endoscopy and microendoscopy of the · pdf fileferdinand g. pamintuan is a consultant of the...
TRANSCRIPT

Reynaldo M. JAVATE Ferdinand G. PAMINTUAN Susan Irene E. LAPID-LIM
Raul T. CRUZ, Jr.
ENDOSCOPY AND MICROENDOSCOPY OF THE LACRIMAL DRAINAGE SYSTEM
®

Reynaldo M. Javate, M.D., F.I.C.S Ferdinad. G. Pamintuan, MD, FPSO-HNS
Susan Irene E. Lapid-Lim, M.D., D.PBO, F.PAO
Raul T. Cruz, Jr., M.D.
Reynaldo M. Javate is Professor and Chairman, Department of Ophthalmology, and Chief of Lacrimal, Orbital and Oculofacial Plastic Surgery, University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines. He has pioneered minimally invasive surgical techniques in ophthalmic plastic and reconstructive surgery including: Endoscopic Radiofrequency-Assisted Dacryocystorhinostomy (ERA-DCR); Mini-Incision DCR using a Radiosurgery Unit; Endoscopic Lacrimal Duct Recanalization (ELDR) using Microendoscope. In the course of his surgical innovations, he has designed instruments like the JAVATE Endoscopic DCR Electrodes, the JAVATE-PAMINTUAN dacryoplasty electrode, and the JAVATE-KHAN endo suction set, which are manufactured and distributed by ELLMAN International, Inc. (3333 Royal Avenue, Oceanside, NY, USA), the JAVATE lacrimal trephine, and the newly-designed JAVATE microendoscope manufactured by KARL STORZ Tuttlingen, Germany.
Dr. Javate has published numerous articles and book chapters on lacrimal, orbital and oculofacial plastic surgeries and has given lectures/presentations, cadaveric and live surgical demonstrations worldwide.
As Professorial Chair Holder in Ophthalmology at the University of Santo Tomas from (1998–2004) he worked extensively on the subject of surgery of the lacrimal system. For this, he has gained awards and citations such as Gold Series Awards, Faculty of Medicine and Surgery, University of Santo Tomas, Best Faculty Research Award for four consecutive 2-year terms (1994-2002), Dangal ng UST Awards (1998, 1999, 2001, 2003), Hall of Fame Award 2004, The Outstanding Thomasian Alumni (TOTAL) for Health-Medi cine 2005, Philippine Academy of Ophthalmology Award of Distinction for the PAO Geminiano De Ocampo Outstanding Researcher in Ophthalmology Award, and the PAO Outstanding Ophthalmic Educator Award.
He is a fellow of the American Society of Ophthalmic Plastic and Reconstruc-tive Surgery, a Life fellow of the Philippine Academy of Ophthalmology (PAO) and a Board Examiner of the Philippine Board of Ophthalmology (PBO), Past President of the Philippine Society of Ophthalmic Plastic and Reconstructive Surgery, Congress President of the 10th World Congress of the International Society of Dacryology and Dry Eye, and President of the 11th World Congress of the International Society of Dacryology and Dry Eye.
Ferdinand G. Pamintuan is a Consultant of the Department of Oto laryngology Head and Neck Surgery, and Chief of Section for Maxillo facial, Plastic and Reconstructive Surgery, and member of the Residency Training Committee at the University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines.
He has co-authored with Dr. Javate papers on Endoscopic Radiofrequency – Assisted Dacryocystorhinostomy (ERA-DCR) and Endoscopic Lacrimal Duct Recanalization (ELDR) published in both the Journal of Surgical Technique in Ophthalmic Plastic and Journal of Reconstructive Surgery and Ophthalmic Plastic Reconstructive Surgery. He, likewise has published several articles and book chapters on lacrimal surgery and has delivered lectures and workshops in this fi eld.
He belongs to the regional faculty for Asia in the AO-Association for the Study of Internal Fixation (ASIF). In line with this, he has given lectures about facial trauma in various Asian countries.
He is a Fellow of the Philippine Society of Otolaryngology Head and Neck Surgery Inc., Associative Board Examiner for the Philippine Board of Oto laryngology, and the current President of the Philippine Academy of CranioMaxillofacial Surgery.
Susan Irene Lapid-Lim is Visiting Consultant with the Department of Ophthalmology of the University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines. She completed her ophthalmology residency training in the same hospital as Chief Resident. She is a Diplomate of the Philippine Board of Ophthalmology and Fellow of the Philippine Academy of Ophthalmology.
Dr. Lapid-Lim has shown continued interests in research and publication on ophthalmic plastic and reconstructive surgery. She has co-authored winning research papers and other papers presented in national and international meetings including “Peg and Prosthesis Coupling with the Porous Biphasic Calcium Phosphate Sphere: A Philippine-Manufactured Integrated Orbital Implant” (Jesus Eusebio, Sr. Research Paper Contest, 1999); “EndoscopicGuided Repair of Canalicular Laceration, Case Report” (PAO free paper session).
She has co-authored published articles and book chapters including: “Refi nements in Surgical Technique of External Dacryocystorhinostomy”, and “Sutureless Dacryocystorhinostomy Surgery” (Operative Techniques in Oculoplastic, Orbital, and Reconstructive Surgery, 1998); “Radiofrequency for Use in Dacryocystorhinostomy” (New Waves in Dacryocystorhino stomy, Oculoplastic Surgery With Radiofrequency, Aimino G. et al, 1999);“Radio frequency Dacryocystorhinostomy” (The Lacrimal System Diagnosis, Management and Surgery, Springer, 2006).
Raul T. Cruz Jr. is a Consultant at the Department of Ophthalmology, University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines where he has done all his medical activity and completed his training as Chief Resident. He is also an Active Consultant at the St. Anthony Medical Center, Marikina City, Philippines, Alfonso Specialist Hospital, Pasig City, Philippines and Family Clinic Inc., Manila, Philippines. He has been the CEO/active consultant of Centro Estetico Rejuvenation Center, Quezon City, Philippines since 2008.
He has co-authored several lectures in lacrimal, orbital, and oculofacial plastic surgery.
He has been fully dedicated since its beginning to the development and advancement of microendoscopy of the lacrimal system research studies and the publication of its article.
He has deeply involved in Radiofrequency Technology in aesthetic research studies, publication of its article and its inclusion in Aesthetic Oculofacial Rejuvenation by W.B. Saunders (2010).
Armida L. Suller, who contributed to this silver booklet as academic collaborator, is Resident at the Department of Ophthalmology, University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines.

ENDOSCOPY ANDMICROENDOSCOPY OF THELACRIMAL DRAINAGE SYSTEM
Reynaldo M. JAVATE, M.D.Ferdinand G. PAMINTUAN, M.D.Susan Irene E. LAPID-LIM, M.D.
Raul T. CRUZ, Jr., M.D.Department of Ophthalmology, University of Santo Tomas Hospital
University of Santo Tomas, Manila, Philippines
Department of Otorhinolaryngology, University of Santo Tomas HospitalUniversity of Santo Tomas, Manila, Philippines
Academic collaborator:
Armida L. SULLER, M.D.Resident, Department of Ophthalmology
University of Santo Tomas HospitalUniversity of Santo Tomas, Manila, Philippines
®

Endoscopy and Microendoscopy of the Lacrimal Drainage System4
Endoscopy and Microendoscopy of the Lacrimal Drainage SystemReynaldo M. Javate, M.D., Ferdinand G. Pamintuan, M.D.,Susan Irene E. Lapid-Lim, M.D. and Raul T. Cruz, Jr., M.D.Department of Ophthalmology, University of Santo Tomas Hospital, University of Santo Tomas, Manila, PhilippinesDepartment of Otorhinolaryngology, University of Santo Tomas Hospital,University of Santo Tomas, Manila, Philippines
Academic Collaborator: Armida L. Suller, M.D.Resident, Department of Ophthalmology, University of Santo Tomas Hospital, University of Santo Tomas, Manila, Philippines
Correspondence address of the author: Prof. R.M. Javate, M.D.,48 Tirad Pass, corner Sultan Kudarat Sts.,Ayala Heights Village, Quezon City, PhilippinesFax: +63 (2) 732-7481E-mail: rmjavate@pacifi c.net.ph
All rights reserved.1st edition 2012© 2015 ® GmbHP.O. Box, 78503 Tuttlingen, GermanyPhone: +49 (0) 74 61/1 45 90Fax: +49 (0) 74 61/708-529E-mail: [email protected]
No part of this publication may be translated, reprinted or reproduced, trans-mitted in any form or by any means, electronic or mechanical, now known or hereafter invent ed, including photocopying and recording, or utilized in any information storage or retrieval system without the prior written permission of the copyright holder.
Editions in languages other than English and German are in preparation. For up-to-date information, please contact ® GmbH at the address shown above.
Design and Composing:® GmbH, Germany
Printing and Binding:Straub Druck + Medien AGMax-Planck-Straße 17, 78713 Schramberg, Germany
05.15-0.3
ISBN 978-3-89756-187-8
Important notes:Medical knowledge is ever changing. As new research and clinical experience broaden our knowledge, changes in treat ment and therapy may be required. The authors and editors of the material herein have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accept ed at the time of publication. However, in view of the possibili ty of human error by the authors, editors, or publisher, or changes in medical knowledge, neither the authors, editors, publisher, nor any other party who has been involved in the preparation of this booklet, warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. The information contained within this booklet is intended for use by doctors and other health care professionals. This material is not intended for use as a basis for treatment decisions, and is not a substitute for professional consultation and/or use of peer-reviewed medical literature.
Some of the product names, patents, and re gistered designs referred to in this booklet are in fact registered trademarks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain.
The use of this booklet as well as any implementation of the information contained within explicitly takes place at the reader’s own risk. No liability shall be accepted and no guarantee is given for the work neither from the publisher or the editor nor from the author or any other party who has been involved in the preparation of this work. This particularly applies to the content, the timeliness, the correctness, the completeness as well as to the quality. Printing errors and omissions cannot be completely excluded. The publisher as well as the author or other copyright holders of this work disclaim any liability, particularly for any damages arising out of or associated with the use of the medical procedures mentioned within this booklet.
Any legal claims or claims for damages are excluded.
In case any references are made in this booklet to any 3rd party publication(s) or links to any 3rd party websites are mentioned, it is made clear that neither the publisher nor the author or other copyright holders of this booklet endorse in any way the content of said publication(s) and/or web sites referred to or linked from this booklet and do not assume any form of liability for any factual inaccuracies or breaches of law which may occur therein. Thus, no liability shall be accepted for content within the 3rd party publication(s) or 3rd party websites and no guarantee is given for any other work or any other websites at all.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 5
Table of Contents1.0 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62.0 Anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.1 Nasal Cavity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72.2 Nasolacrimal Sac and Duct . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.3 Anatomical Variations in the Lacrimal System by Race and Gender . . . . . . . . . . 92.4 Dimensions of the Nasolacrimal Canal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92.5 Thickness of the Lacrimal Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102.6 Soft Tissue Disparities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102.7 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.0 Evaluation of Patients with Epiphora. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103.1 Schirmer Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113.2 Rose Bengal Test. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113.3 Tear Breakup Time (BUT)
Fluorescein Breakup Time (FBUT). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123.4 Fluorescein Dye Disappearance Test. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123.5 Jones I Test. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123.6 Jones II Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123.7 Canalicular Probing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
4.0 Basic Principles for Surgical Applicationof Radiofrequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134.1 Defi nition of Radiofrequency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Radiofrequency Waveforms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Electrodes in Radiosurgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
5.0 Lacrimal Surgical Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155.1 Endoscopic Radiofrequency-Assisted Dacryocystorhinostomy (ERA-DCR) . . . . . 15
5.1.1 Surgical Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175.1.2 Postoperative Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205.1.3 Discussion: ERA-DCR versus External DCR . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.2 Mini-Incision Dacryocystorhinotomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225.2.1 The Surgical Techniques involved in Mini-Incision DCR . . . . . . . . . . . . . . . . . 22
Preoperative Preparation and Anesthesia . . . . . . . . . . . . . . . . . . . . . . . . 22Skin Incision . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Osteotomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Lacrimal Sac Flaps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Nasal Mucosal Flaps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Anastomosis of the Posterior Flaps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Silicone Intubation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Anastomosis of the Anterior Flaps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Skin Closure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
5.2.2 Postoperative Care in Mini-Incision DCR . . . . . . . . . . . . . . . . . . . . . . . . . 265.2.3 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 5.2.4 Endoscopic Follow-up Documentation after Mini-Incision DCR . . . . . . . . . . . 27
5.3 Endoscopic Lacrimal Duct Recanalization (ELDR) . . . . . . . . . . . . . . . . . . . . . . . . . . 285.3.1 Proper Selection of Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285.3.2 Anatomic Consideration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295.3.3 Operating Room Set Up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295.3.4 Step by Step Approach to ELDR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 305.3.5 Postoperative Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 345.3.6 Advantages and Learning Curve . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355.3.7 Tips and Pitfalls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 365.3.8 Management of Obstructions Proximal to the Lacrimal Sac . . . . . . . . . . . 37
Microendoscopic Canalicular Trephination withSilicone Intubation for Canalicular Obstructions . . . . . . . . . . . . . . . . . . . . 38
5.3.9 Videoendoscopic Images of the Lacrimal Excretory System . . . . . . . . . . . 39Normal Lacrimal Drainage System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Sac and Lacrimal Duct before and after ELDR . . . . . . . . . . . . . . . . . . . . . 39
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40

Endoscopy and Microendoscopy of the Lacrimal Drainage System6
1.0 IntroductionEpiphora, or excessive tearing, is a manifestation of obstruction within the lacrimal system in segments or its entirety. A partial or complete hindrance to lacrimal fl ow can result in stagnation of fl uid and debris that predisposes to purulent infections. This gives rise to signs and symptoms like epiphora, mucus discharge, excessive mattering, conjunctivitis, visual fl uctuations in varying degrees, periocular swelling, dermatitis, or cellulitis. The inconvenience to patients can range from benign to severe.
In 1893, G.W. Caldwell performed the very fi rst surgery directed at the lacrimal system. His dacryocystorhinostomy through an endonasal approach evaded popularity because of poor intra-operative visualization from bleeding at the surgical site. In 1904, Addeo Toti introduced the external dacryocystorhinostomy (DCR) technique for the surgical correction of teary eye. The Toti DCR has been the gold standard against which adaptations in surgical strategies for nasolacrimal duct obstruction (NLDO) are compared.
Since its inception, DCR has undergone a multi-faceted evolution. In recent decades, management shifted again to endonasal applications, then external methods, and back. Only one aspect in the surgical correction of medically refractory NLDO stays constant: its dynamism. The emergence of operative modifi cations continues with the goal of establishing a paradigm in the standards of NLDO management.
Toti’s external dacryocystorhinostomy is the prototype for operative correction of NLD obstruction. Success rate for symptom correction after external DCR has been reported at 80–95%. Despite this favourable outcome, the external approach is accompanied by considerable trauma and hemorrhage risk. Likewise, the cosmetic effect of incisional scarring is a deterrent that makes this procedure unacceptable to some patients. Technically, the complexity of this relatively lengthy method primarily disregards the the anato-physiology of the natural tear drainage system.
The transnasal DCR has matured through the years since Caldwell’s initial attempts. Parallels by West (1910) and Mosher (1921) have since been followed by more modifi cations. Proponents attribute to the endonasal approach minimal operative bleed, shortened operative time, less patient discomfort and downtime, as well as avoidance of a cutaneous scar. More recently, lasers and radiofrequency have emerged as endonasal adjunctive techniques. Initial outcomes with endonasal laser- or Radiofrequency-Assisted DCR, however, have failed to approximate the highly acceptable rates of standard external approach. Many ophthalmologists remained critical of what they regarded as disadvantages of these methods: the need for re-familiarization with the intricacies of intranasal anatomy, the need for collaboration with ENT colleagues, the technical challenge in the use of new equipment, and the relatively steep learning curve.
Eventually, another minimally invasive technique surfaced. Microendoscopes for the direct visualization of the lacrimal system were developed. This made possible the micro endoscopic transcanalicular approach to diagnosis and treatment of lacrimal system pathology, such as obstruction, neoplasm, fi stula, foreign bodies, dacryoliths, or mucosal infl ammation. With a microendoscope, any obstruction and pathologies in the lacrimal system can be visualized directly. Obstructions can be surgically

Endoscopy and Microendoscopy of the Lacrimal Drainage System 7
removed precisely, greatly limiting injury to surrounding normal tissues resulting in less hemorrhage. The method leaves no facial scar, requires a shorter operative time, and results in less postoperative pain. The technique preserves the pumping function of the orbicularis oculi muscle and can be performed even in the presence of active infection of the lacrimal system. The microendoscopic transcanalicular approach has comparable anatomic and functional success rate to the external approach, making it an acceptable alternative to external dacryocystorhinostomy.
This compilation of surgical techniques will cater to experienced or beginning ophthalmologists interested in acquiring newer or in relearning older approaches to lacrimal surgery. It presents technical innovations and procedural variations that may be adapted into personal surgical protocols. More importantly, it may serve as a springboard to further brainstorming and experimentation that may offer even better techniques to resolve lacrimal system disorders.
The silver booklet lays down the following:
� general indications for and operative approaches to the obstructed nasolacrimal system;
� variations in dacryocystorhinostomy surgery that have been tried and testedby the authors to address problematic situations involving the obstructed naso lacrimal system; and,
� innovations in the repair of canalicular obstruction.
Its goal is to provide a comprehensive understanding of current lacrimal system surgic al techniques that will benefi t ophthalmologists and other surgeons.
2.0 Anatomy
2.1 Nasal CavityThe nasal cavity, an air-fi lled fossa occupying the space above and behind the nose, is divided into internal and external parts. The internal part is much larger than the external portion. The external nose, which projects from the face, has supporting structures composed of nasal bones, lateral nasal wall, greater alar and lesser alar cartilages, and fi brofatty tissues. The entire nasal cavity extends from the nostrils anteriorly to the choanae posteriorly.
The nasal cavity is divided by a septum that forms the medial wall for the right and left halves. Each half is further bounded by a roof, a fl oor and a lateral wall. The fl oor of the nasal cavity consists of the palatine process of the maxilla and the horizontal plate of the palatine bone. The narrow roof is formed by several bones and cartilages: the bridge of the nose, anteriorly; the ethmoidal cribriform plate, intermediately; and the fl oor of the sphenoid sinus, posteriorly. The nasal cavity is divided by the nasal septum which is partly osseous and partly cartilagenous. Each lateral wall is marked by three projections (called turbinates or conchae): the superior, middle and inferior conchae. The area below each concha is referred to as meatus.

