escitalopram: an open-label study of bereavement-related depression and grief
TRANSCRIPT

Journal of Affective Disorders 113 (2009) 142–149www.elsevier.com/locate/jad
Research report
Escitalopram: An open-label study of bereavement-relateddepression and grief
Paula L. Hensley a,⁎, Carol K. Slonimski b, E.H. Uhlenhuth a, Paula J. Clayton c
a Department of Psychiatry, School of Medicine, University of New Mexico Health Sciences Center, Albuquerque, New Mexico, United Statesb Advanced Medical Centers of Alaska, Fairbanks, Alaska, United States
c American Foundation for Suicide Prevention, New York City, New York, United States
Received 29 January 2008; received in revised form 21 May 2008; accepted 22 May 2008Available online 2 July 2008
Abstract
Background: Approximately 8 million Americans suffer the loss of an immediate family member each year. Chronic depressionmay develop following bereavement—about 15% of the bereaved are depressed at 1 year. Several studies of psychotropicmedications have demonstrated improvement in depression ratings, but little data exists for selective serotonin reuptake inhibitortreatment in bereavement-related depression.Methods: Thirty adults were treated with escitalopram for 12 weeks in open fashion for a major depressive episode following loss of aclose family member (parent, sibling, child, or spouse/significant other). Main outcome measures were the Hamilton DepressionRating Scale, the Montgomery–Asberg Rating Scale, the Texas Revised Inventory of Grief, and the Inventory of Complicated Grief.Results: Twenty-nine of thirty participants returned for at least one set of efficacy measures after starting medication. Nineteensubjects (66%) experienced a 50% or greater improvement on the Hamilton Depression Scale. Fifteen subjects (52%) achievedremission, defined as a final score of 7 or less on the Hamilton Depression Scale. Escitalopram significantly reduced depressivesymptoms (Pb0.001) over time. Subjects with uncomplicated grief and those with complicated grief improved similarly over time.Subjects with and without PTSD improved to a similar degree. Escitalopram was well tolerated.Limitations: Open-label design, psychotherapy was not controlled, relatively short treatment period, variation in grief scales makecomparisons to other studies difficult, all subjectswith complicated grief alsowere clinically depressed, and gender discrepancy of sample.Conclusions: Escitalopram improved depressive, anxiety, and grief symptoms in individuals experiencing a major depressiveepisode related to the loss of a loved one.© 2008 Elsevier B.V. All rights reserved.
Keywords: Depression; Bereavement; Grief; Complicated grief; Post-traumatic stress disorder
1. Introduction
In the US, approximately 800,000 people are newlywidowed each year (Zisook et al., 1994a). Approxi-
⁎ Corresponding author. 2118 Central Ave SE, Suite 37, Albuquer-que, NM 87 106, United States.
E-mail address: [email protected] (P.L. Hensley).
0165-0327/$ - see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.jad.2008.05.016
mately 8 million Americans per year suffer the loss of animmediate family member. In the Diagnostic andStatistical Manual of Mental Disorders, 4th edition-TR(DSM-IV-TR, American Psychiatric Association,2000), bereavement is listed as a V code for additionalconditions that may be a focus of clinical attention. ByDSM conventions, in circumstances in which depres-sion follows bereavement, MDD is not diagnosed until

143P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
at least 2 months have passed since the loss. There aresome symptoms, however, that the DSM notes may helpto distinguish a grief reaction from a Major DepressiveEpisode—guilt, thoughts of suicide, worthlessness,psychomotor retardation, marked functional impair-ment, and hallucinations, which are symptoms thattypically occur only in depression (DSM-IV-TR, 2000).If we disregard the usual convention of not diagnosingdepression until 2 months have passed since the loss,40% of bereaved individuals meet depressive criteriawithin 1 month of the loss (Clayton and Darvish, 1979).Chronic depression may develop following bereave-ment; approximately 15–16% of the bereaved aredepressed at 1 year (Clayton andDarvish, 1979; Clayton,1990; Zisook and Shuchter, 1991) and approximately7% are depressed at 2 years following a loss by death(Zisook et al., 1994b). Bereavement-related depressionappears to have a 1:1 gender distribution, unlike majordepressive disorder's 2:1 greater prevalence in women.
