environmentalchemicals williamj. meggs departmentofemergencymedicine, eastcarolina universityschool...
TRANSCRIPT
....-. .~...
Neurogenic Inflammation and Sensitivity toEnvironmental ChemicalsWilliam J. MeggsDepartment of Emergency Medicine, East Carolina University School of Medicine,Greenville, NC 27858 USA
Neurogenic inflammation as a pathway dis-tinct firom iven, immuine-meit-ed infla n m pl a piol leiunderstadn a broad cssof eniomn-*~~~~~~~~~~~~~~6al hedth problm resut fro chemicalexposures. Recen pressing the mediatorsr s, and egulation ofneurogenic inflmmaon is reviewed. Ev-idence for andC tions about "a-ole forneuronic inflammation inesablished dts-Orders such as asha rhinits, cnact de¢r-
~~~~~~~~~~~~~~. .. ... . .matitis, iriehaah,adremtiarthritis are presented. The:-sic buidingsyndrome andm ipl cchemica sivitysyndrome hawbeen defined as:, c d enti-
.... ... .....g: sre ttdisshe :Cu t an e*.existence of chemical irritant recepton....the airwaya-nd sknr disc e;ne renic atin isg from tilaiof chemical in reeptor is a: possiblemodel to explain many of thc aspects ofchemical sen-sitivities. Key s-Mn. ashm,A<:hemicd se£ies~~~~.findoor air puion, mutil chmcll se-
~~~~~~~W
siti*ity syndrome, ..ur.... inla.:: .:.. ::.:..:.... :..... :..:.:...neutral endopepdasereacti.ve.airways dys
fiunction sydoe ecieuppier araysdysfu ion sndme, rhinitis, ssn P,sick building syndrome. Environ HealshPerspece 101: 234-238(1993)
Sensitivity to environmental chemicals ingeneral, and in particular to volatile organ-ic chemicals (VOCs) in indoor air, needsto be elucidated. The lack of an estab-lished mechanism to explain how exposureto concentrations of VOCs that are welltolerated by the population at large canproduce the array of symptoms seen insensitized individuals has hampered pro-gress in understanding these disorders.Over the past few years progress has beenmade in understanding neurogenic in-flammation, chemical irritant receptors,and the regulation of neurogenic inflam-mation. Here I review these topics,emphasizing those aspects that may beapplicable to elucidating the mechanismof chemical sensitivity as a disorder of theregulation of neurogenic inflammation.Possible application to specific clinicalentities is discussed, with suggestions forclinical research to study the association.
Neurogenic InflammationInflammation is an abnormal condition ofredness, swelling, heat, and pain localizedto a tissue. Histologically, inflammationis characterized by edema, vasodilatation,
and infiltrates of leukocytes. A number ofchemical mediators of inflammation havebeen identified biochemically. Inflam-mation may be triggered by the immunesystem, in which foreign materials interactwith leukocyte receptors created after asensitizing exposure to trigger an inflam-matory cascade. Neurogenic inflamma-tion is a well-defined process by whichinflammation is triggered by the nervoussystem.
Early in the study of neurogenic in-flammation, chemical stimulation was rec-ognized as a trigger of neurogenic inflam-mation. As early as 1910, it was recog-nized that the application of mustard oilto the conjunctival sac in experimentalmodels produces inflammation that can beblocked by sensory nerve ablation (1,2).The neuropeptides substance P (SP), neu-rokinen A (NA), and calcitonin gene-relat-ed peptide (CGRP) are now known tocoexist in sensory neurons and to havepotent vasodilatory properties (3-6).Direct stimulation of sensory nerves pro-duces vasodilatation (7,8), which can beblocked by depletion of substance P withcapsaicin (9-11). The sensory fibersinvolved in neurogenic inflammation havebeen identified as C-fibers with a slowvelocity of 1-2 m/sec (14.
Progress has been made in understand-ing the regulation of neurogenic inflam-mation (13). A cell-surface enzyme, neu-tral endopeptidase (NEP), downregulatesneurogenic inflammation by degradatingsubstance P. In the lung this enzyme isinhibited by cigarette smoke, viral infec-tions, and toluene diisocynate, whereascorticosteroids increase NEP.
