epidemiologic dental the interpretation clinical...
TRANSCRIPT

Aug., 1951
Epidemiologic Studies in Dental Caries,III: The Interpretation of Clinical Data
Relating to Caries Advance*tJULIAN D. BOYD, M.D., AND KENNETH E. WESSELS, D.D.S.Department of Pediatrics, College of Medicine; and Department of Pedodontics,
College of Dentistry, State University of Iowa, Iowa City, Ia.
TWENTY-FIVE years ago we firstobserved that children with diabetes
mellitus tended to have less advknce oftooth decay than does the usual child.'Further observations indicated that suchfreedom from advancing decay was con-ditioned. by the degree in which thechild's food intake approached acceptednutritional standards, and in which hisdiabetic anomaly was controlled throughthe use of insulin.2 Within two monthsafter the routine of diet and insulinmanagement had been established, opencavities would become stony hard attheir base, and no new cavities woulddevelop. Among diabetic children whofailed to observe the prescribed regimen,caries tended to appear and to advanceas rapidly or more rapidly than in theaverage child. The serial dental datafor a group of diabetic girls are sum-marized in the first chart (Figure 1).Each horizontal bar represents thedental course of one child for successiveyears; the zones shaded black representperiods when no new caries could be de-tected. It will be noted that most of theperiods of observation were character-ized by non-advance of caries, and thatthe total increment of new caries wasvery low.8
* Piesented at a Joint Session of the Dental Healthand Food and Nutrition Sections of the American PublicHealth Association at the Seventy-eighth Annual Meet-ing in St. Louis, Mo., November 2, 1950.
t This study was made possible through a grantfrom the Sugar Research Foundation.
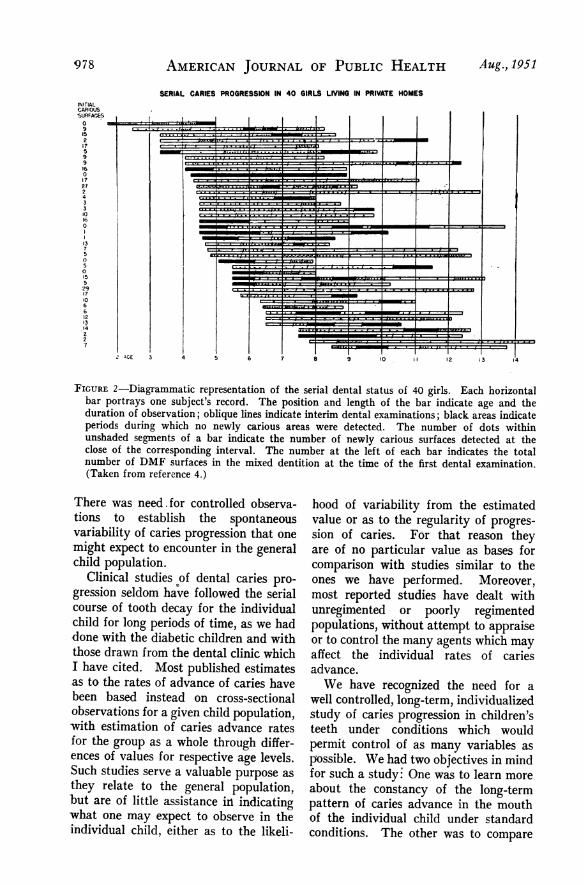
To serve as an index of the common-ness of such findings among non-diabeticchildren, we reviewed the dental recordsof 100 school children who had beencared for at the university dental in-firmary for not less than three consecu-tive years. The graphic record of the40 girls from this series is shown in thenext chart (Figure 2). It will be notedthat most subjects had some periodsof non-advance of caries, but that cariesprogression was the rule and that formost of them the caries increment wasnotable from one year to the next.4
Influenced by the published work ofBeust5 and of Bodecker,6 we had inter-preted the hardening at the bases of theopen cavities as evidence of depositionof sclerotic dentin. Occasional histologicstudies of teeth which clinically haddeveloped arrest of caries showed thatthe dentin lying between the enameldefect and the pulp had become denseand stain-resistant. Naturally shed,deciduous teeth of children who had beenunder diabetic management for longperiods before exfoliation showed dentinmore completely sclerosed than is cus-tomary in children's teeth: more nearlyanalogous to the sclerosed dentin of thepermanent teeth of adults. We believedthat caries had become arrested in thediabetic patient's teeth through theeffect of homeostatic mechanisms work-ing from within the tooth. This beliefhas led to the premise that the body
[9761

DENTAL CARIES
LONG TERM DENTAL RECORDS OF 59 DIABETIC GIRLS
6I
I 1 1 f 12 i1
'I -I- I I
* I'I~~~~~~~~~~~~~~~~~~~~.I,.