In Clayton's work with several samples of bereavedpatients, few significant differences emerged to predictlong-term outcome. She foundminimal symptomatic diffe-rences between women and men, between those in a goodmarriage vs. a bad one, between those who consideredthemselves religious vs. those who did not, and betweenthose who experienced a sudden loss vs. a loss that was notsudden (Clayton et al., 1968, 1971; Clayton and Darvish,1979). In Clayton and Darvish's report on 171 subjects, 62of whom were under age 45, a third of the deaths (N=56)were sudden, defined as an illness length of 4 days or less(Clayton andDarvish, 1979). Of 29 symptoms evaluated inthe 149 subjects who completed interviews at 1 month and13 months following the loss, two symptoms weresignificantly different in the sudden loss group at thesecond interview. The sudden loss group endorsed lesscrying than the non-sudden loss group yet reported greaterfeelings of anger about the death at 13 months.
Apart from bereavement-related major depression,complicated grief (CG), previously referred to as trau-matic grief, is another potential consequence of loss. CGis not a DSM diagnosis at this time. Present in approx-imately 10 to 20% of bereaved people, CG is adebilitating disorder whose sufferers typically report asense of disbelief about the death, anger, bitterness,yearning, longing, and preoccupation with the deceased(Shear et al., 2005). Comorbidity with other psychiatricconditions is high. In a sample of patients seekingtreatment for complicated grief, current major depressivedisorder was present in 52%, post-traumatic stressdisorder in 30%, and panic disorder in 26%; overallonly 9% of the patients had no current or lifetime Axis Idiagnosis by DSM-IV criteria (Melhem et al., 2001).
In several open-label studies (Jacobs et al., 1987;Pasternak et al., 1991; Zisook et al., 2001; Zygmont et al.,1998), a double-blind, parallel group study (Oakley et al.,2002), and one double-blind placebo-controlled study(Reynolds et al., 1999), individuals with bereavement-related depression and CG have been treated successfully.The first of the open-label studies treated 10 widows andwidowerswith a tricyclic antidepressant (desipramine in 9subjects and nortriptyline in 1) for 4 weeks. Seven of thesubjects were rated as very much or much improved indepression ratings by the end of the trial (Clinical GlobalImpression, CGI of 1 or 2) (Jacobs et al., 1987). In sevenof eight subjects in whom grief intensity was assessed,grief intensity declined, but only three of these exper-ienced a decrease in grief “ofmajor proportion” accordingto the authors (Jacobs et al., 1987).
In the second open-label trial, thirteen widows andwidowers received treatment with nortriptyline until theyachieved a response, defined as attaining a HamiltonDepression Rating Scale (HAM-D) score of less than orequal to 10 for three or more weeks with a therapeuticblood level of nortriptyline, then continued medicationfor an additional 16 weeks (Pasternak et al., 1991).Treatment began between 2 and 25 months after the loss.The pre- to post-treatment means on the HAM-D dec-lined by 67.9% (Pasternak et al., 1991). Grief intensitydeclined in eleven of the thirteen subjects, but meandecrease in scores on the Texas Revised Inventory ofGrief (TRIG; Faschingbauer, 1981) was only 9.3%.
In the third open-label trial, 22 depressed widows andwidowers were treated with bupropion SR for 8 weeks(Zisook et al., 2001). All subjects entered the studywithin 8 weeks of bereavement. Thirteen subjectsexperienced at least a 50% reduction in HAM-D scores,and twelve were very much or much improved on theCGI. Mean scores of grief, as measured by the Inventoryof Complicated Grief (ICG), improved by 18% overall.
In a fourth open-label trial, 15 subjects with com-plicated grief (then called traumatic grief) were treatedfor 4 months with paroxetine and a new psychotherapytreatment for complicated grief, which was in develop-ment at the time (Zygmont et al., 1998). Medicationtreatment began at a median of 17 months after the loss(range was 6–139 months). The paroxetine and psycho-therapy treated subjects were compared with a group of22 subjects participating in a separate trial of nortripty-line for treatment of bereavement-related depression(Reynolds et al., 1999). Scores on the ICG declined by53%, and HAM-D scores fell by 54% in the paroxetineand psychotherapy group. The authors reported compar-able improvement in the nortriptyline group, but specificmean improvements were not detailed.

144 P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
In a double-blind trial using nortriptyline and sertraline,ten elderly widows and widowers were treated fordepression within 3 months of the loss (Oakley et al.,2002). In this study inwhich the resultswere pooled for thetwo medications, HAM-D scores improved by 57%; griefwas not measured independently (Oakley et al., 2002).
