epicardial vt ablation the cleveland clinic experience · pdf filelandor associates created...
TRANSCRIPT
Epicardial VT Ablation The Cleveland Clinic Experience
Walid Saliba, MD, FHRSDirector, EP LabCardiac ElectrophysiologyHeart and Vascular Institute

• Why Epicardial
• Special considerations: Access , Ablation and Complications
• Cleveland Clinic experience
Epicardial Access in the EP Lab

LK
• 45 year old male with palpitations .
• Documented VT on ILR monitioring
• Failed prior endocardial VT ablation
• Investigations: – Echo: mild LV dysfunction LVEF 45-50-%– Non obstructive CAD – Cardiac MRI: No LV/RV scars

Clinical VT: RBBB / LS axis

Endocardial Regional Mapping
Not early

Now What?
• Decision to go Epicardial – Failed Ablation– EKG– NICM– Nothing interesting endocardial
• Anticoagulation Reversed
• Epicardial Access Obtained

Epicardial Mapping
Mid diastolic potential

Coronary Angiography
Prior to Ablation
• Away from coronaries: 5 mm– Selective angiography
• Away from Phrenic nerve– High amplitude pacing
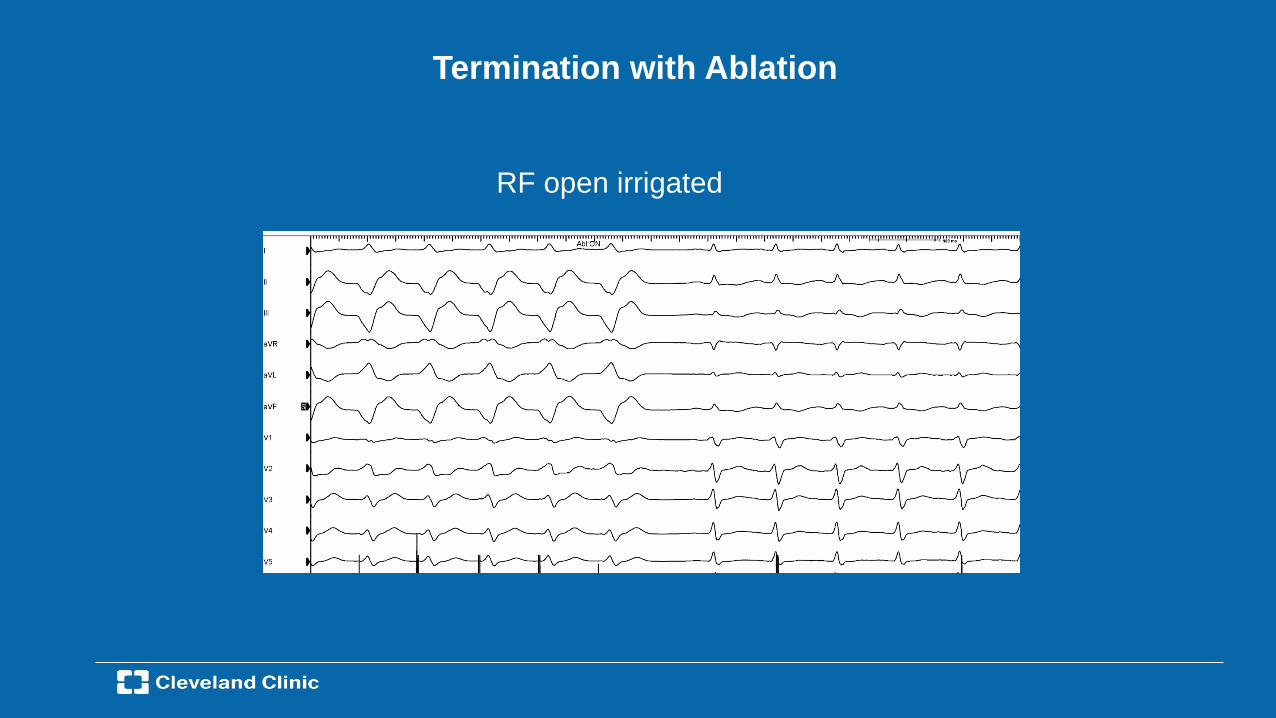
Termination with Ablation
RF open irrigated

Epicardial Ablation: Why
NDCMICM
–Arrhythmia Circuits can be deep–Ablation lesion may not be that deep.