FIGURE 1-Individual records of progressive dental status of 59 girls with diabetes mellitus.Length of each bar indicates duration of intermittent dental observation; solid black areasrepresent periods of freedom from new dental lesions; unshaded areas contain symbols toindicate number of tooth surfaces with new lesions which appeared during the correspondingperiod. Symbols have meanings as follows: diagonal line, one dmf (deciduous) tooth surface;crossed diagonal lines, one DMF (permanent) surface; dot, one surface with a precariouslesion apparently limited to the enamel (preponderantly pits and fissures, developmental inorigin, present when tooth first erupted). Intervals of prolonged non-observation are indicatedby a horizontal line through the bar. The duration of diabetes mellitus prior to the initialdental examination is indicated by the length of the single horizontal line to the left of eachbar graph. (DMF signifies decayed, missing or filled). (Taken from reference 3.)
possesses natural defense mechanismswhich can prevent the development orthe advance of tooth decay if propermetabolic conditions can be maintained.
This concept of natural defensemechanisms for the tooth has beendifficult to reconcile with the classic ex-pression of the chemico.-parasitic theoryof caries causation. Most individualsholding to the regional concept of cariescausation have assumed that the eruptedtooth is an inert structure, incapable ofchange of composition through inter-
change with the internal fluids of thebody. Proponents of the chemico-para-sitic theory explained our findings indiabetic children's teeth as dependent onthe prohibition of sugar from diabeticdiets. We had observed numerous in-stances where dental caries came toarrest among children who were notdiabetic and who had continued to in-gest sugar, but our data were not suffi-cient in numbers nor were the variablefactors controlled sufficiently to givestatistical significance to these findings.
AGE
___ >
_~ .'
I I5 6 7 a 9 10
Em"e=
4~'~ _
977Vol. 41
AMERICAN JOURNAL OF PUBLIC HEALTH
SERIAL CARIES PROGRESSION IN 40 GIRLS LIVING IN PRIVATE HOMES
--....... .. . _ _
K:zJ
=--
$ I. =
=
..I. . . I.... _ ,,_, n
.1
]FIGURE 2-Diagrammatic representation of the serial dental status of 40 girls. Each horizontalbar portrays one subject's record. The position and length of the bar indicate age and theduration of observation; oblique lines indicate interim dental examinations; black areas indicateperiods during which no newly carious areas were detected. The number of dots withinunshaded segments of a bar indicate the number of newly carious surfaces detected at theclose of the corresponding interval. The number at the left of each bar indicates the totalnumber of DMF surfaces in the mixed dentition at the time of the first dental examination.(Taken from reference 4.)
There was need. for controlled observa-tions to establish the spontaneousvariability of caries progression that onemight expect to encounter in the generalchild population.