Reynolds et al. (1999) reported on eighty subjectsgrieving the loss of a spouse, child, parent, or sibling, allof whomhad developed depressionwithin a time frame ofbetween 6 months prior to the death and 12 months afterit. Subjects were randomly assigned to 16 weeks of treat-ment with one of the four treatment conditions: nortripty-line plus interpersonal psychotherapy (IPT), nortriptylinealone in a medication clinic, placebo plus interpersonalpsychotherapy, or placebo alone in a medication clinic(Reynolds et al., 1999). Remission (Hamilton Depressionscores of 7 or less for three consecutive weeks) rates forthe treatment conditions were as follows: (1) nortriptylineplus IPT, 69%, (2) nortiptyline, 56%, (3) placebo plus IPT,29%, and (4) placebo, 45%.
In addition to these trials focusing on treatment ofbereavement-related depression, Shear and colleaguespublished the first randomized controlled trial of atargeted complicated grief treatment (CGT) (Shear et al.,2005). To qualify, patients had to meet diagnostic criteriafor CG as defined by a minimum score of 30 on the ICG.Subjects were randomized to receive either CGT or IPTfor approximately 16 weeks. Median time from the losswas 2.1 years (range 0.5 to 36.6) for the CGT group and2.5 years (range 0.5 to 22.3) for the IPT group, aninsignificant difference. Antidepressant medicationswere permitted during the treatment as long as medica-tion was stable for at least 3 months, the dose had beenthe same for at least 6 weeks, and medication manage-ment was transferred to the study doctor. Nearly half ofthe subjects (45%) concurrently took antidepressantmedication during the study.
Both treatments led to improvements in the symp-toms of complicated grief. However, the response ratefor CGT (51%) was greater than that for IPT (28%,p=0.02). The number needed to treat was 4.3. Thosepatients who took antidepressants during therapyshowed slightly better response rates in both conditions.For those randomized to get CGT, 13 of 22 subjects whotook antidepressants, or 59%, responded (95% con-fidence interval, CI, 38–80%) vs. 11 of 26 subjects whodid not take antidepressants, or 42%, responded (95%CI, 23–61%). For those in the IPT condition, 8 of 20subjects who took antidepressants, or 40%, responded(95% CI, 19–61%) vs. 5 of 26 subjects who did not takeantidepressants, or 19%, responded (95% CI, 4–34%).The authors conclude that “…complicated grief is a
specific condition in need of a specific treatment.”(Shear et al., 2005).
In addition, Simon et al. report on a case series of 4women who had a primary diagnosis of complicatedgrief treated in open fashion with escitalopram for10 weeks (Simon et al., 2007). All 4 had a history ofdepression, 2 were currently depressed, and 3 of the 4had PTSD. Mean ratings on the ICG decreased by 76%,and mean scores on the HAM-D fell by 75%.
Overall, ratings of depression in the majority of thesetrials tended to improve more than ratings of griefsymptoms. We hypothesized that escitalopram treatmentof bereavement-related depression would improve symp-toms of depression, anxiety and grief.
2. Methods
Potential subjects were recruited via advertisements(flyers, newspaper ads, and radio ads), with the majorityresponding to the radio ads. Respondents to the adver-tising were screened briefly over the phone, using anInstitutional Review Board-approved prescreen instru-ment, by a research assistant, research psychologist, orresearch physician. Those who remained interested in thestudy and who seemed to meet the study criteria werescheduled for a screening appointment with a studypsychiatrist or psychologist. Prior to any study-relatedprocedures or interviews, subjects were informed aboutthe study and signed an informed consent document thathad been approved by the University of New MexicoHuman Research Review Committee.
Inclusion criteria included (1) capable of understandingand writing the English language and capable of informedconsent, (2) subject age 18 and above, (3) death of aspouse/significant other, parent, sibling or child within the12months preceding the screening interview and onset of amajor depressive episode using DSM-IVTR criteria withina window of 1 month prior to the death and 12 monthsfollowing the death, with or without a previous history ofdepression (patients with a history of depressionmust havehad 3 months free of depression prior to the beginning ofthe current bereavement-related depressive episode toqualify for inclusion in the study), (4) a minimum score of16 on the 17-item Hamilton Depression Rating Scale(HAM-D17, excluding question about sexual function) atboth the screening visit and the second visit, whenmedicationwas started, and (5) stablemedical condition(s).
