eradicating blinding trachoma: what is working?
TRANSCRIPT
Saudi Journal of Ophthalmology (2010) 24, 15–21
King Saud University
Saudi Journal of Ophthalmology
www.ksu.edu.sawww.sciencedirect.com
REVIEW ARTICLE
Eradicating blinding trachoma: What is working?
Imtiaz A. Chaudhry, MD, PhD, FACS *
Oculoplastic and Orbit Division, King Khaled Eye Specialist Hospital, P.O. Box 7191, Riyadh 11462, Saudi Arabia
Received 12 December 2009; accepted 12 December 2009Available online 21 December 2009
*
E-
13
re
do
KEYWORDS
Trachoma;
Chlamydia trachomatis;
Visual loss;
Adnexal complications;
Evaluation;
Treatment
Tel.: +966 1 4821234x3771;mail address: orbitdr@yahoo
19-4534 ª 2009 King Saud
view under responsibility of
i:10.1016/j.sjopt.2009.12.008
Production and h
fax: +96.com
Univers
King Sau
osting by E
Abstract Trachoma remains the leading cause of preventable corneal blindness in developing
countries. The disease is contracted in early childhood by repeated infection of the ocular surface
by C. trachomatis. Initial clinical manifestation is a follicular conjunctivitis which if not treated
on timely basis, may lead to conjunctival and eyelid scarring that may eventually result in corneal
scarring and loss of vision. Over the past two decades, a remarkable reduction in the prevalence of
active trachoma has occurred due to the World Health Organization’s (WHOs) program GET 2020
for the elimination of trachoma with adoption of the SAFE strategy incorporating Surgery, Anti-
biotic treatment, Facial cleanliness and Environmental hygiene. However, patients who already had
infection at young age may present with adnexal-related complications of trachomatous scarring
that may cause corneal scarring and visual loss. These patients may present with evidence of trichi-
asis/entropion as well as eyelid retraction. Lacrimal complications may include nasolacrimal-duct
obstruction, dacryocystitis and canaliculitis requiring intervention. In addition to the increased risk
for corneal scarring, trichiasis/entropion may further increase the risks for microbial keratitis in
patients who may have unrecognized dacryocystitis and canaliculitis. Female patients may have
more trachomtous-related complications and may present at an early age. Available evidence indi-
cates that SAFE strategy may be effective and on the right track towards achieving GET 2020 goal
for the eradication of trachoma.ª 2009 King Saud University. All rights reserved.
6 1 4821908.
ity. All rights reserved. Peer-
d University.
lsevier

16 I.A. Chaudhry
Contents
1. Scope of the problem. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162. Risk factors for C. trachomatis infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3. Mechanism of scarring. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174. Mechanism of vision loss in trachoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185. Mechanism of nasolacrimal system damage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 196. Treatment: medical and surgical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
1. Scope of the problem
Trachoma is the most common infectious cause of blindnessworldwide. It afflicts some of the poorest regions of the globe,
predominantly in Africa and Asia (Al-Rifai, 1988; Solomonand Mabey, 2007). The disease is initiated in early childhoodby repeated infection of the ocular surface byChlamydiatracho-
matis, an intracellular gram-negative bacterium (Burton, 2007).During acute infection, the disease may remain asymptomaticbut some patients may complain of eye redness, irritation and
discharge (Burton, 2007). The principal initial clinical manifes-tation is a follicular conjunctivitis. A population based surveyof trachoma and blindness from a rural Nile Delta hamlet, atrachoma hyper-endemic region found that active trachoma
was common among pre-school children (Courtright et al.,1989). Among inhabitants 25 years or older, 90% had substan-tial conjunctival scarring. Severe conjunctival scarring was
common among women (84%) than men (58%), and three-quarters of older women had trichiasis/entropion comparedwith 57% of older men. Blindness was associated with old
age; 17% of residents aged 50 and over had significant blind-ness (Courtright et al., 1989). Trachoma is one of the maincause of preventable blindness in Saudi Arabia (Tabbara and
Ross-Degnan, 1986; Tabbara and Al-Omar, 1997; Tabbara,2001). Early surveys during 1955–70 in Eastern Provincerevealed prevalence rate of trachoma as 100% in Al Hasa,98% in Qatif Oasis and 93% in Qatif town dwellers (Murray
et al., 1960; Nichols et al., 1966, 1967, 1969; McComb and Nic-hols, 1969, 1970; Bobb andNichols, 1969; Bell et al., 1970). Pre-liminary study by Ministry of Health, Eastern Province in 1986
revealed 3.74% of the population had blindness among them10.1% due to trachoma (Tabbara and Al-Omar, 1997). In1986, Ministry of Health established Regional Prevention of
Blindness and Ophthalmic Medical Education Committee,Eastern Province with six sub-divisions in Al Hasa, Qatif,Dammam, Al Khobar/Dhahran, Jubail and Hafr Al Batin.The whole health care was divided in primary, secondary and
tertiary level in 1987 and incorporated primary eye health carewith primary health care. The Trachoma Center was started inAl Hasa in 1987 and a mass trachoma eradication program was
launched in 1988. Improvement in socio-economic status andstructured health care system over the following 10 years leadsto public awareness, prevention and treatment of bulk of active
trachoma in this region (Tabbara and Al-Omar, 1997). Morerecently, provision of comprehensive eye care by completingpreliminary tertiary level care Eye Hospital in Dhahran has fur-
ther reduced the incidence of active trachoma below 0.5%. In1984, evidence of trachoma (active and inactive) was foundamong 22.2% of the Saudi population; 6.2% of them had evi-
dence of active trachoma. In addition, 17.4% had conjunctivalscarring as a result of old trachoma, and 1.5% had entropion ortrichiasis. In 1994, clinical evidence of trachoma (active and
inactive) was found among 10.7% of the Saudi populationwhile 2.6% had active trachoma. Conjunctival scarring as a re-sult of healed trachoma was seen in 8.1% and 0.2% had trichi-
asis and entropion (Tabbara and Al-Omar, 1997).
