esophagus
TRANSCRIPT

OESOPHAGUS

Surgical anatomy
The esophagus is a two-layered
mucosa-lined muscular tube that
journeys through the neck, chest, and
abdomen and rests unobtrusively in
the posterior mediastinum.
It commences at the base of the
pharynx at C6 and terminates in the
abdomen, where it joins the cardia of
the stomach at T11
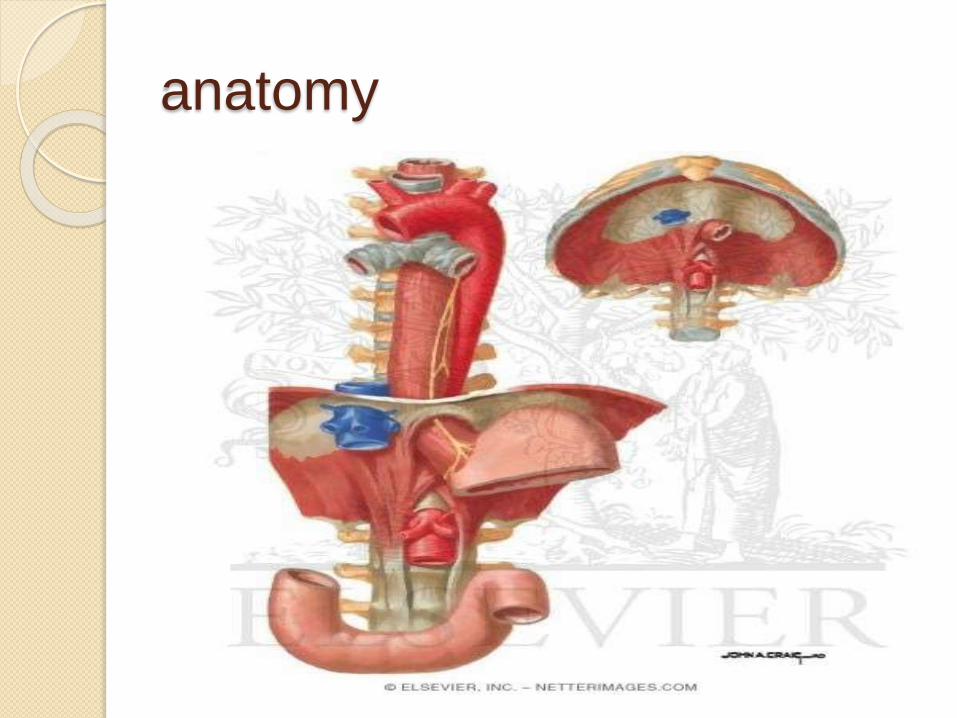
anatomy

Anatomy
Arch of aorta makes an impression on oesophagus–radiograph & endoscopy
Symptoms of
oesophageal
disorders
Dysphagia. This term means a sensation ofobstruction
during the passage of liquid or solid through the
pharynx or oesophagus, i.e. within 15 seconds of food
leaving the mouth.
The characteristics of the
progression of dysphagia to solids can be helpful, e.g.
intermittent slow progression with a history of heartburn
suggests a benign peptic stricture;
Relentless progression over a few weeks suggests a malignant
stricture.
The slow onset of dysphagia for solids and
liquids at the same time suggests a motility disorder

Odynophagia is pain during the act
of swallowing and
is suggestive of oesophagitis.
Causes include reflux,
infection, chemical oesophagitis

Substernal discomfort, heartburn. This is a common
symptom of reflux of gastric contents into the oesophagus
usually a retrosternal burning pain thatcan spread to the neck, across the chest, and whensevere can be difficult to distinguish from the pain ofischaemic heart disease.

