epidemiology therapeutic management of carpal...
TRANSCRIPT

1Evans RB, carpal tunnel lecture, 2014
Therapeutic Managementof
Carpal Tunnel Syndrome
Roslyn B. Evans, Roslyn B. Evans, OTR/L, CHTOTR/L, CHT
Philadelphia: DK LecturePhiladelphia: DK Lecture20142014
EpidemiologyEpidemiology> morbidity than any other illness> morbidity than any other illness99 per 100,00099 per 100,00010% general population10% general populationMost common surgery in US… Most common surgery in US… 500,000 per year 500,000 per year
Most common Most common dxdx txtx ASHTASHTProfound economic impact > 2 Profound economic impact > 2 billion per yearbillion per year
Medline SearchMedline Searchhttp:www.ncbi.nlm.nih.gov/entrez http:www.ncbi.nlm.nih.gov/entrez
Unlimited Unlimited articlesarticles8,615 Oct 20148,615 Oct 201430 minutes?30 minutes?
rbe5
Controversy in the LiteratureControversy in the Literature
CauseCauseTechniques of Techniques of evaluationevaluationResults with Results with conservative careconservative careTechnique of Technique of surgerysurgeryValue of postValue of post--operative careoperative care
Effect of occupationEffect of occupationon CTS…on CTS…passionate debate!passionate debate!
Substantiating Our InterventionsSubstantiating Our Interventions
Calling for evidenceCalling for evidence––Insurance Insurance
CompaniesCompanies––Managed care Managed care
networksnetworks––PatientsPatients
RBE18
What is Evidence Based Practice?What is Evidence Based Practice?The integration of best research evidence The integration of best research evidence with clinical expertise and patient values with clinical expertise and patient values SackettSackett et al. 2000et al. 2000
The practice of The practice of EBP EBP consists of:consists of:Formulated clinical questionFormulated clinical questionSystematic review of literatureSystematic review of literatureCritical appraisalCritical appraisalApplication for patientsApplication for patientsPerformance reviewPerformance review
rbe9

Slide 3
rbe5 In Medline search 12/02 with the key words evidence based practice and carpal tunnel syndrome, only
2 papers came up...both on acupunhcture, NIH consensus statementRos Evans, 2/23/2003
Slide 5
RBE18 Be careful how you write this up...study on knee arthroscopy demonstrated that it was not effective as
no evidence based outcomes....now govt is looking into denying claims for medicare, etc and other
insurance companies will follow.Roslyn Evans, 3/1/2003
Slide 6
rbe9 Move is on from opinion based education to evidence based education.the quality or research evidence
available, the reliability of the evidence, the utility of the evidence, how valid is the evedence, how
reliable....this was a plot on the part of the program committee to make me realize how bad my
research is, and to reinforce my thoughts about being put out to pasture....however we can take hope
in the fact that there are levels of research depending on quality...1 to 4 (see MacDermid)...back to
levedl 3. Ros Evans, 2/23/2003

2Evans RB, carpal tunnel lecture, 2014
MetaMeta--analysisanalysis
A statistical method for combining the A statistical method for combining the results of available research studies results of available research studies to increase statistical powerto increase statistical powerThe steps of metaThe steps of meta--analysis are:analysis are:
Identification of questionIdentification of questionSearch and selection of trialsSearch and selection of trialsAnalysisAnalysis
HinotsuHinotsu S, S, AkazaAkaza. . GanGan To Kagaku To Kagaku RyohoRyoho20022002
The Problem: The Problem: Inadequate Outcome Inadequate Outcome Measures and ReportingMeasures and Reporting
MetaMeta--analysis is only feasible if RCT’s are analysis is only feasible if RCT’s are clinically clinically homogeneous:homogeneous:
Patient populationPatient populationInterventionsInterventionsComparisonsComparisonsOutcomesOutcomesTiming of followTiming of follow--up measurementup measurement
–– GerritsenGerritsen AAM. et. al. Enabling MetaAAM. et. al. Enabling Meta--Analysis Analysis in Systematic Reviews on Carpal Tunnel in Systematic Reviews on Carpal Tunnel Syndrome. JHS 2002.Syndrome. JHS 2002.
rbe10
Clinical ExposureClinical Exposureconflicting or limiting evidenceconflicting or limiting evidence
Little evidence on the Little evidence on the reliability, validity, and reliability, validity, and responsiveness to change responsiveness to change with current non surgical with current non surgical treatments for CTStreatments for CTSStudy techniques and Study techniques and reporting of results are not reporting of results are not homogeneoushomogeneous–– Metaanalysis:Gerristen2002Metaanalysis:Gerristen2002–– SchadeSchade; 2008,Scangas ; 2008,Scangas 20082008
MetaMeta--analysisanalysisConservative Treatment CTSConservative Treatment CTS
GerritsenGerritsen AA et al. J AA et al. J NeurolNeurol 20022002Short term relief:Short term relief:
Diuretics, pyridoxine, nonDiuretics, pyridoxine, non--steroidal antisteroidal anti--inflammatoriesinflammatories, yoga, laser, yoga, laser--acupuncture ineffective acupuncture ineffective (conflicting evidence)(conflicting evidence)
Efficacy of ultrasound and oral steroids Efficacy of ultrasound and oral steroids (conflicting evidence)(conflicting evidence)SteriodSteriod injection effective injection effective (limited(limited evidence).evidence).
Long term relief:Long term relief:Efficacy of ultrasound Efficacy of ultrasound (limited evidence)(limited evidence)Splinting is less effective than surgerySplinting is less effective than surgeryLittle know about efficacy of conservative Little know about efficacy of conservative txtx
Conservative ManagementConservative ManagementLittle is known about the efficacy of Little is known about the efficacy of most most conservative treatmentsconservative treatments–– GerritsenGerritsen AA, 2002, AA, 2002, metameta--analysisanalysis
Support for therapySupport for therapy–– Level IV; case series with no controlsLevel IV; case series with no controls–– Level V; expert opinion without critical Level V; expert opinion without critical
appraisal or bench appraisal or bench researchresearch–– Splinting, US, nerve gliding, carpal bone Splinting, US, nerve gliding, carpal bone
mobs, magnets, yoga. mobs, magnets, yoga. MacDermid 2004MacDermid 2004
Surgical versus NonSurgical versus Non--Surgical Surgical Treatment for CTS. Treatment for CTS.
Verdugo Verdugo et al. et al. Cochrane Database Cochrane Database SystSyst Rev Rev 2002/ 20082002/ 2008
Surgery more effective Surgery more effective Significant number of patients treated Significant number of patients treated medically will go on to surgerymedically will go on to surgeryRisk of reoperation low Risk of reoperation low Unclear if mild Unclear if mild sxsx can be treated with can be treated with splints and injectionsplints and injection
rbe11

Slide 8
rbe10 Possible solutions to the problems of clinical heterogenity of outcome measures and inadequate
reporting of results for randomized controlled trials (RCT's) on CTS are presented.Meta-analysis was
impeded for 2 reviews on conservative and operative management of CTS. To resolve the problem of
clinical heterogenity of the outcomes there should be consensus on the validated outrcomes that should
be used for CTS. Ros Evans, 2/23/2003
Slide 12
rbe11 Only one randomized controlled trial found. 22 female patients...11 treated with surgery, 11 with
splinting and of those 8 of 11 required operation, none of operated in first group were reoperated at
one year. Ros Evans, 2/23/2003
3Evans RB, carpal tunnel lecture, 2014
Evidence Based MedicineEvidence Based Medicinefor Treatment of CTSfor Treatment of CTS
RCT’s; Systematic ReviewsRCT’s; Systematic ReviewsSurgery most effective Surgery most effective txtx
Cochrane Database Cochrane Database SystSyst Rev 2002Rev 2002AssmusAssmus 2007; 2007; AAOS 2008AAOS 2008Uchiyama J Ortho Uchiyama J Ortho SciSci: 2010: 2010
OCTR preferredOCTR preferred–– Systematic review of RCT’sSystematic review of RCT’s–– GerritsonGerritson 20012001 ; Uchiyama 2010; Uchiyama 2010
Surgical Options for CTSSurgical Options for CTS
Cochrane Database Cochrane Database SSystyst ReviewReview–– 20142014–– VasiliadisVasiliadiset alet al
–– ECTR vs OCTRECTR vs OCTR–– Low level evidence/no significant differenceLow level evidence/no significant difference–– ECTR associated with less minor ECTR associated with less minor
complication, no difference majorcomplication, no difference major–– ECTR RTW 8 days soonerECTR RTW 8 days sooner
Guidelines Guidelines DxDx and and TxTx 20072007
Evidence Based Evidence Based ssupradisciplinaryupradisciplinaryguidelinesguidelines–– Important: Important: accurate history: clinical tests, accurate history: clinical tests,
EMG, NCSEMG, NCS–– Optional: Optional: radiography, MRI, USradiography, MRI, US
German SocietiesGerman Societies–– AssmusAssmus et al. 2007et al. 2007
AAOS 2007, 2008AAOS 2007, 2008EBM Guidelines for EvaluationEBM Guidelines for EvaluationApprovedApproved–– Patient historyPatient history
Physical examPhysical examSensory testSensory testMotor testMotor testProvocative testingProvocative testing
–– Discriminatory Discriminatory tests for tests for alternate alternate dxdx
–– EMG, NCSEMG, NCS
Not approvedNot approved––MRIMRI––CAT scanCAT scan––Pressure Pressure
sensorisensori--motor motor devices in wrist devices in wrist or handor hand
AAOS 2009AAOS 2009
Conservative optionsConservative options–– Recommend 9 guidelines for Recommend 9 guidelines for txtx CTSCTS–– Local steroid injectionLocal steroid injection–– Oral steroidsOral steroids–– UltrasoundUltrasound
CTR best option!CTR best option!––level I evidencelevel I evidence
Adherence AAOS UE CPGAdherence AAOS UE CPGMatzonMatzon et al. et al. OrthopaedicsOrthopaedics 20132013
Members of ASSH Members of ASSH do not universally do not universally adhere to the AAOS CLINICAL PRACTCE adhere to the AAOS CLINICAL PRACTCE GUIDELINES FOR CTSGUIDELINES FOR CTS–– 53% wait recommended time before operating53% wait recommended time before operating–– 32% always order 32% always order electodiagnosticelectodiagnostic testingtesting–– 30% splint PO30% splint PO
Followed: Followed: 98% nighttime splinting;98% nighttime splinting;85% corticosteroid injection85% corticosteroid injection

