espnic epic diploma applicant guide - rev 2016 02 · epic diploma™ applicant guide rev. 2015 11...
TRANSCRIPT
EPIC Diploma™ European Paediatric / neonatal Intensive Care Diploma™
Applicant Guide Copyright © 2015‐2016 European Society of Paediatric and Neonatal Intensive Care. “ESPNIC”, the ESPNICSM service mark, “EPIC Diploma”, the EPIC Diploma™ certification mark, and “European Paediatric / neonatal Intensive Care Diploma™” are the intellectual property of the European Society of Paediatric and Neonatal Intensive Care. All rights reserved.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 2 of 24
TABLE OF CONTENTS
EPIC DIPLOMA™ PROGRAM PURPOSE / MISSION STATEMENT ......................................................................................... 3
EPIC DIPLOMA PROGRAM COMPONENTS......................................................................................................................... 3
TOPICAL SCOPE, GEOGRAPHIC SCOPE, AND LANGUAGE ................................................................................................... 3
ELIGIBILITY REQUIREMENTS ............................................................................................................................................. 4
GENERAL ELIGIBILITY REQUIREMENTS ............................................................................................................................................... 4 PART 1 ADDITIONAL ELIGIBILITY REQUIREMENTS ................................................................................................................................ 4 PART 2 ADDITIONAL ELIGIBILITY REQUIREMENTS ................................................................................................................................ 5
ETHICS AND PROFESSIONALISM ....................................................................................................................................... 5
APPLYING FOR THE EPIC DIPLOMA ................................................................................................................................... 7
EPIC DIPLOMA EXAM FEES ............................................................................................................................................... 8
CANCELLATION POLICY .................................................................................................................................................................. 8
TAKING THE EXAM ........................................................................................................................................................... 9
SPECIAL ACCOMMODATIONS ........................................................................................................................................................ 10
EXAM RESULTS .............................................................................................................................................................. 11
PREPARING FOR THE EPIC DIPLOMA EXAM .................................................................................................................... 12
GENERAL STRATEGIES FOR TAKING WRITTEN TESTS........................................................................................................................... 12 EXAM SPECIFICATIONS / SYLLABUS / TOPICAL BLUEPRINT ................................................................................................................... 13 AUTHORITATIVE REFERENCES ........................................................................................................................................................ 14 ONLINE STUDY GROUP ................................................................................................................................................................ 21
RECERTIFICATION / RENEWAL / MAINTENANCE OF CERTIFICATION ................................................................................ 22
IRREGULAR BEHAVIOR ................................................................................................................................................... 23
REVALIDATION OF EPIC DIPLOMA PROGRAM EXAM CONTENT ....................................................................................... 23
GRIEVANCES, POLICY INTERPRETATION REVIEWS, AND APPEALS ................................................................................... 24
DATA CONFIDENTIALITY AND RELEASE OF CREDENTIALING INFORMATION TO THIRD PARTIES ....................................... 24

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 3 of 24
EPIC Diploma™ Program Purpose / Mission Statement The purpose of the European Paediatric / neonatal Intensive Care Diploma™ (EPIC Diploma™) program is to harmonize and improve quality standards for safe, independent practice in paediatric and neonatal intensive care in Europe and elsewhere. The EPIC Diploma program assesses the minimal competencies necessary to practice as a paediatric / neonatal intensive care specialist. The EPIC Diploma program is intended to be complementary to national standards and enhance the competent, ethical, and professional care of critically ill children.
EPIC Diploma program Components The EPIC Diploma program consists of two component credentials that constitute a pathway of professional development for paediatric and neonatal intensive care practitioners. These two parts are: Part 1 – Certificate in Paediatric and Neonatal Intensive Care Part 2 – EPIC Diploma (European Paediatric / neonatal Intensive Care Diploma) Periodic recertification ensures that those who maintain their EPIC Diploma remain competent and continually enhance their competency as the subspecialty’s body of knowledge, technical content, and scope of practice evolves over time.
Topical Scope, Geographic Scope, and Language While the focus of the EPIC Diploma program is on harmonizing the standard of practice among paediatric and neonatal intensivists in Europe, and the exam content is limited to practice in Europe, practitioners from around the world are encouraged to apply for and become certified through the EPIC Diploma program. Candidates of any nationality are eligible to apply for the EPIC Diploma program. Initially, the EPIC Diploma program’s assessments and other materials will be in English. In recognition of varying levels of bilingualism across Europe, and respectful of the potential impact on exam pass rates of requiring candidates to take the exam in a language other than their primary language, the ESPNIC Diploma Advisory Board has decided to phase in localized translations of the exam and supporting materials over time, in collaboration with national societies. Neonatal intensive care is covered in the EPIC Diploma exam, but not neonatology aside from neonatal intensive care. Advanced Nurse Practitioners—and equivalent high‐level allied health professionals—performing essentially the same role as paediatric / neonatal intensive care physicians will be eligible to participate in the Diploma Program. As indicated in the EPIC Diploma program Purpose / Mission Statement, the EPIC Diploma program is intended to harmonize and improve quality standards and be complementary to national standards. In effect, this means that some national authorities may choose to accept the EPIC as satisfying all national requirements for authorized practice as a paediatric / neonatal intensive care specialist, and other national authorities may choose to impose additional, localized requirements for specialist practice.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 4 of 24
Eligibility Requirements Eligibility requirements must be met, without exception in any circumstances. To be eligible to take an EPIC Diploma examination, applicants must satisfy the requirements by the date of application:
General Eligibility Requirements
General Medical Training Medical school / faculty / university degree
Primary Specialty Training
Completion of a training program in one of the following primary specialties: Anaesthesiology, paediatrics, paediatric surgery, or intensive care
Licensure
A valid (current), unrestricted medical license in at least one jurisdiction. If multiple licenses are held, each must be valid and unrestricted (“restricted” means “restricted for some action”—licenses that are merely expired are acceptable).
To enable the EPIC Diploma program’s assessment content to be incorporated into a training curriculum, the exam is divided into two Parts.