Chest pain-GERD;motility
disorders
Regurgitation is the effortless
reflux of oesophageal contents into
the mouth and pharynx.
it occurs frequently in patients with
gastro-oesophageal reflux disease or
organic stenosis.

reflux
Passive return of gastro duodenal
contents to mouth
Occurs in GERD
Symptoms-
1. loss of weight
2. Change of voice-irritation of vocal
cord
3. Cough or dyspnoe-tracheal
aspiration

Investigation of oesophageal
disorders Barium swallow and meal.
endoscopy
1. Oesophagoscopy.
2. Video endoscopy
Manometry
PH recording

Radiographic Evaluation
The first diagnostic test in patients
with suspected esophageal disease
should
be a barium swallow including a full
assessment of the stomach and
duodenum
radiography
Plain x-ray-foreign body
Barium swallow-motility
disorders,space occupying lesion
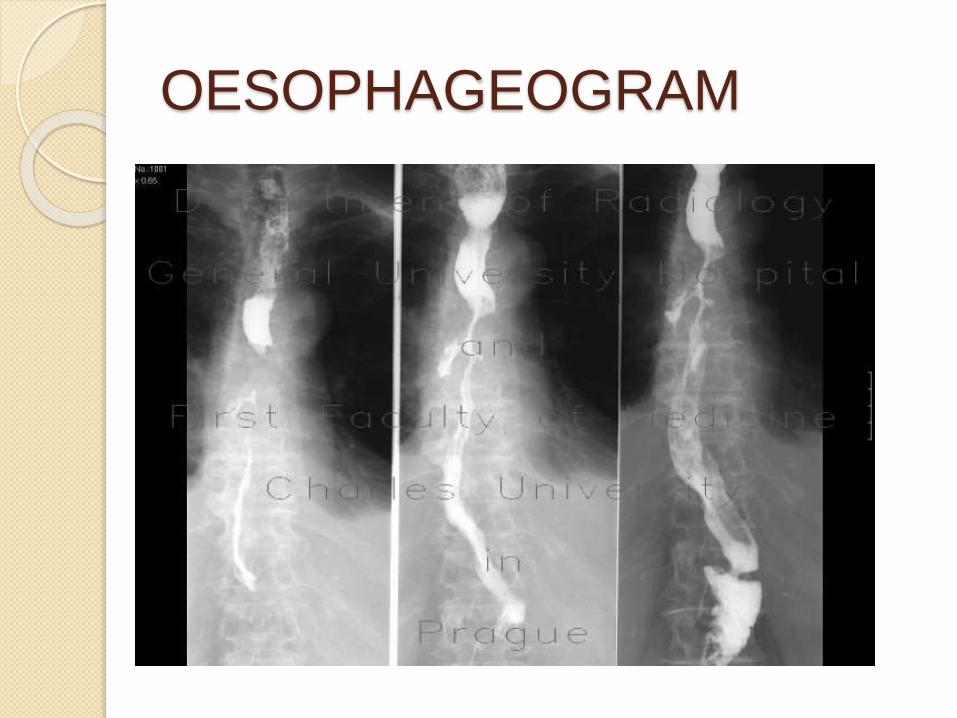
OESOPHAGEOGRAM
endoscopy
To view inside of oesophagus &
oesophagogastric jn
Types
1. Rigid oesophagoscope
2. Flexible video endoscope
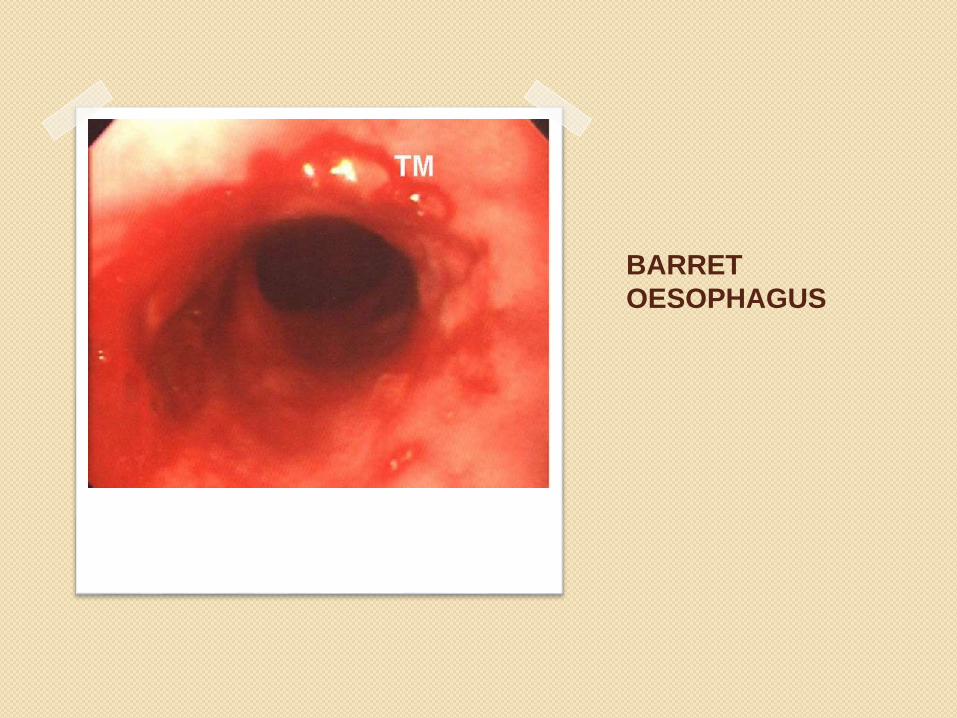
BARRET
OESOPHAGUS

