english skills needed by health service professionals of
TRANSCRIPT

ENGLISH SKILLS NEEDED BY HEALTH SERVICE
PROFESSIONALS OF THE ASEAN ECONOMIC
COMMUNITY: A STUDY IN PRACHUABKIRIKHAN
BY
SUPAKARN SOOKHOM
A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE
REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS IN
TEACHING ENGLISH AS A FOREIGN LANGUAGE
LANGUAGE INSTITUTE
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2018
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25615721042223AND

ENGLISH SKILLS NEEDED BY HEALTH SERVICE
PROFESSIONALS OF THE ASEAN ECONOMIC
COMMUNITY: A STUDY IN PRACHUABKIRIKHAN
BY
SUPAKARN SOOKHOM
A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE
REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS IN
TEACHING ENGLISH AS A FOREIGN LANGUAGE
LANGUAGE INSTITUTE
THAMMASAT UNIVERSITY
ACADEMIC YEAR 2018
COPYRIGHT OF THAMMASAT UNIVERSITY
Ref. code: 25615721042223AND

(2)
Thesis Title ENGLISH SKILLS NEEDED BY HEALTH
SERVICE PROFESSIONALS OF THE ASEAN
ECONOMIC COMMUNITY: A STUDY IN
PRACHUABKIRIKHAN
Author Miss Supakarn Sookhom
Degree Master of Arts
Major Field/Faculty/University Teaching English as a Foreign Language
Language Institute
Thammasat University
Thesis Advisor
Academic Year
Associate Professor Sripathum Noom-ura
2018
Ref. code: 25615721042223AND

(3)
ABSTRACT
The study focuses on English language functional skills needed for health
service professionals involved in three ASEAN occupations that are associated with
mobility in the labor market: medical, dental, and nursing services. The participants,
selected by stratified random sampling, comprised 30 doctors, 11 dentists, and 210
nurses (251 health services professionals in total) from eight governmental hospitals
in Prachuabkirikhan, Thailand: Hua Hin Hospital, Pranburi Hospital, Samroiyod
Hospital, Kuiburi Hospital, Prachuabkirikhan Hospital, Thapsakae Hospital,
Bangsaphan Hospital, and Bangsaphan Noi Hospital. The instrument used in this
study was a self-administered questionnaire which included authentic tasks from
medical setting. The participants were required to rate their current proficiency and
needs of four English skills in performing each medical task. The finding revealed
that the language proficiency of the doctors and dentists ranged from moderate to high
and nurses rated their ability as low and moderate. The majority had highest ability in
reading and writing; nevertheless, four English skills were highly demanded in every
medical task. For doctors, reading skill was ranked the highest; for dentists, the four
English skills were equally rated as high and for nurses, listening, speaking, and
reading skills were rated the highest. Recommendations given to researchers and
curriculum developers were to further the study with health services professionals in
various health facilities in different areas to enrich the current literature, design ESP
courses regarding particular needs and interests of learners, and promote professional
communication among Thai health services workers as a preparation for the
integration of the ASEAN Economic Community.
Keywords: English for Specific Purposes (ESP), Needs Analysis (NA), English for
Occupational Purposes (EOP)
Ref. code: 25615721042223AND

(4)
ACKNOWLEDGEMENTS
I would like to express my greatest appreciation and sincere gratitude to
those who have contributed to the completion of my master’s thesis. First and
foremost, I would like to thank my advisor, Associate Professor Sripathum Noom-ura,
for her devotion, attention, constant encouragement, kindness, expert guidance, and
invaluable advice throughout this study. Without her, this study would never have
been completed.
I am particularly grateful to Alisa Ratanapruks, Ph.D., the chairman of the
committee, for her valuable time, advice, and dedication; moreover, I would like to
extend my thankfulness to my thesis committee, Ratikorn Sirisatit, Ph.D., for her
useful and constructive recommendations on my study. Without their support, the
completion of my thesis would not have been possible.
My special thanks go to hospital directors, doctors, dentists, and nurses of
eight governmental hospitals in Prachuabkirikhan who contributed their time and
assistance to the collection of my data.
Next, I would like to offer my appreciation to all the instructors and
academic staff of the Language Institute, Thammasat University who devoted time,
knowledge, and assistance for all M.A. students.
Finally, I would like to extend my deepest thanks to my family for their
tremendous support and encouragement throughout my study.
Supakarn Sookhom
Ref. code: 25615721042223AND

(5)
TABLE OF CONTENTS
Page
ABSTRACT (2)
ACKNOWLEDGEMENTS (3)
LIST OF TABLES (8)
LIST OF FIGURES (10)
CHAPTER 1 INTRODUCTION 1
1.1 Background 1
1.2 Objective of the study 6
1.3 Research questions 6
1.4 Scope of the study 7
1.5 Definition of terms 7
1.6 Significance of the study 8
1.7 Organization of the study 8
CHAPTER 2 REVIEW OF LITERATURE 9
2.1 English for Specific Purposes (ESP) 9
2.1.1 Definitions of English for Specific Purposes 9
2.1.2 Characteristics of English for Specific Purposes 12
2.1.3 Objectives of ESP teaching 14
2.2 Needs Analysis (NA) 16
2.2.1 Definitions of Needs Analysis 16
2.2.2 Types of Needs and Needs Analysis 17
2.2.3 Data gathering options for Needs Analysis 18
2.2.3.1 Munby’s Communicative Need Processor 18
Ref. code: 25615721042223AND

(6)
2.2.3.2 Hutchinson and Waters’ Checklists 19
2.2.3.3 Robinson’s seven techniques 20
2.2.4 Steps in Needs Analysis 21
2.3 English for Occupational Purposes (EOP) 23
2.3.1 Definitions and classification of EOP 23
2.3.2 English for Medical Purposes (EMP) 27
2.4 Previous related studies 28
CHAPTER 3 RESEARCH METHODOLOGY 36
3.1 Participants 36
3.1.1 Population 36
3.1.2 Sample size 36
3.1.3 Sampling Procedure 36
3.2 Materials 41
3.3 Procedures 41
3.3.1 Research design 41
3.3.2 Data collection 42
3.4 Data analysis 42
CHAPTER 4 RESULTS 44
4.1 General background information of the participants 44
4.2 Linguistic profile of the participants 46
4.3 English ability of the participants 48
4.3.1 Listening ability of the participants 48
4.3.1.1 Listening ability of the participants in each medical task 49
4.3.2 Speaking ability of the participants 51
4.3.2.1 Speaking ability of the participants in each medical task 51
4.3.3 Reading ability of the participants 55
4.3.3.1 Reading ability of the participants in each medical task 55
4.3.4 Writing ability of the participants 58
Ref. code: 25615721042223AND

(7)
4.3.4.1 Writing ability of the participants in each medical task 59
4.4 English needs of the participants 63
4.4.1 Needs in listening skill of the participants 63
4.4.1.1 Needs in listening skill of the participants in each
medical task 64
4.4.2 Needs in speaking skill of the participants 65
4.4.2.1 Needs in speaking skill of the participants in each
medical task 66
4.4.3 Needs in reading skill of the participants 69
4.4.3.1 Needs in reading skill of the participants in each
medical task 70
4.4.4 Needs in writing skill of the participants 72
4.4.4.1 Needs in writing skill of the participants in each
medical task 73
4.5 Correlation between background and English proficiency
of the participants 79
CHAPTER 5 CONCLUSION AND RECOMMENDATIONS 85
5.1 Summary of the study 85
5.1.1 Objective of the study 85
5.1.2 Research questions 86
5.1.3 Participants 86
5.1.4 Research instrument 86
5.1.5 Data analysis 87
5.2 Summary of the findings 87
5.2.1 General background information of the participants 87
5.2.2 Linguistic profile of the participants 87
5.2.3 English abilities of the participants 87
5.2.4 English needs of the participants 88
5.2.5 Correlation between background and English proficiency
of the participants 88
Ref. code: 25615721042223AND

(8)
5.3 Discussion of the findings 89
5.4 Conclusions 93
5.5 Recommendations for further research 93
REFERENCES 95
APPENDICES 100
APPENDIX A Questionnaire 101
APPENDIX B Letter of Consent 114
BIOGRAPHY 115
Ref. code: 25615721042223AND

(9)
LIST OF TABLES
Table Page
1.1 Mutual Recognition Arrangements in services 3
2.1 Steps in Needs Analysis 22
2.2 Classification of EOP courses 24
3.1 Proportions of healthcare professionals of each hospital 37
3.2 Number of samples from each hospital 38
3.3 Number of samples of each profession from each hospital 38
4.1 General background information of the participants 45
4.2 Linguistic profile of the participants 47
4.3 Listening ability of all participants 48
4.4 Listening ability of each profession 49
4.5 Listening ability of the participants in each medical task 50
4.6 Speaking ability of all participants 51
4.7 Speaking ability of each profession 51
4.8 Speaking ability of the participants in each medical task 53
4.9 Reading ability of all participants 55
4.10 Reading ability of each profession 55
4.11 Reading ability of the participants in each medical task 57
4.12 Writing ability of all participants 59
4.13 Writing ability of each profession 59
4.14 Writing ability of the participants in each medical task 60
4.15 Needs in listening skill of all participants 63
4.16 Needs in listening skill of each profession 64
4.17 Needs in listening skill of the participants in each medical task 65
4.18 Needs in speaking skill of all participants 66
4.19 Needs in speaking skill of each profession 66
4.20 Needs in speaking skill of the participants in each medical task 67
4.21 Needs in reading skill of all participants 69
4.22 Needs in reading skill of each profession 70
4.23 Needs in reading skill of the participants in each medical task 71
Ref. code: 25615721042223AND

(10)
4.24 Needs in writing skill of all participants 73
4.25 Needs in writing skill of each profession 73
4.26 Needs in writing skill of the participants in each medical task 74
4.27 Correlation between background and English proficiency
of the participants 80
Ref. code: 25615721042223AND

(11)
LIST OF FIGURES
Figure Page
2.1 Classification of EOP courses 24
2.2 The tree of ELT 25
2.3 ESP classification by professional area 27
4.1 Listening ability of each profession 62
4.2 Speaking ability of each profession 62
4.3 Reading ability of each profession 62
4.4 Writing ability of each profession 62
4.5 Needs in listening skill of each profession 76
4.6 Needs in speaking skill of each profession 76
4.7 Needs in reading skill of each profession 76
4.8 Needs in writing skill of each profession 76
Ref. code: 25615721042223AND

1
CHAPTER 1
INTRODUCTION
1.1 BACKGROUND
The Association of South East Asian Nations (ASEAN) was officially
initiated in August 8, 1967 by five member states: Indonesia, Malaysia, Philippines,
Singapore, and Thailand and was enlarged when Brunei Darussalam joined the
membership in 1984, Viet Nam in 1995, Lao PDR in 1997, and Cambodia in 1999,
making up today ten member states for the ASEAN. The community was established
upon three main pillars: the ASEAN Political-Security Community (APSC), ASEAN
Economic Community (AEC), and ASEAN Socio-Cultural Community (ASCC) (Das
et al., 2013).
The economic cooperation projects were in the best interest of ASEAN
during the second decade of ASEAN and continued to prosper after the agreement to
establish the ASEAN Free Trade Area (AFTA) was signed in 1992 (Chia & Pacini,
1997). After the ASEAN Economic Community Blueprint was adopted in 2007, the
overall structure of ASEAN economies changed significantly. To accelerate the
national and economic development of ASEAN member states, the AEC was
established upon four pillars: the Single Market and Production Base; the Competitive
Economic Region; Equitable Economic Development; and ASEAN’s Integration into
the Global Economy (Chia, 2013).
The formation of ASEAN’s single market was based on five major
elements: free flow of goods, free flow of services, free flow of investment, freer flow
of capital, and free flow of skilled labor. According to the ASEAN Economic
Community Blueprint (2008), the free flow of goods would grant the elimination of
tariffs and the removal of non-tariff barriers. With the free flow of trade in services,
ASEAN services suppliers would be able to provide services and establish companies
across national borders within the region. All restrictions on the services sectors,
namely, air transport, healthcare, tourism, logistic services, and other services sectors,
would be removed by 2015. The free flow of investment would enhance member
countries’ competitiveness in attracting foreign and intra-ASEAN investments and
Ref. code: 25615721042223AND
2
develop the overall ASEAN economies. Likewise, the freer flow of capital would
promote ASEAN capital market integration, agreement on the recognition of
qualification, education, and experience of professionals, including greater mobility of
capital and labor.
The movement of labor and challenges resulting from labor market
integration were unavoidable.Thus, the free flow of skilled labor was determined to
manage mobility for students, staff, professionals, and skilled labor within the region
through enhancing cooperation among universities, promoting job opportunities,
qualifications and occupational skills required in each service sector, as well as
facilitating entry and employment pass for those who were engaged in trades and
investments within ASEAN.
To accelerate the establishment of an integrated market and increase the
economic competitiveness of ASEAN, at the 9th
ASEAN Summit, a meeting in
October 2003 in Bali, Indonesia, the leaders of the member states affirmed an
agreement on facilitating mobility for skilled labor engaged in eight service sectors:
(1) engineering services
(2) nursing services
(3) architectural services
(4) surveying qualification
(5) accountancy services
(6) dental services
(7) medical services
(8) hotel services and tourism
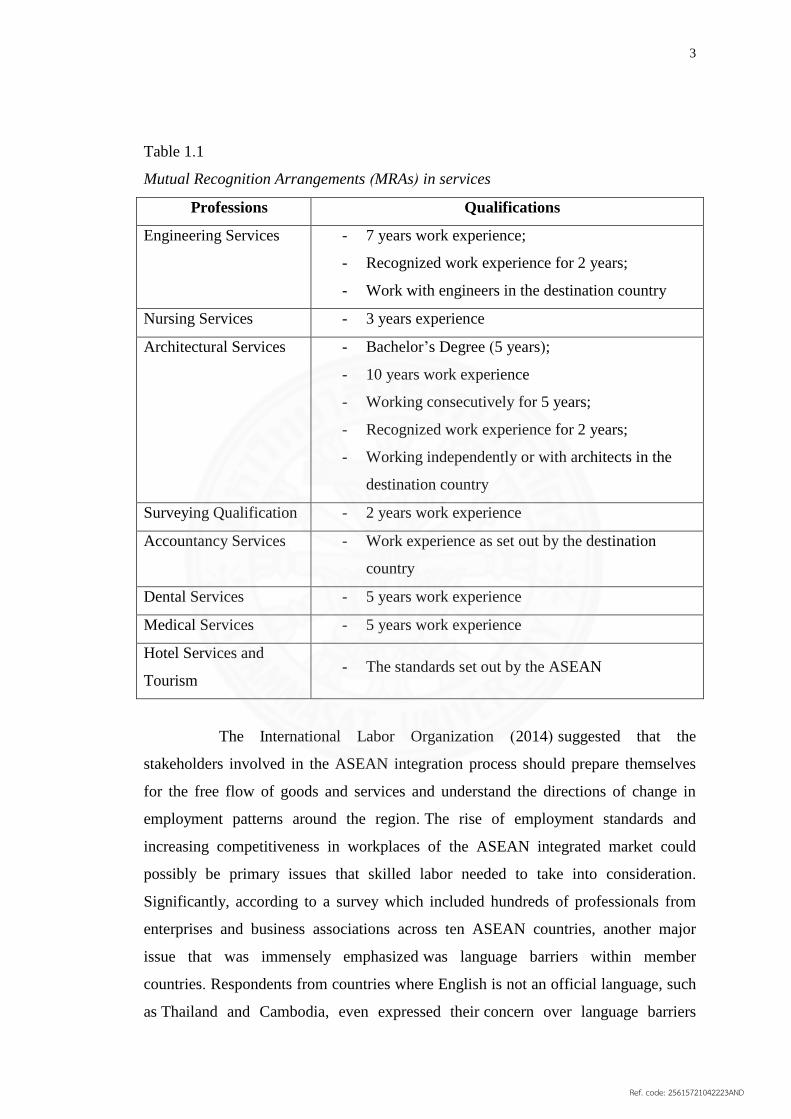
According to Thailand’s Ministry of Labor (2012), skilled labor in the
eight ASEAN occupations must possess qualifications stated in Mutual Recognition
Arrangements (MRAs) in order to be accepted into an ASEAN integrated market.
Ref. code: 25615721042223AND
3
Table 1.1
Mutual Recognition Arrangements (MRAs) in services
Professions Qualifications
Engineering Services - 7 years work experience;
- Recognized work experience for 2 years;
- Work with engineers in the destination country
Nursing Services - 3 years experience
Architectural Services - Bachelor’s Degree (5 years);
- 10 years work experience
- Working consecutively for 5 years;
- Recognized work experience for 2 years;
- Working independently or with architects in the
destination country
Surveying Qualification - 2 years work experience
Accountancy Services - Work experience as set out by the destination
country
Dental Services - 5 years work experience
Medical Services - 5 years work experience
Hotel Services and
Tourism - The standards set out by the ASEAN
The International Labor Organization (2014) suggested that the
stakeholders involved in the ASEAN integration process should prepare themselves
for the free flow of goods and services and understand the directions of change in
employment patterns around the region. The rise of employment standards and
increasing competitiveness in workplaces of the ASEAN integrated market could
possibly be primary issues that skilled labor needed to take into consideration.
Significantly, according to a survey which included hundreds of professionals from
enterprises and business associations across ten ASEAN countries, another major
issue that was immensely emphasized was language barriers within member
countries. Respondents from countries where English is not an official language, such
as Thailand and Cambodia, even expressed their concern over language barriers
Ref. code: 25615721042223AND

4
before mentioning about cross-cultural working skills or management skills. The
researchers from the Regional Office for Asia and the Pacific and Bureau for
Employers’ Activities (2014) reported that language barrier within the ASEAN region
and the increasing internationalization of the labor market made English language
fluency even more necessary, and thus promoting the use of English language should
be another key issue of the ASEAN Economic Community.
As a matter of fact, to be able to compete with skilled labor from other
member countries for positions in foreign industries, merely having professional skills
and years of work experience may not be sufficient. Skilled workers who also have
language skills and are able to demonstrate them when required in their work fields
certainly have greater career opportunities in ASEAN integrated market. However, as
mentioned earlier, countries where English is not an official language usually
encounter the problems of language barriers.
Thailand is considered one of the countries where readiness of skilled
labor in terms of English language fluency is still questionable. To begin with,
English learning in Thailand is not very successful. Although the English language is
one of the compulsory subjects and Thai learners spend more than a decade studying
it, their English abilities are still minimal. Causes of the problem are mainly the lack
of exposure to English language, especially inadequate opportunity to practice using
English in and outside the classroom, the lack of skilled teachers, well-equipped
classrooms and practical learning materials, and the lack of confidence from the
learners themselves when communicating in English (Wiriyachitra, 2003).
Since many fundamental problems of English learning in Thailand are still
unsettled, a great number of Thai learners and workers are potentially at a
disadvantage when joining the ASEAN labor market and foreign industries.
The country’s problem in English proficiency also can be seen in the
annual survey of Education First English Proficiency Index (EF EPI). Since 2011,
Education First has provided the ranking of countries by English skills, including
countries in Europe, Asia, Latin America, Middle East and North Africa, and has
categorized those countries into five groups: very high, high, moderate, low, and very
low proficiency. Among Asian countries, Thailand was one of a few countries that
have been continually ranked in the group of very low proficiency. In the fifth year,
Ref. code: 25615721042223AND
5
the index again showed a decline in the English proficiency of the country. Thai
participants still exhibited poor English skills and thus the country was ranked 62nd
out of 70 nations and was the third-worst country in Asia (EF EPI, 2015).
Furthermore, recent test and score data summary of TOEFL tests revealed
that Thai test takers only got an average score of 77, which was much less than scores
that test takers from other ASEAN member countries such as Singapore, Philippines,
Malaysia, and Indonesia received. Nevertheless, the fact that Thailand was ranked
behind those four countries was not as surprising as the fact that now the country also
falls behind Myanmar and Vietnam since their test takers already passed the
international standardized test score of 80 (Test and Score Data Summary for TOEFL,
2016). When examining previous reports on scores and ranking of countries by
English proficiency, it can be seen that while other ASEAN member countries have
made some progress, Thailand has not really made its advancement manifest.
As the country is one of the founding fathers of ASEAN and a member of
the ASEAN Economic Community (AEC), it is necessary that Thai people, especially
the skilled labor of the eight listed ASEAN occupations, are aware of the challenges
from the free flow of goods, services, and labor and the importance of language skills.
According to the Thailand Board of Investment (2016), among the eight listed
ASEAN occupations, medical services and occupations involved in healthcare
industry are currently in the spotlight as the government spends 14% of its total
budget on the healthcare industry, which is considered to be the highest in ASEAN.
The immense support from the government in the field of health services
is due to the fact that a large number of foreign patients and visitors, especially from
the United States and Western Europe, who need medical treatment and related
services choose Thailand over other countries in the region as their healthcare
destination. Since the early 2000s, the number of foreign patients has continually risen
as medical services in Thailand conformed to internationally accepted standards;
besides, the price, package service, and tourist places in Thailand were found more
attractive. Seeing that the country had potential to be a medical hub and the income
from medical services to foreign patients increased steadily every year, the
government set a vision for Thailand as ‘World Class Healthcare Destination and
Ref. code: 25615721042223AND

6
Academic Medical Hub of Asia’ in 2004 and has been pushing for the continued
development of medical tourism ever since (Ministry of Tourism and Sports, 2010).
Since Thai medical workers have to encounter not only challenges from
the integration of the ASEAN Economic Community but also from the goal of the
country being the ‘Medical Hub’ of Asia, it is even more necessary to emphasize the
importance and the development of English language skills among workers in the
healthcare industry.
Therefore, in this study a needs analysis on English functional skills was
specifically conducted with Thai workers involved in three ASEAN occupations: (1)
medical services, (2) dental services, and (3) nursing services. Targeted participants
were selected from eight governmental hospitals in Prachuabkirikhan: (1) Hua Hin
Hospital, (2) Pranburi Hospital, (3) Samroiyod Hospital, (4) Kuiburi Hospital, (5)
Prachuabkirikhan Hospital, (6) Thapsakae Hospital, (7) Bangsaphan Hospital, and (8)
Bangsaphan Noi Hospital. Considering that Prachuabkirikhan has been one of the
most popular tourist destinations in Thailand and its attractions were number one in
top searches of the TAT official website (Tourism Authority of Thailand, 2016),
health care workers in Prachuabkirikhan, therefore, can be considered important
subjects for the study.
1.2 OBJECTIVE OF THE STUDY
The objective of this study is to investigate English functional skills
needed for three ASEAN health-related occupations: medical services, dental services,
and nursing services.
1.3 RESEARCH QUESTIONS
Regarding the objective, the study seeks answers to the following
questions:
1.3.1 What are the English skills needed for Thai skilled labor involved in
medical services?
Ref. code: 25615721042223AND