Endoscopy and Microendoscopy of the Lacrimal Drainage System8
1 Endoscopic view of the inferior turbinate. 2 Sagittal section. Right lateral wall of the nasal cavity in an anatomical specimen presenting the inferior turbinate (it), middle
turbinate (mt), superior turbinate (st) and supreme turbinate (sut).
The inferior turbinate is an infolding of the lateral nasal wall, about 60 mm in size from anterior to posterior direction (Fig. 1). It forms part of the nasal valve and is embryo logically related to the maxilloturbinal ridge. The middle turbinate lies medial to the anterior ethmoidal air cells, the maxillary sinus ostium. It has a length of around 40 mm and height of 14 mm superiorly and 7 mm inferiorly, and develops from the ethmoturbinals. The uncinate process, which is a sickle-shaped fold projecting into the middle meatus, covers the opening to the maxillary sinus. The nasofrontal duct or frontal recess, the highest part of the medial meatus along its anterior portion, receives drainage from the frontal sinus (Fig. 2). Both the nasofrontal duct and the uncinate process are important anatomic landmarks for endoscopic sinus surgery and endonasal DCR.
The superior turbinate is present in 30% of the population and drainage is from the nasofrontal duct and anterior ethmoids.
The nasal cavity functions as the superior part of the respiratory tract where the organ of olfaction is located. It also serves as an air passageway to the lungs that fi lters impurities, especially dust, from the inspired air and warms and humidifi es the air that we breathe. It aids in phonation and receives secretions from the paranasal sinuses and the nasolacrimal canal.
2.2 Nasolacrimal Sac and DuctThe egress of tears from the external eye occurs via the lacrimal apparatus, starting at the lacrimal puncta found near the medial aspects of the upper and lower lid margins. Each punctum, with an orifi ce measuring 0.3 mm in diameter, is found at the summit of the lacrimal papilla, a fi brous mound of avascular tissue, thus giving the punctum a relatively pale appearance. Tears entering each punctum pass on into a canaliculus which continues 2 mm vertically before taking a 90-degree turn medially into horizontal segments that run a distance of 8 mm through the substance of the orbicularis muscle. The superior and inferior canaliculi coalesce into a common canaliculus in 90 to 94% of individuals before empyting into the lacrimal sac at an acute angle. The valve of Rosenmuller, found at the medial aspect of the common canaliculus, helps prevent tear refl ux.
Both the common canaliculus and lacrimal sac are situated between the anterior and posterior limbs of the medial canthal ligament. The lacrimal sac, averaging 12 to 15 mm in height, has a rounded, closed, superior border extending 3 to 5 mm superior to the medial canthal ligament. This oval tear sac lies immediately external to the orbit, lodged within the lacrimal fossa, a hollow indentation bounded anteriorly by

Endoscopy and Microendoscopy of the Lacrimal Drainage System 9
3 Sagittal section. Maxillary bone (mb) and lacrimal sac (ls). 4 Endoscopic view of the nasolacrimal duct opening.
the bony junction of the frontal process of the maxilla and posteriorly by the thinner lacrimal bone (Fig. 3). Intranasally, the lacrimal sac lies an average of 8.8 mm above the insertion of the middle turbinate. Its narrow lower end continues inferiorly into the nasolacrimal duct (NLD). The NLD or tear duct initially travels in a posterolateral direction within a bony nasolacrimal canal of the maxillary bone (a 12 mm long, superior, intraosseus portion) before continuing 2 to 5 mm intranasally within the nasal mucosa (inferior, membranous portion). The NLD opens up beneath the inferior nasal turbinate into the inferior meatus, located approximately 15 mm above the nasal fl oor and 4 to 6 mm posterior to the head of the inferior turbinate (Fig. 4). Inferiorly, the NLD follows a posterior and slightly lateral course. A mucosal fold, the valve of Hasner, is usually present at the nasal opening.
2.3 Anatomical Variations in the Lacrimal System by Race and Gender
Nasolacrimal surgery demands knowledge on the variations in the bony and soft tissue anatomy of the nasolacrimal system that arise from race and gender. Carter and Gausas (2006) acknowledged differences in nasolacrimal canals of patients as to dimensions, thickness of bones, and proximity to the surrounding ethmoidal air cells. Accordingly, they emphasized the need for surgeons to give due con sideration to soft tissue inter-individual differences among patients. Furthermore, they noted anatomical dissimilarities of the lacrimal system between men and women, and among Caucasians, Asians, and black patients that are pertinent when discussing endoscopic lacrimal surgery.
2.4 Dimensions of the Nasolacrimal CanalSeveral studies have demonstrated a tendency for narrower and longer nasolacrimal ducts in females, supporting higher incidences of involutional stenosis and making them susceptible to nasolacrimal duct obstruction. Carter and Gausas also pointed out this gender disparity with respect to the width and length of the nasolacrimal canal containing the membranous nasolacrimal duct.
Racial variations were cited to explain the higher percentage of NLD obstruction occuring among Caucasian patients opposed to patients of the Asian and black races. The rationale behind such thinking being that Asian and black individuals have shorter and wider nasolacrimal ducts that have lower tendencies to occlude.
Endoscopy and Microendoscopy of the Lacrimal Drainage System10
2.5 Thickness of the Lacrimal BoneAsians and blacks clinically appear to possess lacrimal bones that are thicker than those of white patients. During dacryocystorhinostomy on Finnish patients, Hartikainen et al. measured a mean lacrimal bone thickness of 106 microns. Taiwanese patients, however, were found by Lui et al. to have an average lacrimal bone thickness of 5.8 mm ± 0.9 mm in males and 4.2 ± 0.8 mm in females. Though more clinical studies are needed to substantiate these observations, the fact remains that surgeons need to address such differences in order to anticipate necessary variations in their surgical technique.
Carter and Gausas maintained that the adequacy of the body opening in lacrimal surgery cannot be overemphasized. Routine instrumentation may suffi ce in order to create large osteotomies in the papery lacrimal bones of white patients. The use of adjunctive instruments such as drills must be anticipated, on the other hand, if ample-sized osteotomies are to be achieved in the thicker bones of Asian and black patients. The surgeon’s preference towards an external or endoscopic approach to DCR will, likewise, be largely infl uenced by his/her awareness of such gender and racial deviances in lacrimal bone anatomy.
Race and gender are not the only factors affecting the thickness of lacrimal bones. Systemic conditions may contribute to bone alterations. The thickness and density of the lacrimal bone correlated well with those of systemic bones, in a study by Hinton et al. Osteoporosis has been shown to be associated with thinner, low-density lacrimal bones. Since the prevalence of osteoporosis leans more to women than to men, then it follows that clinical studies have concluded that adequate osteotomies are easier to create in women who are more prone to osteoporosis.
2.6 Soft Tissue DisparitiesSeveral studies discuss that dissimilarities in skin thickness, presence or absence of epicanthal folds, dis parities in nasal projection, and other variations in external soft tissues all fi gure in the selection of DCR technique. An endoscopic, intranasal approach can do away with the external soft tissue scarring problems of external DCR, but may be more diffi cult or even impossible to perform in the face of the thicker lacrimal bone structure of Asian and black individuals.
2.7 SummaryThe challenge to a lacrimal surgeon is not so much the perfection of technique, but the conscious effort to anticipate possible variations in the patient’s lacrimal system. Suffi cient knowledge in racial, gender, and anatomical differences can determine the course of a surgeon’s technique during a DCR surgery.
3.0 Evaluation of Patients with EpiphoraThe management of patients with “wet eye” or epiphora cannot begin without an initial, complete assessment of the external eye and eyelid. Careful inspection should distinguish the cause of excessive tearing as either lacrimal hypersecretion or mechanical occlusions to the drainage system and, thus, eliminate unnecessary surgery or result in erroneous surgical procedures.
Dutton and White presented an excellent summary of external ocular signs that may point to tear hypersecretion or refl ex lacrimation as the primary reason for epiphora including: medial canthal swelling, discharge, and erythema (acute dacryocystitis); entropion and trichiasis (corneal irritation); ectropion with punctal eversion and/or

Endoscopy and Microendoscopy of the Lacrimal Drainage System 11
exposure keratitis (lid laxity of aging or seventh nerve palsy); and corneal pathologies (erosions, ulceration, infections, retained foreign bodies) are possible reasons for excess tearing.
Findings that support partial or complete occlusion at some point along the lacrimal drainage include: punctal occlusion, punctal opposition, mass lesions near the medial canthal area, mucopurulent refl ux, nasal polyps, among others.
3.1 Schirmer TestingFundamental to the evaluation of dry eye or excessive tearing are the tests introduced by Schirmer in 1903.
Schirmer I pays particular attention to the aqueous component of the tear fi lm. It is a gross measure of tear production at best, without indicating how much of this is basic or refl ex lacrimation. Before testing, effort is taken to ensure that the patient’s eyes are dry by wiping away excess tears from the lid margins and palpebral cul-de-sac. Filter paper strips measuring 50 mm x 5 mm (#41 Whatman strips), one for each eye, are folded 5 mm from one end. The lower lid margin is pulled downwards as the patient gazes upward. The folded end of the fi lter strip is positioned gently into the exposed cul-de-sac at the junction of the middle and lateral thirds of the lower lid margins taking care to avoid stimulating the cornea. After the fi lter paper is positioned, the lower lid is released, and the patient is made to gaze forward and blink at a normal rate. Exact techniques may vary (dim room or in ambient light; total length of fi lter paper strip used; eyes gazing forward while blinking normally or eyes closed). What remains consistent with all techniques is that the test is carried out for 5 minutes and on both eyes simultaneously. Results are interpreted as negative if the fi lter paper strips show at least 10 mm of wetting, indicating a normal production of tears. Schirmer I is the more commonly used test for dry eye syndrome, but the inconsistencies in manner and time performed and persons doing the evaluation limit its value to diagnosing severe cases of dry eye.
Disputes continue as to the use of topical anesthesia when performing Schirmer I test. There are advocates who claim that Schirmer I test without topical anesthesia measures both basic and refl ex tearing, while adding a topical anesthetic drop will limit the measure to just refl ex lacrimation. Others contend that with or without topical anesthetic, end results are too similar. Hence, Schirmer II test was devised to measure refl ex secretion of tears.
When Schirmer I test is positive (showing less than 10 mm of wetting), evaluation can proceed to Schirmer II testing in a dimly illuminated room and topical anesthetic (proparacaine 1%) drops instilled in both eyes. The patient keeps both eyes shut for one minute, while the nasal mucosa is mechanically irritated with a cotton-tip applicator or chemically with ammonium chloride. The steps for Schirmer I test are then repeated. The difference in wetting between Schirmer I and II determines the amount of refl ex tear secretion under stress. Equal wetting in both tests point to lack of refl ex tearing. If Schirmer II results exceed Schirmer I wetting, then this may indicate a total block in conjunctival efferent nerves (Dutton and White).
3.2 Rose Bengal TestOne percent Rose Bengal stain is a chloride-substituted iodinated fl uorescein dye. Not only does it stain dead and devitalized epithelial cells and keratin, it is capable of staining epithelial cells that are insuffi ciently covered by tear fi lm and mucin. Staining can be seen even in early or mild conditions of dry eye, thus easily indicating inadequate tear physiology in syndromes like keratoconjunctivitis sicca.

Endoscopy and Microendoscopy of the Lacrimal Drainage System12
3.3 Tear Breakup Time (BUT)Fluorescein Breakup Time (FBUT)
A normal tear fi lm is continuously formed over the ocular surface, and maintained by blinking. Tear breakup times vary depending on the integrity of the mucin layer. This can be tested after touching a slightly moist fl ourescein strip to the lower palpebral conjunctiva to stain the tear fi lm. Utilizing the diffuse cobalt blue setting of the slit lamp illumination, the patient is instructed to blink and keep the eyes open in primary gaze. The length of time between the last blink and the appearance of the fi rst dry spot on the cornea is measured. Fluorescein Breakup Time (FBUT) is between 15 and 30 seconds. An underlying mucin defi ciency and inadequate tear fi lm stability is consistent with BUT’s of 10 seconds and below. Such dry eye conditions may trigger refl ex hypersecretion of the aqueous component of the tear fi lm resulting in epiphora.
3.4 Fluorescein Dye Disappearance TestThis is a simple way to qualitatively estimate the rate at which tears fl ow out of the conjunctival sac. The tear fi lms of both eyes are stained with fl uorescein dye and initially examined under slit lamp microscopy with cobalt blue light. The tear meniscus in each eye is again examined in similar manner after 5 minutes and graded using a scale from 0 to 4+ in terms of dye retention. A clear tear fi lm or Grade 0 or a positive test due to absence of any remaining dye is attributed to normal outfl ow in the lacrimal system. Grade 4+ is given to eyes where all dye remains. This negative test can indicate either an anatomical blockage (lacrimal outfl ow obstruction) or a functional blockage (pump failure), but unfortunately cannot discriminate between the two.
3.5 Jones I TestThe anatomical and physiologic patency of the lacrimal drainage system may be evaluated by confi rming the actual passage of a vital dye through its length. This is the principle behind the commonly used Jones tests (primary and secondary) in the evaluation of patients presenting with epiphora.
The primary Jones (Jones I) test for physiologic patency must be carried out under conditions that approximate the normal. The patient is seated upright during the test, blinking at a normal rate, and does not receive surface ocular anesthesia. The nasal mucosa, however, may be topically anesthesized to keep the patient comfortable (Dutton and White). Fluorescein vital dye (2% solution) is instilled into the inferior palpebral conjunctival fornices near the punctum and the patient is advised to avoid rubbing the eye. After fi ve minutes, the patient is made to occlude the nostril opposite the eye being tested and to blow into white tissue. If fl uorescein dye is not grossly visible with this maneuver, repeat the test. This time, however, a cotton-tipped applica tor is inserted about 10 mm into the nose against the inferior turbinate, at the level of the nasolacrimal duct ostium that opens 5 to 10 mm below the vault of the anterior end of the nasal meatus. The applicator insertion is done at 2 and 5 minutes. A positive Jones I test, where vital dye is recovered from the nose, indicates the system’s anatomic patency and its probable normal function. Partial obstruction or abnormal physiology, however, is not ruled out. Non-retrieval of the fl uorescein dye, or a negative Jones I test, may point to anatomic obstruction, physiologic dysfunction, or a false negative test where lacrimal anatomy and physiology are still normal. Jones I test is unable to single out the particular pathology involved.
3.6 Jones II TestThe secondary Jones test is done if the primary Jones test yields a negative result. With the patient leaning forward, clear saline is irrigated into the nasolacrimal system using a lacrimal cannula through the inferior punctum. The patient then expectorates into a basin or blows his/her nose into white tissue. If clear irrigating fl uid passes into the nose, the nasolacrimal system is patent but may have functional blockage at the level of the punctum or canaliculus since the vital dye failed to enter the nasolacrimal system. Recovery of dye at the nose supports a functional blockage, usually distal to the lacrimal sac, since the dye was able to enter the nasolacrimal system up to that point.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 13
Complete nasolacrimal duct obstruction results in refl ux of irrigating saline with dye through the upper punctum. The absence of dye in the fl uid that backfl ows through the upper punctum, however, is highly indicative of complete occlusion of the common canaliculus.
3.7 Canalicular ProbingProbing of the puncta, canaliculi, and lacrimal sac is done to confi rm the level of obstruction. Topical anesthesia is instilled into the eye and a small probe is inserted into the canaliculus. If blockage or stenosis is present, the probe is clamped at the punctum to measure the distance of the obstruction in millimeters before withdrawal.
4.0 Basic Principles for Surgical Applicationof Radiofrequency
4.1 Defi nition of RadiofrequencyA radiofrequency (RF) unit has become an indispensable tool for both primary care and subspecialty physicians. Compared to traditional scalpel surgery, radiofrequency or modern electrosurgery, as it is sometimes called, is increasingly gaining acceptance in procedures and techniques employed in general surgery, otorhinolaryngology, dermatology and gynecology. In the same way, it continues to gain a foothold as a therapeutic tool in ophthalmic plastic and orbital surgeries (Pfenninger, 2003).
Drs. Harvey Cushing and William T. Bovie pioneered in the use of RF current in medical practice as early as the 1920s, in that they used an electrosurgical device for tissue incision and coagulation for surgery (Sung, 2000). Dr. Bovie, an eccentric physicist and plant physiologist, developed a unique electrosurgical machine that was able to pass alternating current of high frequencies through a human body in order to cut or coagulate tissues. He collaborated with Dr. Cushing, the pioneer of neurosurgery in America, thus introducing the Bovie electrosurgical unit for use in delicate surgical procedures (O’Connor, 1996).
A typical RF unit usually comprises a transformer, an electrode and a ground plate. Radiofrequency energy, modifi ed by the transformer, essentially, travels from the active electrode to the body tissues of a patient, then back to the machine via the ground plate. Radiofrequency energy is a very high-frequency alternating current (AC) that differs from either alternating current of low frequency or direct current. The high-frequency radio waves fl ow from the conductor or active electrode into the immediate surrounding space as electromagnetic waves. These radiofrequency waves exert a “skin effect”. The AC energy is distributed close to the surface of an active conductor. Application of RF energy to tissues at the target site of surgery essentially induces super fi cial tissue alterations, with only minor spread of heat in deeper levels or adjacent areas, thus limiting collateral thermal damage. The current then travels back to the RF generator by way of dispersive electrodes in the ground plate applied to the patient’s body. The heat generated in the tissues rises to temperatures ranging from 60 to 1000º C, enough to induce cellular death resulting in precise incisions, excisions, and/or tissue coagulation (Gupta, 2005).
In principle, radiosurgery is the passage of high-frequency radio waves ranging from 500 KHz to 4 MHz, from an “active electrode” (a thin tungsten wire) in a hand piece through soft tissues, focused by a “passive electrode” (an insulated ground plate / antenna plate) close to, but not necessarily in contact with, the patient (Aimino, 1999).
RF surgery differs from conventional electrosurgery with galvanic energy where currents are delivered to the operative tissues using the patient’s body as a con ductor. Conversely, RF makes use of electrical energy, the generation of which is based on a transmitter-receiver principle. Electrical energy, emitted by a fl at antenna, is concentrated at the apex of an electrical fi eld, and then converged onto the tip of a delivery electrode. From here, the current is distributed through the tissues at the operative fi eld without requiring an electrical conductor. There is an inverse relationship between the intensity of the current applied and the distance between the RF energy source and the tissues being surgically treated. When the tip of the RF electrode is placed closer to the surgical fi eld, then less electrical power is necessary to produce a change in the tissues being treated (Vogt, 2007).

Endoscopy and Microendoscopy of the Lacrimal Drainage System14
Radiofrequency Waveforms Radiofrequency waves can be modifi ed to either cut (excise), cut and coagulate (blend), coagulate (produce hemostasis), or fulgurate (ablate) soft tissues by setting the radiofrequency unit to deliver current at certain waveforms or intensities (Aimino, 1999).
An RF generator has a transformer that modifi es the main voltage input into a high-frequency, high-voltage alternating current. Four possible output waveforms are produced by further fi ltering and rectifi cation (Javate, 2006).
The fi rst is a continuous high-frequency waveform dissipating the smallest amount of lateral heat and effecting a micro-smooth pure cut (Fig. 5a). This fully-fi ltered, fully-rectifi ed, 90% cut + 10% coagulation waveform is preferred when the goal is to produce tissue incisions with the least collateral tissue damage from spreading heat. This waveform is used when cuts are made and bleeding is expected to be minimal (e.g. initial skin incisions, excision biopsies, tissue grafting, etc.) (Javate et al., 2006). The continuous waveform is delivered from a fi ne-wire electrode to produce smooth incisions similar to those created by cold-knife surgery (Older, 2002). Electrosection refers to this cutting effect that avoids crushing pressure on surrounding tissues since the passing radio waves generate enough heat in water molecules along its path, enough to volatize the cells along the way. What results is a precise split through soft tissues (Javate, et al. 2006).
A fully rectifi ed, modulated waveform is emitted with minute wave pulsation, resulting in a less-effective electrosection or cut (Fig. 5b). Unlike the continuous waveform, lateral heat is generated to a degree that is useful to promote hemostasis. This waveform, when delivered with an electrode shaped like a large-diameter needle, is appropriate for dissecting through subcutaneous tissues (Aimino, 1999). This blended (fully rectifi ed 50% cut/ 50% coagulation) cut/coagulation waveform is ideal for excising lesions or subcutaneous tissue dissection, since it blends the minimal tissue injury of a pure cut with the coagulation needed for hemostasis. For instance, this waveform can address the slight bleeding expected when working with lesions like verrucae, nevi, papillomas, keratoses, skin tags, or keloids. It is especially helpful in transconjunctival blepharoplasty (Javate et al., 2006).
When working with vascular soft tissue structures, hemostasis becomes a priority. The surgery will require the partially rectifi ed, modulated waveform (Fig. 5c). The delivery of intermittent, high frequency waves with increased transmission of lateral-spreading heat, affords the surgeon excellent hemostasis (Aimino, 1999). The generation of coagulation currents is based on the principle of molecular oscillations producing heat. This results in tissue dehydration and coagulation without volatizing cells (Javate et al., 2006). This direct/indirect, spot coagulation with minimal lateral heat spread requires a partially rectifi ed (10% cut/90% coagulation) waveform to adequately control bleeding vessels up to 2 mm in diameter. This waveform is appropriate when resecting orbicularis muscle and orbital fat in procedures such as blepharoplasty, ptosis repair, correction of lid retractions, and lesion excisions (e.g., telangiectasias and spider veins). This is also used in external, Mini-Incision, and endonasal DCR (Javate et al., 2006).
The fulguration or spark-gap waveform allows for rapid dessication and destruction of tissues that the active electrode comes in contact with (Fig. 5d). The modifi ed electrical current causes limited tissue destruction through the insulating effect of carbonized tissues and a space or air gap the spark must leap across. The spark-gap waveform is most appropriate for fulguration purposes since it produces signifi cant lateral heat. It is useful when destruction and superfi cial hemostasis is required, e.g., when excising small lesions of basal cell carcinomas or cysts. This mechanism is similar to unipolar diathermy using a Hyfrecator.
A 1.7 MHz bipolar waveform is preferred for wet-fi eld cauterization, when precision hemostasis is required, or when control of individual, microsurgical bleeders is critical (Fig. 5e). The waveform specifi cally avoids adherence of tissues to the tip of forceps.
5 The various radiosurgery waveforms: Fully Filtered (Cut) (a). Fully Rectifi ed
(Cut/Coag) (b). Partially Rectifi ed (Hemo) (c). Fulguration (d). Bipolar (e).
e
d
c
b
a
6 The various radiosurgery electrodes: Round loop electrode (a). Fine wire
electrode (b). Vari-tip™ wire electrode (c). Empire® electrode (d).
ba c d

