epidemiology, antibiotic resistance trends and the cost of enteric fever in east london, 2005–2010
TRANSCRIPT

Travel Medicine and Infectious Disease (2011) 9, 206e212
ava i lab le at www.sc iencedi rect .com
journal homepage : www.e lsev ie rhea l th .com/ journals / tmid
Epidemiology, antibiotic resistance trends and thecost of enteric fever in East London, 2005e2010
Srinivasulu Reddy a,*, Jayakeerthi Rangaiah a, Sarah Addiman b,David Wareham c, Peter Wilson d, Armine Sefton c
aDepartment of Microbiology, Barts and The London NHS Trust, 3rd Floor, Pathology and Pharmacy Building, 80 Newark St.,London E1 2ES, United KingdombNorth East and North Central London Health Protection Unit, United KingdomcCentre for Immunology and Infectious Disease, Blizard Institute of Cell & Molecular Science,Barts and The London School of Medicine & Dentistry, United KingdomdDepartment of Microbiology, Newham University Hospital NHS Trust & Barts and The London NHS Trust, United Kingdom
Received 10 November 2010; received in revised form 14 March 2011; accepted 17 March 2011Available online 1 June 2011
KEYWORDSS. typhi;S. paratyphi;Cost of enteric fever;Azithromycin;Resistance
* Corresponding author. Tel.: þ44 2E-mail address: drsrinivasulu63@ya
1477-8939/$ - see front matter ª 201doi:10.1016/j.tmaid.2011.03.003
Summary Introduction: Enteric fever seen in the UK has usually been acquired abroad. Thecost to the NHS of treating enteric fever cases is not known. Data on the epidemiology of entericfever, inpatient treatment costs and the public health management is needed to make decisionsregarding the cost benefit considerations of introducing targeted prevention strategies.Methods: A retrospective study of laboratory confirmed enteric fever cases was conducted toestimate the cost of inpatient treatment and to determine antimicrobial resistance patternsat two hospitals in East London between January 2005 and the end of August 2010.Results: 138 cases of enteric fever were identified during the study period (90 S.ser.Typhi and 48S. ser. Paratyphi). 92% had a recent history of foreign travel, 57% had travelled to visit friends andrelatives (VFRs), 26% sought pre-travel health advice and 26% of patients had received typhoidvaccination. The inpatient treatment cost of 138 cases to the NHS was £272,747. The proportionof isolates with high level ciprofloxacin resistance (MICs>1mg/L) has increased from 10% in 2006to 30% in 2010. Our data also shows the emergence of isolates with high azithromycin MICs(>32 mg/L); 60% (six out of ten) isolates tested in JulyeAugust 2010.Conclusions: There is a significant direct cost of treating enteric fever cases on the NHS. Costreductionmeasures are confined due to the lack of effective oral antibiotics following the emer-gence of high level resistance to ciprofloxacin and azithromycin. Outpatient parenteral antibi-otic therapy service and improved preventative public health measures aimed at VFRtravellers in particular may be helpful in reducing costs.ª 2011 Elsevier Ltd. All rights reserved.
032460312; fax: þ44 2032460325.hoo.com (S. Reddy).
1 Elsevier Ltd. All rights reserved.

Enteric fever in East London 207
Introduction
Enteric fever is a systemic infection caused by Salmonellaenterica subsp. enterica serovar. Typhi (S.ser.Typhi) orSalmonella enterica subsp. enterica serovar.Paratyphi(S.ser.Paratyphi). These organisms pose a risk to travel-lers visiting endemic areas. Enhanced surveillance ofenteric fever in England, Wales and Northern Ireland fromMay 2006 to April 2007 reported 457 cases of entericfever; most cases were from the London area (40% ofcases) and 86% had travelled to visit friends and relatives(VFRs) in the Indian subcontinent.1,2 The incidence ofenteric fever among travellers from UK to India, Pakistanand Bangladesh was 17.32 per 100,000 visits.1 The risk ofenteric fever is six fold higher in VFRs compared to othertravellers.1
The London Boroughs of Tower Hamlets and Newham,which are ethnically diverse, account for sixteen percent ofenteric fever cases (121/757) reported for London(2006e2009). Notably the annual rate of S.ser.Paratyphi per100,000 in Tower Hamlets (2.11) is almost double the ratefor London (1.09) and over four times higher than the ratefor England (0.46). The annual rate of S.ser.Typhi in New-ham (5.58) is over four times the rate for London (1.38) andover eleven times higher than the rate for England (0.48) asshown in Table 1.