7
1.3.2 What are the English skills needed for Thai skilled labor involved in
dental services?
1.3.3 What are the English skills needed for Thai skilled labor involved in
nursing services?
1.3.4 What background factors correlate with English proficiency of the
skilled labor?
1.4 SCOPE OF THE STUDY
This study focuses on needs for English skills of Thai skilled labor of
three ASEAN health-related occupations: medical services, dental services, and
nursing services. The participants in this study comprised 251 healthcare
professionals from eight governmental hospitals in Prachuabkirikhan:
(1) Hua Hin Hospital
(2) Pranburi Hospital
(3) Samroiyod Hospital
(4) Kuiburi Hospital
(5) Prachuabkirikhan Hospital
(6) Thapsakae Hospital
(7) Bangsaphan Hospital
(8) Bangsaphan Noi Hospital
1.5 DEFINITION OF TERMS
The definitions of key terms of this study are as follows:
1.5.1 English skills refers to English functional skills in listening,
speaking, reading, and writing that health services professionals use in medical
settings.
1.5.2 Health services professionals of AEC refers to skilled workers of
three healthcare occupations—medical, dental, and nursing services—that are granted
mobility in the labor market of the ASEAN Economic community.
Ref. code: 25615721042223AND

8
1.6 SIGNIFICANCE OF THE STUDY
1.6.1 The study enhances understanding about English functional skills
needed for three ASEAN occupations: medical services, dental services, and nursing
services, and provides insights into the analysis of English needs of Thai healthcare
workers.
1.6.2 The study provides implications for course design of English for
Medical Purposes (EMP) for curriculum designers and those involved in ELT.
1.6.3 The study enriches the current literature on English for Specific
Purposes (ESP) and English for Occupational Purposes (EOP) in the Southeast Asian
context.
1.7 ORGANIZATION OF THE STUDY
This research paper is divided into five chapters as follows:
1.7.1 Chapter one introduces the research paper which involves
background, objective of the study, research questions, scope of the study, definition
of terms and significance of the study.
1.7.2 Chapter two reviews research and literature that are relevant to the
study.
1.7.3 Chapter three describes the methodology of the study which
includes the participants (population, sample size, and sampling procedure), research
instrument, procedures of data collection and data analysis.
1.7.4 Chapter four reports the result of the study.
1.7.5 Chapter five provides conclusion, discussion, and recommendations
for further study.
Ref. code: 25615721042223AND

9
CHAPTER 2
REVIEW OF LITERATURE
This chapter reviews the literature in four areas: (1) English for Specific
Purposes (ESP), (2) Needs Analysis (NA), (3) English for Occupational Purposes
(EOP) and (4) previous related studies.
2.1 ENGLISH FOR SPECIFIC PURPOSES
2.1.1 Definitions of English for Specific Purposes
The term English for Specific Purposes (ESP) has been defined by a
number of scholars and practitioners. According to Kennedy and Bolitho (1984), ESP
is one particular aspect of English Language Teaching (ELT) that emerges due to the
growth in demands of English language speaking as a common medium of
communication. These demands come from groups of learners with specific purposes
or particular reasons connected with their studies or their jobs. ESP courses are thus
based on the needs of learners in their situations. Their purposes of learning, needs,
and interests are key information that can be used as a guideline for the content of a
course.
Hutchinson and Waters (1987) define English for Specific Purposes (ESP)
as the type of language teaching that has its focus on aspects of language used in a
particular discipline and interest in learner-centered approaches in which learners’
reasons for learning are considered an important factor that affects all decisions
related to language teaching and syllabus content. They explain further that the
emergence of ESP was considered as a phenomenon that grew out of trends in the
1940s. The new generation of learners in that period of time did not learn English for
the pleasure or in order to be regarded as educated people, instead they learned
English for their specific purposes, for example, learners who were businessmen
wanted to learn English in order to be able to sell their products in international
markets and learners who were mechanics needed English in order to be able to read
instruction manuals and work with foreign companies. Given that there was a wide
variety of language usage in each context, language instruction shifted its attention
Ref. code: 25615721042223AND
10
from defining the formal features of the language and describing its usage to finding
the ways in which language was actually used in real situation. Due to this new
interest in English language learning, ESP courses were developed and designed
according to linguistic characteristics of learners’ area of work and study and what
they need the language for.
Streven (1988) offers a definition of ESP by identifying its characteristics:
(1) The absolute characteristics are that ESP consists of English language
teaching which is:
designed to meet specified needs of the learner;
related in content, i.e., in its themes and topics to particular disciplines,
occupations, and activities;
centered on the language appropriate to those activities in syntax, lexis,
discourse, semantics and so on, and analysis of the discourse;
in contrast with ‘General English’.
(2) The variable characteristics are that ESP may be:
restricted as to the language skills to be learned (e.g. reading only);
not taught according to any pre-ordained methodology (pp.1-2).
Robinson (1991), unlike other scholars, states that a simple, absolute
definition of ESP is not easy to produce as the full term ‘English for Specific
Purposes’ itself can be interpreted as 'what is specific and appropriate in one part of
the globe may well not be elsewhere’. Nevertheless, she points out that ESP is
basically goal-directed since students study English not because they are interested in
the language but because they need the language for their academic or career
purposes. Thus, ESP courses are designed based on needs analysis which identifies
aims and goals of learners and what exactly they need English language for. Usually,
ESP courses have a specified time period for the course, so it is necessary that
objectives of learning are clearly specified from the beginning and stakeholders of the
Ref. code: 25615721042223AND

11
course, i.e., organizers, planners, teachers, and students collaborate during the process
in order to design the course according to time available.
Dudley-Evans and St. John (1998) view ESP as a separate activity within
English Language Teaching (ELT) and part of a more general movement of teaching
Language for Specific Purposes (LSP) which has its focus on teaching languages, i.e.,
French and German for specific purposes as well. Although ESP is often seen as
lacking an underlying theory, they believe that the theory of ESP can be outlined
based on “the specific nature of the texts that learners require knowledge of, or on the
basis of the needs-related nature of teaching”. Thus, in their definition ESP teaching
has its own methodology and the interaction between the teachers and the learners in
ESP class may be very different from that in a general English class.
Instead of providing a simple definition of ESP, Dudley-Evans and St.
John clarify the term by presenting its features and categorizing them into two
groups:
(1) Absolute characteristics:
ESP is designed to meet specific needs of the learner;
ESP makes use of the underlying methodology and activities of the
disciplines it serves;
ESP is centered on the language (grammar, lexis, register), skills,
discourse, and genres appropriate to these activities.
(2) Variable characteristics:
ESP may be related to or designed for specific disciplines;
ESP may use, in specific teaching situations, a different methodology
from that of general English;
ESP is likely to be designed for adult learners, either at a tertiary level
institution or in a professional work situation. It could, however, be used
for learners at secondary school level;
Ref. code: 25615721042223AND

12
ESP is generally designed for intermediate or advanced students. Most ESP
courses assume basic knowledge of the language system, but it can be used
with beginners (pp. 4-5).
Anthony (1997) points out that Streven’s (1988) theory had considerable
influence on Dudley-Evans’ definition of ESP. In Dudley-Evans and St. John’s (1998)
version, it is obvious that they modify Streven’s (1988) by removing one absolute
characteristic that says ESP is in contrast with ‘General English’ and including two
more variable characteristics. In their view, ESP should be seen as a simple approach
to teaching that is not necessarily concerned with a specific age group or ability range.
Anthony (1997) adds that when it comes to arguments about what is and what is not
ESP, Dudley-Evans and St. John’s modified version of ESP characteristics can be
very helpful in making a distinction between those that are concerned with ESP and
those that are not.
2.1.2 Characteristics of English for Specific Purposes
Carver (1983) stated that there are three main characteristics of ESP:
authentic materials, purpose-related orientation, and self-direction. ESP usually makes
use of authentic learning materials and simulation of communicative tasks required of
the target setting (purpose-related orientation). Learners of ESP will get to practice
their target language in various functional tasks, for example, in a simulation of a
conference in an English for Medical Science program, the first group of students are
assigned to give presentations on case studies of patients while the second group have
to do research on the topic and prepare for discussion; in English for business courses,
students have to design presentations of company products, create a logo, and do
market research.
As for self-direction, ESP course design is often influenced by learners.
However, in order for it to occur, the cooperation between learners and planners also
needs to be encouraged. In other words, planners and teachers may design the
learning strategies and teach the learners how to learn but they also have to give the
learners a certain degree of freedom to decide what, when and how they will study.
Ref. code: 25615721042223AND

13
According to Widdowson (1983), many discussions on the characteristics
of ESP also involve the comparative relationship between ESP and EGP (or English
for General Purposes). Widdowson states that the distinctive difference between ESP
and EGP lies in their focuses: the main focus of ESP is on training while in EGP, the
main focus is often on education. English taught in ESP is intended to be used in a
specific context, for example, in business, legal, medical, or any other context
depending on what learners need the language for. On the contrary, English for
General Purposes is usually considered as one of a school’s compulsory subjects in
which English is taught along with other subjects for educational purposes. The
selection of contents for an ESP course thus tends to be easier than the selection of
contents for an EGP course since the language context and objectives of learning are
clearly specified from the beginning.
Fiorito (2006) points out that the difference between ESP and EGP is also
in the aims of instruction. In EGP all four English skills: listening, reading, speaking,
and writing are stressed equally. However, in ESP it depends on an assessment of
purposes and needs of the learners and the functions for which English is required; for
example, an ESP course for learners who study English in order to work in the
tourism industry may center on the development in speaking skill while an ESP
course for learners who study English in order to work in business administration may
emphasize reading skill more than the three other skills.
Furthermore, Fiorito adds that ESP covers a wider range of subjects than
EGP. The context varies from accounting, engineering and medical to business
management, hotel and tourism. ESP focuses more on language skills and the context
in which they will be used than grammar or sentence structures. In an ESP classroom,
English language will be integrated into subject matters that are important to the
learners so that they can study the language through a field that is relevant to them.
This relevance, in turn, will enhance learners’ interest in language learning and
motivate them to interact with speakers and texts.
Ref. code: 25615721042223AND

14
2.1.3 Objectives of ESP teaching
According to Stern (1992), objectives of ESP teaching can be
distinguished into four types:
(1) Proficiency objectives—mastery of skills, i.e., listening, speaking,
reading, and writing;
(2) Knowledge objectives—the acquisition of linguistic and cultural
information;
(3) Affective objectives—the development of positive feelings toward the
subject of study;
(4) Transfer objectives—the ability to generalize from what has been
learnt in one situation to other situations.
Based on Stern (1992)’s concept, Basturkmen (2006) develops her
categorization, comprising five broad objectives of ESP teaching:
(1) To reveal subject-specific language use
ESP teaching with this objective is linked to Stern’s knowledge objective
(linguistic and cultural knowledge). The learners will be taught to understand how
English is used in the target environment. The instruction oriented to this objective
involves language analysis and language with socio-cultural rules (e.g. norms, values,
what is acceptable and what is not).
(2) To develop target performance competencies
This objective is linked to Stern’s proficiency objectives. The emphasis of
the instruction is oriented toward the operation of language, for instance, what people
do with the language and the skills they need to do it. Courses are built around core
English skills (listening, speaking, reading, and writing) and micro-skills in term of
competencies. The construction of the courses is basically based on the needs analysis
Ref. code: 25615721042223AND
15
which identifies what expectations of the target situation are and how the teacher can
help the learners meet those demands or the level of competency expected.
(3) To teach underlying knowledge
ESP teaching with this objective emphasizes on both linguistic
proficiency and knowledge and knowledge and understanding of disciplinary
concepts. To teach underlying knowledge is to impart to students the knowledge
about linguistic and cultural information which means that the learners will study
content areas related to their professions or disciplines alongside the language use in
their specific contexts, i.e., teaching medical students about cases of early-stage
cancer while teaching language use for describing processes of treatment to the
patients.
(4) To develop strategic competence
Strategic competence can be defined as the means that enables language
knowledge and content knowledge to be used in communication. ESP teaching with
this objective focuses on the link between context of situation and language
knowledge from which appropriate teaching approach can be identified and assigned
to the course. For example, in order to deliver a successful ESP course to the class of
postgraduate students from highly specialized fields, a team teaching strategic, which
involves three parties: the ESP teacher, the subject specialist, and the students, is
developed and applied to the course.
(5) To foster critical awareness
ESP teaching with this objective aims to point out that not all norms and
practices in English language teaching are necessarily desirable. The learners will be
taught to understand how norms and communicative practices in the target
environments become established, raise their critical awareness of the negative
aspects, and discuss the way to change or modify the situation so that a more sensible
relation between their circumstances and the norms can be established.
Ref. code: 25615721042223AND
16
2.2 NEEDS ANALYSIS
2.2.1 Definitions of Needs Analysis
Hutchinson and Waters (1987) regard the term ‘needs analysis’ as the
basis of any course design in a sphere of teaching English for Specific Purposes. An
awareness of the needs can determine what is and what is not acceptable as reasonable
content in the language course and what potential can be exploited. Although on the
surface ESP courses are likely to be categorized by their content, for example,
medicine, commerce, and tourism, it is, in fact, only a secondary consequence of the
primary matter of being able to specify why the learners need English.
In detailed explanation of ‘needs’, they add that in the language-centered
approach, the term can be referred to as “the ability to comprehend and/ or produce
the linguistic features of the target situation”.
Robinson (1991) states that ‘needs’ refers to what learners would like to
gain from the language course. Learners themselves may have personal aims in
addition to, or even opposite to, the requirements of their studies or jobs. In other
senses, the term may be interpreted differently, for instance, in a goal-oriented
definition, the term ‘needs’ can refer to what learners have to be able to do at the end
of their language course. Needs in this sense can be regarded as objective needs. In
process-oriented definition, however, the term refers to what learners need to do to
actually acquire the language. Furthermore, ‘needs’ can also be considered as lacks
which means what the learners do not know or cannot do in English.
Brown (1995) notes that naturally, in education programs, needs analysis
focuses on the learning needs of the students. Their needs then will be translated into
learning objectives which serve as the basis for further development in the
curriculum, for example, development in teaching materials, learning activities, and
evaluation strategies. Thus, needs analysis can be considered one of the main
components of a language learning program.
Dudley-Evans and St. John (1998) considered needs analysis as the
process of establishing the ‘what’ and ‘how’ of a course. Their concept of needs
analysis in ESP includes consideration of the following aspects:
Ref. code: 25615721042223AND

17
(1) Professional information about the learners
(2) Personal information about the learners
(3) English language information about the learners
(4) The learners’ lacks
(5) Language learning information
(6) Professional communication information
(7) What is wanted from the course
(8) Information about the environment in which the course will be run.
2.2.2 Types of Needs and Needs Analysis
Hutchinson and Waters (1987) divide needs into two main types: target
needs and learning needs.
Target needs refers to what the learners need to do in the target situation.
These types of needs can be further divided into three forms:
(1) Necessities: what the learners have to know in the target situation.
(2) Lacks: the gap between learners’ present abilities and what the
learners have to know in the target situation.
(3) Wants: the learners’ image of their own needs.
Learning needs refers to what the learners need to do in order to learn.
Long and Doughty (2011) provided a combination of West’s (1994; 1997)
and Jordan’s (1997) lists of different types of needs analysis which includes the
following nine types of language needs analysis:
(1) Target-situation analysis seeks information on the language
requirements learners face in learning a language.
(2) Deficiency analysis seeks learners’ current wants, needs, and their
lacks.
(3) Present-situation analysis focuses on the students’ proficiencies at the
beginning of instruction.
(4) Learning-oriented analysis takes the view that needs (in terms of
syllabus, content, teaching, methods, materials, etc.) should be negotiated between
learners and other stakeholders.
Ref. code: 25615721042223AND

18
(5) Strategy analysis investigates learners’ preferences in terms of
learning strategies, error correction, class sizes, etc.
(6) Mean analysis focuses on the learning situation, with as few
preconceptions as possible in terms of practicality, logistics, cultural appropriateness,
etc.
(7) Language audits focuses on a large-scale view of needs analysis in
terms of strategic language policies for companies, professional sectors, governmental
departments, countries, etc.
(8) Set menu analysis sets out to create a menu of main courses from
which the sponsors or learners can select.
(9) Computer-based analysis is done by computer to match perceived
needs to a database of materials, from which the course content can be negotiated
between learners and teachers.
2.2.3 Data gathering options for Needs Analysis
2.2.3.1 Munby’s (1978) Communication Needs Processor (CNP)
To find target situation needs, Munby (1978, cited in Hutchinson and
Waters, 1987) created a highly-detailed set of procedures that consisted of a range of
questions about variables that affect communication needs called the Communication
Needs Processor (CNP).
Learners’ needs can be identified after their information is examined
and sorted into the following categories (Munby, 1978, cited in Gillett, 1989):
- Participant (e.g. age, sex, nationality, present ability)
- Purposive Domain (type of ESP, e.g., commerce, law, tourism)
- Setting (time and place)
- Intersection (the role of participants, including status, social
relationship etc.)
- Instrumentality
I. Medium of communication (e.g. spoken: receptive and
productive)
II. Channel of communication (e.g. face to face, print)
- Dialect (e.g. British or American accents and dialects)
Ref. code: 25615721042223AND

19
- Target level (level of linguistic proficiency)
- Communicative event (what learners have to do with English,
e.g., attend lectures or participate in seminar)
- Communicative key (e.g. formal/ informal, a range of attitudes)
- Profile (what learners need to be able to do)
The comprehensive data banks are regarded as a ‘profile of needs’ which
simply means a description of what the learner will be expected to do with language
at the end of the course (Gillett, 1989). Once learners’ target situation is completely
plotted, the insight can be used as checklists for a resultant syllabus and the stage at
which ‘good enough’ competence for learners’ goals can be determined (Robinson,
1991).
2.2.3.2 Hutchinson and Waters’ (1987) checklists
Hutchinson and Waters state that there are a number of ways to gather
the data for needs analysis. The analyst may choose to use a questionnaire, conduct an
interview, observation, or any other options that they consider desirable and in
accordance with the time and resources available. The most important thing is that the
chosen method must cover all the points stated in the following frameworks:
Target needs framework
1. Why is the language needed?
2. How will the language be used?
3. What will the content areas be?
4. Who will the learner use the language with?
5. Where will the language be used?
6. When will the language be used?
Learning needs framework
1. Why are the learners taking the course?
2. How do the learners learn?
3. What resources are available?
4. Who are the learners?
5. Where will the ESP course take place?
6. When will the ESP course take place?
Ref. code: 25615721042223AND
20
2.2.3.3 Robinson (1991)’s seven techniques
To investigate learners’ needs, Robinson suggests the following
techniques:
(1) Questionnaires
Questionnaires can be beneficial when there are a large number of
people involved in the analysis of needs; however, the need analyst may not be able to
fully take control of the method since there is no guarantee that all respondents will
complete and return the questionnaires. Nevertheless, if one decides to use
questionnaires, Robinson suggests that he or she should prepare a pilot version and try
it out on a few respondents first in order to check if the questions are comprehensible
and the answers can be easily analyzed and compared.
(2) Interviews
The structured interview is highly recommended in the analysis of
learners’ needs since the interviewer can plan an agenda beforehand, guide the
interviewees through the questionnaires and pursue any interesting new line of
enquiry that develops.
(3) Observation
Observation can be a supplement to the analysis of needs. The analyst
may gather respondents’ opinion by using questionnaires and interview; however, it is
best to have a direct observation so that learners’ target-level behavior and their actual
performance can be identified. In conducting an observation, it is essential that the
observer establish good relations with the participants. The process may be time-
consuming; thus, the observer has to be patient and at the same time be careful of any
interference he or she may cause during the observation.
(4) Case studies
A case study approach is similar to observation but the method gives
more in-depth information about the person being observed. It provides the
opportunity for the observer to closely examine learners’ difficulties and needs in
more detail than in the oral interview or the questionnaires and for the course planner
to gain more insights into learners’ methods of learning. The disadvantages, however,
are that the method may consume even more time than the simple observation and
Ref. code: 25615721042223AND

21
since it does not involve a large number of participants, the result may not be
generalizable.
(5) Tests
The test allows the analyst and the course designer to have some idea
of learners’ present ability. Since it requires the learners to perform target-level tasks,
learners will have to show what they are capable of and what their deficiencies are. It
is essential that the test is reliable and validated so that the result can be used in the
course design.
(6) Authentic data collection
Authentic data collection refers to the making of audio or video
recordings in situations where the language is used, for example, in a business
meeting, university seminar, or lecture room, and to the collection of print material,
for example, samples of students’ examinations, books and journal articles that they
have to read. The records will show what kind of linguistic component, actions, and
gestures are involved in such situation. The analyst and the course designer have to
decide which one of them are useful and need to be included in the course.
(7) Participatory needs analysis
This method involves the learners more actively. Apart from using
questionnaires to investigate learners’ opinion, there are also discussions about their
needs between learners and course designer. Moreover, learners will be encouraged to
make recommendations as to what happens in the resultant course and about the needs
that emerge during learning process.
As this study focuses on English skills needed for professionals of
medical, dental, and nursing services in Prachuabkirikhan, Thailand, a large number
of participants were involved in the study. Thus, the best option was to apply a
quantitative approach such as questionnaires to collect the data. Regarding
Robinson’s suggest, the questionnaires would be piloted with a few respondents to
confirm its comprehensibility before distributing to a focus group for this study.
2.2.4 Steps in Needs Analysis
Long and Doughty (2011) stated that there are many scholars who
propose sets of steps in the needs analysis process, for example, Schutz and
Ref. code: 25615721042223AND