Endoscopy and Microendoscopy of the Lacrimal Drainage System 15
Table 1 Disadvantages of External DCR
� Presence of a cutaneous scar.
� Potential for injury to medial canthal structures.
� Cerebrospinal fl uid rhinorrhea.
� Functional interference with the physio logical action of the lacrimal pump.
� Postoperative morbidity including peri orbital bruising, risk of copious hemorrhage and late DCR failure.
Table 2 Disadvantages of Laser-Assisted DCR
Argon, KTP laser not designed for bone removal
CO2 laser cumbersome, lack of a fi beroptic delivery system
Ho:YAG laser requires adjunctive use of a drill
Table 3 Disadvantages of External DCR
� Extensive technical support required
� Cost of purchasing and maintaining the laser has been prohibitive
8 Endoscopic laser-assisted DCR using a CO2 laser (a). Endoscopic laser-assisted
DCR using a Potassium titanyl phosphate (KTP) laser (b).
a
b
7 KARL STORZ IMAGE1 Camera Control Unit (top), HOPKINS® rod-lens nasal endoscope (middle), available in various angles of view, 0°, 30° and 45° (left).
0°
30°
45°
Electrodes in Radiosurgery Radiofrequency procedures typically involve that the surgeon is faced with decisions not only as to which waveform, but also which electrode type to use. The choice of the appropriate electrode depends on the various lesions to be treated, surgical procedures to be performed, degree of hemostasis needed, or the cosmetic results desired. The selective use of a fi ne needle electrode, a wire-loop electrode, a scalpel blade electrode or other types of electrodes will help deliver the correct current while resulting in minimal tissue lateral damage, minimal scarring, and a faster, cosmetically-acceptable healing (Fig. 6) (Javate et al., 2006).
When minimal scarring from a very fi ne skin incision is desired, for example, an extra-fi ne Empire® electrode may be utilized. Excision of small lesions (as occuring in eyelid areas) or excision biopsy for collecting specimens from bigger neoplasm may call for the use of round-loop electrodes. Skin lesions raised above the base, or pedunculated lesions may be excised using triangular or oval-loop electrodes. Coagulation may necessitate the use of ball-type electrodes (Javate et al., 2006).
In Endoscopic Radiofrequency-Assisted Forehead (ERAF) lift procedures, Javate et al. make use of the endoscopic forehead lift electrode. For endonasal DCR, Mini-Incision DCR and standard external DCR procedures, the authors prefer the use of the Ellman JAVATE DCR electrode (Javate et al., 1995).
5.0 Lacrimal Surgical Techniques
5.1 Endoscopic Radiofrequency-Assisted Dacryocystorhinostomy (ERA-DCR)
Standard external dacryocystorhinostomy (SE-DCR) has been the traditional mainstay among surgical approaches to nasolacrimal obstruction management for the past millenium. This gold standard, however, is not without its disadvantages (Table 1) including cutaneous incisional scarring, potential injury to medial canthal structures, cerebrospinal fl uid rhinorrhea, functional interference with lacrimal pump physiology, postoperative morbidity including periorbital bruising, risk of copious hemorrhage, and late DCR failure.
Rigid 0º and 30º-HOPKINS® rod-lens nasal endoscopes (Fig. 7) made endoscopic DCR possible with direct visualization of the intranasal cavity (Shun-Shin and Thurairajan, 1997). Lasers later came into use for the endonasal approach (Heharet al., 1997).
Carbon dioxide (CO2) or Potassium titanyl phosphate (KTP) lasers for endoscopic laser-assisted DCR have been described by Gonnering, Lyon and Fisher (Figs. 8a–b). The limitations with laser-assisted procedures are primarily economic as they can make operative costs for lacrimal surgery prohibitive (Tables 2–3).

Endoscopy and Microendoscopy of the Lacrimal Drainage System16
In 2005, Javate and Pamintuan described the Endoscopic Radiofrequency-Assisted DCR (ERA-DCR) as an alternative to laser-assisted DCR (Fig. 9). This innovation required commonly cost-effective instrumentation like curette, KERRISON punch, FREER periosteal elevator, HOPKINS® endoscope, Ellman Surgitron Dual Frequency Unit (Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA), and the JAVATE DCR electrodes designed for the procedure (Figs. 10a–c) (Table 4).
In 1995, Javate, Campomanes et al. fi rst reported use of a radio frequency adjunct for endonasal DCR yielding a surgical success rate of 90%. Since then, the original ERA-DCR technique with the addition of double stenting using a Griffi ths collar button (Javate and Pamintuan, 2005) (Fig. 11a). The Griffi ths collar button is a nasolacrimal catheter designed to fi t within the lacrimal fossa, while extending through the nasal mucosa. The collar button has a 5-mm interfl ange distance and a 3-mm lumen. The silicone tubes are made to run through the lumen of the catheter that is kept in place for 5–6 months to ensure patency of the nasal ostium (Fig. 11b). The anterior and posterior fl anges have fl at top confi gurations measuring 8 mm in diameter by 0.5 mm in thickness that allow fl exibility during the catheter placement and removal. The fl ange virtually eliminates migration of the catheter either distally into the nasal cavity or retrograde into the lacrimal sac (Javate and Pamintuan, 2005).
9 Endoscopic Radiofrequency-Assisted DCR (ERA-DCR).
10 JAVATE DCR electrodes (a). Ellman Surgitron Dual RF S5 (Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA) (b).
JAVATE-PAMINTUAN ERA-DCR recommended instrument set (c).
a
c
b
11 Griffi ths collar button (a). Griffi ths collar button with silicone tubes (b). Preoperative nasal packing (c).
a b
c
Table 4 Instrument Set for Endoscopic Radiofrequency-Assisted Dacryocystorhinostomy (ERA-DCR)
� HOPKINS® Rhinoscopes 0° and 30°(KARL STORZ Tuttlingen, Germany)
� BLAKESLEY nasal forceps � Aquagel (Parker Laboratories, Fairfi eld, NJ, USA)
� Retinal light pipe � Ellman Surgitron Dual Frequency Unit (Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA)
� JAVATE DCR Ellman electrodes � Suction unit (KARL STORZ Tuttlingen, Germany) with tip
� Headlight (KARL STORZ Tuttlingen, Germany)
� Bayonet forceps
� Nasal speculum
� Cotton pledgets
� Oxymetazoline HCl 0.05%
� Spinal anesthesia needle
� Lidocaine solution 2% with 1:100,000 epinephrine, lidocaine 4%, bupivacaine 0.75%
� Wydase®, (Hyaluronidase)
� Bone curette � KERRISON punch � Crawford Bicanaliculus Intubation Set (S1-1270u, FCI, 20–22 rue Louis Armand, 75015 Paris, France)
� Mitomycin (2 mg/mL solution) � Corneal eyeshields � Griffi ths collar button (Griffi ths Nasal Catheter No. 5206; Visitec)
� Collagen absorbable haemostat � Suction cannula � Endoscope lens anti-fogging agent
Endoscopy and Microendoscopy of the Lacrimal Drainage System 17
5.1.1 Surgical Technique
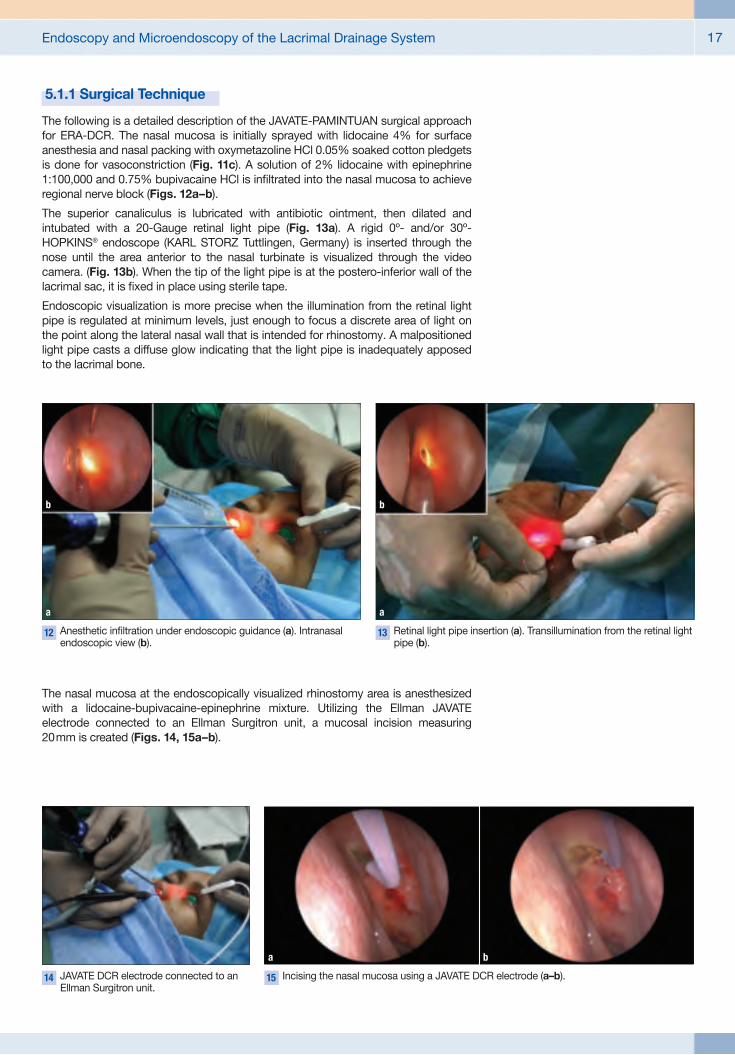
The following is a detailed description of the JAVATE-PAMINTUAN surgical approach for ERA-DCR. The nasal mucosa is initially sprayed with lidocaine 4% for surface anesthesia and nasal packing with oxymetazoline HCl 0.05% soaked cotton pledgets is done for vasoconstriction (Fig. 11c). A solution of 2% lidocaine with epinephrine 1:100,000 and 0.75% bupivacaine HCl is infi ltrated into the nasal mucosa to achieve regional nerve block (Figs. 12a–b).
The superior canaliculus is lubricated with antibiotic ointment, then dilated and intubated with a 20-Gauge retinal light pipe (Fig. 13a). A rigid 0º- and/or 30º-HOPKINS® endoscope (KARL STORZ Tuttlingen, Germany) is inserted through the nose until the area anterior to the nasal turbinate is visualized through the video camera. (Fig. 13b). When the tip of the light pipe is at the postero-inferior wall of the lacrimal sac, it is fi xed in place using sterile tape.
Endoscopic visualization is more precise when the illumination from the retinal light pipe is regulated at minimum levels, just enough to focus a discrete area of light on the point along the lateral nasal wall that is intended for rhinostomy. A malpositioned light pipe casts a diffuse glow indicating that the light pipe is inadequately apposed to the lacrimal bone.
12 Anesthetic infi ltration under endoscopic guidance (a). Intranasal endoscopic view (b).
a
b
13 Retinal light pipe insertion (a). Transillumination from the retinal light pipe (b).
b
a
The nasal mucosa at the endoscopically visualized rhinostomy area is anesthesized with a lidocaine-bupivacaine-epinephrine mixture. Utilizing the Ellman JAVATE electrode connected to an Ellman Surgitron unit, a mucosal incision measuring 20 mm is created (Figs. 14, 15a–b).
14 JAVATE DCR electrode connected to an Ellman Surgitron unit.
15 Incising the nasal mucosa using a JAVATE DCR electrode (a–b).
a b

Endoscopy and Microendoscopy of the Lacrimal Drainage System18
A FREER periosteal elevator is used to lift the incised nasal mucosa off from the under lying bone, followed by initial punc-ture at the rhinostomy target area using a curette (Figs. 16a–b).
16 A FREER periosteal elevator is used to lift the incised nasal mucosa off (a) from the underlying bone (b).
a b
17 A KERRISON punch is used to enlarge the osteotomy to a 10–15 mm sized ostium (a–b).
a
18 Indenting the sac wall using the retinal light pipe (a–b).
a
19 Incision of postero-inferior and antero-inferior walls using JAVATE DCR electrodes (a–b).
a
b
b
b
Indenting the sac wall using the retinal light pipe facilitates the procedure to ensure an incisional opening measuring between 5 mm to 10 mm (Figs. 18a–b).
The authors recommend shorter electrodes to incise through normal-sized or enlarged lacrimal sacs. The longer electrodes are preferred for scarred, malformed sacs. Should there be excess marginal lacrimal sac tissues, these may be excised using BLAKESLEY nasal forceps (Fig. 20). The authors have found that the use of Ellman JAVATE DCR electrodes and the BLAKESLEY nasal forceps in endoscopic DCR gives the surgeon an option what laser DCR cannot: direct visualization and biopsy of the lacrimal sac.
Once the lacrimal sac is visualized, its postero-inferior and antero-inferior walls are incised with Ellman JAVATE DCR electrodes (Figs. 19a–b). Occasions arise when cicatrization may prevent adequate identifi cation and visualization of the lacrimal sac. In these cases, Aquagel (Parker Laboratories, Inc., Fairfi eld, NJ) may be injected through the canaliculus in order to dilate the sac. This is a precaution against accidental injury to the common canaliculus when incising through the sac walls.
A KERRISON punch is used to place an initial puncture in the target area of rhino-stomy and to enlarge the ostium to a size of 10 to 15 mm, making sure that the rhinostomy includes part of the frontal process of the maxilla (anterior lacrimal crest) (Figs. 17a–b).

Endoscopy and Microendoscopy of the Lacrimal Drainage System 19
22 Crawford Bicanaliculus Intubation Set (S1-1270u, FCI, 20–22 rue Louis Armand, 75015 Paris, France).
a
20 Excision of excess marginal lacrimal sac tissues using BLAKESLEY nasal forceps.
Bicanalicular silicone intubation through the superior and inferior canaliculi.
b
The guidewire tip has been passed through the intranasal ostium.
c
21 Mitomycin-C 2 mg/vial (a). Cotton balls soaked in mitomycin-C (0.5 mg/mL) are applied over the underlying mucosa for 3 minutes (b).
a b
Once the surgeon decides that the nasal mucosa, rhinostomy and lacrimal sac incisions are of ample measure, cotton balls soaked in mitomycin (0.5 mg/mL) are applied over the underlying mucosa for 3 minutes with the goal of preventing scarring from overactive fi broblastic proliferation (Figs. 21a–b). Measures must then be taken to aggressively wash off all mitomycin from the operative site with generous irrigation using sterile saline solution.
A Crawford Bicanaliculus Intubation Set (S1-1270u, FCI, 20–22 rue Louis Armand, 75015 Paris, France) is utilized for bicanalicular silicone intubation of the nasolacrimal fi stula (Figs. 22a–c).
The probes of the canalicular tubes are inserted through the central lumen of the Griffi ths collar button (Griffi ths Nasal Catheter No. 5206; Visitec) after which the catheter is pushed superiorly through the nostril and positioned with alligator forceps or a curette to ensure that its fl anges straddle the bony ostium (Figs. 23a–b). The tubes are fi nally secured with two square knots, fi xed by a 5-0 silk suture, and cut to appropriate lengths within the nose.
Lacrimal irrigation around the silicone stent is done under endoscopic view to ensure intra-operative patency of the fi stula (Fig. 24).
24 Lacrimal irrigation around the silicone stent.
23 Probes of the bicanalicular tubes are inserted through the central lumen of the
Griffi ths collar button.
a
The positioned Griffi ths collar button withsilicone tubes in place.
b

Endoscopy and Microendoscopy of the Lacrimal Drainage System20
The average length for the ERA-DCR cases that the authors performed ranged from 35 to 40 minutes.
5.1.2 Postoperative Care
Operative and postoperative bleeding can be controlled by positioning oxidized regenerated cellulose at the tip of the middle turbinate using bayonet forceps. The cellulose absorbs spontaneously (Fig. 25).
The authors’ medical postoperative regimen comprises the following: ofl oxacin ophthalmic solution (Inofl ox, Santen Pharmaceutical Co. Ltd, Osaka, Japan), applied four times daily; thrice daily nasal irrigation with saline; fi nally, fl uticasone proprionate nasal spraying beginning on the fi rst day following surgery.
Patient follow-up is scheduled on the fi rst postoperative day and on the fi rst, second, and third postoperative weeks. For each follow-up visit, the patient undergoes lacrimal irrigation and removal of any residual nasal debris. Likewise, the intranasal ostium is examined endoscopically (Figs. 26a–b).
The Griffi ths collar button is removed on the second or third month following surgery or until the scarring process around the catheter is endoscopically confi rmed to be complete (Fig. 27). Removal of this catheter is a relatively easy offi ce-procedure.
The lacrimal stent must be kept in place for 6 months postoperatively (Fig. 28). Premature removal of the stent might spell DCR failure caused by canalicular system closure.
For their series of patients, the authors reported a postoperative follow-up length ranging 12 to 80 months. Success rates were reported at 98% (110 out of 112 patients).
5.1.3 Discussion: ERA-DCR versus External DCR
The ERA-DCR is deemed successful when the following are confi rmed during patient follow-up: resolution of preoperative epiphora, restored nasolacrimal patency confi rmed by lacrimal irrigation under endoscopic observation at one-year postoperative visit; and endoscopic visualization of fl uorescein dye fl ow from the tear meniscus into the nose (Fig. 29) (Table 5).
Table 5 An operation is defi ned as success if:
� Preoperative epiphora has resolved.
� Nasolacrimal patency as confi rmed by lacrimal irrigation.
� Endoscopic observation of fl uorescein dye fl owing through the surgical ostium on lacrimal irrigation.
25 Oxidized regenerated cellulose placed at the tip of the middle
turbinate using bayonet forceps.
26 Postoperative follow-up using a rigid HOPKINS® endoscope to visualize the intranasal ostium (a). Endoscopic view one week
postoperatively (b).
a b
27 The Griffi ths collar button is removed on the second or third
month following surgery.
28 Intranasal ostium after stent removal.
29 Patency of the intranasal ostium is confi rmed with
irrigation of fl uorescein dye under endoscopic visualization at one year postsurgery.
30 The lacrimal paradox. 31 Backwash of fl uid debrisfrom the residual second
compartment – the lacrimal sac.
Tear Lacrimal Nasal lake sac space
Tear Dilated Nose lake lacrimal sac
Backwashof debris
Smallrhinostomy
1st 2nd 2nd
3rd

Endoscopy and Microendoscopy of the Lacrimal Drainage System 21
Advocates of endoscopic DCR give value to the absence of external cutaneous scarring. An added plus is the greater ability to curb injury to the nasolacrimal fi stula (Table 6). On the other hand, some surgeons remain skeptical about the long-term patency following endonasal DCR since it does not emphasize the need for formal mucosal fl aps and it results in smaller rhinostomies.
In standard external DCR, the nasal mucosa is sutured to the lacrimal sac mucosa to encourage healing by primary intention. These sutured mucosal fl aps serve as scaffolds upon which a new epithelium-lined passage forms for the smooth egress of tears.
As opposed to this, endonasal DCR has been found to encourage greater postoperative fi brosis due to tissue healing by secondary intention. Reported lower success rates in endonasal DCR may have resulted from such reasoning. For instance, healing around the osteotomy site has been associated with endoscopic evidence of fi brous tissue scarring and granulation. These same healing characteristics may encourage adhesion of the osteotomy to the turbinates and septum. Common canalicular obstruction is also a possibility.
Dr. Geoffrey Rose elucidated on the “lacrimal paradox” to clarify the drawbacks from a smaller rhinostomy following endonasal DCR (Fig. 30). Creating a smaller- diameter fi stula to connect the lacrimals to the nasal space produces persistent volume symptoms explained by the backwash of fl uid debris from the residual second compartment – the lacrimal sac (Fig. 31).
Therefore, for endonasal DCR to achieve better results, it requires a wider channel from the lacrimal sac to the nasal cavity by eliminating the sac and eliminating volume signs and symptoms. The original anatomy described as a three-compartment hydraulic system is essentially rearranged into a two-compartment system (Fig. 32). In such cases, wide soft tissue anastomosis can be assured when a large osteotomy, anterior ethmoidectomy, and sutured mucosal fl aps are incorporated into dacryo-cystorhinostomy.
The complications of ERA-DCR with Griffi ths collar button were reported as: tissue granulation (sometimes visualized at the intranasal ostium, but not necessarily indicating occlusion of the ostium) (Fig. 33) ; and, nasal mucosa that migrates to cover the distal fl ange of the Griffi ths collar button (Fig. 34).
The Griffi ths collar button has been shown to improve the success rate of ERA-DCR to 98% (Javate and Pamintuan, 2005). This catheter appears to function as an impediment to: progressive ostium occlusion by cicatrization, ostium adhesion to the middle turbinate; synechiae formation between the ostium and nasal septum (Table 7). In DCR procedures where mucosal fl aps are not fashioned, a Griffi ths collar button straddling the rhinostomy site for a few months postoperatively replaces the absent mucosal fl aps to serve as the scaffold upon the new epithelium-lined channel is formed.
32 The original anatomy, described as a three-
compartment hydraulic system is rearranged into a two-compartment system.
33 Granulation tissue at the edge of the Griffi ths collar
button (arrow).
34 Migration of the nasal mucosa over the distal
fl ange of the Griffi ths collar button.
Tear Nasal space lake and former lacrimal sac
3rd
1st
Table 6 Advantages of Endonasal DCR
� Avoidance of a cutaneous incision and scar.
� Limitation of tissue injury to the site of the nasolacrimal duct.
� Decreased intraoperative hemorrhage.
� Decreased postoperative morbidity and enhanced recovery.
Table 7 Griffi ths collar button prevents
� Progressive cicatricial closure of the ostium
� Development of adhesions between the ostium and the middle turbinate
� Formation of synechiae between the ostium and the nasal septum

