epiduroscopy in the 21 th century: state of the art jan willem kallewaard, alysis zorggroep arnhem 5...
TRANSCRIPT

Epiduroscopy
in the 21th Century:
State of the art
Jan Willem Kallewaard, Alysis zorggroep Arnhem
5 maart 2010 Veldhoven
Evidence Based Medicine• Best available evidence
• Interventional techniques
– Largely lack valid comparators, such as no treatment
– Are crippled by a lack of vigorous self-evaluation of its role in the treatment of chronic pain
• Evidence-based medicine movement gives little guidance to practitioners whose
tools are still under development
• Advice:
– Monitor your outcomes using valid measures
– Be more reflective and systematic in studying your own outcomes and patterns of care
– Provide this information to your patients as part of the decision-making process
– Apply outcome instruments that are sensitive and precise enough to detect clinically
significant change in the practical setting
Merrill DG. Reg Anesth Pain Med 2003; 28: 547-560Rathnell & Carr. Editorial. Reg Anesth Pain Med 2003; 28: 498-501Praktische richtlijnen anesthesiologische pijnbestrijding 2009
Pain management EBM
• Short term effects>3mnth
• Long term effects>6mnth

Current algorithm FBSS patient
• Conservative therapy ( Med/FT/TENS)• Epidural injection//PRF• Neuroplasty ( RACZ)• Epiduroscopy• Neuromodulation
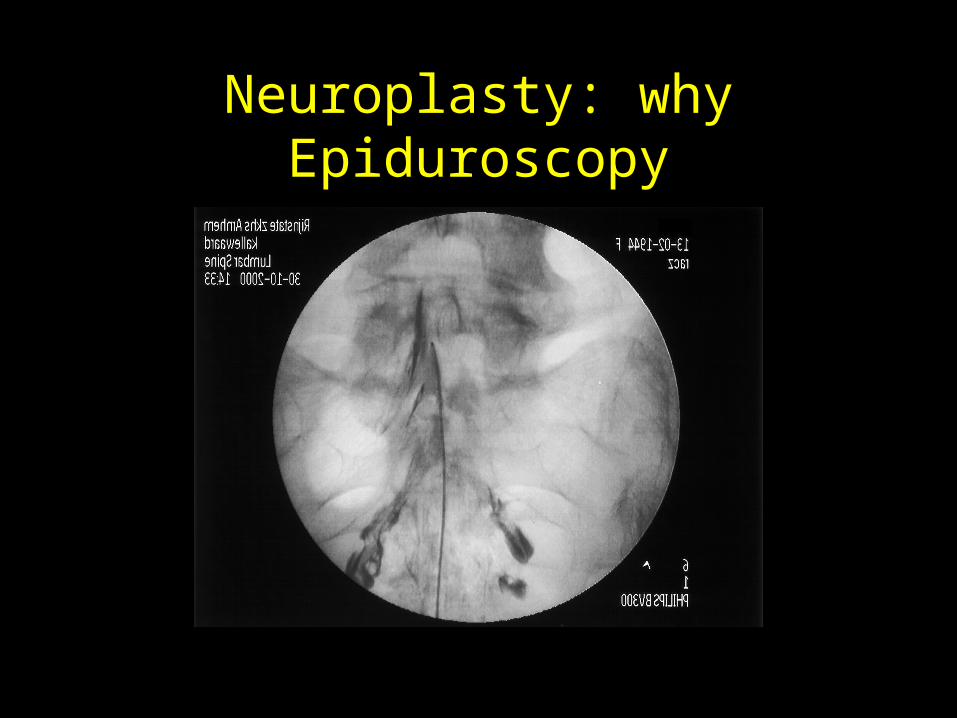
Neuroplasty: why Epiduroscopy
History• 1931 Burman visualisation spinal canal; s.o.
• 1936 Elias Stern; s.o.; animalexperiments.
• 1937 Pool 1th spinal endoscopy; pat.• 1970 Ooi et al Fiberoptic scope; pat.
• 1970 Blomberg; s.o.; 10 pat.; rigid scope
• ± 1985 flexible scope• Igarashi et al
– Thoracic en Lumbar– age, pregnancy, : epid structures– Indication: spinal stenosis
• Diagnostic tool– Adhaesive arachnoiditis
• 1991 Shimoji et al; diam. <<; fiber- flexible scoop;