Clinical studies of dental caries pro-gression seldom have followed the serialcourse of tooth decay for the individualchild for long periods of time, as we haddone with the diabetic children and withthose drawn from the dental clinic whichI have cited. Most published estimatesas to the rates of advance of caries havebeen based instead on cross-sectionalobservations for a given child population,with estimation of caries advance ratesfor the group as a whole through differ-ences of values for respective age levels.Such studies serve a valuable purpose as
they relate to the general population,but are of little assistance in indicatingwhat one may expect to observe in theindividual child, either as to the likeli-
hood of variability from the estimatedvalue or as to the regularity of progres-sion of caries. For that reason theyare of no particular value as bases forcomparison with studies similar to theones we have performed. Moreover,most reported studies have dealt withunregimented or poorly regimentedpopulations, without attempt to appraiseor to control the many agents which mayaffect the individual rates of cariesadvance.We have recognized the need for a
well controlled, long-term, individualizedstudy of caries progression in children'steeth under conditions which wouldpermit control of as many variables aspossible. We had two objectives in mindfor such a study.: One was to learn moreabout the constancy of the long-termpattern of caries advance in the mouthof the individual child under standardconditions. The other was to compare
NITIALCARIOUS-SURFACES0
915217599160
172724331016
1 1 . I L@_ 1.1-<---_ X * t * z * t | 8 . f . . ............... , . L * - t * 3...... .... .1 . . _ I . f. 7==:=_ _t..tJ. .._ f . . 1.. -. . . . 1 .- . . . t /' - *_g * , ... J'.' ..................................... s o$ z t-.--; _ _r. . . . . . . J . ^ . . . . , . . , . . , . _ .l .i ..... ... z - i ..... ; v .. _7 .. ^ __ 3=, .
w
.... . ., - ,. r h X :;j.w ... n , . .. -.-. . . . . . .......................... .. . . . . , . . . . . . . . ......................... . . . . . . . . . .sm .............. ,. ;.'*_' .. .... ...,.. .,...; ,, ..... , ...... ... . .a . , ... , -, - _... ....... .... | . , ., , . ,5 ! . i w ] TTT_ T . _ . . .
t' * i * _*1 .vis =e . -S. A .... 1 . : .... - . . . w . . , f_ z ,.* *-i ,.-. ........ ........ 1 * - t-- , ............................. *.. ....-
. .. I .1 ..
.W1.
-4
C=
5 6 7 a
978 Aug., 1951

DENTAL CARIES
the rate and pattern of caries advanceamong children whose sugar intake wasmanipulated widely, with the correspond-ing pattern before and after the dietregimentation had been in effect, as wellas with the rate and pattern observedconcurrently in a group of control sub-jects.When opportunity permitted, we
undertook such a study. To meet theexacting requirements as fully as possi-ble, it was necessary to use subjectsalready living under conditions oflimited regimentation. The most appro-priate group for our purpose was thatto be found in one of our state schoolsfor the mentally retarded. Out of apopulation of about 2,000 persons of allages, we found 250 boys and girls be-tween the ages of 13 and 20 years.This age group seemed best for studybecause it avoided the consideration ofdeciduous teeth. We would have pre-ferred greater uniformity of age, butwe needed more subjects than could beprovided with a narrower age range.Not many more than 200 proved to havecapacities for adequate cooperation inour study. The experimental subjectswere chosen from the girls; the remain-ing girls and the boys served as separatecontrol groups. This report will belimited primarily to consideration of theexperimental and control groups of girlsubjects (Table 1).
During midsummer of 1946 the initialdental examinations were made. Similarexaminations have been made severaltimes each year since then, and theystill are in progress. As a corollary ofthe dental examinations, estimations ofLactobacillus frequency in saliva havebeen made recurrently for most of thesubjects. During the first two yearsof the study we were able to establishrates for the spontaneous advance ofcaries for each subject while all phasesof institutional life still remained un-modified.
During the second year, about 70 of
, TABLE 1
Initial Status of Girls Who Comprised theExperimental and Control Groups, and Num-ber of Dental Examinations Each Year of
StudyExperimental Control
Group Group
Number of subjectsAge when first examined
(months): 1st quartileMedian3rd quartile
Initial number of DMF toothsurfaces: MeanS.D.
Filled tooth surfaces: % oftotal number of carioussurfaces
Incidence of poor dentalhygiene
Number of dental examinationsmade during each of the fouryears of the study: 1946-19471947-19481948-19491949-1950
64 52
153 148178 190193 208
7.6 8.34.3 6.1
22% 19%
25% 40%
129173254118
19717613160
the girls were chosen from the group asa whole to serve as a pool from whichthe experimental personnel would bedrawn. Graduate dietitians appraisedthe diet practices at the institution andstudied means for bringing the qualityof food intake for the experimentalgroup up to the National ResearchCouncil's recommendations. Two setsof menus were prepared, relatively con-stant as to content of protein, minerals,vitamins, and caloric equivalence, butso designed that one set avoided the useof any refined sugar or its products,while the other provided not less thanthree ounces of sucrose daily, usuallyas a constituent of foods, sometimes ascandy which would be eaten at the tablewith the meal. Foods not availablethrough the institution were purchasedor else were furnished through thecourtesy of various agencies.* Furtherdetails relating to the routine of man-agement have been published.7The diets devoid of refined sugar were
* We are indebted to the Pineapple Research Insti-tution of Hawaii, to the Io*a Dairy Industry Com-mission, and to the Vitex Corporation for the provision*of pineapple juice, dried skim milk, apd Vitamin Dconcentrate, respectively.