Part 1 Additional Eligibility Requirements
Part 1 is based on finishing one year of specialist training in paediatric / neonatal intensive care, and completing training in the following core topics (equivalent allowed if approved by ESPNIC):
o BASIC course (see http://www.wfpiccs.org/projects/basic‐course/) or its equivalent covering:
Airway management Acute respiratory failure Mechanical ventilation Haemodynamic monitoring Management of shock Severe sepsis Interpretation of arterial blood gasses Transport of critically ill patients Severe trauma Neurological emergencies
Oliguria and acute renal failure Cardiopulmonary resuscitation Arrhythmias Nutrition Sedation and analgaesia Venous thromboembolic disease Stress ulceration Cardiovascular and respiratory physiology Metabolic and electrolyte disturbances
o Paediatric sepsis o Liver and nutrition in the ICU o Renal support and paediatric CRRT o Ventilation (i.e., respiratory support, including mechanical ventilation) o Neurotrauma and critical care
Upon submitting verified documentation of meeting the general initial eligibility standards and the Part 1 training requirements, paying the Part 1 Exam Fee, and passing Part 1 of the EPIC Diploma exam, a Certificate in paediatric and neonatal intensive care will be issued.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 5 of 24
Part 2 Additional Eligibility Requirements
Part 2 is based on the completion of an additional year of specialist training (beyond the one year required for eligibility to take the Part 1 exam), and completing training in the following advanced topics:
o Ethics, family‐centred care, and professionalism o Safe unit structure, staffing, and leadership o Safe transport and advanced monitoring o Neonatal intensive care, and care of term and surgical infant o Cardiac ICU / ECMO / VAD
Upon submitting verified documentation of the additional training requirements, paying the Part 2 Exam Fee, and passing Part 2 of the Diploma exam, candidates will be awarded the EPIC™ (Paediatric / neonatal European Diploma Program in Intensive Care™). Those who earn the EPIC are authorized by ESPNIC’s Diploma Advisory Board to refer to themselves as a “Board Certified Specialist in Paediatric and Neonatal Intensive Care.” In this context, “Board Certified” means “certified by the Diploma Advisory Board of the European Society of Paediatric and Neonatal Intensive Care.” (For clarity, please note that ESPNIC is a scientific society, not a governmental regulatory authority, and not yet a Section, Division, or Multidisciplinary Joint Committee of the UEMS.)
Eligibility to take an EPIC Diploma program exam shall be for one year from the date of the eligibility notice. Practitioners who have already completed the training required for both Parts 1 and 2 may choose to take both parts of the exam on the same day or may take Part 2 on a later date. Candidates may not apply for only Part 2 without also applying for Part 1 (unless they already have passed Part 1). If a candidate who takes Parts 1 and 2 on the same day fails Part 1 but passes Part 2, that candidate will not earn the Diploma until he or she successfully passes Part 1. If the candidate passes Part 1 within one year of passing Part 2, he or she will not have to take the Part 2 exam again.
Ethics and Professionalism The European Society of Paediatric and Neonatal Intensive Care is committed to promoting excellence and professionalism through the EPIC Diploma program. Those who earn a credential from the European Society of Paediatric and Neonatal Intensive Care affirm their commitment to upholding the highest standards of personal and professional behaviour in the conduct of their endeavours, and commitment to comply with the ESPNIC Official Statements (http://espnic‐online.org/About/Official‐Statements). To file a complaint against a person who has a currently valid EPIC, please email espnic.diploma@espnic‐online.org. All credential holders against whom a complaint is filed shall be entitled to due process in the resolution of that complaint, including the right to utilize legal counsel at their own expense, and to face their accuser.
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 6 of 24

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 7 of 24
Applying for the EPIC Diploma To apply, please complete the Application Form that is available at: https://www.surveymonkey.com/r/EPICapplication. Using the same form, you may apply for Part 1 only, or both Part 1 and Part 2. The first opportunities to take the EPIC Diploma exam will be of the “beta” version of the exam; the exam content has been refined and approved by the ESPNIC Assessment Development Committee, but as a final quality‐control step we will measure the performance of those exam questions. To reward those leaders within the practice who are “early adopters” and help us acquire the exam performance data we need to finalize the exam content, those candidates who take the beta exam but do not pass will be able to retake the exam in its final form, without paying the Retest Fee (for the first retest only). Those who pass the beta version of Part 1 of the exam will earn the Certificate; those who pass both Part 1 and Part 2 will earn the Diploma. After the beta exam administrations, the exam will subsequently be available at test sites around the world. We anticipate launching the final version of the exam in Autumn 2016. Questions about the application process may be directed to espnic.diploma@espnic‐online.org or +41 22 560 7401. One of our Certification Department team members will respond to your message within three business days.
Approximately fifteen business days after your application is received, ESPNIC will notify you of your eligibility status. Eligible candidates will be provided with logistical details related to the exam and will be invited to the EPIC Diploma Candidate Study Group. Applicants who are deemed ineligible may appeal that determination to the Appeals Committee of the European Society of Paediatric and Neonatal Intensive Care Diploma Advisory Board by emailing espnic.diploma@espnic‐online.org.
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 8 of 24
EPIC Diploma Exam Fees
There is an exam fee for Part 1 and an exam fee for Part 2, with differentiated rates for ESPNIC Members / nonmembers and for applicants with current residence addresses in countries with Low‐Income / Lower‐Middle Income / Upper‐Middle Income / High‐Income economies per the World Bank classification at http://data.worldbank.org/about/country‐and‐lending‐groups#Low_income. Current exam fees are published on the ESPNIC website, http://espnic‐online.org/Education/Diploma. EPIC Diploma Exam Fees are nonrefundable if the applicant is deemed ineligible. Applicants are encouraged to review the eligibility requirements thoroughly and ask us questions (via email to espnic.diploma@espnic‐online.org or telephone at +41 22 560 7401) before submitting your application if you are unsure whether you are eligible.
Cancellation Policy EPIC Diploma Exam Fees are nonrefundable under any circumstances. If an applicant cancels at least ten (10) calendar days before that applicant’s scheduled exam date, ESPNIC will apply the fee that applicant paid towards a subsequent EPIC Diploma program application received by ESPNIC within one (1) year of the original scheduled exam date. Cancellations received later than ten (10) calendar days before an applicant’s scheduled exam date (including if an applicant is a no‐show at the scheduled exam administration) shall result in a complete forfeiture of the Exam Fee by that candidate, with no opportunity to defer the fee to a subsequent application cycle. Any difference between the original Exam Fee paid and the new Exam Fee will need to be paid by the applicant. Eligibility determinations are not deferrable; the applicant will need to satisfy all of the application requirements (work experience, application procedures, etc.) in effect at the time of the new application.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 9 of 24
Taking the Exam Eligible candidates will be provided with logistical details related to the exam. The EPIC beta exam components have the following number of questions and time allowed:
Exam Component Number of Questions Time Allowed to Complete Exam
Part 1 75 180 minutes (3 hours)
Part 2 75 180 minutes (3 hours)
Only pre‐registered and confirmed candidates will be admitted to the exam room. To confirm your identity, you must have with you a currently valid, government‐issued photo ID bearing the exact same name as the name you used on your application. If your government‐issued photo ID reflects a different name, you will not be able to gain admission to the test site. Please email espnic.diploma@espnic‐online.org if you need to update our records of your name to ensure that it matches your ID. EPIC Diploma exams are proctored and administered under strict security and standardized conditions. You must follow all proctor instructions. You will not be permitted to bring into the exam room any reference materials, notes, dictionaries, language translation dictionaries or devices, cellular telephones, PDAs, computers or tablets, calculators, cameras, video cameras, scanners, digital watches, or other electronic or communications devices.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 10 of 24
Special Accommodations Reasonable special accommodations for administration of the EPIC Diploma exams will be made for eligible candidates with documented disabilities in accordance with applicable law. Only those accommodations that do not, in ESPNIC’s sole discretion, compromise the validity of the exam results, will be approved. If circumstances indicate that administration of an EPIC Diploma exam would jeopardize the security of exam materials or the integrity of exam results, ESPNIC may cancel the administration of the exam. If a special accommodation is requested, supporting documentation must accompany the application from a licensed or otherwise properly credentialed healthcare professional who possesses expertise in the disability for which the modifications or accommodations are sought and has made an individualized assessment of the candidate, describing the disability and the need for the requested accommodation. For accommodation requests based on mental or cognitive impairment, supporting tests must have been conducted within five years prior to the date of the accommodations request. ESPNIC may make a request for supplemental information if the documentation submitted does not clearly establish the nature of the impairment or the need for the requested accommodations. Common reasons accommodations requests are deemed insufficient include:
Supporting documentation is from a person who is not licensed or otherwise properly credentialed
Supporting documentation is from a person who does not possess expertise in the disability for which the modifications or accommodations are sought
Supporting documentation is from a person who has not made an individualized assessment of the candidate
Supporting documentation does not describe the disability
Supporting documentation does not explain how the requested accommodation will negate the impact of the candidate’s disability on the fair assessment of the candidate’s EPIC Diploma program‐related competencies
ESPNIC shall consider all facts and explanations offered by the candidate regarding his or her history or the need for the requested testing accommodations, as well as objective evidence relating to the candidate’s diagnosed impairment and its impact on the candidate. ESPNIC shall not reject or deny an accommodation request based solely on the candidate’s average or above‐average IQ score, high level of academic success, or lack of a formal history of receiving that accommodation. ESPNIC may have the documentation submitted by or on behalf of a candidate reviewed by one or more qualified professionals of ESPNIC’s choosing at ESPNIC’s request and expense. ESPNIC will attempt to respond to each request for accommodations within 14 business days of receipt. Applicants who are not satisfied with ESPNIC’s decision regarding requested accommodations may appeal that determination to the Appeals Committee of ESPNIC’s Diploma Advisory Board by emailing espnic.diploma@espnic‐online.org.