Exclusion criteria were (1) history of mania or psy-chosis, (2) current substance abuse/dependence or historyof such within the preceding year, (3) current homi-cidal ideation or active suicidal ideation, (4) previousfailure of, intolerance to, or contraindication to using

Table 1Patient demographics
Characteristics
Age in years Mean 45.67
SD 11.91
Range 20 to 76
N %
Sex Female 27 90Male 3 10
Race/Ethnicity White/of Hispanic origin 11 37Native American 9 30White/Not of Hispanic origin 9 30African American 1 3
Marital status Married/significant other 14 47Widowed 5 17Divorced/separated 9 30Single/never married 2 7
Current psychotherapy Yes 3 10No 27 90
Relationship of deceasedto the subject
Child 7 23Parent 13 43Husband/male significant other 5 17Sibling 4 13Female significant other 1 3
Time since loss 1–90 days 8 2791–180 days 7 23181–270 days 8 27271–365 days 7 23
Anticipation of loss Not anticipated 25 83Anticipated 5 17
145P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
escitalopram or citalopram, (5) current treatment withother antidepressants, antipsychotics, sedative hypnotics,or herbal preparations with behavioral effects, (6) evi-dence of cognitive impairment (b25 on the Mini MentalStatus Examination), (7) unstable medical condition(s),(8) clinically significant laboratory abnormalities onscreening laboratory examination, consisting of completeblood count, chemistry panel, and thyroid screening, and(9) women who were pregnant, breast-feeding, or whowere able to become pregnant and unwilling to use anacceptable form of birth control to prevent pregnancyduring the study. Specific psychotherapeutic interven-tions were not provided by the trial, but subjects wereallowed to obtain psychotherapy and support serviceselsewhere. Referrals were provided for those requestingthem.
Diagnoses were determined through a clinical inter-view and completion of the Mini NeuropsychiatricInterview (MINI, version 5.0.0). In addition, the symp-toms of post-traumatic stress disorder were explored indetail using DSM-IVTR criteria. The study cliniciancompleted the HAM-D17 (with the question about sexuallibido deleted to be sensitive to the potential distress ofwidows and widowers), Montgomery–Asberg Depres-sion Rating Scale (MADRS), Hamilton Anxiety RatingScale (HAM-A), CGI for severity of illness of depression(CGI-S-D), and CGI for severity of illness of grief (CGI-S-G) at each visit. In addition, the study cliniciancompleted the CGI Scale for improvement of depression(CGI-I-D) andCGI-I for grief (CGI-I-G) at each visit afterthe screening visit (visit 1). Subjects completed the TexasRevised Inventory of Grief (TRIG) and the Inventory ofComplicated Grief (ICG) at each visit.
In accord with common clinical practice, we classifiedpatients as having uncomplicated grief or complicatedgrief. We utilized the 18-item ICG scale which omits thefinal question of the19-item scale, which reads: “I feellonely a great deal of the time since s/he died… [.]”Weusedthe 18-item scale throughout, sowe caution againstmakingcomparisons to others' work which may report scores onthe versions of the scale with different numbers of items.Using the ICG, the diagnosis of complicated grief requiresthat (1) more than 6 months have passed since the loss and(2) a score of greater than 25 (inmost reports) using the 19-item scale. For this report, we utilized a cut-off score ofgreater than or equal to 25 for those subjects who weregreater than 6 months from their loss at baseline (visit 2).
Following screening procedures at visit 1 and receiptof the laboratory findings, eligible subjects were invitedback for a second visit (visit 2) to commence medicationtreatment. Thirty subjects were started on escitalopram10 mg/day. Visits 3 and 4 were scheduled at weekly
intervals. Visit 5 occurred 2 weeks later; thereafter visitswere scheduled at monthly intervals for 2 months (visits6 and 7). The total treatment time was 12 weeks, and thedosing regimen allowed the medication to be increasedto 20 mg/day at or after visit 4 (week 4), which was2 weeks after medication initiation. Dosing adjustmentswere made taking individual response, side effects, andpatient preferences into consideration. Information aboutadverse events and concurrent medications were col-lected systematically at each visit. Following completionof the trial, we asked the subjects if they wanted tocontinue treatment with escitalopram and providedfurther treatment until a link with a primary carephysician or psychiatrist could be made. For those whodid not want to continue medication, we recommended astrategy for discontinuing the medication and offered afollow-up visit. We also provided referrals for psy-chotherapy and support groups for those who did notwant to consider further medication treatment.