Endoscopy and Microendoscopy of the Lacrimal Drainage System22
The postoperative care after standared external DCR is relatively routine: 3 to 4 follow-up visits that require removal of the skin sutures, and eventually, the silicone tubes on the last visit. Endonasal DCR, in comparison, needs a more demanding postoperative regimen: frequent follow-up visits during which mucus and debris at the rhinostomy are cleansed when indicated. Besides endonasal debridement, the edges of the distal fl ange of the Griffi ths collar button must be mobilized to disallow nasal mucosal migration over the fl ange. Again, for each follow-up visit, endoscopic visualization is required.
Mitomycin-C as adjunct in endonasal DCR to ensure rhinostomy patency was described by Bousch et al. in 1994. Mitomycin-C has been reported to push endonasal DCR success rates up to 99.2% in a study done by Camara et al. The same was used in earlier reports on ERA-DCR to modify healing at the rhino stomy by inhibiting fi broblastic proliferation and scarring that would otherwise result in rhinostomy occlusion.
It is generally agreed that smaller rhinostomies created during DCR result in a smaller healed ostium, making the “sump” syndrome likely due to poorly draining remnants of the lacrimal sac. Interest has recently surfaced, however, in “inferior” or “terminal” endonasal DCR. This creates a relatively small ostium at the point where the lacrimal sac meets with the nasolacrimal duct, thereby decreasing the occurrence of lacrimal sump syndrome. With a KERRISON punch, an area of underlying bone and frontal maxillary process measuring 8 to 10 mm in diameter, is removed, creating a bony opening suffi cient in size for the proximal fl ange of the Griffi ths collar button to be inserted.
5.2 Mini-Incision DacryocystorhinotomyStandard external DCR usually begins with a cutaneous incision made along the lateral nasal wall. The incision is a relatively vertical, straight cut that usually leaves insignifi cant deformity or scarring in older patients. More overt blemishes can result in the thicker nasal skin of younger patients with vigorous healing mechanisms that may explain more visible scarring (Figs. 35a–b).
Harris, Sakol and Beatty, in 1989, introduced their modifi cation to the cutaneous incision. They incised through the lower eyelid crease incision creating a cut 12 to 15 mm long, positioned about 4 mm below the lid margin, and extending to the nasal end of the eyelid. As this incision runs along the periorbital relaxed skin tension lines, the cutaneous scarring was reported to be relatively inconspicuous.
In 2001, however, Javate et al. presented their modifi cation to the Harris, Sakol and Beatty incisional technique which resulted in better cosmetic results. This modifi cation involves the use of the Ellman-JAVATE DCR electrode attached to the Ellman Surgitron® Dual RF S5 Unit (Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA) set in cut mode, and a skin incision is defi ned measuring8–10 mm in length, positioned about 7–8 mm below the lower lid margin. The authors reported less incisional scarring with this incision as compared to one set at3–4 mm beneath the lower lid margin, the latter being prone to ectropion from wound contracture. More scarring is noted also from orbital fat prolapse seen in incisions made just above the orbital septum. The radiofrequency electrode used for skin incision has an added purpose of controlling hemorrhage, preventing obscuration of tissue anatomy or poor healing incisions postoperatively. The Mini-Incision offers less postoperative painful infl ammation, ease with spectacle wear, and less downtime.
5.2.1 The Surgical Techniques involved in Mini-Incision DCR
Preoperative Preparation and Anesthesia Mini-Incision DCR may be performed under local or general anesthesia, based on patient age, medical condition, or personal preference. The authors perform anterior ethmoidal and infraorbital nerve blocks with a local anesthetic concoction of lidocaine HCl 2% + bupivacaine 0.75% + epinephrine 1:200,000 solution. Additional anesthesia is infi ltrated subcutaneously at the skin incision.
The cornea is protected with a contact lens. Cotton pledgets soaked in a mixture of oxymetazoline HCl 0.05% and lidocaine HCl 4% are applied to the nasal mucosa anterior to the middle turbinate to induce vasoconstriction.
35 Visible scars 6 months after standard external DCR.
a
b
Table 8 The increased success rate of ERA-DCR can be attributed to
� Additional modifi cation in the surgical technique.
� Proper instrumentation.
� Mastery of surgical details.
� Careful postoperative follow-up.
Endoscopy and Microendoscopy of the Lacrimal Drainage System 23
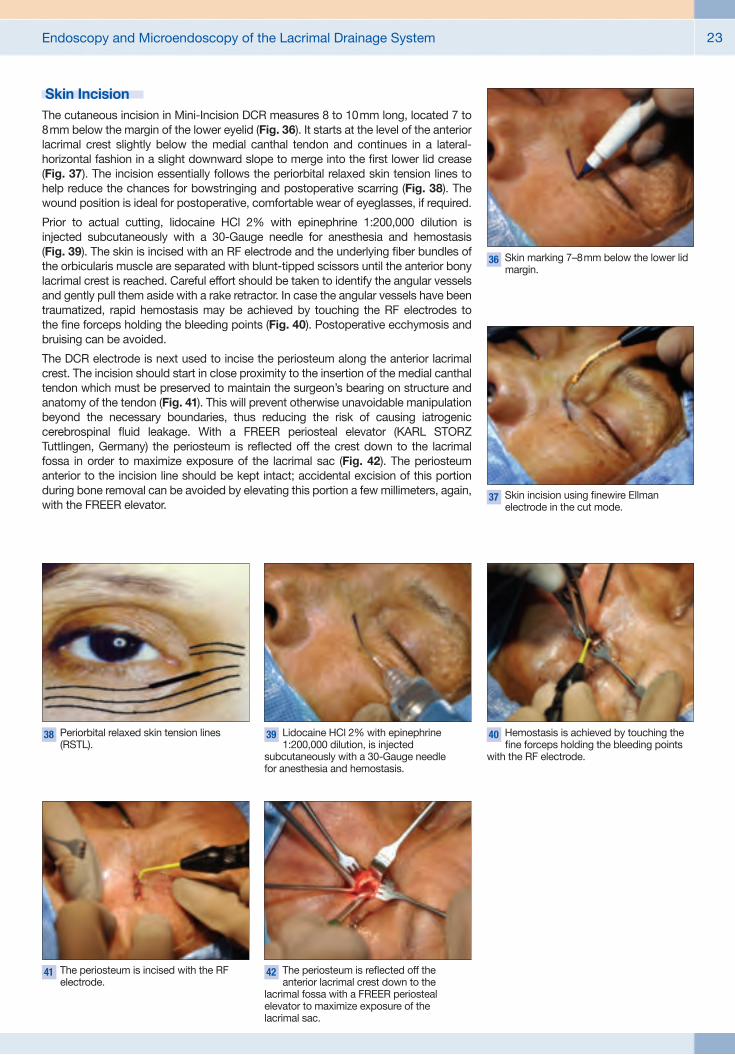
Skin Incision The cutaneous incision in Mini-Incision DCR measures 8 to 10 mm long, located 7 to 8 mm below the margin of the lower eyelid (Fig. 36). It starts at the level of the anterior lacrimal crest slightly below the medial canthal tendon and continues in a lateral-horizontal fashion in a slight downward slope to merge into the fi rst lower lid crease (Fig. 37). The incision essentially follows the periorbital relaxed skin tension lines to help reduce the chances for bowstringing and postoperative scarring (Fig. 38). The wound position is ideal for postoperative, comfortable wear of eyeglasses, if required.
Prior to actual cutting, lidocaine HCl 2% with epinephrine 1:200,000 dilution is injected subcutaneously with a 30-Gauge needle for anesthesia and hemostasis (Fig. 39). The skin is incised with an RF electrode and the underlying fi ber bundles of the orbicularis muscle are separated with blunt-tipped scissors until the anterior bony lacrimal crest is reached. Careful effort should be taken to identify the angular vessels and gently pull them aside with a rake retractor. In case the angular vessels have been traumatized, rapid hemostasis may be achieved by touching the RF electrodes to the fi ne forceps holding the bleeding points (Fig. 40). Postoperative ecchymosis and bruising can be avoided.
The DCR electrode is next used to incise the periosteum along the anterior lacrimal crest. The incision should start in close proximity to the insertion of the medial canthal tendon which must be preserved to maintain the surgeon’s bearing on structure and anatomy of the tendon (Fig. 41). This will prevent otherwise unavoidable manipulation beyond the necessary boundaries, thus reducing the risk of causing iatrogenic cerebrospinal fl uid leakage. With a FREER periosteal elevator (KARL STORZ Tuttlingen, Germany) the periosteum is refl ected off the crest down to the lacrimal fossa in order to maximize exposure of the lacrimal sac (Fig. 42). The periosteum anterior to the incision line should be kept intact; accidental excision of this portion during bone removal can be avoided by elevating this portion a few millimeters, again, with the FREER elevator.
36 Skin marking 7–8 mm below the lower lid margin.
37 Skin incision using fi newire Ellman electrode in the cut mode.
38 Periorbital relaxed skin tension lines (RSTL).
39 Lidocaine HCl 2% with epinephrine 1:200,000 dilution, is injected
subcutaneously with a 30-Gauge needlefor anesthesia and hemostasis.
40 Hemostasis is achieved by touching the fi ne forceps holding the bleeding points
with the RF electrode.
41 The periosteum is incised with the RF electrode.
42 The periosteum is refl ected off the anterior lacrimal crest down to the
lacrimal fossa with a FREER periosteal elevator to maximize exposure of thelacrimal sac.

Endoscopy and Microendoscopy of the Lacrimal Drainage System24
Osteotomy The osteotomy is started with the FREER periosteal elevator after exposing the nasal mucosa overlying the area of the lacrimal bone lying beneath the lacrimal maxillary suture. A blunt instrument like the FREER elevator is suffi cient to puncture this papery-thin area of bone with. It is a simple, painless technique minus the noise from drills, saws or trephines that can be daunting to a conscious patient undergoing DCR with local anesthesia. Following the initial puncture, a KERRISON punch inserted between the nasal mucosa and the maxillary frontal process is utilized to create a 15 mm x 15 mm osteotomy (Fig. 43). The osteotomy is positioned making certain that the common internal punctum lies within the central portion (at least 5 mm from the edge) of the bony window instead of near the edge. The boundaries of the osteotomy are: anteriorly, 5 mm anterior to the anterior lacrimal crest; posteriorly, to the posterior lacrimal crest; inferiorly, to the curve of the crest where it merges with the inferior orbital margin; and superiorly, to the sac fundus or the level below the refl ected part of the medial canthal tendon.
It is important that the osteotomy dimensions be 15 mm x 15 mm, even if the remaining intranasal septum heals to a small size. The osteotomy should be large enough to allow easy mobilization and approximation of the mucosal fl aps.
Bleeding may be controlled by application of oxymetazoline HCl 0.05% with cotton pledgets, or by infi ltration anesthesia to cause nasal mucosal blanching.
Lacrimal Sac Flaps Lacrimal sac fl aps must be created before attempting to fashion the fl aps on the side of the nasal mucosa. The size and shape of the resulting sac fl aps are needed to help decide on how the fl aps on the side of the nasal mucosa should be made.
The following steps describe the creation of lacrimal sac fl aps. A Bowman probe (No. 00) is passed through the superior canaliculus until its tip indents the lacrimal sac (Fig. 44). The indentation indicates the point of where a stab incision is made into the sac using a sickle knife (No. 12 blade) or Beaver knife (No. 15 blade) (Fig. 45). Then, a Jameson muscle hook is inserted into the cavity of the sac, its end guided toward the point where the sac and nasolacrimal duct join (Fig. 46). The muscle hook lifts both the inner mucosa and loose outer covering of the lacrimal sac, and guides the incising blade from the fundus of the sac to the nasolacrimal duct (Fig. 47). Using the muscle hook is a technique the authors found to be helpful in guiding the sickle or beaver blade from the sac fundus to the nasolacrimal duct junction. This ensures that the sac incision is full thickness and follows a proper orientation.
After the initial longitudinal incision has been completed, H-shaped lacrimal sac fl aps are created using vertical incisions on either end of the fi rst cut.
When the lacrimal sacs are cicatrized or diffi cult to delineate, it is dilated with viscoelastic substance in order to facilitate incising through its wall without damaging the nearby common canaliculus.
43 A KERRISON punch, inserted between the nasal mucosa and the maxillary
frontal process, is utilized to create a15 mm x 15 mm osteotomy.
44 Tenting of the sac with a Bowman probe (No. 00).
45 A stab incision is made into the sac using a sickle knife.
46 A Jameson muscle hook is inserted into the lumen of the sac.
47 The muscle hook lifts both the inner mucosa and loose outer covering of the
lacrimal sac, and guides the incising blade from the fundus of the sac to the nasolacrimal duct.
48 Infi ltration of anesthetic solution into the nasal mucosa.
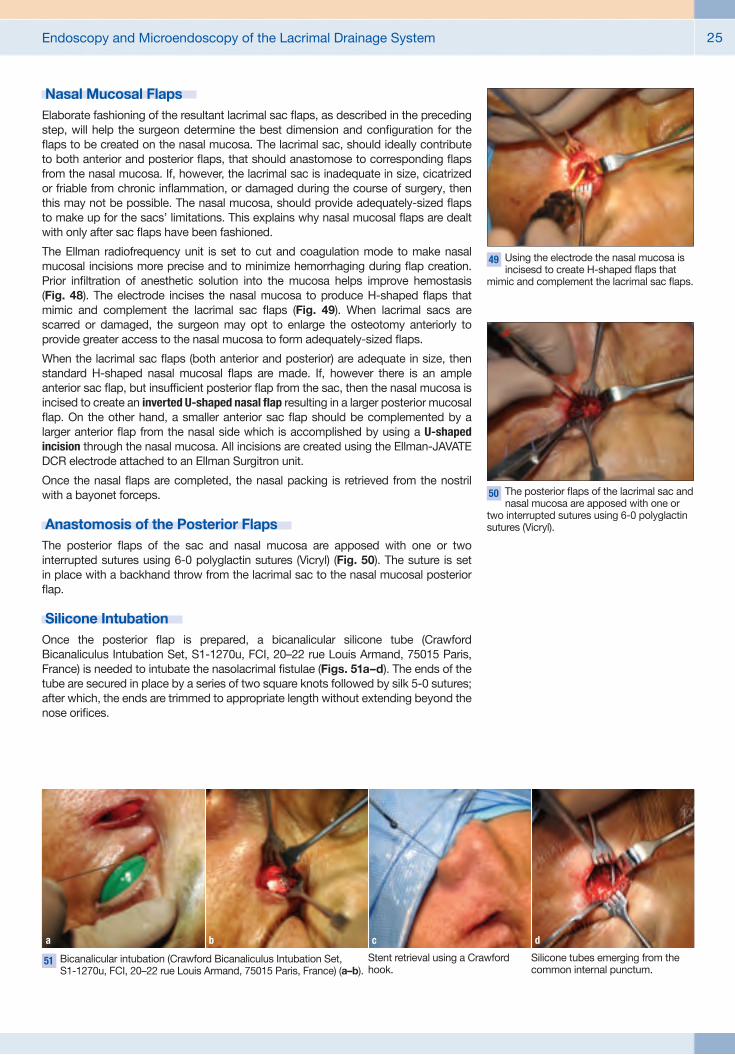
Endoscopy and Microendoscopy of the Lacrimal Drainage System 25
Nasal Mucosal Flaps Elaborate fashioning of the resultant lacrimal sac fl aps, as described in the preceding step, will help the surgeon determine the best dimension and confi guration for the fl aps to be created on the nasal mucosa. The lacrimal sac, should ideally contribute to both anterior and posterior fl aps, that should anastomose to corresponding fl aps from the nasal mucosa. If, however, the lacrimal sac is inadequate in size, cicatrized or friable from chronic infl ammation, or damaged during the course of surgery, then this may not be possible. The nasal mucosa, should provide adequately-sized fl aps to make up for the sacs’ limitations. This explains why nasal mucosal fl aps are dealt with only after sac fl aps have been fashioned.
The Ellman radiofrequency unit is set to cut and coagulation mode to make nasal mucosal incisions more precise and to minimize hemorrhaging during fl ap creation. Prior infi ltration of anesthetic solution into the mucosa helps improve hemostasis (Fig. 48). The electrode incises the nasal mucosa to produce H-shaped fl aps that mimic and complement the lacrimal sac fl aps (Fig. 49). When lacrimal sacs are scarred or damaged, the surgeon may opt to enlarge the osteotomy anteriorly to provide greater access to the nasal mucosa to form adequately-sized fl aps.
When the lacrimal sac fl aps (both anterior and posterior) are adequate in size, then standard H-shaped nasal mucosal fl aps are made. If, however there is an ample anterior sac fl ap, but insuffi cient posterior fl ap from the sac, then the nasal mucosa is incised to create an inverted U-shaped nasal fl ap resulting in a larger posterior mucosal fl ap. On the other hand, a smaller anterior sac fl ap should be complemented by a larger anterior fl ap from the nasal side which is accomplished by using a U-shaped incision through the nasal mucosa. All incisions are created using the Ellman-JAVATE DCR electrode attached to an Ellman Surgitron unit.
Once the nasal fl aps are completed, the nasal packing is retrieved from the nostril with a bayonet forceps.
Anastomosis of the Posterior Flaps The posterior fl aps of the sac and nasal mucosa are apposed with one or two interrupted sutures using 6-0 polyglactin sutures (Vicryl) (Fig. 50). The suture is set in place with a backhand throw from the lacrimal sac to the nasal mucosal posterior fl ap.
Silicone Intubation Once the posterior fl ap is prepared, a bicanalicular silicone tube (Crawford Bicanaliculus Intubation Set, S1-1270u, FCI, 20–22 rue Louis Armand, 75015 Paris, France) is needed to intubate the nasolacrimal fi stulae (Figs. 51a–d). The ends of the tube are secured in place by a series of two square knots followed by silk 5-0 sutures; after which, the ends are trimmed to appropriate length without extending beyond the nose orifi ces.
49 Using the electrode the nasal mucosa is incisesd to create H-shaped fl aps that
mimic and complement the lacrimal sac fl aps.
50 The posterior fl aps of the lacrimal sac and nasal mucosa are apposed with one or
two interrupted sutures using 6-0 polyglactin sutures (Vicryl).
51 Bicanalicular intubation (Crawford Bicanaliculus Intubation Set, S1-1270u, FCI, 20–22 rue Louis Armand, 75015 Paris, France) (a–b).
a
b
Stent retrieval using a Crawford hook.
c
Silicone tubes emerging from the common internal punctum.
d
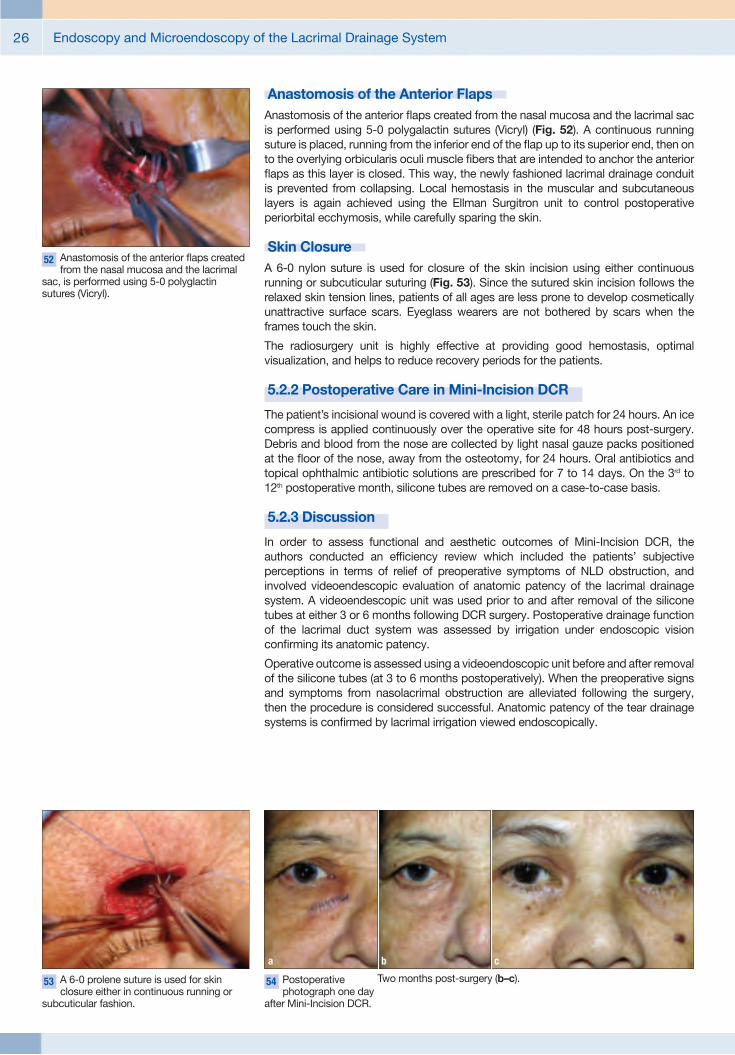
Endoscopy and Microendoscopy of the Lacrimal Drainage System26
Anastomosis of the Anterior Flaps Anastomosis of the anterior fl aps created from the nasal mucosa and the lacrimal sac is performed using 5-0 polygalactin sutures (Vicryl) (Fig. 52). A continuous running suture is placed, running from the inferior end of the fl ap up to its superior end, then on to the overlying orbicularis oculi muscle fi bers that are intended to anchor the anterior fl aps as this layer is closed. This way, the newly fashioned lacrimal drainage conduit is prevented from collapsing. Local hemostasis in the muscular and subcutaneous layers is again achieved using the Ellman Surgitron unit to control postoperative periorbital ecchymosis, while carefully sparing the skin.
Skin Closure A 6-0 nylon suture is used for closure of the skin incision using either continuous running or subcuticular suturing (Fig. 53). Since the sutured skin incision follows the relaxed skin tension lines, patients of all ages are less prone to develop cosmetically unattractive surface scars. Eyeglass wearers are not bothered by scars when the frames touch the skin.
The radiosurgery unit is highly effective at providing good hemostasis, optimal visualization, and helps to reduce recovery periods for the patients.
5.2.2 Postoperative Care in Mini-Incision DCR
The patient’s incisional wound is covered with a light, sterile patch for 24 hours. An ice compress is applied continuously over the operative site for 48 hours post-surgery. Debris and blood from the nose are collected by light nasal gauze packs positioned at the fl oor of the nose, away from the osteotomy, for 24 hours. Oral antibiotics and topical ophthalmic antibiotic solutions are prescribed for 7 to 14 days. On the 3rd to 12th postoperative month, silicone tubes are removed on a case-to-case basis.
5.2.3 Discussion
In order to assess functional and aesthetic outcomes of Mini-Incision DCR, the authors conducted an effi ciency review which included the patients’ subjective perceptions in terms of relief of preoperative symptoms of NLD obstruction, and involved videoendescopic evaluation of anatomic patency of the lacrimal drainage system. A videoendescopic unit was used prior to and after removal of the silicone tubes at either 3 or 6 months following DCR surgery. Postoperative drainage function of the lacrimal duct system was assessed by irrigation under endoscopic vision confi rming its anatomic patency.
Operative outcome is assessed using a videoendoscopic unit before and after removal of the silicone tubes (at 3 to 6 months postoperatively). When the preoperative signs and symptoms from nasolacrimal obstruction are alleviated following the surgery, then the procedure is considered successful. Anatomic patency of the tear drainage systems is confi rmed by lacrimal irrigation viewed endoscopically.
52 Anastomosis of the anterior fl aps created from the nasal mucosa and the lacrimal
sac, is performed using 5-0 polyglactin sutures (Vicryl).
53 A 6-0 prolene suture is used for skin closure either in continuous running or
subcuticular fashion.
54 Postoperative photograph one day
after Mini-Incision DCR.
a
Two months post-surgery (b–c).
b c
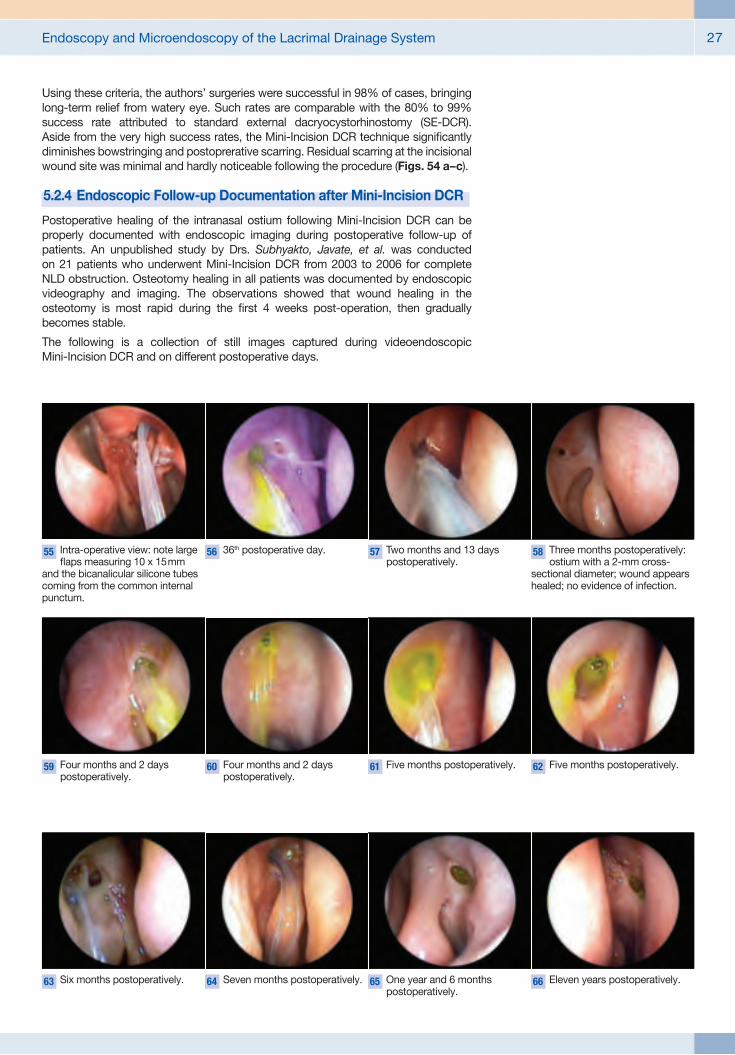
Endoscopy and Microendoscopy of the Lacrimal Drainage System 27
Using these criteria, the authors’ surgeries were successful in 98% of cases, bringing long-term relief from watery eye. Such rates are comparable with the 80% to 99% success rate attributed to standard external dacryocystorhinostomy (SE-DCR). Aside from the very high success rates, the Mini-Incision DCR technique signifi cantly diminishes bowstringing and postoprerative scarring. Residual scarring at the incisional wound site was minimal and hardly noticeable following the procedure (Figs. 54 a–c).
5.2.4 Endoscopic Follow-up Documentation after Mini-Incision DCR
Postoperative healing of the intranasal ostium following Mini-Incision DCR can be properly documented with endoscopic imaging during postoperative follow-up of patients. An unpublished study by Drs. Subhyakto, Javate, et al. was conducted on 21 patients who underwent Mini-Incision DCR from 2003 to 2006 for complete NLD obstruction. Osteotomy healing in all patients was documented by endoscopic videography and imaging. The observations showed that wound healing in the osteo tomy is most rapid during the fi rst 4 weeks post-operation, then gradually becomes stable.
The following is a collection of still images captured during videoendoscopic Mini-Incision DCR and on different postoperative days.
55 Intra-operative view: note large fl aps measuring 10 x 15 mm
and the bicanalicular silicone tubes coming from the common internal punctum.
59 Four months and 2 days postoperatively.
56 36th postoperative day.
60 Four months and 2 days postoperatively.
57 Two months and 13 days postoperatively.
61 Five months postoperatively.
58 Three months postoperatively: ostium with a 2-mm cross-
sectional diameter; wound appears healed; no evidence of infection.
62 Five months postoperatively.
63 Six months postoperatively. 64 Seven months postoperatively. 65 One year and 6 months postoperatively.
66 Eleven years postoperatively.