Travellers with enteric fever usually present witha nonspecific febrile illness with insidious onset. Death andserious complications are unusual among travellers withenteric fever.3,4 There was no significant difference inclinical presentation or outcome between S.ser.Typhi andS.ser.Paratyphi cases.3 Isolates with reduced susceptibilityto ciprofloxacin [minimum inhibitory concentration (MIC) e0.125e1 mg/L] have emerged in recent years.4,5 Thirdgeneration cephalosporins and azithromycin are increas-ingly being used as first line antibiotics for the treatment ofenteric fever.6
The UK enhanced surveillance report recommendedstudies looking at the length of hospital stay and cost ofinpatient treatment of enteric fever cases.1 To our knowl-edge, there are no studies from the UK estimating thedirect inpatient costs of treating enteric fever cases. Theprimary objective of our study was to determine the costassociated with inpatient treatment. The secondaryobjective was to describe local epidemiology and trends inantibiotic resistance among S.ser.Typhi and S. ser. Para-typhi bacteraemia isolates.
Table 1 Total number of cases of S.ser. Typhi and S.ser. ParaTower Hamlets and Newham (2006e2009).
Area S.ser. Typhi cases
Total cases Mean rate & 95
Englanda 992 0.48 (0.45e0.51Londona 423 1.38 (1.25e1.52Tower hamletsb 28 3.11 (2.06e4.49Newhamb 54 5.59 (4.10e7.29a Travel Health and Migrant Section, Centre for Infections, HPA, Labb North East & Central Health Protection Unit Notifications and O
utilised.
Methods
Study design
We conducted a retrospective laboratory based surveil-lance study of all patients admitted with S.ser.Typhi ORS. ser. Paratyphi bacteraemia to the Royal London Hospitaland Newham University Hospital between 1 January 2005and 30 August 2010. The Royal London Hospital is a largetertiary hospital which serves a large Bangladeshi pop-ulation in the London borough of Tower Hamlets; 33% of thetotal borough population are of Bangladeshi origin and one-half of the total UK Bangladeshi population live in TowerHamlets.7 Newham hospital provides an acute medicalservice to people living in the London Borough of Newhamwhich is the second most ethnically diverse London boroughwith a large Asian population; 38% of the total boroughpopulation (Indians-12.2%, Bangladeshi-10%, Pakistani-8.9%).7
Enhanced enteric fever surveillance data from NorthEast and North Central London Health Protection Unit wasreviewed for the following data: ethnicity, history of recentforeign travel, reason for travel, pre-travel health advice,and typhoid vaccination. Hospital electronic records werereviewed for patient demographics, length of hospital stayand clinical outcome.
Microbiology
Blood culture isolates were analysed using bioMerieuxBacT/ALERT automated blood culture system, identifiedwith API20E biochemical identification kit (bioMerieux,France) and species was confirmed by using polyvalent andmonovalent sera. S.ser.Typhi and S.ser.Paratyphi isolateswere referred to the Health Protection Agency (HPA)Salmonella Reference unit at Colindale for the confirmationof identification, serotyping and phage typing. Suscepti-bility of the isolates to ampicillin, chloramphenicol,trimethoprim, ceftriaxone, cefuroxime and nalidixic acidwas determined by British Society of AntimicrobialChemotherapy (BSAC) disc susceptibility method.8 Prior to2006, nalidixic acid resistance was used as a surrogatemarker of ciprofloxacin resistance and MICs by E test werenot routinely performed. Reduced ciprofloxacin suscepti-bility was defined as an isolate with Ciprofloxacin MIC of0.125e1 mg/L by E test.9 Isolates with an MIC of >1 mg/L
typhi and mean rate/100,000 per year for England, London,
S.ser. Paratyphi cases
% C.Is Total cases Mean rate & 95% C.Is
) 958 0.47 (0.43e0.49)) 334 1.09 (0.97e1.21)) 19 2.11 (1.26e3.29)) 20 2.07 (1.26e3.19)
oratory confirmed cases.NS (Office of National Statistics) mid year population estimates