4Evans RB, carpal tunnel lecture, 2014
Practice patterns: 25 year perspectivePractice patterns: 25 year perspectiveLeinberryLeinberry et al JHS Am 2012et al JHS Am 2012
PreoperativelyPreoperatively–– Increase use splint, corticosteroid injectionsIncrease use splint, corticosteroid injections–– TxTx nonnon--operatively longeroperatively longer–– Narrowed surgical indicationsNarrowed surgical indications
PostPost--operativelyoperatively–– Use tourniquetsUse tourniquets,, corticosteroids lesscorticosteroids less–– Place deep sutures less oftenPlace deep sutures less often–– Decrease concomitant proceduresDecrease concomitant procedures–– Orthotic use and time decreasedOrthotic use and time decreased
CTS CTS DxDx and and TxTx::A Survey of members of the ASSHA Survey of members of the ASSH
Lane et al JHS AM 2014/ SeptLane et al JHS AM 2014/ Sept
AAOS 2007AAOS 2007--2009 developed 2009 developed CClinical linical Practice Guidelines/literature reviewPractice Guidelines/literature review–– Lack strong evidence; recommendations: Lack strong evidence; recommendations:
strong, weak, controversialstrong, weak, controversial
Survey ASSH membersSurvey ASSH members–– 72% operate with +72% operate with +hxhx/exam;+steroid injection/exam;+steroid injection–– 47% EDX not needed if above +47% EDX not needed if above +–– 79% order EDX based on CPG/79% order EDX based on CPG/–– 57% order EDX for medical57% order EDX for medical--legal implicationslegal implications
Why is this most common of all treated Why is this most common of all treated disorders in the upper extremity the disorders in the upper extremity the subject of so much controversy and subject of so much controversy and research?research?
Experience teaches that with a Experience teaches that with a knowledgeable therapist and skilled knowledgeable therapist and skilled surgeon is easy to diagnose, operate, and surgeon is easy to diagnose, operate, and bring to functional recovery.bring to functional recovery.
Do We Know What We Think Do We Know What We Think We Know?We Know?
EvaluationConservative ManagementSurgical ManagementPostoperative ManagementReturn to Work
Well ….what do Well ….what do we know about we know about carpal tunnel?carpal tunnel?
AnatomyAnatomyInelastic conduitInelastic conduit9 flexor tendons9 flexor tendonsMedian nerve, Median nerve, anterior portion anterior portion directly under TCLdirectly under TCLVarying Varying synoviumsynoviumFloor: carpal bones Floor: carpal bones Roof: TCL Roof: TCL PL inserts into the PL inserts into the TCLTCL
Carpal canal tendons excised

5Evans RB, carpal tunnel lecture, 2014
Tissue Fluid pressures in CTTissue Fluid pressures in CT2.5 mmHg in normal subjects2.5 mmHg in normal subjects
32 mmHg in patients with 32 mmHg in patients with dxdx of CTSof CTS
> 30mmHg applied over time induce nerve > 30mmHg applied over time induce nerve damagedamage
>50>50--60mmHg: complete block of sensory 60mmHg: complete block of sensory 1010--30 min before motor conduction30 min before motor conduction
Increase in Tissue Pressure:Increase in Tissue Pressure:CausesCauses
Decrease:Decrease:TransectionalTransectionalArea Area
--OROR--Increase: Increase: Volume Volume of Contentsof Contents
Carpal Tunnel with Tendons Excised
Increased Increased IntratunnelIntratunnel Pressures:Pressures:CausesCauses
Anatomic: CSA Anatomic: CSA vsvs ContentsContentsExternal ForcesExternal ForcesAltered Altered physiologyphysiologyMicrocirculationMicrocirculationAlterations in Alterations in Fluid BalanceFluid Balance
Median Nerve Fascicles
Increase in Critical Levels of Increase in Critical Levels of Tissue Pressure Tissue Pressure : : ResultsResults
Change in Change in intraneuralintraneuralmicrocirculationmicrocirculationAlterations in vascular Alterations in vascular permeabilitypermeabilityAlterations in nerve fiber Alterations in nerve fiber structurestructureNerve edemaNerve edemaRestricted tissue glidingRestricted tissue glidingDeterioration of nerve functionDeterioration of nerve function
Clinical Picture:Clinical Picture:Decreased sensibility, Decreased sensibility, > long finger,> long finger,pain, soft edema, flexor pain, soft edema, flexor inflammationinflammationmotor loss motor loss opponensopponens
Median nerve compression CT
Opponens atrophy
Elevated intraElevated intra--carpal pressurescarpal pressures
Anatomical compressionAnatomical compressionInflammatory , neuropathic conditionsInflammatory , neuropathic conditionsMechanical forcesMechanical forcesObesityObesity

6Evans RB, carpal tunnel lecture, 2014
Increase in CTP:Increase in CTP: Altered physiologyAltered physiology
NeuropathicNeuropathicDiabetes:Diabetes: no correlation incidence no correlation incidence Lee et al Lee et al IntInt J Rheum Dis 2014J Rheum Dis 2014alcoholismalcoholism
Inflammatory Inflammatory Rheumatoid arthritisRheumatoid arthritisGoutGoutNonNon--specific specific tenosynovitstenosynovits
Alterations fluid balanceAlterations fluid balancePregnancyPregnancyMenopauseMenopauseThyroid: Thyroid: modest correlation, meta modest correlation, meta analysis:analysis: ShiraShira: Muscle: Muscle--Nerve 2014Nerve 2014
Increase in CTPIncrease in CTPVariables Influenced by Variables Influenced by
Conservative ManagementConservative Management
PosturePostureWrist, finger, thumb, forearm positionWrist, finger, thumb, forearm position
Tendon load/muscle activityTendon load/muscle activityPalmaris Longus, FDP, FDS, FPL, Palmaris Longus, FDP, FDS, FPL, LumbricalsLumbricals
External forcesExternal forcesApplied external pressure, vibrationApplied external pressure, vibration
The effect of low and high velocity tendon The effect of low and high velocity tendon excursion on excursion on tthe mechanical properties of he mechanical properties of
human cadaver SSCThuman cadaver SSCTFiliusFilius et al et al J J OrthopOrthop Res Res 20142014
Fibrosis Fibrosis subsynovialsubsynovial connective tissue in connective tissue in CT most common histologic finding in CTCT most common histologic finding in CTLowLow--velocity tendon excursions can velocity tendon excursions can irreversibly damage SSCTirreversibly damage SSCTIncreasing velocity increases fibrosis Increasing velocity increases fibrosis SSCT, more likely to break than stretchSSCT, more likely to break than stretch
Risk factors: Obesity/SexRisk factors: Obesity/SexBody Mass IndexBody Mass Index––>29 2.5X greater>29 2.5X greater
than < 20 BMIthan < 20 BMI
––> >10 pounds> >10 poundsFemaleFemaleSquare WristsSquare Wrists
Aerobic activity and fitness should be stressed
MetaanalysisMetaanalysis for the Evaluation of Risk for the Evaluation of Risk Factors for CTS: Factors for CTS: General FactorsGeneral Factors
SpahnSpahn G et al 2012G et al 2012
CTS prevalence 10.6%CTS prevalence 10.6%Female patientsFemale patientsIncrease in age (40Increase in age (40--60 years)60 years)Overweight or obesityOverweight or obesityMore frequent dominant handMore frequent dominant hand“non“non--white race”white race”Diabetes/alcoholismDiabetes/alcoholism
MetaanalysisMetaanalysis for the evaluation of risk for the evaluation of risk factors for carpal tunnel syndrome Part II.factors for carpal tunnel syndrome Part II.
Occupational Risk Factors Occupational Risk Factors SpahnSpahn et al 2012et al 2012Incidence in working populationIncidence in working population–– 11% workers vs 8% general population11% workers vs 8% general population
Heterogeneity of study designs precludes Heterogeneity of study designs precludes prevalence with any job titleprevalence with any job titleRepetitionRepetitionChronic wrist flexionChronic wrist flexionPower gripPower gripChronic vibration loadChronic vibration load