Neurogenic inflammation is now awell-defined physiological mechanism bywhich mediators are directly released fromsensory nerves to produce-vasodilatation,edema, and other manifestations of in-flammation. The nerve fibers have beenidentified as slow velocity C-fibers, andthe regulation of neurogenic inflammationhas been studied.
Chemical Irritant ReceptorsThe common chemical sense is a nasalsensation provoked by airborne chemicalswhich is distinct from taste and smell(14). This sense is experienced as a burn-ing and painfil sensation in the upper air-ways and eyes upon exposure to irritant
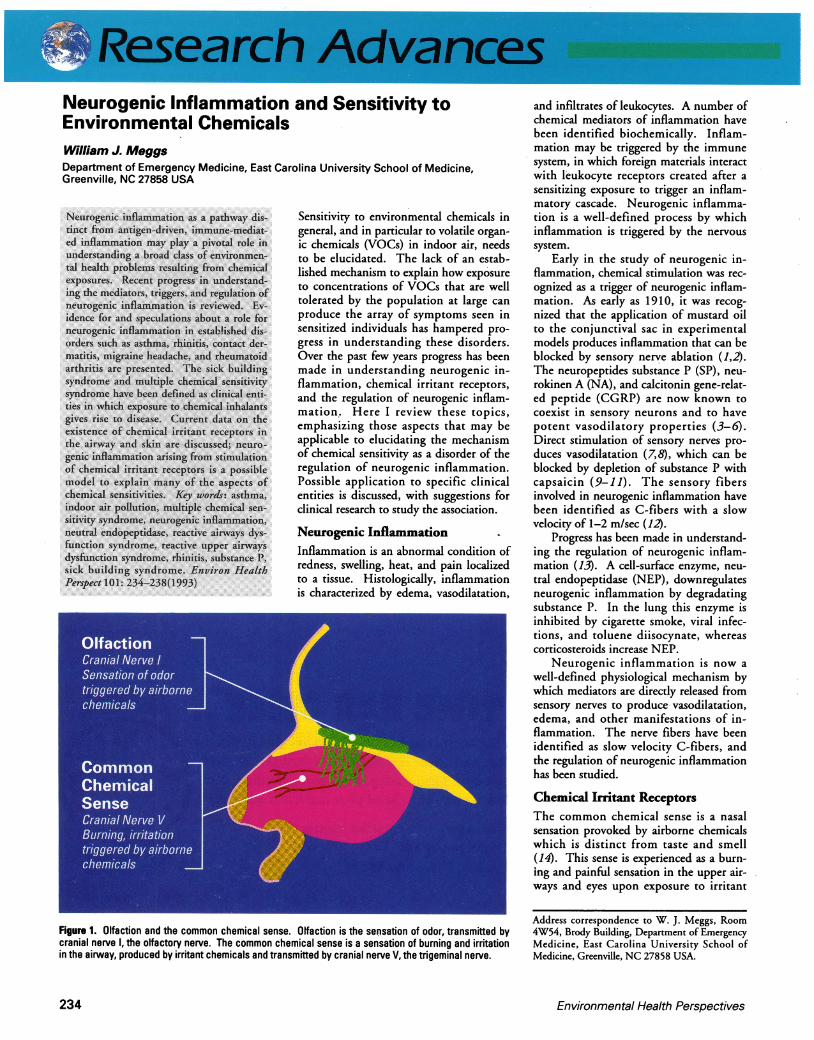
Figure 1. Olfaction and the common chemical sense. Olfaction is the sensation of odor, transmitted bycranial nerve 1, the olfactory nerve. The common chemical sense is a sensation of burning and irritationin the airway, produced by irritant chemicals and transmitted by cranial nerve V, the trigeminal nerve.
Address correspondence to W. J. Meggs, Room4W54, Brody Building, Department of EmergencyMedicine, East Carolina University School ofMedicine, Greenville, NC 27858 USA.