Vol. 41 979
AMERICAN JOURNAL OF PUBLIC HEALTH
t TABLE 2
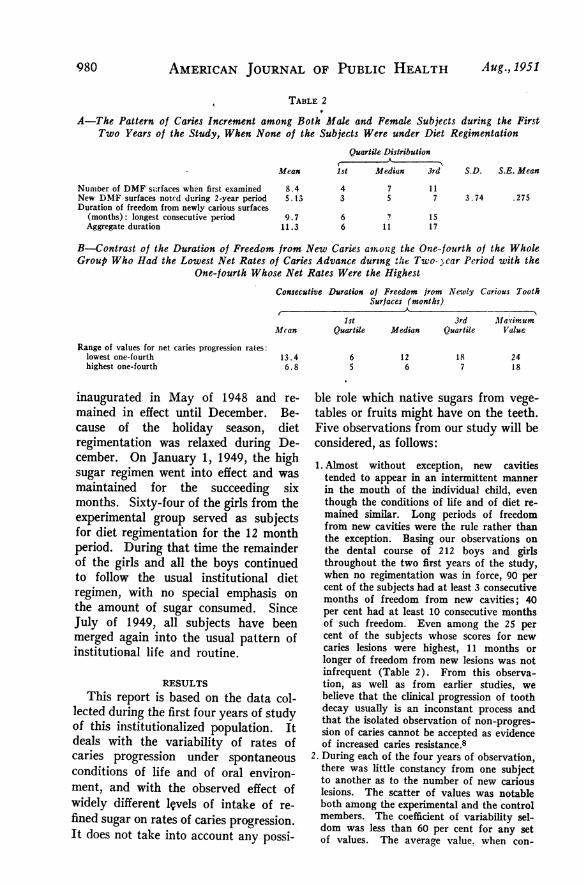
A-The Pattern of Caries Increment among Both Alale and Female Subjects during the FirstTwo Years of the Study, When None of the Subjects Were under Diet Regimentation
Quartile Distributiont A
Mean lst Median 3rd S.D. S.E. Mean
Number of DMF surfaces when first examinedNew DMF surfaces notcd during 2-year periodDuration of freedom from newly carious surfaces
(months): longest consecutive periodAggregate duration
8.45.13
4 7 113 5 7 3.74 .275
9.7 6 ? 1511.3 6 11 17
B-Contrast of the Duration of Freedom from New Caries am^on;g the One-fourth of the WholeGroup Who Had the Lowest Net Rates of Caries Advance during the Two- car Period with the
One-fourth Whose Net Rates Were the HighestConsecutive Duration of Freedom from Newly Carious Tootk
Surfaces (months)-A Ak
1stMcan Quartile
Range of values for net caries progression rates:lowest one-fourth 13.4highest one-fourth 6. 8
inaugurated in May of 1948 and re-mained in effect until December. Be-cause of the holiday season, dietregimentation was relaxed during De-cember. On January 1, 1949, the highsugar regimen went into effect and wasmaintained for the succeeding sixmonths. Sixty-four of the girls from theexperimental group served as subjectsfor diet regimentation for the 12 monthperiod. During that time the remainderof the girls and all the boys continuedto follow the usual institutional dietregimen, with no special emphasis onthe amount of sugar consumed. SinceJuly of 1949, all subjects have beenmerged again into the usual pattern ofinstitutional life and routine.
