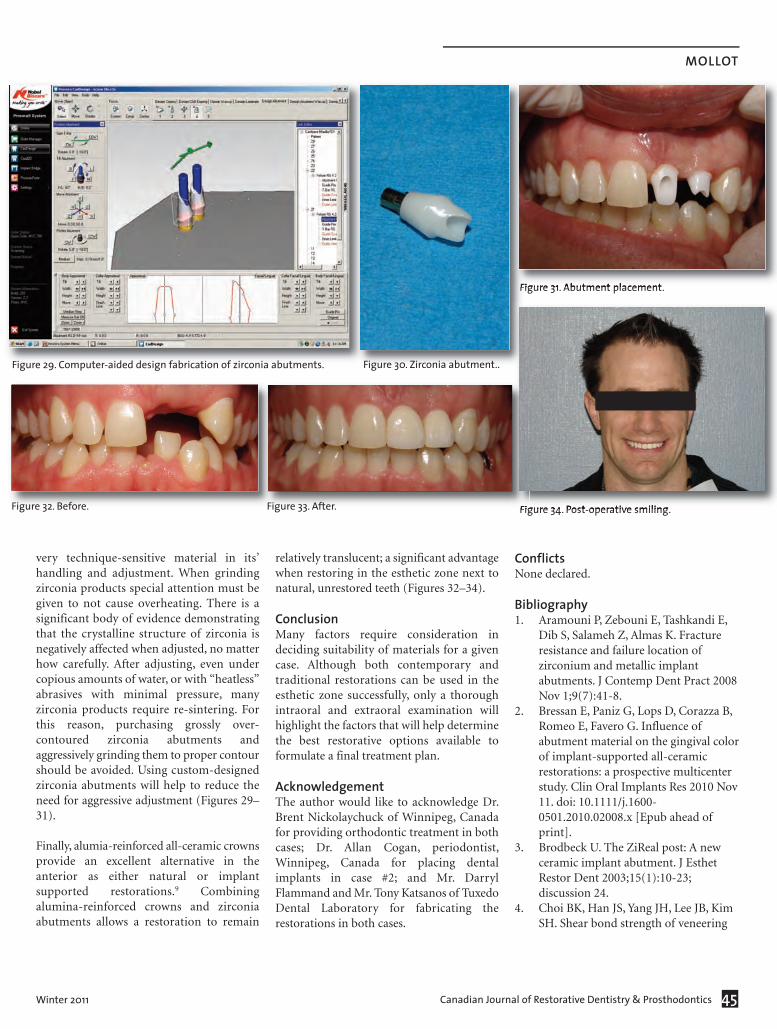
MOLLOT
very technique-sensitive material in its’handling and adjustment. When grindingzirconia products special attention must begiven to not cause overheating. There is asignificant body of evidence demonstratingthat the crystalline structure of zirconia isnegatively affected when adjusted, no matterhow carefully. After adjusting, even undercopious amounts of water, or with “heatless”abrasives with minimal pressure, manyzirconia products require re-sintering. Forthis reason, purchasing grossly over-contoured zirconia abutments andaggressively grinding them to proper contourshould be avoided. Using custom-designedzirconia abutments will help to reduce theneed for aggressive adjustment (Figures 29–31).
Finally, alumia-reinforced all-ceramic crownsprovide an excellent alternative in theanterior as either natural or implantsupported restorations.9 Combiningalumina-reinforced crowns and zirconiaabutments allows a restoration to remain
relatively translucent; a significant advantagewhen restoring in the esthetic zone next tonatural, unrestored teeth (Figures 32–34).
ConclusionMany factors require consideration indeciding suitability of materials for a givencase. Although both contemporary andtraditional restorations can be used in theesthetic zone successfully, only a thoroughintraoral and extraoral examination willhighlight the factors that will help determinethe best restorative options available toformulate a final treatment plan.