2. Risk factors for C. trachomatis infection
Trachoma prevalence is disproportionately high among wo-men and children in poor rural communities. In particular, risk
factors include lack of facial cleanliness, poor access to watersupplies, lack of latrines, and a large number of flies. House-hold overcrowding, and the lack of clean water are factors that
predispose to the transmission of the disease (Barenfanger,1975). In one of the study that compared trends in the preva-lence of active inflammatory trachoma among children under10 years of age in Marakissa (a small rural village in the Gam-
bia) between the results of eye examinations conducted in1959, 1987, and 1996, the prevalence of active trachoma infec-tion dropped from 65.7 cases per 100 in 1959 to 2.4 per 100 in
1996 (Dolin et al., 1997). Declines were also recorded amongchildren 10–19 years old (from 52.5 to 1.4/100) and amongthose 20 years and older (from 36.7 to 0 cases/100). This
dramatic fall, which occurred without any specific trachomacontrol programs in the area, was attributed to bothimprovements in socio-economic standards and the training
of village health workers and traditional birth attendants ineye care (Dolin et al., 1997). Another study of trachoma con-trol in Burma over a 30-years period also found a remarkabledecline in trachomatous blindness (Evans et al., 1996). An epi-
demiological study of trachoma in Central Tanzania, foundthat active inflammatory disease peaked in pre-school children,with 60% showing signs of trachoma (West et al., 1991). Evi-
dence of past infection, scarring, trichiasis, and corneal opac-ity, rose with age. In this population, 8% of those over age55 had trichiasis/entropion. Females of all ages had more tra-
choma than males, with a fourfold increased risk of trichiasisobserved in females. Women who were taking care of childrenappeared to have more active disease than non-caretakers. Evi-dence of clustering of trachoma by village, and within village,
by neighbor-hood was also found. Clustering persisted evenafter accounting for differences in distance to water, localreligion, and proportion of children with unclean faces.
These findings may have important implications for a tra-choma control strategy (West et al., 1991). Trachoma remainsa public health issue in Central Australia. Landers et al. (2005),
found that although the prevalence of the cicatricial and

Figure 1 A 75-years-old-male patient with history of severe
complications of trachoma in the form of eyelid retraction,
trichiasis/entropion and severe dry eye syndrome.
Figure 2 An 85-years-old male patient with long standing
history of eyelid trichiasis/entropion and associated corneal
scarring presented with inability to open his eyes. Surgical
correction in the form of entropion repair resulted in patient’s
ability to open his eyes.
Figure 3 A 60-years-old male with bilateral upper eyelid
retraction (A) due to tarsal/conjunctival contraction and corneal
scarring as Herbert’s pits (B and C), characteristic of trachoma.
Eradicating blinding trachoma: What is working? 17
blinding consequences of trachoma was decreasing in patientsaged 40 years or greater, it still remained a significant health
issue in an indigenous population within Central Australiawhen compared with other areas of Australia.
Presence of distichiasis and/or dysplastic eyelashes in tra-
chomatous trichiasis cases warrants further analytical studiesto confirm the observation and establish any causal association(Khandekar et al., 2004). In a prospective evaluation of theprevalence of distichiasis and/or dysplastic eyelashes among
trachomatous trichiasis cases at the oculoplasty unit of a hos-pital in Oman over 3 months period, among 80 cases, 58(72.5%) had abnormal eyelashes in addition to trachomatous
trichiasis (Khandekar et al., 2004). Dysplastic and distichiasiseyelashes were significantly more prevalent in trachomatoustrichiasis cases aged <50 years and those with entropion.
Severe trichiasis reflects the magnitude of the trachoma prob-lem in areas such as Ethiopia. Visual impairment due to trichi-asis may be highly associated with disease severity and
duration (Figs. 1 and 2). Among the 1635 individuals withtrichiasis presenting for surgery in the Wolayta Zone ofEthiopia, 82% had bilateral trichiasis and 91% of them re-ported trichiasis duration of >2 years (Melese et al., 2005).
Epilation was practised by over three fourths of the study sub-jects. A high proportion of patients tested positive for ocular
C. trachomatis at presentation; among them 17% had monoc-ular blindness and 8% had blindness in their both eyes.Corneal opacity was highly associated with the trichiasis dura-tion, severity and visual loss (Melese et al., 2005).