Environmental Health Perspectives234

I.,A - M- - - . --ol~,
Figure 2 Schematc diagram of neurogenic inflammation triggered by chemical irritants. Chemical irri-tants (C) bind chemical irritant receptors on sensory nerves to release substance P (P) and other media-tors from nerve endings. Substance P binds receptors on effector cells to trigger inflammation. Neutralendopeptidase (nep), an enzyme located on the membranes of effector cells, degrades substance P anddownregulates neurogenic inflammation. It is proposed that chemical sensitivity syndromes are disor-ders of the regulation of neurogenic inflammation.
substances and results from exposure oftrigeminal nerve endings to the irritants.The skin and other mucous membraneshave similar responses to irritant chemi-cals. Recent studies in anosmic subjectshave separated the common chemicalsense from olfaction (15). The commonchemical sense and olfaction are depictedin Figure 1. There is evidence that pro-tein receptors on cell membranes are theactivation site for chemical irritants. It isthought that sensory nerves act as bothafferent and efferent nerves for neurogenicinflammation triggered by chemical irri-tants. In the nose, substance P release hasbeen verified for exposures to nicotine,capsaicin, ether, formaldehyde, and ciga-rette smoke (16,17). Hence, stimulationof the chemical irritant receptors leads toneurogenic inflammation. The relation-ship among chemical irritants, sensorynerves, substance P, and NEP is summa-rized in Figure 2.
Regulation of NeurogenicInflammationNeutral endopeptidase degrades substanceP (13). NEP is located on the surfaces ofcells with substance P receptors, i.e., thetarget cells of substance P. Substances thatdecrease neutral endopeptidase levelsincrease neurogenic inflammation, whilesubstances that increase neutral endopepti-dase suppress neurogenic inflammation.Human recombinant NEP suppresses neu-
rogenic inflammation (18-20). Exogenoussubstances that inhibit NEP include ciga-rette smoke (21), respiratory viruses(22-25), and the volatile organic chemicaltoluene diisocyanate (26).
Possible Roles ofNeurogenicInflammationNeurogenic inflammation may play a rolein a variety of disorders, from asthma andrhinitis to migraine headache, rheumatoidarthritis, and fibromyalgia. Such a role is
Table 1. Immunogenic versus neurogenic asthma
Immunogenic NeurogenicTriggered by Protein aeroallergens Volatile organic chemicalsInteracting with IgE antibody Chemical irritant receptorsLocated on Mast cells Sensory nerve C-fibersReleasing Histamine, leukotrienes, Neuropeptides: substance P,
prostoglandins, chemotactic neurokinen A, calcitoninfactors gene-related peptide
Stimulating Sensory nerve C-fibers Mast cell degranulationProducing Bronchial inflammation Bronchial inflammationManifesting as Asthma Asthma
supported by a combination of animalstudies, pharmacological responses of thesedisorders, and circumstantial evidence. Atthe current time these associations aresomewhat speculative, but there is suffi-cient evidence to justify investigations.
It is now known that the neuropeptidesof neurogenic inflammation reproduce thepathology of asthma (27), and the role ofneurogenic inflammation has been docu-mented in animal models of asthma (28).Barnes (29) has recently reviewed the cur-rent evidence for the role of neurogenicinflammation in asthma and has suggestedstrategies for reducing neurogenic inflam-mation in this disease. It is increasinglyrecognized that respiratory irritants such asVOCs and environmental tobacco smokecan exacerbate asthma and rhinitis (30-32).A number of studies have documented anincrease in the incidence of asthma inindustrialized countries, over both the longterm and during the 1980s (33). In addi-tion, studies during the 1980s establishedthat the American population is exposed toVOCs in the indoor air (34).
The role of neurogenic inflammationand chemical irritants in these respiratorydisorders and the upregulation of neuro-genic inflammation by inhalant irritantsdiscussed above indicate that there may bea relationship between indoor air pollutionwith VOCs and the worsening asthma epi-demic. Pursuit of this relationship shouldbe a research priority. In the past asthmawas divided into extrinsic asthma, triggeredby protein aeroallergens, and intrinsic asth-ma of unknown cause. This distinctionwas made before the role of neurogenicinflammation in asthma was appreciated.It may be that asthma would be better clas-sified as immunogenic or neurogenic(Table 1). The distinction between neuro-genic and immunologic asthma is limitedto the catalysts because the two types crossover after the release of mediators, in thatthe mediators of neurogenic inflammationtrigger mast cell degranulation, and mastcell mediators stimulate peripheral nerves.This "bidirectional regulatory circuit" hasrecently been reviewed (35).