Most outcome measures were analyzed using analysisof variance for repeated measures as implemented in theNumber Cruncher Statistical System (Hintz, 2004). Thefactor within subjects was time (baseline and final
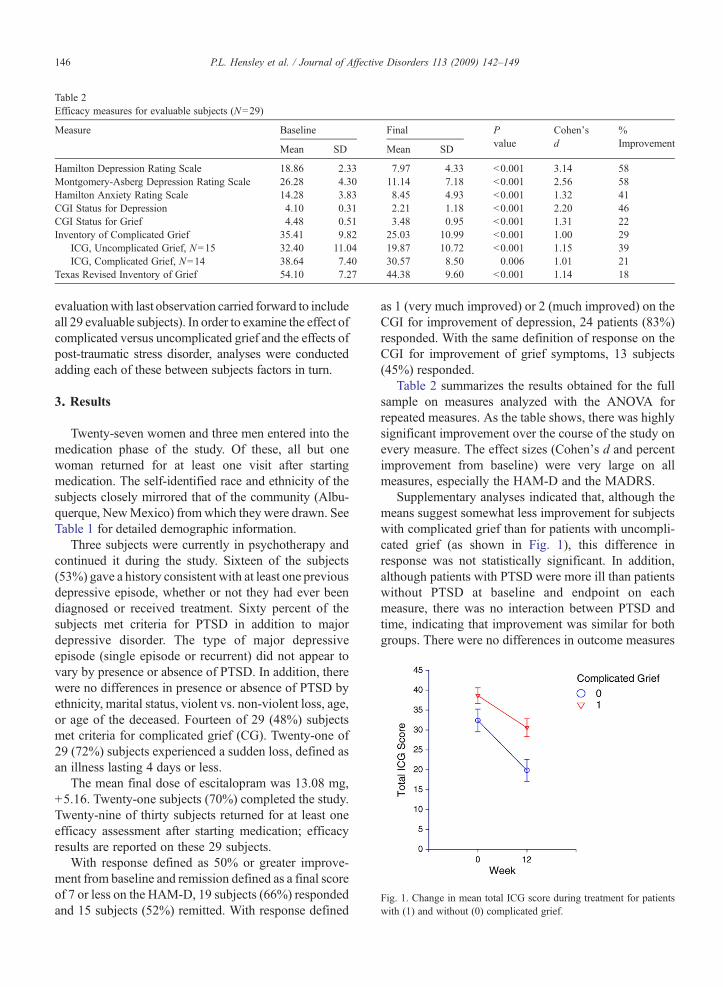
Table 2Efficacy measures for evaluable subjects (N=29)
Measure Baseline Final Pvalue
Cohen'sd
%Improvement
Mean SD Mean SD
Hamilton Depression Rating Scale 18.86 2.33 7.97 4.33 b0.001 3.14 58Montgomery-Asberg Depression Rating Scale 26.28 4.30 11.14 7.18 b0.001 2.56 58Hamilton Anxiety Rating Scale 14.28 3.83 8.45 4.93 b0.001 1.32 41CGI Status for Depression 4.10 0.31 2.21 1.18 b0.001 2.20 46CGI Status for Grief 4.48 0.51 3.48 0.95 b0.001 1.31 22Inventory of Complicated Grief 35.41 9.82 25.03 10.99 b0.001 1.00 29
ICG, Uncomplicated Grief, N=15 32.40 11.04 19.87 10.72 b0.001 1.15 39ICG, Complicated Grief, N=14 38.64 7.40 30.57 8.50 0.006 1.01 21
Texas Revised Inventory of Grief 54.10 7.27 44.38 9.60 b0.001 1.14 18
Fig. 1. Change in mean total ICG score during treatment for patientswith (1) and without (0) complicated grief.
146 P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
evaluationwith last observation carried forward to includeall 29 evaluable subjects). In order to examine the effect ofcomplicated versus uncomplicated grief and the effects ofpost-traumatic stress disorder, analyses were conductedadding each of these between subjects factors in turn.
3. Results
Twenty-seven women and three men entered into themedication phase of the study. Of these, all but onewoman returned for at least one visit after startingmedication. The self-identified race and ethnicity of thesubjects closely mirrored that of the community (Albu-querque, NewMexico) fromwhich they were drawn. SeeTable 1 for detailed demographic information.
