episodes of care: background and issues james m naessens, scd division of health care policy &...
TRANSCRIPT

Episodes of Care:Episodes of Care: Background and Issues Background and Issues
James M Naessens, ScDJames M Naessens, ScD
Division of Health Care Policy & ResearchDivision of Health Care Policy & Research
Mayo ClinicMayo Clinic

OutlineOutline
• Episodes of CareEpisodes of Care• BackgroundBackground• ApproachesApproaches
• Current Issues with EpisodesCurrent Issues with Episodes• CMSCMS• Health Affairs Sept/Oct 2009Health Affairs Sept/Oct 2009
• Mayo Clinic StudiesMayo Clinic Studies• Referral PracticeReferral Practice• Chronic Disease CohortsChronic Disease Cohorts

Episodes of CareEpisodes of Care
• Concept first introduced in 1960’s by Concept first introduced in 1960’s by Solon J, et al.^ Solon J, et al.^
• Advanced by Hornbrook M, et al.*Advanced by Hornbrook M, et al.*
“ “series of temporally contiguous series of temporally contiguous health care services related to health care services related to treatment of a given spell of illness or treatment of a given spell of illness or provided in response to a specific provided in response to a specific request by the patient” request by the patient”
* Med Care Rev. 1985;42:163-218 ^ American Journal of Public Health. 1967;57:401-408

Episode of Care UsesEpisode of Care Uses
• Provide measurement and treatment Provide measurement and treatment guidelines for physicians guidelines for physicians
• Define boundaries of reimbursement Define boundaries of reimbursement
• Determine risk adjustment Determine risk adjustment
• For health care utilization analysisFor health care utilization analysis
• Operational aspects of health care Operational aspects of health care delivery delivery (Mayo Clinic medical record (Mayo Clinic medical record management) management)

Episode of Care Episode of Care Current Basis for Payment ProjectsCurrent Basis for Payment Projects
• Geisinger - Cardiac Surgery Geisinger - Cardiac Surgery “guarantee”“guarantee”
• Medicare Acute Care Demonstration Medicare Acute Care Demonstration Project – bundling for ortho and CV Project – bundling for ortho and CV proceduresprocedures
• Medicare Physician Hospital Medicare Physician Hospital Collaboration demonstration – Collaboration demonstration – immediate post hospital periodimmediate post hospital period

Our ProblemOur ProblemOutpatient Care AnalysisOutpatient Care Analysis
• Capitated model / primary careCapitated model / primary care PatientPatient
• Fee for service modelFee for service model EncounterEncounter ServiceService
• Referral careReferral care Episode (??)Episode (??)
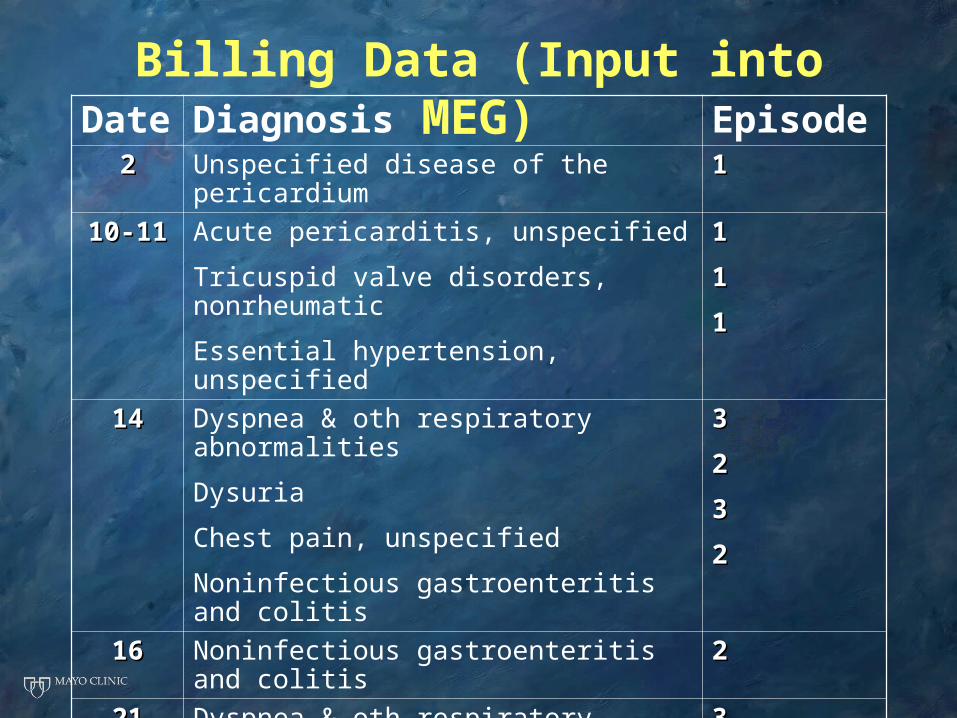
Billing Data (Input into MEG)Date Diagnosis Episode
22 Unspecified disease of the pericardium 11
10-1110-11 Acute pericarditis, unspecified
Tricuspid valve disorders, nonrheumatic
Essential hypertension, unspecified
11
11
11
1414 Dyspnea & oth respiratory abnormalities
Dysuria
Chest pain, unspecified
Noninfectious gastroenteritis and colitis
33
22
33
22
1616 Noninfectious gastroenteritis and colitis 22
2121 Dyspnea & oth respiratory abnormalities
Chest pain, unspecified
33
33
2525 Unspecified disease of the pericardium 11