Endoscopy and Microendoscopy of the Lacrimal Drainage System28
5.3 Endoscopic Lacrimal Duct Recanalization (ELDR)The success of any surgical procedure is considerably improved when the surgeon is able to directly visualize structures within the operative fi eld. Before technological advances in surgery surfaced, the surgeon’s operative perspective was limited to gross anatomy. However, with the emergence of endoscopes, video signal display and recording devices, operative magnifying lenses, and similar instrumentation, surgeons are empowered to better visualize anatomical areas in greater detail and to perform surgical maneuvers that cause minimal trauma to surrounding tissues, targeting only those structures that need to be included in operative treatment.
These innovative developments have given birth to procedures such as balloon angioplasty, and now even lacrimal duct recanalization procedures. The level of diffi culty inherent in these two procedures may be signifi cantly different, and the gravity of their medical indications may be worlds apart. Yet, these seemingly unrelated procedures are similar in their goals to relieve obstructions or to create passages that reroute or bypass obstructions.
Endoscopic dacryoplasty (ELDR using a micro endoscope), a minimally invasive approach to lacrimal system outfl ow problems, is now possible. Lacrimal surgery that addresses the occluded ducts with minimal trauma to surrounding tissues can be performed using miniature telescopes (micro endoscopes). The lacrimal duct is directly visualized by lacrimal endoscopy or dacryo endoscopy, proceeding from the upper lacrimal punctum to the point where the nasolacrimal duct exits in the inferior nasal meatus.
The fi rst applied research in lacrimal system endoscopy was performed by Ebran, Maigret and Bechetoille in 1989. A one-millimeter diameter metal tube catheter was placed within the inferior canaliculus allowing soft fi beroptic endoscopes to be introduced directly into the tubes. Hard and soft endoscopes were tried in both cadavers and then in live DCR patients. Microendoscopy was also described by Kuchar, Novak and colleagues in 1997. They successfully recanalized presaccal stenoses using a fl exible endoscope and an Erbium:YAG laser to address upper, lower and common canalicular stenoses. Emmerich, Luchtenberg and colleagues also performed studies in therapeutic dacryoendoscopy. It was Piffaretti, however, who had a key impact on the development of endoscopic instrumentation for diagnostic and therapeutic applications in lacrimal system problems as early as 1993. In more recent years, Valazzi et al. have stepped up the development of dedicated endoscopic equipment to further refi ne lacrimal microendoscopy. More and more surgeons have taken interest in perfecting the technique.
Described, hereafter, is the technique adapted by Javate et al. in endoscopic dacryoplasty for restoration of lacrimal outfl ow system patency.
5.3.1 Proper Selection of Patients
The endoscopic dacryoplasty procedure detailed below is recommended for recanalizing lacrimal canaliculi or nasolacrimal ducts in:
� Complete or partial primary acquired nasolacrimal duct obstruction (PANDO); and
� Canalicular stenoses.
However, patients with the following conditions are not considered good candidates for the endoscopic technique:
� Presence of bony alteration, such as post-traumatic bony deformity or previous fractures, which can inhibit the recanalization of the nasolacrimal duct;
� Mucocele of the lacrimal sac, because plastic surgery of the sac wall cannot be performed via an endoscopic approach;
� History of acute dacryocystitis or conditions that result in a dilated sac, which has lost its fi broelastic resiliency.
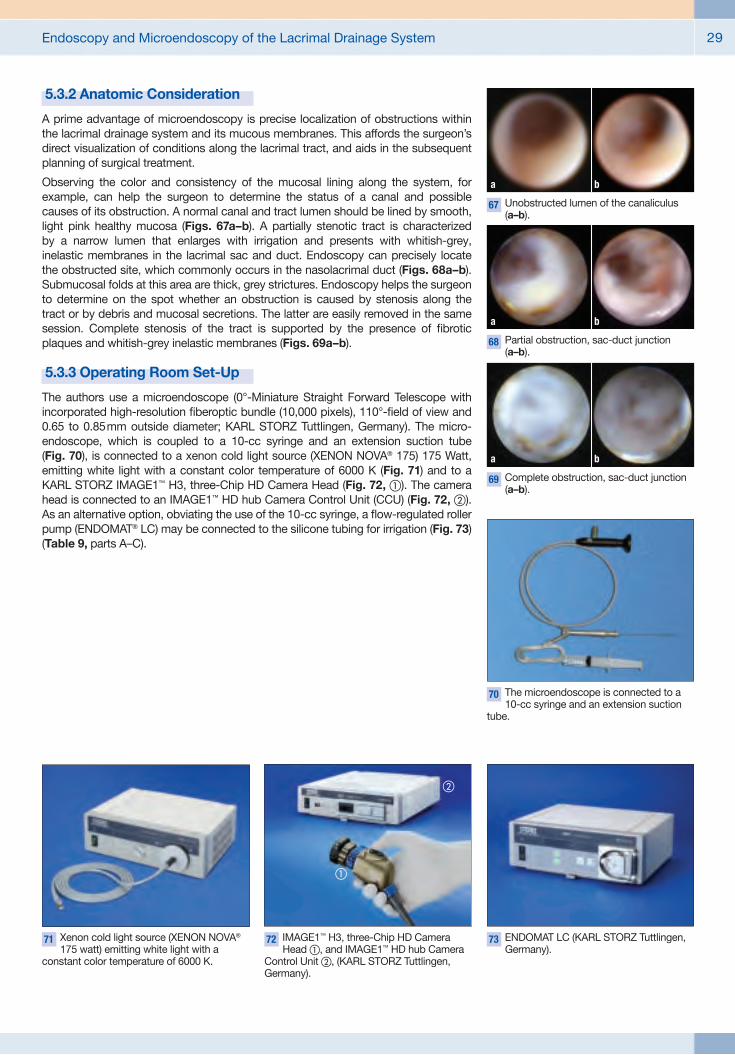
Endoscopy and Microendoscopy of the Lacrimal Drainage System 29
5.3.2 Anatomic Consideration
A prime advantage of microendoscopy is precise localization of obstructions within the lacrimal drainage system and its mucous membranes. This affords the surgeon’s direct visualization of conditions along the lacrimal tract, and aids in the subsequent planning of surgical treatment.
Observing the color and consistency of the mucosal lining along the system, for example, can help the surgeon to determine the status of a canal and possible causes of its obstruction. A normal canal and tract lumen should be lined by smooth, light pink healthy mucosa (Figs. 67a–b). A partially stenotic tract is characterized by a narrow lumen that enlarges with irrigation and presents with whitish-grey, inelastic membranes in the lacrimal sac and duct. Endoscopy can precisely locate the obstructed site, which commonly occurs in the nasolacrimal duct (Figs. 68a–b). Submucosal folds at this area are thick, grey strictures. Endoscopy helps the surgeon to determine on the spot whether an obstruction is caused by stenosis along the tract or by debris and mucosal secretions. The latter are easily removed in the same session. Complete stenosis of the tract is supported by the presence of fi brotic plaques and whitish-grey inelastic membranes (Figs. 69a–b).
5.3.3 Operating Room Set-Up
The authors use a microendoscope (0°-Miniature Straight Forward Telescope with incorporated high-resolution fi beroptic bundle (10,000 pixels), 110°-fi eld of view and 0.65 to 0.85 mm outside diameter; KARL STORZ Tuttlingen, Germany). The micro-endoscope, which is coupled to a 10-cc syringe and an extension suction tube (Fig. 70), is connected to a xenon cold light source (XENON NOVA® 175) 175 Watt, emitting white light with a constant color temperature of 6000 K (Fig. 71) and to a KARL STORZ IMAGE1™ H3, three-Chip HD Camera Head (Fig. 72, �). The camera head is connected to an IMAGE1™ HD hub Camera Control Unit (CCU) (Fig. 72, �). As an alternative option, obviating the use of the 10-cc syringe, a fl ow-regulated roller pump (ENDOMAT® LC) may be connected to the silicone tubing for irrigation (Fig. 73) (Table 9, parts A–C).
67 Unobstructed lumen of the canaliculus (a–b).
a b
68 Partial obstruction, sac-duct junction (a–b).
a b
69 Complete obstruction, sac-duct junction (a–b).
a b
70 The microendoscope is connected to a 10-cc syringe and an extension suction
tube.
71 Xenon cold light source (XENON NOVA® 175 watt) emitting white light with a
constant color temperature of 6000 K.
72 IMAGE1™ H3, three-Chip HD Camera Head �, and IMAGE1™ HD hub Camera
Control Unit �, (KARL STORZ Tuttlingen, Germany).
73 ENDOMAT LC (KARL STORZ Tuttlingen, Germany).
�
�
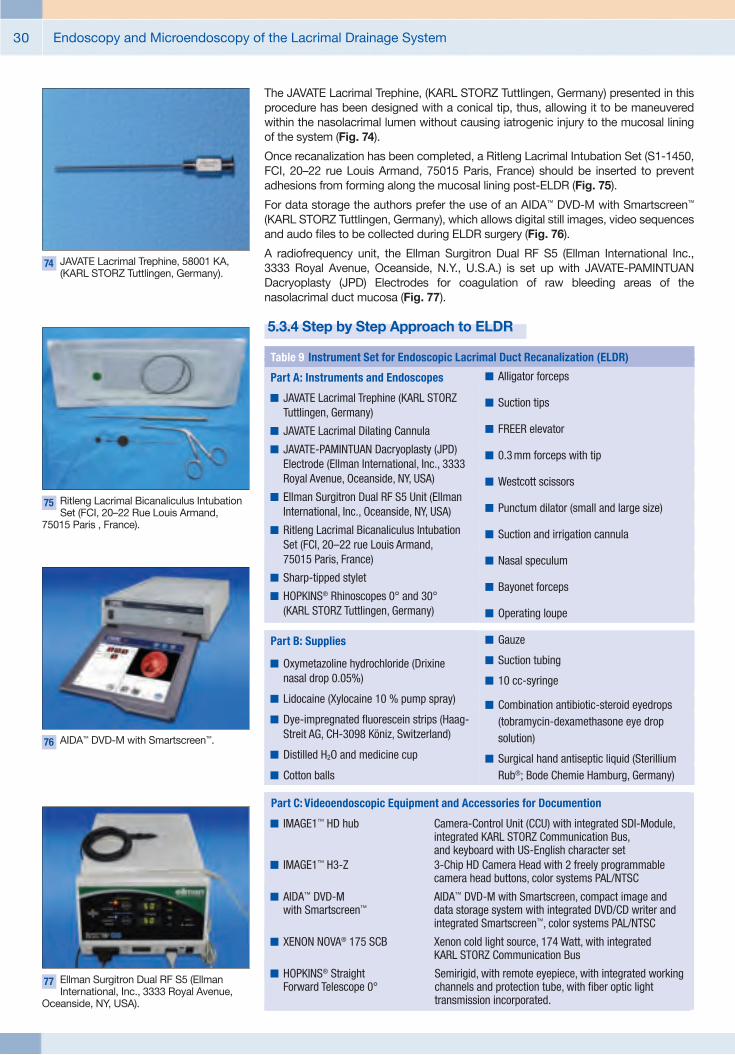
Endoscopy and Microendoscopy of the Lacrimal Drainage System30
The JAVATE Lacrimal Trephine, (KARL STORZ Tuttlingen, Germany) presented in this procedure has been designed with a conical tip, thus, allowing it to be maneuvered within the nasolacrimal lumen without causing iatrogenic injury to the mucosal lining of the system (Fig. 74).
Once recanalization has been completed, a Ritleng Lacrimal Intubation Set (S1-1450, FCI, 20–22 rue Louis Armand, 75015 Paris, France) should be inserted to prevent adhesions from forming along the mucosal lining post-ELDR (Fig. 75).
For data storage the authors prefer the use of an AIDA™ DVD-M with Smartscreen™ (KARL STORZ Tuttlingen, Germany), which allows digital still images, video sequences and audo fi les to be collected during ELDR surgery (Fig. 76).
A radiofrequency unit, the Ellman Surgitron Dual RF S5 (Ellman International Inc., 3333 Royal Avenue, Oceanside, N.Y., U.S.A.) is set up with JAVATE-PAMINTUAN Dacryoplasty (JPD) Electrodes for coagulation of raw bleeding areas of the nasolacrimal duct mucosa (Fig. 77).
5.3.4 Step by Step Approach to ELDR
74 JAVATE Lacrimal Trephine, 58001 KA, (KARL STORZ Tuttlingen, Germany).
75 Ritleng Lacrimal Bicanaliculus Intubation Set (FCI, 20–22 Rue Louis Armand,
75015 Paris , France).
76 AIDA™ DVD-M with Smartscreen™.
77 Ellman Surgitron Dual RF S5 (Ellman International, Inc., 3333 Royal Avenue,
Oceanside, NY, USA).
Table 9 Instrument Set for Endoscopic Lacrimal Duct Recanalization (ELDR)
� Alligator forceps
� Suction tips
� FREER elevator
� 0.3 mm forceps with tip
� Westcott scissors
� Punctum dilator (small and large size)
� Suction and irrigation cannula
� Nasal speculum
� Bayonet forceps
� Operating loupe
� Gauze
� Suction tubing
� 10 cc-syringe
� Combination antibiotic-steroid eyedrops (tobramycin-dexamethasone eye drop solution)
� Surgical hand antiseptic liquid (Sterillium Rub®; Bode Chemie Hamburg, Germany)
Part A: Instruments and Endoscopes
� JAVATE Lacrimal Trephine (KARL STORZ Tuttlingen, Germany)
� JAVATE Lacrimal Dilating Cannula
� JAVATE-PAMINTUAN Dacryoplasty (JPD) Electrode (Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA)
� Ellman Surgitron Dual RF S5 Unit (EllmanInternational, Inc., Oceanside, NY, USA)
� Ritleng Lacrimal Bicanaliculus Intubation Set (FCI, 20–22 rue Louis Armand, 75015 Paris, France)
� Sharp-tipped stylet
� HOPKINS® Rhinoscopes 0° and 30°(KARL STORZ Tuttlingen, Germany)
Part B: Supplies
� Oxymetazoline hydrochloride (Drixine nasal drop 0.05%)
� Lidocaine (Xylocaine 10 % pump spray)
� Dye-impregnated fl uorescein strips (Haag-Streit AG, CH-3098 Köniz, Switzerland)
� Distilled H2O and medicine cup
� Cotton balls
Part C: Videoendoscopic Equipment and Accessories for Documention
� IMAGE1™ HD hub Camera-Control Unit (CCU) with integrated SDI-Module,integrated KARL STORZ Communication Bus,and keyboard with US-English character set
� IMAGE1™ H3-Z 3-Chip HD Camera Head with 2 freely programmable camera head buttons, color systems PAL/NTSC
� AIDA™ DVD-M AIDA™ DVD-M with Smartscreen, compact image andwith Smartscreen™ data storage system with integrated DVD/CD writer and
integrated Smartscreen™, color systems PAL/NTSC
� XENON NOVA® 175 SCB Xenon cold light source, 174 Watt, with integrated KARL STORZ Communication Bus
� HOPKINS® Straight Semirigid, with remote eyepiece, with integrated workingForward Telescope 0° channels and protection tube, with fi ber optic light
transmission incorporated.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 31
ELDR can be performed under local or general anesthesia, depending on patient’s medical status and/or personal preference.
The ipsilateral nostril is packed with cotton pledgets soaked in 0.05% oxymetazoline hydrochloride and sprayed with 10% lidocaine. This induces vasoconstriction of the nasal mucosa (Fig. 78).
Regional nerve-block anesthesia is used. For this purpose, a mixture of lidocaine 2%, epinephrine 1:200,000, and bupivacaine hydrochloride 0.75% solution is prepared and infi ltrated in the medial canthal, anterior ethmoid, and infraorbital areas, as well as in the inferior turbinate (Fig. 79).
Based on the authors’ experience, access to the area where the nasolacrimal duct empties into the inferior meatus is facilitated by infracturing the inferior turbinate medially (Figs. 80a–d) with a FREER elevator under endoscopic visualization with a 30º-HOPKINS® rhinoscope, diameter 4 mm (Fig. 81).
Proparacaine hydrochloride 0.5% solution is instilled into the conjunctival cul-de-sac for ocular surface anesthesia (Fig. 82). The superior lacrimal punctum and canaliculus are expanded using two punctum dilators of increasing calibre (Figs. 83a–b)
78 Nasal packing with cotton pledgets soaked in 0.05% oxymetazoline
hydrochloride.
79 Regional nerve-block anesthesia.
80 Once the rhinoscope has been inserted in the left nostril,
the FREER elevator is introduced.
a
Endoscopic view of the inferior meatus prior to medial infractureof the inferior turbinate using a FREER elevator.
b
During infracture.
c
After infracture.
d
81 30º-HOPKINS® rhinoscope, diameter4 mm (KARL STORZ Tuttlingen, Germany).
82 Proparacaine hydrochloride 0.5% solution is instilled into the conjunctival cul-de-sac
for ocular surface anesthesia.
83 Punctum dilatation using a small-caliber dilator (a) and a large-caliber dilator (b).
a b