RESULTSThis report is based on the data col-
lected during the first four years of studyof this institutionalized population. Itdeals with the variability of rates ofcaries progression under spontaneousconditions of life and of oral environ-ment, and with the observed effect ofwidely different l1vels of intake of re-fined sugar on rates of caries progression.It does not take into account any possi-
3rd allaCirumMedian Quartile Value
6 12 18 245 6 7 18
ble role which native sugars from vege-tables or fruits might have on the teeth.Five observations from our study will beconsidered, as follows:1. Almost without exception, new cavitiestended to appear in an intermittent mannerin the mouth of the individual child, eventhough the conditions of life and of diet re-mained similar. Long periods of freedomfrom new cavities were the rule rather thanthe exception. Basing our observations onthe dental course of 212 boys and girlsthroughout the two first years of the study,when no regimentation was in force, 90 percent of the subjects had at least 3 consecutivemonths of freedom from new cavities; 40per cent had at least 10 consecutive monthsof such freedom. Even among the 25 percent of the subjects whose scores for newcaries lesions were highest, 11 months orlonger of freedom from new lesions was notinfrequent (Table 2). From this observa-tion, as well as from earlier studies, webelieve that the clinical progression of toothdecay usually is an inconstant process andthat the isolated observation of non-progres-sion of caries cannot be accepted as evidenceof increased caries resistance.8
2. During each of the four years of observation,there was little constancy from one subjectto another as to the number of new cariouslesions. The scatter of values was notableboth among the experimental and the controlmembers. The coefficient of variability sel-dom was less than 60 per cent for any setof values. The average value. when con-
980 Aug., 1951

DENTAL CARIES 981
TABLE 3
Average Number of Newly Affected Tooth Surfaces During Each of Four Successive Years ofObservation of the Girls from the Experimental and the Control Groups
Nature of Diet Control1'ear of , A
Study Experimental Group Control Group
.A-Beginning with Midsummer, 1946:
First Unmodified UnmodifiedSecond Unmodified Unmodified'Third No refined sugar for Unmodified
6 months; then 3oz. sucrose daily forthe next 6 months
Fourth Unmodified Unmodified
B-Beginning with Midwinter, 1946:
-First Unmodified Unmodified-Second First 6 months un- Unmodified
modified; then norefined sugar forthe next 6 months
'Third 3 ounces sucrose daily Unmodifiedfor 6 months; un-modified diet forthe next 6 months
Number of New DMF Tooth Surfaces Per AnnumExperimental Group Control Group
Ar),kA
Mean S.D. S.E. Mean Mean S.D. S.E. Mean
2.82 2.46 0.43 3.0 1.8 0.393.02 2.30 0.346 3.12 2.1 0.4464.9 1.03 0.134 5.62 4.90 0.83
3.56 2.54 0.352 2.39 2.44 0.508
2.6 2.32 0.34 3.5 1.6 0.345.2 4.1 0.55 5.6 3.2 0.70
3.2 2.26 0.31 4.0 4.35 1-06
TABLE 4
Analysis of Variability of Rates of Caries Progression for Experimental and forControl Groups for the Same Year *
-A-For the Four Successive Years Beginning With Midsummer of 1946:
Mean Value, Difference S.E., Diff. C
New DMF TS of Means of Means
.First yearExperimental group 2.82Control group 3.0 -0.18 0.58
-Second yearExperimental group 3.02Control group 3.12 -0.10 0.565
Third yearExperimental group 4.9Control group 5.62 -0.72 0.93
-Fourth yearExperimental group 3.56Control group 2.39 + 1.17 0.62
B-For the Three Successive Years Beginning With Midwinter, 1Q46:
First yearExperimental group 2.6Control group 3.5 -0 9 0.48
:Second yearExperimental group 5.2Control group 5.6 -0.4 0.89 0
Third yearExperimental group 3.2Control group 4.0 -0 8 1.43 0
* Based on data from Table 3.