Example: one patient’s visits for one monthExample: one patient’s visits for one month1 2 3 4 5 6 7
8 9 10 11 12 13 14
15 16 17 18 19 20 21
22 23 24 25 26 27 28
29 30 31
Episode 1
Episode 1
Episode 1
Episode 1
Episode 3
Episode 3
Episode 2
Episode 2
Colored days represent days the patient was received services.
Episode GroupersEpisode Groupers
• Rosen and Mayer-Oakes* compared Rosen and Mayer-Oakes* compared four major episode grouper four major episode grouper programs:programs:
• Episode Treatment Groups (ETG)Episode Treatment Groups (ETG)
• Clinical Episode Groups (CEG)Clinical Episode Groups (CEG)
• Physician Review SystemPhysician Review System
• CareTrend CareTrend
With no distinctly superior product With no distinctly superior product *Jt Comm J Qual Improv. 1999;25:111-28

Episode Groupers:Episode Groupers:Methodological IssuesMethodological Issues
• Starting Point (diagnosis, symptom or Starting Point (diagnosis, symptom or visit) visit)
• End Point (defined length or “clean End Point (defined length or “clean period”)period”)
• Comprehensiveness of Services Comprehensiveness of Services (concurrent episodes?)(concurrent episodes?)
• Clinical Complexity (chronic disease Clinical Complexity (chronic disease with flare-ups, unrelated acute illness, with flare-ups, unrelated acute illness, multiple comorbidities)multiple comorbidities)
• Provider AttributionProvider Attribution

CMS Episode Grouper Listening CMS Episode Grouper Listening Session November 10, 2009 Session November 10, 2009
• CMS intends on using input to write CMS intends on using input to write RFP on developing a transparent RFP on developing a transparent software for episodes of care for software for episodes of care for Medicare beneficiaries Medicare beneficiaries • Multiple Chronic Conditions Multiple Chronic Conditions • Post-acute Care Post-acute Care • Length of Chronic Episode Length of Chronic Episode • Physician Services Physician Services • Risk Adjustment Risk Adjustment

Health Affairs Health Affairs Sept/Oct 2009 issueSept/Oct 2009 issue
• Episode-Based Performance Episode-Based Performance Measurement And Payment: Making Measurement And Payment: Making It A RealityIt A Reality Peter S. Hussey et al.Peter S. Hussey et al.
• From Volume To Value: Better Ways From Volume To Value: Better Ways To Pay For Health CareTo Pay For Health Care Harold D. MillerHarold D. Miller
• Measurement Of And Reward For Measurement Of And Reward For Efficiency In California’s Pay-For-Efficiency In California’s Pay-For-Performance ProgramPerformance Program James C. Robinson et al.James C. Robinson et al.