3. Mechanism of scarring
Trachoma appears to initiate a vicious cycle of mucus defi-
ciency, chronic conjunctival inflammation and conjunctivalscarring (Blodi et al., 1988). The basic mechanisms involvedin tissue damage and scarring following C. trachomatis remain
to be elucidated (Fig. 3). In specimens taken from patientswith active trachoma, the inflammatory infiltrate is organizedas lymphoid follicles in the underlying stroma and impression
cytology shows cytoplasmic elementary bodies. Immunohisto-chemical studies of conjunctival biopsies from children withactive trachoma demonstrate the presence of both humoral
and cell-mediated immune responses (Abu el-Asrar et al.,2001). In the active trachomatous conjunctivitis, macrophagesmay play an active role in conjunctival scarring by up-regulat-ing local production of extracellular matrix by the expression

18 I.A. Chaudhry
of the fibrogenic and angiogenic connective tissue growthfactor (Abu El-Asrar et al., 2006). In the chronic phase,inflammation causes scarring of the conjunctiva followed by
dry eye which can result in blindness. Trachoma may causedryness of the eye by decreased mucus production and aque-ous secretions (Fig. 1). Light microscopy may show subepi-
thelial fibrosis, membranes formation, squamous metaplasia,loss of goblet cells, pseudogland formation, degeneration oforbicularis oculi muscle fibres, subepithelial vascular dilata-
tion, localized perivascular amyloidosis and subepithelial lym-phocytic infiltration. Conjunctival impression cytology mayreveal significant reduction of goblet cell population amongthese patients. Accessory lacrimal glands and ducts may be
compromised by subepithelial infiltration and scarring. Thecontraction of the subepithelial fibrous tissue formed by col-lagen fibers and anterior surface drying are the main factors
contributing to the chronic cicatrization and entropion forma-tion (Guzey et al., 2000). Severe cases of trachoma may leadto contracture of the conjunctiva and deeper tissues including
Muller muscle and the tarsal plate. Hence, the upper eyelidsof these patients may show eyelid retraction that also mayshow as eyelid lag on patient’s down-gaze (Alsuhaibani and
Al-Fakey, 2007).
4. Mechanism of vision loss in trachoma
Repeated eye infection with C. trachomatis organism may trig-ger recurrent chronic inflammatory episodes leading to thedevelopment of conjunctival scarring. This scar tissue con-tracts, distorting the eyelids (entropion) causing contact be-
tween the eyelashes and the surface of the eye (trichiasis)compromising the cornea with blinding opacification (Tabbara,2001). Trichiasis/entropion may be the most common single
factor leading to the significant blinding complication. Infact,entropion may be the most significant predictor of cornealopacity (Figs. 1, 2 and 4). Eyelids of patients with inactive tra-
choma may be thickened. This thickening could be attributedto trachomatous changes in the conjunctiva and tarsus. Lightmicroscopy studies of tarsal plates and palpebral conjunctivae
obtained from the upper eyelids of patients having inactivetrachoma show a thick and compact subepithelial fibrous mem-
Figure 4 A 68-years-old female with severe trichiasis/entropion
and corneal scarring requiring penetrating keratoplasty for her
right eye. She had previous multiple hyfercations and entropion
repair of her right upper eyelid resulting in loss of anterior eyelid.
brane adherent to the tarsal plate (Al-Rajhi et al., 1993). Otherhistopathologic findings include atrophy of the meibomianglands with thickening of the acinar basement membrane, loss
of goblet cells, retention cysts, and hyaline degeneration of thetarsal plate with focal replacement by adipose tissue (Al-Rajhiet al., 1993). Chronic trichiasis and eyelid entropion can result
in significant corneal scarring and associated visual loss. In aretrospective study of 137 patients from Senegal who under-went 199 surgical procedures, over 51% of them already had
some kind of corneal complications due to abnormalities oftheir eyelid conditions. The average age of these patients was49 years with a higher percentage of women (Ndoye et al.,1997). Entropion is the most significant predictor of corneal
opacity. Cross sectional associations suggest that epilationmay not be helpful for eyes with mild entropion, but may offerprotection against corneal opacity in eyes with moderate to se-
vere entropion. Epilation may not be a substitute for trichiasissurgery, as 43% of eyes with severe entropion that have epila-tion performed may still have corneal opacities (West et al.,
2006). Marginal rotation by a posterior approach is an effectiveand simple procedure with fewer complications, even when per-formed by non-ophthalmologists. A study from the indigenous
population from the Upper Rio Negro basin of Brazil, on 73upper eyelids of 46 Indians (35 females, 11 males) with cicatri-cial upper eyelid trichiasis/entropion requiring surgery whichhad been performed by non-ophthalmologist physician who
had general surgery experience with an extremely short period(one week) of ophthalmic training has been reported (Soaresand Cruz, 2004). The surgery was performed by using a mar-
ginal rotational procedure by a posterior approach. Reevalua-tion 6 months after surgery revealed that 56 eyelids (76.7%)were free from trichiasis, whereas residual trichiasis was ob-
served in 17 eyelids (23.3%) of 10 subjects. In these cases, trichi-asis was either lateral or medial to the central portion of the lid.Of these 10 patients, only four reported that the surgery did not
improve the irritative symptoms (Soares and Cruz, 2004).Surgery for entropion may result in healing of superficial
keratopathy and improve tear film stability. The realigned eye-lid margin may spread tears evenly and efficiently, contributing
to improved vision. These changes may take place over 1–90days and should be considered when contemplating keratopl-asty, intraocular or keratorefractive procedures after
entropion correction (Monga et al., 2008). Patients with tra-chomatous trichiasis/entropion suffer in the physical, psycho-logical and environmental domains of health-related quality
of life even when vision is normal. Timely intervention is essen-tial not only to prevent corneal blindness but also to reduce thesuffering caused by the non-visual symptoms. In one prospec-tive, case-controlled, interventional study, health-related qual-
ity of life among the 60 patients with trachomatous trichiasis/entropion was found to be improved after intervention(Dhaliwal et al., 2006). Cornea grafting may be necessary in
patients who have significant corneal opacity despite correc-tion of trichiasis/entropion (Fig. 4). A recent study from KingKhaled Eye Specialist Hospital, treating 127 patients with
trachomatous corneal scarring undergoing penetrating kera-toplasty revealed that the procedure had a good prognosisfor graft survival in over 80% of patients over a 4-year
period (Al-Fawaz and Wagoner, 2008). Patients with mild orwell-controlled ocular surface disease and absent or previouslysurgically corrected eyelid abnormalities had the best visualoutcome.