22
Derwing’s (1981) eight steps, Jordan’s (1997) ten steps, and Graves’s (2000) seven
steps. Noticing some overlap in previous three sets, they combined and sorted the
steps into three general stages:
(1) Get ready to do NA;
(2) Do the NA research;
(3) Use the NA results.
Table 2.1
Steps in Needs Analysis (adapted from Long & Doughty, 2011)
Stages Steps
Get ready to do NA 1. Define the purpose of the NA
2. Delimit the learner population
3. Decide upon approach(es) and
syllabus(es)
4. Recognize constraints
5. Select data collection procedures
Do the NA research 6. Collect data
7. Analyze data
8. Interpret results
Use the NA results 9. Determine objectives (Implement
decisions, i.e., assessments,
materials, teaching strategies, etc.)
10. Evaluate the report on the NA
project
The selection of data collection methods for the study can be outlined
based on the steps suggested by Long and Doughty (2011). Considering that the
purpose of this study was to identify English needs of Thai skilled labor of the AEC,
the subjects of this study thus should be those involved in the eight occupations that
are granted mobility in the AEC, which includes engineers, nurses, architects,
accountants, doctors, and dentists. However, nowadays, medical tourism in Thailand
is booming and the country is now striving to be the ‘Medical Hub’ of Asia, so more
Ref. code: 25615721042223AND
23
studies on the English proficiency of Thai healthcare workers and their ability to deal
with language barriers are necessary at the moment. Thus, the emphasis of this study
was placed on the English needs of Thai skilled labor involved in three ASEAN
occupations: medical, dental, and nursing services.
As Robinson (1991) suggested, the questionnaire is considered a suitable
method for data collection when there are a large number of people involved in the
analysis of needs. Other advantages are that the questionnaire provides researchers
with standardized data since it can produce large amounts of data and so increase the
reliability and validity of findings. Also, generalizations are consequently much easier
to draw from the larger databases that this method makes possible. When compared to
the use of interviews, there is also a lower risk of manipulation of the data on the part
of the interviewer, and so interviewer bias is minimized. A further advantage of the
questionnaire is that they tend to be completed by respondents and returned to the
researchers in complete anonymity. Anonymous informants may feel less inhibited
about answering questions on certain kinds of topics, allowing the researcher to
access information on an individual or organization that might be considered sensitive
(Huhta, Vogt, Johnson, Tulkki, & Hall, 2013).
In designing questionnaires, Munby’s (1987) framework can be beneficial
for plotting participants’ target situation needs and Hutchinson and Waters’ (1987)
checklists can help cover points that should be asked in questionnaires. The data
collected from the participants can show not only what English skills are necessary in
their working conditions but also their present abilities and their lacks as well.
2.3 ENGLISH FOR OCCUPATIONAL PURPOSES
2.3.1 Definitions and classifications of English for Occupational
Purposes
According to Kennedy and Bolitho (1984), English for Occupational
Purposes (EOP) is one of English for Specific Purposes (ESP)’s main divisions. EOP
is generally taught in a situation in which learners need to use English as part of their
work or profession. For example, an intermediate course in secretarial services for
company secretaries who need English practical skills and theoretical knowledge and
an advanced course for ones who are already qualified secretaries but now need to
Ref. code: 25615721042223AND

24
operate in English. Each EOP course is different depending on whether the learners
are learning English before, during or after the time they are being trained in their job
or profession. Citing Stevens (1977), subdivisions of EOP are as follows:
Figure 2.1 Classification of EOP Courses (adapted from Stevens, 1977)
Robinson’s (1991) classification of EOP is also similar to Kennedy and
Bolitho’s (1984). She makes a distinction between EOP and EAP, stating that EOP is
involved with work-related needs and training only while EAP is concerned with
academic study needs. She divides EOP courses into three types: (1) pre-experience,
(2) simultaneous/ in-service, and (3) post-experience. The classification and the
components of the course are determined by learners’ professional stages whether
they are newcomers to the field of work, on the way to become expert, or already
expert.
Table 2.2
Classification of EOP Courses (adapted from Robinson, 1991)
Types of learners Components of EOP course
Newcomers (pre-experience) Instruction in the concepts
Practices of that field
Experienced learners (simultaneous/ in-
service and post-experience)
Operational materials (that boost
the ability to function in English)
Experienced learners (simultaneous/ in-
service and post-experience)
Application of knowledge and
concept in authentic tasks
Ref. code: 25615721042223AND

25
Robinson (1991) points out that the important distinction is between English
which is instructional and English which is operational. The key elements that EOP
teachers need to take into consideration are learners’ stages and situation since they
will determine the kind of content knowledge and the degree of generality or
specificity of the course.
Another famous classification of ESP is presented by Hutchinson and
Waters (1987). They created a chart called ‘The Tree of ELT’ in order to clarify the
relationship between ELT and ESP, and their divisions, which include EOP and EAP:
Figure 2.2 The Tree of ELT (Hutchinson & Waters, 1987)
Ref. code: 25615721042223AND

26
Hutchinson and Waters (1987) stated that ESP can be categorized into two
main types depending on the purposes of the learners:
(1) English for Academic Purposes (EAP) which is for learners who
require English for academic study;
(2) English for Occupational Purposes/ English for Vocational Purposes/
Vocational English as a Second Language (EOP/ EVP/ VESL) which is for learners
who require English for work or training.
However, when considering the bigger picture and taking the general
nature of the learners’ specialties into consideration, ESP courses are divided into
three categories: English for Science and Technology (EST), English for Business and
Economics (EBE), and English for Social Studies (ESS) of which EAP and EOP are
two main subdivisions.
Hutchinson and Waters (1987) explained that although EAP and EOP are
two different branches, there is actually no clear-cut distinction between them since
people can work and study simultaneously and in many cases the language they learn
in a study environment can be used later in a vocational environment as well.
Gatehouse (2001) notes that Hutchinson and Waters (1987) classification of ESP and
Carver’s (1983) share some similarities since Carver categorizes EAP and EOP under
the same division. Gatehouse (2001) notes that Carver believed that the purposes of
EAP and EOP are the same since both are concerned with employment. Although the
means to achieve is very different, the end purpose is still identical.
Dudley-Evans and St. John (1998) regarded the term EOP as English that
is for professional purposes in administration, medicine, law and business, and
vocational purposes for non-professionals in work or pre-work situations.
Ref. code: 25615721042223AND

27
Figure 2.3 ESP Classification by Professional Area (Dudley-Evans & St. John, 1998)
In their classification, Dudley-Evans and St. John (1998) give further
explanation on EOP and its subdivisions as follows:
English for Business Purposes (EBP): EBP is a large and important
category; thus, it is usually seen as separate from EOP. However, EBP is
still concerned with occupational purposes. It is thus logical to classify
EBP as an EOP subdivision.
English for Vocational Purposes (EVP): Pre-Vocational English is
concerned with finding a job and interview skills while Vocational
English is centered on the language of training for specific trades or
occupations.
Language and discourse in EOP courses are designed for functional
purposes. For example, a course for occupational (professional) purposes
is likely to be designed for learners who are in the work field, i.e.,
practicing doctors, while a course for academic purposes is more
appropriate for learners who still need instruction on concepts and
training, i.e., medical students.
2.3.2. English for Medical Purposes (EMP)
English for Medical Purposes (EMP) is considered a branch of English for
Occupational Purposes. The teaching of English in EMP is closely related to ESP,
however, EMP has its emphasis on linguistic aspects of biomedical communication
Ref. code: 25615721042223AND
28
(e.g. grammatical problems in modern medical writing, styles of medical writing,
public speaking) and a specific set of medical discourse which involves particular
terminology that personnel in the medical profession employ to effectively and
accurately achieve a communicative purpose in healthcare settings (Gylys &
Wedding, 1983).
Shi (2009, as cited in Hoekje & Tipton, 2011) explains that the teaching
of English in EMP on the macro level is either professional or educational; the former
is for medical learners who already use English in their job, and the latter is for those
who enter education programs to prepare for professional medical and health careers.
On the micro level, EMP can be subcategorized into specializations or different
communication tasks that the medical learners perform in healthcare settings. Bosher
and Smalkowski (2002) noted that in order to attain the optimum effectiveness of the
teaching in EMP, a needs analysis for EMP courses should be conducted with extreme
care. The key to success also involves the effective selection of the instrument for the
needs analysis. They suggest that a needs analysis should be based on questionnaires
about the complexities of the healthcare language from the medical learner,
interviews, and/ or observations of different EMP classes.
Shi, Corcos, and Storey (2001) state that there are various types of needs
analyses that can be used to determine EMP course selection and delivery. One of
those that they found effective and recommend is the ‘deficiency needs analysis’
which identifies gaps between the proficiency required to be successful at the targeted
task and current student performance. Their long-period study in Hong Kong Hospital
revealed for researchers and course designers of EMP the authentic language used in
medical contexts, topics and types of interactions, and also the importance of bilingual
competence in mother tongue and technical English for successful provider-patient
communication.
2.4 PREVIOUS RELATED STUDIES
In recent years ESP has developed into one of the most influential
approaches to English teaching due to the effects of globalization within industry and
academia. In the industrial context, workers, especially those involved in
Ref. code: 25615721042223AND
29
collaboration with foreign industry, need strong English skills to succeed in their jobs
while in academia, students need English skills not only for achievement in academic
goals but also for future career prospects. The greater interest in ESP thus has resulted
in increased pressure on ESP planners and teachers to create and deliver successful
ESP courses with effective teaching methods and materials to their classes (Anthony,
2015).
In Asian societies, the status of English is rapidly changing. For example,
in China, Japan, and Korea, English is required in most business meetings and all
sorts of communication in workplaces (e.g. telephone calls, emails, letters) and is also
widely used as a medium in classes at tertiary level (Anthony, 2013). Due to the
globalization of economic and academia in Asia and many other parts of the world
and the increasing necessity of English language, a wider range of subject matters in
ESP has been investigated.
For example, Shi, Corcos, and Storey (2001) analyzed and identified the
communicative skills and needs of medical students who were expected to work in
hospitals as doctors. By observing and videotaping, they clearly identified the specific
authentic talks those participants needed and thus suggested those tasks that should be
employed to develop a syllabus that provides the necessary content areas related to
medical discourse. Situations such as doctor-patient consultation and more specific
discourse functions such as reporting case histories, giving an explanation of an
illness, and explaining the procedures of physical examinations require the application
of authentic materials, role-playing, and simulations.
Orr (2002) examined an EMP course designed for non-native student
nurses at an Australian university. The main focus of the course was English for
admission and registration. The course materials were designed by both a nursing
instructor and English teacher. The results indicated that an EMP course needed by
the students was one that covered both linguistic and communicative features of the
topic and the content areas related to medical topics such as conversations among
patients, doctors and nurses.
Ref. code: 25615721042223AND

30
Tongvivat (2008) investigated the needs of nurses in the Cardiac Intensive
Care Unit (ICCU) of a private hospital in Bangkok in order to develop an English
course specifically for ICCU nurses. In the study, a questionnaire was developed
based on authentic medical discourse, related linguistic features and characteristics of
provider-patient interactions (e.g. asking for patients’ histories, giving advice or
instructions to patients, explaining drug interactions, administering medication,
communicating on the phone). This was distributed to 22 nurses who worked in the
Cardiac Intensive Care Unit. The findings revealed that among the four principal
English language skills, listening and speaking skills were most essential and should
be the major focus of the course and the course subject matter should deal with both
general English and English for nurses that is applicable for nurses’ working
situations.
Patel (2015) studied engineering undergraduates in India who have little
English for the technical part of their academic and professional purposes and their
need of ESP. Through surveying the students’ communicative competence and
reviewing profession needs among engineers and employers of engineers in industry,
it was found that most students only learned English to pass their examinations but
when they started working on a professional platform, they were not able to meet the
corporate requirements. Patel suggested that an ESP course for engineering students
should be relevant to the industry and thus incorporate a variety of professional
competencies in both academic disciplines and knowledge concerned with
professional communication.
In literature on a holistic approach to ESP, Huhta, Vogt, Johnson, Tulkki,
and Hall (2013) addressed the significance of needs analysis on language course
design for business and industry and provided guidelines for a syllabus focusing on
various forms and uses of language in relevant communication situations, for
instance, social situations (introductions, small talks), client contacts, meetings and
negotiations, explaining a process or a working method, discussions concerning
deliveries, installations, and maintenance, giving a presentation (company profile,
product presentation), reading manuals and instructions, and writing emails, reports,
and documents.
Ref. code: 25615721042223AND

31
With the establishment of the ASEAN Economic Community, the role of
English language became even more important as it was formally adopted as an
official language of the ASEAN Community (Kirkpatrick, 2008). The development in
English proficiency, particularly in English communication skills, will benefit both
the workforce and agencies in moving forward sustainably towards the AEC
(Ministry of Labor, 2014). Within this circumstance, it is not surprising that in recent
years literature and studies on English for Specific Purposes and English teaching and
learning as a preparation for AEC have increased substantially, especially in Asian
contexts.
For example, Gass’s (2012) research on Needs Analysis and Situational
Analysis of Thai Nurses was conducted due to the expanding medical tourism
industry in Thailand. The researcher investigated and identified what English skills
were most needed by Thai nurses to design a learner-centered specialized English
curriculum to improve their communicative skills. The subjects of this study were
eight nurses with an average age of 28 – 43. Besides nurses, the data was collected
from foreign patients, the hospital director, TESOL experts, and a nursing expert. The
instruments used to collect data included a questionnaire, an observation, experts’
evaluations, curriculum evaluation, and pre-test/post-test. The results showed that
cultural differences, a different background knowledge, shyness and lack of
confidence were some of the conditions that were preventing the nurses from
interacting with foreign patients. Nevertheless, they had an urgent need for English in
this service. Listening and speaking skills and vocabulary related to the field were
vital for Thai nurses and they needed a course that covered topics related to medical
discourse, such as giving an explanation of an illness, giving instructions on medical
care, explaining drug interactions and administering medication.
Purwanto’s (2014) research on Needs Analysis of English for Specific
Purposes (ESP) for the students of Business and Economic Faculty (FEB)
UNISBANK Semarang (Indonesia) investigated a possible reconstruction of ESP for
the students of FEB through the analysis of their needs in English for the ASEAN
Economic Community (AEC) 2015. The subjects of this study were four faculty
Ref. code: 25615721042223AND

32
officers and one ex-officer, three ESP lecturers and 124 randomly selected students.
The survey was conducted online through MonkeySurvey Software in which the
respondents expressed their opinion about the proposed ESP program. The analysis,
automatically done by the software, indicated that the majority of respondents
expressed positive response to the course constructed under the criteria of Cambridge
University’s Certificate of Proficiency in English (B2 level) which formulated:
(1) Reading Competency Standards—understanding of written texts of
various genres and the use of technical terms;
(2) Listening Competency Standards—understanding of spoken texts of
various genres and the use of technical terms;
(3) Speaking Competency Standards—interacting with native speakers
skilled orally either initiating or responding to spoken text without difficulty on both
sides;
(4) Writing Competency Standard—interacting with native speakers
skilled in writing either initiating or responding to written text without difficulty on
both sides and describing in detail an opinion containing pros and cons of various
things in coverage.
The participants agreed that the proposed ESP program satisfied their
English needs toward the AEC and that it should be offered in the syllabus of the
university.
Prommeechai’s (2014) study looked at the needs of English preparation
for Thai undergraduate students in the Faculty of Architecture in response to the AEC
and opinions on (1) English courses that are currently provided by the Faculty of
Architecture and (2) English language skills that would meet the expectations of the
AEC. The study was conducted with 300 undergraduate architecture students, ten
instructors, and five stakeholders in the architectural field. By means of
questionnaires and interviews, the findings revealed that the participants were aware
of the expansion of labor market in ASEAN and undergraduate students needed to
improve their English language proficiency in order to be competitive in the job
market. Therefore, the participants proposed that the approach of English for Specific
Purposes (ESP) and language content that is practical for working situations should be
Ref. code: 25615721042223AND

33
integrated into English language courses offered by the subject Faculty of
Architecture.
Araminta and Halimi’s (2015) research on the ASEAN Economic
Community 2015: Needs Analysis of Universitas Indonesia’s engineering students
involved 111 alumni and 150 students from the Faculty of Engineering. The
instruments used in this study were questionnaires and semi-structured interviews.
The findings revealed that students’ needs for English language learning were
considered not as high as their needs for English language use. The authors
recommended that the Faculty of Engineering should incorporate an optional course
on English for Professional Purposes into the curriculum and the course should be
collaboratively taught by English professional teachers and lecturers from the Faculty
of Engineering.
Nguyen and Ngo’s (2015) article on English Language Teaching and
Learning in ASEAN Countries and Preparatory Steps to Integrate into the ASEAN
Economic Community (AEC) 2015 provided information and recommendations for
English Language Teaching (ELT) in Vietnam and in other ASEAN Countries. The
authors reviewed studies and literature on issues of ELT in ASEAN countries and
presented eight preparatory steps in ELT to policy makers, researchers, and English
language educators in Vietnam and other countries. These included step (1) having an
English-speaking year and using English (reading and writing) on a particular day;
step (2) having bilingual educational programs; step (3) designing curriculums for the
ASEAN countries and setting up projects on ASEAN studies; step (4) using English
as a medium of instruction in different disciplines at tertiary level; step (5) teaching
English to workers and enhancing teaching English for specific purposes (ESP); step
(6) raising students’ awareness of the importance of the AEC; step (7) giving students
encouragement to learn ASEAN languages and study ASEAN cultures; step (8)
giving students encouragement to take part in English proficiency examinations
before graduation. The article ended with implications for ELT in Vietnam and other
ASEAN countries, stating that the emphasis of ELT should be placed on
communicative purposes and the use of a variety of Englishes in ASEAN region
should be encouraged. Four language skills should be incorporated in language
assessment, and collaboration between ASEAN member countries in raising
Ref. code: 25615721042223AND
34
awareness of the importance of English in the context of the AEC should be
promoted.
Chen, Chang and Chang’s (2016) research on Needs Analysis of English
learning in Taiwan investigated the needs of English learning from the viewpoints of
students and the real needs of employers regarding English usage at the workplace.
The study involved 60 participants comprising 30 senior students from a technology
college in Central Taiwan and 30 employers working in service, tourism, banking,
insurance, construction, manufacturing, and media communications. The results from
the study showed that student and employer perceptions toward English skills needed
in workplaces were very different. The majority of students did not have skills that the
employers needed, such as social communication skills (for overseas exhibition,
hosting VIPs, and socializing with clients) and writing skills for specific tasks (e.g.
minutes and notices). To help students transition successfully to their future careers
after graduation, the researchers thus recommended that students and teachers should
know the skills expected for the workplace and pay more attention to textbook
selection, material compilation, and course design; besides, textbook designers should
survey what the market needs and provide more realistic and adequate materials for
English teachers and learners.
Studies reviewed above support the proposition that to enrich current
studies on English for Specific Purposes in a Thai context and promote English
language development for Thai skilled workers of the AEC, investigation into the
operation of language and competency expected in the target situation needs to be
conducted. Considering that Thailand is also striving to be the ‘Medical Hub’ of Asia
at present, it is necessary that Thai medical workers are able to deal with language
barriers and have a certain level of proficiency in English. Thus, in this study, the
emphasis is placed on Thai workers involved in three ASEAN occupations—medical,
dental, and nursing services—in terms of what they do with the language and the
skills they need to do it. Based on the theory of needs analysis, a research instrument
was developed to investigate English needs of medical workers which involve core
English skills (listening, speaking, reading, and writing) and micro-skills in terms of
medical-related competencies. The content of the questionnaire used in the study
Ref. code: 25615721042223AND

35
includes topics of medical discourse and authentic communication tasks that the
medical workers perform in healthcare settings:
Listening activities: listening to patients’ histories, medical needs, and
inquiries, listening to diagnosis and symptom management, listening to
lectures, talks in conferences, podcast and video instructions, and listening
to various dialects and accents;
Speaking activities: greeting, making general conversation, asking for
patients’ histories, describing symptoms and diagnosis, explaining
medication and treatment, giving medical advice and response to patients’
inquiries, communicating on the telephone, giving presentation, lectures,
and talks at the seminar or international conference;
Reading activities: reading patients’ medical records, reading medical
diagnoses, examination results, medical prescriptions, and manuals or
instructions about medical equipment, reading medical journals, research
articles, textbooks, and general publications;
Writing activities: writing medical records, medical notes, prescriptions,
medical research and articles for medical journals, writing a letter, email,
memo, and resumes.
Ref. code: 25615721042223AND

36
CHAPTER 3
RESEARCH METHODOLOGY
This chapter describes the methodology used in this study. It consists of
(1) the participants, (2) the materials, (3) the procedures used in the data collection,
and (4) the data analysis.
3.1 PARTICIPANTS
3.1.1 Population
The target population of this study was 1,019 Thai male and female
doctors, dentists, and nurses from eight governmental hospitals in Prachuabkirikhan:
(1) Hua Hin hospital, (2) Pranburi hospital, (3) Samroiyod hospital, (4) Kuiburi
hospital, (5) Prachuabkirikhan hospital, (6) Thapsakae hospital, (7) Bangsaphan
hospital, and (8) Bangsaphan Noi hospital.
3.1.2 Sample size
The sample size of this research, which was calculated by using the Taro
Yamane formula (Yamane, 1973) with 95% confidence level, was 251 people.
The calculation formula of Taro Yamane is as follows:
* n = the sample size
N = the population size
e = the acceptable sampling error
3.1.3 Sampling procedure
Participants in this study were selected by stratified random sampling:
(1) Combine numbers of doctors, dentists, and nurses of each hospital
together and apply the rule of three to find the proportion of samples out of total
population (1,019 people).
Ref. code: 25615721042223AND

37
Table 3.1
Proportions of Healthcare Professionals of Each Hospital
Hospitals in
Prachuabkirikhan
Healthcare professionals Proportions (out of total
population) Doctor Dentist Nurse
Hua Hin hospital 50 12 281 0.34
Total = 343
Pranburi hospital 6 3 54 0.06
Total = 63
Samroiyod hospital 7 4 53 0.06
Total = 64
Kuiburi hospital 4 3 44 0.05
Total = 51
Prachuabkirikhan
hospital
31 7 235 0.27
Total = 273
Thapsakae hospital 7 5 52 0.06
Total = 64
Bangsaphan hospital
13 4 102 0.12
Total = 119
Bangsaphan Noi
hospital
4 2 36 0.04
Total = 42
Prachuabkirikhan Public Health Office (2016)
(2) Find the number of samples that should be drawn from each hospital
by multiplying the number of total sample size (251) with each proportion from the
previous table.
Ref. code: 25615721042223AND