This crossover phenomenon does notmean that neurogenic inflammation andimmunologic inflammation are clinicallyidentical in all cases. In the upper airwaysand skin, the initial complaint associatedwith exposure to chemical irritants is burn-ing or pain, whereas itching is the initialcomplaint associated with immune-medi-ated exposures. It may be that there isindividual variability in the degree towhich crossover is clinically manifested.The two mechanisms might be differenti-ated by testing patients with challengingdoses of antigens and nonallergenic chemi-cal irritants while monitoring clinical
Volume 101, Number3, August 1993 235

--i S MI I I lI I
symptoms and measuring mediators. Thisresearch would best be carried out bystudying upper airway responses, as nasalwashings can be easily obtained for quanti-fying mediators.
Another disorder that increased signifi-cantly during the 1980s is migraine head-aches (36). Headache is an early and con-sistent consequence of exposure to VOCs.On the basis of pharmaceutical responsesof migraine and animal experiments,Nicolodi and Sicuteri proposed that neuro-genic inflammation plays a role in thepathophysiology of migraine headaches(37). Silberstein argued that both tensionheadaches and migraine may be generatedby neurogenic inflammation (38). Buzziand Moskowitz demonstrated that stimula-tion of trigeminal sensory fibers leads tochanges consistent with those of migrainein a rat model, and these changes can beblocked by the antimigraine drugs suma-triptan and dihydroergotamine (39).Hardebo has pointed out that the postulatethat neurogenic inflammation mediatesmigraine provides a rational explanationfor why serotonin antagonists are effectivein treating migraine (40). Challenge stud-ies with VOCs on migraine patients, withand without specific pharmacologicalblockage of relevant receptors, is needed toelucidate the role of neurogenic inflamma-tion and chemical irritants in migraine.
A comparison of neuropeptide stainingin the synovium of patients with rheuma-toid arthritis, osteoarthritis, and controlsfound weaker staining in the nerve fila-ments of the rheumatoid arthritis group(41). The authors suggest that this weakerstaining is evidence of release from nerve
fibers in rheumatoid arthritis, and neuro-genic inflammation may play a role i9 thisdisorder. Zimmerman has suggested thatneurogenic inflammation may play a rolein fibromyalgia (44.Role ofNeurogenic Inflammation inChemical Sensitivity Syndromes"Sick building syndrome" (SBS) is a termused to designate an outbreak of illnessassociated with indoor air contaminants innew and tightly sealed buildings. Symp-toms include irritation of the eyes, nose,and throat, skin irritation, and neurotoxicsymptoms including mental fatigue anddifficulty concentrating (43). The syn-drome is an acquired disorder with onsetrelated to moving into a new or renovatedbuilding, and there is wide individual vari-ability in onset and symptoms after expo-sure.
Multiple chemical sensitivity syn-drome (MCS) is a related syndrome withonset related to an environmental expo-sure, most commonly a solvent or pesti-cide. After the initial exposure, individu-als become sensitive to low-level chemicalexposures with symptoms involving morethan one organ system. Though this syn-drome was de-scribed four decades ago(44.45), it re-mains highly controversial.
Reactive airways dysfunction syn-drome (RADS) is an asthmalike illnessthat develops within minutes to hoursafter an acute exposure to dust, smoke, orsolvent. There is persistent bronchialhyperreactivity with positive methacholinechallenge. The asthma becomes chronicafter the initial exposure and can be diffi-cult to treat (46).
Figure 3. Chemical sensitivity syndromes. The multiple chemical sensitivity syndrome (MCS), sick build-ing syndrome (SOS), reactive airways dysfunction syndrome (RADS), the reactive upper airways dysfunc-tion syndrome. (RUDS) have many features in common. These syndromes may all be disorders of the reg-ulation of neurogenic inflammation.
Reactive upper-airways dysfunctionsyndrome (RUDS) also follows a chemicalexposure, and there is persistent chronicrhinitis. The chief complaint of patientswith RUDS is chemical sensitivity (47).Unlike patients with RADS, medical atten-tion is not sought on the day of exposure,which probably reflects the fact thatbreathing is compromised in RADS butnot in RUDS. Preliminary study of thenasal mucosa found lymphocytic infil-trates, and electron microscopy has shownthickening of the basement membrane anddesquamation of the respiratory epithelium(48).