When do you go epicardial?
• The circuit is epicardial or mid-myocardial– Defining the EKG – Interval and Morphology Criteria– Defining the substrate – DCM, ARVC vs. ICM
• Journey to the endocardium has been futile– Failed prior endocardial ablation– No endocardial targets found
• Access to the endocardium not possible/dangerous– Double mechanical valves– Intramural thrombus

When do you go epicardial?
• The circuit is epicardial or mid-myocardial– Defining the EKG – Interval and Morphology Criteria

When do you go epicardial?
• The circuit is epicardial or mid-myocardial– Defining the EKG – Interval and Morphology Criteria– Defining the substrate – DCM, ARVC vs. ICM
Need for epicardial ablation
• ICM: Less Frequent (10-15%)
• NICM: More frequent (30- 50%)
• ARVC: Very Frequent (40- 70%)
• Other: Brugada, sarcoid..? frequent

VT in DCM
1. The scar is greater on the epicardium than on the endocardium.
2. Most Scars localized to base of LV in the perivalvular region.
Endo Map Epic Map
>1.0 mV
<0.5 mV
When do you go epicardial?
• The circuit is epicardial or mid-myocardial– Defining the EKG – Interval and Morphology Criteria– Defining the substrate – DCM, ARVC vs. ICM
• Journey to the endocardium has been futile– Failed prior endocardial ablation– No endocardial targets found
• Access to the endocardium not possible/dangerous– Double mechanical valves– Intramural thrombus

Epicardial Access , Navigation and Ablation

Subxyphoid Epicardial Access Puncture SiteAnatomical Consideration
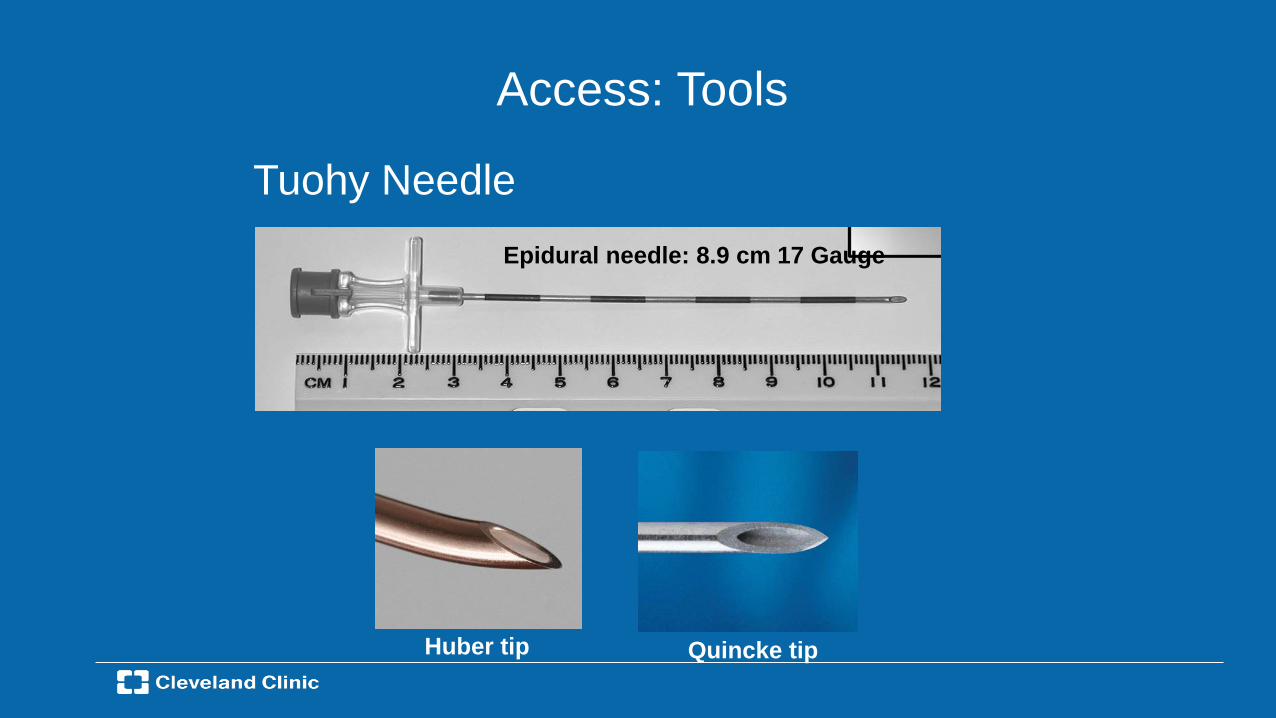
Tuohy NeedleEpidural needle: 8.9 cm 17 Gauge
Access: Tools
Huber tip Quincke tip