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 11 of 24
Exam Results The pass / fail point (“cut score”) for each EPIC Diploma exam is set by the Assessment Development Committee, then reviewed and approved by the Diploma Advisory Board. To set the cut score, the Assessment Development Committee uses generally‐accepted, criterion‐referenced standard‐setting procedures (e.g., the Modified Angoff method). The cut scores will be announced approximately one month following the exam administration date. Approximately six weeks after the exam administration, ESPNIC will send you a report of your exam results. The report will indicate whether you passed or failed. Your results report will not provide any detailed information about your performance on individual test questions or other information that could compromise the security or validity of the exam. If you pass, ESPNIC will send you a Certificate (for Part 1) or Diploma (for Part 2) and other materials to recognize your achievement. If you do not pass on your first attempt, there is no limit on the number of times you may retake an EPIC Diploma exam, but you must demonstrate that you meet the eligibility requirements for each exam administration when you reapply, and you must pay the current Retest Fee when retaking the exam. However, candidates who take the beta version of the exam but do not pass will be able to retake the exam (in its final form) without paying the Retest Fee (for the first retest only). If ESPNIC’s Diploma Advisory Board determines that results of the exam do not represent a valid assessment of knowledge as sampled by the exam, such as due to irregular behavior or other reasons related to the exam administration, the results may be deemed invalid (neither pass nor fail). Examinees whose results are deemed invalid must retake the exam and achieve a passing score to achieve certification.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 12 of 24
Preparing for the EPIC Diploma exam General Strategies for Taking Written Tests The format of both Part 1 and Part 2 of the EPIC Diploma exam is multiple‐choice questions (MCQ) with five distinct answer options (there is no oral exam). Here are some general hints for taking this type of test:
Most importantly, the test is designed to have only one answer that is best, among the five options given.
Your attitude about the examination process can make a difference. Approach the test confidently. Arrive early to the test site, so you do not feel rushed.
The instructions read to you by the exam proctor are very important, so be sure to listen carefully. Ask questions if you do not understand any of the instructions, but be aware that your proctor cannot answer questions about test content.
Read all directions carefully—twice, if necessary.
Your score on this test will be based only on the number of correct choices you make (the number of times you select the best choice from the five answer options given). Blank responses and incorrect responses are both worth zero points. That means that you have nothing to lose by guessing the best answer to questions about which you are uncertain. You may want to mark uncertain guesses in your question booklet as you proceed through the test, then revisit those guesses if you have time after you finish the entire test.
Each test item is equally weighted, even though the exam’s topical content areas are weighted; the number of test items in a particular topical content area is proportionate to the weighting of that topical content areas.
Read each question carefully, making sure that you fully understand the question and your five choices before you answer the question. Do not waste time on questions that seem too unfamiliar or difficult. Interpret words according to their generally accepted meanings. Rephrase or underline key words in difficult questions. No question is intended to be a "trick" or "catch" question.
Answer easy questions first; postpone more difficult questions until later, making an initial guess in case you do not have enough time to revisit it. Check your answers if you have time; however, remember that your first response is often correct.
Watch your time carefully during the test.