• Saberski et al– Hiatus sacralis: less chance of dura perforation– 2 canals
• Richardson et al– Epidural pressure monitoringI

Main Indications (2009)
• Chronic radiculopathic pain• Spinal stenosis• Diagnostic tool
Applications – Diagnostical Features
• Confirmation of presumed diagnoses unverifiable by conventional diagnostics (e.g., CT/MRI):
• epidural adhesions• inflammation• tumors• anatomical abnormalities• biopsies
• Support & facilitation of catheter placement and electrode implantation
• ? Postoperative assessment• ? Electrical stimulation (case report: PRF through endoscope)
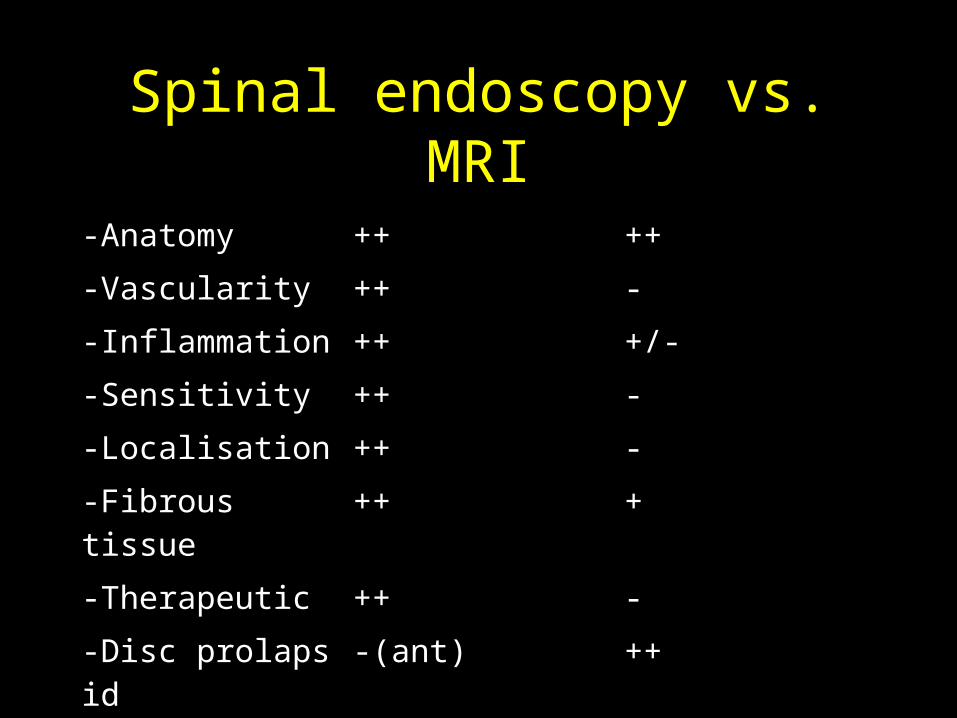
Spinal endoscopy vs. MRI
-Anatomy ++ ++
-Vascularity ++ -
-Inflammation ++ +/-
-Sensitivity ++ -
-Localisation ++ -
-Fibrous tissue ++ +
-Therapeutic ++ -
-Disc prolaps id -(ant) ++
-Canal size +/- ++

NormalNormal1
Perineural adhesions (7) + inflammation (6)
Normal9
Perineural adhesionsPerineural adhesions10
EpiduroscopyMRIPatients
(20)
Geurts et al, Region Anesth Pain Med 2002, 27, 343-352
Applications – Diagnostical Features

Diagnostical featuresEpiduroscopy vs. MRI
• Heavner 2009: Pain Practice: Incidence and severity of epidural fibrosis after back surgery: an endoscopic study
• Epiduroscopy: 95% fibrosis-MRI 16%fibrosis
• Concordant pain with fibrosis 84%