CriticalRatio
0.31
).178
0.775
1.88
.87
.45
.56
Vol. 41

AMERICAN JOURNAL OF PUBLIC HEALTH
TABLE 5
Analysis of Variability of Rates of Caries Progression for the Same Group ofSubjects During Successive Years *
A-For the Four Successive Years Beginning With Midsummer. 1946:
Contrasted Years:
1:2 1:3 1:4 2:3 2:4
Experimental group:Diffensnce of meansStandard error, difference of means
Critical ratioControl group:
Difference of meansStandard error, difference of means
Critical ratio
0.20 2.08 0.74 1.88 0.540.55 0.605 0.555 0.548 0.4940.364 3.44 1.33 3.43 1.09
0.12 2.62 0.610.91 1.1 0.950.12 2.38 0.64
2.50 0.731.17 0.982.14 0.745
B-For the Three Successive Years Beginning With Midwinter, 1946:
Contrasted Years
1:2 1:3 2:3
Experimental group:Difference of meansStandard error, difference of means
Critical ratioControl group:
Difference of meansStandard error, difference of means
Critical ratio
* Based on data from Table 3.
sidered together with the standard deviation,served to indicate the course of the entiregroup but was of little value for predictingthe course of any individual subject (Table3).
3. Using the average number of newly carioussurfaces within each group for each yearas a criterion, there was great variabilityfrom one year to another, both for the ex-perimental and for the control groups. Fora given year, the type and degree of oscilla-tion of the average value tended to beparallel for the experimental and the controlgroups. Even among the subjects who wereunder no manner of imposed regimentation,and who seemed to be living under com-parable conditions throughout the fouryears of the study, the differences of themeans from one year to another presentedsignificant differences (Table 4).
4. The differences between the experimentalsubjects and the control group during theperiods of contrasted diet tended to besmaller than those between either of thegroups' values for successive years of thestudy. There was no significant differenceas to the average rate of caries advance be-tween the experimental and the controlgroup, either for the year of sugar manipula-tion or for the next year. Moreover, whenthe 12 month period of sugar manipulation
2.6 0.6 2.00.65 1.04 0.6334.0 0.58 3.15
2.1 0.5 1.60.79 1.236 1.272.66 0.49 1.26
was redivided so that the 6 months of sugarabstention were included with the 6 monthsof unmodifie(I diet which preceded them,and similarly the 6 months of high sugaringestion were included with the next 6months of unmodified diet, still there wasno significant difference between the meanvalues. The pattern of frequency distribu-tion of individual values within the twogroups also was similar (Table 5).
5. We have not been able to demonstrate any-significant relationship between the numberof Lactobacilli in the saliva of our subjectsand the respective rate of caries advance dur-ing the year which preceded, coincided with,or followed the collection of the salivasamples. No significant difference was evi-dent when the average values for newcaries among those with zero counts werecompared with those with counts exceeding30,000 Lactobacilli per ml. of saliva.9
DISCUSSIONMany fundamental questions relating
to dental caries as a human disease re-main unanswered. Answers often havebeen taken for granted, even amongstudents of dental caries, and the errorsof interpretation which have resulted
982 Aug., 1951

DENTAL CARIES
have deprived various critical studieson caries progression of the meaningwhich they might otherwise haveafforded. Further carefully controlledstudies will be needed to establishanswers to these basic questions, and itis important that such studies be so de-signed that as many variables as possiblebe avoided, or their potential effect onthe outcome properly weighted. If not,the summated effect of the uncontrolledvariables may well outweigh the differ-ences ascribed to the agent being investi-gated.One important question calling for
answer is the length of time which mustelapse before an agent being investi-gated can lead to clinically recognizablecaries. Another equally important ques-tion deals with the course of the cariouslesion once initiated: Is its progressinexorable? Is it steady? Under whatcircumstances can it be brought to arrest,and how can the observer recognize sucharrest?
These recent studies of ours illustratethe variability of caries progression fromindividual to individual and the varia-bility in the mouth of a given subjectfrom month to month under supposedlystandard conditions. Many studiespreviously reported have ignored thelikelihood of latency of response ofteeth to change; have assumed con-stancy of caries progression; have failedto establish patterns of caries advancefor members of their study groups priorto the regimentation of their experi-mental subjects; and have depended onpreviously determined rates of cariesadvance as control values for the cur-rent studies. Our observations indicatethat such techniques can lead to falseinterpretations of the efficacy of anyregimen being studied.