38
Table 3.2
Number of Samples from Each Hospital
Sample size = 251
Hospitals in Prachuabkirikhan Number of samples
Hua Hin hospital 85
Pranburi hospital 15
Samroiyod hospital 15
Kuiburi hospital 13
Prachuabkirikhan hospital 68
Thapsakae hospital
15
Bangsaphan hospital 30
Bangsaphan Noi hospital 10
(3) Find the number of samples of each occupation that should be drawn
from each hospital by applying the rule of three with the number of healthcare
professionals of each occupation and the total number of healthcare professionals in
each hospital to find the proportions, then multiply each proportion with the number
of sample size of each hospital from the previous table.
Table 3.3
Number of Samples of Each Occupation from Each Hospital
Hospitals in
Prachuabkirikhan
Healthcare professionals
Doctor Dentist Nurse
Hua Hin Hospital
Total = 343
Sample size = 85
50 12 281
Proportions 0.146 0.035 0.819
Number of samples 12 3 70
Ref. code: 25615721042223AND
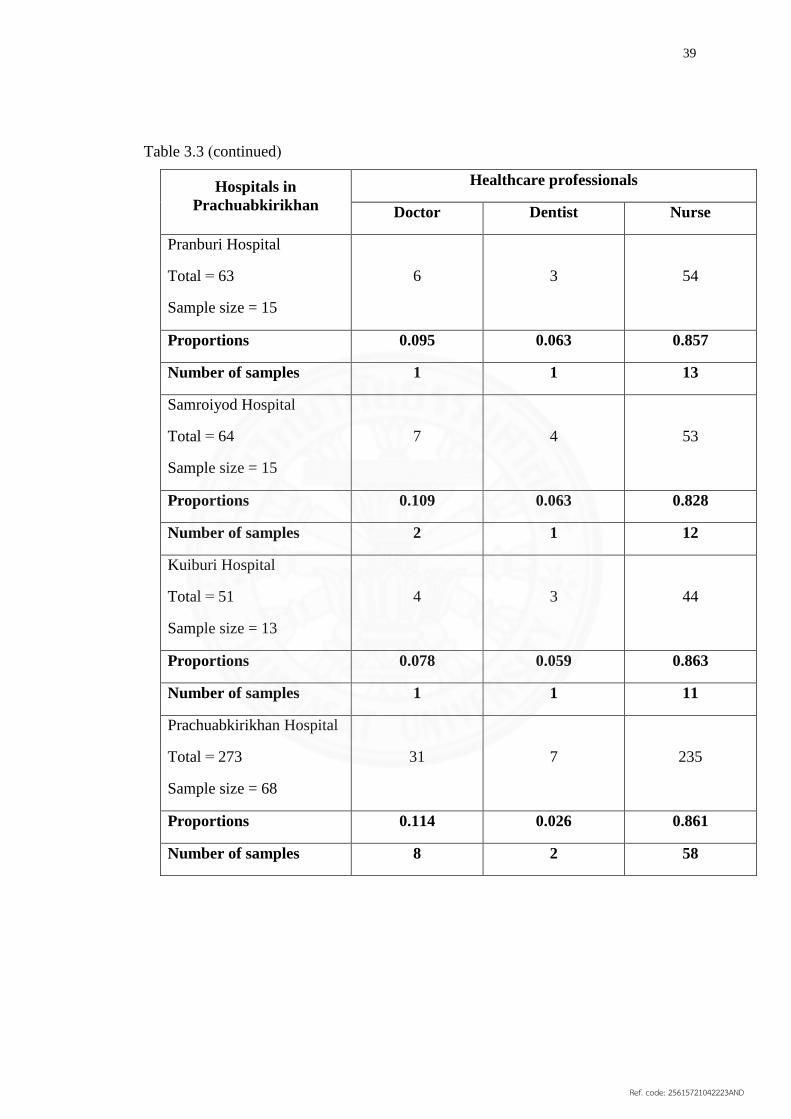
39
Table 3.3 (continued)
Hospitals in
Prachuabkirikhan
Healthcare professionals
Doctor Dentist Nurse
Pranburi Hospital
Total = 63
Sample size = 15
6 3 54
Proportions 0.095 0.063 0.857
Number of samples 1 1 13
Samroiyod Hospital
Total = 64
Sample size = 15
7 4 53
Proportions 0.109 0.063 0.828
Number of samples 2 1 12
Kuiburi Hospital
Total = 51
Sample size = 13
4 3 44
Proportions 0.078 0.059 0.863
Number of samples 1 1 11
Prachuabkirikhan Hospital
Total = 273
Sample size = 68
31 7 235
Proportions 0.114 0.026 0.861
Number of samples 8 2 58
Ref. code: 25615721042223AND

40
Table 3.3 (continued)
Hospitals in
Prachuabkirikhan
Healthcare professionals
Doctor Dentist Nurse
Thapsakae Hospital
Total = 64
Sample size = 15
7 5 52
Proportions 0.109 0.078 0.813
Number of samples 2 1 12
Bangsaphan Hospital
Total = 119
Sample size = 30
13 4 102
Proportions 0.109 0.034 0.857
Number of samples 3 1 26
Bangsaphan Noi Hospital
Total = 42
Sample size = 10
4 2 36
Proportions 0.095 0.048 0.857
Number of samples 1 1 8
In conclusion, the participants of this study were as follows:
12 doctors, 3 dentists, and 70 nurses from Hua Hin hospital
1 doctor, 1 dentist, and 13 nurses from Pranburi hospital
2 doctors, 1 dentist, and 12 nurses from Samroiyod hospital
1 doctor, 1 dentist, and 11 nurses from Kuiburi hospital
8 doctors, 2 dentists, and 58 nurses from Prachuabkirikhan hospital
2 doctors, 1 dentist, and 12 nurses from Thapsakae hospital
3 doctors, 1 dentist, and 26 nurses from Bangsaphan hospital
1 doctor, 1 dentist, and 8 nurses from Bangsaphan Noi hospital
The total number of participants in this study = 251
Ref. code: 25615721042223AND

41
3.2 MATERIALS
The instrument used in this study was a set of self-administered
questionnaires (see Appendix A), developed by evidence from the literature review.
Initially, the questionnaire was designed in English, and then Thai-translations were
inserted in parentheses. The first version of the questionnaire was administered to 10
participants in order to pretest the questionnaire, verify its validity, and extract
specific responses from the participants. The results from the pilot study confirmed
the comprehensibility of the questionnaires.
The questionnaire in this study used a 5-point Likert scale and was
comprised of three sections of questions formulated both in closed-ended and open-
ended formats:
Part 1: Demographics—the first section of the questionnaire was
designed to gather general background information of the participants.
Part 2: Linguistic profile—the second section required the participants
to evaluate their experiences with English skills.
Part 3: English abilities and needs of English skills for the AEC —the
third section required the participants to rate their abilities and needs of English skills
for the AEC. In this part, the 5-point Likert scale was used with the following criteria:
5 = very extensive necessity/ ability
4 = extensive necessity/ ability
3 = moderate necessity/ ability
2 = little necessity/ ability
1 = very little necessity/ ability
3.3 PROCEDURES
3.3.1 Research design
The research was considered as descriptive research. It was aimed to
describe the needs of English skills of Thai health services professionals involved in
three ASEAN occupations: medical, dental, and nursing services. After reviewing
literature and studies in related fields, the quantitative approach was adopted and the
self-administered questionnaire comprising sections of proficiency and needs of
Ref. code: 25615721042223AND

42
listening, speaking, reading, and writing skills in medical setting was developed and
distributed to the participants. The data collected was analyzed and then the
conclusions were drawn and presented.
3.3.2 Data collection
The questionnaire developed from the review of literature was pretested
with 10 participants (three doctors, two dentists, and five nurses who worked and
resided in Prachuabkirikhan) to confirm the comprehensibility of the questionnaire
and extract specific responses from the participants. After receiving feedback from the
participants, the format and language use of the questionnaire was adjusted. To verify
the validity of the instrument, the Index of Item Objective Congruence (IOC) was
conducted by three experts: a physician, Weerawit Wateetip, M.D., a dentist,
Unchalee Wongpanich, D.D.S., and an English lecturer who was a former nurse,
Chalong Rattanapong, Ph.D. The result for each item in the questionnaire was higher
than 0.50 which confirmed the validity of the questionnaire. To collect the data from
doctors, dentists, and nurses, the consent form (Appendix B) was sent to the director
of each hospital in advance. After receiving permission, the researcher distributed
questionnaires to the participants of eight governmental hospitals in
Prachuabkirikhan. Due to the tight schedules of the participants, the completed
questionnaire was collected 1-2 weeks later and the analysis of data was carried out.
3.4 DATA ANALYSIS
The data obtained was statistically analyzed using the Statistical Package
for the Social Sciences (SPSS) version number 21.
3.4.1 Results from Part One of the questionnaire
The data collected from part one of the questionnaire was analyzed by
using frequency distribution and percentage. The first part of the questionnaire
includes general information about the participants: genders, age, education,
profession, and years of work experience.
3.4.2 Results from Part Two of the questionnaire
The data collected from part two of the questionnaire was also analyzed
by using frequency distribution and percentage. The second part of the questionnaire
includes linguistic profile of the participants: frequency of use of English in the job,
Ref. code: 25615721042223AND

43
experience of participating in international conferences, experience of studying and
working abroad, and English proficiency test-taking experience.
3.4.3 Results from Part Three of the questionnaire
In the final part of the questionnaire, the participants were required to rate
their abilities and needs of English skills: listening, speaking, reading, and writing
skills in performing medical tasks for the AEC. The data collected from part three of
the questionnaire was analyzed by using the form of frequency and percentage. Then,
a Chi-squared test was used to find relations between the data collected from part one,
part two and part three.
Ref. code: 25615721042223AND

44
CHAPTER 4
RESULTS
In this chapter, the results reveal the abilities and needs of English
language functional skills for doctors, dentists, and nurses of eight governmental
hospitals in Prachuabkirikhan, Thailand. The data, obtained through the use of self-
administered questionnaires, was analyzed and processed by the Statistical Package
for the Social Science (SPSS) version number 21. The objective of the research was to
seek answers to the following questions:
1. What are the English skills needed for Thai skilled labor involved in
medical services?
2. What are the English skills needed for Thai skilled labor involved in
dental services?
3. What are the English skills needed for Thai skilled labor involved in
nursing services?
4. What background factors correlate with English proficiency of the
skilled labor?
The findings of the study are reported in literature, tables, and figures. The
results of the data analysis are described in five main topics as follows:
4.1 General background information of the participants
4.2 Linguistic profile of the participants
4.3 English ability of the participants
4.4 English needs of the participants
4.5 Correlation between background and English proficiency of the
participants
4.1 GENERAL BACKGROUND INFORMATION OF THE PARTICIPANTS
This part of the data was intended to describe demographic variables of
the sample and to assess for any influence on the research findings. The demographic
section consisted questions on gender, age, education, profession, and working
experience. The subject of this study comprised 251 doctors, dentists, and nurses from
Ref. code: 25615721042223AND

45
eight governmental hospitals in Prachuabkirikhan, Thailand. Of the total number of
respondents in this study, 91.20 percent were women and 8.80 percent were men. The
biggest age group was 21-30; the majority were Bachelor degree holders. The detailed
information is presented in Table 4.1.
Table 4.1
General background information of the participants (N=251)
General Background
Information
Frequency Percentage
Gender
Female
Male
229
22
91.20
8.80
Age
Below 20
21-30
31-40
41-50
51-60
1
88
67
71
24
0.40
35.10
26.70
28.30
9.60
Education
Bachelor’s Degree
Master’s Degree
175
76
69.72
30.28
Profession
Doctor
Dentist
Nurse
30
11
210
12.00
4.40
83.70
Ref. code: 25615721042223AND

46
Table 4.1 (continued)
General Background
Information
Frequency Percentage
Work Experience
Below 10 years
11-20 years
21-30 years
31-40 years
102
74
58
17
40.60
29.50
23.10
6.8
4.2 LINGUISTIC PROFILE OF THE PARTICIPANTS
This part of the data was intended to describe variations in experience
with English skills of the sample and to assess for any influence on the research
findings. The section of linguistic profiles consisted of questions on frequency of
using English in the workplace, experience with international conference, training in
medical facilities abroad, working abroad, and taking standardized tests of English
proficiency.
The majority of the participants in this study were found to be using
English in their workplace (83.30 percent). About 16 percent of them indicated that
they had participated in international conferences in the United States of America,
Germany, New Zealand, Australia, or Japan, while the rest of them had never been to
such a conference due to limited opportunity, tight schedule of work, or their field of
work that did not relate to any program of a conference. However, only a few of them
had experience with training and working abroad and surprisingly, a large number of
them had never taken any standardized test of English proficiency (e.g. TOEFL,
IELT, and TOEIC). The detailed information is presented in Table 4.2.
Ref. code: 25615721042223AND

47
Table 4.2
Linguistic profile of the participants (N=251)
Linguistic Profile Frequency Percentage
Frequency of using English in
workplaces
Frequently
Occasionally
Never
36
209
6
14.30
83.30
2.40
Experience with international
conference
Yes
No
42
209
16.70
83.30
Experience in training in
medical facility abroad
Yes
No
10
241
4.00
96.00
Experience with working abroad
Yes
No
1
250
0.40
99.60
Experience with taking
standardized tests
Yes
No
12
239
4.80
95.20
Ref. code: 25615721042223AND

48
4.3 ENGLISH ABILITIES OF THE PARTICIPANTS
In this part, the data analysis of the English abilities of the sample is
presented. The respondents were expected to rate their level of English proficiency in
listening, speaking, reading, and writing and then rate themselves in each task under
the four skills of language. The questionnaire included a Likert-scale providing five
choices: very little, little, moderate, extensive and very extensive. In the following
discussions of findings and tables, answers with ‘very little’ and ‘little’ were
categorized as ‘low proficiency’ and those reported as ‘extensive’ and ‘very
extensive’ were considered as ‘high proficiency’ while ‘moderate’ remained as
‘moderate proficiency’.
4.3.1 Listening ability of the participants
In terms of proficiency in listening skill, 55 percent of the respondents
rate their ability as ‘low proficiency’ while 39 percent considered themselves having
‘moderate proficiency’ in listening skills and only 6 percent rate their ability as ‘high
proficiency’. The detailed information is presented in Table 4.3.
Table 4.3
Listening ability of all participants (N=251)
Levels of Proficiency Frequency Percentage
Low 138 55.00
Moderate 98 39.00
High 15 6.00
Total 251 100
Of the three professions, dentists were found to be the biggest group of
‘high proficiency’ participants (27.30 percent), the next were doctors (26.70 percent),
and nurses (1.90 percent) respectively. The detailed information is presented in Table
4.4.
Ref. code: 25615721042223AND
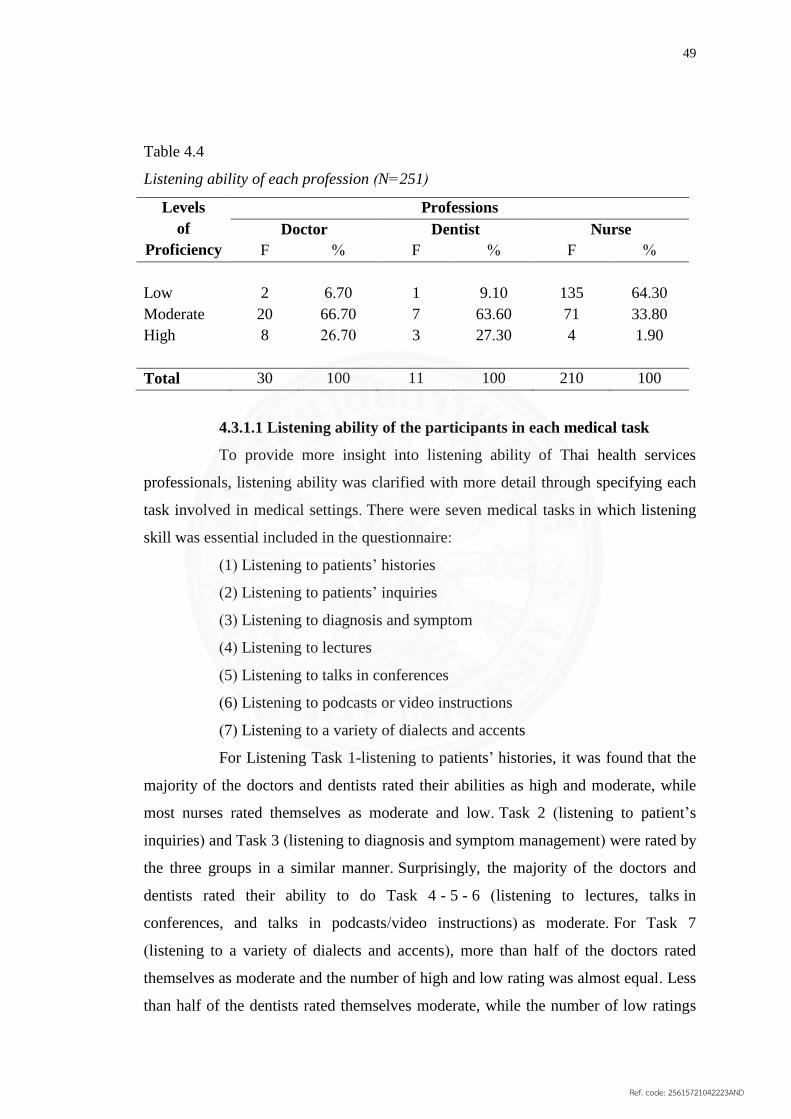
49
Table 4.4
Listening ability of each profession (N=251)
Levels
of
Proficiency
Professions
Doctor Dentist Nurse
F % F % F %
Low
Moderate
High
2
20
8
6.70
66.70
26.70
1
7
3
9.10
63.60
27.30
135
71
4
64.30
33.80
1.90
Total 30 100 11 100 210 100
4.3.1.1 Listening ability of the participants in each medical task
To provide more insight into listening ability of Thai health services
professionals, listening ability was clarified with more detail through specifying each
task involved in medical settings. There were seven medical tasks in which listening
skill was essential included in the questionnaire:
(1) Listening to patients’ histories
(2) Listening to patients’ inquiries
(3) Listening to diagnosis and symptom
(4) Listening to lectures
(5) Listening to talks in conferences
(6) Listening to podcasts or video instructions
(7) Listening to a variety of dialects and accents
For Listening Task 1-listening to patients’ histories, it was found that the
majority of the doctors and dentists rated their abilities as high and moderate, while
most nurses rated themselves as moderate and low. Task 2 (listening to patient’s
inquiries) and Task 3 (listening to diagnosis and symptom management) were rated by
the three groups in a similar manner. Surprisingly, the majority of the doctors and
dentists rated their ability to do Task 4 - 5 - 6 (listening to lectures, talks in
conferences, and talks in podcasts/video instructions) as moderate. For Task 7
(listening to a variety of dialects and accents), more than half of the doctors rated
themselves as moderate and the number of high and low rating was almost equal. Less
than half of the dentists rated themselves moderate, while the number of low ratings
Ref. code: 25615721042223AND

50
was double the high rating. Nurses consistently rated their ability as low and
moderate. The detailed information is presented in Table 4.5.
Table 4.5
Listening ability of the participants in each medical task (N=251)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Ability/ % L M H L M H L M H
1 Listening to
patients’
histories
6.70 30.00 63.30 9.10 45.50 45.50 48.60 43.30 8.10
2 Listening to
patients’
inquiries
10.00 33.30 56.70 9.10 45.50 45.50 58.60 35.70 5.70
3 Listening to
diagnosis and
symptom
6.70 30.00 63.30 9.10 36.40 54.50 43.80 46.20 10.00
4 Listening to
lectures 10.00 66.70 23.30 18.20 72.70 9.10 73.80 23.80 2.40
5 Listening to
talks in
conferences
10.00 73.30 16.70 27.30 63.30 10.00 77.60 20.50 1.90
6 Listening to
podcasts or
video
instructions
10.00 73.30 16.70 18.20 54.50 27.30 69.50 28.10 2.40
7 Listening to a
variety of
dialects and
accents
23.30 56.70 20.00 36.40 45.50 18.20 73.80 23.80 2.40
Note: When the participant response was ‘little’ and ‘very little’, the level of
proficiency was categorized as ‘low’; ‘moderate’ was at ‘moderate’; and
‘extensive’ and ‘very extensive’ was at the ‘high proficiency level’.
Ref. code: 25615721042223AND

51
4.3.2 Speaking ability of the participants
In terms of proficiency in speaking skill, 60.60 percent of the respondents
rated their ability as ‘low proficiency’ while 33.90 percent considered themselves
having ‘moderate proficiency’ in listening skills and only 5.60 percent rated their
ability as ‘high proficiency’. The detailed information is presented in table 4.6.
Table 4.6
Speaking ability of all participants (N=251)
Levels of Proficiency Frequency Percentage
Low 152 60.60
Moderate 85 33.90
High 14 5.60
Total 251 100
Of the three professions, dentists were found to be the biggest group of
‘high proficiency’participants (27.30 percent), the next were doctors (23.30 percent),
and nurses (1.90 percent) respectively. The detailed information is presented in Table
4.7.
Table 4.7
Speaking ability of each profession (N=251)
Levels
of
Proficiency
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
2
21
7
6.70
70.00
23.30
4
4
3
36.40
36.40
27.30
146
60
4
69.50
28.60
1.90
Total 30 100 11 100 210 100
4.3.2.1 Speaking ability of the participants in each medical task
To provide more insight into the speaking ability of the Thai health
service professionals, speaking ability was clarified with more detail through
Ref. code: 25615721042223AND