AcknowledgementThe author would like to acknowledge Dr.Brent Nickolaychuck of Winnipeg, Canadafor providing orthodontic treatment in bothcases; Dr. Allan Cogan, periodontist,Winnipeg, Canada for placing dentalimplants in case #2; and Mr. DarrylFlammand and Mr. Tony Katsanos of TuxedoDental Laboratory for fabricating therestorations in both cases.
ConflictsNone declared.
Bibliography1. Aramouni P, Zebouni E, Tashkandi E,
Dib S, Salameh Z, Almas K. Fracture resistance and failure location of zirconium and metallic implant abutments. J Contemp Dent Pract 2008Nov 1;9(7):41-8.
2. Bressan E, Paniz G, Lops D, Corazza B, Romeo E, Favero G. Influence of abutment material on the gingival colorof implant-supported all-ceramic restorations: a prospective multicenter study. Clin Oral Implants Res 2010 Nov 11. doi: 10.1111/j.1600-0501.2010.02008.x [Epub ahead of print].
3. Brodbeck U. The ZiReal post: A new ceramic implant abutment. J Esthet Restor Dent 2003;15(1):10-23; discussion 24.
4. Choi BK, Han JS, Yang JH, Lee JB, Kim SH. Shear bond strength of veneering
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 45
Figure 30. Zirconia abutment..
Figure 31. Abutment placement.
Figure 32. Before. Figure 33. After. Figure 34. Post-operative smiling.
Figure 29. Computer-aided design fabrication of zirconia abutments.

46 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
TRADITIONAL VERSUS CONTEMPORARY? IMPLANT FIXED PROSTHETIC TREATMENT
porcelain to zirconia and metal cores. J Adv Prosthodont 2009 Nov;1(3):129−35. Epub 2009 Nov 30.
5. Jiang YL, Sun J, Weng WM, Zhang FQ. Long-term observation of 920 porcelainfused to metal prostheses [In Chinese]. Shanghai Kou Qiang Yi Xue 2006;15(5):490−2.
6. Jung RE, Holderegger C, Sailer I, Khraisat A, Suter A, Hämmerle CH. The effect of all-ceramic and porcelain-fused-to-metal restorations on marginal peri-implant soft tissue
color: a randomized controlled clinical trial. Int J Periodontics Restorative Dent2008 Aug;28(4):357–65.
7. Sailer I, Philipp A, Zembic A, PjeturssonBE, Hämmerle CH, Zwahlen M. A systematic review of the performance ofceramic and metal implant abutments supporting fixed implant reconstructions. Clin Oral Implants Res2009 Sep;20 Suppl 4:4–31.
8. Sailer I, Zembic A, Jung RE, Hämmerle CH, Mattiola A. Single-tooth implant reconstructions: esthetic factors
influencing the decision between titanium and zirconia abutments in anterior regions. Eur J Esthet Dent 2007Autumn;2(3):296−310.
9. Zarone F, Sorrentino R, Vaccaro F, RussoS, De Simone G. Retrospective clinical evaluation of 86 Procera AllCeram anterior single crowns on natural and implant-supported abutments. Clin Implant Dent Relat Res 2005;7 Suppl 1:S95–103.

Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 47
PRODUCT PROFILE / PROFIL DU PRODUIT
What cement should I use? In years pastthis was a relatively simple question to
answer when dentistry was essentially limited tometal ceramic or metal restoration. Asrestorative materials have continued to evolveand the demand for a natural looking smile hasincreased the decision of which cement shouldbe used has become more and morecomplicated. Today’s ceramic materials displayincredible levels of translucency and cementshave had to evolve, so that they blend into therestoration and minimize potential opaquingissues that are prevalent in traditional powder-liquid type cements. Traditionally, ceramicrestorations have been cemented utilizing resin-based systems with excellent success; however,these multi-step systems tend to be quitetechnique sensitive and meticulous control ofthe environment is paramount to success. Overthe last seven to 10 years numerousmanufacturers have invested tremendousresources to develop cements that display manyof the excellent physical properties of resincements yet minimize the traditionally difficulttechnique. Along with these advancement manyresearch papers and product technical bulletinshave been released comparing things such asshear, tensile, and compressive bond strengths,yet very little information has been shownrelating laboratory testing to clinical relevancein the hands of practitioners. This synopsis willcorrelate various physical properties
traditionally discussed in published media andthe clinical relevance of each of these properties.The ultimately goals for all cements that willprovide a link between prepared tooth structureand fixed restoration are biocompatibility, cariesinhibition, high strength (shear, tensile, andcompressive), low solubility, colour stability,radiopacity, low film thickness, low levels linearexpansion, and predictability of use,intentionally or unintentionally.