If you find an exam item that you believe may be flawed, you can comment on the feedback page at the end of the exam. This is especially important during the beta exam administration. Try to focus on doing well on many items on the test, rather than getting bogged down on "making your case" on a single item that is worth just one point. Please include your reasons for believing that the item may be flawed. Exam item feedback comments must be completed during the time allotted for the exam. Subject‐matter experts and occupational testing specialists will carefully review all feedback comments. ESPNIC uses extensive quality‐control measures to optimize the validity and reliability of the certification exam, including panel reviews by qualified subject‐matter experts in the field and state‐of‐the‐art computerized scoring and item analysis techniques.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 13 of 24
Exam Specifications / Syllabus / Topical Blueprint The topical content of the exam is as follows:
Domains Weight (% of exam items)
1. Resuscitation and initial management of the acutely ill child 10%
2. Clinical assessment, investigation, data interpretation and monitoring 9%
3. Organ system support and therapeutic interventions 13%
A: Brain and nervous system 15% of 13% (2% overall)
B: Respiratory system 30% of 13% (3% overall)
C: Cardiovascular system 25% of 13% (3% overall)
D: Liver and gastrointestinal system 7% of 13% (1% overall)
E: Renal system and electrolytes 10% of 13% (1% overall)
F: Skin 1% of 13% (1% overall)
G: Haematology and coagulation 8% of 13% (1% overall)
H: Endocrine 4% of 13% (1% overall)
4. Perioperative care 5%
5. Compassionate and family‐oriented care and end‐of‐life care 4%
6. Patient safety 5%
7. Transport 3%
8. Trauma and burns 5%
9. Sepsis 7%
10. Professionalism and ethics 5%
11. Basic sciences 3%
12. Pharmacology and toxicology 5%
13. Unit management/governance 3%
14. Congenital defects / prematurity 4%
15. Long‐term care, home care, and discharge planning 2%
16. Environmental emergency 1%
17. Infectious disease 6%
18. Metabolism and nutrition 5%
19. Haemato‐oncology, oncology, and haematopoietic stem cell transplantation (HSCT) 3%
20. Management of the older child in the ICU 2%
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 14 of 24
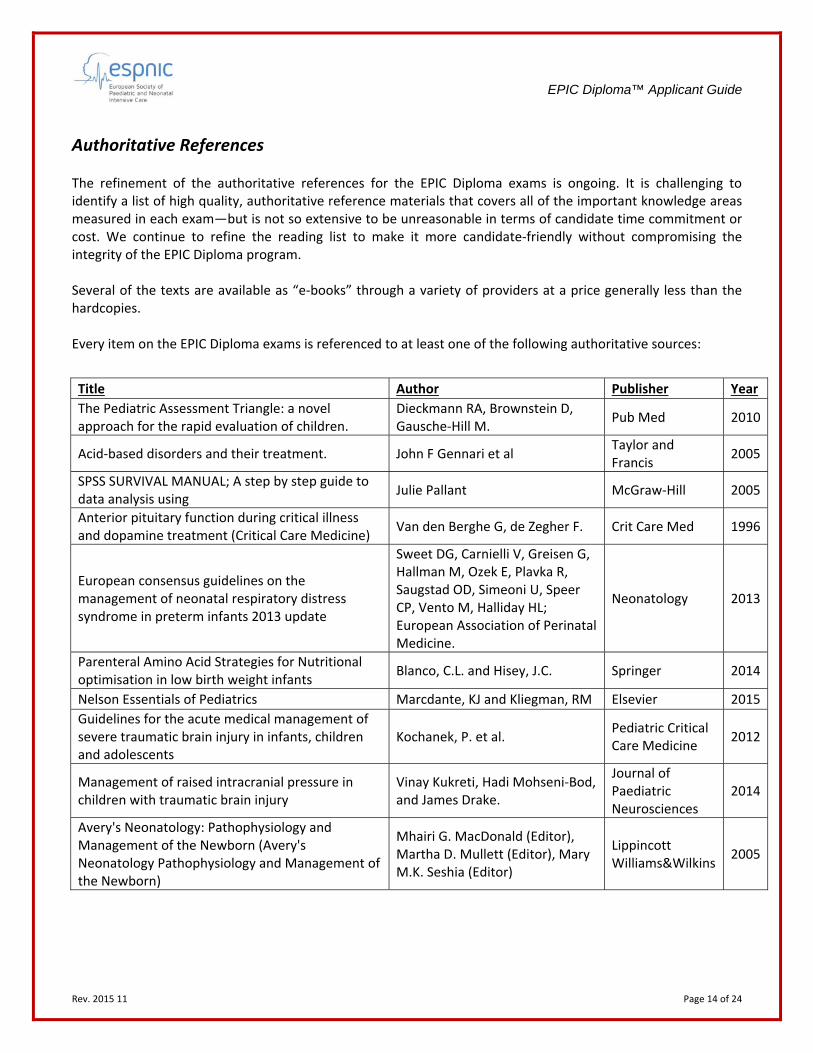
Authoritative References The refinement of the authoritative references for the EPIC Diploma exams is ongoing. It is challenging to identify a list of high quality, authoritative reference materials that covers all of the important knowledge areas measured in each exam—but is not so extensive to be unreasonable in terms of candidate time commitment or cost. We continue to refine the reading list to make it more candidate‐friendly without compromising the integrity of the EPIC Diploma program. Several of the texts are available as “e‐books” through a variety of providers at a price generally less than the hardcopies. Every item on the EPIC Diploma exams is referenced to at least one of the following authoritative sources:
Title Author Publisher Year
The Pediatric Assessment Triangle: a novel approach for the rapid evaluation of children.
Dieckmann RA, Brownstein D, Gausche‐Hill M.
Pub Med 2010
Acid‐based disorders and their treatment. John F Gennari et al Taylor and Francis
2005
SPSS SURVIVAL MANUAL; A step by step guide to data analysis using
Julie Pallant McGraw‐Hill 2005
Anterior pituitary function during critical illness and dopamine treatment (Critical Care Medicine)
Van den Berghe G, de Zegher F. Crit Care Med 1996
European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants 2013 update
Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, Saugstad OD, Simeoni U, Speer CP, Vento M, Halliday HL; European Association of Perinatal Medicine.
Neonatology 2013
Parenteral Amino Acid Strategies for Nutritional optimisation in low birth weight infants
Blanco, C.L. and Hisey, J.C. Springer 2014
Nelson Essentials of Pediatrics Marcdante, KJ and Kliegman, RM Elsevier 2015
Guidelines for the acute medical management of severe traumatic brain injury in infants, children and adolescents
Kochanek, P. et al. Pediatric Critical Care Medicine
2012
Management of raised intracranial pressure in children with traumatic brain injury
Vinay Kukreti, Hadi Mohseni‐Bod, and James Drake.
Journal of Paediatric Neurosciences
2014
Avery's Neonatology: Pathophysiology and Management of the Newborn (Avery's Neonatology Pathophysiology and Management of the Newborn)
Mhairi G. MacDonald (Editor), Martha D. Mullett (Editor), Mary M.K. Seshia (Editor)
Lippincott Williams&Wilkins
2005
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 15 of 24
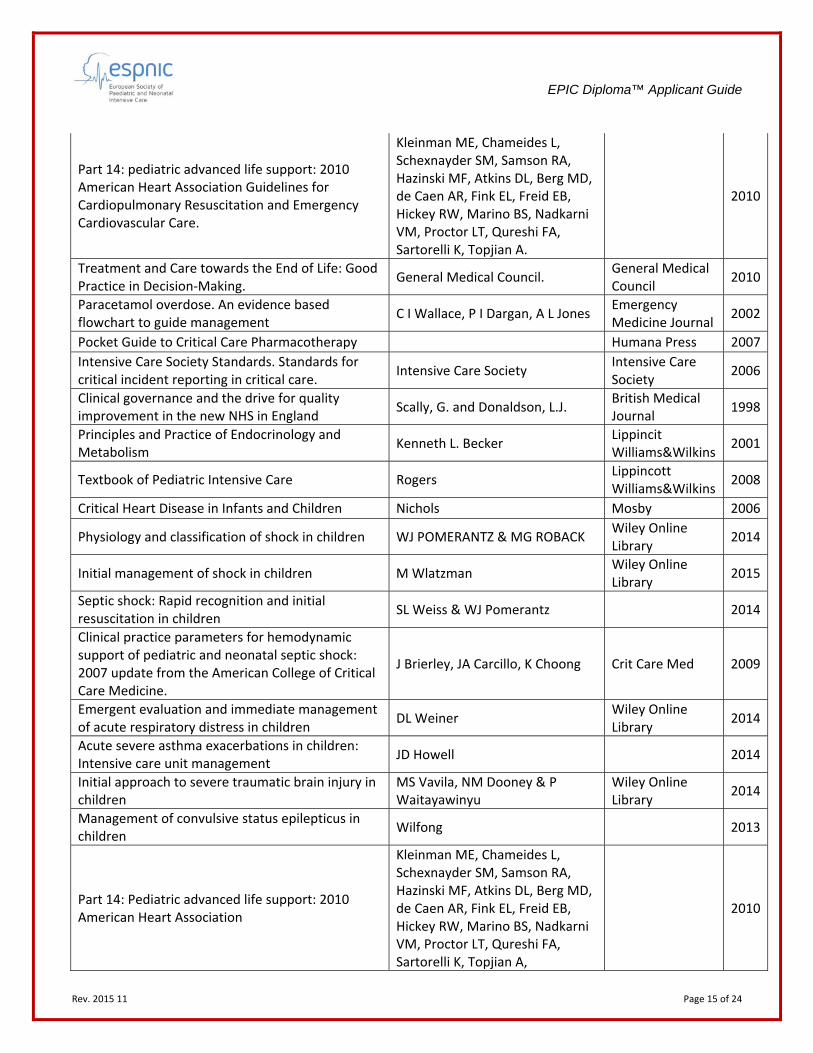
Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.
Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, Hickey RW, Marino BS, Nadkarni VM, Proctor LT, Qureshi FA, Sartorelli K, Topjian A.
2010
Treatment and Care towards the End of Life: Good Practice in Decision‐Making.
General Medical Council. General Medical Council
2010
Paracetamol overdose. An evidence based flowchart to guide management
C I Wallace, P I Dargan, A L Jones Emergency Medicine Journal
2002
Pocket Guide to Critical Care Pharmacotherapy Humana Press 2007
Intensive Care Society Standards. Standards for critical incident reporting in critical care.
Intensive Care Society Intensive Care Society
2006
Clinical governance and the drive for quality improvement in the new NHS in England
Scally, G. and Donaldson, L.J. British Medical Journal
1998
Principles and Practice of Endocrinology and Metabolism
Kenneth L. Becker Lippincit Williams&Wilkins
2001
Textbook of Pediatric Intensive Care Rogers Lippincott Williams&Wilkins
2008
Critical Heart Disease in Infants and Children Nichols Mosby 2006
Physiology and classification of shock in children WJ POMERANTZ & MG ROBACK Wiley Online Library
2014
Initial management of shock in children M Wlatzman Wiley Online Library
2015
Septic shock: Rapid recognition and initial resuscitation in children
SL Weiss & WJ Pomerantz 2014
Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine.
J Brierley, JA Carcillo, K Choong Crit Care Med 2009
Emergent evaluation and immediate management of acute respiratory distress in children
DL Weiner Wiley Online Library
2014
Acute severe asthma exacerbations in children: Intensive care unit management
JD Howell 2014
Initial approach to severe traumatic brain injury in children
MS Vavila, NM Dooney & P Waitayawinyu
Wiley Online Library
2014
Management of convulsive status epilepticus in children
Wilfong 2013
Part 14: Pediatric advanced life support: 2010 American Heart Association
Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, Hickey RW, Marino BS, Nadkarni VM, Proctor LT, Qureshi FA, Sartorelli K, Topjian A,
2010

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 16 of 24
Rapid sequence intubation (RSI) in children D Agrawal Wolters Kluwer / Lippincott & Wilkins
2014
Intracranial epidural hematoma in children: Clinical features, diagnosis, and management
ES Ahn & MR Proctor Wiley Online Library
2014
Airway foreign bodies in children FE Ruiz 2013
Initial assessment and stabilization of children with respiratory or circulatory compromise
S Fuchs Wiley Online Library
2015
Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies (Lancet)
Fleming S, Thompson M, Stevens R, et al
The Lancet 2011
Prevention and management of acute kidney injury (acute renal failure) in children
P Devarajan 2015
Management of heart failure in infants and children
RK Singh & TP Singh
2014
Etiology, clinical manifestations, and evaluation of neonatal shock
LM Adcock
2014
Overview of complications occurring in the post‐anesthesia care unit
DB Glick
2015
Tonsillectomy (with or without adenoidectomy) in children: Postoperative care and complications
AH Messner
2015
Anesthesia for elective spine surgery in adults MJ Brown 2015
Postoperative analgesia in infants and children PA Lönnqvist British Journal of anesthesia
2005
Common postoperative complications in children D Pawar Indian Journal of Anaesthesia
2012
Pediatric Acute respiratory distress syndrome: consensus recommendations from the pediatric acute lung injury consensus conference
Pediatric Acute Lung Injury Consensus Conference Group
Pediatric Critical Care Medicine
2015
Weaning and extubation readiness in pediatric patients
CJL Newth Pediatric Critical Care Medicine
2009
Surviving Sepsis Campaign: Guidelines. Special Considerations in Paediatrics
Dellinger et al. Crit Care Med 2013
0‐18 years: Guidance for all doctors General Medical Council General Medical Council
2007
The Paediatric Airway: Normal and Abnormal Shariffuddin, I.I and Chan, L. Springer 2014
Continuous Renal Replacement Therapy John A Kellum, Ronaldo Bellomo and Claudio Ronco
Oxford University Press
2010
Use of 2% 2‐phenoxyethanol and 0.1% octenidine as antiseptic in premature newborn infants of 23‐26 weeks gestation. (Journal of Hospital Infection)
Buhrer. C Elsevier 2002
Validation of the COMFORT Behavior scale and the FLACC scale for pain assessment in Chinese children after cardiac surgery (Pain management nursing)
Bai, J., Hsu, L., Tang, Y., & van Dijk, M
Elsevier 2012
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 17 of 24
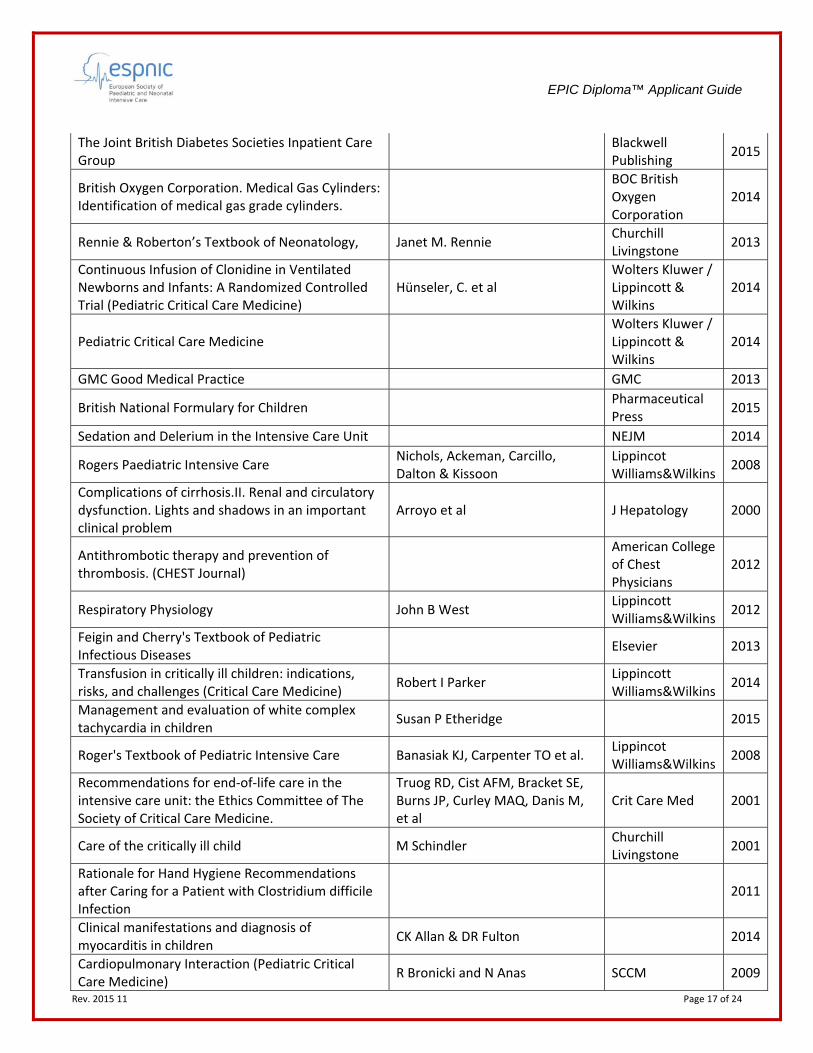
The Joint British Diabetes Societies Inpatient Care Group
Blackwell Publishing
2015
British Oxygen Corporation. Medical Gas Cylinders: Identification of medical gas grade cylinders.
