ereferral: implementing change to improve specialty access margot kushel, md associate professor of...
TRANSCRIPT
eReferral: implementing change to improve specialty accessMargot Kushel, MDAssociate Professor of Medicine in Residence
What is eReferral?
Electronic referral system for specialty care at San Francisco General Hospital
SFGH: public hospital of city/county of SF Operated by SFDPH Has longstanding affiliation with UCSF All physicians are UCSF faculty members, paid by UCSF via
affiliation agreement with CCSF Serves as cornerstone of Community Health Network Network of SFDPH funded community-based primary care
clinics, specialty hospital (SFGH) and LHH

Who receives specialty care at SFGH? under and uninsured patients
working poor socially chaotic (homeless, substance abuse) ethnic and racially diverse limited english proficiency chaotic social situations
Patients referred from CHN clinics, hospital based primary care clinics, community consortium clinics (FQHC)

Who provides specialty care at SFGH? UCSF faculty specialists, fellows,
residents Many clinicians who see patients for short
periods of times (fellows, residents) or for few clinic sessions a week
How are physicians reimbursed?
Salaried, paid by UCSF Clinical time is partially covered by
CCSF/UCSF affiliation agreement Under funds clinical time
A lot of time is “donated”

What were the problems?
Supply/demand mismatch Limited physician time to see large numbers of patients Long wait times
Poor communication Hand written referrals, free form
Hard to read, unclear question, got lost Triage by “hassle”
PCPs could page fellows to beg for earlier appointments Took everyone’s time Relied on personal connections which weren’t evenly distributed No rationale way to determine appointments
Many patients “overbooked” led to chaotic specialty clinic sessions Little communication back to PCP
No letters, chart notes handwritten, often lost

These data led to a pilot solution… Hal Yee MD PhD joined UCSF in 2005 to be
division chief of GI Recognized supply/demand mismatch
GI had wait time for new appointments of 11.5 months Did not have option to increase supply Recognized inefficiencies in system
Initiated GI eConsult with input from: IT, primary care providers, GI, and risk management
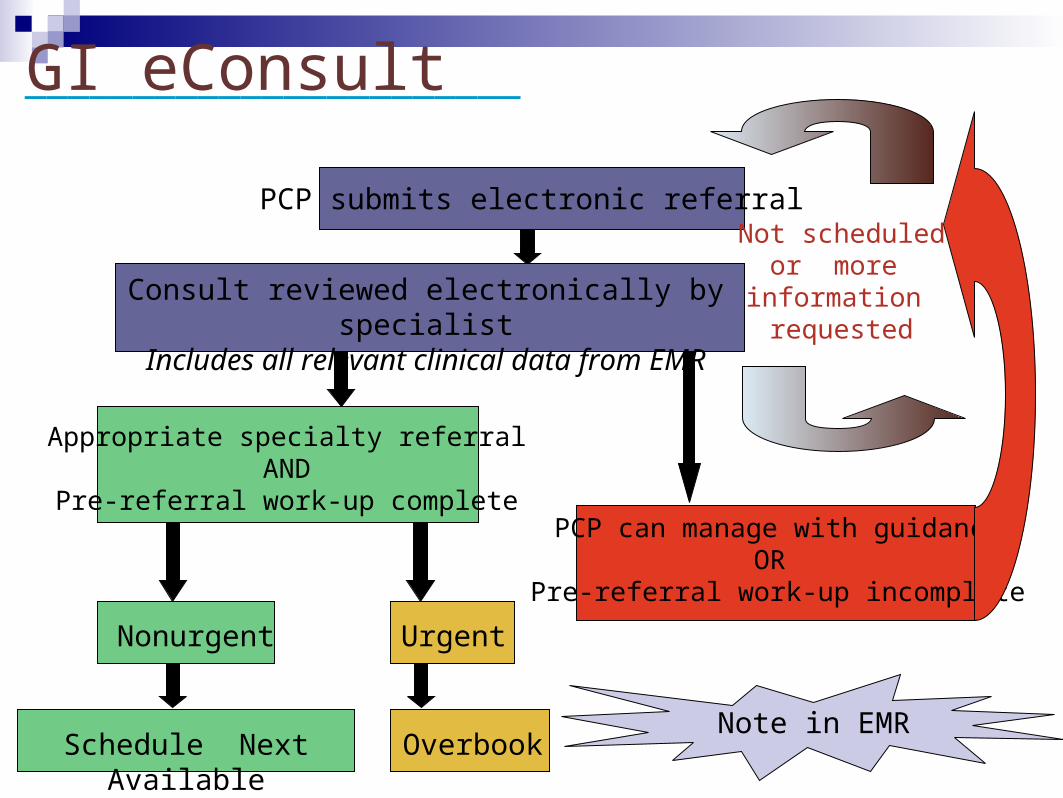
PCP submits electronic referral
Consult reviewed electronically by specialistIncludes all relevant clinical data from EMR
Appropriate specialty referralAND
Pre-referral work-up completePCP can manage with guidance
OR Pre-referral work-up incomplete
Schedule Next Available Overbook
Nonurgent Urgent
Not scheduledor more
information requested
Note in EMR
GI eConsult_______________________