BiocompatibilityEssentially luting cements should not have anegative impact on the body tissue and fluidsthat they may come in contact with.Additionally they should have a very low chanceof creating any type of potential allergicresponse for the patient, clinician, and auxiliarystaff that may handle the material. In regards toresin cements that require light polymerizationbiocompatibility must also be tested in regardsto incomplete polymerization. In restorationsthat exceed 2 mm in thickness a self or dual-cureluting agent should be considered to minimizethe biocompatibility risk of partiallypolymerized resins.1
Caries InhibitionThe critical point of failure for any restorativematerial is at the interface between therestoration and the natural tooth structure. Interms of indirect restorations this area
represents the marginal interface with minimalor no microleakage. An ideal cement wouldhave sufficient fluoride release or othercariostatic components to protect this interfaceand prevent caries propagation at the margin.2
Shear Bond StrengthShear bond strength is routinely tested for whenevaluating various restorative materials. Whenone thinks of shear bond strength, it’s like ahook on a wall being held on with adhesive andthe hook is holding a towel. Clinically speakingthis shear movement would relate to the forceexerted between the cement and prepared toothstructure on an axial wall of a full coveragerestoration when a pulling force is applied.
Shear bond strength measurements aregenerally taken over various time spans to testboth immediate bond that is achieved as welldelayed bond strength. The bond strengthstudies are conducted utilizing water storage aswell as thermo cycling. Thermo cycling is meantto measure the hot and cold (5-55 Celsius)temperature swings that result from eating anddrinking. As taper on a preparation increased agiven cements tensile strength, it is also testedwhen a vertical pulling force is applied.
Tensile Bond StrengthSimilar to shear bond strength, tensile bondstrength is often cited in literature in regards
Understanding Self-Adhesive Resin Cements (G-CEM by GC America)
Compréhension des ciments résines auto-adhésifsBy Dr. Parag R. Kachalia
About the Author
Dr. Parag R. Kachalia is an assistant professor of restorative dentistry at University of the Pacific’s ArthurA. Dugoni, School of Dentistry. He serves as the director of new technologies, course director for fixedprosthodontics and is a core faculty member within Pacific’s prestigious complex and estheticrehabilitation program. He is a published author in the areas of digital dental photography, digital fixedprosthodontics, and financial management. His research is primarily focused on advances of CAD/CAMdentistry as well as new technologies entering the restorative marketplace.