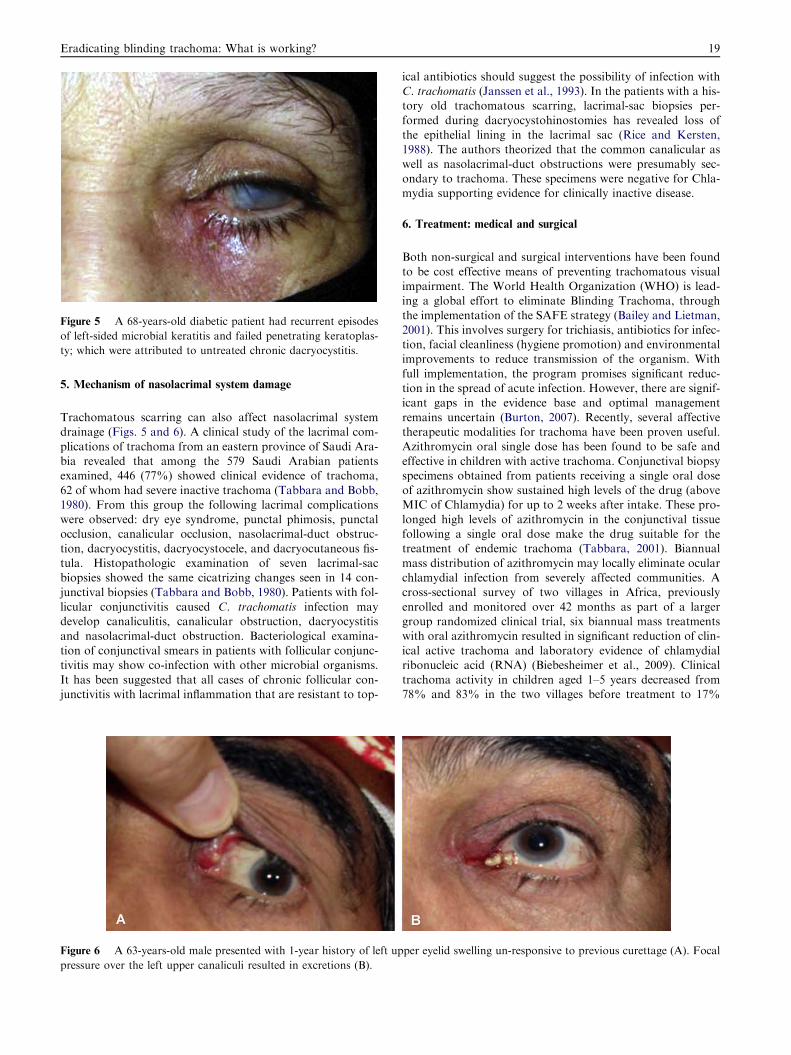
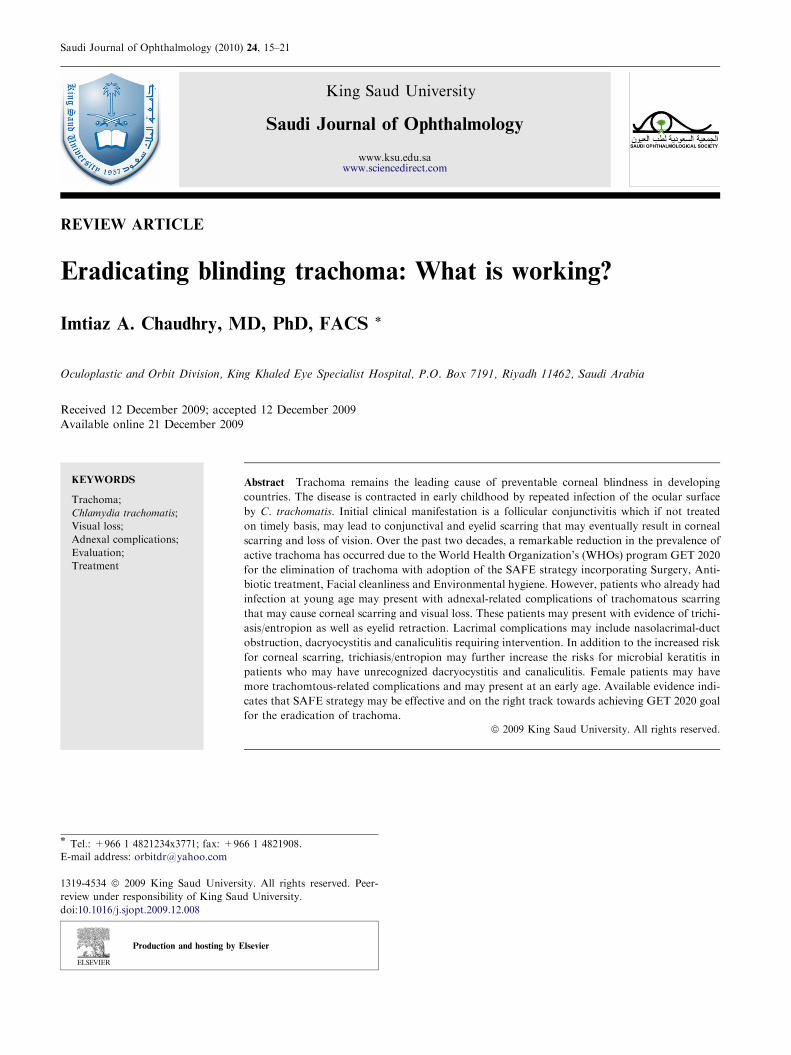
Figure 5 A 68-years-old diabetic patient had recurrent episodes
of left-sided microbial keratitis and failed penetrating keratoplas-
ty; which were attributed to untreated chronic dacryocystitis.