208 S. Reddy et al.
were reported as ciprofloxacin resistant.8 The azithromycinMIC breakpoints and zone diameters have not been clearlydefined for Salmonella isolates. BSAC methods for suscep-tibility testing suggest the possibility of using azithromycinto treat S.ser.Typhi infections (MIC<16 mg/L).8 Azi-thromycin MICs for drug sensitive control strains of S.ser.-Typhi and S.ser.Paratyphi A are not greater than 8 mg/L and12 mg/L respectively.10 None of isolates (50 S.ser.Typhi and40 S.ser.Paratyphi A) tested at HPA Salmonella referenceunit in 2006 had MICs higher than MICs of the drug sensitivecontrol strains.10 We determined azithromycin MICs by Etest (AB biodisk, Solna, Sweden) method on Iso-sensitestagar medium (Oxoid, Basingstoke, UK) on all isolates fromJuly 2010. This method is currently used by the HPASalmonella Reference Unit (Steve Connell, personalcommunication). Iso-sensitest agar is the most widely usedmedium in the UK and the pH of this medium is around 7.4.The physiological extracellular pH is around 7.5 and webelieve that in vitro testing at this pH is clinically useful.MIC values were read at 80% inhibition. Isolates with azi-thromycin MICs greater than the above cut-off points wereregarded as azithromycin resistant.
Inpatient treatment cost calculations
Payment by results (PbR) is a system by which NHSproviders are paid a standard tariff for the clinical activitythey undertake. Standard tariff is set on the basis ofaverage cost of providing a particular clinical activity; usingdata gathered from all NHS Hospitals.11 HealthcareResource Groups (HRG) are standard groupings of clinicallysimilar treatments which use common levels of healthcareresource. The HRG version 4 code for enteric fever withoutcomplications (S.ser.Typhi and S.ser.Paratyphi A, B, C ) isFZ36C.12 The cut-off point for calculation of excess bed
Table 2 Antibiotic susceptibility data of S.ser.Typhi and S.ser.P
Antibiotic resistance data
S.ser.Typhi (n Z 90)MDRa
Nalidixic acid resistantb
Ciprofloxacin MIC (0.125e1 mg/L)Ciprofloxacin MIC (>1 mg/L)Azithromycin MIC (>8 mg/L) : (n Z 2)
S.ser.Paratyphi (n Z 48)MDRa
Nalidixic acid resistantb
Ciprofloxacin MIC (0.125e1 mg/L)Ciprofloxacin MIC (>1 mg/L)Azithromycin MIC (>12 mg/L): (n Z 8)
All Enteric fever isolates (n Z 138)MDRNalidixic acid resistantb
Ciprofloxacin MIC (0.125e1 mg/L)Ciprofloxacin MIC (>1 mg/L)a MDR e Multidrug resistance was defined as resistance to 3 classesb Ciprofloxacin MIC by E test was routinely performed from year 2006
on nalidixic acid test results.
days for an enteric fever case without complications basedon the national data is 16 days and any bed days above thiscut-off point are counted as excess bed days. This cut-offpoint is called trim point which is equal to the upperquartile of the national distribution (length of hospital stay)plus 1.5 times the interquartile range. For e.g. If the totallength of stay for an enteric fever patient is 20 days, thenthe excess bed day for that patient is 4 days based on a trimpoint of 16 days. The non-elective 2010e2011 tariff fora case of enteric fever without complications was £1929and the excess bed day tariff was £187 per day.12 Cumu-lative excess bed days were calculated for all patients withlength of hospital stay greater than 16 days.