Hussey articleHussey article
• Applies ETGs and MEGs to Medicare part A & B data for 3 states, 2004-6.
• Identifies Issues with:Identifies Issues with:• Defining Episodes Defining Episodes
• Different settingsDifferent settings• Single- vs. multi-condition focusSingle- vs. multi-condition focus• Within group heterogeneityWithin group heterogeneity
• Attributing responsibilityAttributing responsibility
• Calls for more empirical workCalls for more empirical work
Miller articleMiller article
• Suggests that each of 4 methods: FFS, Episodes, Capitation, Comprehensive care payments (condition-adjusted capitation) has role
• Issues to address:• Bundling challengesBundling challenges• Setting payment amountsSetting payment amounts• Assuring qualityAssuring quality• Aligning incentivesAligning incentives

Robinson articleRobinson article
• Reviews the California Integrated Healthcare Association Pay for Performance experience addressing efficiency using episodes (MEG)
• Issues:• Small numbers of patients/episode• Incomplete data• Weights (standard or actual costs)

Mayo Cardiovascular Referral Practice Mayo Cardiovascular Referral Practice Study GoalsStudy Goals
• Do Medstat’s Episodes provide a Do Medstat’s Episodes provide a useful management tool to help useful management tool to help understand a multi-specialty group understand a multi-specialty group practice?practice?
• Can we use MEG as a basis to Can we use MEG as a basis to understand different use patterns understand different use patterns between rural and urban patients? between rural and urban patients?

MethodsMethodsPatientsPatients
• All patients seen in 2003All patients seen in 2003 For outpatient service For outpatient service By a cardiovascular providerBy a cardiovascular provider N=102,406N=102,406
SettingSetting
• Mayo Clinic, Rochester, MinnesotaMayo Clinic, Rochester, Minnesota

Comparisons of InterestComparisons of Interest
• Primary care vs. referral Primary care vs. referral
• Mayo Health System Mayo Health System
• Local vs. regional vs. national Local vs. regional vs. national

Episode OutcomesEpisode Outcomes• Cardiovascular intensityCardiovascular intensity
Low DiagnosticLow Diagnostic Cardiovascular E & MCardiovascular E & M High DiagnosticHigh Diagnostic Therapy Procedures Therapy Procedures
• HospitalizationHospitalization
• CostCost

Statistical MethodologyStatistical Methodology• Outcome modelsOutcome models
Do the types of episodes differ?Do the types of episodes differ? Are the outcomes (average cost, Are the outcomes (average cost,
hospitalization, and cardiovascular hospitalization, and cardiovascular intensity) different between rural vs. intensity) different between rural vs. urban patient after incorporating urban patient after incorporating episode type, severity of episode and episode type, severity of episode and comorbidity?comorbidity?

Statistical MethodologyStatistical Methodology• Logistic and linear regression Logistic and linear regression
models developed to account for models developed to account for impacts of Mayo primary care, impacts of Mayo primary care, distance traveled, age, gender, pay distance traveled, age, gender, pay source, and physician vs. self-source, and physician vs. self-referred.referred.
• Impact of rural-urban influence Impact of rural-urban influence added to adjusted model. added to adjusted model.

Summary FindingsSummary Findings
• 96,601 patients with CV 96,601 patients with CV
provided service in 2003provided service in 2003
• 287,162 outpatient CV 287,162 outpatient CV
visits and 29,369 visits and 29,369
hospitalizations hospitalizations
in 464,067 episodes in 464,067 episodes
(90,922 CV episodes) (90,922 CV episodes)
CV Episodes
0
5
10
15
20
25
PrimaryCare
Other%

Most Frequent Episodes with Most Frequent Episodes with Cardiologist E & M VisitCardiologist E & M Visit
## %%
Angina pectorisAngina pectoris 91169116 11.011.0
ArrhythmiasArrhythmias 69936993 8.48.4
Essential hypertension, chronic maintEssential hypertension, chronic maint 42704270 5.25.2
Preventive health servicesPreventive health services 29712971 3.63.6
Other respiratory symptomsOther respiratory symptoms 28822882 3.53.5
Complications surgical/medical careComplications surgical/medical care 23462346 2.82.8
CardiomyopathiesCardiomyopathies 22242224 2.72.7
OsteoarthritisOsteoarthritis 19331933 2.32.3
Aortic stenosisAortic stenosis 17491749 2.12.1
Mitral stenosisMitral stenosis 16651665 2.02.0