GI eConsult: results____________________________
Next Available New Patient Appointment in GI (eReferral implemented 07/01/2005)
0
50
100
150
200
250
300
350
400
7/1/
2005
8/1/
2005
9/1/
2005
10/1
/200
5
11/1
/200
5
12/1
/200
5
1/1/
2006
2/1/
2006
3/1/
2006
4/1/
2006
5/1/
2006
6/1/
2006
7/1/
2006
8/1/
2006
9/1/
2006
10/1
/200
6
11/1
/200
6
12/1
/200
6
1/1/
2007
2/1/
2007
Date of Review
Nu
mb
er o
f D
ays
1st AvailAppt
2nd AvailAppt
3rd AvailAppt
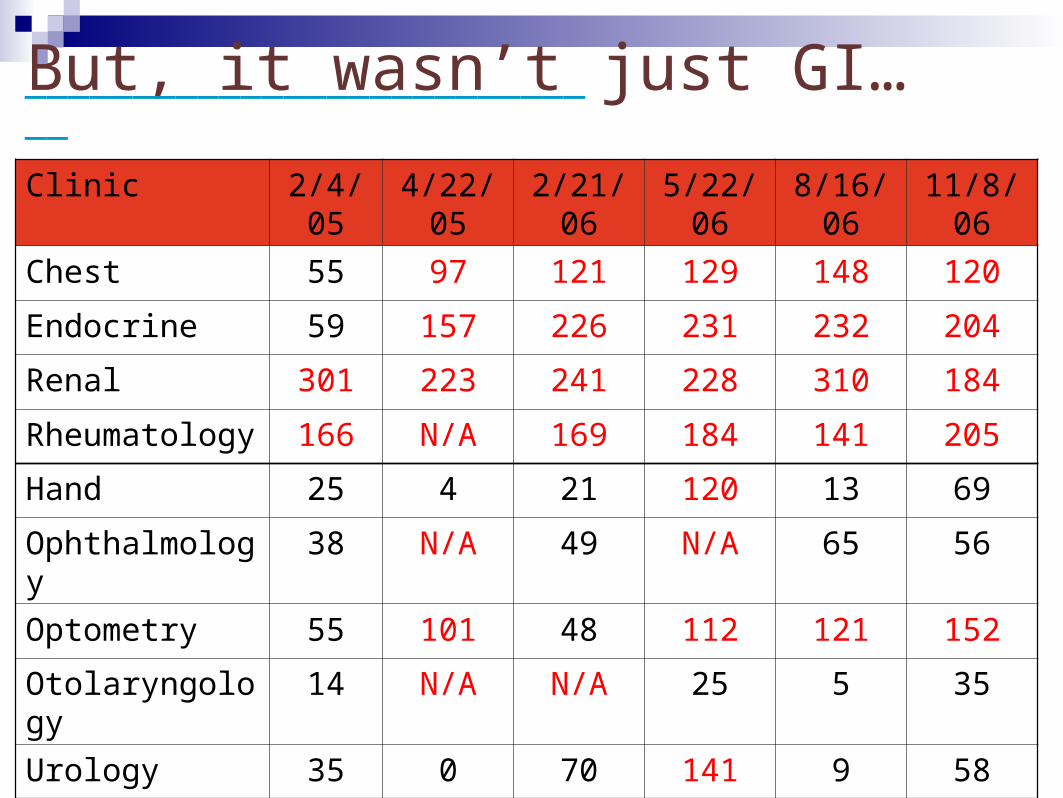
But, it wasn’t just GI…____________________________
Clinic 2/4/05 4/22/05 2/21/06 5/22/06 8/16/06 11/8/06
Chest 55 97 121 129 148 120
Endocrine 59 157 226 231 232 204
Renal 301 223 241 228 310 184
Rheumatology 166 N/A 169 184 141 205
Hand 25 4 21 120 13 69
Ophthalmology 38 N/A 49 N/A 65 56
Optometry 55 101 48 112 121 152
Otolaryngology 14 N/A N/A 25 5 35
Urology 35 0 70 141 9 58