Results
Microbiology
A total of 138 enteric fever cases were identified betweenJanuary 2005 and August 2010. Ninety (65%) and forty eight(35%) cases were caused by S.ser.Typhi and S.ser.Paratyphirespectively. Antibiotic resistance data are shown in Table 2.Fig. 1 shows the trends in ciprofloxacin resistance. 40%(36/90) of S.ser.Typhi isolates were multidrug resistant. 54%(49/90) of S.ser.Typhi isolates exhibited reduced suscepti-bility to ciprofloxacin and 7% (6/90) of S.ser.Typhi isolateswere resistant to ciprofloxacin. In contrast, none of theS.ser.Paratyphi isolates were multidrug resistant. Fifty sixpercent (27/48) of S.ser.Paratyphi isolates had reducedsusceptibility to ciprofloxacin and 12.5% (6/48) isolates wereresistant to ciprofloxacin. Eighty three percent (10/12) ofciprofloxacin resistant isolates (MIC>1mg/L) identifiedwereobtained during the year 2009 and 2010. 80% (8/10) entericfever isolates obtained in JulyeAugust 2010 were
aratyphi isolates (January 2005eAugust 2010).
No. of Isolates (%)36 (40%)63 (70%)49 (54%)6(7%)2/2 (MICs Z 12 mg/L)
034(71%)27(56%)6(12.5%)6/8 (MICs-32 mg/L)
36 (26%)97 (70%)76 (55%)12 (8.6%)
of antibiotics (ampicillin, chloramphenicol and trimethoprim).. Isolates from 2005 were reported as ciprofloxacin resistant based

Figure 1 Ciprofloxacin resistance among enteric fever isolates, January 2005eAugust 2010. Note: Ciprofloxacin MIC data was notavailable on all isolates in 2005. Therefore nalidixic acid susceptibility was used to classify the isolates. None of the isolates in 2005had Ciprofloxacin MIC >1 mg/L.
Enteric fever in East London 209
azithromycin resistant as per our definition; Six out of eight(75%) S.ser.Paratyphi A isolates had azithromycin MICs of32 mg/L and two S.ser.Typhi isolates had azithromycin MICsof 12 mg/L. One patient with uncomplicated enteric feverdue to azithromycin resistant isolate had poor clinicalresponse with azithromycin (persistent pyrexia) and wasreadmitted for intravenous ceftriaxone therapy. Theremaining seven azithromycin resistant cases were treatedwith intravenous ceftriaxone and therefore we are unable toestablish therapeutic failure due to high azithromycin MICs.
Patient demographic and surveillance data
Enhanced surveillance and demographic details was avail-able for 138 enteric fever cases (Jan 2005eAugust 2010) andare shown in Table 3. The median age was 27 years (range;1e72 years); 92 cases (67%) and 25 cases (18%) were reportedin age group 16e40 yrs andunder 16 years respectively. Malesaccounted for 75 cases (54%) compared to 63 cases (46%)among females. Ethnic background information was avail-able in 98 (76%) cases. Indian, Pakistani and Bangladeshipatients made up the majority of cases (85/98 cases; 87%).New entrants and foreign visitors accounted for 10% of cases.Ninety two percent (112/122) of cases had a history of recentforeign travel; 57% (48/84) patients had travelled to visitfriends and relatives and 23% patients were new entrants/foreign visitors fromthe Indian subcontinent. Inpatientswitha complete dataset on travel advice, only 26% (14/41) ofpatients sought pre-travel health advice before their trip and26% (13/50) patients had a history of typhoid vaccination. Ofthose patients who received typhoid vaccinations, 6 hadinfectionwith S.ser.ParatyphiAand7with S.ser.Typhi. Therewas no significant difference in the length of stay betweenvaccinated and nonvaccinated cases.
Hospitalisation costs
Ninety five percent (132/138) of cases were admitted to thehospital and themedian lengthof hospital staywaseight days(range: 1e26days). Therewasno significant difference in the
length of stay between patients with ciprofloxacin suscep-tible and ciprofloxacin intermediate/resistant enteric fevercases (6.5 days Vs 8 days). There were no deaths in our studypopulation. The cost of treating 138 enteric fever episodes isshown in Table 4. The total cost of treating 138 enteric fevercases was estimated at £272,747 with average cost at £1976per patient. When the inpatient treatment costs are coupledwith the approximate public health costs [environmentalhealth services (£120) and health protection input (£60)], theaverage cost of each enteric fever case rises to approxi-mately £2109 per patient. However this cost excludes otherindirect costs; including the potential loss of earnings forcases excluded from work, the management of contacts,laboratory costs for stool cultures for clearance for contacts,particularly those in risk groups, and antibiotic treatment ofchronic carriers.