7Evans RB, carpal tunnel lecture, 2014
Goal of TreatmentGoal of TreatmentDecrease CTPDecrease CTP
NonNon--SurgicalSurgical–– Activity modificationActivity modification–– LumbricalLumbrical block splintingblock splinting–– wrist control splintwrist control splint–– NSAIDS; InjectionNSAIDS; Injection
SurgicalSurgical–– Release TCL, OCTR or ECTRRelease TCL, OCTR or ECTR
Normal Intratunnel PressuresNormal Intratunnel Pressures
2.5 mmHg2.5 mmHg wrist wrist neutralneutral31 mmHg31 mmHg wrist wrist flexionflexion30 mmHg30 mmHg wrist wrist extensionextension>90 mmHg>90 mmHg in CTS in in CTS in wrist flex or wrist flex or extensionextension
Gelberman RH, et al J BJS: 1981Gelberman RH, et al J BJS: 1981
The Effect The Effect ofof
Wrist PostureWrist Posture
The Effect of Wrist PostureThe Effect of Wrist PostureBurke et al 1994; Weiss et al 1995Burke et al 1994; Weiss et al 1995
CT pressure lowest CT pressure lowest with wrist with wrist 22degreesdegrees flexion, flexion, 33degreesdegrees of ulnar of ulnar deviationdeviation2.5 mm Hg2.5 mm Hg wrist wrist neutralneutral3030--40 mm Hg40 mm Hg with with wrist in extensionwrist in extension
lowest
highest
The Effect of Wrist PostureThe Effect of Wrist PosturePL tension on FR with extensionPL tension on FR with extension
Shape of CT changes Shape of CT changes with wrist positionwith wrist position
The Effect of Wrist PostureThe Effect of Wrist Posturewith tendon loadwith tendon load
CTP higher with wrist extension than CTP higher with wrist extension than flexion regardless of loadflexion regardless of load (Keir et al. 1997, (Keir et al. 1997, 2000)2000)
Flexor tendons increase shear forces Flexor tendons increase shear forces on Median Nerve on Median Nerve (Keir, Wells, 1999)(Keir, Wells, 1999)
Extrinsic finger muscles have the Extrinsic finger muscles have the potential to move into the CT with wrist potential to move into the CT with wrist extension extension (Keir and Bach 2000)(Keir and Bach 2000)

8Evans RB, carpal tunnel lecture, 2014
Clinical ImplicationsClinical ImplicationsWrist PositionWrist Position
SplintingSplinting2 degrees wrist 2 degrees wrist flexionflexion3 degrees ulnar 3 degrees ulnar deviationdeviation
Work and exercise Work and exercise positionposition
NeutralNeutralAvoid wrist extension Avoid wrist extension combined with load combined with load to flexorsto flexors
?
The Effect of Wrist PostureThe Effect of Wrist PostureClinical ImplicationsClinical Implications
70 mm Hg in wrist extension70 mm Hg in wrist extension
Clinical ImplicationsClinical ImplicationsCombined Wrist and Finger PosturesCombined Wrist and Finger Postures
Flexor Muscle Flexor Muscle Incursion Incursion
Keir, Bach 2000Keir, Bach 2000
Incursion of flexor Incursion of flexor muscles into the muscles into the carpal tunnel with carpal tunnel with wrist extension is a wrist extension is a potential cause of potential cause of increased carpal increased carpal tunnel pressuretunnel pressure
The use of flexor The use of flexor muscles should be muscles should be avoided when the avoided when the wrist and fingers are wrist and fingers are extendedextended
RBE17
The Effect The Effect ofof
Finger PostureFinger Posture
The Effect of Finger PostureThe Effect of Finger PostureThe Effect of Finger PostureThe Effect of Finger Posture
Decreasing Carpal Tunnel PressuresDecreasing Carpal Tunnel PressuresLumbrical Block SplintingLumbrical Block Splinting
Wrist 0 degrees, MP 0-20 flex, IP’s free; decreases long tendon excursion, lumbrical entry into CT

Slide 45
RBE17 The most distal muscle fibres from the deep and superficial finger flexors were measured relative to the
pisiformbone in 8 cadaveric specimens The mean distances from the pisiform were 9.3 for the FDP, and
4.9mm for the FDS respectively. The excursions expected with wrist extension indicate that many
muscles have the potential to enter the carpal tunnel, especially those within 5 mm of the pisiform
bone.Roslyn Evans, 3/1/2003

9Evans RB, carpal tunnel lecture, 2014
The Effect of Finger PostureThe Effect of Finger Posture
Four lumbricals Four lumbricals originate off FDP originate off FDP tendons tendons Rest distal to CT Rest distal to CT with digits in with digits in extensionextensionRest within CT Rest within CT with fingers with fingers actively flexedactively flexed
The Effect of Finger PostureThe Effect of Finger PostureLumbrical Incursion Lumbrical Incursion Cobb et al 1994Cobb et al 1994
Finger extension:Finger extension:7.8 mm distal CT7.8 mm distal CT
50% finger flexion50% finger flexion14 mm into CT14 mm into CT75% finger flexion75% finger flexion25.5 mm into CT25.5 mm into CT100% finger flexion:100% finger flexion:30 mm into CT30 mm into CT
The Effect of Finger PostureThe Effect of Finger PostureMRI of CT at Level of Hook of HamateMRI of CT at Level of Hook of Hamate
T
HCT
The Effect of Finger PostureThe Effect of Finger PostureCTP with Intact LumbricalsCTP with Intact Lumbricals
Finger PositionFinger Position Mean PressureMean Pressure
Digits extendedDigits extended 299 mm Hg299 mm Hg50% fist50% fist 313 mm Hg313 mm Hg75% fist75% fist 326 mm Hg326 mm Hg100% fist100% fist 361 mmHg361 mmHg
No pressure change any position with excised No pressure change any position with excised lumbricalslumbricals
Greatest change between 75 and 100% finger flexionGreatest change between 75 and 100% finger flexionCobb et al, JHS 1995Cobb et al, JHS 1995
The Effect of Finger PostureThe Effect of Finger Postureplotted with and without lumbricalsplotted with and without lumbricals
Cobb et al.
The Effect of Finger PostureThe Effect of Finger PostureFinger FlexionFinger Flexion
Alters fat compressionAlters fat compression
Flattens and displaces Flattens and displaces median nerve median nerve in the in the presence of lumbrical presence of lumbrical musclesmuscles
Pressure deep and Pressure deep and superficial tendonssuperficial tendons
Ham SJ et al. JHS 21A, 1996Ham SJ et al. JHS 21A, 1996

10Evans RB, carpal tunnel lecture, 2014
UltrasonographicUltrasonographic median nerve changes under median nerve changes under tendon gliding exercise in patients with CTS tendon gliding exercise in patients with CTS
and healthy controlsand healthy controls
HorngHorng YS et al; JHT YS et al; JHT 20142014
Median nerve Median nerve compresses in compresses in fist position in fist position in both patients with both patients with CTS and healthy CTS and healthy controlscontrols
73 with CTS73 with CTS53 healthy controls53 healthy controlsSignificant changes Significant changes in cross sectional in cross sectional area of median area of median nerve when moving nerve when moving from straight to from straight to hook and hook to hook and hook to fist positionfist position
Clinical Significance of StudiesClinical Significance of StudiesDecreasing CTP with Finger PositionDecreasing CTP with Finger Position
In some cases:In some cases: Limit Limit 50% finger flexion, MP’s 50% finger flexion, MP’s 0 to 20 degrees0 to 20 degrees
Well developed Well developed lumbricals; + Bergerlumbricals; + BergerFlexor synovitisFlexor synovitisTriggering digitsTriggering digits“Compulsive gripper”“Compulsive gripper”
MP’s 45 degreesMP’s 45 degreesKeir et al. 1998 Keir et al. 1998
Clinical Significance of StudiesClinical Significance of StudiesDecreasing CTP with Finger PositionDecreasing CTP with Finger Position
Alter work postures Alter work postures with repetitive with repetitive gripping and gripping and sustained intrinsic sustained intrinsic contractioncontractionStrengthen with Strengthen with isometric flexion at isometric flexion at 50% rather than 50% rather than repetitive flexion into repetitive flexion into DPCDPC
The Effect of The Effect of Combined Combined
Finger and Wrist Finger and Wrist Posture with Posture with
LoadLoad
Combined Effect of Posture and LoadCombined Effect of Posture and Load
Muscle load elevates CTP above critical Muscle load elevates CTP above critical pressures pressures (defined greatest to lowest)(defined greatest to lowest)
PL greatest in wrist extensionPL greatest in wrist extensionLoad to digital flexors with wrist Load to digital flexors with wrist flexionflexionFPL with wrist in ulnar deviationFPL with wrist in ulnar deviationForceful grip with wrist in ulnar Forceful grip with wrist in ulnar deviationdeviation
Keir PJ, et al. JHS 22A; 1997Keir PJ, et al. JHS 22A; 1997
Highest: PL tension on Flexor Retinaculum
2.5x< than withwrist neutral
Pressures 2x > with FPL load in UD
Forceful grip in wrist UD