Three subjects were currently in psychotherapy andcontinued it during the study. Sixteen of the subjects(53%) gave a history consistent with at least one previousdepressive episode, whether or not they had ever beendiagnosed or received treatment. Sixty percent of thesubjects met criteria for PTSD in addition to majordepressive disorder. The type of major depressiveepisode (single episode or recurrent) did not appear tovary by presence or absence of PTSD. In addition, therewere no differences in presence or absence of PTSD byethnicity, marital status, violent vs. non-violent loss, age,or age of the deceased. Fourteen of 29 (48%) subjectsmet criteria for complicated grief (CG). Twenty-one of29 (72%) subjects experienced a sudden loss, defined asan illness lasting 4 days or less.
The mean final dose of escitalopram was 13.08 mg,+5.16. Twenty-one subjects (70%) completed the study.Twenty-nine of thirty subjects returned for at least oneefficacy assessment after starting medication; efficacyresults are reported on these 29 subjects.
With response defined as 50% or greater improve-ment from baseline and remission defined as a final scoreof 7 or less on the HAM-D, 19 subjects (66%) respondedand 15 subjects (52%) remitted. With response defined
as 1 (very much improved) or 2 (much improved) on theCGI for improvement of depression, 24 patients (83%)responded. With the same definition of response on theCGI for improvement of grief symptoms, 13 subjects(45%) responded.
Table 2 summarizes the results obtained for the fullsample on measures analyzed with the ANOVA forrepeated measures. As the table shows, there was highlysignificant improvement over the course of the study onevery measure. The effect sizes (Cohen's d and percentimprovement from baseline) were very large on allmeasures, especially the HAM-D and the MADRS.
Supplementary analyses indicated that, although themeans suggest somewhat less improvement for subjectswith complicated grief than for patients with uncompli-cated grief (as shown in Fig. 1), this difference inresponse was not statistically significant. In addition,although patients with PTSD were more ill than patientswithout PTSD at baseline and endpoint on eachmeasure, there was no interaction between PTSD andtime, indicating that improvement was similar for bothgroups. There were no differences in outcome measures

Table 3Adverse events reported by 2 or more patients (N=30)
Adverse event N %
Headache 10 33Somnolence 10 33Dry mouth 9 30Nausea 7 23Menstrual irregularity ⁎ 3 11Diarrhea 3 10Insomnia 3 10Increased muscle tension 2 7Tremulousness 2 7Increased sweating 2 7Palpitations 2 7
⁎ Percentage based on female population only.
147P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
for the group who experienced a sudden loss versusthose who experienced a non-sudden loss.
Escitalopram was generally well tolerated. Threesubjects (two women and a man) discontinued due toadverse events (headaches in one; nausea, headaches,lightheadedness, and itching in the second; and nausea,increased anxiety, somnolence, and headache in thethird); all occurred early in treatment. See Table 3 foradverse events.
4. Discussion
Treatment with escitalopram led to significantimprovement in symptoms of depression, anxiety, andgrief in this 12-week study of bereavement-relateddepression. Overall, 83% of the subjects were responderson the CGI scale. On the HAM-D, 66% were respondersand 52%were remitters. Escitalopram was well toleratedwith few discontinuations due to side effects.
These data add to a growing body of literature on theuse of antidepressants to treat bereavement-relateddepression and complicated grief (Jacobs et al., 1987;Pasternak et al., 1991; Zygmont et al., 1998; Zisooket al., 2001; Oakley et al., 2002; Reynolds et al., 1999).The majority of the previous studies have restricted entryto individuals grieving the loss of a spouse (Jacobs et al.,1987; Pasternak et al., 1991; Zisook et al., 2001; Oakleyet al., 2002), although both the Zygmont et al. (1998)study and the Reynolds et al. (1999) study includedindividuals grieving other losses of close relatives. Oursample also included subjects suffering bereavementfrom a variety of losses, which we believe makes ourfindings more generalizable. We, as physicians, shouldexpand our appreciation of the potential for multipletypes of bereavement to usher in chronic depression. Ourethnically and racially diverse population in the studyalso aids in generalizability of findings.
The rate of remission of depression as defined byHAM-D b7 was 51.7%, representing 15 of the 29evaluable subjects. This rate of remission is similar torates seen in other open-label trials of non-bereavementrelated depression. From this report, it's difficult to drawconclusions on the optimal length of time for treatingbereavement-related depression. Although ours was arelatively short trial, we saw a notable improvement insymptoms of depression, anxiety, and grief.