Discussion
We conducted a retrospective review of enteric fever casesadmitted to two hospitals in East London over a five yearstudy period. Ninety two percent of enteric fever cases wereassociated with foreign travel and 57% of these patients hadtravelled to visit friends and relatives (VFRs) in the Indiansubcontinent. Overrepresentation of enteric fever in VFRtravellers is evident in this study (57%) and consistent withnational findings.1,2 VFR travellers are at increased risk ofacquiring several travel related infections including entericfever. They are also less likely to seek pre-travel advice andadhere to recommended medication and precautions.2
UK enhanced surveillance of enteric fever cases wasimplemented from 1 May 2006; therefore pre-travel adviceand typhoid vaccination data was not available for the 40cases diagnosed before 1 May 2006 in our study. A highpercentage of cases (74%) did not obtain pre-travel advice,with only seven out of ninety S.ser.Typhi cases having beenvaccinated prior to travel. This is despite 93% of generalpractices across Newham and Tower Hamlets providingtravel health services (Health Protection Unit 2007 unpub-lished) and national travel health campaigns and travel

Table 3 Demographic and epidemiological data forenteric fever cases January 2005eAugust 2010.
Total No of Enteric fever cases 138S.ser.Typhi 90 (65%)
S.ser.Paratyphi A, B & C 48 (35%)
Hospital siteNewham Hospital 69 (50%)Royal London Hospital 69 (50%)
SexMales 75 (54%)Females 63 (46%)
Age<16 25 (18%)16e40 92 (67%)>40 21 (15%)
EthnicityAsian/Asian British e Bangladeshi 41(42%)
Asian/Asian British e Indian 25(26%)
Asian/Asian British e Pakistani 19 (19%)
Black or Black British e African 3 (3%)Foreign visitor fromIndian subcontinent
5 (5%)
New entrant fromIndian subcontinent
5(5%)
Not knowna 40
Foreign travelYes 112 (92%)
No 10 (8%)Not knowna 16
Reason for travelVisiting friends and relatives 48 (57%)
New entrant 11 (13%)
Holiday 11 (13%)Business 2 (2%)Mixture 3 (4%)Foreign visitor 9 (11%)Not knowna 54
Risk groupsChild < 5yrs 5 (5%)
Food handler 9 (9%)
Healthcare worker 4 (4%)
Doubtful hygiene 2 (2%)No risk factors 77 (79%)
Not knowna 41
Pre-travel adviceYes 14 (26%)No 41(74%)Not applicableb 28Not knowna 55
Typhoid vaccinationYes 13 (26%)No 37(74%)Not applicableb 28Not knowna 60
Table 3 (continued )
Salmonella species isolatedfrom vaccinated patients
S.ser.Paratyphi A 6S.ser.Typhi 7a Enhanced surveillance dataset was incomplete due to
various reasons: patient lost to follow-up, patients not notifiedto health protection unit, incomplete data for patients diag-nosed in 2005 because enhanced surveillance was introduced in2006.Please note all percentage figures have been calculatedafter exclusion of patients with incomplete dataset.b Pretravel advice and typhoid vaccination was not applicable
in new entrants and foreign visitors from Indian subcontinent.
210 S. Reddy et al.
literature, including S.ser.Typhi specific leaflets, beingwidely available. These findings are consistent withprevious studies which have shown poor typhoid vaccina-tion uptake among travellers; only 4% (36/1027) of patientswith travel associated typhoid fever having receivedtyphoid vaccination.13 A major barrier to typhoid vaccina-tion uptake among VFR travellers may be a misperceptionabout the risk of acquiring enteric fever in comparison totourists.14
HPA antibiotic resistance surveillance data from 2006showed that 68% of S.ser.Typhi isolates and 64% S.ser.Par-atyphi isolates had decreased susceptibility to ciprofloxacin(0.125e1 mg/L).10 In 2006, 2% of S.ser.Typhi isolates and 9%of S.ser.Paratyphi isolates were resistant to ciprofloxacin(>1 mg/L).10 Our data shows that there has been furtherincrease in the proportion of ciprofloxacin resistantisolates; S.ser.Typhi [7.6% (1/13) in 2006 vs 18% (2/11) in2010] and S.ser.Paratyphi A [14.2% (1/8) vs. 44.4%(4/9)].Ten out of twelve ciprofloxacin resistant isolates wereidentified in the years 2009e2010. None of the isolates from2010 were fully susceptible to ciprofloxacin.