52
responses to specific tasks involved in medical settings. There were fourteen medical
tasks in which speaking skill was essential included in the questionnaire:
(1) Greeting and making small talk/ general conversations
(2) Asking for patients’ histories
(3) Describing symptoms and diagnosis
(4) Explaining steps of treatment and medication
(5) Explaining care plan and follow-up
(6) Giving medical advice/ instructions
(7) Giving response to patients’ inquiries
(8) Applying non-technical terms/language to develop a better
understanding of patients
(9) Providing encouragement and comfort to patients
(10) Delivering bad news to patients
(11) Communicating on telephone
(12) Giving presentation
(13) Giving lectures
(14) Giving speech or talk (e.g. at the seminar, international conference)
According to the findings, the majority of the doctors and dentists rated
their abilities as moderate and high, while most nurses rated themselves as moderate
and low in Tasks 1 - 2 - 3 (greeting and making small talk or general conversations,
asking for patients’ histories, describing symptoms and diagnosis). It was also found
that the majority of doctors, dentists, and nurses rated their ability to do Tasks 4 - 5
(explaining steps of treatment and medication, explaining care plan and follow-up) in
a similar manner. For Tasks 6 - 7 (giving medical advice or instructions, giving
response to patients’ inquiries), most doctors and nurses still rated their proficiency as
moderate and low, while most dentists rated their ability to do these tasks as
moderate. The majority of dentists, doctors, and nurses rated their abilities as high,
moderate, and low in Task 8 (applying non-technical terms or language to develop a
better understanding of patients), respectively. Nurses consistently rated their ability
as low in Tasks 9 - 10 - 11 (providing encouragement and comfort to patients,
delivering bad news to patients, and communicating on the telephone), while doctors
and dentists rated themselves as moderately proficient. Task 12 (giving a
Ref. code: 25615721042223AND
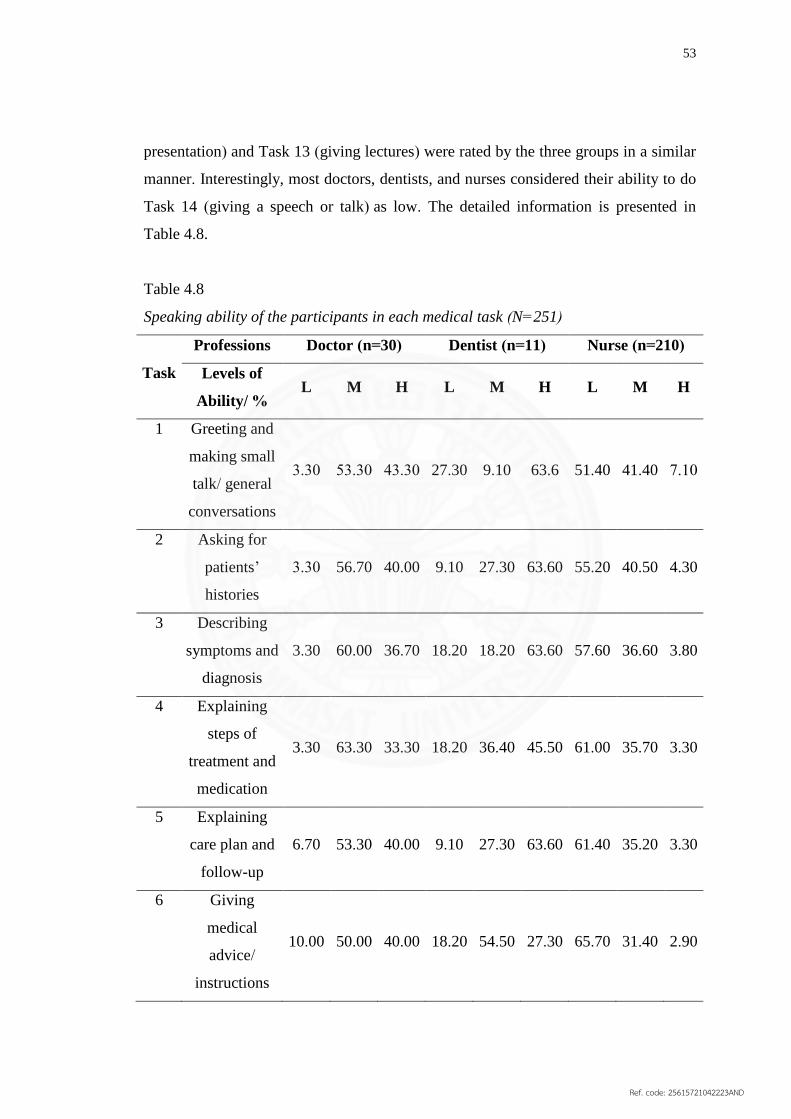
53
presentation) and Task 13 (giving lectures) were rated by the three groups in a similar
manner. Interestingly, most doctors, dentists, and nurses considered their ability to do
Task 14 (giving a speech or talk) as low. The detailed information is presented in
Table 4.8.
Table 4.8
Speaking ability of the participants in each medical task (N=251)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Ability/ % L M H L M H L M H
1 Greeting and
making small
talk/ general
conversations
3.30 53.30 43.30 27.30 9.10 63.6 51.40 41.40 7.10
2 Asking for
patients’
histories
3.30 56.70 40.00 9.10 27.30 63.60 55.20 40.50 4.30
3 Describing
symptoms and
diagnosis
3.30 60.00 36.70 18.20 18.20 63.60 57.60 36.60 3.80
4 Explaining
steps of
treatment and
medication
3.30 63.30 33.30 18.20 36.40 45.50 61.00 35.70 3.30
5 Explaining
care plan and
follow-up
6.70 53.30 40.00 9.10 27.30 63.60 61.40 35.20 3.30
6 Giving
medical
advice/
instructions
10.00 50.00 40.00 18.20 54.50 27.30 65.70 31.40 2.90
Ref. code: 25615721042223AND

54
Table 4.8 (continued)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Ability/ % L M H L M H L M H
7 Giving
response to
patients’
inquiries
6.70 66.70 26.70 27.30 36.40 36.40 35.20 31.90 2.90
8 Applying non-
technical terms/
language to
develop a better
understanding
of patients
13.30 63.30 23.30 36.40 9.10 54.50 60.50 35.20 4.30
9 Providing
encouragement
and comfort to
patients
10.00 46.70 30.00 36.40 45.50 18.20 70.50 26.20 3.30
10 Delivering bad
news to patients 26.70 46.70 26.70 63.60 18.20 18.20 77.60 21.00 1.40
11 Communicating
on telephone 26.70 50.00 23.30 36.40 45.50 18.20 76.70 21.00 2.40
12 Giving
presentation 13.30 73.30 13.30 27.30 54.50 18.20 80.00 17.60 2.40
13 Giving lectures 33.30 56.70 10.00 45.50 45.50 9.10 81.00 17.10 1.90
14 Giving speech
or talk (e.g. at
the seminar,
international
conference)
46.70 46.70 6.70 54.50 36.40 9.10 81.90 16.70 1.40
Note: When the participant response was ‘little’ and ‘very little’, the level of
proficiency was categorized as ‘low’; ‘moderate’ was at ‘moderate’; and
‘extensive’ and ‘very extensive’ was at the ‘high proficiency level’.
Ref. code: 25615721042223AND

55
4.3.3 Reading ability of the participants
In terms of proficiency in reading skill, 36.70 percent of the respondents
rate their ability as ‘low proficiency’ while 47.40 percent considered themselves
having ‘moderate proficiency’ and 15.90 percent had ‘high proficiency’ in reading
skills. The detailed information is presented in Table 4.9.
Table 4.9
Reading ability of all participants (N=251)
Levels of Proficiency Frequency Percentage
Low 92 36.70
Moderate 119 47.40
High 40 15.90
Total 251 100
Of the three professions, doctors were found to be the biggest group of
‘high proficiency’ participants (90.00 percent), the next were dentists (63.60 percent),
and nurses (2.90 percent) respectively. The detailed information is presented in Table
4.10.
Table 4.10
Reading ability of each profession (N=251)
Levels
of
Proficiency
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
1
2
27
3.30
6.70
90.00
0
4
7
00.00
36.40
63.60
91
113
6
43.30
53.80
2.90
Total 30 100 11 100 210 100
4.3.3.1 Reading ability of the participants in each medical task
To provide more insight into the reading ability of the Thai health services
professionals, reading ability was clarified with more detail given through specific
Ref. code: 25615721042223AND
56
tasks involved in medical settings. There were nine medical tasks in which reading
skill was essential included in the questionnaire:
(1) Reading patients’ medical records
(2) Reading medical diagnosis/ examination results
(3) Reading medical prescriptions
(4) Reading referral letters
(5) Reading medical textbooks
(6) Reading/ understanding medical terminology and abbreviations
(7) Reading medical journals/ research articles
(8) Reading general publications (e.g. newspaper, journals, novels)
(9) Reading manuals/ instructions about medical equipment
For Reading Task 1 (reading patients’ medical records), it was found that
the majority of the doctors and dentists rated their abilities as high, while most nurses
rated themselves as moderately proficient. Task 2 (reading medical diagnosis/
examination results) and Task 3 (reading medical prescriptions) were rated by the
three groups in a similar manner. For Task 4 and 5 (reading referral letters and
reading medical textbooks), more than 80 percent of the doctors and dentists rated
themselves as highly proficient, while nurses consistently rated their abilities as low.
Task 6 (reading/ understanding medical terminology and abbreviations) was rated by
doctors and dentists in a similar manner. Nurses, however, rated their ability to do this
task as moderate. For Task 7 (reading medical journals/ research articles), Task 8
(reading general publications), and Task 9 (reading manuals/ instructions about
medical equipment), the majority of doctors and dentists rated their ability as high,
while nurses rated themselves as low in proficiency. The detailed information is
presented in Table 4.11.
Ref. code: 25615721042223AND

57
Table 4.11
Reading ability of the participants in each medical task (N=251)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Ability/ % L M H L M H L M H
1 Reading
patients’
medical
records
3.30 6.70 90.00 0.00 18.20 81.80 45.72 47.14 7.14
2 Reading
medical
diagnosis/
examination
results
3.30 3.30 93.30 0.00 18.20 81.80 38.10 47.10 14.80
3 Reading
medical
prescriptions
3.30 6.70 90.00 0.00 27.30 72.70 29.00 44.80 26.20
4 Reading
referral letters 3.30 10.00 86.70 0.00 36.40 63.60 45.70 41.00 13.30
5 Reading
medical
textbooks
3.30 6.70 90.00 0.00 45.50 54.50 54.30 41.90 3.80
6 Reading/
understanding
medical
terminology
and
abbreviations
3.30 3.30 93.30 18.20 36.40 45.50 39.00 46.20 14.80
Ref. code: 25615721042223AND

58
Table 4.11 (continued)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Ability/ % L M H L M H L M H
7 Reading
medical
journals/
research
articles
3.30 26.70 70.00 0.00 45.50 54.50 65.20 31.90 2.90
8 Reading
general
publications
6.70 46.70 46.70 27.30 36.40 36.40 68.10 29.00 2.90
9 Reading
manuals/
instructions
about medical
equipment
3.30 16.70 80.00 0.00 45.50 54.50 48.60 46.20 5.20
Note: When the participant response was ‘little’ and ‘very little’, the level of
proficiency was categorized as ‘low’; ‘moderate’ was at ‘moderate’; and
‘extensive’ and ‘very extensive’ was at the ‘high proficiency level’.
4.3.4 Writing ability of the participants
In terms of proficiency in writing skill, 67.30 percent of the respondents
rated their ability as ‘low proficiency’ while 26.30 percent considered their
proficiency as ‘moderate’ and 6.40 percent had ‘high proficiency’ in writing skills.
The detailed information is presented in Table 4.12.
Ref. code: 25615721042223AND

59
Table 4.12
Writing ability of all participants (N=251)
Levels of Proficiency Frequency Percentage
Low 169 67.30
Moderate 66 26.30
High 16 6.40
Total 251 100
Of the three professions, doctors were found to be the biggest group of
‘high proficiency’ participants (40.00 percent), the next were dentists (18.20 percent),
and nurses (1.00 percent) respectively. The detailed information is presented in Table
4.13.
Table 4.13
Writing ability of each profession (N=251)
Levels
of
Proficiency
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
4
14
12
13.30
46.70
40.00
4
5
2
36.40
45.50
18.20
161
47
2
76.70
22.40
1.00
Total 30 100 11 100 210 100
4.3.4.1 Writing ability of the participants in each medical task
To provide more insight into the writing ability of the Thai health services
professionals, writing ability was investigated with more details from specific tasks
involved in medical setting. There were eleven medical tasks in which writing skill
was essential included in the questionnaire:
(1) Writing medical records
(2) Writing medical notes
(3) Writing medical prescriptions
(4) Writing medical terminology and abbreviations
Ref. code: 25615721042223AND

60
(5) Writing referral letter
(6) Writing medical research
(7) Writing articles for medical journals
(8) Writing letters
(9) Writing emails
(10) Writing memo
(11) Writing resumes
For Writing Task 1 (writing patients’ medical records), it was found that
the majority of the doctors and dentists rated their abilities as moderate, while most
nurses rated themselves as low in proficiency. The majority of doctors and dentists
rated their abilities to do Task 2 (writing medical notes) as high, while most nurses
rated their ability as low. Tasks 3 - 4 - 5 (writing medical prescriptions, writing
medical terminology and abbreviations, and writing referral letter), were rated by the
three groups in a similar manner. Doctors and nurses consistently rated their ability as
high and low, while the number of dentists who rated their ability as high and
moderate was equal. Interestingly, the majority of dentists rated their ability to do
Tasks 6 - 7 - 8 (writing medical research, writing articles for medical journals, and
writing letters) as low, while doctors and nurses considered themselves as moderate
and low in proficiency, respectively. Nurses consistently rated their ability to do Task
9 - 10 - 11 as low, while the majority of doctors rated their ability as high and
moderate. The majority of dentists, however, rated their ability to do these tasks as
moderate and low. The detailed information is presented in Table 4.14.
Table 4.14
Writing ability of the participants in each medical task (N=251)
Task Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Ability/ % L M H L M H L M H
1 Writing medical
records 13.30 46.70 40.00 18.20 54.50 27.30 62.40 33.30 4.30
2 Writing medical notes 10.00 23.30 66.70 36.40 18.20 45.50 76.70 21.00 2.30
Ref. code: 25615721042223AND

61
Table 4.14 (continued)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Ability/
% L M H L M H L M H
3 Writing medical
prescriptions 6.70 26.70 66.60 36.40 36.40 27.20 59.50 34.30 6.20
4 Writing medical
terminology and
abbreviations
3.30 16.70 80.00 36.40 36.40 27.20 44.30 44.70 11.00
5 Writing referral
letter 13.30 36.70 50.00 36.40 36.40 27.30 77.60 20.50 1.90
6 Writing medical
research 33.30 43.40 23.30 54.50 45.50 0.00 80.00 18.10 1.90
7 Writing articles for
medical journals 36.70 46.70 16.70 54.50 36.40 9.10 83.30 15.20 1.40
8 Writing letters 26.70 43.30 30.00 45.50 27.30 27.30 80.50 18.60 1.00
9 Writing emails 23.30 33.30 43.30 36.40 36.40 27.30 76.20 19.50 4.30
10 Writing memo 33.30 43.40 23.30 45.50 45.50 9.10 76.20 21.40 2.40
11 Writing resumes 26.70 30.00 43.30 54.50 36.40 9.10 74.30 22.40 3.30
Note: When the participant response was ‘little’ and ‘very little’, the level of
proficiency was categorized as ‘low’; ‘moderate was at ‘moderate’; and
‘extensive’ and ‘very extensive’ was at the ‘high proficiency level’.
Ref. code: 25615721042223AND

62
Figures 4.1-4.4 show level of proficiency of each skill rated by the three professionals
groups.
Figure 4.1 Listening ability of each
profession
Figure 4.2 Speaking ability of each
profession
Figure 4.3 Reading ability of each
profession
Figure 4.4 Writing ability of each
profession
According to the findings, the majority of doctors and dentists rated their
listening ability as moderate, while nurses rated themselves as low in proficiency. In
terms of speaking ability, doctors and dentists were found the most in the group of
moderate proficiency and nurses were found the most in the group of low proficiency. For
reading and writing skills, doctors and dentists considered themselves as highly
proficient, while nurses rated themselves as moderately proficient.
Ref. code: 25615721042223AND

63
4.4 ENGLISH NEEDS OF THE PARTICIPANTS
In this part data analysis of English needs of the sample are presented. The
respondents were expected to rate their level of English needs in listening, speaking,
reading, and writing skills and then rate themselves in each task under the four skills
of language. The questionnaire included a Likert-scale providing five choices: very
little, little, moderate, extensive and very extensive. In the following discussions of
findings and tables, answers ‘very little’ and ‘little’ were categorized as ‘low need’
and those given as ‘extensive’ and ‘very extensive’ were considered as ‘high need’
while ‘moderate’ remained as ‘moderate need’.
4.4.1 Needs in listening skill of the participants
In terms of needs in listening skill, 64.50 percent of the respondents rated
their level of English language needs as ‘high’ while 23.50 percent and 12 percent
considered their level of needs in listening skills as ‘moderate’ and ‘low’,
respectively. The detailed information is presented in Table 4.15.
Table 4.15
Needs in listening skill of all participants (N=251)
Levels of Needs Frequency Percentage
Low 30 12.00
Moderate 59 23.50
High 162 64.50
Total 251 100
Of the three professions, doctors were found having the highest needs in
listening skill (90 percent), the next were dentists (81.80 percent), and nurses (60.00
percent), respectively. The detailed information is presented in Table 4.16.
Ref. code: 25615721042223AND

64
Table 4.16
Needs in listening skill of each profession (N=251)
Levels
of
Needs
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
0
3
27
0.00
10.00
90.00
1
1
9
9.10
9.10
81.80
29
55
126
13.80
29.20
60.00
Total 30 100 11 100 210 100
4.4.1.1 Needs in listening skill of the participants in each medical task
To provide more insight into needs in listening skill of the Thai health
service professionals, needs in listening skill were clarified with more detail gathered
through ranking tasks involved in medical settings. There were seven medical tasks in
which listening skill was needed included in the questionnaire:
(1) Listening to patients’ histories
(2) Listening to patients’ inquiries
(3) Listening to diagnosis and symptom
(4) Listening to lectures
(5) Listening to talks in conferences
(6) Listening to podcasts or video instructions
(7) Listening to a variety of dialects and accents
The findings in these categories revealed that the majority of the
respondents had ‘high need’ of listening skill in most of listening tasks. For Listening
Tasks 1- 2 - 3 (listening to patients’ histories, listening to patient’s inquiries, and
listening to diagnosis and symptom management) the majority of the doctors, dentists,
and nurses rated their needs as high. The number of nurses who rated their needs as
low and moderate were almost equal. For Task 4 (listening to lectures), it was found
that the majority of doctors and dentists rated their need in listening skill as moderate,
while nurses rated their needs as low. For Tasks 5 - 6 - 7 (talks in conferences, and
talks in podcasts/video instructions, and listening to a variety of dialects and accents)
Ref. code: 25615721042223AND

65
the results were similar to the results from Tasks 1 - 2 - 3. The detailed information is
presented in Table 4.17.
Table 4.17
Needs in listening skill of the participants in each medical task (N=251)
Task Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/ % L M H L M H L M H
1 Listening to
patients’ histories 0.00 6.70 93.30 9.10 18.20 72.70 12.90 18.60 68.60
2 Listening to
patients’ inquiries 0.00 6.70 93.30 9.10 9.10 81.80 14.30 16.70 69.00
3 Listening to
diagnosis and
symptom
0.00 10.00 90.00 9.10 9.10 81.80 12.90 18.10 69.00
4 Listening to lectures 10.00 66.70 23.30 18.20 72.70 9.10 73.80 23.80 2.40
5 Listening to talks in
conferences 3.30 6.70 90.00 9.10 9.10 81.80 23.60 21.00 55.20
6 Listening to
podcasts or video
instructions
00.00 16.70 83.30 9.10 9.10 81.80 21.40 21.40 57.20
7 Listening to a
variety of dialects
and accents
3.30 20.00 76.70 9.10 9.10 81.80 20.50 22.40 57.10
Note: When the participant response was ‘little’ and ‘very little’, the level of need was
categorized as ‘low’; ‘moderate was at ‘moderate’; and ‘extensive’ and ‘very
extensive’ was at the ‘high’.
4.4.2 Needs in speaking skill of the participants
In terms of needs in speaking skill, 61.40 percent of the respondents rated
their level of needs as ‘high’ while 22.70 percent and 15.90 percent considered their
level of needs in speaking skills as ‘moderate’ and ‘low’, respectively. The detailed
information is presented in Table 4.18.
Ref. code: 25615721042223AND
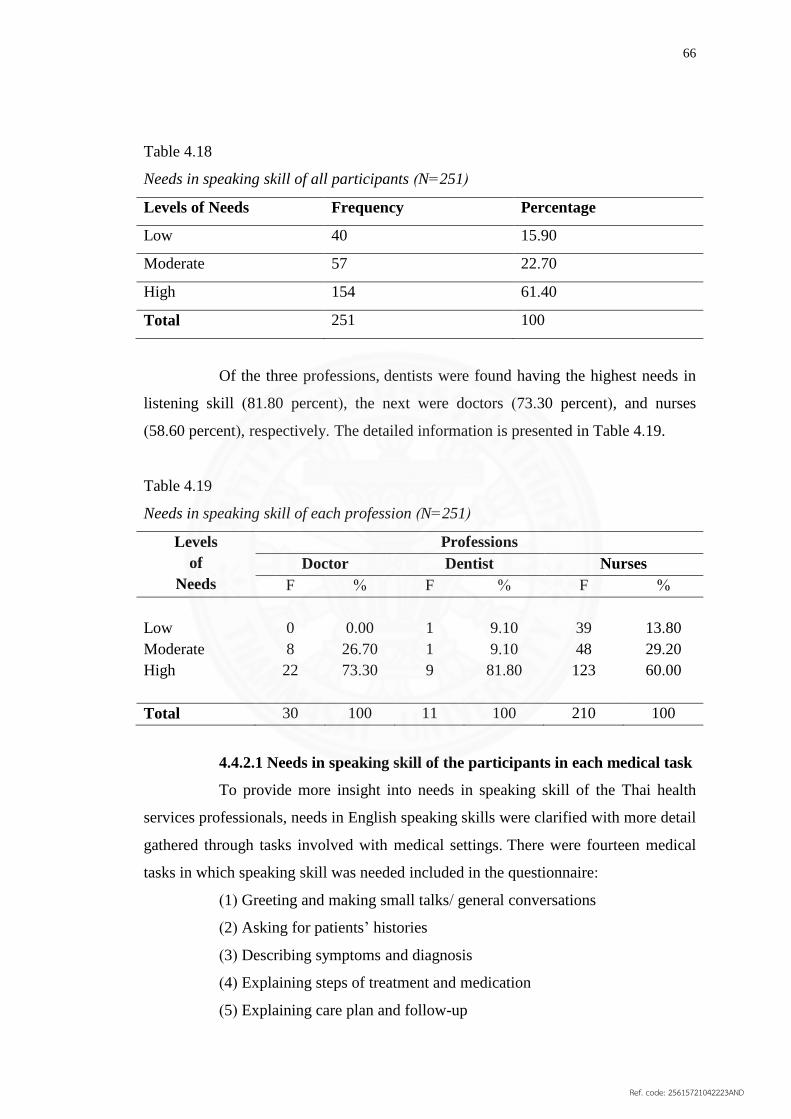
66
Table 4.18
Needs in speaking skill of all participants (N=251)
Levels of Needs Frequency Percentage
Low 40 15.90
Moderate 57 22.70
High 154 61.40
Total 251 100
Of the three professions, dentists were found having the highest needs in
listening skill (81.80 percent), the next were doctors (73.30 percent), and nurses
(58.60 percent), respectively. The detailed information is presented in Table 4.19.
Table 4.19
Needs in speaking skill of each profession (N=251)
Levels
of
Needs
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
0
8
22
0.00
26.70
73.30
1
1
9
9.10
9.10
81.80
39
48
123
13.80
29.20
60.00
Total 30 100 11 100 210 100
4.4.2.1 Needs in speaking skill of the participants in each medical task
To provide more insight into needs in speaking skill of the Thai health
services professionals, needs in English speaking skills were clarified with more detail
gathered through tasks involved with medical settings. There were fourteen medical
tasks in which speaking skill was needed included in the questionnaire:
(1) Greeting and making small talks/ general conversations
(2) Asking for patients’ histories
(3) Describing symptoms and diagnosis
(4) Explaining steps of treatment and medication
(5) Explaining care plan and follow-up
Ref. code: 25615721042223AND