The rate of improvement in grief symptoms in thosesubjects with uncomplicated grief exceeded the improve-ment rate of subjects with complicated grief. However,repeated measures ANOVA did not show significantdifferences between the two groups.Whereasmost studiesthat report the results of treatment for complicated griefinclude only subjectswithCG, our study subjects includedapproximately equal numbers of subjectswith andwithoutcomplicated grief since we were selecting patients withmajor depression regardless of CG status. Other than theZygmont et al. (1998) report (which combined psy-chotherapy and pharmacotherapy) and the case series ofSimon et al. (2007), there are no published studies of thepharmacologic treatment of CG.
Nearly half of the patients in the Shear et al. (2005)report (comparing two types of therapy, CGT and IPT)were concurrently taking antidepressant medication,but treatment was neither randomized nor controlled.Many of the studies of pharmacotherapy for bereave-ment-related depression as detailed in the introductionreported improvement in grief symptoms, but nonereported how many subjects met criteria for CG, andtherefore none were able to compare the responses ofthose with and without CG. In addition, the subjects inour report who met criteria for CG may be differentfrom subjects in the Shear report in that all of ourpatients were seen within the first year since the loss,while the median time from the loss in the Shear reportwas 2.1 to 2.5 years.
Even though patients with PTSD started outslightly worse than those without PTSD, those withPTSD improved to a similar degree to those withoutPTSD. No other studies of the treatment of bereave-ment-related depression reported the results ofpatients with PTSD co-morbid with depression. Ourresults indicate that PTSD should not be considereda contraindication to treating bereavement-relateddepression with escitalopram.
The open-label nature of the studymakes comparisonsto trials utilizing placebo controls difficult. The vastmajority of the literature in this area has not been placebo-controlled, and our results compare favorably to thoseseen in previous reports.

148 P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
As in past reports of treatment of bereavement-related depression, the response of depressive symptomsin this trial was greater than that for grief symptoms.However, the improvement in grief seen here is en-couraging. Because the individuals in our sample wereseen quite recently after their losses, we would anti-cipate grief symptoms untreated to persist in this timeframe. Therefore, a 45% response rate on the CGI forgrief is clinically significant.
There are several limitations of the current report.First, the lack of a control group likely overestimates theresponse rate to the treatment. Second, psychotherapyduring the study period was not controlled. However,only three subjects were being treated with psychother-apy during the study period, and all continuedthroughout. Third, the medication treatment was shortat only twelve weeks. The question of how long thiscondition needs to be treated remains unanswered.Fourth, we utilized the 18-item ICG, so comparisons toother reports should be made cautiously. Fifth, all thesubjects in this trial who had complicated grief were alsoclinically depressed; therefore, the results may or maynot apply to individuals with complicated grief butwithout major depression. Sixth, women outnumberedmen in the trial by 9:1 even though (1) the trial was opento both men and women equally and (2) men andwomen have similar rates of bereavement-relateddepression. Therefore, our results apply primarily towomen.
In summary, escitalopram appears to be an effective,well-tolerated treatment for bereavement-related depres-sion. Significant improvement in symptoms of depres-sion, anxiety, and grief (to a slightly lesser degree) canbe expected with treatment. There were no significantdifferences in the response of patients (1) with andwithout complicated grief and (2) with and with-out PTSD. Controlled trials and longer-term trialsare needed in this field to better define clinicalrecommendations.
Role of funding source
Study funding and medication were provided by the ForestResearch Institute, Jersey City, NJ. Forest Research Institute had nofurther role in study design; in the collection, analysis, andinterpretation of data; in the writing of the report; and in the decisionwhere to submit the paper for publication.
Conflict of interestDr. Hensley has served on the speakers' bureau for and received
honoraria from Forest Pharmaceuticals, Wyeth, and Takeda.Drs. Slonimski and Uhlenhuth have no disclosures to report. Dr. Claytonhas served on the speakers' bureau for and received honoraria fromForest Pharmaceuticals. Ms. Linda Sparks, who was our research
coordinator and whose help we are acknowledging, received partialsalary support from this grant while she was employed by the Universityof New Mexico.
Acknowledgement
The authors wish to acknowledge the assistance ofMs. Linda Sparks in study management and recruitment.