In recent years, azithromycin is being increasingly usedas an alternative oral antibiotic to treat uncomplicatedenteric fever cases who do not need hospital admission.6
Azithromycin susceptibility is not routinely performed dueto lack of a well defined clinical and microbiologicalbreakpoints for S.ser.Typhi and S.ser.Paratyphi.8 The pH ofbroth/agar medium can affect MICs and studies have shownthat there is a 256 fold reduction in MICs when tested at pH8 compared to pH of 6.15 A limitation of our susceptibilitytesting method is the use of a lower pH medium (pH-7.4)which may have led to high MIC values. The clinical efficacyof azithromycin has been explained by its ability to achievehigh intracellular concentrations (100 fold greater thanserum levels).6 However serum azithromycin levels ach-ieved may not be sufficient to inhibit the extracellularbacteria with high MICs (32 mg/L) at physiologic pH (pH-7.4). S.ser.Typhi isolates with high azithromycin MICs(64 mg/ml) have been reported in the past but the clinicalsignificance of these isolates are not known.16 Althoughazithromycin use can lead to significant cost savings byreducing length of hospital stay and lower associated costs,clinicians should exercise caution in its use without thein vitro susceptibility results. Clinicians need to closelymonitor all cases for clinical failure and correlateclinical outcomes with in vitro susceptibility results. The
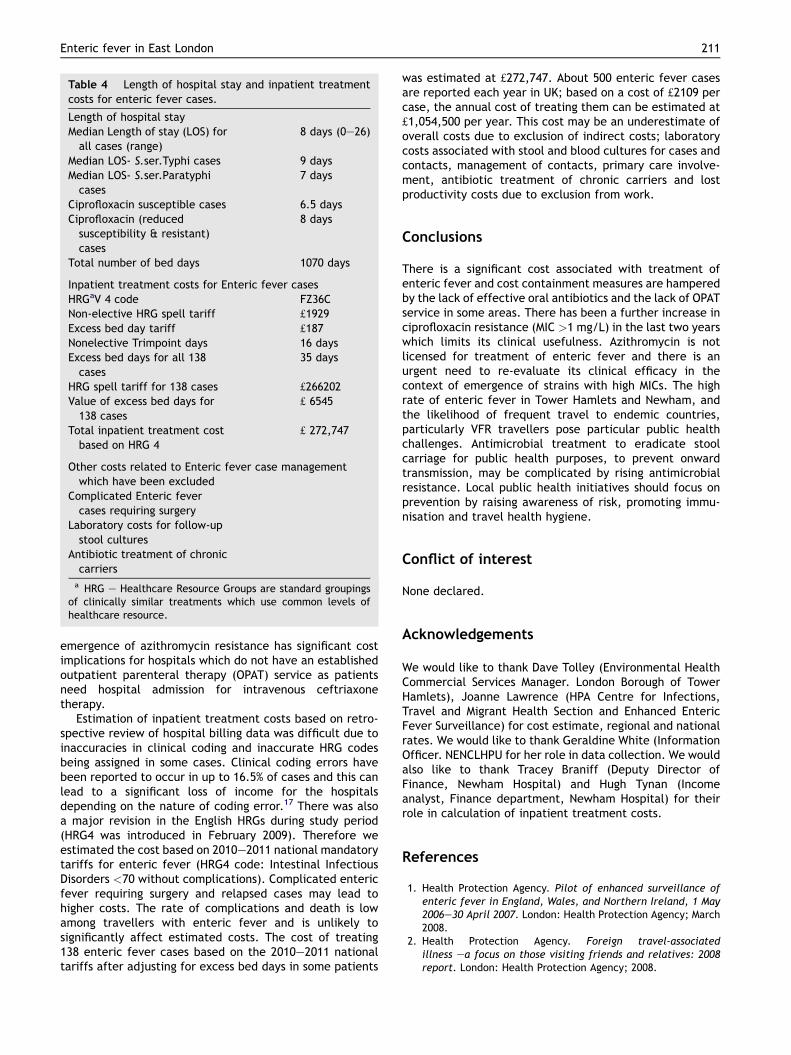
Table 4 Length of hospital stay and inpatient treatmentcosts for enteric fever cases.