67
(6) Giving medical advice/ instructions
(7) Giving response to patients’ inquiries
(8) Applying non-technical terms/ language to develop a better
understanding of patients
(9) Providing encouragement and comfort to patients
(10) Delivering bad news to patients
(11) Communicating on telephone
(12) Giving presentation
(13) Giving lectures
(14) Giving speech or talk (e.g. at the seminar, international conference)
The findings in this category revealed that more than 80 percent of doctors
and dentists and more than 60 percent of nurses agreed that speaking skill was
essential for Tasks 1 – 8 (greeting and making small talks/ general conversations,
asking for patients’ histories, describing symptoms and diagnosis, explaining steps of
treatment and medication, explaining care plan and follow-up, giving medical advice/
instructions, giving response to patients’ inquiries, and applying non-technical terms/
language to develop a better understanding of patients) and thus rated their need in
speaking skill for these tasks as high. Similar results were found in Tasks 9 - 14
(providing encouragement and comfort to patients, delivering bad news to patients,
communicating on telephone, giving presentation, giving lectures, and giving speech
or talk); however, the number of high ratings among the groups of doctors and nurses
were distinctively lower than the eight previous tasks. The detailed information is
presented in Table 4.20.
Table 4.20
Needs in speaking skill of the participants in each medical task (N=251)
Task Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/ % L M H L M H L M H
1 Greeting and making
small talks/ general
conversations
3.30 6.70 90.00 9.10 9.10 81.80 17.10 19.50 63.30
Ref. code: 25615721042223AND

68
Table 4.20 (continued)
Task Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/ % L M H L M H L M H
2 Asking for patients’
histories 0.00 10.00 90.00 9.10 9.10 81.80 15.70 18.60 65.70
3 Describing symptoms
and diagnosis 0.00 10.00 90.00 9.10 9.10 81.80 17.60 17.10 65.20
4 Explaining steps of
treatment and
medication
0.00 10.00 90.00 9.10 9.10 81.80 15.70 19.50 64.80
5 Explaining care plan
and follow-up 0.00 10.00 90.00 9.10 9.10 81.80 15.70 17.60 66.70
6 Giving medical
advice/ instructions 0.00 6.70 93.30 9.10 9.10 81.80 16.70 18.10 65.20
7 Giving response to
patients’ inquiries 0.00 6.70 93.30 9.10 9.10 81.80 16.70 18.10 65.20
8 Applying non-
technical terms/
language to develop a
better understanding
of patients
3.30 6.70 90.00 9.10 9.10 81.80 15.70 22.90 64.10
9 Providing
encouragement and
comfort to patients
3.30 20.00 76.70 9.10 9.10 81.80 20.00 19.00 61.00
10 Delivering bad news
to patients 3.30 20.00 76.70 9.10 9.10 81.80 21.40 19.00 59.50
11 Communicating on
telephone 10.00 23.30 66.70 18.20 0.00 81.80 21.40 21.40 57.10
12 Giving presentation 13.30 23.30 63.30 18.20 0.00 81.80 25.20 26.20 48.60
Ref. code: 25615721042223AND

69
Table 4.20 (continued)
Note: When the participant response was ‘little’ and ‘very little’, the level of need was
categorized as ‘low’; ‘moderate was at ‘moderate’; and ‘extensive’ and ‘very
extensive’ was at ‘high’.
4.4.3 Needs in reading skill of the participants
In terms of needs in English language reading skill, 65.30 percent of the
respondents rated their level of needs as ‘high’ while 23.10 percent and 11.60 percent
considered their level of needs in reading skills as ‘moderate’ and ‘low’, respectively.
The detailed information is presented in Table 4.21.
Table 4.21
Needs in reading skill of all participants (N=251)
Levels of Needs Frequency Percentage
Low 29 11.60
Moderate 58 23.10
High 164 65.30
Total 251 100
Of the three professions, doctors were found having highest needs in
reading skill (96.70 percent), the next were dentists (81.80 percent), and nurses (60.00
percent), respectively. The detailed information is presented in Table 4.22.
Task Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/ % L M H L M H L M H
13 Giving lectures 13.30 30.00 56.70 27.30 9.10 63.60 25.20 25.20 49.60
14 Giving speech or talk
(e.g. at the seminar,
international
conference)
20.00 26.70 53.30 27.30 9.10 63.60 28.60 26.70 44.80
Ref. code: 25615721042223AND

70
Table 4.22
Needs in reading skill of each profession (N=251)
Levels
of
Needs
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
0
1
29
0.00
3.33
96.70
0
2
9
0.00
18.20
81.80
29
55
126
13.80
26.20
60.00
Total 30 100 11 100 210 100
4.4.3.1 Needs in reading skill of the participants in each medical task
To provide more insight into the needs in reading skill of the Thai health
services professionals, needs in reading skill were collected in more detail through
investigating tasks involved in medical settings. There were nine medical tasks in
which reading skill was needed included in the questionnaire:
(1) Reading patients’ medical records
(2) Reading medical diagnosis/ examination results
(3) Reading medical prescriptions
(4) Reading referral letter
(5) Reading medical textbooks
(6) Reading/ understanding medical terminology and abbreviations
(7) Reading medical journals/ research articles
(8) Reading general publications (e.g. newspaper, journals, novels)
(9) Reading manuals/ instructions about medical equipment
The findings revealed that the receptive skill was highly needed in each
medical task. The majority of dentists rated their need in reading skill as high for
every task and, interestingly, the number of high ratings was also equal in every task
except Task 8 (reading general publications), which was slightly lower than the eight
other tasks. Almost all doctors rated their need in reading skill as high for Tasks 1 - 4
(reading patients’ medical records, reading medical diagnosis/ examination results,
reading medical prescriptions, and reading referral letter) and the number of high
ratings in each task was also equal. Similar to the dentists’rankings, needs in reading
Ref. code: 25615721042223AND
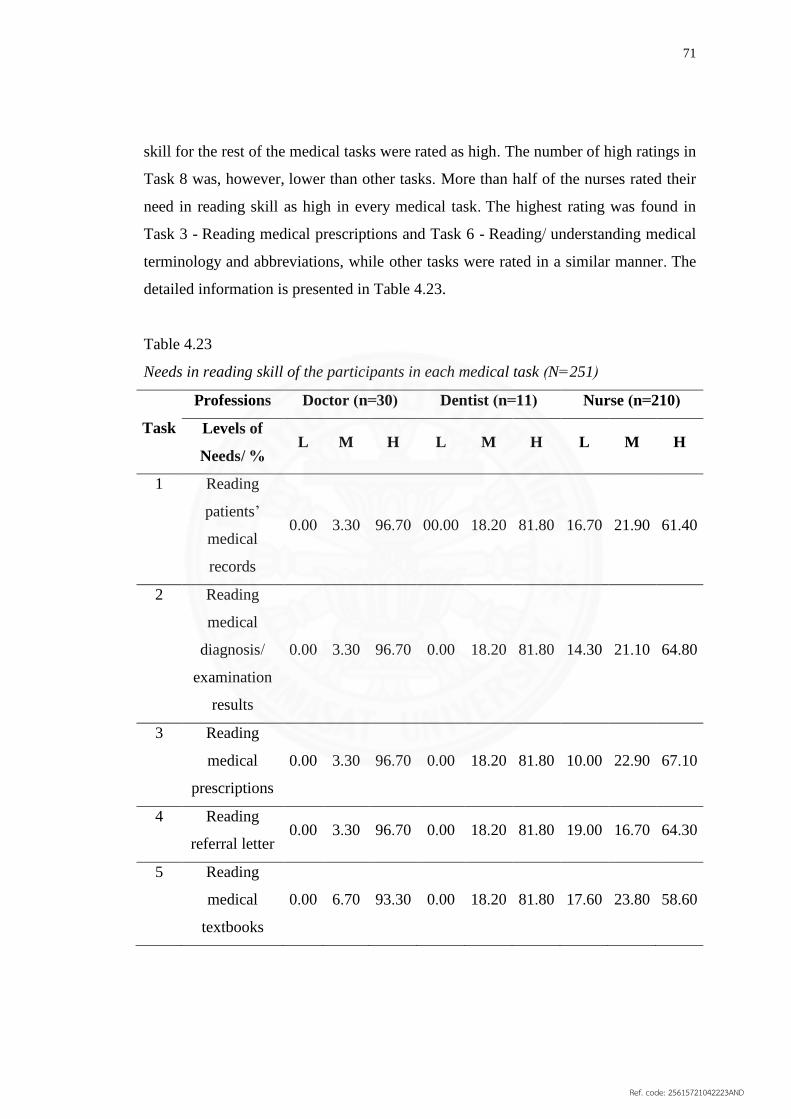
71
skill for the rest of the medical tasks were rated as high. The number of high ratings in
Task 8 was, however, lower than other tasks. More than half of the nurses rated their
need in reading skill as high in every medical task. The highest rating was found in
Task 3 - Reading medical prescriptions and Task 6 - Reading/ understanding medical
terminology and abbreviations, while other tasks were rated in a similar manner. The
detailed information is presented in Table 4.23.
Table 4.23
Needs in reading skill of the participants in each medical task (N=251)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Needs/ % L M H L M H L M H
1 Reading
patients’
medical
records
0.00 3.30 96.70 00.00 18.20 81.80 16.70 21.90 61.40
2 Reading
medical
diagnosis/
examination
results
0.00 3.30 96.70 0.00 18.20 81.80 14.30 21.10 64.80
3 Reading
medical
prescriptions
0.00 3.30 96.70 0.00 18.20 81.80 10.00 22.90 67.10
4 Reading
referral letter 0.00 3.30 96.70 0.00 18.20 81.80 19.00 16.70 64.30
5 Reading
medical
textbooks
0.00 6.70 93.30 0.00 18.20 81.80 17.60 23.80 58.60
Ref. code: 25615721042223AND

72
Table 4.23 (continued)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of
Needs/ % L M H L M H L M H
6 Reading/
understanding
medical
terminology
and
abbreviations
0.00 3.30 96.70 0.00 18.20 81.80 12.40 21.00 66.60
7 Reading
medical
journals/
research
articles
0.00 6.70 93.30 0.00 18.20 81.80 20.00 24.30 55.70
8 Reading
general
publications
0.00 26.70 73.30 0.00 27.30 72.70 21.40 24.80 53.80
9 Reading
manuals/
instructions
about medical
equipment
0.00 10.00 90.00 0.00 18.20 81.80 11.90 25.70 62.40
Note: When the participant response was ‘little’ and ‘very little’, the level of need was
categorized as ‘low’; ‘moderate was at ‘moderate’; and ‘extensive’ and ‘very
extensive’ was at ‘high’.
4.4.4 Needs in writing skill of the participants
In terms of needs in English writing skill, 53.00 percent of the respondents rated their
level of needs as ‘high’ while 25.50 percent and 21.50 percent considered their level
of needs in writing skills as ‘moderate’ and ‘low’, respectively. The detailed
information is presented in Table 4.24.
Ref. code: 25615721042223AND

73
Table 4.24
Needs in writing skill of all participants (N=251)
Levels of Needs Frequency Percentage
Low 54 21.50
Moderate 64 25.50
High 133 53.00
Total 251 100
Of the three professions, dentists were found having highest needs in
writing skill (81.80 percent), the next were doctors (73.30 percent), and nurses (48.60
percent), respectively. The detailed information is presented in Table 4.25.
Table 4.25
Needs in writing skill of each profession (N=251)
Levels
of
Needs
Professions
Doctor Dentist Nurses
F % F % F %
Low
Moderate
High
0
8
22
0.00
26.70
73.30
1
1
9
9.10
9.10
81.80
53
55
102
25.20
26.20
48.60
Total 30 100 11 100 210 100
4.4.4.1 Needs in writing skill of the participants in each medical task
To provide more insight into needs in writing skill of Thai health service
professionals, needs in writing skill were clarified with more detail gathered through
investigating tasks involved in medical settings. There were nine medical tasks in
which writing skill was needed included in the questionnaire:
(1) Writing medical records
(2) Writing medical notes
(3) Writing medical prescriptions
(4) Writing medical terminology and abbreviations
(5) Writing referral letter
Ref. code: 25615721042223AND

74
(6) Writing medical research
(7) Writing articles for medical journals
(8) Writing letters
(9) Writing emails
(10) Writing memo
(11) Writing resumes
The findings revealed that the majority of doctors and dentists rated their
need in writing skill as high for Tasks 1 - 2 - 3 (writing medical records, writing
medical notes, and writing medical prescriptions), especially for Task 3 where a
hundred percent of doctors agreed the writing skill was highly important. Likewise,
about half of the nurses rated their need in writing as high for the three tasks. For
Tasks 4 and 5 (writing medical terminology and abbreviations and writing referral
letter) the three groups rated their need in a similar manner. Interestingly, fewer than
half of the nurses rated their need as high for Tasks 6 - 7 - 8 (writing medical
research, writing articles for medical journals, and writing letters). The majority of the
participants consistently rated their need in writing skill as high for the last three tasks
(writing emails, writing memo, and writing resumes); however, the number of high
ratings in Task 10 was lower than the other tasks and only half of the nurses
considered writing skill was significant regarding Tasks 9 and 11. The detailed
information is presented in Table 4.26.
Table 4.26
Needs in writing skill of the participants in each medical task (N=251)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/ % L M H L M H L M H
1 Writing medical records 3.30 0.00 96.70 9.10 9.10 81.80 20.00 23.80 56.20
2 Writing medical notes 3.30 3.30 93.30 9.10 9.10 81.80 28.10 22.40 49.50
Ref. code: 25615721042223AND

75
Table 4.26 (continued)
Task
Professions Doctor (n=30) Dentist (n=11) Nurse (n=210)
Levels of Needs/
% L M H L M H L M H
3 Writing medical
prescriptions
0.00 0.00 100.00 9.10 9.10 81.80 22.40 24.30 53.30
4 Writing medical
terminology and
abbreviations
0.00 3.30 96.70 9.10 18.20 72.70 13.30 23.80 62.90
5 Writing referral
letter
0.00 10.00 90.00 9.10 9.10 81.80 29.00 19.00 51.90
6 Writing medical
research
10.00 20.00 70.00 9.10 18.20 72.70 31.00 22.40 46.70
7 Writing articles for
medical journals
10.00 23.30 66.70 9.10 18.20 72.70 31.00 22.40 46.70
8 Writing letters 10.00 16.70 73.30 9.10 9.10 81.80 29.50 21.90 48.60
9 Writing emails 6.70 16.70 76.70 9.10 9.10 81.80 27.10 22.40 50.50
10 Writing memo 10.00 40.00 50.00 9.10 27.30 63.60 30.50 22.40 47.10
11 Writing resumes 13.30 20.00 66.70 18.20 9.10 72.70 29.50 20.00 50.50
Note: When the participant response was ‘little’ and ‘very little’, the level of need was
categorized as ‘low’; ‘moderate was at ‘moderate’; and ‘extensive’ and ‘very
extensive’ was at ‘high’.
Ref. code: 25615721042223AND

76
Figures 4.5-4.8 show level of need of each skill rated by the three professional groups.
Figure 4.5 Needs in listening skill of
each profession
Figure 4.6 Needs in speaking skill of
each profession
Figure 4.7 Needs in reading skill of
each profession
Figure 4.8 Needs in writing skill of
each profession
Overall, the majority of doctors, dentists, and nurses rated their needs in
English listening, speaking, reading, and writing skills as high. Doctors rated their need
in reading skill the highest, while dentists’ and nurses’ highest needs were found in the
four English skills equally.
Ref. code: 25615721042223AND

77
To better illustrate the findings, the following is a comparison between
self-rated proficiency and self-rated needs in the listening, speaking, reading, and
writing skills of the participants.
Ref. code: 25615721042223AND

78
Level of Proficiency
Listening skill
Speaking skill
Reading skill
Writing skill
Level of Needs
Listening skill
Speaking skill
Reading skill
Writing skill
Ref. code: 25615721042223AND

79
The summary of the ratings from each profession is as follows:
The majority of doctors rated their English ability as high and moderate. They
had highest ability in reading and writing and highest need in reading skill.
The majority of dentists rated their English ability as high and moderate. They
had highest ability in reading and writing and highest need in all English skills.
The majority of nurses rated their English ability as moderate and low. They
had highest ability in reading and writing and highest need in listening, speaking, and
reading skills.
To study whether participants’ background had any influence on their
proficiency, all variables involved in the general background information section were
statistically analyzed. The detailed information is presented in 4.5
4.5 CORRELATION BETWEEN BACKGROUND AND ENGLISH
PROFICIENCY OF THE PARTICIPANTS
This part of the data was intended to describe correlations between
variables in background and the English proficiency of the participants. All the
variables involved in the general background information section were analyzed by
using Chi-squared ( ). The following were variables that were found correlated with
the proficiency of the participants:
Gender
Gender correlated with the proficiency of the participants; the variable
was found statistically significant at the 0.05 level with = 37.016
Profession
Profession correlated with the proficiency of the participants; the
variable was found statistically significant at the 0.05 level with =
91.387
Education
Education correlated with the proficiency of the participants; the
variable was found statistically significant at the 0.05 level with =
94.057
Ref. code: 25615721042223AND

80
Work experience
Work experience correlated with the proficiency of the participants;
the variable was found statistically significant at the 0.05 level with
= 12.921
Frequency of using English in the workplace
Frequency of using English in the workplace correlated with the
proficiency of the participants; the variable was found statistically
significant at the 0.05 level with = 11.090
Experience with training in medical facility abroad
Experience with training in a medical facility abroad correlated with
the proficiency of the participants; the variable was found statistically
significant at the 0.05 level with = 9.624
Experience with working abroad
Experience with working abroad correlated with the proficiency of the
participants; the variable was found statistically significant at the 0.05
level with = 10.451
The detailed information is presented in Table 4.27.
Table 4.27
Correlation between background and English proficiency of the participants (N=251)
Background
English Proficiency
2
df
P -
value
Low Moderate High
F % F % F %
Gender 37.016 2 0.00*
Male 2 1.60 11 10.70 9 40.90
Female 124 98.40 92 89.30 13 59.10
Total 126 100 103 100 22 100
Ref. code: 25615721042223AND

81
Table 4.27 (continued)
Background
English Proficiency
2
df
P -
value
Low Moderate High
F % F % F %
Age 8.292 8 0.406
Below 20 yrs 1 0.80 0 0.00 0 0.00
21 – 30 yrs 36 28.60 42 40.80 10 45.50
31 – 40 yrs 35 27.80 25 24.30 7 31.80
41 – 50 yrs 38 30.20 29 28.20 4 18.20
Above 60 yrs 16 12.70 7 6.80 1 4.50
Total 126 100 103 100 22 100
Profession 91.387 4 0.00*
Doctor 1 0.80 15 14.60 14 63.60
Dentist 1 0.80 6 5.80 4 18.20
Nurse 124 98.40 82 79.60 4 18.20
Total 126 100 103 100 22 100
Education 94.057 2 0.00*
Bachelor’s
Degree
124 98.40 78 31.10 3 1.20
Master’s
Degree and
above
2 1.60 25 10.00 19 7.60
Total 126 100 103 100 22 100
Ref. code: 25615721042223AND

82
Table 4.27 (continued)
Background
English Proficiency
2
df
P -
value
Low Moderate High
F % F % F %
Work
experience
12.921 6 0.04*
Below 10 yrs 41 32.50 47 45.60 14 63.60
11-20 yrs 38 30.20 32 31.10 4 18.20
21-30 yrs 38 30.20 18 17.50 2 9.10
Above 40 yrs 9 7.10 6 5.80 2 9.10
Total 126 100 103 100 22 100
Frequency of
using English
in the
workplace
11.090 2 0.04*
Occasionally 116 92.10 84 81.60 15 68.20
Frequently 10 7.90 19 18.40 7 31.80
Total 126 100 103 100 22 100
Experience
with
international
conference
9.624 2 0.08
Yes 6 4.80 22 21.40 14 63.60
No 120 95.20 81 78.60 8 36.40
Total 126 100 103 100 22 100
Ref. code: 25615721042223AND

83
Table 4.27 (continued)
Background
English Proficiency
2
df
P -
value
Low Moderate High
F % F % F %
Experience
with training
in medical
facility
abroad
9.624 2 0.008*
Yes 1 0.80 6 5.80 3 13.60
No 125 99.20 97 94.20 19 86.40
Total 126 100 103 100 22 100
Experience
with working
abroad
10.451 1 0.005*
Yes 0 0.00 0 0.00 1 0.04
No 126 100 103 100 21 95.50
Total 126 100 103 100 22 100
Experience
with taking
standardized
tests
5.738 2 0.057
Yes 2 1.60 8 7.80 2 9.10
No 124 98.40 95 92.20 20 90.90
Total 126 100 103 100 22 100
According to the findings, gender, profession, education, work
experience, frequency of using English in the workplace, experience with training in
medical facility abroad, and experience with working abroad correlated with the
proficiency of the participants, while age, experience with international conferences,
and experience with taking standardized tests had no correlation with the proficiency
of the participants.
Ref. code: 25615721042223AND

84
To summarize the study procedure here, a needs analysis was conducted
with 251 health services professionals of eight governmental hospitals in
Prachuabkirikhan, Thailand. The instrument used in this study was a self-administered
questionnaire which included authentic tasks from medical settings. The participants
were required to rate their current proficiency and needs of four English skills in
performing each medical task. The findings revealed that the proficiency of the
participants ranged from low to moderate and that the four English skills were highly
demanded in every medical task. Among the four skills, needs in reading skill was
ranked the highest, followed by needs in listening skill, speaking skill, and writing
skill, respectively. To study whether participants’ background had any influence on
their proficiency, all variables involved in the general background information section
were analyzed by using a Chi-squared ( ) test. The variables that were found
correlated with the proficiency of the participants were gender, profession, education,
work experience, frequency of using English in the workplace, experience with
training in a medical facility abroad, and experience with working abroad; on the
contrary, age, experience with international conferences, and experience with taking
standardized tests (e.g. TOEFL, IELT, and TOEIC) were variables that had no
correlation with the proficiency of the participants.
Ref. code: 25615721042223AND