11Evans RB, carpal tunnel lecture, 2014
Pressure Changes During Pressure Changes During Activity in Normal HandsActivity in Normal HandsNormal CT Pressure 32Normal CT Pressure 32--44 mmHg44 mmHg
Power fist/ hold small object: +223 mm HgHgWrist extension:Wrist extension: +77mm Hg+77mm HgWrist flexion:Wrist flexion: +56 mm Hg+56 mm HgHold object 10.5 cm:Hold object 10.5 cm: + 46 mm Hg+ 46 mm HgIsometric finger flexion:Isometric finger flexion: + 41 mm Hg+ 41 mm Hg
Seradge et al 1995 Seradge et al 1995
The Effect of Finger Tip MotionsThe Effect of Finger Tip Motions
Tendon force in the CT are not Tendon force in the CT are not proportional to finger tip force during proportional to finger tip force during rapid tapping as with key strokingrapid tapping as with key strokingTendon tension continues to increase Tendon tension continues to increase throughout keystroke impactthroughout keystroke impactForces are cumulative and remain Forces are cumulative and remain elevated longer than the keystroke elevated longer than the keystroke forceforce
Dennerline et al. 1999Dennerline et al. 1999
The Effect of The Effect of Thumb Thumb PosturePosture
The Effect of Thumb PostureThe Effect of Thumb Posture
The effect of thumb CMC joint inflammation, The effect of thumb CMC joint inflammation, the pull of the opponens on the flexor the pull of the opponens on the flexor retinaculum and sustained intrinsic retinaculum and sustained intrinsic contraction can increasecontraction can increase CT pressureCT pressure
Lumbrical Pinch TestLumbrical Pinch Test
Firmly pinch paper between Firmly pinch paper between thumb and distal phalanges thumb and distal phalanges of Index and Long, MP’s 90, of Index and Long, MP’s 90, wrist neutralwrist neutralNumbness Median Nerve 60 Numbness Median Nerve 60 seconds, cramping mid palmseconds, cramping mid palmCorrelates with Median nerve Correlates with Median nerve & lumbrical indentation into & lumbrical indentation into distal CTdistal CT

12Evans RB, carpal tunnel lecture, 2014
Clinical SignificanceClinical SignificanceEvaluate and treat Evaluate and treat CMC joint CMC joint inflammationinflammationMinimize pinch Minimize pinch and grip activitiesand grip activitiesAvoid posture that Avoid posture that combines UD and combines UD and oppositionoppositionIncrease grip size Increase grip size toolstools
The Effect of The Effect of Forearm Forearm PosturePosture
The Effect of Combined Forearm Position The Effect of Combined Forearm Position and MP Angles in Normal Subjectsand MP Angles in Normal Subjects
Position Pronation SupinationPosition Pronation Supination
MP 0 16.6mmHgMP 0 16.6mmHg 53.9 mmHg53.9 mmHg
MP 45 MP 45 11.6 mmHg11.6 mmHg 33.7 mmHg33.7 mmHg
MP 90 19.4 mmHgMP 90 19.4 mmHg 55.2 mmHg55.2 mmHg
Rempel D, et al. JHS 1998Rempel D, et al. JHS 1998
53.9mmHg
16.6mmHg
The effect of Forearm PostureThe effect of Forearm PostureClinical ImplicationsClinical Implications
The Effect of The Effect of External External PressurePressure
The Effect of External ForceThe Effect of External ForceCobb TK, An KN, Cooney WP. JHS 20A, 1995Cobb TK, An KN, Cooney WP. JHS 20A, 1995
External force on the External force on the palm increases carpal palm increases carpal tunnel pressure; the tunnel pressure; the magnitude of magnitude of pressure change is pressure change is dependent on dependent on locationlocation1 kg external force in 1 kg external force in cadaver specimencadaver specimen
Highest overHook of hamateRBE13

Slide 72
RBE13 Flexor retinaculm 103 mmHgRoslyn Evans, 2/16/2003

13Evans RB, carpal tunnel lecture, 2014
Clinical ImplicationsClinical ImplicationsTherapy Induced ProblemsTherapy Induced Problems
Pitfalls of Generic TherapyPitfalls of Generic Therapy
Inability to diagnose Inability to diagnose associated problemsassociated problemsInappropriate splint geometryInappropriate splint geometryApplication of external Application of external pressurespressuresExercise regimens that Exercise regimens that increase intraincrease intra--tunnel tunnel pressurespressures
Early dx is key
Kaplan 1990
Clinical EvaluationClinical EvaluationResponsibility shifts dependent Responsibility shifts dependent
on referral sourceon referral source
Clinical ExaminationClinical Examination
HistoryHistorySymptomsSymptomsClinical exam upper Clinical exam upper quadrantquadrantCT clinical screeningCT clinical screeningPhysical provocative Physical provocative testingtestingDiagnostic testingDiagnostic testing
“I have been coached and I know the symptoms”
Referring Referring DxDx Incorrect or Incorrect or Incomplete, often primary careIncomplete, often primary care
Thumb CMC or other carpal arthritisThumb CMC or other carpal arthritisDe’Quervains, other tendonitisDe’Quervains, other tendonitisTrigger fingersTrigger fingersEpicondylitisEpicondylitis
Double CrushDouble CrushCervicothoracic neuropathyCervicothoracic neuropathyMetabolic neuropathyMetabolic neuropathy
Gold standard??Gold standard??
ElectrodiagnosticElectrodiagnostic studies recommended studies recommended by multidisciplinary German Societies by multidisciplinary German Societies based on evidence based reviews 2007based on evidence based reviews 2007Recommended by AAOS Clinical Recommended by AAOS Clinical Guidelines 2008Guidelines 2008--9.9.2014…survey of ASSH members2014…survey of ASSH members–– 47% don’t order if 47% don’t order if hxhx and clinical and clinical evaleval ++–– 57% order for medical57% order for medical--legal reasonslegal reasons

14Evans RB, carpal tunnel lecture, 2014
Guidelines Guidelines DxDx and and TxTx 20072007
Evidence Based Evidence Based ssupradisciplinaryupradisciplinaryguidelinesguidelines–– Important: Important: accurate history: clinical tests, accurate history: clinical tests,
EMG, NCSEMG, NCS–– Optional: Optional: radiography, MRI, USradiography, MRI, US
German SocietiesGerman Societies–– AssmusAssmus et al. 2007et al. 2007
AAOS 2007, 2008AAOS 2007, 2008EBM Guidelines for EvaluationEBM Guidelines for EvaluationApprovedApproved–– Patient historyPatient history
Physical examPhysical examSensory testSensory testMotor testMotor testProvocative testingProvocative testing
–– Discriminatory Discriminatory tests for tests for alternate alternate dxdx
–– EMG, NCSEMG, NCS
Not approvedNot approved––MRIMRI––CAT scanCAT scan––Pressure Pressure
sensorisensori--motor motor devices in wrist devices in wrist or handor hand
Diagnostic Testing CTS…Diagnostic Testing CTS… for most pts with +for most pts with +hxhxand +PE, EDT are not clinically relevant; and +PE, EDT are not clinically relevant;
Graham B. 2008Graham B. 2008
Value of clinical exam:Value of clinical exam:–– RadovikRadoviket al 2014et al 2014
ElectrodiagnosticElectrodiagnostic…searching for …searching for gold standardgold standard
Jordan 2002,Chang 2002Jordan 2002,Chang 2002Resende Resende 20002000Rosenbaum 1999 Rosenbaum 1999
UltrasoundUltrasoundDuncan 1999Duncan 1999Lee 1999Lee 1999
Magnetic Resonance ImagingMagnetic Resonance ImagingZagnoliZagnoli 19991999Andre 1999Andre 1999Jacobson 1999Jacobson 1999KirindienstKirindienst 19981998
“I’ll do it my way”
Peter Amadio 2014Peter Amadio 2014
Brent Graham: Brent Graham: EMG does not add much EMG does not add much to dx of CTS other than to help in to dx of CTS other than to help in prediction of prognosisprediction of prognosis
Patients with abnormal EMG do better Patients with abnormal EMG do better following surgery than those who had following surgery than those who had normal EMG: AAOS guidelinesnormal EMG: AAOS guidelines
Electrodiagnosis of CTSElectrodiagnosis of CTS
Electrodiagnosis is Electrodiagnosis is notnot a useful a useful diagnostic test in patients with clinical diagnostic test in patients with clinical signs of CTSsigns of CTSIn cases of clear cut clinical CTS, In cases of clear cut clinical CTS, electrodiagnosis is not warrantedelectrodiagnosis is not warrantedas a diagnostic test or indicator of as a diagnostic test or indicator of surgical outcome.surgical outcome.Jordan et al 2001Jordan et al 2001
The Value of Diagnostic TestingThe Value of Diagnostic TestingIn Carpal Tunnel SyndromeIn Carpal Tunnel Syndrome
Szabo et al. J Hand Surg 24A 1999Szabo et al. J Hand Surg 24A 1999
“I believe everything he says” RE“I believe everything he says” RE
SensitivitySensitivity SpecificitySpecificityDurkan’s compression 89%Durkan’s compression 89% Hand diagram 76%Hand diagram 76%SW after Phalen’s 83%SW after Phalen’s 83% Tinel’s sign 71%Tinel’s sign 71%Hand Diagram 73%Hand Diagram 73%Night pain 96%Night pain 96%
Electrodiagnostic testing does not improve combo of 4 Electrodiagnostic testing does not improve combo of 4 clinical testsclinical tests