Epicardial Puncture and Larrey’s Space
Not Too LowNot Too steep

Intraabdominal Bleeding
Hematoma

Liver Puncture during Epicardial Catheter Ablation
53 y/o female with diagnosis of WPW , AF

Close Call


Inadvertent RV PunctureUp to 30% of cases
Usually Self limitedUsually benign if
Single stick + No anticoagulation + No Sheathing.

Epicardial Access
• Successful Access: 95% Overall
• Failure due to adhesions –Prior Open Heart Surgery:
–Successful in 20-80%
–Repeat access (5 months later)–Successful in ~80%
–Other Issues–Myocarditis-Pericarditis, Prior transmural MI
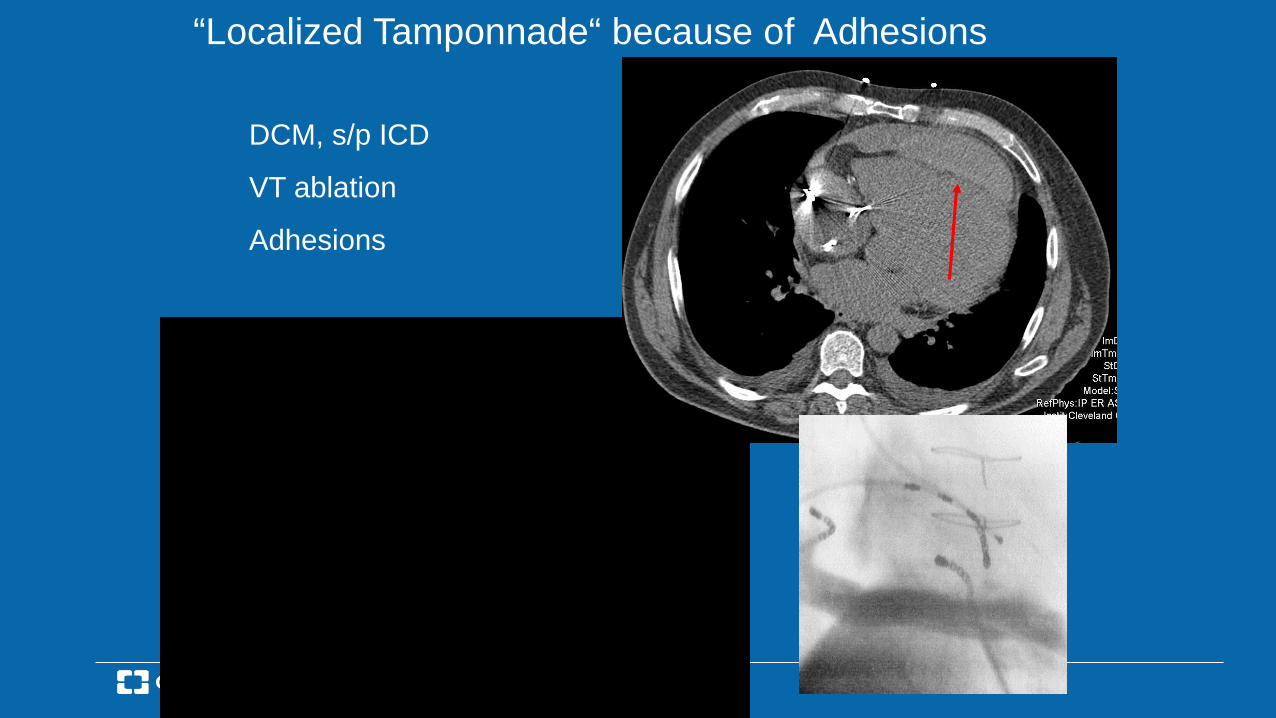
“Localized Tamponnade“ because of Adhesions
DCM, s/p ICD
VT ablation
Adhesions
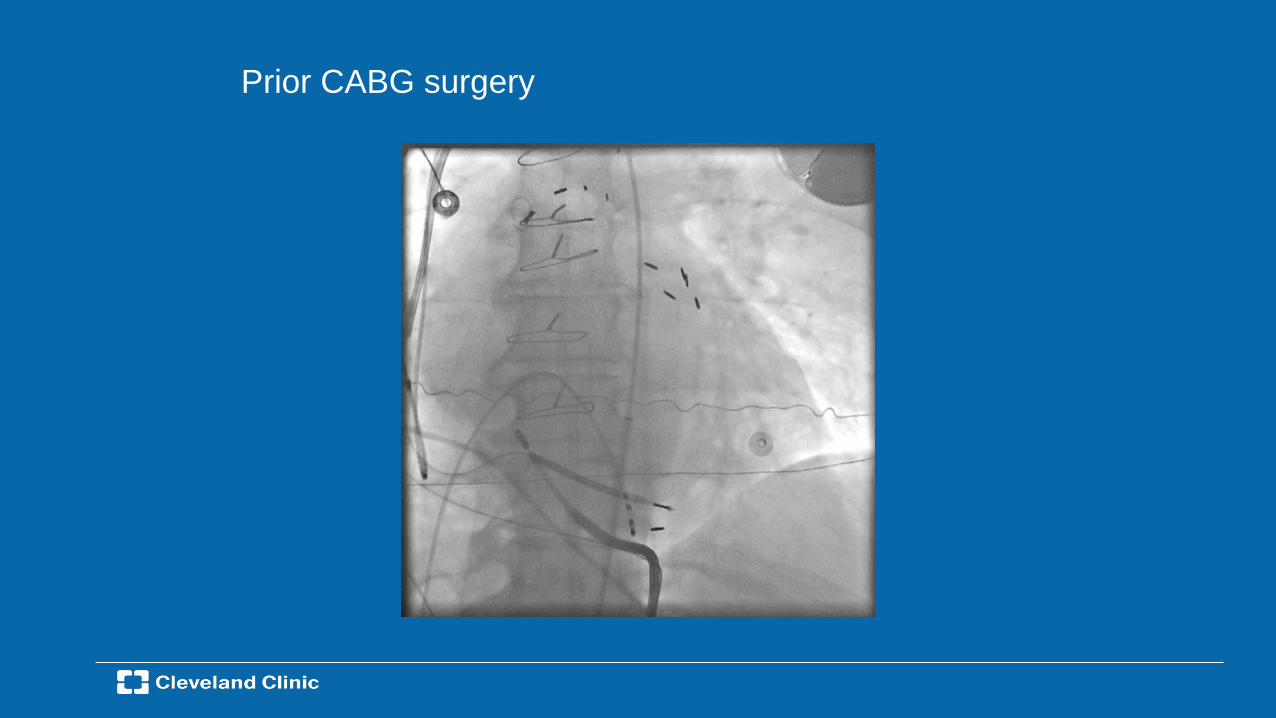
Prior CABG surgery