Episodes withEpisodes withCardiologist E & M VisitCardiologist E & M Visit
CV45%
non-CV55%
• 14 conditions had 14 conditions had 1000+ episodes1000+ episodes
• 22 conditions had 22 conditions had 500 - 999 episodes500 - 999 episodes
• 74 conditions had 74 conditions had 100 - 499 episodes100 - 499 episodes
• 62 conditions had 62 conditions had 50 - 99 episodes50 - 99 episodes
• 450 conditions had 450 conditions had episodesepisodes

Influence of Distance and Primary Influence of Distance and Primary CareCare
Primary Care Patients
91%
9%
Local Non-Local
Local Patients
71%
29%
Primary Care Non Primary Care

Cardiovascular IntensityCardiovascular IntensityEpisodes with CV E & MEpisodes with CV E & M
0% 20% 40% 60% 80% 100%
International
National
Regional
Local
Primary Care
CV E & M
High DX
Therapy PX

Cardiovascular IntensityCardiovascular IntensityEpisodes with CV E & MEpisodes with CV E & M
0% 20% 40% 60% 80% 100%
Self
Physician
CV E & M
High DX
Therapy PX
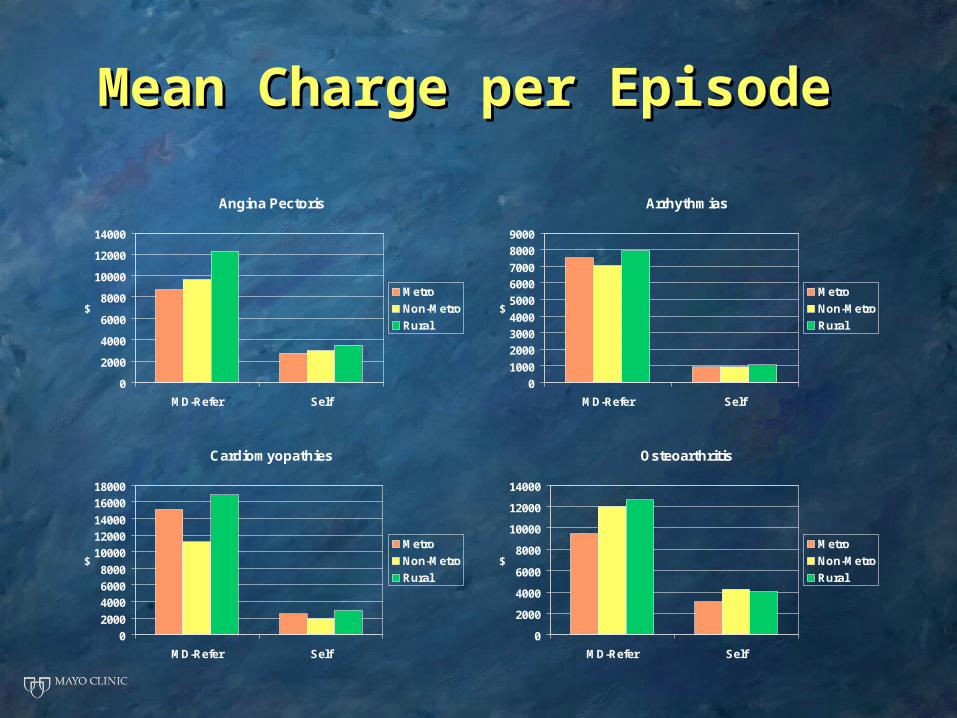
Mean Charge per EpisodeMean Charge per Episode
Angina Pectoris
0
2000
4000
6000
8000
10000
12000
14000
MD-Refer Self
$Metro
Non-Metro
Rural
Arrhythmias
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
MD-Refer Self
$Metro
Non-Metro
Rural
Cardiomyopathies
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
MD-Refer Self
$Metro
Non-Metro
Rural
Osteoarthritis
0
2000
4000
6000
8000
10000
12000
14000
MD-Refer Self
$Metro
Non-Metro
Rural

SummarySummaryEpisodes in Specialty PracticeEpisodes in Specialty Practice
• Episodes of care were able to categorize both Episodes of care were able to categorize both primary care and referral patients. primary care and referral patients.
• However, after adjustment mean costs per However, after adjustment mean costs per episode differed significantly between the two episode differed significantly between the two groups for many types of episodes. groups for many types of episodes.
• Episodes developed for managed care practices Episodes developed for managed care practices may have limited utility for referral specialty may have limited utility for referral specialty practices. practices.
• Further assessment needed on the differences Further assessment needed on the differences between primary care and referral practice between primary care and referral practice episodes. episodes.