Eradicating blinding trachoma: What is working? 19
5. Mechanism of nasolacrimal system damage
Trachomatous scarring can also affect nasolacrimal systemdrainage (Figs. 5 and 6). A clinical study of the lacrimal com-
plications of trachoma from an eastern province of Saudi Ara-bia revealed that among the 579 Saudi Arabian patientsexamined, 446 (77%) showed clinical evidence of trachoma,
62 of whom had severe inactive trachoma (Tabbara and Bobb,1980). From this group the following lacrimal complicationswere observed: dry eye syndrome, punctal phimosis, punctalocclusion, canalicular occlusion, nasolacrimal-duct obstruc-
tion, dacryocystitis, dacryocystocele, and dacryocutaneous fis-tula. Histopathologic examination of seven lacrimal-sacbiopsies showed the same cicatrizing changes seen in 14 con-
junctival biopsies (Tabbara and Bobb, 1980). Patients with fol-licular conjunctivitis caused C. trachomatis infection maydevelop canaliculitis, canalicular obstruction, dacryocystitis
and nasolacrimal-duct obstruction. Bacteriological examina-tion of conjunctival smears in patients with follicular conjunc-tivitis may show co-infection with other microbial organisms.
It has been suggested that all cases of chronic follicular con-junctivitis with lacrimal inflammation that are resistant to top-
Figure 6 A 63-years-old male presented with 1-year history of left up
pressure over the left upper canaliculi resulted in excretions (B).
ical antibiotics should suggest the possibility of infection withC. trachomatis (Janssen et al., 1993). In the patients with a his-tory old trachomatous scarring, lacrimal-sac biopsies per-
formed during dacryocystohinostomies has revealed loss ofthe epithelial lining in the lacrimal sac (Rice and Kersten,1988). The authors theorized that the common canalicular as
well as nasolacrimal-duct obstructions were presumably sec-ondary to trachoma. These specimens were negative for Chla-mydia supporting evidence for clinically inactive disease.
6. Treatment: medical and surgical
Both non-surgical and surgical interventions have been found
to be cost effective means of preventing trachomatous visualimpairment. The World Health Organization (WHO) is lead-ing a global effort to eliminate Blinding Trachoma, through
the implementation of the SAFE strategy (Bailey and Lietman,2001). This involves surgery for trichiasis, antibiotics for infec-tion, facial cleanliness (hygiene promotion) and environmentalimprovements to reduce transmission of the organism. With
full implementation, the program promises significant reduc-tion in the spread of acute infection. However, there are signif-icant gaps in the evidence base and optimal management
remains uncertain (Burton, 2007). Recently, several affectivetherapeutic modalities for trachoma have been proven useful.Azithromycin oral single dose has been found to be safe and
effective in children with active trachoma. Conjunctival biopsyspecimens obtained from patients receiving a single oral doseof azithromycin show sustained high levels of the drug (aboveMIC of Chlamydia) for up to 2 weeks after intake. These pro-
longed high levels of azithromycin in the conjunctival tissuefollowing a single oral dose make the drug suitable for thetreatment of endemic trachoma (Tabbara, 2001). Biannual
mass distribution of azithromycin may locally eliminate ocularchlamydial infection from severely affected communities. Across-sectional survey of two villages in Africa, previously
enrolled and monitored over 42 months as part of a largergroup randomized clinical trial, six biannual mass treatmentswith oral azithromycin resulted in significant reduction of clin-
ical active trachoma and laboratory evidence of chlamydialribonucleic acid (RNA) (Biebesheimer et al., 2009). Clinicaltrachoma activity in children aged 1–5 years decreased from78% and 83% in the two villages before treatment to 17%
per eyelid swelling un-responsive to previous curettage (A). Focal

20 I.A. Chaudhry
and 24% at 42 months. Polymerase chain reaction evidence ofinfection in the same age group decreased from 48% to 0% inboth villages at 42 months. When all age groups were exam-
ined, there were zero cases with evidence of chlamydial RNAamong 758 total villagers tested (Biebesheimer et al., 2009).