Epicardial VT Ablation: What Can you access?
• Access available for the majority of the LV / RV epicardial surface.
• Limitations Can’t access– IV septum– Papillary Muscles
– Epicardial LVOT(LV Summit)

Activation Mapping
Distal CS Aortic Cusps Epicardial
LV Summit
42 yo female with incessant NSVT

LV Summit VT

3D Mapping
LV
Epicardial
RVOT
Cusp
CS

Ablation
• Distal CS: Transient success. (Limited energy)• Epicardial: Transient effect• LCC: No effect• RVOT: No effect• LVOT Under the valve: Transient effect (50W)
Surgery• Dissected under the LM• Opened the ascending aorta• Cryo from Epi and Endocardial regions
LM

CCF--Epicardial Ablation• July 2000 – July 2017• 2530 patients referred for VT ablation• 260 (~11%) Epicardial Approach attempted.• Age: 56±3 yrs (15-83); Male 73%• LVEF: 36±2 % (10%-66%); ICD: 63%
12% 22%
30%37%
No SHDOther
Non-Ischemic HD Ischemic HD
SarcoidosisARVDHOCMBrugada…

Changing patterns over the years
• More likely to go epicardial for DCM
• More likely to start epicardial with ARVC
• Less likely to go epicardial for Summit PVC/VT
• Consider pericardial access if large dense scar

Epicardial Mapping
• Incomplete Epicardial map 10%– Adhesions
• Epicardial Mapping ONLY 10%
• Epicardial + Endocardial mapping (85%) Epicardial Before 20%Endocardial Before 65%
Location of Target Site–Epicardial 46%–Endocardial 28%–Epicardial and endocardial 26%
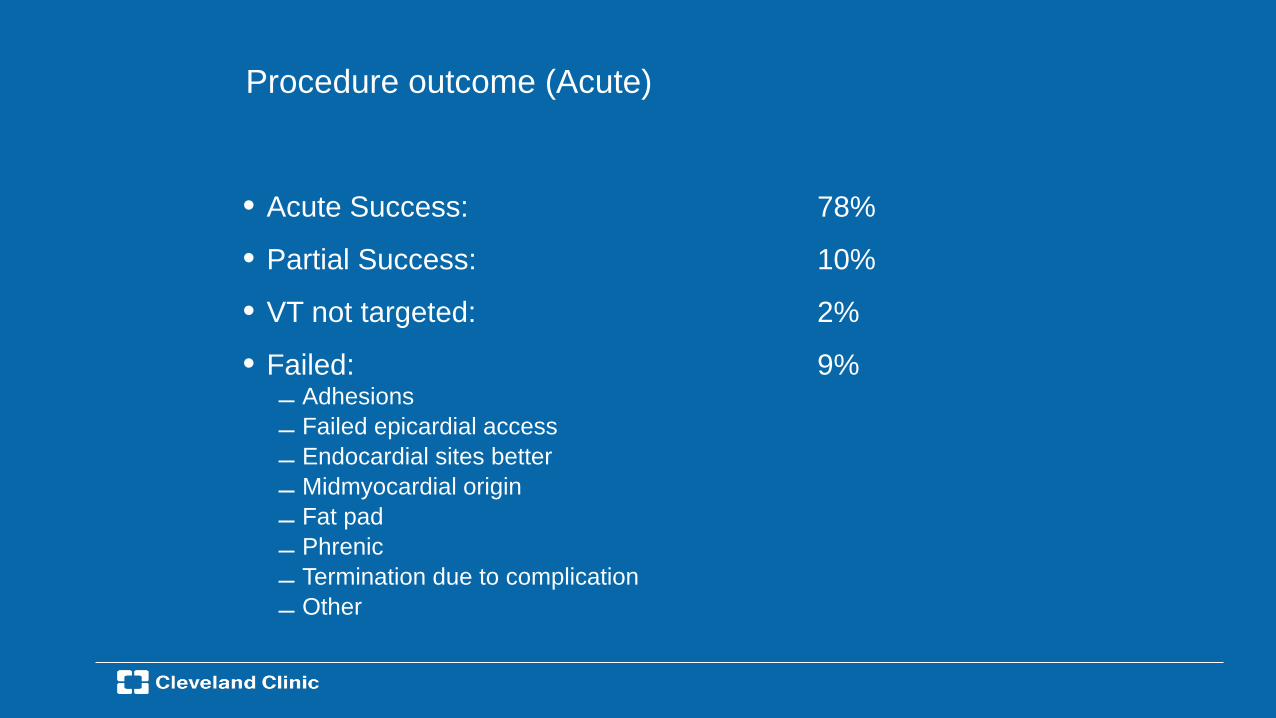
Procedure outcome (Acute)
• Acute Success: 78%
• Partial Success: 10%
• VT not targeted: 2%
• Failed: 9%– Adhesions 14%– Failed epicardial access 10%– Endocardial sites better 49%– Midmyocardial origin 12%– Fat pad 5%– Phrenic 3%– Termination due to complication– Other