Endoscopy and Microendoscopy of the Lacrimal Drainage System32
84 Insertion of JAVATE lacrimal trephine.
85 The microendoscope isintro duced through the lumen
of the trephine.
86 The trephine andmicroendoscope are advanced
horizontally.
87 Endoscopic view of the lumen of the common canaliculus (a–b).
a b
88 Medial wall of the lacrimal sac.
a
Lumen of the lacrimal sac.
b
89 The index fi nger is used to palpate externally the frontal
maxillary process.
90 Whitish fi brous tissue obstruction along the common
canali culus.
91 Whitish fi brous tissueobstruction within the lumen
of the sac.
92 Whitish fi brous tissue obstruction within the lumen
at the sac-duct junction.
93 Endoscopic view throughthe 4-mm HOPKINS®
rhinoscope showing the lacrimal trephine below the vault of the anterior end of the inferior nasal meatus. Whitish fi brous plaque emanates from the lumen of the nasolacrimal duct.
94 Recanalized lumen of the nasolacrimal duct (a–b).
a b

Endoscopy and Microendoscopy of the Lacrimal Drainage System 33
in preparation for insertion of the trephine (Fig. 84). The microendoscope is slowly introduced into the trephine lumen (Fig. 85) and images of the canaliculus are obtained that may be stored on the AIDA™ DVD-M system (Fig. 76). The trephine and micro endoscope are advanced horizontally (Fig. 86) toward the common canaliculus (Figs. 87a–b) and the medial wall of the lacrimal sac (Fig. 88a). The trephine is then rotated to assume a vertical position, allowing the microendoscope to capture images of the lacrimal sac lumen (Fig. 88b). As the trephine, with the microendoscope, passes along the isthmus of the lacrimal sac, the surgeon may use the index fi nger to gently palpate from the external surface of the sac-duct junction for the trephine (Fig. 89). This is usually the point at which the trephine enters the osseus naso lacrimal canal. Throughout the entire downward movement of the trephine- microendoscope, the lumina of the canaliculus, sac and duct are kept dilated by positive pressure from continuous or intermittent fl uid infusion from the 10-cc syringe. A line drawn extern ally, connecting the tear sac and the ala nasi, can serve to guide the surgeon during the course of the trephine’s lateral descent through the nasolacrimal duct until the inferior nasal meatus is reached. Viewing the video images of the microendo-scope as it traverses from punctum to inferior meatus, the surgeon is able to localize any fi brous obstruction along the excretory system (Figs. 90–92). At the same time, the trephine may be utilized to perforate through points of stenoses.
The rigid 4-mm HOPKINS® rhinoscope can be utilized to view the lacrimal trephine below the vault of the anterior end of the inferior nasal meatus (Fig. 93). Next, the micro endoscope is gradually withdrawn to visualize the recanalized nasolacrimal duct (Figs. 94a–b).
The JAVATE-PAMINTUAN lacrimal electrode is connected to the radiofrequency unit (Surgitron Dual RF S5; Ellman International, Inc., 3333 Royal Avenue, Oceanside, NY, USA) which is then inserted into the lumen of the trephine to control bleeding points in coagulation mode (Figs. 95a–b). The micoendoscope is reinserted to assess the outcome of hemostasis and to confi rm that patency of the duct has been reestablished.
A bicanalicular silicone intubation [Ritleng lacrimal intubation set (S1-1450), Ritleng probe (S1-1460), Ritleng endonasal forceps (S1-1470), Ritleng hook (S1-1480); FCI, 20–22 rue Louis Armand, 75015 Paris, France] is inserted to prevent mucosal adhesions from forming (Figs. 96a–b). The ends of the silicone stent are retrieved at the inferior meatus of the nose using the Ritleng hook (Figs. 97a–c). The ends of the silicone tubes are secured with a retinal buckle to prevent the tubes from slipping into the nasolacrimal duct. The tubes stay in place for at least 6 to 12 months.
Steroid eye drops are used to fl ush the nasolacrimal duct mucosa (Fig. 98).
Postoperative photographs one day after ELDR with silicone stent (Figs. 99a–e).
96 Insertion of Ritleng probe (a). Insertion of Ritleng silicone tubes (b).
ba
97 Silicone tubes retrieved using a Ritleng hook (a). Removal of the Ritleng probe (b).
Silicone tubes in place (c).
a
bc
98 Steroid eye drops are administrated to fl ush the nasolacrimal duct mucosa.
95 JAVATE-PAMINTUAN lacrimal electrode (a). Once the JAVATE-PAMINTUAN lacrimal electrode has been connected to the radiofrequency unit (Surgitron Dual RF S5; Ellman
International, Inc., 3333 Royal Avenue, Oceanside, NY, USA), it is inserted into the lumen of the trephine to control bleeding points using the coagulation mode (b).
a b

Endoscopy and Microendoscopy of the Lacrimal Drainage System34
5.3.5 Postoperative Care
Post-ELDR medications include topical antibiotic steroid eye drops instilled every 3 hours and a topical antibiotic ointment applied at bedtime. Debris and blood clots in the lacrimal system are fl ushed out by irrigating the canaliculus on the fi rst postoperative week (Figs. 99a–e). Canalicular irrigation is repeated once a month following surgery to help maintain patency of the tear excretory system. In cases where simple canalicular irrigation results in refl ux, the JAVATE lacrimal dilating cannula (Eagle Labs Company, Rancho Cucamonga, CA, U.S.A.) is passed from the superior punctum to the nasolacrimal duct followed by irrigation to help improve patency (assisted patency) (Fig. 100). Mobilization of the Ritleng stent is also done to dislodge debris and blood clot and to prevent mucosal adhesions from forming.
The following parameters are monitored on a monthly basis to assess the outcome of surgery: subjective relief from preoperative epiphora, positive primary Jones test, patency on irrigation (confi rmation of restored anatomical patency of the lacrimal excretory system), and absence of refl ux on pressure at the lacrimal sac fossa.
This post-ELDR regimen differs from that used for patients who undergo SE-DCR. For the latter patients, continuous application of ice packs over the surgical site for 48 hours; topical antibiotic eye drops are instilled to the ipsilateral eye 4 times a day for 2 months; and the silicone tubes are removed between 3 and 12 months after the operation.
99 Postoperative photographs one day after ELDR with silicone stents (a–e).
a
d
b
e
c
100 Lacrimal dilating cannulas (Eagle Labs Company, Rancho Cucamonga, CA,
U.S.A.).
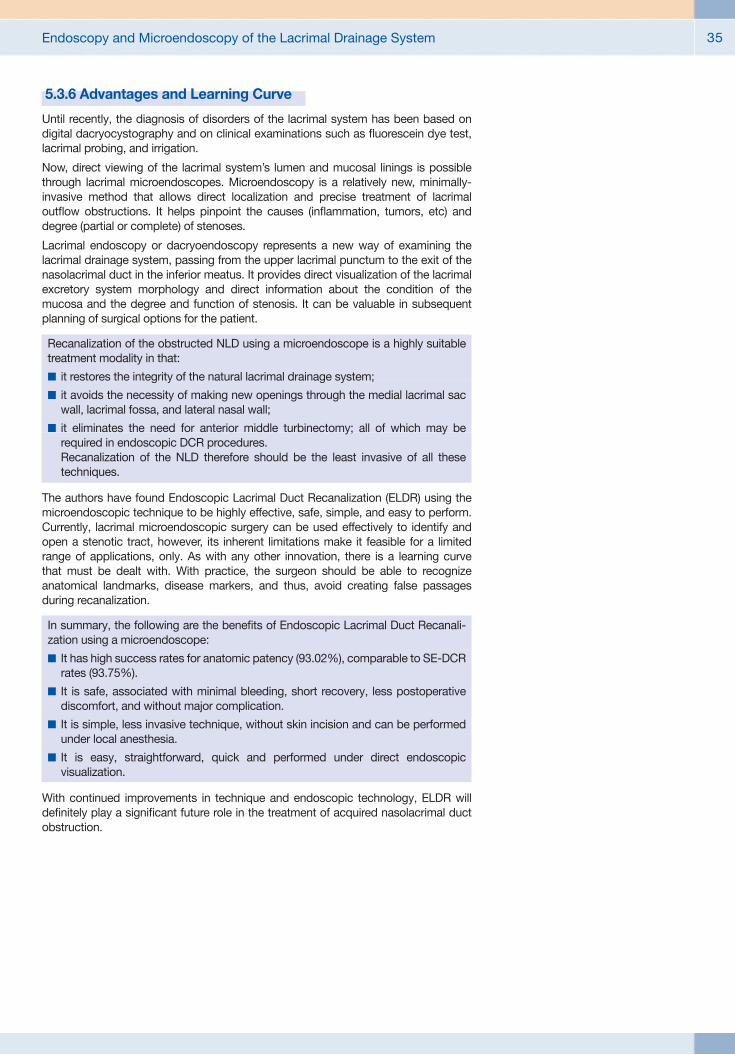
Endoscopy and Microendoscopy of the Lacrimal Drainage System 35
5.3.6 Advantages and Learning Curve
Until recently, the diagnosis of disorders of the lacrimal system has been based on digital dacryocystography and on clinical examinations such as fl uorescein dye test, lacrimal probing, and irrigation.
Now, direct viewing of the lacrimal system’s lumen and mucosal linings is possible through lacrimal microendoscopes. Microendoscopy is a relatively new, minimally-invasive method that allows direct localization and precise treatment of lacrimal outfl ow obstructions. It helps pinpoint the causes (infl ammation, tumors, etc) and degree (partial or complete) of stenoses.
Lacrimal endoscopy or dacryoendoscopy represents a new way of examining the lacrimal drainage system, passing from the upper lacrimal punctum to the exit of the nasolacrimal duct in the inferior meatus. It provides direct visualization of the lacrimal excretory system morphology and direct information about the condition of the mucosa and the degree and function of stenosis. It can be valuable in subsequent planning of surgical options for the patient.
Recanalization of the obstructed NLD using a microendoscope is a highly suitable treatment modality in that:
� it restores the integrity of the natural lacrimal drainage system;
� it avoids the necessity of making new openings through the medial lacrimal sac wall, lacrimal fossa, and lateral nasal wall;
� it eliminates the need for anterior middle turbinectomy; all of which may berequired in endoscopic DCR procedures. Recanalization of the NLD therefore should be the least invasive of all these techniques.
The authors have found Endoscopic Lacrimal Duct Recanalization (ELDR) using the micro endoscopic technique to be highly effective, safe, simple, and easy to perform. Currently, lacrimal microendoscopic surgery can be used effectively to identify and open a stenotic tract, however, its inherent limitations make it feasible for a limited range of applications, only. As with any other innovation, there is a learning curve that must be dealt with. With practice, the surgeon should be able to recognize anatomical landmarks, disease markers, and thus, avoid creating false passages during recanalization.
In summary, the following are the benefi ts of Endoscopic Lacrimal Duct Recanali-zation using a microendoscope:
� It has high success rates for anatomic patency (93.02%), comparable to SE-DCR rates (93.75%).
� It is safe, associated with minimal bleeding, short recovery, less postoperative discomfort, and without major complication.
� It is simple, less invasive technique, without skin incision and can be performed under local anesthesia.
� It is easy, straightforward, quick and performed under direct endoscopic visualization.
With continued improvements in technique and endoscopic technology, ELDR will defi nitely play a signifi cant future role in the treatment of acquired nasolacrimal duct obstruction.