BOC British Oxygen Corporation
2014
Rennie & Roberton’s Textbook of Neonatology, Janet M. Rennie Churchill Livingstone
2013
Continuous Infusion of Clonidine in Ventilated Newborns and Infants: A Randomized Controlled Trial (Pediatric Critical Care Medicine)
Hünseler, C. et al Wolters Kluwer / Lippincott & Wilkins
2014
Pediatric Critical Care Medicine
Wolters Kluwer / Lippincott & Wilkins
2014
GMC Good Medical Practice GMC 2013
British National Formulary for Children
Pharmaceutical Press
2015
Sedation and Delerium in the Intensive Care Unit NEJM 2014
Rogers Paediatric Intensive Care Nichols, Ackeman, Carcillo, Dalton & Kissoon
Lippincot Williams&Wilkins
2008
Complications of cirrhosis.II. Renal and circulatory dysfunction. Lights and shadows in an important clinical problem
Arroyo et al J Hepatology 2000
Antithrombotic therapy and prevention of thrombosis. (CHEST Journal)
American College of Chest Physicians
2012
Respiratory Physiology John B West Lippincott Williams&Wilkins
2012
Feigin and Cherry's Textbook of Pediatric Infectious Diseases
Elsevier 2013
Transfusion in critically ill children: indications, risks, and challenges (Critical Care Medicine)
Robert I Parker Lippincott Williams&Wilkins
2014
Management and evaluation of white complex tachycardia in children
Susan P Etheridge 2015
Roger's Textbook of Pediatric Intensive Care Banasiak KJ, Carpenter TO et al. Lippincot Williams&Wilkins
2008
Recommendations for end‐of‐life care in the intensive care unit: the Ethics Committee of The Society of Critical Care Medicine.
Truog RD, Cist AFM, Bracket SE, Burns JP, Curley MAQ, Danis M, et al
Crit Care Med 2001
Care of the critically ill child M Schindler Churchill Livingstone
2001
Rationale for Hand Hygiene Recommendations after Caring for a Patient with Clostridium difficile Infection
2011
Clinical manifestations and diagnosis of myocarditis in children
CK Allan & DR Fulton 2014
Cardiopulmonary Interaction (Pediatric Critical Care Medicine)
R Bronicki and N Anas SCCM 2009

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 18 of 24
Fluid and electrolytes in paediatrics: A comprehensive handbook
LG Feld and Kaskell, FJ Humana Press 2010
Textbook of Critical Care JL Vincent Wolters Kluwer / Lippincott & Wilkins
2011
Cardiac abnormalities in young women with anorexia nervosa (British Heart Journal)
Scalfi L, Galderisi M, Celentano A, Di Biase G, Tammaro P, Garofalo M, Mureddu GF, de Divitiis O, Contaldo F.
Pub Med 1994
Physiologic and pathophysiologic consequences of mechanical ventilation
RC Hyzy 2014
Severe acute asthma exacerbation in children: a stepwise approach for escalating therapy in a pediatric intensive care unit
Nievas I.F., Anand K.J.
Journal of Pediatric Pharmacology Therapy
2013
Circulatory shock (New England Journal of Medicine)
JL Vincent and D de Backer Massachusetts medical society
2013
Pathogenesis of pulmonary hypertension LJ Rubin & W Hopkins 2015
Critical care in the emergency department: acute kidney injury.
Andrew J Lewington, Andrea E Wootten, Kevin J Sim
Emergency Medicine Journal
2015
Neonatal and Pediatric Parenteral Nutrition (Advanced Critical Care)
Gragasz, Ann Lippincot Williams&Wilkins
2012
Parent Satisfaction in the PICU (Pediatric Clinics of North America)
Latour JM1, van Goudoever JB, Hazelzet JA.
Pediatric Clinics of North America
2008
Electrolyte quintet: Sodium Sumit Kumar and Tomas Berl The Lancet 1998
Advanced Paediatric Life Support: The Practical Approach
Advanced Life Support Group Wiley Online Library
2011
Red Book (30th Ed.) David. W. Kimberlin American Academy of Pediatrics
2015
Asthma Cardiac Arrest
Journal of anaesthesia and intensive care
2010
Guidelines for Environmental Emergencies United Nations 2013
Fluid overload before continuous hemofiltration and survival in critically ill children: a retrospective analysis (Critical Care Medicine)
Foland et al Crit Care Med 2010
Recommendations for the implementation of KMC for low birthweight infants (Acta Paediatrica)
Cattaneo A1, Davanzo R, Uxa F, Tamburlini G.
Wiley Online Library
1998
Extracorporeal Cardiopulmonary Support in Critical Care
Krisa Ed Van Meurs Wolters Kluwer / Lippincott & Wilkins
2012
Effort of breathing in children receiving high flow nasal cannula (Pediatric Critical Care Medicine)
S Rubin et al. Pediatric Critical Care Medicine
2014

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 19 of 24
Oxford Handbook of Medical Statistics Professor Jane Peacock Oxford University Press
2010
Every Error Counts: A web‐based Incident and Reporting Learning System for General Practice (British Medical Journal Quality and Safety)
B. Hoffman British Medical Journal
2008
Neonatology : Management Procedures on‐call problems, diseases and drugs
Tricia Lacy Gomella McGraw‐Hill 2004
Corticosteroids for the prevention and treatment of post‐extubation stridor in neonates, children and adults (Cochrane Database of Systematic Reviews)
Khemani, Randolph and Markovitz
Wiley Online Library
2009
GMC Guidelines GMC 2012
End‐of‐life care decisions in the pediatric intensive care unit: roles professionals play
Kelly Nicole Michelson, R. Patel, N. Haber‐Barker, L. Emanuel & J. Frader
Pediatric Critical Care Medicine
2013
Pulmonary contusion in children Alison Chantal Caviness 2013
The Renal Drug Handbook C ashley and Aileen Currie Radcliffe publishing Oxford‐New York
2014
Transporting newborn infants with suspected duct dependent congenital heart disease on low dose prostaglandin B1 without routine mechanical ventilation (Archives of Disease in Childhood ‐ Fetal and Neonatal Edition)
Kathryn A. Browning Carmo British Medical Journal
2007
The Ethics of Surgery: Conflicts and Controversies. Robert M. Sade Oxford University Press
2015
Manifestations of the shaken baby syndrome (Current Opinion in Ophthalmology)
Kivlin, Jane D. Wolters Kluwer / Lippincott & Wilkins
2001
Guidelines for the Prevention of Intravascular Catheter‐Related Infections (Journal of Vascular and Interventional Radiology)
O'Grady et al. Elsevier 2011
Part 15: Neonatal resuscitation: 2010 AHA Guidelines for Cardiopulmonary resuscitation and Emergency Cardiovascular Care (American Academy of Paediatrics) Circulation
Macmillan Publishers Limited.