Length of hospital stayMedian Length of stay (LOS) forall cases (range)
8 days (0e26)
Median LOS- S.ser.Typhi cases 9 daysMedian LOS- S.ser.Paratyphicases
7 days
Ciprofloxacin susceptible cases 6.5 daysCiprofloxacin (reducedsusceptibility & resistant)cases
8 days
Total number of bed days 1070 days
Inpatient treatment costs for Enteric fever casesHRGaV 4 code FZ36CNon-elective HRG spell tariff £1929Excess bed day tariff £187Nonelective Trimpoint days 16 daysExcess bed days for all 138cases
35 days
HRG spell tariff for 138 cases £266202Value of excess bed days for138 cases
£ 6545
Total inpatient treatment costbased on HRG 4
£ 272,747
Other costs related to Enteric fever case managementwhich have been excluded
Complicated Enteric fevercases requiring surgery
Laboratory costs for follow-upstool cultures
Antibiotic treatment of chroniccarriers
a HRG e Healthcare Resource Groups are standard groupingsof clinically similar treatments which use common levels ofhealthcare resource.
Enteric fever in East London 211
emergence of azithromycin resistance has significant costimplications for hospitals which do not have an establishedoutpatient parenteral therapy (OPAT) service as patientsneed hospital admission for intravenous ceftriaxonetherapy.
Estimation of inpatient treatment costs based on retro-spective review of hospital billing data was difficult due toinaccuracies in clinical coding and inaccurate HRG codesbeing assigned in some cases. Clinical coding errors havebeen reported to occur in up to 16.5% of cases and this canlead to a significant loss of income for the hospitalsdepending on the nature of coding error.17 There was alsoa major revision in the English HRGs during study period(HRG4 was introduced in February 2009). Therefore weestimated the cost based on 2010e2011 national mandatorytariffs for enteric fever (HRG4 code: Intestinal InfectiousDisorders <70 without complications). Complicated entericfever requiring surgery and relapsed cases may lead tohigher costs. The rate of complications and death is lowamong travellers with enteric fever and is unlikely tosignificantly affect estimated costs. The cost of treating138 enteric fever cases based on the 2010e2011 nationaltariffs after adjusting for excess bed days in some patients
was estimated at £272,747. About 500 enteric fever casesare reported each year in UK; based on a cost of £2109 percase, the annual cost of treating them can be estimated at£1,054,500 per year. This cost may be an underestimate ofoverall costs due to exclusion of indirect costs; laboratorycosts associated with stool and blood cultures for cases andcontacts, management of contacts, primary care involve-ment, antibiotic treatment of chronic carriers and lostproductivity costs due to exclusion from work.
Conclusions
There is a significant cost associated with treatment ofenteric fever and cost containment measures are hamperedby the lack of effective oral antibiotics and the lack of OPATservice in some areas. There has been a further increase inciprofloxacin resistance (MIC >1 mg/L) in the last two yearswhich limits its clinical usefulness. Azithromycin is notlicensed for treatment of enteric fever and there is anurgent need to re-evaluate its clinical efficacy in thecontext of emergence of strains with high MICs. The highrate of enteric fever in Tower Hamlets and Newham, andthe likelihood of frequent travel to endemic countries,particularly VFR travellers pose particular public healthchallenges. Antimicrobial treatment to eradicate stoolcarriage for public health purposes, to prevent onwardtransmission, may be complicated by rising antimicrobialresistance. Local public health initiatives should focus onprevention by raising awareness of risk, promoting immu-nisation and travel health hygiene.