There are many similarities betweenSBS, MCS, RADS, and RUDS (Fig. 3). Ineach snydrome, a high-dose exposureinduces the syndrome, and subsequentexacerbations are associated with low-levelexposures. SBS and MCS include symp-toms involving more than one organ sys-tem, with the respiratory mucosal and cen-tral nervous system being prominentlyinvolved. The major difference betweenSBS and MCS is that SBS refers to a clusterof cases associated with a building, whileMCS patients have more generalized com-plaints. RADS and RUDS have prominentairway involvement, with the differencebetween the two being that RADS involvesthe lower airway (asthma), and RUDSinvolves the upper airway (rhinitis). In onesmall series, 100% of patients with RUDShad extra-airway manifestations and metthe Cullen case definition (49) for MCS.
These syndromes may be related at adeeper level. All of these illnesses may bedisorders of the regulation of neurogenicinflammation. The inducing exposure mayalter the respiratory mucosa in one or moreways. The regulation of neurogenic inflam-mation may be disturbed by the depletionof NEP or other enzymes, which wouldresult in a heightened response to subse-quent exposures. The desquamation of therespiratory epithelium seen in RUDS mayremove a barrier to chemical irritants, sothat chemical irritants may reach and trig-ger the irritant receptors at lower concen-trations.
Patients with these illnesses complain ofsymptoms in organ systems in addition tothe airways, and some patients have no air-ways symptoms at all. Mechanisms toexplain how airway irritants can trigger sys-temic symptoms must be considered. First,it is common for inflammatory illnesses pri-marily arising in one organ or tissue to pro-duce systemic manifestations (e.g., theextra-articular manifestations of rheuma-toid arthritis and the systemic manifesta-tions of Crohn's disease). Viral infectionsof the upper airway produce systemicsymptoms, including myalgias, fever,fatigue, and malaise.
Environmental Health Perspectives236

-. A I - I e
*....~~~~~~~~~~~~~~~~~~~~~~W ll '' O d_vie hsis an....p.o. Wlli~O fte'is andfe:. l. .a 1 S *x. U.n.|V~~~~~~~~~~~~~~~~~~~~~~~~~~~4X:d..ce en Misan
~~~~~~~~~~~~~~~~~~~~~..... ...r;._. ................~ ~~...... ............
.......~~~~~~~~~~~~~~~~~~~~~~~~: ... _. ......P Z.n::.: duc1 t.th. r'* ~~~~~~~~~~~~~~~~~~~~.i ;f6-s ot a''- Be{¢loly r gSs* ..~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .1::.: re: ... .....$c.e.n.ces,iicha-ored*.e.bo....a.k...::M.#fVm.~~~~~~~~~~~~~~~~~~~~~~~~............................. ..
Both the mediators and regulators ofinflammation may be released from the siteof inflammation and affect distant sites.Two important regulators of inflamma-tion, interleukin 1 and interleukin 2, sup-press central nervous system activity(50,51). Another possibility is that someform of neural switching may take place.That is, triggering of chemical irritantreceptors in one organ could lead to anefferent signal traveling to another sitethrough an aberrant or conditioned cross-ing of the pathways. A combination ofthese two mechanisms may be operative.
The hypothesis that neurogenic inflam-mation is the mechanism of chemical sen-sitivity syndromes is amenable to scientificstudy. Biopsies of the airways of chemical-ly sensitive individuals should be abnor-mal, with signs of inflammation. Im-munofluorescent monoclonal antibodiescould be used to detect NEP, whichshould be decreased, and substance P,which should be elevated relative to con-trols. Nasal washings should containincreased levels of the mediators of neuro-genic inflammation relative to controls,and the levels should increase after chemi-cal challenge in patients but not controls.Heightened neuronal firing of sensoryfibers should occur after chemical chal-lenges.