Endoscopy and Microendoscopy of the Lacrimal Drainage System36
5.3.7 Tips and Pitfalls
Lacrimal endoscopy permits surgeons to manage obstructive diseases of the lacrimal drainage system with precision while preserving integrity and normality of surrounding tissues. Precision, however, is not synonymous with ease. Surgeons adept at the procedure will make it look seamless, but the diffi culties attributed to this surgery should not be underestimated.
Initial attempts at dacryoendoscopy may be hampered by unclear video images and disorientation on the part of surgeons and their surgical assistants. Fine tuning of instrument-handling and full awareness of the direction to which the endoscope is advancing, takes time to master. With practice, surgeons eventually learn how to preadjust the microendoscope to correctly display video images on the screen (orientation and focusing) (Fig. 101). Presetting of white balance should provide video images of greater contrast and clarity (Fig. 102).
The major technical diffi culty for beginners is how to keep the probe of the micro endoscope coaxial to the lumen of the canaliculus and sac, otherwise the image disappears from the monitor. Initial diffi culties in handling the instruments, evaluation of the mucous membranes, and diagnosis of pathological changes should decrease with experience as the surgeon becomes more adept at recognizing certain landmarks.
The surgeon also have to be careful to ascertain that he performs all maneuvers with caution and lightness of hand, so as not to create false passages.
To avoid false passage or false route, the lateral descent of the nasolacrimal duct can serve as a guide. Clinically, the lateral divergence of the descending course of the nasolacrimal duct can be estimated by drawing a line between the tear sac and the ala nasi. Individuals with narrow interorbital distances and wide noses will show the greatest lateral divergence along the descending course of the nasolacrimal duct (Fig. 103) while those with wide interorbital distances and narrow noses will exhibit a more vertical divergence of the descending course of the nasolacrimal duct (Fig. 104).
During the procedure, it is also very important to keep in mind that the nasolacrimal duct is angled at approximately 15 degrees in posterior direction, and at 10 degrees in medial direction as the canal descends from the lacrimal fossa to the nose. The latter angle can be clinically estimated by a line drawn between the lacrimal fossa and the fi rst molar tooth.
In some cases, the lacrimal aspect of the nasolacrimal canal is almost completely composed of the maxilla and, in turn, correlated with a decrease in the lacrimal bone and inferior turbinate bone contribution, resulting in a narrowed lumen of the naso lacrimal canal.
In 2007, Shigeta, Takegoshi and Kikuchi published a retrospective study based on the results of standard axial sinus CT scans in 314 patients to determine variations in the bony structure of nasolacrimal canals as to sex and age. Their conclusion pointed to a tendency for chronic infl ammation along the nasolacrimal drainage system pre dominantly observed in females. In this context, females were found to have narrower bony lacrimal canals as well as more acute angles between the bony canal and the nasal fl oor. In females, narrowness of the bony nasolacrimal canal and the acute angle between the bony canal and the nasal fl oor makes them prone to chronic infl ammation of the nasolacrimal drainage system. Their quantitative anatomical study may very well explain the more frequent occurrence of primary acquired NLD obstruction in young female patients as opposed to their male counterparts.
It is possible that increased prevalence of PANDO in female subjects is, at least in part, caused by the smaller diameter of the bony nasolacrimal canal. This smaller lumen could explain higher incidences of tear fl uid stasis and infections extending from the nasal cavity in females who tend to have fl atter bony nasolacrimal canals. This could be attributed to smaller midfacial structures in females.
The lacrimal diaphragm consists of the extension of the orbital periosteum covering the lacrimal fossa to which the lateral wall of the tear sac is fi rmly attached. Into it are inserted the fi bers of both the inferior and superior preseptal orbicularis oculi muscle. Once the diaphragm is pulled laterally, a negative pressure is created in the tear sac. When the pull is released, a positive pressure forms due to the fi broelastic resilience of its wall. In patients with dilated sac, the lacrimal pump mechanism is already impaired because the sac has lost its fi broelastic resiliency.
101 Correct preadjustment of the microendoscope.
102 Presetting of white balance should provide video images of greater contrast
and clarity.
103 Narrow interorbital distances and wide noses demonstrate the greatest lateral
divergence along the descending course of the nasolacrimal duct.
104 Wide interorbital distances and narrow noses exhibit a more parallel, vertical
alignment of the descending course of the nasolacrimal duct.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 37
Based on the authors’ experience, in order to avoid false passage, the inferior turbinate is gently mobilized medially for better visualization of the opening of the nasolacrimal duct prior to endoscopic recanalization. It is very important to keep the examined cavities open throughout the procedure by positive pressure from continuous or intermittent fl uid infusion using a 10-cc syringe. Care should be taken to always align the miniature endoscope coaxial to the canaliculus, sac, and sac-duct junction. It is also very important to visualize the lumen of the canaliculus and the movement of the walls of the lacrimal sac during recanalization. The brightness level of the light source is adjusted throughout the procedure to give better contrast and visualization of the digital images. Follow the lateral descent of the nose externally through the nasolacrimal duct until the inferior nasal meatus is reached. The surgeon should palpate externally for the lacrimal trephine at the sac-duct junction. This is usually the point at which the trephine enters the osseous nasolacrimal canal.
Only minor problems were seen by the authors during the fi rst 10 cases (hematoma or edema of surrounding soft tissues after creating false passages, usually in patients with histories of acute dacryocystitis; due to extravasation of fl uid during irrigation or continuous fl uid injection) which resolved by the fourth postoperative day. No major complications were noted.
5.3.8 Management of Obstructions Proximal to the Lacrimal Sac
Problems related to tear fl ow are generally attributed to the most common type of lacrimal outfl ow obstructions which are usually found at the junction between lacrimal sac and nasolacrimal duct. Next in order of frequency are stenoses within the canalicular segments of the drainage system. Accurate localization is considered a critical factor in the successful treatment of canalicular system blockage. Hurwitz et al. reported on technically more demanding surgeries in patients with obstructions found at less than 8 mm distal to the punctum, compared to stenosis located in the common canaliculus (Figs. 105a–b).
Combined Jones tube-canalicular intubation with conjunctivodacryocysto rhinostomy (CDCR) is still the most utilized surgical approach to surgically manage canalicular obstructions. Tube migration and obstruction, however, has been reported to be as high as 85.4% following CDCR with Jones tube placement (Sekhar, 1991). Alternative surgical options to this procedure include trephination, dilatation with balloon catheter, and laser recanalization. Sisler and Allarakhia reported removal of core obstructive tissues within canaliculi using a mini-trephine followed by stenting. Their results showed patients claiming relief from tearing, either complete or relative, in 83.3% of cases studied.
The use of microendoscopes has made recanalization of canalicular obstruction at this site more manageable. Microendoscopy is even more valuable when a surgeon is faced with obstructions proximal to the sac. While simple trephination may on the one hand be applied effectively in the majority of surgically treated cases, complications related to false passages may occur in some patients following trephination, that is essentially carried out “blindly”. According to the treatment protocol adopted at the author’s institution, the micro endoscope is used as an adjunct to canalicular trephination and silicone stent intubation to treat obstructions within the canalicular system. The author and his team conducted a restrospective review of medical records including patients presenting with epiphora between November 2003 and June 2010 at the University of Santo Tomas Hospital Eye Center, University of Santo Tomas, Manila, Philippines. Patients were labeled as having complete canalicular obstruction if, under local anesthesia, a lacrimal probe (4-0 Bowman probe) failed to be advanced beyond a soft-stop within the canaliculus, or when irrigation past the obtruction was impossible.
Qualifying patients underwent microendoscope-aided canalicular trephination with silicone stent intubation (under local anesthesia) (Fig. 106), with or without sub sequent Endoscopic Lacrimal Duct Recanalization or external dacryocystorhinostomy when concurrent nasolacrimal duct obstruction was eventually established (under general anesthesia).
105 Microendoscopic view of canalicular stenosis (a–b).
a b
106 Offi ce-based procedure performed under local anesthesia in a patient treated for
canali cular stenosis with microendoscopy of the lacrimal drainage system involving bicanaliculus intubation with autostable, self-retaining silicone stents.
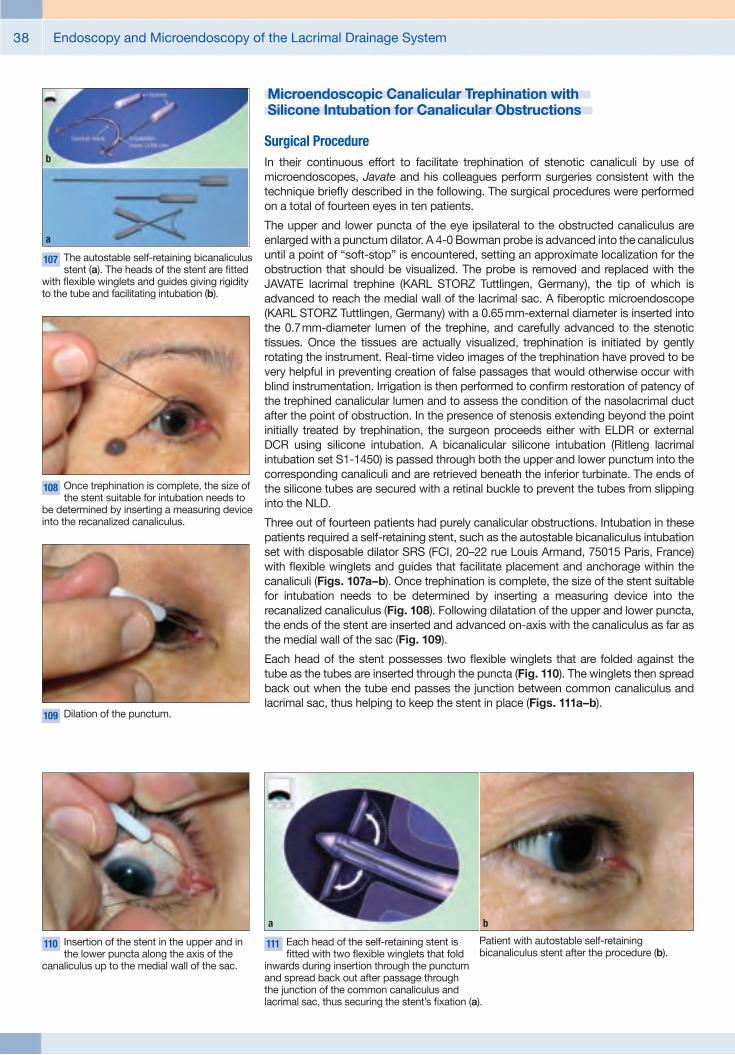
Endoscopy and Microendoscopy of the Lacrimal Drainage System38
Microendoscopic Canalicular Trephination with Silicone Intubation for Canalicular Obstructions
Surgical ProcedureIn their continuous effort to facilitate trephination of stenotic canaliculi by use of microendoscopes, Javate and his colleagues perform surgeries consistent with the technique briefl y described in the following. The surgical procedures were performed on a total of fourteen eyes in ten patients.
The upper and lower puncta of the eye ipsilateral to the obstructed canaliculus are enlarged with a punctum dilator. A 4-0 Bowman probe is advanced into the canaliculus until a point of “soft-stop” is encountered, setting an approximate localization for the obstruction that should be visualized. The probe is removed and replaced with the JAVATE lacrimal trephine (KARL STORZ Tuttlingen, Germany), the tip of which is advanced to reach the medial wall of the lacrimal sac. A fi beroptic microendoscope (KARL STORZ Tuttlingen, Germany) with a 0.65 mm-external diameter is inserted into the 0.7 mm-diameter lumen of the trephine, and carefully advanced to the stenotic tissues. Once the tissues are actually visualized, trephination is initiated by gently rotating the instrument. Real-time video images of the trephination have proved to be very helpful in preventing creation of false passages that would otherwise occur with blind instrumentation. Irrigation is then performed to confi rm restoration of patency of the trephined canalicular lumen and to assess the condition of the nasolacrimal duct after the point of obstruction. In the presence of stenosis extending beyond the point initially treated by trephination, the surgeon proceeds either with ELDR or external DCR using silicone intubation. A bicanalicular silicone intubation (Ritleng lacrimal intubation set S1-1450) is passed through both the upper and lower punctum into the corresponding canaliculi and are retrieved beneath the inferior turbinate. The ends of the silicone tubes are secured with a retinal buckle to prevent the tubes from slipping into the NLD.
Three out of fourteen patients had purely canalicular obstructions. Intubation in these patients required a self-retaining stent, such as the autostable bicanaliculus intubation set with disposable dilator SRS (FCI, 20–22 rue Louis Armand, 75015 Paris, France) with fl exible winglets and guides that facilitate placement and anchorage within the canaliculi (Figs. 107a–b). Once trephination is complete, the size of the stent suitable for intubation needs to be determined by inserting a measuring device into the recanalized canaliculus (Fig. 108). Following dilatation of the upper and lower puncta, the ends of the stent are inserted and advanced on-axis with the canaliculus as far as the medial wall of the sac (Fig. 109).
Each head of the stent possesses two fl exible winglets that are folded against the tube as the tubes are inserted through the puncta (Fig. 110). The winglets then spread back out when the tube end passes the junction between common canaliculus and lacrimal sac, thus helping to keep the stent in place (Figs. 111a–b).
107 The autostable self-retaining bicanaliculus stent (a). The heads of the stent are fi tted
with fl exible winglets and guides giving rigidity to the tube and facilitating intubation (b).
b
a
108 Once trephination is complete, the size of the stent suitable for intubation needs to
be determined by inserting a measuring device into the recanalized canaliculus.
109 Dilation of the punctum.
110 Insertion of the stent in the upper and in the lower puncta along the axis of the
canaliculus up to the medial wall of the sac.
111 Each head of the self-retaining stent is fi tted with two fl exible winglets that fold
inwards during insertion through the punctum and spread back out after passage throughthe junction of the common canaliculus and lacrimal sac, thus securing the stent’s fi xation (a).
a
Patient with autostable self-retaining bicanaliculus stent after the procedure (b).
b

Endoscopy and Microendoscopy of the Lacrimal Drainage System 39
Follow-up and ResultsStents were removed after 3 to 14 (average of 8.7) months. Relief from epiphora was assessed in each patient based on the guidelines set forth by the Royal College of Ophthalmologists. The manifestation of epiphora symptoms is categorized in three levels: absence, improvement, or no change. In their series, Javate et al. noted a 93% complete remission of epiphora (13 out of 14 eyes). Only one patient claimed no change in his tearing symptoms. These success rates are comparable to those of the time-tested approach to canalicular obstructions, CDCR, which has been reported to succeed in 57 to 100% of surgical cases.
The authors hold the opinion that microendoscopy-aided trephination of canalicular obstructions is a procedure that must be highly considered as an alternative to standard CDCR or simple blind trephination. They also mentioned that self-retaining bicanalicular stenting is adequate for intubation in cases where obstruction is confi ned to the canalicular system. It facilitates microendoscopic trephination as an outpatient surgical procedure for purely canalicular stenoses under local anesthesia.
5.3.9 Videoendoscopic Images of the Lacrimal Excretory System
Microendoscopy performed during lacrimal system surgery furnishes the surgeon with actual images of the tissue morphology, lumen patency, and mucosal conditions. The surgeon, thus, has direct knowledge on the presence or absence of anatomical obstruction, as well as degree and function of any stenosis.
Normal Lacrimal Drainage System The following endoscopic photos exemplify a normal, unobstructed lacrimal excretory system. The widely patent lumina of the canaliculus, common canaliculus, lacrimal sac, and nasolacrimal duct are evident. The entire system demonstrates the characteristics of a healthy mucosa: smooth, light pink, mobile during irrigation (Fig. 112).
Sac and Lacrimal Duct before and after ELDR
Partial Obstruction Partial stenosis along the lacrimal drainage tract presents with narrowed lumina that enlarge with irrigation. The lining mucosa usually show whitish-grey inelastic membranes. The photographs on the right show dramatic changes in the pre-and post-ELDR conditions of the tract in patients treated with ELDR for partial obstructions in the lacrimal sac and NLD (Fig. 113). Following surgery, the recanalized sac and NLD again present with wide, patent lumina.
Microendoscopy allows for visual intra-operative evidence of pathologic change such as mucosal strictures and scarring. Mucosal infl ammatory changes, like mucosal folds, are easily visualized and differentiated from partial obstructions. Stenoses are, likewise, differentiated form debris and mucosal secretions which can be easily removed.
Complete ObstructionComplete stenosis presents with fi brotic plaques and whitish-grey, ineslastic membranes (Fig. 114). With microendoscopy, the precise location of stenosis is identifi ed, commonly in the nasolacrimal duct. Stenoses, heralded by whitish-grey, inelastic membranes, whether in the canaliculus, lacrimal sac or nasolacrimal duct, are treated surgically. These are differentiated from mucosal folds that present as thick, grey strictures.
The images also show the widely patent lumen of a recanalized NLD following ELDR.
112 Endoscopic images captured in different segments of the normal lacrimal excretory
system.
113 Partial Obstruction: before and after ELDR.
114 Complete Obstruction: before and after ELDR.

Endoscopy and Microendoscopy of the Lacrimal Drainage System40
References
1. AIMINO G, DAVI G. Principles of Radiofrequency in Oculoplastics. Oculoplast Surg Radiofrequency 1999; 1:13–22
2. BALDESCHI L, NOLST TRENITÉ GJ, HINTSCHICH C et al. The intranasal ostium after external dacryocystorhinostomy and the internal opening of the lacrimal canaliculi. Orbit 2000;19:81–86
3. BARTLEY GB, NICHOLS WL. Hemorrhage associated with dacryocystorhinostomyand the adjunctive use of decompressinin selected patients. Ophthalmology 1991;98:1864–1866
4. BECKER BB. Recanalization of the obstructed nasolacrimal duct system. J Vasc Intern Radiol 2001;12:697–699
5. CALDWELL GW. A new operation for the radical cure of obstruction of the nasal duct. N Y Med J 1893;58:476
6. CARTER SR, GAUSAS RE. Gender and Racial Variations of the Lacrimal System. In:Cohen AJ, Mercandetti M, Brazzo BG, eds. The Lacrimal System Diagnosis, Management and Surgery. New York, NY: Springer, 2006:21–24
7. DUFFY MT. Advances in lacrimal surgery.Curr Opin Ophthalmol 2000;11:352–356
8. DUTTON FJ, WHITE JJ. Imaging and Clinical Evaluation of the Lacrimal Drainage System. In: Cohen AJ, Mercandetti M, Brazzo BG, eds. The Lacrimal System Diagnosis, Management and Surgery. New York, NY: Springer, 2006:74–95
9. EBRAN JM, MAIGRET Y, BECHETOILLE A.Lacrimal ducts microendoscopy Technique and fi rst views. Acta Endoscopica 1989; 19 (2): 115–122
10. FEIN W, DAYKHOVSKY L, PAPAIOANNOU T,et al. Endoscopy of the lacrimal outfl owsystem. Arch Ophthalmol 1992;110:1748–1750
11. GROESSL SA, SIRES BS, LEMKE BN.An anatomical basis for primary acquired nasolacrimal duct obstruction. Arch Ophthalmol 1997; 115:71–74
12. GUPTA PJ. Radiofrequency surgery: offering a novel approach to ano-rectal diseases. Middle East Journal of Family Medicine, 2005; Vol.3(1)
13. HÄUSLER R, CAVERSACCIO M. Microsurgical Endonasal Dacryocystorhinostomy with Long-term Insertion of Bicanalicular Silicone Tubes. Arch Otolaryngol Head Neck Surg 1998;124:188–191
14. HEJAR SS, JONES NS, SADIQ SA et al. Endoscopic Holmium:Yag laserdacryocystorhinostomy – safe and effective as a day-case procedure.J Laryngol Otol 1997;111:1056–1059
15. ILGIT ET, YÜKSEL D, ÜNAL M, et al. Transluminal balloon dilatation of the lacrimal drainage system for the treatment of epiphora. Am J Roentgenol 1995;165:517–1524
16. JAVATE RM, CAMPOMANES BS JR, CO ND,et al. The endoscope and the radiofrequency unit in DCR surgery. Ophthal Plast Reconstr Surg 1995;11:54–58
17. JAVATE RM, PAMINTUAN FG. Endoscopic Radiofrequency-Assisted Dacryocystorhino-stomy and the Griffi ths Collar Button. Oper Techn Oculoplast Orbital Reconstr Surg 1998;1(2):73–80
18. JAVATE RM, PAMINTUAN FG. Endoscopic Radiofrequency-Assisted Dacryocystorhino-stomy with Double Stent: A Personal Experience. Orbit 2005;24:15–22
19. JAVATE RM, PAMINTUAN FP, CRUZ RT. Effi cacy of Endoscopic Lacrimal DuctRe canalization Using Microendoscope. Ophthal Plast Reconstr Surg 2010;26:330–333
20. JAVATE RM, PAMINTUAN FG, LAPID-LIM SI.New waves in dacryocystorhinostomy. In: Aimino G, Davi G, Santella M, eds.Oculoplastic Surgery With Radiofrequency. Milano: Editor Full Image, 1999: 99–104.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 41
21. JAVATE RM, PAMINTUAN FG, LAPID-LIM SI. Radiofrequency dacryocystorhinostomy.In: Cohen AJ, Mercandetti M, Brazzo BG, eds.The Lacrimal System Diagnosis, Manage ment and Surgery. New York, NY: Springer, 2006:212–222
22. JAVATE RM, SYJUCO MA, LAPID-LIM SI. Refi nements in surgical technique of extern al dacryocystorhinostomy. Oper Techn Oculo plastic Orbital Reconstr Surg 1998;1(2):49–57
23. JAVATE RM, SYJUCO MA, LAPID-LIM SI. Sutureless Dacryocystorhinostomy Surgery. Oper Techn Oculoplastic Orbital Reconstr Surg 1998;1(2):93–97
24. KUCHAR A, NOVAK P, PIEH S et al.Endoscopic laser recanalisation of presaccal canalicular obstruction. Br J Ophthalmol 1999; 83:443–447
25. MAIER M, SCHMIDT T, SCHMIDT M.Endoscopically controlled surgery with the micro–drill and intubation of the lacrimal ducts. Ophthalmologe 2000;97:870–873
26. O’CONNOR JL, BLOOM DA. WILLIAM T.Bovie and electrosurgery. Surgery 1996;119(4):390–396
27. OLDER JJ. The value of radiosurgery in oculoplastics.Ophthalmic Plast Reconstr Surg 2002;18(3):214–218
28. PFENNINGER JL, DEWITT DE. Radiofrequency Surgery (Modern Electrosurgery). In: Pfenniger JL, Fowler GC, eds. Pfenninger and Fowler’s Procedures for Primary Care, 2nd ed. Philadelphia, PA: Mosby, 2003:213–224
29. ROSE GE. The lacrimal paradox: toward a greater success in lacrimal surgery. Ophthal Plast Reconstr Surg 2004:20(4):262-265
30. SEKHAR GC, DORTZBACH RK, GONNERING RSet al. Problems associated with conjunctivodacryocystorhinostomy. Am J Ophthalmol 1991;112:502–6
31. SHIGETA K, TAKEGOSHI H, KIKUCHI S. Sex and age differences in the boy nasolacrimal canal: an anatomical study. Arch Ophthalmol Dec 2007; 125 (12): 1677–1681
32. SHUN-SHIN GA, THURAIRAJAN G. External dacryocystorhinostomy – an end of an era? Br J Ophthalmol. 1997;81:716–717
33. SISLER HA, ALLARAKHIA L. New minitrephine makes lacrimal canalicular rehabilitation an offi ce procedure. Ophthal Plast Reconstr Surg 1990;6:203–206
34. SNELL RS. Clinical Anatomy by Regions8th ed. Baltimore, MD; Lippincott Williams& Wilkins, 2008.
35. SONG HY, AHN HS, PARK CK et al. Complete obstruction of the nasolacrimal system.Part II. Treatment with expandable metallic stents. Radiology 1993;186:372–376
36. SUNG RJ, LAUER MR. Fundamental Approaches to the Management of cardiac arrhythmias. Kluwer Academic Publishers, 2000
37. TOTI A. Nuovo metodo conservatore di cura radicale delle suppuratzioni croniche del sacco lacrimale (dacriocistorhinostomia).Clin Mod 1904;10:33–34
38. TSIRBAS A, DAVIS G, WORMALD PJ.Mechanical endonasal dacryocystorhinos-tomy versus external dacryocystorhinostomy. Ophthal Plast Reconstr Surg 2004;20:50–56
39. VOGT K . Radiofrequency Surgery in Otorhinolaryngology. Endo-Press®, Tuttlingen, Germany, 2009
40. WOBIG JL, DAILEY RA. Anatomy of the Lacrimal System. In: Wobig JL, Dailey RA, eds. Oculofacial Plastic Surgery: Face, Lacrimal System, and Orbit. New York, NY: Thieme, 2004:129 –137
41. XIANG N, HU W, YUAN J et al. Diagnosis and therapy of lacrimal system diseases by micro lacrimal endoscope. Front Med China 2009;3(1):113–117
42. YAZICI B, YAZICI Z. Final nasolacrimal ostium after external dacryocystorhinostomy.Arch Ophthalmol 2003;121:76–80
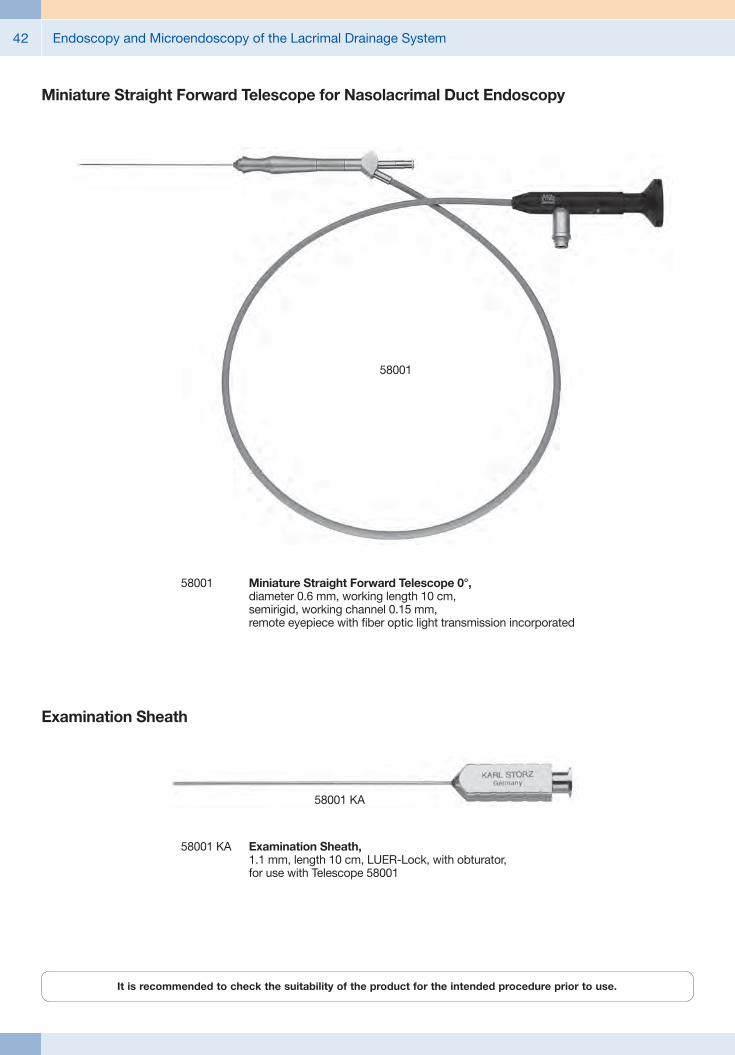
Endoscopy and Microendoscopy of the Lacrimal Drainage System42
58001 Miniature Straight Forward Telescope 0°, diameter 0.6 mm, working length 10 cm, semirigid, working channel 0.15 mm, remote eyepiece with fiber optic light transmission incorporated
58001
Miniature Straight Forward Telescope for Nasolacrimal Duct Endoscopy
58001 KA
58001 KA Examination Sheath, 1.1 mm, length 10 cm, LUER-Lock, with obturator, for use with Telescope 58001
Examination Sheath
It is recommended to check the suitability of the product for the intended procedure prior to use.
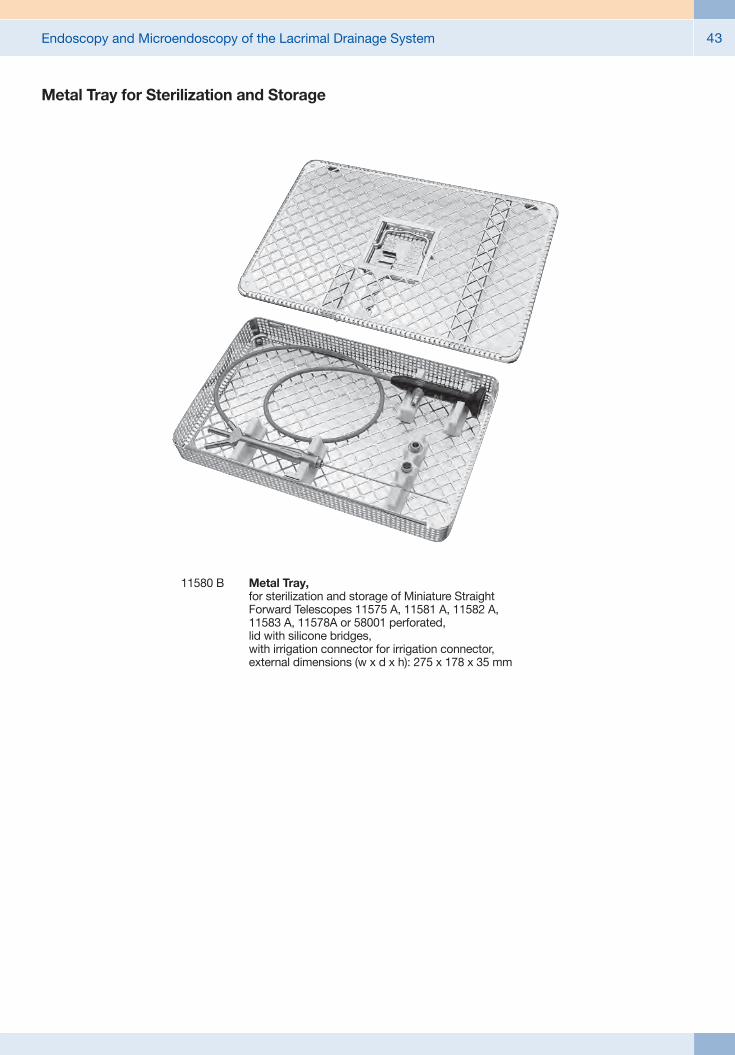
Endoscopy and Microendoscopy of the Lacrimal Drainage System 43
11580 B Metal Tray, for sterilization and storage of Miniature Straight Forward Telescopes 11575 A, 11581 A, 11582 A, 11583 A, 11578A or 58001 perforated, lid with silicone bridges, with irrigation connector for irrigation connector, external dimensions (w x d x h): 275 x 178 x 35 mm
Metal Tray for Sterilization and Storage