References
American Psychiatric Association, 2000. Diagnostic and StatisticalManual of Mental Disorders, 4th ed. American PsychiatricAssociation, Washington DC. text rev.
Clayton, P.J., 1990. Bereavement and depression. J. Clin. Psychiatry51 (7), 34–40 (Suppl).
Clayton, P.J., Darvish, H.S., 1979. Course of depressive symptomsfollowing the stress of bereavement. In: Barrett, J., Rose, R.M.,Klerman, G.L. (Eds.), Stress and Mental Disorder. Raven Press,New York, pp. 121–136.
Clayton, P., Desmarais, L., Winokur, G., 1968. A study of normalbereavement. Am. J. Psychiatry 125 (2), 168–178.
Clayton, P.J., Halikes, J.A., Maurice, W.L., 1971. The bereavement ofthe widowed. Diseases of the Nervous System 32 (9), 597–604.
Faschingbauer, J.R., 1981. Texas Revised Inventory of Grief Manual.Honeycomb Publishing, Houston, Texas.
Hintz, J., 2004. NCSS and PASS. Number Cruncher StatisticalSystems. Kaysville, Utah. www.NCSS.com.
Jacobs, S.C., Nelson, J.C., Zisook, S., 1987. Treating depressions ofbereavement with antidepressants: a pilot study. Psychiatr. Clin.North Am. 10, 501–510.
Melhem, N.M., Rosales, C., Karageorge, J., Reynolds III, C.R., Frank,E., Shear, M.K., 2001. Comorbidity of axis I disorders in patientswith traumatic grief. J. Clin. Psychiatry 62 (11), 884–887.
Oakley, F., Khin, N.A., Parks, R., Bauer, L., Sunderland, T., 2002.Improvements in activities of daily living in elderly followingtreatment for post-bereavement depression. Acta Psychiatr. Scand.105, 231–234.
Pasternak, R.E., Reynolds III, C.F., Schlernitzauer, M., Hoch, C.C.,Buysse, D.J., Houck, P.R., Perel, J.M., 1991. Acute open-label trialof nortriptyline therapy of bereavement-related depression in latelife. J. Clin. Psychiatry 52 (7), 307–310.
Reynolds III, C.F., Miller, M.D., Pasternak, R.E., Frank, E., Perel, J.M.,Cornes, C., Houck, P.R., Mazumdar, S., Dew, M.A., Kupfer, D.J.,1999. Treatment of bereavement-related major depressive episodesin later life: a controlled study of acute and continuation treatmentwith nortriptyline and interpersonal psychotherapy. Am. J.Psychiatry 156 (2), 202–208.
Shear, K., Frank, E., Houck, P.R., Reynolds III, C.F., 2005. Treatment ofcomplicated grief: a randomized controlled trial. JAMA 293 (21),2601–2608.
Simon, N.M., Thompson, E.T., Pollack, M.H., Shear, M.K., 2007.Complicated grief: a case series using escitalopram. Am. J.Psychiatry 164 (11), 1760–1761.
Zisook, S., Shuchter, S.R., 1991. Depression through the first year afterthe death of a spouse. Am. J. Psychiatry 148 (10), 1346–1352.
Zisook, S., Shuchter, S.R., Sledge, P.A., 1994a. Diagnostic andtreatment considerations in depression associated with late-life bereavement. In: Schneider, L.S., Reynolds, C.F., Lebowitz,B.D., Friedhoff, A.J. (Eds.), Diagnostic and Treatment of

149P.L. Hensley et al. / Journal of Affective Disorders 113 (2009) 142–149
Depression in Late Life. American Psychiatric Press, Washing-ton, DC, pp. 419–435.
Zisook, S., Shuchter, S.R., Sledge, P.A., Paulus, M., Judd, L.L., 1994b.The spectrum of depressive phenomena after spousal bereavement.J. Clin. Psychiatry 55 (4), 29–36 (Suppl).
Zisook, S., Shuchter, S.R., Pedrelli, P., Sable, J., Deaciuc, S.C., 2001.Bupropion sustained release for bereavement: results of an opentrial. J. Clin. Psychiatry 62 (4), 227–230.
Zygmont, M., Prigerson, H.G., Houck, P.R., Miller, M.D., Shear, M.K.,Jacobs, S., Reynolds, C.F., 1998. A post hoc comparison ofparoxetine and nortriptyline for symptoms of traumatic grief. J. Clin.Psychiatry 59 (5), 241–245.