15Evans RB, carpal tunnel lecture, 2014
The Validity of Physical TestingThe Validity of Physical Testingfor CTSfor CTS
DxDx of CTS is clinical and not of CTS is clinical and not neurophysiologicalneurophysiological KitsisKitsis 20022002
Supports clinical testing over NCS, EMSSupports clinical testing over NCS, EMSSzabo 1999; Richter 1999Szabo 1999; Richter 1999
Sensitivity, specificity vary with comparison Sensitivity, specificity vary with comparison subjectssubjectsGerrGerr et al. J Hand et al. J Hand SurgSurg (Br) 1998(Br) 1998
MasseyMassey--WestroppWestropp: : A systematic Review of the Clinical A systematic Review of the Clinical Diagnostic Tests for CTS. JHS 25A, 2000Diagnostic Tests for CTS. JHS 25A, 2000 ..
Clinical Diagnostic TestsClinical Diagnostic Tests
Tinel/PercussionTinel/PercussionVibrometry, 256 cps tuning forkVibrometry, 256 cps tuning forkStatic 2Static 2--point discriminationpoint discriminationPhalen/wrist flexionPhalen/wrist flexionDurkan/carpal compressionDurkan/carpal compressionLumbrical Incursion/BergerLumbrical Incursion/BergerReverse PhalenReverse PhalenSemmesSemmes--Weinstein monofilamentsWeinstein monofilaments
Screen for Proximal CompressionScreen for Proximal Compression
Accessory head of FPL Accessory head of FPL Fibrous bridge between heads of FDSFibrous bridge between heads of FDSBetween humeral and Between humeral and ulnarulnar heads of heads of pronatorpronator teresteresBeneatheBeneathe lacertuslacertus fibrosis; Struthers fibrosis; Struthers ligament; ligament; bicipitalbicipital aponeurosisaponeurosisThoracic outletThoracic outletC6C6--8 8 radiculopathyradiculopathy–– Pratt: J Hand Pratt: J Hand TherTher 2005; 2005; BilecenogluBilecenoglu et al, 2005et al, 2005
Clinical Diagnosis CTSClinical Diagnosis CTSSemmes Weinstein MonofilamentsSemmes Weinstein Monofilaments
Conflicting SupportConflicting SupportLight touch/deep Light touch/deep pressure pressure thresholdsthresholdsSupports use of Supports use of SW SW BellBell--Krotoski 1995Krotoski 1995
Liberal SW kit in Liberal SW kit in confirmed CTS, no confirmed CTS, no utility in diagnosis.utility in diagnosis.Pagel et al 2002Pagel et al 2002
Defines issues with PCBMN, CDN, DN
Clinical Diagnostic Tests CTSClinical Diagnostic Tests CTSLumbrical Provocation TestLumbrical Provocation Test
Hold hand in fist for 1 minute Hold hand in fist for 1 minute to evaluate changes in to evaluate changes in paresthesiaparesthesiaLPT has limited use in LPT has limited use in predicting CTS compared predicting CTS compared with electrodiagnosis and with electrodiagnosis and hand diagram.hand diagram.Karl AI, et al. Arch Phys Med Karl AI, et al. Arch Phys Med Rehabil 2001 Rehabil 2001 (blinded (blinded comparison of 3 diagnostic comparison of 3 diagnostic tests)tests) Berger Test
Carpal Compression Test (CCT)Carpal Compression Test (CCT)
�� Direct pressure on carpal Direct pressure on carpal tunnel and underlying tunnel and underlying median nerve. Highly median nerve. Highly sensitive (87%)and specific sensitive (87%)and specific 90% in diagnosis of CTS 90% in diagnosis of CTS when done with thumb when done with thumb pressure. pressure. Durkan 1991Durkan 1991
Marginal Marginal utility when utility when compared to compared to gold standard gold standard neurophysiolneurophysiologic testing.ogic testing.Kaul MP et al Kaul MP et al Muscle Nerve Muscle Nerve 2001 20012001 2001Not sensitive or Not sensitive or specific for dx specific for dx CTSCTS. Wainner et . Wainner et al 2000al 2000

16Evans RB, carpal tunnel lecture, 2014
Clinical Diagnosis CTSClinical Diagnosis CTSHand Elevation TestHand Elevation Test Ahn DS,2001Ahn DS,2001
Hand elevation can reproduce the Hand elevation can reproduce the symptoms of CTSsymptoms of CTSProspective study in 200 hands diagnosed Prospective study in 200 hands diagnosed with CTS, and control 200 handswith CTS, and control 200 handsUseful provocative testUseful provocative testHand ElevationHand Elevation Phalen’sPhalen’s Tinel’sTinel’s–– Sensitivity:Sensitivity: 75.5%75.5% 67.5% 67.5%67.5% 67.5%–– Specificity: Specificity: 98.5%98.5% 91.0% 90.0%91.0% 90.0%
Clinical Evaluation TestsClinical Evaluation TestsCarpal Tunnel SyndromeCarpal Tunnel Syndrome
Subjective swelling: a new sign for Subjective swelling: a new sign for carpal tunnel syndromecarpal tunnel syndrome
Burke et al. Am J Phys Med Rehab 1999Burke et al. Am J Phys Med Rehab 1999
A new provocative test for CTS: A new provocative test for CTS: Assessment of wrist flexion and nerve Assessment of wrist flexion and nerve compression.compression.
Tetro et al. 1998Tetro et al. 1998
My ApproachMy Approach …… quick screenquick screen
Subjective complaintsSubjective complaintsSemmes Weinstein neutral and after Semmes Weinstein neutral and after Phalen’sPhalen’sTinel’s (percussion)Tinel’s (percussion)Berger (lumbrical incursion)Berger (lumbrical incursion)Durkan’s (external pressure)Durkan’s (external pressure)Soft edema, inflammationSoft edema, inflammationProvocative tests for proximal Provocative tests for proximal compression (forearm, cervical)compression (forearm, cervical)
I will Recommend EMG, NCS,I will Recommend EMG, NCS,Surgical consult ….Surgical consult ….
Nocturnal painNocturnal painDaytime Daytime paresthesiaparesthesiaIncrease Increase sxsx with sustained pinch or gripwith sustained pinch or grip+ provocative tests+ provocative tests–– Phalen’sPhalen’s, Berger, , Berger, Tinel’sTinel’s, , Durkan’sDurkan’s. Pinch . Pinch
Semmes Weinstein > 3.61 Long digitSemmes Weinstein > 3.61 Long digitAtrophy Atrophy opponensopponens
Conservative ManagementConservative Management
Little is known about the Little is known about the efficacy of most efficacy of most conservative treatment conservative treatment optionsoptions
(Gerritsen AA, 2002, meta(Gerritsen AA, 2002, meta--analysis)analysis)
MetaMeta--analysisanalysisConservative Treatment CTSConservative Treatment CTS
Gerritsen AA et al. J Neurol 2002Gerritsen AA et al. J Neurol 2002Short term relief:Short term relief:
Diuretics, pyridoxine, nonDiuretics, pyridoxine, non--steroidal antisteroidal anti--inflammatories, yoga, laserinflammatories, yoga, laser--acupuncture ineffective acupuncture ineffective (conflicting evidence)(conflicting evidence)
Efficacy of ultrasound and oral steroids Efficacy of ultrasound and oral steroids (conflicting evidence)(conflicting evidence)
Steriod injection effective Steriod injection effective (limited(limitedevidence).evidence).
Long term relief:Long term relief:Efficacy of ultrasound Efficacy of ultrasound (limited evidence)(limited evidence)Splinting is less effective than surgerySplinting is less effective than surgery
17Evans RB, carpal tunnel lecture, 2014
Surgical versus NonSurgical versus Non--Surgical treatment Surgical treatment for CTS.for CTS.
Cochrane Database Cochrane Database SystSyst Rev Rev 2002 update 20082002 update 2008
Conclusion? Conclusion?
Surgery more effectiveSurgery more effective than than splintingsplintingFurther research to determine if Further research to determine if surgery better than steroid surgery better than steroid injection for people with mild injection for people with mild sxsx . . Verdugo, et al.Verdugo, et al.
rbe8
Conservative Management CTSConservative Management CTSnothing proven!nothing proven!
NSAIDSNSAIDSCorticosteroid Corticosteroid injection into injection into Carpal TunnelCarpal TunnelMetabolic control Metabolic control other problemsother problemsWeight lossWeight lossSplintingSplinting
Tendon and nerve Tendon and nerve glidingglidingIontophoresisIontophoresisUltrasoundUltrasoundVitaminsVitaminsChanges in Changes in posture and loadposture and loadAerobic exerciseAerobic exercise
AAOS 2009AAOS 2009
Conservative optionsConservative options–– Recommend 9 guidelines for Recommend 9 guidelines for txtx CTSCTS–– Local steroid injectionLocal steroid injection–– Oral steroidsOral steroids–– UltrasoundUltrasound
CTR best option!CTR best option!––level I evidencelevel I evidence
Surgical Options for CTSSurgical Options for CTS
Cochrane Database Cochrane Database SSystyst Review Review 20142014–– VasiliadisVasiliadiset alet al
–– ECTR vs OCTRECTR vs OCTR–– Low level evidence/no significant differenceLow level evidence/no significant difference–– ECTR associated with less minor ECTR associated with less minor
complication, no difference majorcomplication, no difference major–– ECTR RTW 8 days soonerECTR RTW 8 days sooner
Cochrane Database Cochrane Database SSystyst Review 2008Review 2008
Endoscopic Release CTSEndoscopic Release CTSVasiliadisVasiliadis et al et al
Cochrane Database Cochrane Database SystSyst Rev 2014Rev 2014
OCTR and ECTR equally effectiveOCTR and ECTR equally effectiveNo major difference in complicationsNo major difference in complicationsECTR earlier return to work (8 days)ECTR earlier return to work (8 days)ECTR slightly better grip strength, functionECTR slightly better grip strength, functionConclusions limitedConclusions limited–– “High “High risk of bias, statistical imprecision, risk of bias, statistical imprecision,
inconsistency in inconsistency in included studies”.included studies”.
Oral SteroidsOral SteroidsNSAIDSNSAIDS
Short term low dose oral steroids Short term low dose oral steroids are effective for CTSare effective for CTS..
RCTRCTChang MH et al 2002Chang MH et al 2002