carcinoma
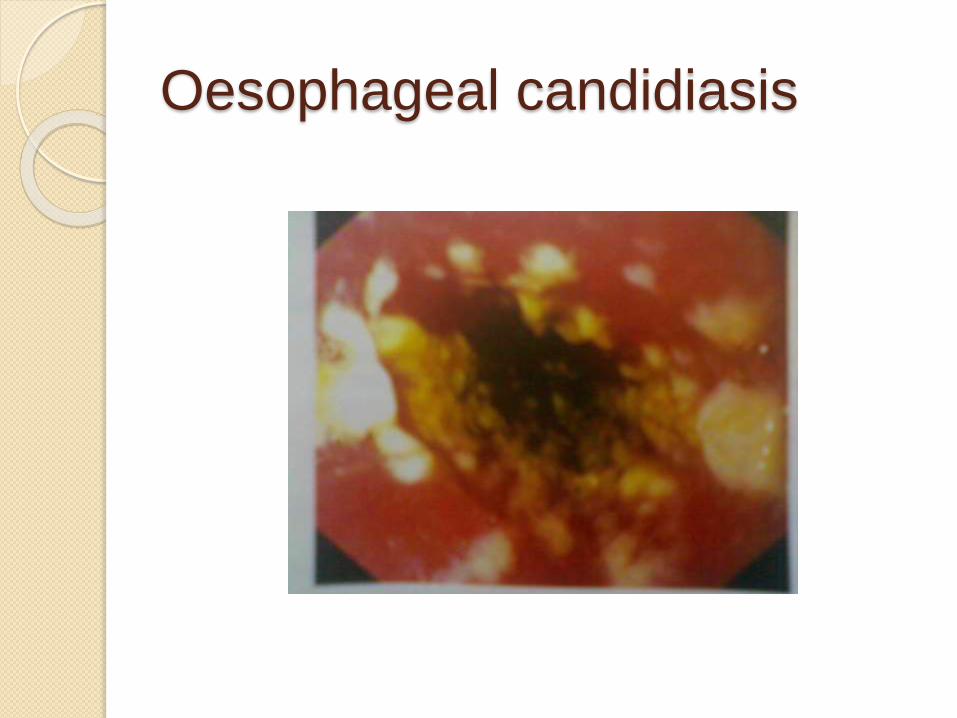
Oesophageal candidiasis

Oesophageal manometry
manometry is particularly necessary to
confirm the diagnosis of specific
primary
esophageal motility disorders (i.e.,
achalasia, diffuse esophageal spasm,
nutcracker esophagus, and
hypertensive LES).

24hr ph monitoring
Prolonged monitoring
of esophageal pH is performed by placing the pH probe or telemetry capsule
5 cm above the manometrically measured upper border of the distal sphincter
for 24 h.
It measures the actual time the esophagealmucosa is exposed to
gastric juice, measures the ability of the esophagus to clear refluxed acid, and
correlates esophageal acid exposure with the patient’s symptoms.
Congenital anomalies
Ectopic gastric mucosa can occur in
upper third of oesophagus
Atresia- lack of lumen formation- usually
asso-tracheo-oesophageal fistula
Fistula- aspiration & paroxysmal
suffocation from food are obvious hazards-
detected immediately after birth- aspiration
pneumonia-
O.stenosis-narrowing of lumen
Dysphagia lusoria due to vascular anomaly