Mayo Chronic Disease Cohort Mayo Chronic Disease Cohort Study GoalStudy Goal
• How well do various systems capture How well do various systems capture and characterize the health care and characterize the health care costs of people with chronic costs of people with chronic disease?disease?

MethodsMethodsPatientsPatients
• Mayo employees/dependents with continuous Mayo employees/dependents with continuous health benefit enrollment from 2003-2006health benefit enrollment from 2003-2006 Cohort 1: Meet HEDIS definitions for Cohort 1: Meet HEDIS definitions for
diabetes in 2000-2003diabetes in 2000-2003 Cohort 2: Meet HEDIS definitions for CAD Cohort 2: Meet HEDIS definitions for CAD
in 2000-2003in 2000-2003
Data SourceData Source
• Medical and Pharmacy ClaimsMedical and Pharmacy Claims

MethodsMethods
• Generate Total Costs for 2003-2006Generate Total Costs for 2003-2006
• Apply Prometheus Models to CohortApply Prometheus Models to Cohort
• Apply ETGs to CohortApply ETGs to Cohort
• WORK IN PROGRESS!WORK IN PROGRESS!
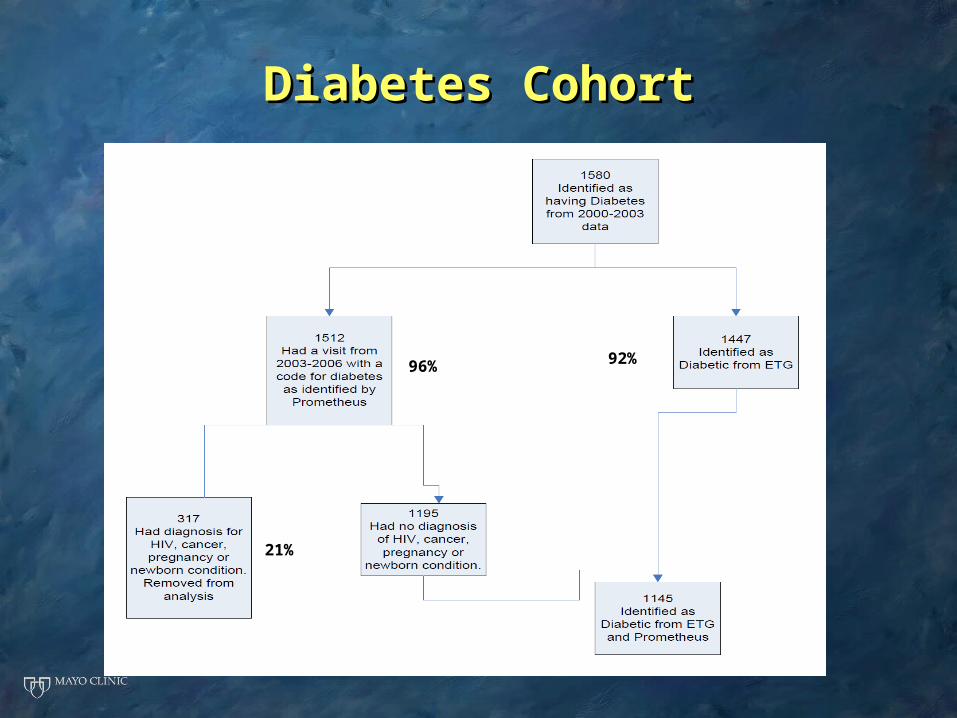
Diabetes CohortDiabetes Cohort
96%96% 92%
21%

CAD CohortCAD Cohort
69% 60%
16%
SummarySummaryEpisodes in Chronic Disease Episodes in Chronic Disease
CohortsCohorts• Different schemes identify different Different schemes identify different
patients in disease cohorts.patients in disease cohorts.
• ETGs and Prometheus capture only a ETGs and Prometheus capture only a portion of costs of Diabetes and CAD portion of costs of Diabetes and CAD cohorts.cohorts.
• ETG hierarchy influences what they ETG hierarchy influences what they consider as disease-related costs.consider as disease-related costs.