Slide 97
rbe8 Only one randomized controlled trial found. 22 female patients...11 treated with surgery, 11 with
splinting and of those 8 of 11 required operation, none of operated in first group were reoperated at
one year. Ros Evans, 2/23/2003

18Evans RB, carpal tunnel lecture, 2014
Local Corticosteroid InjectionLocal Corticosteroid Injection
Greater improvement over placebo at Greater improvement over placebo at one monthone monthSymptom relief beyond one month not Symptom relief beyond one month not demonstrateddemonstratedNo improvement compared to antiNo improvement compared to anti--inflammatory inflammatory txtx and splinting or laser and splinting or laser txtxMarshall et al.Marshall et al. Cochrane Database Cochrane Database SystSystRev 2002; Rev 2002; update 2007update 2007
Local Steroid InjectionLocal Steroid Injection
Gelberman et al. Carpal tunnel syndrome. Gelberman et al. Carpal tunnel syndrome. Results of a prospective trial of steroid Results of a prospective trial of steroid injection and splinting. JBJS. 1980injection and splinting. JBJS. 1980Indexed by American Society for Surgery Indexed by American Society for Surgery of the Handof the Hand22% of 41 patients were symptom free at 22% of 41 patients were symptom free at mean 18 month followmean 18 month follow--up with steroid up with steroid injection and splinting.injection and splinting.High relapse rate with more severe sx; High relapse rate with more severe sx; sx greater than one yearsx greater than one year
The Efficacy of SplintingThe Efficacy of Splinting
Supports the wear of full time neutral wrist Supports the wear of full time neutral wrist splints over night time splinting alone. splints over night time splinting alone. RCTRCT. . Walker et al. 2000Walker et al. 2000
Splinting combined with NSAIDS and Splinting combined with NSAIDS and steroid injection into CTS resulted in steroid injection into CTS resulted in significant improvement.significant improvement. RCT.RCT. Celiker et Celiker et al. 2002al. 2002
OCTR better outcomes than wrist OCTR better outcomes than wrist splinting in patients with CTSsplinting in patients with CTS. . RCTRCTGerritsen et al 2002Gerritsen et al 2002
rbe3
rbe4
The Efficacy of SplintingThe Efficacy of Splinting
Splint that maintains the wrist in neutral Splint that maintains the wrist in neutral position while restraining the digits beyond position while restraining the digits beyond 75% of a full fist would be most effective in 75% of a full fist would be most effective in decreasing carpal tunnel.decreasing carpal tunnel. ApfelApfel et al 2002et al 2002Splint effective in reducing symptoms and Splint effective in reducing symptoms and functional loss.functional loss. RCTRCT. . ManamenteManamente G. et al G. et al 20012001Support for Splinting, RCT.Support for Splinting, RCT. ManenteManente et al et al 20012001No Benefit: No Benefit: LuchettiLuchetti 19981998
Splinting for CTSSplinting for CTSPage et al: Page et al: Cochrane Database Cochrane Database SSystyst Rev 2012Rev 2012
Compare effectiveness of splinting for Compare effectiveness of splinting for CTS with no CTS with no txtx, placebo or another , placebo or another nonsurgical interventionnonsurgical intervention
Limited evidence to support in Limited evidence to support in short termshort termSome benefit over other conservative Some benefit over other conservative txtxStudies evaluated not homogeneousStudies evaluated not homogeneous
The Efficacy of SplintingThe Efficacy of Splinting

Slide 105
rbe3 Ros Evans, 2/23/2003
rbe4 Walker study: Ros Evans, 2/23/2003

19Evans RB, carpal tunnel lecture, 2014
Sleeping PositionsSleeping Positionscervical, shoulder, elbow,cervical, shoulder, elbow,wrist, and in severe cases wrist, and in severe cases the digitsthe digits Ø
Neural Mobilization: limited evidenceNeural Mobilization: limited evidence
Efficacy not clearEfficacy not clear–– Systematic Review: Systematic Review:
Medina et al. 2008Medina et al. 2008
Duration, frequency, Duration, frequency, amplitude not confirmedamplitude not confirmedWalsh Walsh
Excessive strain with Excessive strain with functional activities functional activities may play a role in may play a role in peripheral nerve sx.peripheral nerve sx.
ExerciseExerciseNOPENOPE
Tendon gliding: 67% improvement with Tendon gliding: 67% improvement with sxsxseverity. Not RCT.severity. Not RCT. SeradgeSeradge, et al. 2002, et al. 2002Tendon and nerve gliding: No statistical Tendon and nerve gliding: No statistical improvement in full time splinting vs. full improvement in full time splinting vs. full time splinting with exercise. RCT.time splinting with exercise. RCT. AkalinAkalinet al. 2002et al. 2002Aerobic exercise: Aerobic exercise: sxsx relieved. Not RCT.relieved. Not RCT.Nathan et al. 2001Nathan et al. 2001““nerve excursion may improve axonal transport”nerve excursion may improve axonal transport”
Exercise, mobilization interventions for CTSExercise, mobilization interventions for CTSCochrane Database Cochrane Database SSystyst Rev Rev 20122012
Page et alPage et al
Compare ex and mobs to no Compare ex and mobs to no txtx, , placebo, other nonplacebo, other non--surgical surgical txtxStudies heterogeneousStudies heterogeneousLimited/low quality studiesLimited/low quality studiesNO EVIDENCE TO SUPPPORTNO EVIDENCE TO SUPPPORT
Tendon Gliding Through the CTTendon Gliding Through the CT Manual TherapyManual TherapyNo supportNo support
Carpal Bone MobilizationCarpal Bone MobilizationMedian Nerve MobilizationMedian Nerve MobilizationNo TreatmentNo TreatmentRCT, no difference in tx. RCT, no difference in tx. TalTal--Akabi A, Rushton A. Man Ther Akabi A, Rushton A. Man Ther 20002000

20Evans RB, carpal tunnel lecture, 2014
The Problem with Therapy ToysThe Problem with Therapy Toys
Effect of posture and Effect of posture and loadloadCT pressure < 200 CT pressure < 200 mmHg in full fistmmHg in full fist
What Are They Smoking?What Are They Smoking?This nerve is crushed!This nerve is crushed!
VitaminsVitaminsMagnetsMagnetsCarpal mobilizationCarpal mobilizationNerve glidingNerve glidingAcupuncture Acupuncture
AerobicsAerobicsAcupunctureAcupunctureLasersLasersTherapeutic touchTherapeutic touchUS/ IontoUS/ Ionto
IontophoresisIontophoresis
Administration of Administration of medications by medications by direct currentdirect currentSome reports of Some reports of ionto followed by ionto followed by pulsed ultrasoundpulsed ultrasoundControlled studies Controlled studies insufficient insufficient Fedorczyk Micklovitz Fedorczyk Micklovitz 19951995
UltrasoundUltrasoundMinimal SupportMinimal Support
Systematic review of 35 RCT’s for use Systematic review of 35 RCT’s for use of US in people with musculoskeletal of US in people with musculoskeletal injuries and soft tissue lesions.injuries and soft tissue lesions.10 RTC’s met criteria with acceptable 10 RTC’s met criteria with acceptable methodsmethodsResults of Results of 2 trials2 trials suggest that US is suggest that US is more effective in treating CTS and more effective in treating CTS and calcific tendonitis of the shoulder than calcific tendonitis of the shoulder than placebo US, but placebo US, but 8 trials8 trials suggest it is suggest it is not.not.
Robertson VJ, Baker KG. Phys Ther 2001Robertson VJ, Baker KG. Phys Ther 2001
Therapeutic Ultrasound for CTSTherapeutic Ultrasound for CTSCochrane Database Cochrane Database SSystyst Rev Rev
2013……2013…… Page et alPage et al
Poor quality evidence Poor quality evidence from limited data to from limited data to support US over support US over placebo or any other placebo or any other conservative regimenconservative regimen
Insufficient support of Insufficient support of one type US regimen one type US regimen over anotherover another
Acupuncture (Nope)Acupuncture (Nope)No evidence that acupuncture No evidence that acupuncture is an effective therapy for CTis an effective therapy for CT
Systematic review of RCT’sSystematic review of RCT’s–– SimSim et al. J Pain 2011et al. J Pain 2011
“She responded well to “She responded well to acupuncture which provided acupuncture which provided good symptomatic treatment good symptomatic treatment rather than cure and allowed her rather than cure and allowed her to continue her work as a school to continue her work as a school crossing lady whilst she awaited crossing lady whilst she awaited surgical release”surgical release”
Acupuncture Medicine Acupuncture Medicine 20022002