48 Journal canadien de dentisterie restauratrice et de prosthodontie Hiver 2011
PRODUCT PROFILE
adhesive bonding. In relation to tensilestrength one must imagine the palms of one’shands together again and slowly peeling apartfrom the fingertips down to the wrists. Thisaction in terms of a restorative material wouldcause tension and pulling apart of a bond thatmay be formed. In clinical terms one mustconsider a resin bonded bridge replacing amaxillary later incisor that utilizes the lingualsurfaces of the adjacent canine and centralincisors. If a blunt force was applied to thelateral incisor pontic and retainers pulled awayfrom their corresponding lingual surfaces thiswould be as a result of a tensile bond failure.In relation to a full coverage restoration that isundergoing a vertical pulling force when anindividual is chewing a piece of gum, a tensilebond is being maintained between therestoration and the adhesive cement as well asthe adhesive cement and the prepared toothsurface. Similar to shear strength, tensile bondstrength studies are conducted utilizing timesranging from immediate bond to bondstrength post multicycle thermocycling.Thermocycling is simply a laboratoryprocedure that is used to simulate oralenvironment over a given period of time. G-CEM, self-adhesive resin cement actuallyimproves bond strengths to the dentin, enameland Zirconia restoration after thermocycling.5
Compressive StrengthAt any one time, all forces are in play. Tensilebond strength and shear bond strength areprimarily referred to in terms of crownremoval or dislodgement. Equally importantto these two measurements is that ofcompressive strength. When one thinks ofcompressive strength it is essentially ameasurement where force is applied to a givenflat surface of restorative material until itbreaks. A high compressive strength isparticularly important when one thinks of aresin cement that may be placed under apartial or full coverage ceramic restoration thatwill undergo biting pressure. A propercompressive strength is important in theocclusal region to prevent compression of therestoration and potential fracture if thecompressive strength is too low. In today’sworld of digitally designed restorations it is notuncommon to see gaps between the preparedtooth surface and the underside (intaglio) of amilled restorations. These gaps form whenhighly defined occlusal tables are prepared and
tooling of the milling systems are forced tounder-mill these defined anatomical forms.When this occurs, the resin cement isessentially acting as a mini buildup to supportthe biting force that may be placed on therestoration. A high compressive strength is alsoimportant at the marginal interface. It isunderstood that all restoration will exhibit aminor gap at the marginal interface and thatthis interface will ideally be filled with cement.Under biting pressure a given amount ofcompression will occur at the margin and thechosen cement should have enough strengthto hold up to this force and not undergomarginal wear. If the chosen cement has a lowcompressive strength this area of cement canfracture and potentially lead to marginalleakage and loss of restoration integrity.
Cohesive and Adhesive PropertiesAnytime an adhesion must occur between onematerial and another the cohesive andadhesive properties of the material must betaken into account. If a cemented restorationis to come off in one’s mouth as a result of apulling force this failure may have occurred ata few different levels. Essentially if the bondbetween the restoration and the cement gaveway cleanly this would be considered anadhesive failure. Additionally if the cementcompletely adhered to the restoration butseparated from its dental/enamel interface thiswould also be considered an adhesive failure.In the event that the cement properly adheredto both the tooth and restoration interface, yetthe restoration came free under a tensile forcea cohesive failure most likely occurred. Acohesive failure is generally observed when thebond strength to the given substrates is greaterthan inherent physical properties of thecement itself; in essence the cement isseparating from itself. A cohesive plateau isreached when the bond to any given substratematches the tensile strength of the cementitself. Bond strengths greater than this amountgenerally lack any clinical significance.
Low SolubilityAn ideal cement should be completelyimpermeable to oral fluids and resist washoutover the lifespan of the fixed restoration. Theintegrity of the restoration’s marginal seal isparamount to the long-term success of therestoration. Generally speaking, resin cements
have very low solubility over time whenrestorations are placed in an environment withproper moisture control.3 G-CEM has beenshown to have very low solubility incomparison to other self-etching resin cementsin the marketplace.5
Colour StabilityAs dentistry continues to evolve and theexpectations of patient’s rise, it is imperativethat dental restorations blend in with one’ssmile. Clinicians, auxiliary staff, and laboratorytechnicians all do their part in preparing teethproperly, selecting ideal shades, and creatinglifelike restorations. In terms of all ceramicrestorations the final result cannot be deemeda success until the restoration is cemented inone’s mouth and properly blends in with theadjacent teeth. Being that all ceramicrestorations have a certain amount oftranslucency the colour of the chosen cementcan play a significant role in the finalappearance of the restoration. Furthermorethe cement must display the propercharacteristics, so that the color of the cementstays true over time and does not degrade. G-CEM is available in four different shades toallow the practitioner the freedom to choosean accurate underlying cement colour and notdeleteriously effect the final restoration with aone size fits all mentality.