Applications – Therapeutic Features
• Targeted application of therapeutical agents, e.g.,• anti-inflammatory agents• analgesics• LA
• Diluting inflammatoy mediators
• Removal of harmful epidural contents, e.g.,• EPIDURAL FIBROSIS (mechanical/laser/coablation)• drain cysts ( case report)• foreign bodies, e.g., torn epidural/spinal catheters ( case
reports)

In- & Exclusion criteria
• Inclusion criteria
• refractory lumbosacral radicular pain
not responding to conservative measures
or other minimal invasive techniques
• dermatome-like radiation pattern
• VAS leg > VAS back
• VAS leg > 4,0
• Spinal stenosis
• Exclusion criteria
• progressive signs
• coagulopathy
• infection
• increased intracranial pressure
• space-occupying CNS processes
• cerebrovascular disease
• pregnancy
• manifest bladder & bowel dysfunction
• sensory disturbances S2-S4
• renal insufficency
• cancer, allergy, language problems, etc.

Technique/Materials
Epi-C polyDiagnostO.D. 2.4 mm
BIOMET EBI-Vue CathO.D. 2.7 mm
MyelotecO.D. 2.7 mm/3,0mm
AND OTHERS….

procedure
• In hospital• Diagnostic• Therapeutic• Neural flossing

Developments 2010
• Resascope
• 4 Directions• Extra lumen• Adhesiolysis with tools (
foggerty/resaflex)


Complications & Adverse Effects
• infection
• epidural hematoma
• retinal hemorrhage
• nerve root damage
• dural perforation & postpuncture headache
• inadvertent spinal injection of medication
• increase of preexisting pain
• pain at catheter insertion place (sacral hiatus)

Complications & Adverse Effects
• infection
• epidural hematoma
• retinal hemorrhage
• nerve root damage
• dural perforation & postpuncture headache
• inadvertent spinal injection of medication
• increase of preexisting pain
• pain at catheter insertion place (sacral hiatus)


Systematic review of effectiveness and complications
of adhesiolysis (2009)• Is spinal endoscopy superior over
standard therapy?:• Superior over epidural steroid injections,
especially after failed percutaneous adhesiolysis, and in lumbar spinal stenosis.
Systematic review of effectiveness and complications
of adhesiolysis (2009)• Strong evidence short and long term
effect of spinal endoscopy in radicular pain
• Moderate effect in spinal stenosis