21Evans RB, carpal tunnel lecture, 2014
Low level laser plus TENSLow level laser plus TENS
Low level laser therapy Low level laser therapy (LLLT) plus TENS (LLLT) plus TENS applied to acupuncture applied to acupuncture points significantly points significantly reduced pain in reduced pain in 1111 CTS CTS subjects in VA setting subjects in VA setting who failed surgical or who failed surgical or conservative treatmentconservative treatmentRandomized Controlled Randomized Controlled TrialTrialNaeser MA. et al. Arch Naeser MA. et al. Arch Phys Med Rehabil 2002Phys Med Rehabil 2002
Would a flashlightWork as well?
Magnet TherapyMagnet Therapy
Use of a magnet for reducing pain to Use of a magnet for reducing pain to CTS was CTS was no more effectiveno more effective than the than the use of placebo. use of placebo. RCTRCT
Carter et al. J Fam Pract 2002.Carter et al. J Fam Pract 2002.
CTracCTrac“first and only clinically proven modality “first and only clinically proven modality
for treating CTS without surgery”for treating CTS without surgery”
Therapeutic Touch (TT)Therapeutic Touch (TT)Randomized Controlled TrialRandomized Controlled Trial
Sham TT vs. TTSham TT vs. TTTherapeutic touch Therapeutic touch no better than no better than placebo in placebo in influencing median influencing median motor nerve distal motor nerve distal latencies, pain latencies, pain scores, relaxation scores, relaxation scores.scores.Blankfield et al 2001
Everybody liked Everybody liked to be rubbed: to be rubbed: EvansEvans
Activity ModificationInadequate evidenceto implicate occupational Factors: Lozano 2008
22Evans RB, carpal tunnel lecture, 2014
National Institute for Occupational Safety National Institute for Occupational Safety and Health and Health recognizesrecognizes risk factorsrisk factors
ASSH no proven relationshipASSH no proven relationshipAustralian court system, RSI does not exist Australian court system, RSI does not exist
Ergonomic Positioning or equipment Ergonomic Positioning or equipment for treating CTSfor treating CTS
Cochrane Database Cochrane Database SSystyst Rev Rev 20122012O’Connor et alO’Connor et al
Ergonomic vs placebo keyboardsErgonomic vs placebo keyboardsInsufficient evidence Insufficient evidence from RCT’s to from RCT’s to determine if ergonomic positioning or determine if ergonomic positioning or equipment is beneficial or harmfulequipment is beneficial or harmfulNo association proven No association proven
Computers and CTSComputers and CTSMediouniMediouni Z et al, J Z et al, J OccupOccup Environ Med 2014Environ Med 2014
: :
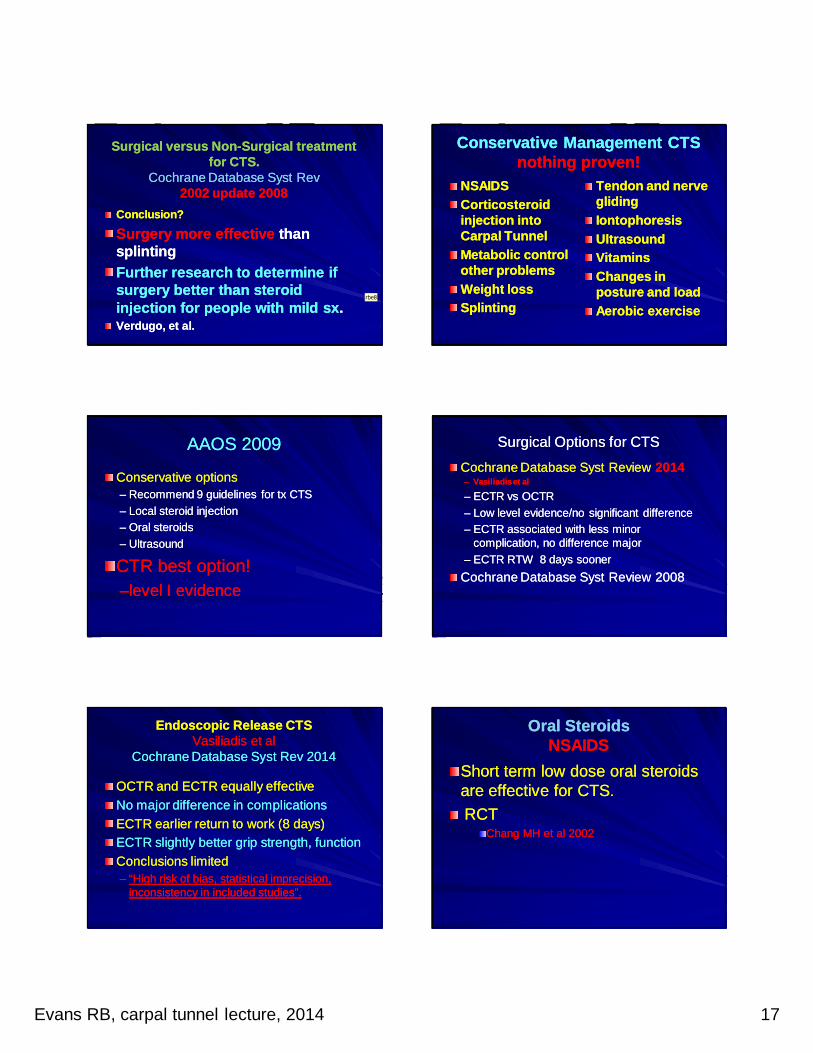
Occupational ExposureOccupational ExposureMetaMeta----analysisanalysis
Prolonged exposure to nonProlonged exposure to non--neutral wrist neutral wrist increases risk for CTS 2xincreases risk for CTS 2x–– You et al: You et al: SafSaf Health Work Health Work 20142014
Occupational exposure to excess Occupational exposure to excess vibration, increased hand force and vibration, increased hand force and repetition increase risk of developing CTSrepetition increase risk of developing CTS–– BarcenillaBarcenilla et al et al PheumatologyPheumatology (Oxford) (Oxford) 20122012
TriggersFlexor tendonitis
CTP at 40 mmHG
CTP at 280 mmHG
Protective effect of Glove on CompressionProtective effect of Glove on CompressionNo SupportNo Support
Gel padded glove Gel padded glove does not have a does not have a protective effect on protective effect on CTS induced by CTS induced by compression in the compression in the workplace.workplace.Does provide Does provide significant comfortsignificant comfortRandomized Clinical Randomized Clinical TrialTrialDeltombe et al 2001Deltombe et al 2001
Conservative ManagementConservative ManagementMy ApproachMy Approach
Evaluate associate problems with high Evaluate associate problems with high index of suspicionindex of suspicionDecrease Carpal tunnel PressuresDecrease Carpal tunnel Pressures
SplintSplintActivity modificationActivity modificationEducationEducation
Modalities to decrease edemaModalities to decrease edemaMedications to reduce inflammationMedications to reduce inflammation

23Evans RB, carpal tunnel lecture, 2014
Conservative Management Conservative Management Splint the MP Joints 0Splint the MP Joints 0--40 Degrees40 Degrees
Positive lumbrical Positive lumbrical incursionincursionTriggering or Triggering or tenderness A1tenderness A1Flexor or Flexor or extensor extensor tenosynovitistenosynovitisThe inadvertant The inadvertant grippergripper
Postoperative ManagementPostoperative ManagementCarpal Tunnel ReleaseCarpal Tunnel Release
ComplicationsComplicationsOpen and Endoscopic ReleaseOpen and Endoscopic ReleaseWounds dehisce (early suture removal)Wounds dehisce (early suture removal)Infection/suture Infection/suture abcessabcess/ hematoma/ hematomaPainful scar (crossing the wrist?)Painful scar (crossing the wrist?)Pillar Pain….Pillar Pain….injury to PCBMNinjury to PCBMNIncomplete releaseIncomplete releaseTendon adhesionTendon adhesionTrigger fingers/ tendonitisTrigger fingers/ tendonitisCRPS; CRPS; neuromaneuroma in continuityin continuityPalmaris Palmaris LongusLongus inflammationinflammation
ASSH review/5 year periodASSH review/5 year periodPalmer, Palmer, TTolvonenolvonen JHS Am 1999JHS Am 1999
455 major complications from ECTR 455 major complications from ECTR txtx by by 708 respondents708 respondents–– 100 median, 88 ulnar, 77 digital nerve lacerations100 median, 88 ulnar, 77 digital nerve lacerations
–– 121 vessel, 69 tendon lacerations121 vessel, 69 tendon lacerations
283 major complications from OCTR 616 283 major complications from OCTR 616 respondentsrespondents–– 147 median, 29 ulnar,54 digital nerve lacerations147 median, 29 ulnar,54 digital nerve lacerations
–– 34 vessel, 19 tendon lacerations34 vessel, 19 tendon lacerations
An Outcome Protocol for CTS: An Outcome Protocol for CTS: A Comparison of A Comparison of Outcomes in Patients with and without MedicalOutcomes in Patients with and without MedicalComorbidities: Comorbidities: Cagle PJ, et al JHS Am Cagle PJ, et al JHS Am 20142014
950 OCTR950 OCTRSelf reported severity Self reported severity and functional scores and functional scores Boston Carpal Tunnel Boston Carpal Tunnel Outcomes QuestionnaireOutcomes Questionnaire2,6,12 weeks2,6,12 weeks
Significant Significant improvements in improvements in sxsxseverity and hand severity and hand functional after functional after OCTR can be OCTR can be expected expected regardless of age, regardless of age, coco--morbidity, WC morbidity, WC statusstatus
Problems to be Solved POProblems to be Solved PO
DoubleDouble--crush, compression other crush, compression other levelslevelsLoss tendon glide/ tendon adhesionLoss tendon glide/ tendon adhesionUndiagnosed, untreated trigger fingersUndiagnosed, untreated trigger fingersWeaknessWeaknessPain from basilar thumb arthritisPain from basilar thumb arthritisADL/ ergonomic issuesADL/ ergonomic issuesEmployer expectationsEmployer expectations