Consideration also should be given tothe initial state of the teeth before ex-perimental conditions have been im-posed. If one is measuring cariesadvance in terms of the rate of appear-
ance of newly carious areas, then oppor-tunities for advance are limited by thenuu-ber of teeth or tooth surfaces whichinitially are free from caries attack atthe outset of the study. Likewise onemay expect a difference in results onthe basis of the number of susceptibletooth surfaces which have been filledprior to the start of the study.Even more important as potential
sources of experimental error are thenature and amount of reparative dentalservices which the patient receives whilethe study is in progress. The placementof fillings is itself a technique employedto lessen caries progression. Conse-quently we should not compare cariesprogression rates among children whosepatterns of initial or concurrent dentalrepair differed significantly. The authorshave been impressed by the general lackof consideration of these importantfactors by experimenters in their choiceof samples for the study of caries ad-vance. Our own subjects had receivedonly minimal amounts of dental repairprior to the beginning of our study, andduring its course only emergencyreparative services were given. Cavitiesinitially present remained untreated andunfilled throughout the course of thestudy unless they caused the child mani-fest discomfort.Even criteria for the diagnosis of
dental caries are inconstant. Theremay be widespread disagreement amongexamining dentists as to whether or nota specific dental lesion is carious.Serial examinations of the same tooth,even though made by the same examinerat different times, may result in differentinterpretations from one examination toanother as to whether a break in thecontinuity of the enamel represents theearly stage of a cavity or whether it isa developmental defect. When a seriesof examiners is used and each employshis own criterion of judgment and tech-nique of examination, the results for thetotal caries score for a given mouth may
Vol.41 983
AMERICAN JOURNAL OF PUBLIC HEALTH Aug., 1951
differ by as much as 100 per cent.10In serial examinations, cavities once de-scribed may disappear from the record,due to a change in interpretation.
Such statistical dilemmas have led usto adopt the serial consideration of eachtooth surface as a measure of caries ad--vance, rather than to place dependenceon the serial total values for affectedtooth surfaces for a given mouth. Wetake into consideration also the extentof the described dental lesion. Mostexaminers make no distinction in theirreports between an incipient cavity andone which has become unmistakable. Asa consequence, the total caries score mayvary widely through errors of judgmentpossibly greater in degree than the dif-ference which the examiner ascribes tosome agent he has been testing for itspower to affect caries progression.
Thus there are many potential sourcesof error in clinical studies relating torates of caries advance. The summa-tion of such errors can lead to manifestmistakes of interpretation. It becomesnecessary to choose techniques of sam--pling and of control, of examination andof record, which are as stringent as theobjective of the study requires if dataof value are to be obtained. Considera-tion of affected tooth surfaces or ofindividual caries lesions is more reliableas an estimate of cadies progression thanis the limitation of attention to thenumber of affected teeth.Our own data permit us to distinguish
caries progression on the basis of thesize, depth, location, and consistencyof each carious area listed in our records.The serial study of specific teeth willeliminate many errors which otherwisemight arise from the faulty interpreta-tion of individual caries lesions. Whenit is possible to express results clearlyand individually for respective teeth,this seems a better statistical approachthan to lose identity of teeth or even ofsubjects through the merging of data interms of group averages.
SUMMARY AND CONCLUSIONSTime does not permit any further ex-
ploration of sources of potential errorswhich are inherent in dental data. Wehave tried to illustrate the errors whichmay be concealed in dental statistics andto lead the reader to question the resultsof reported dental studies until thevalidity of the experimental conditions,as well as of the conclusions, has beenestablished. In view of the fact thatspontaneous variability from one childto another is great, and that such vari-ability seldom is given consideration inclinical studies of caries progression,there is reason to question those reportswhich have attributed beneficial orharmful effects on the teeth to the useof any specific agency.
Within specific limitations of investi-gation, we have been unable to demon-strate differences in the caries advancerates among adolescent children whenthe ingestion of refined sugar was arbi-trarily prohibited or was given daily inlarge amounts. However we wish todraw attention to these limits of ourobservations, and request that no in-ferences be drawn which lie beyond theconditions of our study. These condi-tions are as follows:
a. The study dealt with altered intake of re-fined sugar and its products only; duringboth periods of diet control our subjectsreceived liberal amounts of the sugars whichare native constituents of vegetables andfruits.
b. During the period of high sugar ingestion,the sugar was given only with meals, andusually as a constituent of prepared foods.
c. The girls receiving the diets of altered sugarcontent were under a regimen which wasdesigned to provide a complete diet, bothquantitatively and qualitatively. The caloricallowance was constant during the periods ofcontrasted sucrose intake.
d. Lactobacillus counts proved to offer no re-liable index of the likelihood or the ratesof caries progression among our subjects,either among those under diet regimentationor- among the members of the control groups.