Conflict of interest
None declared.
Acknowledgements
We would like to thank Dave Tolley (Environmental HealthCommercial Services Manager. London Borough of TowerHamlets), Joanne Lawrence (HPA Centre for Infections,Travel and Migrant Health Section and Enhanced EntericFever Surveillance) for cost estimate, regional and nationalrates. We would like to thank Geraldine White (InformationOfficer. NENCLHPU for her role in data collection. We wouldalso like to thank Tracey Braniff (Deputy Director ofFinance, Newham Hospital) and Hugh Tynan (Incomeanalyst, Finance department, Newham Hospital) for theirrole in calculation of inpatient treatment costs.
References
1. Health Protection Agency. Pilot of enhanced surveillance ofenteric fever in England, Wales, and Northern Ireland, 1 May2006e30 April 2007. London: Health Protection Agency; March2008.
2. Health Protection Agency. Foreign travel-associatedillness ea focus on those visiting friends and relatives: 2008report. London: Health Protection Agency; 2008.

212 S. Reddy et al.
3. Clark TW, Daneshvar C, Pareek M, Perera N, Stephenson I.Enteric fever in a UK regional infectious diseases unit: a 10 yearretrospective review. J Infect 2010;60:91e8.
4. Patel TA, Armstrong M, Morris-Jones SD, Wright SG, Doherty T.Imported enteric fever: case series from the hospital fortropical diseases, London, United Kingdom. Am J Trop Med Hyg2010;82:1121e6.
5. Cooke FJ, Day M, Wain J, Ward LR, Threlfall EJ. Cases oftyphoid fever imported into England, Scotland and Wales(2000e2003). Trans R Soc Trop Med Hyg 2007;101:398e404.
6. Parry CM, Ho VA, Phuong le T, Bay PV, Lanh MN, Tung le T,et al. Randomized controlled comparison of ofloxacin, azi-thromycin, and an ofloxacineazithromycin combination fortreatment of multidrug-resistant and nalidixic acid-resistanttyphoid fever. Antimicrob Agents Chemother 2007;51:819e25.
7. Census. Office for National Statistics, www.statistics.gov.uk;2001 (accessed 24 February 2011).
8. BSAC methods for antimicrobial susceptibility testing, version9.1, www.bsac.org.uk; March 2010 (accessed 24 February2011).
9. Threlfall EJ, Ward LR. Decreased susceptibility to ciprofloxacinin Salmonella enterica serotype typhi, United Kingdom. EmergInfect Dis 2001;7:448e50.
10. Threlfall EJ, de Pinna E, Day M, Lawrence J, Jones J. Alter-natives to ciprofloxacin use for enteric fever, United Kingdom[letter]. Emerg Infect Dis 2008;14:860e1.
11. Kings Fund Briefing: Payment by Results. www.kingsfund.org.uk/document.rm?idZ7210. (accessed 24 February 2011).
12. 2010e2011 National mandatory tariffs for admitted patientcare. Department of Health, www.dh.gov.uk; 2010 (accessed24 February 2011).
13. Steinberg EB, Bishop R, Haber P, Dempsey AF, Hoekstra RM,Nelson JM, et al. Typhoid fever in travellers: who should betargeted for prevention? Clin Infect Dis 2004;39:186e91.
14. Angell SY, CetronMS. Health disparities among travellers visitingfriends and relatives abroad. Ann Intern Med 2005;142:67e72.
15. Butler T, Frenck RW, Johnson RB, Khakhria R. In vitro effects ofazithromycin on Salmonella typhi: early inhibition by concen-trations less than the MIC and reduction of MIC by alkaline pHand small inocula. J Antimicrob Chemother 2001;47:455e8.
16. Capoor MR, Rawat D, Nair D, Hasan AS, Deb M, Aggarwal P,et al. In vitro activity of azithromycin, newer quinolones andcephalosporins in ciprofloxacin-resistant Salmonella causingenteric fever. J Med Microbiol 2007;56:1490e4.
17. Audit Commission. Improving data quality in the NHS report,www.audit-commission.gov.uk; 2010 (accessed 24 February2011).