SFHP funds eReferral spread
three separate grants
• 4 medicine clinics
• 8 surgical clinics
• outpatient MRI, CT and U/S
project goals
• to decrease wait times
• to improve communication between specialists and primary care providers
____________________________

implementation schedule____________________________
JANCardiology Chest
Sleep Studies
FEB MARCH APRIL
MAYEndocrinology Rheumatology
JUNE JULYNeurosurgery
Orthopedics 5M Breast Clinic
AUG
SEPT OCT NOVPodiatry Urology
DEC
JANNeurology
Renal
FEB MARCH APRILPlastics
MAYENT
Hematology
JUNE JULY AUGUST
2007
2008
MedicineSurgery
RadiologyNot Grant Funded
Next: MRI, Diabetes, Obstetrics-Gynecology
eReferral evaluation
Made argument to the funders that we needed to fund evaluation
Decided to use evaluation as both evaluation and as feedback
As lead evaluator, worked alongside implementation team, attended all team meetings, provided input at all stages

What metrics?
Original pilot data looked at wait times Thinking about broader goals, hoped to
impact:Wait timesQuality of referralsEfficiency for both specialists and PCPsAcceptability
eReferral evaluation activities
Access and process measures eReferral database Time surveys of reviewers
Primary care provider survey (Yeuen Kim) Electronic questionnaire to all primary care providers (SFGH-based, CHN,
consortium clinic) Specialty Survey
Brief questionnaire Unit of analysis: new patient specialty visit (yes/no eReferral) 8 clinics; pre and post eReferral
Cost analyses (with RAND) Time costs Multiple interviews with key informants
Upcoming: (renal clinic focus) Proportion of new RRT patients whose first visit was 6 months prior to RRT

eReferral evaluation:eReferral database
Access indicatorsWait times
Process indicatorsProportion overbooked, regularly scheduled, not
initially scheduledProportion never scheduled
Payer mix/show ratesNo-show ratesPayer mix

Routinely scheduled appointments: wait times
Wait times for new appointments (routine) Feb 07- Feb 08: Medicine Clinics
0
20
40
60
80
100
120
140
160
180
Feb Apr Jun Aug Oct Dec Feb
Month
# o
f d
ays
(ave
rag
e)
GI
Cards
Pulm
Endo (5/14/07 startdate)
Rheum (5/14/07 startdate)

Proportion of appointments never scheduled
% of eReferrals Never Scheduled: Medicine Clinics (for eReferrals submitted January-June 07)
0
5
10
15
20
25
30
35
40
45
Cards Pulm Endo GI Rheum Total
Clinic
% o
f A
pp
oin
tme
nts
Ne
ve
r S
ch
ed
ule
d

Proportion overbooked versus routinely scheduled (among those scheduled)
Clinic GI Cardiology Pulmonary Endo Rheum
Number of scheduled appointments 1810 865 379 204 324
Routine 1390 (77%) 581(67%) 297(78%) 114 (56%) 116 (36%)
Overbooked 420 (23%) 284 (33%) 82(22%) 88 (44%) 208 (64%)