Management of trachomatous cicatricial trichiasis and
entropion of the eyelids presents a difficult problem (Yorstonand Mabey, 2006). Over the years, many surgical approacheshave been developed to address it (Yorston and Mabey,
2006; Cockburn, 1943; Chandra and Taneja, 1964; Sandford-Smith, 1976; Thommy, 1980; Niederer and Sutter, 1981; Riceet al., 1989; Teichmann, 1988; Nasr, 1991; Bujger et al.,2004; Sadiq and Pai, 2005). Although the WHO document
WHO/PBL/93.29 recommends the bilamellar tarsal rotationoperation for trachomatous entropion, Bujger et al. (2004),has described an operation that has proved to be very reliable.
It is a modified tarsal wedge resection and the eversion splint-ing-grey line incision. A possible additional correction of thegrey line incision may improve the results. By this method,
the rate of failed operations, which consisted of incompleteclosure of the lids or more than two inverted lashes remaining,was 6.9% (Bujger et al., 2004). A modified version of Wies’s
operation offers the correction of cicatricial entropion in whichthe most important modification being a different plane for theincision through the eyelid (Sandford-Smith, 1976). Certaininterventions have been shown to be more effective at eliminat-
ing trichiasis. Most effective surgery, however, is the full-thick-ness incision of the tarsal plate and rotation of the terminaltarsal strip 180�. Full thickness incision of the tarsal plate
and rotation of the lash-bearing lid margin through 180� isprobably the best technique and is preferable in the communitysettings. The use of double-sided sticking plaster is more effec-
tive than epilation as a temporary measure. Surgery may becarried out by an ophthalmologist or a trained ophthalmicassistant. The addition of azithromycin treatment at the time
of surgery may not improve the outcome (Yorston andMabey,2006). A modified surgical technique combining bilamellar tar-sal margin rotation procedure with blepharoplasty has beenadvocated (Sadiq and Pai, 2005). With this technique, the eye-
lids as well as the normal eyelashes can be rotated away fromthe surface of the eye. These eyes may have adequate lid clo-sure and regular lid margin. This modified technique prevents
any overhanging baggy fold of skin at operation site. Further,the modified technique of combining bilamellar tarsal rotationprocedure with blepharoplasty appears to be an effective surgi-
cal technique in the management of the trachomatous cicatri-cial entropion of the upper eye lid. It achieves successfulanatomical correction along with more acceptable cosmeticappearance (Sadiq and Pai, 2005). Isolated cilia posterior to
normal lash line can be treated by hyfercation.In developing countries, where manpower and other re-
sources are limited and patient-load high, ophthalmic surgeons
should choose a procedure that is simple, quick and effective.In a prospective study lids with moderate or severe trachoma-tous entropion were compared for the efficacy of three com-
mon surgical procedures of increasing complexity in thecorrection of trachomatous entropion by either terminal tarsalrotation, tarsal rotation with tarso-conjunctival advancement,
or anterior lamellar repositioning with lid margin split andwedge resection of tarsus (Dhaliwal et al., 2004). The proce-dures were compared for improvement of symptoms, durationof surgery, cosmesis, rate and type of complications, anatom-
ical correction, failure and recurrence. Terminal tarsal rota-tion, the simplest technique took significantly less time. Thethree procedures were comparable in achieving cosmesis, ana-
tomical correction, and rate of complications. In general, ter-minal tarsal rotation after transverse tarsotomy should bethe procedure of choice in the correction of moderate or severe
(without lid gap) trachomatous entropion. A lid-splitting pro-cedure by using a bare-tarsus technique and omitting anygrafting has been recommended by Teichmann (1988), in pa-
tients with trachomatous entropion. Additional radial inci-sions at the nasal and temporal edges of the anterior lamellamay be advantageous, as the often superimposed blepharo-spasm can be abolished by the weakening of the tarsal part
of the orbicularis muscle (Teichmann, 1988). Also, there maybe low tendency for the recessed anterior lamella to creep backdown to the lid margin. Cicatricial entropion with hard palate
mucous membrane grafting for both upper and lower eyelidsurgery may offer high symptomatic and anatomical curerates. The requirement for further surgical intervention may
be low (Swamy et al., 2008).In conclusion, by the establishment of the GET 2020 goal,
the WHO has set an ambitious target for country programs.
The currently recommended SAFE strategy targets all key ele-ments believed to be necessary for a short- and long-term inter-vention program. Additional research may enhance theimplementation of the SAFE strategy. In the current climate
of significant political and social momentum for trachomacontrol, the SAFE strategy is a safe bet to accomplish the erad-ication of blinding trachoma (West, 2003).
References
Abu el-Asrar, A.M., Geboes, K., Missotten, L., 2001. Immunology of
trachomatous conjunctivitis. Bull. Soc. Belge. Ophtalmol. 280, 73–
96.
Abu El-Asrar, A.M., Al-Kharashi, S.A., Missotten, L., Geboes, K.,
2006. Expression of growth factors in the conjunctiva from patients
with active trachoma. Eye 20, 362–369.
Al-Fawaz, A., Wagoner, M.D., 2008. King Khaled Eye Specialist
Hospital corneal transplant study group. Penetrating keratoplasty
for trachomatous corneal scarring. Cornea 27, 129–132.