REFERENCES1. Boyd, Julian D., and Drain, C. L. The Arrest of

Vol.41 DENTAL CARIES 985
Dental Caries in Childhood. J. A. M. A. 90:1867(June 9), 1928.
2. Boyd, Julian D., Drain, C. L., and Nelson, M.Dietary Control of Dental Caries. Am. J. Dis. Child.38:721 (Oct.), 1929.
3. Boyd, Julian D. Long Term Control of DentalCaries among Diabetic Children. Am. J. Dis. Child.66:349 (Oct.), 1943.
4. Boyd, Julian D., and Cheyne, V. D. EpidemiologicStudies in Dental Caries: I. The Pattern of DentalCaries in Iowa City Children. J. Pediat. 29:157(Aug.), 1946.
S. von Beust, Th. A Contribution to the Study ofImmunity to Dental Caries. Dental Cosmos.54:659 (June), 1912; Demonstration of Sclerosisof Dentin in Tooth Maturation and Caries. Ibid.76:305 (Mar.), 1934.
6. Bodecker, C. F., and Applebaum, E. Metabolismof Dentin: Its Relationship to Dental Caries andto the Treatment of Sensitive Teeth. Dental Cosmos.73:995 (Oct.), 1931.
Bodecker, C. F. Nutrition of the Dental Tissues.Am. J. Dis. Child. 43:416 (Feb.), 1932.
7. Boyd, Julian D., and Cheyne, V. D. EpidemiologicStudies in Dental Caries: II. The Incidence ofCaries among Institutionalized Children. J. Pediat.31:306 (Sept.), 1947;Boyd, Julian D., Cheyne, V. D., and Wessels, K. E.Long Term Studies of Dental Caries Progressionamong Teen-Aged Inmates of a Custodial Insti-tution. J. Calif. State Dent. A. 26:30 (May-June),1950: supplementary issue.
8. Boyd, Julian D., Wessels, K. E., and Cheyne, V. D.Normal Discontinuity of Progression of DentalCaries. Proc. Soc. Exper. Biol. & Med. 73:285(Feb.), 1950.
9. Idem. Is the Salivary Lactobacillus Count a ValidIndex of Activity of Dental Caries? Proc. Soc.Exper. Biol. & Med. 71:535 (Aug.), 1949.
10. Dunning, J. M. Variability in Dental Caries Ex-perience and its Implicationr upon Sample Size.J. Dent. Research 29:541 (Aug.), 1950.
White House Conference ContinuesA committee to carry out the ob-
jectives of the Mid-Century WhiteHouse Conference on Children andYouth has been formed. Called theNational Mid-Century Committee forChildren and Youth, its chairman isLeonard . W. Mayo, director of theSociety for the Aid of Crippled Chil-dren, who was also chairman of theexecutive committee of the recent WhiteHouse Conference.The committee will base its program
on the purpose of the White House Con-ference: ". . . to consider how we candevelop in children the mental, emo-tional, and spiritual qualities essentialto individual happiness and to responsi-ble citizenship." It believes a toppriority to be the conservation andstrengthening of family life amid
the stresses of a defense economy.The National Committee will offer
field service to state committees and na-tional organizations with a continuingprogram, to achieve Conference ob-jectives. It will maintain an informa-tion service, and will shortly considerwhat its research program should be inrelation to the many gaps in knowledgeabout how children develop healthypersonalities. Beginning in September,it will publish a bulletin regularly.Elma Phillipson, who was the White
House Conference consultant on na-tional organizations, is executive secre-tary of the new committee, Lois Gratzis its staff field consultant, and BenjaminGoldenberg the information consultant.Offices are at 4th and IndependenceAve., S.W., Washington 25, D. C.