DiscussionNeurogenic inflammation leads to inflam-mation independent of the immune sys-tem. Polypeptide mediators are stored innerve endings and released when irritantreceptors on nerves are stimulated bychemicals. The role of neurogenic inflam-mation in a number of inflammatory con-ditions is currently under investigation.There is strong evidence that neurogenicinflammation is operative in asthma andrhinitis..There is circumstantial evidencethat neurogenic inflammation may play arole in migraine headache. Evidence for arole in rheumatoid arthritis and fibromyal-gia is not as compelling at this time. Thesignificance of these associations for envi-ronmental health is that neurogenic in-flammation can be triggered in the airways
by environmental chemicals such as ciga-rette smoke and solvents. Hence, any dis-order mediated by neurogenic inflamma-tion can potentially be exacerbated byenvironmental chemicals. Study of thehypothesis that chemical sensitivity syn-dromes such as SBS and MCS may resultfrom neurogenic inflammation arisingfrom stimulation of irritant receptors byenvironmental chemicals may lead to anunderstanding of these disorders. It is ofinterest that the symptoms of headache,myalgia, arthralgias and arthritis, and air-way symptoms reported by MCS patientsoverlap with those disorders for which arole for neurogenic inflammation has beenreported.
The hypothesis that neurogenic inflam-mation triggered by environmental chemi-cals plays a role in human health is amen-able to scientific study. Research shouldfocus on noninvasive methods for detect-ing biomarkers of neurogenic inflamma-tion. Are there degradation products ofsubstance P or other mediators of neuro-genic inflammation that are elevated in theurine or serum of patients with activationof this system? Are there evoked potentialsor nerve conduction parameters that canbe used to detect activation of neurogenicinflammation? Two groups of patientsshould be studied with challenge tests:patients with disorders in which neuro-genic inflammation is suspected to play arole (i.e., asthma, rhinitis, migraine,rheumatoid arthritis, fibromyalgia) andpatients with chemical sensitivity syn-dromes. These patients should be isolatedfrom VOCs in a specially constructed din-ical research unit and monitored for reso-lution of their symptoms. Chemical chal-lenges should be conducted while patientsare monitored for provoked symptoms.Biomarkers of neurogenic inflammationshould be measured throughout the courseof these challenges.
REFERENCES
1. Bruce AN. Uber die Beziehung der SensiblenNervenendigungen zum Enzundungsvorgang.Arch Exp Pathol Pharmakol 63:424(1910).
2. Bruce AN. Vaso-dilatory axon reflexes. Q J
Exp Physiol 6:339-354(1913).3. Tanaka DT, Grunstein MM. Vasoactive
effects of substance P on isolated rabbit pul-monary artery. J Appi Physiol 58:1291(1985).
4. Foreman JC. Peptides and neurogenic inflam-mation. Br Med Bull 43:386(1987).
5. Lundberg JM, Lundblad L, Martling CR, SariaA, Stjarne P, Anggard A. Coexistence of multi-ple peptides and classic transmitters in airwayneurons. Am Rev Respir Dis 136:16(1987).
6. Uddman R, Grunditz T, Larsson A, Sundler F.Sensory innervation of the ear drum and mid-dle ear mucosa. Cell Tissue Res 252:141(1988).
7. Hinsey JC and Gasser HS. The component ofthe dorsal root mediating vasodilatation andthe Sherrington contracture. Am J Physiol92:679(1930).
8. Jancso-Gabor, A., Szolcsany J. Action of rareearth metal complexes on neurogenic as well ason bradykinin induced inflammation. J PharmPharmacol 22:366:135(1970).
9. Gasparovic I, Hadzovic S, Hukovic S, Stern P.Contribution to the theory that substance Phas a transmitter role in sensitive pathways.Med Exp 10:155-159(1964).
10. Gazelius B, Brodin E, Olgart L, Panopoulos P.Evidence that substance P is a mediator ofantidromic vasodilatation using somatostatin asa release inhibitor. Acta Physiol Scand 113:155-159(1981).
11. Chahl LA. Antidromic vasocilatation and neu-rogenic inflammation. Pharmacol Ther 37:275-300(1988).
12. Ehrlanger J, Glasser HJ. The action potentialin fibers of slow conduction in spinal roots andsomatic nerves. Am J Physiol 90:338-339(1929).
13. Nadel JA. Neutral endopeptidase modulatesneurogenic inflammation. Eur Respir J 4:745-754(1991).
14. Nielsen GD. Mechanisms of activation of thesensory irritant receptor by airborne chemicals.Crit Rev Toxicol 21:183-208(1991).