Al-Rajhi, A.A., Hidayat, A., Nasr, A., Al-Faran, M., 1993. The
histopathology and the mechanism of entropion in patients with
trachoma. Ophthalmology 100, 1293–1296.
Al-Rifai, K.M., 1988. Trachoma through history. Int. Ophthalmol. 12,
9–14.
Alsuhaibani, A.H., Al-Fakey, Y.H., 2007. Unilateral eyelid lag and
retraction as sequelae of trachoma. Ophthal. Plast. Reconstr. Surg.
23, 169–170.
Bailey, R., Lietman, T., 2001. The SAFE strategy for the elimination
of trachoma by 2020: will it work? Bull. World Health Organ. 79,
233–236.
Barenfanger, J., 1975. Studies on the role of the family unit in the
transmission of trachoma. Am. J. Trop. Med. Hyg. 24, 509–515.
Bell, S.D., McComb, D.E., Nichols, R.L., Roca-Garcia, M., 1970.
Studies on trachoma. VII. Isolation of a mixture of type 1 and type
2. Trachoma strains from a child in Saudi Arabia. Am. J. Trop.
Med. Hyg. 19, 842–845.
Biebesheimer, J.B., House, J., Hong, K.C., Lakew, T., Alemayehu, W.,
Zhou, Z., Moncada, J., Roger, A., Keenan, J., Gaynor, B.D.,
Schachter, J., Lietman, T.M., 2009. Complete local elimination of
infectious trachoma from severely affected communities after six
biannual mass Azithromycin distributions. Ophthalmology 116,
2047–2050.
Eradicating blinding trachoma: What is working? 21
Blodi, B.A., Byrne, K.A., Tabbara, K.F., 1988. Goblet cell population
among patients with inactive trachoma. Int. Ophthalmol. 12, 41–
45.
Bobb Jr., A.A., Nichols, R.L., 1969. Influence of environment on
clinical trachoma in Saudi Arabia. Am. J. Ophthalmol. 67, 235–
243.
Bujger, Z., Cerovski, B., Kovacevic, S., Nasic, M., Pokupec, R.,
Tojagic, M., 2004. A contribution to the surgery of the trachom-
atous entropion and trichiasis. Ophthalmologica 218, 214–218.
Burton, M.J., 2007. Trachoma: an overview. Br. Med. Bull. 84, 99–
116.
Chandra, P., Taneja, K.L., 1964. Correction of cicatricial entropion of
upper lid by insertion of acrylic plate. J. All India Ophthalmol. Soc.
12, 107–113.
Cockburn, C., 1943. An operation for entropion of rachoma. Br. J.
Ophthalmol. 27, 308–310.
Courtright, P., Sheppard, J., Schachter, J., Said, M.E., Dawson, C.R.,
1989. Trachoma and blindness in the Nile Delta: current patterns
and projections for the future in the rural Egyptian population. Br.
J. Ophthalmol. 73, 536–540.
Dhaliwal, U., Monga, P.K., Gupta, V.P., 2004. Comparison of three
surgical procedures of differing complexity in the correction of
trachomatous upper lid entropion: a prospective study. Orbit 23,
227–236.
Dhaliwal, U., Nagpal, G., Bhatia, M.S., 2006. Health-related quality
of life in patients with trachomatous trichiasis or entropion.
Ophthal. Epidemiol. 13, 59–66.
Dolin, P.J., Faal, H., Johnson, G.J., Minassian, D., Sowa, S., Day, S.,
Ajewole, J., Mohamed, A.A., Foster, A., 1997. Reduction of
trachoma in a sub-Saharan village in absence of a disease control
programme. Lancet 349, 1511–1512.
Evans, T.G., Ranson, M.K., Kyaw, T.A., Ko, C.K., 1996. Cost
effectiveness and cost utility of preventing trachomatous visual
impairment: lessons from 30 years of trachoma control in Burma.
Br. J. Ophthalmol. 80, 880–889.
Guzey, M., Ozardali, I., Basar, E., Aslan, G., Satici, A., Karadede, S.,
2000. A survey of trachoma: the histopathology and the mechanism
of progressive cicatrization of eyelid tissues. Ophthalmologica 214,
277–284.
Janssen, K., Gerding, H., Busse, H., 1993. Recurrent canaliculitis and
dacryocystitis as a sequela of persistent infection with Chlamydia
trachomatis. Ophthalmologe 90, 17–20.
Khandekar, R., Kidiyur, S., Al-Raisi, A., 2004. Distichiasis and
dysplastic eyelashes in trachomatous trichiasis cases in Oman: a
case series. East Mediterr. Health J. 10, 192–197.
Landers, J., Kleinschmidt, A., Wu, J., Burt, B., Ewald, D., Henderson,
T., 2005. Prevalence of cicatricial trachoma in an indigenous
population of Central Australia: the Central Australian Trachoma-
tous Trichiasis Study (CATTS). Clin. Exp. Ophthalmol. 33, 142–146.
McComb, D.E., Nichols, R.L., 1969. Antibodies to trachoma in eye
secretions of Saudi Arab children. Am. J. Epidemiol. 90, 278–284.
McComb, D.E., Nichols, R.L., 1970. Antibody type specificity to
trachoma in eye secretions of Saudi Arab children. Infect. Immun.
2, 65–68.
Melese, M., West, E.S., Alemayehu, W., Munoz, B., Worku, A.,
Gaydos, C.A., West, S.K., 2005. Characteristics of trichiasis
patients presenting for surgery in rural Ethiopia. Br. J. Ophthal-
mol. 89, 1084–1088.