2010
Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup (Intensive Care Medicine)
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent JL, Moreno R.
Springer 2013
Textbook of Palliative Care for Children Goldman, Hain & Liben Oxford University Press
2012
EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 20 of 24
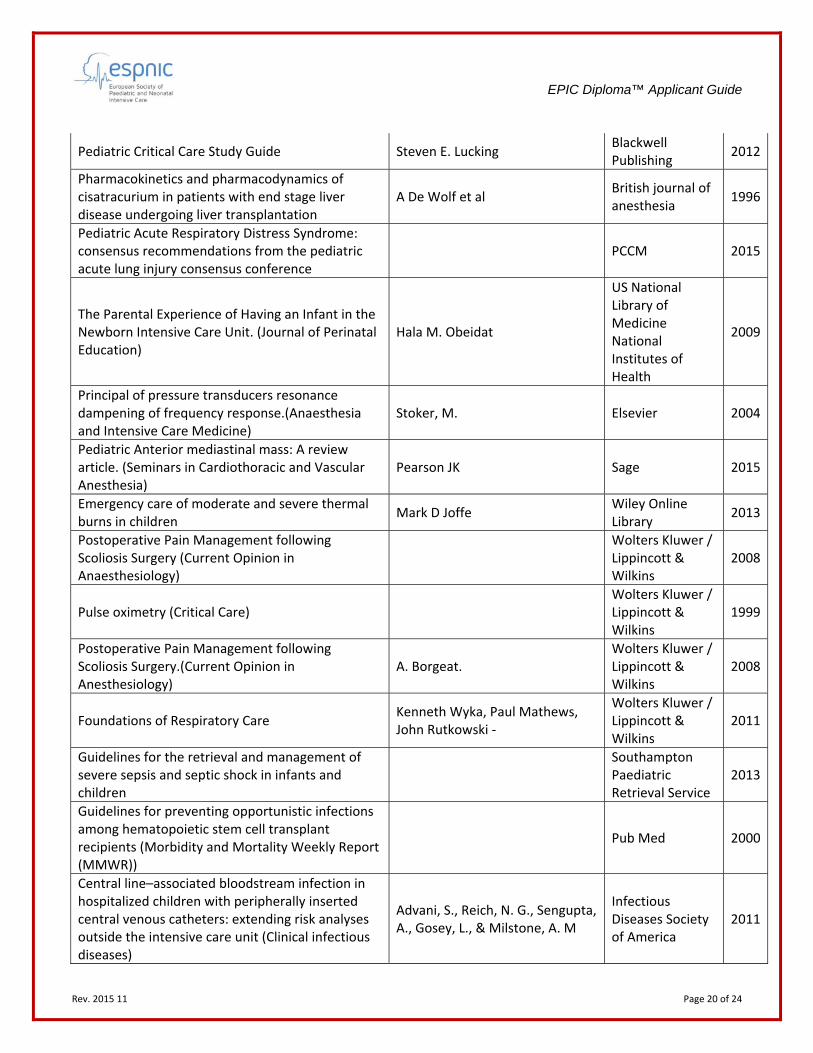
Pediatric Critical Care Study Guide Steven E. Lucking Blackwell Publishing
2012
Pharmacokinetics and pharmacodynamics of cisatracurium in patients with end stage liver disease undergoing liver transplantation
A De Wolf et al British journal of anesthesia
1996
Pediatric Acute Respiratory Distress Syndrome: consensus recommendations from the pediatric acute lung injury consensus conference
PCCM 2015
The Parental Experience of Having an Infant in the Newborn Intensive Care Unit. (Journal of Perinatal Education)
Hala M. Obeidat
US National Library of Medicine National Institutes of Health
2009
Principal of pressure transducers resonance dampening of frequency response.(Anaesthesia and Intensive Care Medicine)
Stoker, M. Elsevier 2004
Pediatric Anterior mediastinal mass: A review article. (Seminars in Cardiothoracic and Vascular Anesthesia)
Pearson JK Sage 2015
Emergency care of moderate and severe thermal burns in children
Mark D Joffe Wiley Online Library
2013
Postoperative Pain Management following Scoliosis Surgery (Current Opinion in Anaesthesiology)
Wolters Kluwer / Lippincott & Wilkins
2008
Pulse oximetry (Critical Care)
Wolters Kluwer / Lippincott & Wilkins
1999
Postoperative Pain Management following Scoliosis Surgery.(Current Opinion in Anesthesiology)
A. Borgeat. Wolters Kluwer / Lippincott & Wilkins
2008
Foundations of Respiratory Care Kenneth Wyka, Paul Mathews, John Rutkowski ‐
Wolters Kluwer / Lippincott & Wilkins
2011
Guidelines for the retrieval and management of severe sepsis and septic shock in infants and children
Southampton Paediatric Retrieval Service
2013
Guidelines for preventing opportunistic infections among hematopoietic stem cell transplant recipients (Morbidity and Mortality Weekly Report (MMWR))
Pub Med 2000
Central line–associated bloodstream infection in hospitalized children with peripherally inserted central venous catheters: extending risk analyses outside the intensive care unit (Clinical infectious diseases)
Advani, S., Reich, N. G., Sengupta, A., Gosey, L., & Milstone, A. M
Infectious Diseases Society of America
2011

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 21 of 24
Measures to Control and Prevent Clostridium difficile Infection (Clinical infectious diseases)
D. N. Gerding Infectious Diseases Society of America
2008
Clinical Practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 Update from American College of Critical Care Medicine (Critical Care Medicine)
Joe Brierley. Wolters Kluwer / Lippincott & Wilkins
2009
Recommendations for end of life care in the Intensive Care Unit: American College of Critical Care Medicine
Robert D Truog Wolters Kluwer / Lippincott & Wilkins
2008
Surviving sepsis campaign: International Guidelines for Management of Severe Sepsis and Septic Shock (Critical Care Medicine)
R. Phillip Dellinger. Wolters Kluwer / Lippincott & Wilkins
2013
Diagnostic Accuracy of Delirium Diagnoses in Pediatric Intensive Care: A Systematic Review (Critical Care Medicine)
A. Daoud Wolters Kluwer / Lippincott & Wilkins
2014
How to investigate and analyse clinical incidents: clinical risk unit and association of litigation and risk management protocol (British Medical Journal)
Vincent C, Taylor‐Adams S, Chapman EJ, Hewett D, Prior S, Strange P, Tizzard A
British Medical Journal
2000
Evidence based medicine: What it is and what it isn’t.