RadiopacityAn often overlooked area when considerscements is its radiopacity. At the marginalinterface of all restorations a micro-gap exists.If the cement that fills this area does not havethe proper radio-opacity the margin mayappear open when a digital radiograph ismagnified. Ideally the radio-opacity of one’schosen cement should be at least as radio-opaque as enamel, so that the marginalinterface does not have the appearance ofradiographic decay. Additionally, by beingradio-opaque radiographic evidence can aidin identifying residual cement that may havemigrated below the gum line upon restorationcementation. G-CEM capsules have a radio-opacity that is 25% more opaque than3M-ESPEs Unicem (Clicker Version).5
Low Film ThicknessIt is imperative that cements have amanageable film thickness. Historically onedownside of resin cements has been their

KACHALIA
Winter 2011 Canadian Journal of Restorative Dentistry & Prosthodontics 49
relatively high film thickness and a higherincidence of tilted castings because of unevencement thickness. If the film thickness is toohigh, restorations may not seat appropriatelyand may lead to a clinically unseated crownthat leads to a bite that may seem too high toa patient. One of the other issues if filmthickness is too high is that the cement maybreak internal to itself. Many of today’s selfadhesive resin cements have film thicknessmeasurements that are less than the 22–25microns characteristic of zinc phosphate.Properly mixed G-CEM demonstrates a filmthickness of approximately 12 microns.5
Low Levels of Linear ExpansionThe ideal cement should have the versatility tobe used in many applications as well as withmany restorative materials.4 Ceramicmaterials are highly prevalent in today’s worldand require a cement that does not have anextensive amount of expansion that could leadto fracture and catastrophic failure of therestoration. Additionally these cements mustmaintain essentially zero expansion when theyare exposed to water. Equally importantexpansion should be minimized anytime apre-fabricated or a custom post is cementedwithin a canal space. Excessive expansion canlead to fracture of a patient’s root and deemthe tooth non-restorable. Generally speakingself adhesive resin cements have a very lowlevel of expansion and most recently G-CEMdemonstrated less than 0.2 % expansion over
28 days. Similar to glass ionomer cements G-CEM released fluoride; however it does nothave the expansion issues that were prevalentwith pure glass ionomer cements.
Predictability of UseRepeatable results are of paramountimportance. Time and time again results maybe obtained in a laboratory setting; however,these results are only relevant if repeatabilityis possible in a clinical environment.Numerous studies overtime have shown thatin a hand-mixed cement system, operatortechnique can greatly influence cementperformance in either a positive or negativemanner. Additionally the delivery systems ofthe cement should allow for both intracanaldelivery for post systems as well, intra-prepdelivery for partial coverage restorations, andintra restoration delivery for full coveragerestorations. The ideal delivery system shouldbe consistent over multiple restorations in amanner that minimizes any potential waste. G-CEM’s automix tip is substantially smallerthan its competitors allowing for a greaternumber or restorations to be cemented per/mlof material in each syringe.
ConclusionResin cements have truly evolved over timeand for the vast majority of multi and singleunit restorations G-CEM can be the go-tocement of choice. The complicated multi-stepresin cements can be reserved for intricate
veneer deliveries that may require a higherbond strength due to lack of inherentretention. In addition autopolymerizingcements can be used for metal, metal-ceramic,and all ceramic restorations in a predictablerepeatable manner with easy cleanup.
References1. de Souza Costa CA, Hebling J, Randall
RC. Human pulp response to resin cements used to bond inlay restorations. Dent Mater 2006;22:954-962.
2. Radovic I, Monticelli F, Goracci C, Vulicevic ZR, Ferrari M Self-adhesive resin cements: a literature review. J Adhes Dent. 2008 Aug;10(4):251-8
3. Anusavice K, Cements for Bonding Application, Phillips’ Science of Dental Materials, Tenth Edition, 1996 pg 576
4. Burgess J, Ghuman T, Cakir D. Critical Appraisal: Self Adhesive Resin Cements. J Esthet Restor Dent. 2010 Dec;22(6):412-9.