24Evans RB, carpal tunnel lecture, 2014
Value of therapy PO RehabValue of therapy PO Rehab
Limited, low evidence for PO interventionsLimited, low evidence for PO interventions–– Splint, wound care, exercise, cold or ice Splint, wound care, exercise, cold or ice
therapy, multimodal hand rehab, therapy, multimodal hand rehab, lazerlazer, , electrical modalities, scar desensitization and electrical modalities, scar desensitization and arnica.arnica.
–– Peters et al: Peters et al: Cochrane Database Review Cochrane Database Review 20132013
Faster return to work but no effect on Faster return to work but no effect on functional recoveryfunctional recovery. . ProvincialiProvinciali 20002000Cost for Cost for uncomplicateduncomplicated CTR unjustified CTR unjustified Pomerance 2007Pomerance 2007
Postoperative Therapy CTR Postoperative Therapy CTR Opinion Based (MINE)Opinion Based (MINE)
Wound care/ prevent tensionWound care/ prevent tensionEducation for edema control, exerciseEducation for edema control, exerciseWrist control splint ( MP’s/ thumb?)Wrist control splint ( MP’s/ thumb?)Address associated problemsAddress associated problems–– Double crush, triggers, OA CMCDouble crush, triggers, OA CMCScar managementScar managementCoordinate return to workCoordinate return to work
PO Splinting CTR DebatedPO Splinting CTR Debated
Finsen 1999Martins 2006Bury 1995Cebesoy 2007Huemer 2007
Does Does splintagesplintage help pain after CTR?help pain after CTR?
Randomized Clinical TrialRandomized Clinical Trial102 102 ptpt PO CTRPO CTR
No differences in pain levelsNo differences in pain levels–– Bhatia et al 2000Bhatia et al 2000
Little therapeutic benefit Little therapeutic benefit Trend away from splintingTrend away from splinting–– Henry et al, 2008Henry et al, 2008
PO Splinting 2PO Splinting 2--3 weeks 3 weeks author preferenceauthor preference
Control overuseControl overusePrevent inflammationPrevent inflammationPrevent wound site Prevent wound site tensiontensionPain relief, address Pain relief, address issues of CMC OAissues of CMC OANerve and tendon Nerve and tendon gliding addressed with gliding addressed with exercise exercise
Minimize Scar ComplicationsMinimize Scar Complications
Short incisionShort incisionMinimize tension Minimize tension with splint and with splint and exercise exercise techniquetechniqueSutures 17 daysSutures 17 daysMicroporeMicropore paper paper tapetape

25Evans RB, carpal tunnel lecture, 2014
Dehisced OCTR IncisionDehisced OCTR IncisionInfection.. early suture removal…Infection.. early suture removal…
Incisions that cross the wristIncisions that cross the wrist
Predictors of Return to Work.Predictors of Return to Work.Katz et al 1995Katz et al 1995
Correlation with failure RTWCorrelation with failure RTWPersistent symptomsPersistent symptomsScar tendernessScar tenderness
Work disability at 6 months is 29%Work disability at 6 months is 29%
Principal predictor is relief of sx and Principal predictor is relief of sx and scar tendernessscar tenderness
Nerve Density in the PalmNerve Density in the PalmCassidy et al 1995Cassidy et al 1995
OCTR + SynovectomyProblems with tendon glide
Wound tension, OCTR Palmaris longus nicked OCTR
Incision crossing the wristIncreased tensionCutaneous nerve density high
TenosynovectomyTenosynovectomy not indicatednot indicatedShrumShrum et al. 2002et al. 2002
A AAOS 2007A AAOS 2007
No problem
Oh, my
Scar ManagementScar ManagementPaper tapePaper tapeTopical silicone gel Topical silicone gel sheeting (SGS) sheeting (SGS) MassageMassageUltrasoundUltrasoundIontophoresisIontophoresisLidocaine Patch 5%Lidocaine Patch 5%DesensitizationDesensitization

26Evans RB, carpal tunnel lecture, 2014
Scar ManagementScar ManagementIontophoresisIontophoresis
Administration of Administration of medications by medications by direct currentdirect currentSome reports of Some reports of ionto followed by ionto followed by pulsed ultrasoundpulsed ultrasoundControlled studies Controlled studies insufficient insufficient Fedorczyk Micklovitz Fedorczyk Micklovitz 19951995
Scar ManagementScar ManagementUltrasoundUltrasound
Insufficient Insufficient supportsupportMichlovitz S. Michlovitz S. Rehab of the Hand Rehab of the Hand , 4th ed. 1990, 4th ed. 1990Nussbaum E. The Nussbaum E. The Influence of Influence of Ultrasound on Ultrasound on Healing Tissues. J Healing Tissues. J Hand Ther 1998Hand Ther 1998
Cold Therapy TreatmentCold Therapy Treatment
RCTRCTEfficacy ice therapy 72 patients CTREfficacy ice therapy 72 patients CTRPatients treated with Temperature Patients treated with Temperature Controlled Cooling Blanket (CCT) had Controlled Cooling Blanket (CCT) had greater reduction in pain, took fewer greater reduction in pain, took fewer narcotics, had less edema by day 3 narcotics, had less edema by day 3 PO than those treated with traditional PO than those treated with traditional ice therapy.ice therapy.Hochberg J. J Hand Ther 2001Hochberg J. J Hand Ther 2001
Tendon AdhesionTendon AdhesionPeriPeri--articular Stiffnessarticular Stiffness
Tendon Gliding Through the CTHunter and Wehbe
27Evans RB, carpal tunnel lecture, 2014
Sympathetic FlareSympathetic FlareSympathetic Maintained Pain SyndromeSympathetic Maintained Pain Syndrome
Contrast bathsContrast bathsStress loadingStress loadingDaily gentle Daily gentle therapytherapyNeurontinNeurontinStellate ganglion Stellate ganglion blocksblocksMissed diagnosisMissed diagnosis
Flare Reaction or NeuropraxiaFlare Reaction or Neuropraxia
Assess inciting lesionAssess inciting lesionAntiAnti--inflammatories, inflammatories, Medrol, neurontin, Medrol, neurontin, blocksblocksPatient may be Patient may be overworking, therapist overworking, therapist or splints may apply or splints may apply too much force.too much force.
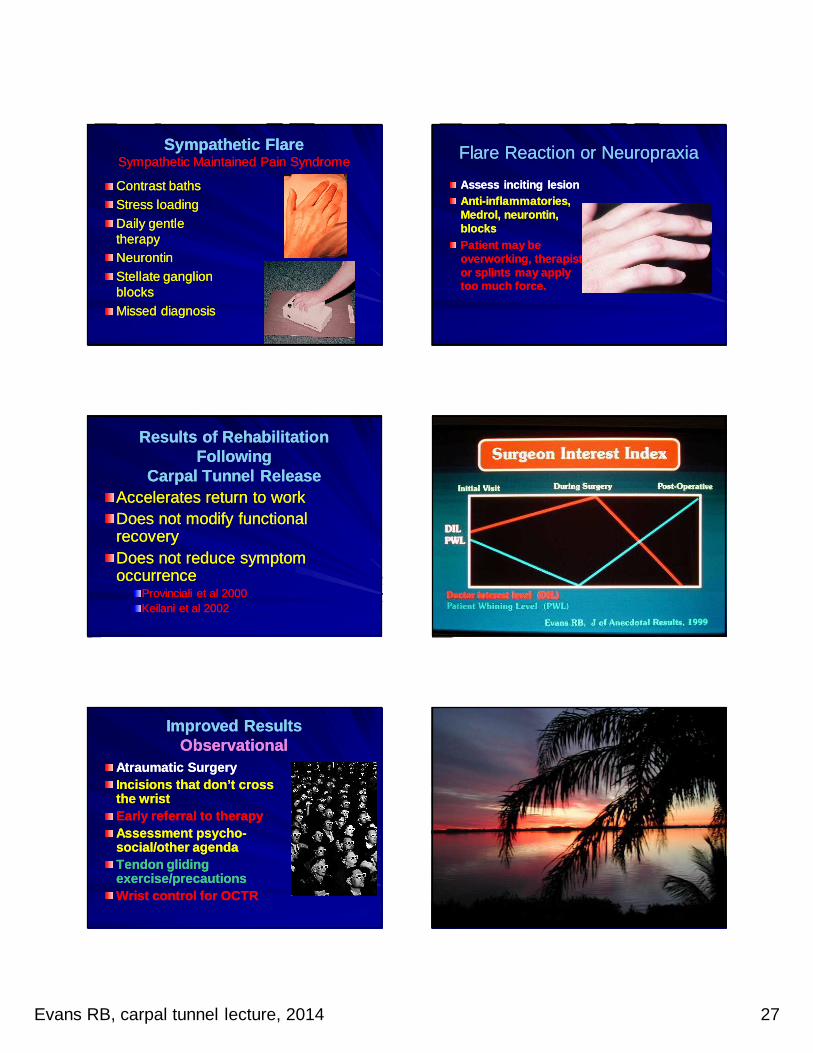
Results of Rehabilitation Results of Rehabilitation FollowingFollowing
Carpal Tunnel ReleaseCarpal Tunnel ReleaseAccelerates return to workAccelerates return to workDoes not modify functional Does not modify functional recoveryrecoveryDoes not reduce symptom Does not reduce symptom occurrenceoccurrence
Provinciali et al 2000Provinciali et al 2000Keilani et al 2002Keilani et al 2002
Improved ResultsImproved ResultsObservational Observational
Atraumatic SurgeryAtraumatic SurgeryIncisions that don’t cross Incisions that don’t cross the wristthe wristEarly referral to therapyEarly referral to therapyAssessment psychoAssessment psycho--social/other agendasocial/other agendaTendon gliding Tendon gliding exercise/precautionsexercise/precautionsWrist control for OCTRWrist control for OCTR

28Evans RB, carpal tunnel lecture, 2014
Hands holding starsHands holding stars