• Follow up : 13 months
• Mortality (30 days): 4.3%
• Freedom from VT/ICD shock: 42%
• Redo Procedures (VT Ablation): 8%
(Results for the first 138 pts)
Long Term Outcome
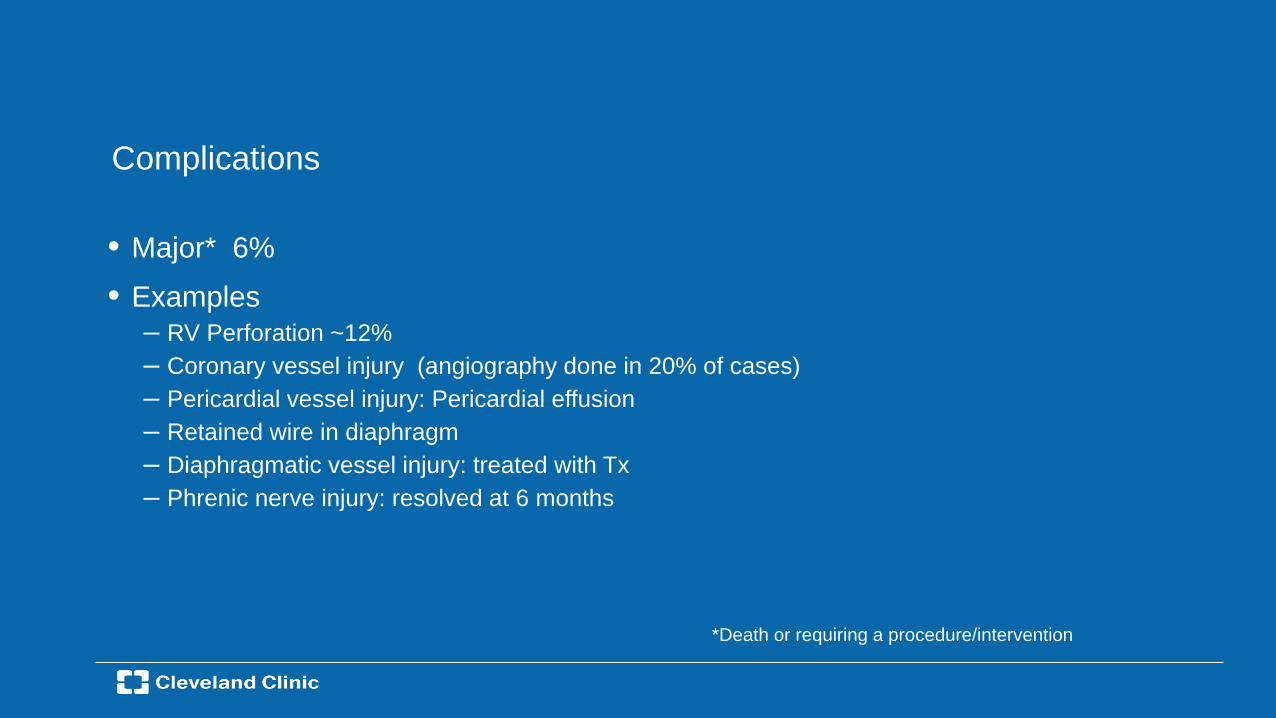
Complications
• Major* 6%• Examples
– RV Perforation ~12%– Coronary vessel injury (angiography done in 20% of cases)– Pericardial vessel injury: Pericardial effusion– Retained wire in diaphragm– Diaphragmatic vessel injury: treated with Tx– Phrenic nerve injury: resolved at 6 months
*Death or requiring a procedure/intervention

Phrenic nerve injury
Pacing Maneuvers
Protective devices
LV
RA
SVC A
o
Balloon
Catheter
Buch et al. Heart Rhythm 2007; 4: 95-98

Delayed complications
• Coronary stenosis (>2 weeks)– Mostly delayed stenosis related to
media hyperplesia
• Pericarditis, Adhesions– IP injection of steroids – 2.0 mg/kg triamcinolone
10 x 4 months after RFA
Triamcinolone 2 mg/kg

Conclusion
• Epicardial access is feasible with a high success rate– Access may be limited secondary to prior surgery
• Ablation target are most frequently epicardial in Nonischemic Cardiomyopathy and ARVC.
• The decision to obtain early epicardial access depends on clinical suspicion: cardiac substrate, EKG and prior endocardial failure.
• Complications of Epicardial Ablation are relatively infrequent but tend to be severe when they occur
• Epicardial fat limits lesion size and mapping accuracy
• Surgical ablation in selected patients (LV summit, coronaries, intramural scar)
• Need for better tools

Thank you