5. Data on file.
For further information three G-CEM videoscan be found at the websites below: http://www.gcamerica.com/multimedia/index.phphttp://www.gcamerica.com/multimedia/22.phphttp://www.gcamerica.com/products/operatory/G-Cem/
READERS' CORNER / COIN DES LECTEURS
Fall Occlusion Issue Well Received Numéro Occlusion, automne, bien apprécié
Re: Article - Rinchuse and Kandasamy
Sir/Madam,I just read this article over a 12-hour periodincluding checking many of the refs. Here isone orthodontist that entirely agrees with theauthors who have done an absolutelyoutstanding job. This is the nearest attemptto a gold standard, Cochrane-level analysis, I
have seen in over 35 yrs of practice. I lookedhard for something to disagree with, on aliterature and/or clinical experience, empiricbasis – all to no avail!
Dentistry needs more efforts like this toensure our day-to-day practices, clinically, arebased on science and not (as is all toofrequent) glossy, coloured ads and weekend
courses. One would hope that upcomingstudents are exposed to this level of intensescrutiny of the available data.
Yours collegially.Andrew F. Thompson, Dental Specialist www.drthompson.ca www.parklanedental.ca


* Versus competitive materials tested. / Par rapport aux matériaux concurrents mis à l’essai.© 2011, 3M. All rights reserved. 3M, ESPE and Filtek are trademarks of 3M or 3M ESPE AG. Used under license in Canada. © 3M, 2011. Tous droits réservés. 3M, ESPE et Filtek sont des marques de commerce de 3M ou de 3M ESPE AG, utilisées sous licence au Canada. 1103-00997 B
Deux composites innovateurs. Une marque de confiance.Nos matériaux de restauration fluide et universel se manipulent aisément.
La nanotechnologie exclusive à 3M ESPE permet d’obtenir :
MC Supreme Ultra 3MMC ESPEMC se complètent
Deux excellents matériaux de restauration...
un systèmepolyvalent.
Matériaux de restauration fluide et universel
FiltekMC Supreme Ultra
One trusted brand.
3M ESPE’s unique nanotechnology can deliver:
3M™ ESPE™ ™ Supreme Ultra
Filtek™ Supreme Ultra Universal and FlowableRestoratives
Two excellent restoratives...
one versatilesystem.
s™kk™etilF
metsyys
p. p
ealvlyyoppuates re dxuairéatM
.tnenoiatru
esviatrtoResod Flnl aasrevinU
emrpuSketilF
bedtusr tenO
elbawoartl Uem
danr b
qrae mUnom cxueD
ecnafinoe ce du.suretavonn isetsiopm
eemrpuSMCketilF
elsrevi unt eediufluates re dxuairéatM
artl Ue
noiatru
™EPS E™3M
qui uns’EPS EM3
bedtusr tenO
artl Uemer Sup™™
ervil dena cygoolchnetona ne
.danr b
nhcetona naL
ait nelupinamauirétas moN
qrae mUn
a
:r
pEPSM Ee à 3visulcxe eigolon
. tnemisént ue ediun floitarautese rx d
.ecnafinoe ce du
MC
:niretbod’t emrep
l seserevi
3M,vés.ous droits réserTTous droits réser 2011.© 3M, ES 3M,ved.All rights reser 3M.© 2011, / P ersus competitive materials tested.V*
EPS E3M
ESPE et Filtek sont des marques de commerce de 3M ou de 3M ESP Used under lice AG. SPE and Filtek are trademarks of 3M or 3M ESPE
Par rapport aux matériaux concurrents mis à l’essai.
artl Uemer Sup
UemerSup
1103-00997 B utilisées sous licence au Canada.AG, E ense in Canada.
a
oe c sMCEPS EMCM 3artl U
nt eètlpmo