Literature
Study RA/P No. <3mn 3mn 6mn 12m St<3 Lt>3
Manc2005
RA,DB
33 33%/90%
0%/80%
0%/56%
0%/48%
P P
Igar 2004
P 5/8 Si SI Si Si P P
Geur2002
P 20 68% 68% 63% 46% P P
Richa2001
P 34 Si Si Si Si P P
Manc1999
P 60 100% 75% 40% 22% P P
Manc2000
P 85 100% 77% 52% 21% P P
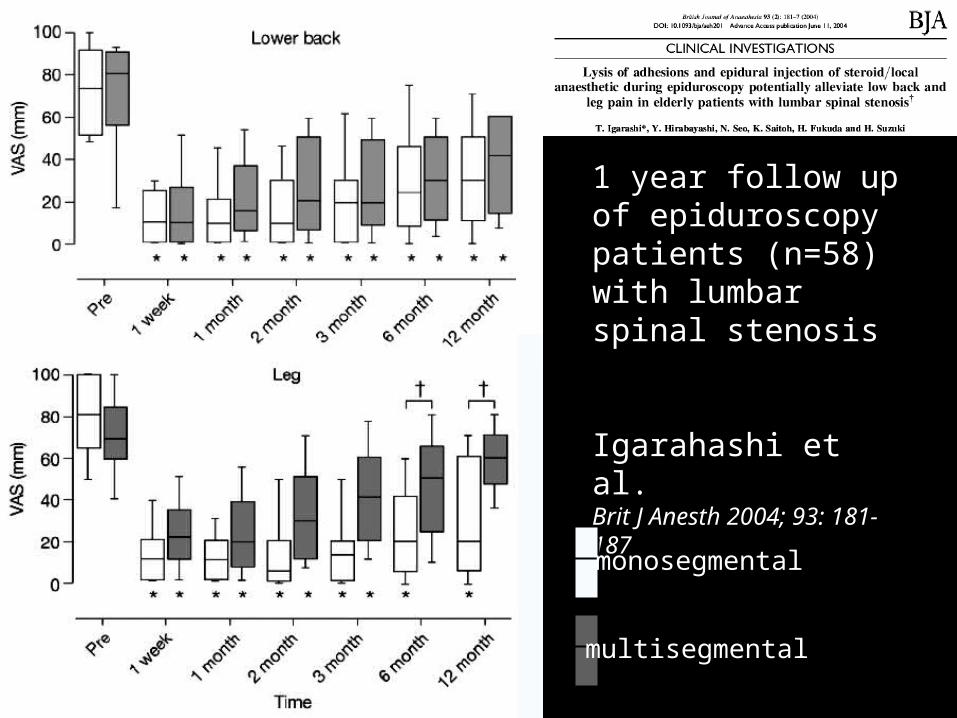
1 year follow up of epiduroscopy patients (n=58) with lumbar spinal stenosis
Igarahashi et al. Brit J Anesth 2004; 93: 181-187
monosegmental
multisegmental
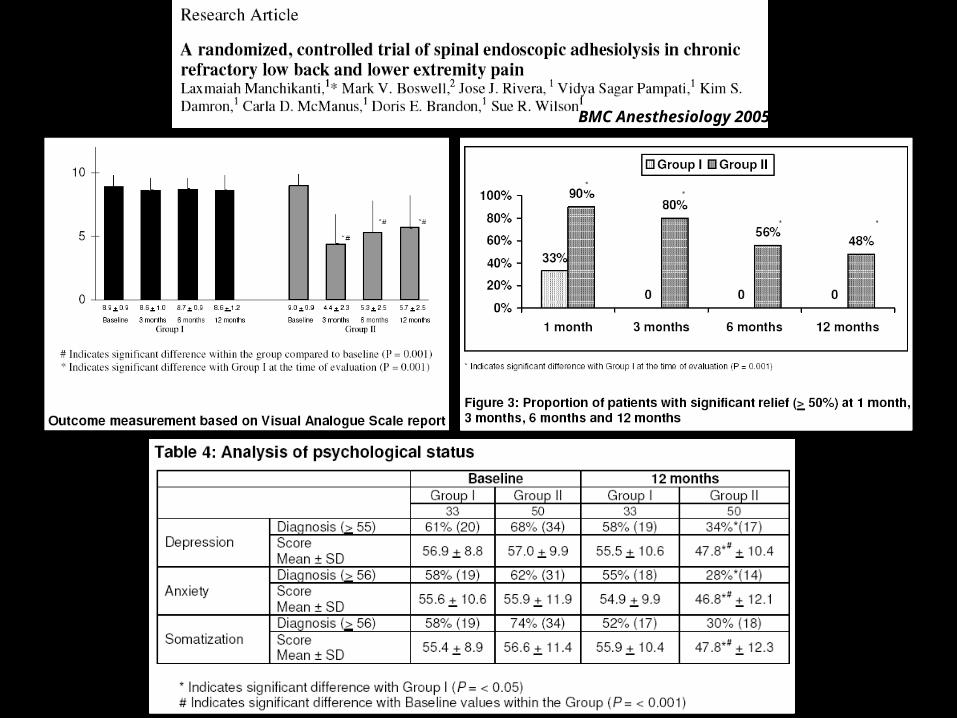
BMC Anesthesiology 2005