Primary Care Survey
Electronic questionnaire to all PCPs in SFGH based, CHN and consortium primary care clinics that see adults
Asked about time spent doing eReferrals compared to paper methods, guidance of work-up, wait times, whether they thought it improved care overall
Gave room for free text as well Total n=368 Had 81% response rate without incentives Study n=298
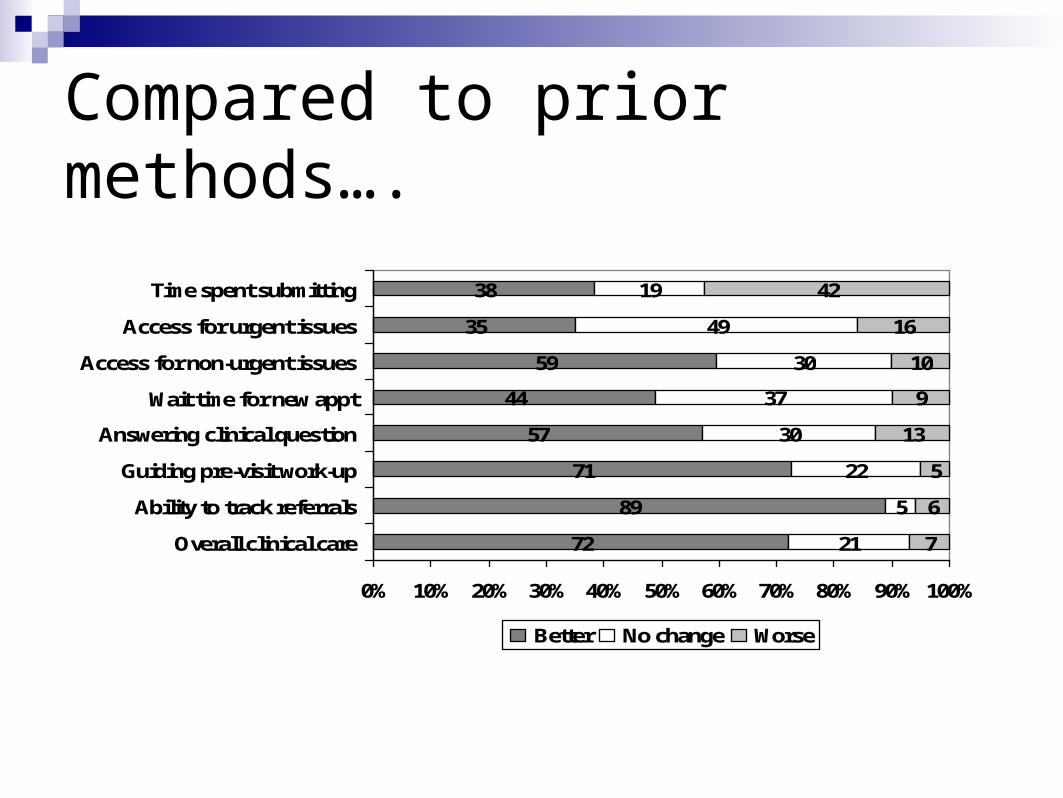
Compared to prior methods….
72
89
71
57
44
59
35
38
21
5
22
30
37
30
49
19
7
6
5
13
9
10
42
16
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Overall clinical care
Ability to track referrals
Guiding pre-visit work-up
Answering clinical question
Wait time for new appt
Access for non-urgent issues
Access for urgent issues
Time spent submitting
Better No change Worse

In multivariate analysis…
. Providers from non-county-funded clinics (AOR 0.40, 95% CI 0.14-0.79) and those who spent ≥6 minutes submitting an electronic referral (AOR 0.33, 95%CI 0.18-0.61) were significantly less likely than other participants to report that electronic referrals had improved clinical care.
Kim et al. Under review

Specialty Survey
We created short (<2 minute) questionnaire to attach to patient charts in selected specialty clinics before and after eReferral
Asked first specialist to see patient to fill it out Asked about clarity of question, appropriateness of
visit, need for follow-up, could follow-up have been averted
Wanted to get specialists sense of eReferral: was this improving their ability to care for patients

Specialty Survey: n=450ish
Proportion of respondents for whom it was somewhat/very difficult to identify the
consultation/clinical question
0
5
10
15
20
25
30
35
40
45
Medicine Surgical
% p
erce
nta
ge
of
resp
on
ses
Yes eReferral
No eReferral

Specialty Clinic Survey
Proportion of follow-up visit(s) that could have been avoided if WORK-UP HAD BEEN MORE COMPLETE
prior to visit (*Question asked only for patients for whom a follow-up appointment is scheduled)
0
5
10
15
20
25
30
35
40
45
50
Medicine Surgical
% o
f re
sp
on
ses
Yes eReferral
No eReferral

What role has evaluation played? Help define what metrics we should use to
measure success Provide mid-course corrections Provide data for business plan/funders to make
case for spread of eReferral Provide data to “nudge” constituents and
powers that be i.e. issue of dictating notes
Overall, eReferral thought to be a success In clinics with most resource limitation, reduced
wait times Both PCPs and specialists believed it improved
communication Extra burden on PCP generally well tolerated Acceptance in part dependent on IT issues
Further from SFGH (IT wise), the less well accepted We have not evaluated patient outcomes and
acceptance
What were the factors that led to success? Motivated, coordinated effort
PCPs, specialists, IT, administration, funders Interest aligned with our payment system
In system that is “capitated,” everyone agrees on wanting to avoid “avoidable” appointments
Interactive evaluationAble to make mid-course corrections

What were factors that led to success? Effective team leadership, met regularly Used data to make mid course
corrections and relayed results back to stakeholders frequently
An idea whose time had come, which was well implemented…