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS.
British Medical Journal
1996
Treatment of burns in the first 24 hours: Simple and practical guide by answering ten questions in a step‐by‐step form (World Journal of Emergency Surgery)
Ziyad Alharbi BioMed Central 2012
Pediatric Acute Respiratory Distress Syndrome: consensus recommendations from the pediatric acute lung injury consensus conference (Pediatric Critical Care Medicine)
The pediatric acute lung injury consensus conference group
Pediatric Critical Care Medicine
Acute severe asthma exacerbations in children: Endotracheal intubation and mechanical ventilation
Joy D Howell 2014
Goodman & Gilman's The Pharmacological Basis of Therapeutics
Bruce Chabner, Laurence Brunton, Bjorn Knollman, Bruce A. Chabner
McGraw‐Hill 2011
Online Study Group ESPNIC has established an EPIC Diploma Candidate Study Group, hosted online as a LinkedIn Group, to empower eligible candidates to share knowledge, work with mentors, and network with peers who also plan to take the exam. Candidates will be invited to the EPIC Diploma Candidate Study Group upon being notified that they are eligible.

Rev. 2015 11 Page 22 of 24
Recertification / Renewal / Maintenance of Certification
Frequency of Recertification
Period
Barring suspension or revocation, the EPIC is valid for five (5) years and may be renewed—either by exam (to ensure continued minimal competence) or by continuing professional development (CPD) (to ensure continual enhancement of competence).
By Exam Board Certified Specialists in Paediatric and Neonatal Intensive Care choosing to recertify by exam must take the full‐length, current version of the initial certification exam as of the last year of the recertification period.
By Continuing Professional Development
Board Certified Specialists in Paediatric and Neonatal Intensive Care choosing to recertify by continuing professional development must earn 100 CPD points over the course of the 5‐year recertification period, with at least 1 CPD point earned every year.
To count towards EPIC recertification, all CPD activity topics must align with the EPIC Diploma exam specifications.
CPD activities include:
1) Continuing Medical Education (CME) 1 CPD point per 60 minutes of instructional time of a CME activity accredited by ECCME or
ACCME CME activities must be a minimum of 30 minutes; shorter sessions do not count for CPD
points *At least 40 CPD points must be in this category
2) Teaching 2 CPD points per 60 minutes of instructional time of a CME activity accredited by ECCME or
ACCME CME activities must be a minimum of 30 minutes; shorter sessions do not count for CPD
points
3) Research / Authorship 5 CPD points for lead development and presentation / 2 CPD points for contributing
development and presentation of a peer‐reviewed poster at a medical congress 10 CPD points for lead authorship / 5 CPD points for contributing authorship of a peer‐
reviewed article in a journal or a peer‐reviewed chapter in a textbook 20 CPD points for lead authorship / 10 CPD points for contributing authorship of a peer‐
reviewed textbook
4) Quality Improvement 20 CPD points for completing a quality improvement project that incorporates strategies for
improvement and tracks performance over time *At least 20 CPD points must be in this category
5) Leadership and Service 1 CPD point per hour of actual meeting time for service on a relevant committee or board 1 CPD point per draft Diploma exam item accepted as viable by the ESPNIC Assessment
Development Committee
Professional Standing / Probity / Personal Health
A valid, unrestricted medical license in at least one jurisdiction. If multiple licenses are held, each must be valid and unrestricted.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 23 of 24
Irregular Behavior Any behavior that threatens the integrity or security of the EPIC Diploma program application, exams, or credentialing processes is considered by ESPNIC to be irregular behavior. Irregular behavior includes, but is not limited to:
Making false representations on initial certification or recertification applications or falsifying supporting documentation.
Altering or falsifying EPIC certificates or diplomas, or otherwise misrepresenting certification status.
Altering or falsifying EPIC Diploma exam results reports or otherwise misrepresenting exam performance.
Seeking or having access to EPIC Diploma exam content (other than official, ESPNIC‐sanctioned exam preparatory materials) before the exam is administered.
Impersonating an examinee or engaging someone else to take an EPIC Diploma exam by proxy.
Copying exam answers from someone else or allowing answers to be copied.
Copying or memorizing and reproducing exam items for personal or competing use or distribution.
Purchasing or stealing EPIC Diploma exam materials.
Possessing unauthorized materials or equipment during an EPIC Diploma exam administration.
Making a false or intentionally misleading report accusing others of irregular behavior. To help ESPNIC maintain the integrity of its credentialing processes, anyone acting in good faith that has information or evidence that irregular behavior has occurred is encouraged to submit a written statement to the Ethics and Professionalism Committee of ESPNIC’s Diploma Advisory Board (by email to espnic.diploma@espnic‐online.org) detailing the incident and providing copies of any supporting evidence or documentation. If the Ethics and Professionalism Committee determines that irregular behavior has occurred, it may invalidate scores, suspend or revoke existing credentials, temporarily or permanently bar individuals from certification, or impose other sanctions or take other actions as it deems appropriate, including civil or criminal legal action. Adverse decisions of the Ethics and Professionalism Committee may be appealed by the sanctioned individual to the Appeals Committee of ESPNIC’s Diploma Advisory Board by emailing espnic.diploma@espnic‐online.org.
Revalidation of EPIC Diploma Program Exam Content To ensure the continuing relevance, accuracy, and validity of the content of the EPIC Diploma exams, ESPNIC performs a revalidation (updating the exam specifications, initial eligibility standards, and recertification standard) periodically according to the pace of change in the practice. Currently, the Diploma Advisory Board has defined this period as every five years.

EPIC Diploma™ Applicant Guide
Rev. 2015 11 Page 24 of 24
Grievances, Policy Interpretation Reviews, and Appeals If an EPIC Diploma program applicant, eligible candidate, or current or past certificant (Board Certified Specialist in Paediatric and Neonatal Intensive Care) disagrees with a credentialing decision or policy, review of the decision or policy may be requested. Such requests must be submitted to the Appeals Committee of ESPNIC’s Diploma Advisory Board by email to espnic.diploma@espnic‐online.org and should include all appropriate supporting documentation. The Appeals Committee will review all requests and provide a response within a reasonable time—usually within 90 days of receipt.
Data Confidentiality and Release of Credentialing Information to Third Parties All data provided to ESPNIC or its representatives, contractors, or agents as part of the credentialing process is maintained under strictest security. ESPNIC may provide information necessary for compliance with laws and court orders. ESPNIC and its credentialing management team may share initial certification applicant data, exam results, candidate exam comments, and recertification applicant data with members of the Diploma Advisory Board and its relevant committees. ESPNIC and its credentialing management team may confirm credentialing status to third parties, including date of issuance and expiration date, but ESPNIC will provide no other information relative to an individual’s credentialing status without written authorization by the individual in question.