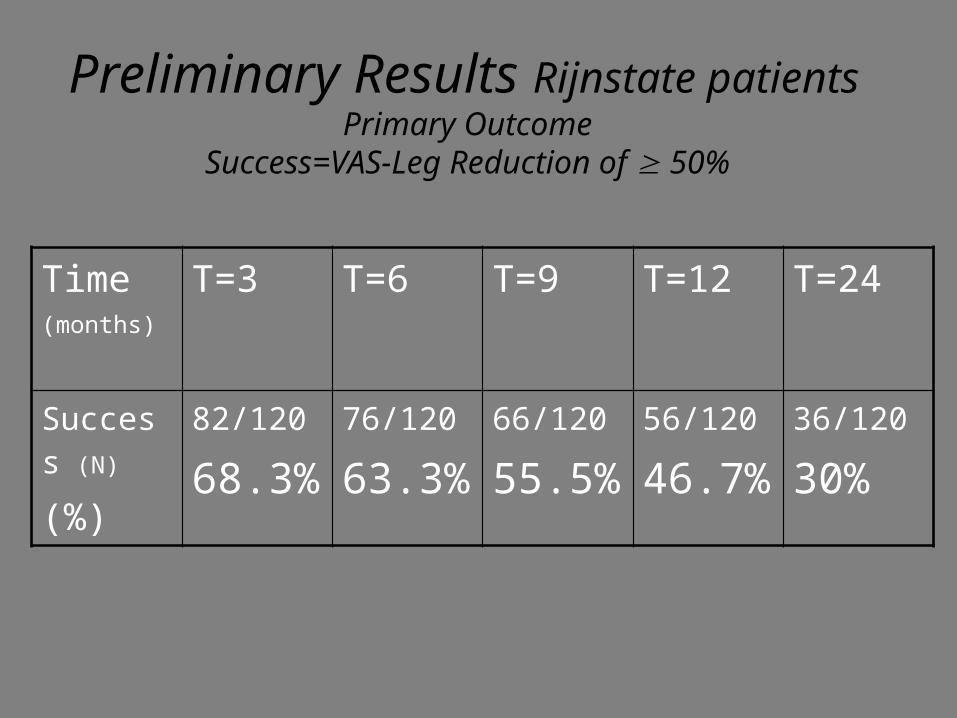
Time(months)
T=3 T=6 T=9 T=12 T=24
Success (N)
(%)
82/120
68.3%76/120
63.3%66/120
55.5%56/120
46.7%36/120
30%
Preliminary Results Rijnstate patients
Primary OutcomeSuccess=VAS-Leg Reduction of 50%

* Richardson J, Kallewaard JW, Groen GJ (2005) Spinal endoscopy for chronic sciatica. Br J Anaesth 95: 275-276
Caudal epidural placement of steroid and spinal endoscopic placement of steroid are effective in patients with sciatica of 6-18 months with superior but not significantly superior results in the caudal epidural group
Comment*• In their study none of the patients had undergone back surgery in contrast
to other studies
• In their study group very little scar tissue; in only 3pt adhesiolysis is
performed
• Relatively short symptom duration compared to other studies (max 18mnth)

Lanset study
• 2002 foundation• Dutch quality system• 15 licensed hospitals• 1 hospital development centre ( Alysis)• Supported by government ( ZN/CVZ)

Protocol
• indications• in-,
exclusioncriteria• treatment per
protocol• technique/materials• classification &
registration of data• number of
procedures• psychometric tests
• training hands on• informed consent• follow up• adv. eff./
complications• data ownership• feedback of results &
implementation (pilots)
• company independence
Conclusions I• Spinal endoscopy has strong evidence for short term relief and
moderate evidence for long term relief
• These results seems to be better compared to classic epidural
steroid injections and effective where percutaneous
adhesiolysis fails.
• The benefits of therapeutic spinal endoscopy seems to be time-
limited (note: results of re-do procedures produce the same results in most patients)
• Only one RCT setting so figures are only a strong indication

Conclusions 2: further research
LANSET• 2 year follow up 500 patients ( results 2009)• 15 hospitals multicentre study ( 2006-2009)• Prospective observational study 1000 patients
(started)• RCT• Quality control
Conclusions 3
• Technique development!!!!!• Tools ( resaflex; laser etc.)
• 2007: start of European network• We need to work together!!
Discussion
• Which place in the algorithm of treatment of radicular pain???
• Last option vs. early treatment
• We need more RCT’s
Anesthesiological Treatments
Inhibition of excitation & Excitation of inhibition & Conduction block
Are you ready?
Here I come...!
Spinal endoscopy is not THE solution,
but might be A solution

Thank You!
Literature 2009-2010
• Praktische richtlijnen Anesthesiologische pijnbestrijding (may 2009) ISBN: 978-90-77411-04-09
• Epiduroscopy: G Schutze ( ISBN: 978-3-540-87544-4)