85
CHAPTER 5
CONCLUSION AND RECOMMENDATIONS
This chapter presents a summary of the study, summary of the findings,
discussion of the findings, conclusion and recommendations for further research.
5.1 SUMMARY OF THE STUDY
The establishment of the ASEAN Economic Community, followed by the
free flow of goods, services, and labor requires the awareness of the direction of
changes in employment patterns and standards, including preparation for the
challenges from the increasing internationalization of the labor market from the
stakeholders involved in the ASEAN integration process. However, when compared
to other member countries, English abilities of Thai people, on the whole, are rather
minimal. Thus, the readiness for the AEC of Thai skilled labor in terms of English
language proficiency is still questionable.
Based on the problem statement, in this study a needs analysis of English
functional skills and an investigation into English proficiency of Thai skilled labor
involved in eight ASEAN occupations were conducted. Considering the fact that the
importance of the healthcare industry in Thailand has risen and the country is striving
to be the World Class Healthcare Destination and Academic Medical Hub of Asia, the
focus group of the study was the healthcare workers.
The objective of the study, research questions, participants, research
instrument, and data analysis are summarized as follows:
5.1.1 Objective of the study
The objective of this study is to investigate English functional skills
needed for three ASEAN health-related occupations: medical services, dental services,
and nursing services.
Ref. code: 25615721042223AND

86
5.1.2 Research questions
1. What are the English skills needed for Thai skilled labor involved in
medical services?
2. What are the English skills needed for Thai skilled labor involved in
dental services?
3. What are the English skills needed for Thai skilled labor involved in
nursing services?
4. What background factors correlate with English proficiency of the
skilled labor?
5.1.3 Participants
Selected by stratified random sampling, the participants of this study are
30 doctors, 11 dentists, and 210 nurses (251 health services professionals in total)
from eight governmental hospitals in Prachuabkirikhan, Thailand: Hua Hin Hospital,
Pranburi Hospital, Samroiyod Hospital, Kuiburi Hospital, Prachuabkirikhan Hospital,
Thapsakae Hospital, Bangsaphan Hospital, and Bangsaphan Noi Hospital.
5.1.4 Research instrument
The instrument used in this study was a set of self-administered
questionnaire, comprising three parts of questions: (1) general background
information, (2) linguistic profile, and (3) English abilities and needs of English skills
for the AEC. The participants were required to provide their background information,
including gender, age, education, profession, and work experience in the first part and
frequency of using English in the workplace, experience with international
conferences, experience with training in medical facilities abroad, experience with
working abroad, and experience with taking standardized tests (e.g. TOEFL, IELT,
and TOEIC) in the second part. In the third part, the participants had to rate their
proficiency and needs in listening, speaking, reading, and writing skills through a 5-
point Likert scale.
Ref. code: 25615721042223AND

87
5.1.5 Data analysis
After 251 questionnaires were completed and returned, the data obtained
was analyzed by the Statistical Package for the Social Sciences (SPSS) version
number 21, using the form of frequency and percentage to determine the results of
self-rated proficiency and self-rated needs in four English skills of the participants.
Moreover, to study whether participants’ background had any influence on their
proficiency, all variables involved in the general background information section were
analyzed by using a Chi-squared ( ) test to find correlations between the data.
5.2 SUMMARY OF THE FINDINGS
The detailed findings in Chapter 4 can be summarized as follows:
5.2.1 General background information of the participants
91.20 percent of the participants were female and 8.80 percent were male.
The largest age group was 31-50 years old (55.00 percent) and the next was between
21-30 years old (35.10 percent). 83.70 percent of the participants were nurses,
followed by doctors (12.00 percent) and dentists (4.40 percent), respectively. Most of
the three groups had a Bachelor’s Degree (81.70 percent) and had less than 10 years
of work experience (40.60 percent).
5.2.2 Linguistic profile of the participants
The majority of the participants occasionally use English language in their
workplaces (83.30 percent). 14.30 percent had experience with international
conferences and 4.80 percent had taken standardized tests (e.g. TOEFL, IELT, and
TOEIC). 4.00 percent had experience with training in a medical facility abroad, but
only 0.40 percent had ever worked abroad.
5.2.3 English abilities of the participants
Four English skills were presented in this study: listening, speaking,
reading, and writing. The participants were required to rate their proficiency in
various medical tasks involving the four English skills. According to the analysis of
251 questionnaires, it was found that the majority of the health services professionals
Ref. code: 25615721042223AND

88
had moderate and low ability. Doctors and dentists rated their ability as high and
moderate, while the majority of nurses rated themselves as moderate and low in
proficieny. When comparing between the four skills, it was found that reading skill
was ranked as the highest proficiency of the participants, the next was listening skill,
speaking skill, and writing skill, respectively.
5.2.4 English needs of the participants
English needs were divided into four types: needs in listening skill, needs
in speaking skill, needs in reading skill, and needs in writing skill. Overall, it was
found that all four skills were highly demanded by the majority of health services
professionals. Doctors, dentists, and nurses rated their need in listening, speaking,
reading, and writing skills as high in every medical task. When comparing between
needs in each skill, it was found that needs in reading skill was ranked the highest, the
next was needs in listening skill, speaking skill, and writing skill, respectively.
5.2.5 Correlation between background and English proficiency of the
participants
To study whether participants’ background had any influence on their
proficiency, all variables involved in the general background information section were
analyzed by using a Chi-squared ( ) test. The variables that were found correlated
with the proficiency of the participants were gender, profession, education, work
experience, frequency of using English in the workplace, experience with training in
medical facilities abroad, and experience with working abroad (the variables were
found statistically significant at the 0.05 level with = 37.016, 91.387, 94.057,
12.921, 11.090, 9.624, and 10.451, respectively). Age, experience with international
conferences, and experience with taking standardized tests (e.g. TOEFL, IELT, and
TOEIC), however, were variables that had no correlation with the proficiency of the
participants.
Ref. code: 25615721042223AND

89
5.3 DISCUSSION OF THE FINDINGS
The objective of this study was to investigate English functional skills
needed for three ASEAN occupations—medical, dental, and nursing services—thus,
the study seeks answers to the following questions:
What are the English functional skills needed for Thai skilled labor
involved in medical services?
The results revealed that the majority of the doctors rated their needs in
English skills as high in every medical task. Out of four categories of needs, reading
skill was ranked the highest. It was needed the most when they had to handle patients’
medical records, examination results, prescriptions, referral letters, and medical
terminology and abbreviations. The second was listening skill, which was needed
when they had to listen to patients’ history and inquiries. Need in speaking skill was
ranked third and was highlighted in giving medical advice and responding to patients’
inquiries, while writing skill was in the last place and was needed especially for
medical prescriptions, records, terminology and abbreviations writing.
What are the English functional skills needed for Thai skilled labor
involved in dental services?
According to the findings, needs in English skills of the dentists were
rated as high in every medical task. Similar to the group of doctors, the results showed
that needs in receptive skills of the dentists were higher than needs in productive
skills. The top rank was reading skill, which the majority agreed was essential to
every medical task except for general publications reading (e.g. English newspapers,
journals, novels) for which the rating was slightly lower than the others. The next was
needs in listening skill. The dentists specifically needed the skill for listening to
patients’ inquiries, diagnosis and symptoms, and in other situations such as listening
to talks in conferences, video instructions, and a variety of dialects and accents. Need
in speaking skill was ranked third, followed by need in writing skill. The former was
rated as high in almost every medical task, while the latter skill was needed for
medical records, medical notes, prescriptions, and referral letter writing, and a few
work-related tasks such as letters and emails writing.
Ref. code: 25615721042223AND

90
What are the English functional skills needed for Thai skilled labor
involved in nursing services?
Overall, the majority of nurses rated their needs in listening, speaking,
reading, and writing skills as high in every medical task. The findings revealed that
reading skill was needed the most, especially for medical prescriptions, terminology
and abbreviation reading. The second was listening skill which was intensively used
for listening to patients’ histories, inquiries, and diagnosis. Need in speaking and
writing skills were ranked the third and the fourth needs, respectively. Nurses needed
speaking skill mostly when they had to ask for patients’ histories and explain care
plan and follow-up to patients. For writing skill, although the demand was lower than
other categories, the majority agreed it was necessary for medical records,
terminology and abbreviations writing.
What background factors correlate with English proficiency of the
skilled labor?
Concerning the influence of personal background on English proficiency,
the results indicated that seven out of ten background factors correlated with level of
proficiency of the participants. These were gender, profession, education, work
experience, frequency of using English in the workplace, experience with training in
medical facility abroad, and experience with working abroad. The variables were
found statistically significant at the 0.05 level with = 37.016, 91.387, 94.057,
12.921, 11.090, 9.624, and 10.451, respectively. However, factors such as age,
experience with international conferences, and experience with taking standardized
tests had no correlation with the proficiency of the participants.
According to the findings, it can be concluded that health services
professionals—doctors, dentists, and nurses—from eight governmental hospitals in
Prachuabkirikhan agreed that receptive skills were first and foremost, while needs in
productive skills such as speaking and writing skills were lesser in their jobs.
Furthermore, the four skills were rather required in tasks that were work-related than
tasks that were not directly involved in medical settings such as listening to lectures,
giving speech, reading general publications, and writing memos.
Ref. code: 25615721042223AND

91
This confirmed Shi, Corcos, and Storey’s (2001) study on needs analysis
of medical students in the University of Hong Kong and the study on needs analysis
and situational analysis for designing an ESP curriculum for Thai nurses of Gass
(2012) which stated that among the topics related to medical and nursing fields and
that the participants needed and wanted the courses to cover were mostly medical
tasks, for example, reporting and discussing the case, educating the patients, giving
advices, giving instructions, checking understanding, explaining drugs interactions,
and administering medication, whereas only a few cultural topics were required.
However, the needs analysis results which, surprisingly, indicated that
receptive skills were rather prerequisite to medical workers were in contrast with the
findings from Shi, Corcos, and Storey’s (2001) and Gass’s (2012) which regarded
speaking and communicative skills (as well as listening) as predominant needs of
medical services personnel.
Gass (2012), nevertheless, explained that needs in communicative skills of
nurses and caregivers can vary, depending on various conditions, for example, the
amount of English exposure, characteristics of jobs, and their level of proficiency and
confidence in using English. Thus, for those whose jobs do not allow them much
opportunity to interact with patients (e.g. inpatient department) and those who are not
confident with using English, their needs in communicative skills may be moderate to
low. On the contrary, for those who position themselves or are positioned in the
context where English is very much used such as an outpatient department, which is a
sector that all patients are required to go through, communicative skills are demanded
for developing a higher quality of their services.
In addition, in a Thailand context, especially where the participants of the
study were governmental employees who resided and worked in Prachuabkirikhan,
the chances to have conversations with foreign patients were quite limited. Although
it is known that many foreigners flood into this province for long-term stays due to
the natural beauty of many tourist attractions, the daily life of the participants was
rather confined to their workplace, and the opportunity to be exposed to English or
improve their language skill was limited. The language barrier in hospital seems to be
the point that foreigners are aware of, evidenced from the advice (Berthier, n.d.) in
expatbriefing.com as quoted:
Ref. code: 25615721042223AND

92
Healthcare standards in Thailand can be viewed as
good overall. All doctors in Thailand speak English to a more
or less acceptable degree, but language issues may arise for
everything else. This can be for anything like talking to
nurses, calling an emergency helpline, or looking for
information that is available in Thai only.
The comment was confirmed by the findings of this study because among
the 251 participants, doctors and dentists rated their ability as high and moderate,
while the majority of nurses rated themselves as moderate or low in proficiency.
However, language barriers do not occur only in Thailand. In a reverse
case, the study of Moreno, Odom Walker, and Grumbach (2010) stated that there has
been an increase in the adverse influence of language barriers on the quality of
medical care in the United States. As a lot of immigrants, for example, the Spanish,
Mexican, and Asian ethnic groups, reside in the US, an estimated 24 million people
speak English “less than very well” and are considered to have limited English
proficiency. These people are at risk of facing language barriers or experiencing
suboptimal doctor-patient communication. This may support the idea that, not only
the service providers alone, but also the patients need to equip themselves with the
language necessary to facilitate their stay, or else the use of interpreters is required,
and that involves more complicated procedures and outcomes.
As suggested by Shi, Corcos, and Storey (2001), Orr (2002), and Gass
(2012), to overcome the language barriers and cope with deficiency of English ability
of medical learners and healthcare workers, an English course developed from
particular needs and interests of learners would be an effective solution. They
conducted a needs analysis of English skills and found that an EMP course that
covered linguistic and communicative features of the medical topics and the content
areas related to the authentic use of language in medical settings was most needed by
medical learners and workers. Likewise, in this study, a needs analysis was conducted
in order to investigate current proficiency and needs of healthcare workers and
propose indications for EMP course development. Nevertheless, to study whether
personal background of the participants had any influence on their proficiency, the
Ref. code: 25615721042223AND
93
correlation between background factors and level of proficiency was further
investigated. The findings indicated that factors such as gender, profession, education,
work experience, frequency of using English in the workplace, experience with
training in medical facilities abroad, and experience with working abroad correlated
with the proficiency of the participants. Considering that an ESP and an EMP course
should be formulated based on professional information, personal information,
English language information, learners’ lacks, wants, and target situation (Dudley-
Evans & St. John, 1998), it would be appropriate to build a course upon findings from
a needs analysis and background information of the subjects.
5.4 CONCLUSIONS
This study was aimed at investigating English functional skills needed for
three ASEAN occupations—medical, dental, and nursing services. The study was
conducted with 251 doctors, dentists, and nurses from eight governmental hospitals in
Prachuabkirikhan, Thailand. The participants were required to rate their current
proficiency and needs in four English skills through a self-administered questionnaire
which included authentic tasks from medical settings. After the data was statistically
analyzed, the results revealed that among the four skills, needs in reading skill were
ranked the highest, followed by needs in listening skill, speaking skill, and writing
skill, respectively. Although the results were in contrast with findings from other
studies in similar fields, the matters being confirmed were that English functional
skills were rather more demanded in medical tasks than tasks that were not directly
involved with medical settings. In order to effectively develop an ESP course and
promote professional communication among Thai skilled labor of the AEC, giving
attention to their background, particular needs, and interests would be recommended.
5.5 RECOMMENDATIONS FOR FURTHER RESEARCH
Based on the findings and conclusion of this study, the following
recommendations are proposed for further research.
5.5.1 The study was based on quantitative approach. The results presented
were drawn from 251 self-administered questionnaires. To generate more perspectives
and comprehensive understanding in needs of English skills of personnel in medical,
Ref. code: 25615721042223AND

94
dental, and nursing services, further study might include qualitative methods such as
interviews and observations in medical settings.
5.5.2 The participants in this study were highly skilled practitioners
involved in medical, dental, and nursing services which are three out of eight
occupations that are granted mobility into ASEAN integrated market. To enrich
current studies on needs analysis of Thai skilled labor in the AEC context, researchers
might consider further studies in the other five services sectors which involve
engineering services, architectural services, accountancy services, hotel services and
tourism, and surveying qualifications.
5.5.3 The study was carried out in eight governmental hospitals in
Prachuabkirikhan: Hua Hin Hospital, Pranburi Hospital, Samroiyod Hospital, Kuiburi
Hospital, Prachuabkirikhan Hospital, Thapsakae Hospital, Bangsaphan Hospital, and
Bangsaphan Noi Hospital, all of which are located in the western part of Thailand.
Thus, further study could explore needs in English skills from healthcare
professionals in different areas, for instance, in the northern, southern, eastern, or
northeastern parts of Thailand, and not only in governmental hospitals but also in
private hospitals, sub-district health promoting hospitals, or other health facilities.
5.5.4 This study focused on needs analysis for English functional skills of
personnel involved in medical services. The results from the findings, thus, may be
used as part of a database for researchers and curriculum designers in developing
English for Medical Purposes (EMP) courses that serve the needs and interests of the
learners in medical contexts.
Ref. code: 25615721042223AND

95
REFERENCES
Anthony, L. (1997). English for specific purposes: What does it mean? Why is it
different?. On-CUE, 5(3), 9-10. Retrieved from
http://www.laurenceanthony.net/abstracts/ESParticle.html
Anthony, L. (2013). ESP research in Asia. Retrieved from
http://www.academia.edu/24801088/ESP_research_in_Asia
Anthony, L. (2015). The changing role and importance of ESP in Asia. Retrieved
from http://www.ncku.edu.tw/lang/chinese/eagle/01%20Anthony.pdf
Araminta, L. D. W., & Halimi, S. S. (2015). Asian Economic Community 2015:
Needs analysis of universitas Indonesia’s engineering students. Indonesian
Journal of Applied Linguistics, 5(1), 10-17.
ASEAN free trade area agreements. (n.d.). Retrieved from
http://investasean.asean.org/index.php/page/view/asean-free-trade-area-
agreements/view/757/newsid/872/asean-trade-in-goods-agreement.html
ASEAN integration report 2015. (2015). Retrieved from http://www.asean.org/asean-
integration-report-2015-4/
Basturkmen, H. (2006). Ideas and options in English for specific purposes. London:
Lawrence Erlbaum Associates.
Berthier, E. (n.d.). Doctors and hospitals for expats in Thailand. Retrieved from
https://www.expatbriefing.com/country/thailand/healthcare/doctors-and-
hospitals-for-expats-in-thailand.html
Bosher, S., & Smalkoski, K. (2002). From needs analysis to curriculum development:
Designing a course in health-care communication for immigrant students in
the USA. English for Specific Purposes, 21(1), 59–79.
Brown, J. D. (1995). The elements of language curriculum design: A systematic
approach to program development. Boston: Heinle & Heinle.
Chen, I., Chang, Y., & Chang, W. (2016). I learn what I need: Needs analysis of
English learning in Taiwan. Universal Journal of Educational Research 4(1),
1-5. Retrieved from http://www.hrpub.org/download/20151231/UJER1-
19503865.pdf
Ref. code: 25615721042223AND

96
Chia, S. Y. (2013). The ASEAN Economic Community: Progress, challenges, and
prospects. ADBI Working Paper no. 440. Tokyo: Asian Development Bank
Institute.
Chia, S. Y., & Pacini, M. (1997). ASEAN in the new Asia: Issues & trends. Singapore:
Institute of Southeast Asian Studies.
Das, S. B., Menon, J., Severino, R. C., & Shrestha, O. L. (2013). The ASEAN
Economic Community: A work in progress. Singapore: Institute of Southeast
Asian Studies.
Dudley-Evans, T., & John, M. S. (1998). Developments in English for specific
purposes: A multi-disciplinary approach. Cambridge, U.K.: Cambridge
University Press.
EF English Proficiency Index. (2015). Retrieved from http://www.ef.edu/epi/
Fiorito, L. (2006). Teaching English for Specific Purposes (ESP). Retrieved from
http://www.usingenglish.com/articles/teaching-english-for-specific-purposes-
esp.html
Gass, J. (2012). Needs analysis and situational analysis: Designing an ESP
curriculum for Thai nurses. Retrieved from http://www.esp-
world.info/Articles_36/Gass_Nurses.pdf
Gatehouse, K. (2001). Key issue in English for Specific Purposes (ESP) curriculum
development. The Internet TESL Journal, 7(10). Retrieved from
http://iteslj.org/Articles/Gatehouse-ESP.html
Gillett, A. J. (1989). Designing an EAP course: English language support for further
and higher education. Journal of Further and Higher Education, 13(2), 92-
104.
Gylys, B. A., & Wedding, M. E. (1983). Medical terminology. New York: F.A. Davis
Co.
Ref. code: 25615721042223AND
97
Hoekje, B. J., & Tipton, S. M. (2011). English language and the medical profession:
Instructing and assessing the communication skills of international physicians.
Bingley: Emerald Group Publishing.
Huhta, M., Vogt, K., Johnson, E., Tulkki, H., & Hall, D. R. (2013). Needs analysis for
language course design: A holistic approach to ESP. Cambridge: Cambridge
University Press.
Hutchinson, T., & Waters, A. (1987). English for Specific Purposes: A learning-
centred approach. Cambridge: Cambridge University Press.
Kennedy, C., & Bolitho, R. (1984). English for Specific Purposes. London:
Macmillan.
Kirkpatrick, A. (2008). English as the official working language of the Association of
Southeast Asian Nations (ASEAN): Features and strategies. ENGLISH
TODAY, 24 (02), 27-34. doi: 10.1017/S0266078408000175
Long, M. H., & Doughty, C. (2011). The handbook of language teaching. Oxford:
Wiley-Blackwell.
McFarland, J. (2009). Teaching English to the medical profession: Developing
communication skills and bringing humanities to medicine. Retrieved from
http://www.medtrad.org/panacea/IndiceGeneral/n30_tribuna-McFarland.pdf
Medical tourism hub promotion project under the cooperation of Indonesia-Malaysia-
Thailand Growth Triangle: Final report. (2010). Bangkok: The Ministry of
Tourism and Sports.
Ministry of Labor. (2014). Ministry of Labour develops skills of workforce in
preparation for ASEAN Economic Community. Retrieved from
http://www.mol.go.th/en/anonymouse/news/40796
Moreno, G., Walker, K. O., & Grumbach, K. (2010). Self-reported fluency in non-
English languages among physicians practicing in California. Family
Medicine, 42(6), 414–420.
Nguyen, T. Q., & Ngo, C. C. (2015). English language teaching and learning in
ASEAN countries and preparatory steps to integrate into the ASEAN
Economic Community (AEC) 2015. Retrieved from
http://www.uef.edu.vn/newsimg/tap-chi-uef/2015-09-10-24/14.pdf
Ref. code: 25615721042223AND