Monga, P., Gupta, V.P., Dhaliwal, U., 2008. Clinical evaluation of
changes in cornea and tear film after surgery for trachomatous
upper lid entropion. Eye 22, 912–917.
Murray, E.S., Bell Jr., S.D., Hanna, A.T., Nichols, R.L., Snyder, J.C.,
1960. Studies on trachoma. 1. Isolation and identification of strains
of elementary bodies from Saudi Arabia and Egypt. Am. J. Trop.
Med. Hyg. 9, 116–124.
Nasr, A.M., 1991. Eyelid complications in trachoma: diagnosis and
management. Acta Ophthalmol. (Copenh) 69, 200–204.
Ndoye, P.A., Ngom, A., Ndiaye, C.S., Ba, E.A., Ndiaye, P.A.,
Ndiaye, M.R., Wade, A., 1997. Trachomatous entropion
trichiasis at the ophthalmologic clinic of Dantec CHU (apro-
pos of 199 cases). Rev. Int. Trach. Pathol. Ocul. Trop.
Subtrop Sante Publique 74, 97–106.
Nichols, R.L., Bell Jr., S.D., Murray, E.S., Haddad, N.A., Bobb, A.A.,
1966. Studies on trachoma. V. Clinical observations in a field trial
of bivalent trachoma vaccine at three dosage levels in Saudi Arabia.
Am. J. Trop. Med. Hyg. 15, 639–647.
Nichols, R.L., Bobb, A.A., Haddad, N.A., McComb, D.E., 1967.
Immunofluorescent studies of the microbiologic epidemiology of
trachoma in Saudi Arabia. Am. J. Ophthalmol. 63, 1372–1408.
Nichols, R.L., Bell Jr., S.D., Haddad, N.A., Bobb, A.A., 1969. Studies
on trachoma. VI. Microbiological observations in a field trial in
Saudi Arabia of bivalent rachoma vaccine at three dosage levels..
Am. J. Trop. Med. Hyg. 18, 723–730.
Niederer, W., Sutter, E., 1981. Different methods of treatment of
upper lid entropion (author’s transl.). Klin Monatsbl Augenheilkd
178, 464–468.
Rice, C.D., Kersten, R.C., 1988. Absence of Chlamydia in trachom-
atous lacrimal sacs. Am. J. Ophthalmol. 105, 203–206.
Rice, C.D., Kersten, R.C., Al-Hazzaa, S., 1989. Cryotherapy for
trichiasis in trachoma. Arch. Ophthalmol. 107, 1180–1182.
Sadiq, M.N., Pai, A., 2005. Management of trachomatous cicatricial
entropion of the upper eye lid: our modified technique. J. Ayub.
Med. Coll. Abbottabad. 17, 1–4.
Sandford-Smith, J.H., 1976. Surgical correction of trachomatous
cicatricial entropion. Br. J. Ophthalmol. 60, 253–255.
Soares, O.E., Cruz, A.A., 2004. Community-based transconjunctival
marginal rotation for cicatricial trachoma in Indians from the
Upper Rio Negro basin. Braz. J. Med. Biol. Res. 37, 669–674.
Solomon, A., Mabey, D., 2007. Trachoma. Clin. Evid. (Online). 7, pii:
0706.
Swamy, B.N., Benger, R., Taylor, S., 2008. Cicatricial entropion repair
with hard palate mucous membrane graft: surgical technique and
outcomes. Clin. Exp. Ophthalmol. 36, 348–352.
Tabbara, K.F., 2001. Trachoma: a review. J. Chemother. 13 (Suppl. 1),
18–22.
Tabbara, K.F., 2001. Blindness in the Eastern Mediterranean coun-
tries. Br. J. Ophthalmol. 85, 771–775.
Tabbara, K.F., Al-Omar, O.M., 1997. Trachoma in Saudi Arabia.
Ophthal. Epidemiol. 4, 127–140.
Tabbara, K.F., Bobb, A.A., 1980. Lacrimal system complications in
trachoma. Ophthalmology 87, 298–301.
Tabbara, K.F., Ross-Degnan, D., 1986. Blindness in Saudi Arabia.
JAMA 255, 3378–3384.
Teichmann, K.D., 1988. Correction of severe upper eyelid entropion.
Int. Ophthalmol. 12, 37–39.
Thommy, C.P., 1980. A modified technique for correction of
trachomatous cicatricial entropion. Br. J. Ophthalmol. 64, 296–
298.
West, S.K., 2003. Blinding trachoma: prevention with the safe strategy.
Am. J. Trop. Med. Hyg. 69, 18–23.
West, S.K., Munoz, B., Turner, V.M., Mmbaga, B.B., Taylor, H.R.,
1991. The epidemiology of trachoma in central Tanzania. Int. J.
Epidemiol. 20, 1088–1092.
West, E.S., Munoz, B., Imeru, A., Alemayehu, W., Melese, M., West,
S.K., 2006. The association between epilation and corneal opacity
among eyes with trachomatous trichiasis. Br. J. Ophthalmol. 90,
171–174.
Yorston, D., Mabey, D., Hatt, S., Burton, M., 2006. Interventions
for trachoma trichiasis. Cochrane Database Syst. Rev. 3
(CD004008).