Esophageal atresia and tracheooesophageal fistula
Commonest C
C.Blind upper segment,fistula between the lower segment & trachea
Clinical features-oesophageal
atresia Baby regurgitates all feeds
Saliva –continuosly from mouth
Coughing & cyanosis on feeding
As a part of;
Vertibral body segmentation
Anal atresia
Cvs-PDA
TE fistula
Renal agenesis

diagnosis
NG tube comes against an obstuction
with in 10 cm
Lateral CXR-lucent proximal pouch
that displace the trachea anteriorly
Corrective surgery – thoracotomy at
the level of 5th ics
Lower segment is divided at its
entrance in to trachea & fistula is
closed
treatment

complication
Pneumonia
Leakage from anastamosis

Foreign bodies-common
impacted material is
food
in children-coin,pin…
Foreign body
The flexible upper gastrointestinal
endoscope should be inserted under
direct visualization to avoid
inadvertently striking an object and
further impacting it or causing it to
penetrate the esophageal wall. Blunt
foreign bodies such as coins can be
securely grasped with a forceps or a
snare. A firm grasp on the foreign
body is required before withdrawal is
attempted.

COIN IN OESOPHAGUS

Button Batteries
A button battery lodged in the
esophagus is a true emergency and
immediate removal is indicated to
avoid the rapid corrosive action of
the alkaline substance on the
mucosa and subsequent
complications.
perforation Perforation of the esophagus is a surgical emergency.
Early detection and surgical repair within the first 24 hours results in 80% to 90% survival; after 24 hours, survival decreases to less than 50%.
Upon presentation, patients suspected of having a perforation based on initial history and physical exam are evaluated quickly so that surgical intervention may be initiated promptly.
Perforation from forceful vomiting (Boerhaave'ssyndrome), foreign body ingestion, or trauma accounts for 15%, 14%, and 10% of cases, respectively.
Most esophageal perforations occur after endoscopic instrumentation for a diagnostic or therapeutic procedure, including dilation, stent placement, and laser fulguration.
Other iatrogenic causes that have been noted include difficult endotracheal intubation, blind insertion of a mini-tracheostomy, and inadvertent injury during dissections in the neck, chest and abdomen.

1. Boerhaave's Syndrome-baro
trauma recurrent emesis disrupts the
normal vomiting reflex that enables
sphincter relaxation, resulting in an
increase in intrathoracic
esophageal pressure and
perforation. Postemetic rupture of
the esophagus, now known as
Boerhaave's syndrome, is only one
of many causes of esophageal
rupture.
C/F
Severe pain in chest following meal
Upper abdomen rigid
Mistaken as MI or perforated peptic
ulcer

2.Pathological perforation
Perforation of ulcers(barret ulcer or
tumours)
Causes erosion in to aorta or
ventricle-fatal
3 .Penetrating injury by knifes &
bullet-un common
4.During removal of foreign body
5.Instumental perforation
Diagnosis
Mediastinal emphysema, a strong
indicator of perforation
The diagnosis is confirmed with a
contrast esophagogram, which will
demonstrate extravasation in 90
percent of patients.
The use of a watersoluble
medium such as Gastrografin is
preferred


Treatment
The management of patients with esophagealperforation takes place in both the ICU and in the operating room.
Patients with an esophageal perforation can progress rapidly to hemodynamic instability and shock.
If perforation is suspected, appropriate resuscitation measures with the placement of large-bore peripheral IV catheters, a urinary catheter, and a secured airway are undertaken before the patient is sent for diagnostic testing.
IV fluids and broad-spectrum antibiotics are started immediately, and the patient is monitored in an ICU

Surgery is not indicated for every
patient with a perforation of the
esophagus, and management is
dependent on several variables:
stability of the patient, extent of
contamination, degree of
inflammation, underlying
esophageal disease, and location of
perforation

three criteria for the nonoperative
management
of esophageal perforation: (1) the
barium swallow must show the
perforation to be contained within the
mediastinum and drain well back into
the esophagus, (2) symptoms should
be mild, and (3) there should be
minimal
evidence of clinical sepsis.

Principles of non op mgmnt
Analgesia
Nil by mouth
Abx
IV fluids

Op management
Thoracotomy & repair of perforation
done with in few hours of perforation
Insertion of stents for treatment of
perforated cancer
1/18/2015 43