98
Orr, T. (2002). English for specific purposes: Case studies in TESOL practice.
Alexandria, VA: TESOL.
Patel, B. (2015). Need of ESP for engineers communication competence. ELT VIBES:
International E-Journal for Research in ELT. 1(2), 19-29.
Prachuabkirikhan Public Health Office. (2016). The annual report of
Prachuabkirikhan Public Health Office. Prachuabkirikhan: Author.
Preparation for flow of labor in the ASEAN Community. (n.d.). Retrieved from
http://www.mol.go.th/en/node/22558
Prommeechai, S. (2014). A study of English preparation needs for Thai
undergraduate students in the Faculty of Architecture for the incoming
ASEAN Economic Community (Master’s thesis). Chulalongkorn University,
Bangkok.
Purwanto, S. (2014). Needs analysis of English for specific purposes (ESP) for the
students of Business and Economics Faculty (FEB) UNISBANK Semarang.
Retrieved from file:///C:/Users/Administrator/Downloads/fulltext_stamped.pdf
Questions and answers on the CEPT for AFTA: Plus basic CEPT documents, CEPT
agreement, interpretative notes, rules of origin, operational procedures.
(1993). Jakarta: ASEAN Secretariat.
Robinson, P. C. (1991) ESP today: A practitioner’s guide. Hertfordshire: Prentice
Hall International (UK).
Rybushkina, S. V., & Sidorenko, T. V. (2015). Modular approach to teaching ESP in
engineering programs in Russia. Retrieved from
http://www.weef2015.eu/Proceedings_WEEF2015/proceedings/papers/Contri
bution1015.pdf
Shi, L., Corcos, R. D., & Storey, A. M. (2001). From patient's bedside to English
classroom: An ESP course for clinical training. Retrieved from
http://cei.ust.hk/files/public/3f221-238.pdf
Shi, L., Corcos, R. D., & Storey, A. M. (2001). Using student performance data to
develop an English course for clinical training. English for Specific Purposes,
20(3), 267– 291.
Siddique, S., & Kumar, S. (2003). The 2nd ASEAN reader. Singapore: Institute of
Southeast Asian Studies.
Ref. code: 25615721042223AND

99
Stern, H. H. (1992). Issues and options in language teaching. Oxford: Oxford
University Press.
Strevens, P. (1988). ESP after twenty years: A re-appraisal. In M. Tickoo (Ed.), ESP:
State of the art. Singapore: SEAMEO Regional Language Centre.
Survey of ASEAN employers on skills and competitiveness emerging markets
consulting. (2014). Bangkok: ILO.
Thailand Board of Investment. (2016). Thailand poised to be Asia’s medical hub:
Thailand’s healthcare industry sees a tremendous surge in growth. Thailand
Investment Review, 26(5), 3-4. Retrieved from
http://www.boi.go.th/upload/content/TIR_MAY_56933.pdf
TOEFL test and score data summary. (2016). Princeton, NJ: Educational Testing
Service.
Tongvivat, Y. (2008). Needs assessment for English skills of ICCU nurses in a private
hospital in Bangkok (Master’s thesis). Thammasat University, Bangkok.
Widdowson, H. G. (1983). Learning purposes and language use. Oxford: Oxford
University Press.
Wiriyachitra, A. (2003). Thai teachers’ role in teaching: Motivating students and
guiding their learning. Thai TESOL Focus, 16(2), 25-27.
Yamane, T. (1973). Statistics: An introductory analysis. New York: Harper & Row.
Ref. code: 25615721042223AND

100
APPENDICES
Ref. code: 25615721042223AND

101
APPENDIX A
QUESTIONNAIRE
ENGLISH SKILLS NEEDED BY HEALTH SERVICES PROFESSIONALS OF
ASEAN ECONOMIC COMMUNITY: A STUDY IN PRACHUABKIRIKHAN
แบบสอบถาม ความจ าเปนในการใชทกษะภาษาองกฤษของกลมบคลากรผใหบรการดานสขภาพเพอการท างาน
รองรบประชาคมเศรษฐกจอาเซยน: การศกษาในเขตพนทจงหวดประจวบครขนธ
____________________________________________________________________
This questionnaire is a part of research as a partial fulfillment of the requirements for
Master of Arts in Teaching English as Foreign Language, Language Institute,
Thammasat University. The information you contributed will be used only for the
survey of demand of English skills for Thai healthcare workers involved in three
ASEAN occupations: medical, dental, and nursing services. Please be assured that the
information will be treated with the highest confidentiality and used for research
purposes only. Your cooperation in answering this questionnaire is greatly
appreciated.
This questionnaire comprises three parts:
Part One: General background information of the respondent
Part Two: Linguistic profile of the respondent
Part Three: English abilities and needs of English skills for the AEC
_____________________________________________________________________
แบบสอบถามนเปนสวนหนงของงานวจยในระดบปรญญาโทดานการสอนภาษาองกฤษเปนภาษาตางประเทศ
สงกดสถาบนภาษา มหาวทยาลยธรรมศาสตร มจดประสงคเพอส ารวจความจ าเปนในการใชทกษะภาษาองกฤษ
ของบคลากรผใหบรการดานสขภาพ 3 วชาชพ คอ แพทย ทนตแพทย และพยาบาล ซงเปนวชาชพทสามารถ
เคลอนยายอยางเสรไดในประชาคมเศรษฐกจอาเซยน ผวจยเรยนขอความอนเคราะหใหผตอบแบบสอบถามตอบ
ตามความเปนจรง เนองจากค าตอบของทานมความส าคญตอการวเคราะหขอมลเปนอยางยง ขอรบรองวาขอมล
จากแบบสอบถามของทานจะถกเกบเปนความลบและน าไปใชเพอจดประสงคทางการศกษาเทานน ผวจยหวงเปน
อยางยงวาจะไดรบความรวมมอจากทานเปนอยางด และขอขอบพระคณอยางสงมา ณ โอกาสน แบบสอบถามน
ประกอบดวย 3 ตอน ดงน 1) ขอมลทวไปเกยวกบผตอบแบบสอบถาม 2) ประสบการณดานการใชภาษาองกฤษ
ของผตอบแบบสอบถาม และ 3) ความสามารถและความจ าเปนในการใชทกษะภาษาองกฤษของผตอบ
แบบสอบถามเพอการท างานรองรบประชาคมเศรษฐกจอาเซยน
Ref. code: 25615721042223AND

102
Part One: General Background Information (ขอมลทวไปเกยวกบผตอบแบบสอบถาม)
Directions: Please check (√) all that apply and write the answer in space provided.
(ค าชแจง: โปรดใสเครองหมาย √ ในกลองสเหลยมหนาตวเลอกทตรงกบทานมากทสด และเขยนค าตอบของทาน
ลงในชองวางทก าหนดให)
1. Gender (เพศ): □ male (ชาย) □ female (หญง)
2. Age (อาย) ………………………….
3. Education (วฒการศกษา):
□ Doctor of Medicine (แพทยศาสตรบณฑต)
□ Doctor of Dental Surgery (ทนตแพทยศาสตรบณฑต)
□ Bachelor of Nursing Science (พยาบาลศาสตรบณฑต)
□ Master of Nursing Science (พยาบาลศาสตรมหาบณฑต)
□ Doctor of Nursing Science (พยาบาลศาสตรดษฎบณฑต)
□ Other (อนๆ โปรดระบ) (please specify……………………................................)
4. Profession (อาชพ): □ Doctor (แพทย)
□ Dentist (ทนตแพทย)
□ Nurse (พยาบาล)
5. How many years have you been working in healthcare services? (ทานท างานดานการ
ใหบรการดานสขภาพมากป) ................................year(s) (ป)
Ref. code: 25615721042223AND

103
Part Two: Linguistic Profile (ประสบการณดานการใชภาษาองกฤษของผตอบแบบสอบถาม)
Directions: Please check (√) all that apply and write the answer in space provided.
(ค าชแจง: โปรดใสเครองหมาย √ ในกลองสเหลยมหนาตวเลอกทตรงกบทานมากทสด และเขยนค าตอบของทาน
ลงในชองวางทก าหนดให)
6. How often do you use English in your workplace? (ทานใชภาษาองกฤษในทท างานบอย
เพยงใด)
□ Frequently (บอยครง) □ Occasionally (บางโอกาส)
□ Rarely (นานๆครง) □ Never (ไมเลย)
7. Have you ever participated in an international conference? (ทานเคยเขารวมประชมสมมนา
วชาการระดบนานาชาตหรอไม)
□ Yes (please specify) (เคย โปรดระบ) …………………….. times (ครง)
□ No (ไมเคย)
8. Have you ever been trained/ observed work in medical facility abroad? (ทานเคยเขารบ
การอบรมหรอดงานในสถานพยาบาลตางประเทศหรอไม)
□ Yes (please specify) (หากเคย โปรดระบ ชอประเทศ ระยะเวลา ป/เดอน)
8.1 Country………………………………for……….year(s)……………..month(s)
8.2 Country………………………………for……….year(s)…………….month(s)
8.2 Country………………………………for……….year(s)…………….month(s)
□ No (ไมเคย)
9. Have you ever worked abroad? (ทานเคยท างานในตางประเทศหรอไม)
□ Yes (please specify) (หากเคย โปรดระบ ชอประเทศ ระยะเวลา ป/เดอน)
9.1 Country………………………………for……….year(s)……………..month(s)
9.2 Country………………………………for……….year(s)……………..month(s)
9.2 Country………………………………for……….year(s)……………..month(s)
□ No (ไมเคย)
Ref. code: 25615721042223AND
104
10. Have you ever taken any standardized test of English proficiency (TOEIC,
TOEFL, IELTS)? [ทานเคยสอบขอสอบมาตรฐานเพอวดความสามารถดานภาษาองกฤษหรอไม (โทอค/
โทเฟล/ ไอเอล)]
□ Yes (please specify) (หากเคย โปรดระบ ชอขอสอบ และคะแนนทได)
10.1 …………………………………………………score…………………………….
10.2………………………………………………….score…………………………….
10.3………………………………………………….score…………………………….
□ No (ไมเคย)
Part Three: English abilities and needs of English skills for the AEC (ความสามารถ
และความจ าเปนในการใชทกษะภาษาองกฤษของผตอบแบบสอบถามเพอการท างานรองรบประชาคมเศรษฐกจ
อาเซยน)
Directions: Please check (√) in the boxes on the left to rate your English proficiency
and check (√) in the boxes on the right to rate your English needs for the AEC.
(ค าชแจง: โปรดใสเครองหมาย √ ลงในชองทางซายมอเพอระบระดบความสามารถททานมในการใช
ภาษาองกฤษในสถานการณตางๆ และใสเครองหมาย √ ลงในชองทางขวามอเพอระบความจ าเปนในการใช
ภาษาองกฤษในสถานการณเหลานน เพอการท างานรองรบประชาคมเศรษฐกจอาเซยน)
11. To what extent do you rate your proficiency in English skills, and to what extent
do you need these skills for the AEC? (ทานมความสามารถในการใชภาษาองกฤษแตละทกษะมาก
นอยเพยงใด และทานมความจ าเปนตองใชภาษาองกฤษแตละทกษะเพอการท างานรองรบประชาคมเศรษฐกจ
อาเซยนมากนอยเพยงใด)
Ref. code: 25615721042223AND
105
Proficiency
(ระดบความสามารถในการใชภาษาองกฤษ)
Skills
(ทกษะ)
Needs
(ระดบความจ าเปนตองใชภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
V
ery
lit
tle
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
Listening
(การฟง)
Speaking
(การพด)
Reading
(การอาน)
Writing
(การเขยน)
12. To what extent do you rate your proficiency in listening skill, and to what extent
do you need this skill for the AEC? (ทานสามารถใชทกษะการฟงภาษาองกฤษในสถานการณเหลาน
มากนอยเพยงใด และทานมความจ าเปนตองใชทกษะการฟงภาษาองกฤษเหลานมากนอยเพยงใดเพอการท างาน
รองรบประชาคมเศรษฐกจอาเซยน)
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Listening skill
(ทกษะการฟง)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
1) Listening to patients
histories (e.g. their
symptoms, medical
needs) (ฟงประวตผปวยเปน
ภาษาองกฤษ เชน อาการโรค
ความตองการทางการแพทยของ
ผปวย เปนตน)
Ref. code: 25615721042223AND

106
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Listening skill
(ทกษะการฟง)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
2) Listening to patients’
inquiries (ฟงขอซกถามจาก
ผปวยเปนภาษาองกฤษ)
3) Listening to diagnosis
and symptom
management (ฟงการตรวจ
วนจฉยและการรกษาอาการโรค
เปนภาษาองกฤษ)
4) Listening to lectures (ฟงการบรรยายภาษาองกฤษ)
5) Listening to talks in
conferences (ฟงการสมมนา
ภาษาองกฤษ)
6) Listening to podcasts/
video instructions (ฟงไฟล
เสยง วดโอ หรอสอการสอน
ภาษาองกฤษ)
7) Listening to a variety
of dialects and accents
(ฟงภาษาองกฤษส าเนยง
หลากหลาย)
8) Other (please specify
………………………..)
(อนๆ โปรดระบ)
Ref. code: 25615721042223AND

107
13. To what extent do you rate your proficiency in speaking skill, and to what extent
do you need this skill for the AEC? (ทานสามารถใชทกษะการพดภาษาองกฤษในสถานการณเหลาน
มากนอยเพยงใด และทานมความจ าเปนตองใชทกษะการพดภาษาองกฤษเหลานมากนอยเพยงใดเพอการท างาน
รองรบประชาคมเศรษฐกจอาเซยน)
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Speaking skill
(ทกษะการพด)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
1) Greeting and making
small talks/ general
conversations (ทกทายและ
พดคยเรองทวไปเปน
ภาษาองกฤษ)
2) Asking for patients’
histories (ซกถามประวตผปวย
เปนภาษาองกฤษ)
3) Describing symptoms
and diagnosis (อธบายอาการ
และการตรวจวนจฉยโรคเปน
ภาษาองกฤษ)
4) Explaining steps of
treatment and medication
(อธบายขนตอนการรกษาและการ
ใชยาเปนภาษาองกฤษ)
5) Explaining care plan
and follow-up (อธบาย
แผนการรกษาและการนดหมาย
เปนภาษาองกฤษ)
Ref. code: 25615721042223AND
108
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Speaking skill
(ทกษะการพด)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
6) Giving medical
advice/ instructions (ให
ค าแนะน าหรอขอชแนะทาง
การแพทยเปนภาษาองกฤษ)
7) Giving response to
patients’ inquiries (ตอบขอ
ซกถามของผปวยเปน
ภาษาองกฤษ)
8) Applying non-
technical terms/ language
to develop a better
understanding of patients
(ใชค าทไมใชศพทหรอภาษาทาง
การแพทยในการสอสารกบผปวย
เพอใหผปวยเขาใจไดดขน)
9) Providing
encouragement and
comfort to patients (ให
ก าลงใจผปวยเปนภาษาองกฤษ)
10) Delivering bad news
to patients (แจงขาวรายผปวย
เปนภาษาองกฤษ)
11) Communicating on
telephone (พดคยทาง
โทรศพทเปนภาษาองกฤษ)
Ref. code: 25615721042223AND

109
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Speaking skill
(ทกษะการพด)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
12) Giving presentation
(น าเสนองานเปนภาษาองกฤษ)
13) Giving lectures (สอน
หรอบรรยายเปนภาษาองกฤษ)
14) Giving speech or talk
(e.g. at the seminar,
international conference)
(ปาฐกถาเปนภาษาองกฤษในท
ประชมหรองานสมมนาระดบ
นานาชาต)
15) Other (please specify
………………………..)
(อนๆ โปรดระบ)
14. To what extent do you rate your proficiency in reading skill, and to what extent do
you need this skill for the AEC? (ทานสามารถใชทกษะการอานภาษาองกฤษในสถานการณเหลานมาก
นอยเพยงใด และทานมความจ าเปนตองใชทกษะการอานภาษาองกฤษเหลานมากนอยเพยงใดเพอการท างาน
รองรบประชาคมเศรษฐกจอาเซยน)
Ref. code: 25615721042223AND

110
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Reading skill
(ทกษะการอาน)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
1) Reading patients’
medical records (อานแฟม
ประวตผปวยเปนภาษาองกฤษ)
2) Reading medical
diagnosis/ examination
results (อานผลการตรวจ
วนจฉยเปนภาษาองกฤษ)
3) Reading medical
prescriptions (อานใบสง
แพทยเปนภาษาองกฤษ)
4) Reading referral letter
(อานจดหมายสงตวผปวยเปน
ภาษาองกฤษ)
5) Reading medical
textbooks (อานต าราการแพทย
ภาษาองกฤษ)
6) Reading/
understanding medical
terminology and
abbreviations (อาน/ เขาใจ
ศพทและตวยอทางการแพทย
ภาษาองกฤษ)
7) Reading medical
journals/ research articles
(อานวารสารทางการแพทยและ
บทความจากงานวจยภาษาองกฤษ)
Ref. code: 25615721042223AND

111
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Reading skill
(ทกษะการอาน)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
8) Reading general
publications (e.g. English
newspaper, journals,
novels) (อานสอสงพมพ
ภาษาองกฤษทวไป เชน
หนงสอพมพ วารสาร นวนยาย
เปนตน)
9) Reading manuals/
instructions about
medical equipment (อาน
คมอหรอวธการใชเครองมอทาง
การแพทยภาษาองกฤษ)
10) Other (please specify
………………..………)
(อนๆ โปรดระบ)
15. To what extent do you rate your proficiency in writing skill, and to what extent do
you need this skill for the AEC? (ทานสามารถใชทกษะการเขยนภาษาองกฤษในสถานการณเหลาน
มากนอยเพยงใด และทานมความจ าเปนตองใชทกษะการเขยนภาษาองกฤษเหลานมากนอยเพยงใดเพอการท างาน
รองรบประชาคมเศรษฐกจอาเซยน)
Ref. code: 25615721042223AND

112
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Writing skill
(ทกษะการเขยน)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
1) Writing medical
records (เขยนแฟมประวตทาง
การแพทยของผปวยเปน
ภาษาองกฤษ)
2) Writing medical notes
(เขยนใบรบรองแพทยเปน
ภาษาองกฤษ)
3) Writing medical
prescriptions (เขยนใบสง
แพทยเปนภาษาองกฤษ)
4) Writing medical
terminology and
abbreviations (เขยนศพท
และตวยอทางการแพทยเปน
ภาษาองกฤษ)
5) Writing referral letter
(เขยนจดหมายสงตวผปวยเปน
ภาษาองกฤษ)
6) Writing medical
research (เขยนงานวจยทางการ
แพทยเปนภาษาองกฤษ)
7) Writing articles for
medical journals (เขยน
บทความส าหรบวารสารทาง
การแพทยเปนภาษาองกฤษ)
Ref. code: 25615721042223AND

113
Proficiency
(ระดบความสามารถในการใช
ภาษาองกฤษ) Writing skill
(ทกษะการเขยน)
Needs
(ระดบความจ าเปนตองใช
ภาษาองกฤษในยค AEC)
Ver
y e
xte
nsi
ve
(มากทส
ด)
E
xte
nsi
ve
(มาก)
M
od
erat
e
(ปาน
กลาง)
L
ittl
e
(นอย)
V
ery
lit
tle
(นอยทส
ด)
Ver
y e
xte
nsi
ve
(มากทส
ด)
Ex
tensi
ve
(มาก)
Mod
erat
e
(ปาน
กลาง)
Lit
tle
(นอย)
Ver
y l
ittl
e
(นอยทส
ด)
5 4 3 2 1 5 4 3 2 1
8) Writing letters (เขยน
จดหมายเปนภาษาองกฤษ)
9) Writing emails (เขยน
อเมลเปนภาษาองกฤษ)
10) Writing memo (เขยน
บนทกสนหรอเรองแจงในองคกร
เปนภาษาองกฤษ)
11) Writing resumes (เขยน
จดหมายสมครงานเปน
ภาษาองกฤษ)
12) Other (please specify
………………...………)
(อนๆ โปรดระบ)
16. Do you have any other English needs or English skills that you find necessary for
your profession in the AEC? (ทานมความจ าเปนตองใชทกษะภาษาองกฤษในดานอนๆ หรอมทกษะ
ภาษาองกฤษนอกเหนอจากทไดกลาวมาททานเหนวามความจ าเปนตอวชาชพของทานในยคประชาคมเศรษฐกจ
อาเซยนหรอไม) …………………………………………………………………………………………
……………………………………………………………………………….
……………………………………………………………………………
…………………………………………………………………………… …………………………………………………………………………………………
Thank you for your time and cooperation
(ขอบพระคณทสละเวลาตอบแบบสอบถามและใหความรวมมอ)
Ref. code: 25615721042223AND

114
APPENDIX B LETTER OF CONSENT
ท ศธ 0516.40/24 สถาบนภาษา มหาวทยาลยธรรมศาสตร เลขท 2 แขวงพระบรมมหาราชวง เขตพระนคร กรงเทพฯ 10200
9 กมภาพนธ 2560 เรอง ขออนญาตเกบขอมลประกอบการท าวทยานพนธ เรยน ผอ านวยการโรงพยาบาล...........................................
ดวยนางสาวศภกานต สขหอม เลขทะเบยน 5721042223 นกศกษาหลกสตรศลปศาสตร-มหาบณฑต สาขาวชาการสอนภาษาองกฤษเปนภาษาตางประเทศ (ภาคภาษาองกฤษ) สถาบนภาษา มหาวทยาลยธรรมศาสตร ท าวทยานพนธ เรอง “English Skills Needed by Health Service Professionals of the ASEAN Economic Community: A Study in Prachuabkirikhan” ในการท าวจยเรองดงกลาวจะใชการเกบรวบรวมขอมลโดยใชแบบสอบถามกบแพทย จ านวน.........คน ทนตแพทย จ านวน.........คน และพยาบาล จ านวน.........คน โดยม รองศาสตราจารย ศรปทม นมอรา เปนอาจารยทปรกษาวทยานพนธ ซงการท าวทยานพนธเปนสวนหนงของการศกษาตามหลกสตร
จงเรยนมาเพอขอความอนเคราะหจากทานไดโปรดพจารณาอนญาตให นางสาวศภกานต สขหอม ไดด าเนนการเกบขอมล เพอประโยชนทางวชาการ และขอขอบพระคณเปนอยางสงมา ณ โอกาสน ขอแสดงความนบถอ ( รองศาสตราจารย ดร. พรศร สงหปรชา ) ผอ านวยการสถาบนภาษา ส านกงานโครงการบณฑตศกษา สถาบนภาษา มหาวทยาลยธรรมศาสตร ทาพระจนทร โทร. 0-2613-3106, โทรสาร 0-2623-5136
Ref. code: 25615721042223AND

115
BIOGRAPHY
Name Miss Supakarn Sookhom
Date of Birth April 15, 1992
Educational Attainment
Academic Year 2013:
Bachelor of Arts
Thammasat University
Work Position Teacher (2017-present)
Hua Hin School
Ref. code: 25615721042223AND