15. Cometto-Muniz JE, Cain WS. Thresholds forodor and nasal pungency. Physiol Behav48:719-725(990).
16. Lundblad L. Protective reflexes and vasculareffects in the nasal mucosa elicited by activa-tion of capsaicin-sensitive substance P im-munoreactive trigeminal neurons. Acta PhysiolScand 529(suppl) (1984).
17. Lundberg JM, Lundbblad L, Saria A, AngaardA. Inhibition of cigarette smoke-induced oede-ma in the nasal mucosa by capsaicin pretreat-ment and a substance P antagonist. Naunyn-Schmiedebergs Arch Pharmakol 326: 181(1984).
18. Kohrogi H, Nadel JA, Malfroy B, Gorman C,Bridenbaugh R, Patton JS, Borson DB.Recombinant human enkephalinase (neutralendopeptidase) prevents cough induced bytachykinins in awake guinea pigs. J Clin Invest84:781-786(1989).
19. Iwamoto I, Ueki IF, Borson DB, Nadel JA.Neutral endopeptidase modulates tachykinin-induced increase in vascular permeability inguinea pig skin. Int Arch Allergy Appl Im-munol 88:288-293(1989).
20. Rubenstein I, Iwamoto I, Ucki IF, Borson DB,Nadel JA. Recombinant neutral endopeptidaseattenuates substance P induced plasma extrava-sation in the guinea pig skin. Int Arch AllergyAppl Immunol 91:232-238(1990).
21. Dusse DJ, Djokic TD, Borson DB, Nadel JA.Cigarette smoke induces bronchoconstrictorhyperresponsiveness in substance P and inacti-
Volume 101, Number 3, August 1993 237

1- -. 4j -
vates airway neutral endopeptidases in theguinea pig. Possible role of free radicals. JClin Invest 84:900-906(1989).
22. Jacobi DB, Tamaoki J, Borso DB, and NadelJA. Influenza infection causes airway hyperre-sponsiveness by decrcasing enkephalinase. JAppl Physiol 64:2653-2658(1988).
23. Dusser DJ, Jacoby DB, Djokic TD,Rubenstein I, Borson DB, and Nadel JA.Virus induces airway hyperresponsivenss totachykinins: role of neutral endopeptidase. JAppl Physiol 67:1504-1511(1989).
24. Borson DB, Brokaw JJ, Sekizawa K,McDonald DM, and Nadel JA. Neutralendopeptidase and neurogenic inflammation inrats with respiratory infections. J Appl Physiol66:2653-2658(1989).
25. Piedimonte G, Nadel JA, Umeno E,McDonald DM. Sendai virus infection poten-tiates neurogenic inflammation in the rat tra-chea. J Appl Physiol 68:754-760(1990).
26. Sheppard D, Thompson JE, Scypinski L,Dusser D, Nadel JA, Borson DB. Toluenediisocyanate increases airway responsiveness tosubstance P and decreases airway enkephali-nase. J Clin Invest 81:1111-1115(1988).
27. Barnes PJ. Neurogenic inflammation in air-ways. Int Arch Allergy Appl Immunol 94:303-309(1991).
28. Lundberg JM, Saria A, Lundberg L, AnggardA, Martling C-R, Thesodorsson-Norheim E,Stjarne P, Hokfelt TG. Bioactive peptides incapsaicin-sensitive C-fiber afferents of the air-ways: functional and pathophysiological impli-cations. In: The airways neural control inhealth and disease (Kaliner MA, Barnes RJ,eds). New York:Marcel Dekker, 1987;417-445.
29. Barnes PJ. Neurogenic inflammation and asth-ma. J Asthma 29:165-180 (1992).
30. Shim C, Williams MH, Jr. Effect of odors inasthma. Am J Med 80:18-22(1986).
31. Stankus RP, Menon PK, and Rando RJ,Glindmeyer H, Salvaggio JE, and Lehrer SB.Cigarette smoke sensitive asthma: chaliengestudies. J Allergy Clin Immunol 82:331-338(1988).
32. Meggs WJ. Health effects of indoor air pollu-tion. NC Med J 53:354-358(1992).
33. Weiss KD, Wagener DK Asthma surveillancein the United States: a review of current trendsand knowledge gaps. Chest 98(suppl 5):1795-1845(1990).
34. Wallace LA. Recent field studies of personaland indoor exposures to environmental pollu-tants. Ann NYAcad Sci 641:7-16(1992).
35. Lewis RM. Bidirectional regulatory circuitbetween the immune and neuroendocrine sys-tems. Year Immunol 4:241-252(1989).
36. Anonymous. Prevalence of chronic migraineheadaches-United States, 1980-1989.MMWR 40:337-338(1991).
37. Nicolodi M, Sicuteri F. Links between head-ache mechanisms and new medications. Clin JPain 7(suppl):S64-71(1991).
38. Silberstein SD. Advances in understanding thepathophysiology of headache. Neurology 42(suppl 2):6-10(1992).
39. Buzzi MG, Moskowitz MA. The trigemino-vascular system and migraine. Pathol Biol40:313-317(1992).
40. Harbedo, J. A cortical excitatory wave maycause both the aura and the headache ofmigraine. Cephalalgia 12:75-80(1992).
41. Gronblad M, Konttinen YT, Korkala 0, LiesiP, Hukkanen M, Polak JM. Neuropeptides insynovium of patients with rheumatoid arthritisand osteoarthritis. J Rheum 15:1807-1810(1988).
42. Zimmerman M. Pathophysiologic mecha-nisms of fibromyalgia. Clin J Pain 7 (suppl1):S8-15, 1991
43. Molhave L. The sick buildings-a subpopula-tion among the problem buildings. In: Indoor
Air '87: Proceedings of the IV internationalconference on indoor air quality and climate,vol 2 (Sefert B, Esdorn H, Fischer M, eds),Berlin:Institute for Water, Soil, and AirHygiene, 1987;469-473.
44. Randolph TG. Human ecology and suscepti-bility to the chemical environment. Spring-field, Illinois: C. C. Thomas, 1962.
45. Tabershaw IR, Cooper WC. Sequelae of acuteorganic phosphate poisoning. J Occup Med8:5-19(1966).
46. Brooks SM, Weiss MA, and Bernstein IL.Reactive airways dysfunction syndrome(RADS): persistent asthma syndrome after highlevel irritant exposurc. Chest 88:376-384(1985).
47. Meggs WJ, Cleveland CH. Rhinolaryngo-scopic findings in the multiple chemical sensi-tivity syndrome. Arch Environ Health 48:14-18(1993).
48. Meggs WJ, Cleveland CH, Metzger WJ,Larkin E, Albernaz M. Reactive upper-airwaysdysfunction syndrome (RUDS): a form ofchemical irritant rhinitis following an acuteexposure. J Allergy Clin Immunol 89:145(1992).
49. Cullen MR The worker with chemical sensi-tivities: an overview. State Art Rev OccupMed 2:655-661(1987).
50. Obal F Jr, Opp M, Cady AB, Johannsen L,Postlethwaite AE, Poppleton H, Seyer JE, andKrueger JM. Interleukin 1 alpha and intcr-leukin 1 beta fragments are somnogenic. Am JPhysiol 259:R439-446(1990).
51. De Sarro GB, Masuda Y, Ascioti C, AndinoMG, and Nistico G. Behavioral and ECGspectrum changes induced by intracerebralinfusion of interferons and interleukin 2 in ratsare antagonized by naloxone. Neuropharma-cology 29:167-179(1990).
A LONG-STANDING TRADMON CON71NUES. h
Environmental Health
SupplementsIN CELEBRATION OF20 YEARS OF ENVIRONMENTAL HEALTH PERSPECTIVESwe are pleased to announce publication of Environmental HealthPerspectives Supplements, Volume 1 00, an issue dedicated toDr. David P. Rall, founder of the journal and former director of theNational Institute of Environmental Health Sciences. This issue,"Twenty Years of Environmental Health Research," is a series ofperspectives on various topics that have been key issues in the fieldof environmental health in the last two decades.
To order your copy, contact:GOVERNMENT PRINTING OFFICE, WASHINGTON, DC 20402or call 202-512-2406.
238 Environmental Health Perspectives