Endoscopy and Microendoscopy of the Lacrimal Drainage System44
20 2120 40 / 20 2121 40
20 2120 40 PAL TELECAM 20 2121 40 NTSC One-Chip Camera Head
color system PAL, autoclavable, soakable, gas-sterilizable, with integrated Parfocal Zoom Lens, f = 14 – 28 mm (2x), 2 freely programmable camera head buttons, including plastic container 39301 ACT for sterilization
Natural illumination## LED high-performance light source
## Natural colour rendition close to sunlight with a colour temperature of 6400 K
## Up to 30,000 hours lamp operating time
Ordering InformationTP100 EN TELE PACK X LED, endoscopic video
unit for use with all KARL STORZ TELECAM one-chip camera heads and video endoscopes, incl. LED-light source on a similar niveau as the Power LED 175, with integrated digital Image Processing Module, 15" LCD monitor with LED backlight, USB/SD memory module, color systems PAL/NTSC, power supply 100 - 240 VAC, 50/60 Hz,
including: USB Silicone Keyboard
with Touchpad, with US character set
Unique benefits of the KARL STORZ TELE PACK X LED at a glance
Flexible storage possibilities## SD card-slot allows high storage capacity
## USB-slot for external HDDs and flash drives
## Picture gallery for records
## Playback of saved videos
## Print-ready patient report documentation
Crystal clear image## 15" LCD monitor with LED backlight
## Rotatable image display
## 24 Bit color intensity for natural color rendition
## DVI video input for pristine picture quality
## DVI video output for connecting HD monitors
Easy control combined with highest safety## Membrane keyboard approved for wipe disinfection
## Hot-Keys assuring fast and direct adjustment
## Arrow keys for intuitive control
## Pedal control available
Additional information## Sturdy, portable casing
## Ergonomic design allows comfortable transport ## Universal power supply unit: 100 – 240 VAC, 50/60 Hz
## Measurement (H x W x D): 450 mm x 350 mm x 150 mm
## Weight: 7 kg
n

Endoscopy and Microendoscopy of the Lacrimal Drainage System 45
Innovative Design## Dashboard: Complete overview with intuitive menu guidance
## Live menu: User-friendly and customizable## Intelligent icons: Graphic representation changes when settings of connected devices or the entire system are adjusted
## Automatic light source control## Side-by-side view: Parallel display of standard image and the Visualization mode
## Multiple source control: IMAGE1 S allows the simultaneous display, processing and documentation of image information from two connected image sources, e.g., for hybrid operations
Dashboard Live menu
Side-by-side view: Parallel display of standard image and Visualization mode
Intelligent icons
Economical and future-proof## Modular concept for flexible, rigid and 3D endoscopy as well as new technologies
## Forward and backward compatibility with video endoscopes and FULL HD camera heads
## Sustainable investment## Compatible with all light sources
IMAGE1 S Camera System n
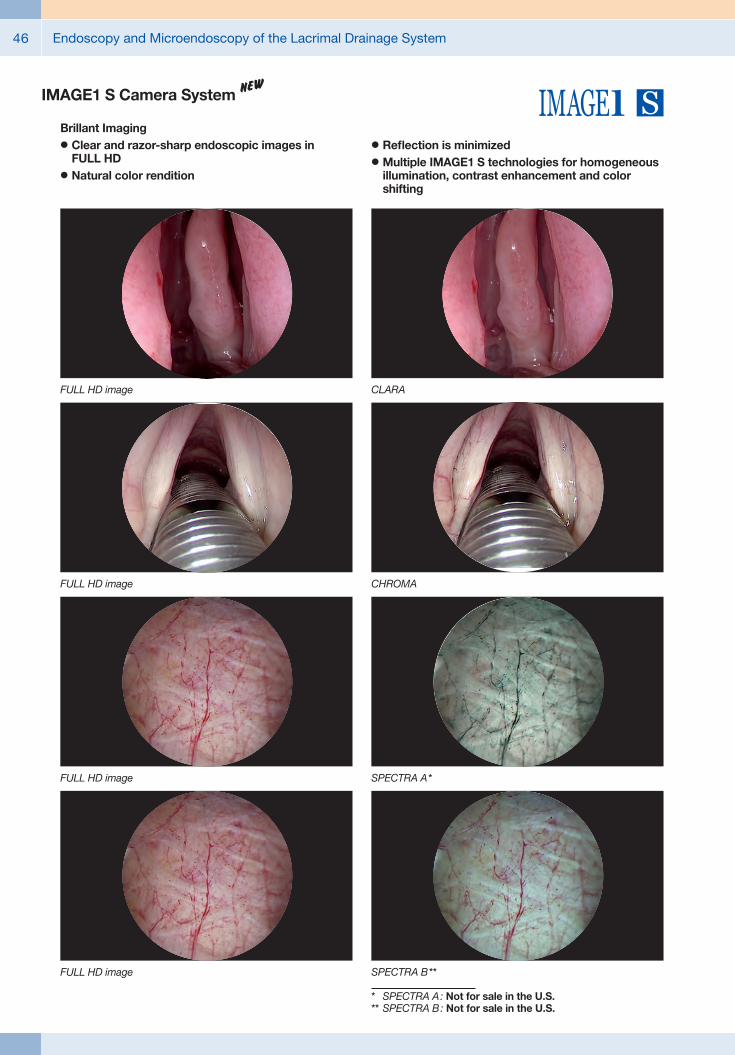
Endoscopy and Microendoscopy of the Lacrimal Drainage System46
Brillant Imaging## Clear and razor-sharp endoscopic images in FULL HD
## Natural color rendition
## Reflection is minimized## Multiple IMAGE1 S technologies for homogeneous illumination, contrast enhancement and color shifting
FULL HD image CHROMA
FULL HD image SPECTRA A *
FULL HD image
FULL HD image CLARA
SPECTRA B **
* SPECTRA A : Not for sale in the U.S.** SPECTRA B : Not for sale in the U.S.
IMAGE1 S Camera System n
Endoscopy and Microendoscopy of the Lacrimal Drainage System 47
TC 200EN* IMAGE1 S CONNECT, connect module, for use with up to 3 link modules, resolution 1920 x 1080 pixels, with integrated KARL STORZ-SCB and digital Image Processing Module, power supply 100 – 120 VAC/200 – 240 VAC, 50/60 Hz
including: Mains Cord, length 300 cm DVI-D Connecting Cable, length 300 cm SCB Connecting Cable, length 100 cm USB Flash Drive, 32 GB, USB silicone keyboard, with touchpad, US
* Available in the following languages: DE, ES, FR, IT, PT, RU
Specifications:
HD video outputs
Format signal outputs
LINK video inputs
USB interface SCB interface
- 2x DVI-D - 1x 3G-SDI
1920 x 1080p, 50/60 Hz
3x
4x USB, (2x front, 2x rear) 2x 6-pin mini-DIN
100 – 120 VAC/200 – 240 VAC
50/60 Hz
I, CF-Defib
305 x 54 x 320 mm
2.1 kg
Power supply
Power frequency
Protection class
Dimensions w x h x d
Weight
TC 300 IMAGE1 S H3-LINK, link module, for use with IMAGE1 FULL HD three-chip camera heads, power supply 100 – 120 VAC/200 – 240 VAC, 50/60 Hz, for use with IMAGE1 S CONNECT TC 200ENincluding:Mains Cord, length 300 cm
Link Cable, length 20 cm
For use with IMAGE1 S IMAGE1 S CONNECT Module TC 200EN
IMAGE1 S Camera System n
TC 300 (H3-Link)
TH 100, TH 101, TH 102, TH 103, TH 104, TH 106 (fully compatible with IMAGE1 S) 22 2200 55-3, 22 2200 56-3, 22 2200 53-3, 22 2200 60-3, 22 2200 61-3, 22 2200 54-3, 22 2200 85-3 (compatible without IMAGE1 S technologies CLARA, CHROMA, SPECTRA*)
1x
100 – 120 VAC/200 – 240 VAC
50/60 Hz
I, CF-Defib
305 x 54 x 320 mm
1.86 kg
Camera System
Supported camera heads/video endoscopes
LINK video outputs
Power supply
Power frequency
Protection class
Dimensions w x h x d
Weight
Specifications:
TC 200EN
TC 300
* SPECTRA A : Not for sale in the U.S.** SPECTRA B : Not for sale in the U.S.

Endoscopy and Microendoscopy of the Lacrimal Drainage System48
TH 104
TH 104 IMAGE1 S H3-ZA Three-Chip FULL HD Camera Head, 50/60 Hz, IMAGE1 S compatible, autoclavable, progressive scan, soakable, gas- and plasma-sterilizable, with integrated Parfocal Zoom Lens, focal length f = 15 – 31 mm (2x), 2 freely programmable camera head buttons, for use with IMAGE1 S and IMAGE 1 HUB™ HD/HD
IMAGE1 FULL HD Camera Heads
Product no.
Image sensor
Dimensions w x h x d
Weight
Optical interface
Min. sensitivity
Grip mechanism
Cable
Cable length
IMAGE1 S H3-ZA
TH 104
3x 1/3" CCD chip
39 x 49 x 100 mm
299 g
integrated Parfocal Zoom Lens, f = 15 – 31 mm (2x)
F 1.4/1.17 Lux
standard eyepiece adaptor
non-detachable
300 cm
Specifications:
For use with IMAGE1 S Camera System IMAGE1 S CONNECT Module TC 200EN, IMAGE1 S H3-LINK Module TC 300 and with all IMAGE 1 HUB™ HD Camera Control Units
TH 100 IMAGE1 S H3-Z Three-Chip FULL HD Camera Head, 50/60 Hz, IMAGE1 S compatible, progressive scan, soakable, gas- and plasma-sterilizable, with integrated Parfocal Zoom Lens, focal length f = 15 – 31 mm (2x), 2 freely programmable camera head buttons, for use with IMAGE1 S and IMAGE 1 HUB™ HD/HD
IMAGE1 FULL HD Camera Heads
Product no.
Image sensor
Dimensions w x h x d
Weight
Optical interface
Min. sensitivity
Grip mechanism
Cable
Cable length
IMAGE1 S H3-Z
TH 100
3x 1/3" CCD chip
39 x 49 x 114 mm
270 g
integrated Parfocal Zoom Lens, f = 15 – 31 mm (2x)
F 1.4/1.17 Lux
standard eyepiece adaptor
non-detachable
300 cm
Specifications:
IMAGE1 S Camera Heads n
TH 100

Endoscopy and Microendoscopy of the Lacrimal Drainage System 49
9826 NB
9826 NB 26" FULL HD Monitor, wall-mounted with VESA 100 adaption, color systems PAL/NTSC, max. screen resolution 1920 x 1080, image fomat 16:9, power supply 100 – 240 VAC, 50/60 Hzincluding:External 24 VDC Power SupplyMains Cord
9619 NB
9619 NB 19" HD Monitor, color systems PAL/NTSC, max. screen resolution 1280 x 1024, image format 4:3, power supply 100 – 240 VAC, 50/60 Hz, wall-mounted with VESA 100 adaption,including:
External 24 VDC Power SupplyMains Cord
Monitors
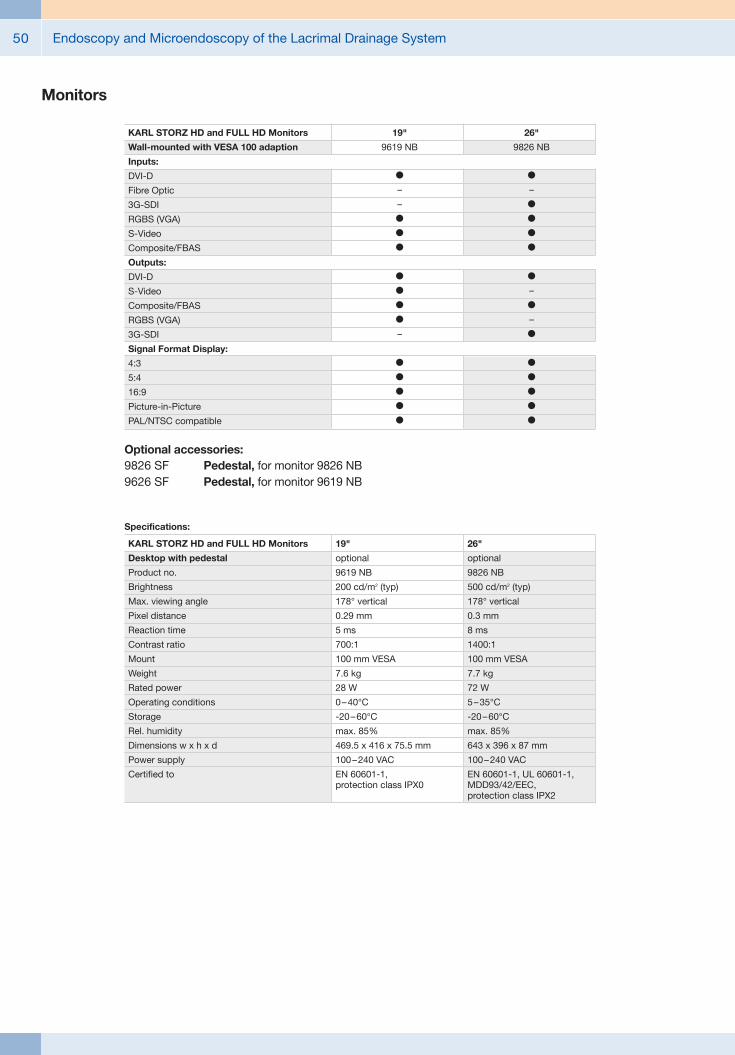
Endoscopy and Microendoscopy of the Lacrimal Drainage System50
Monitors
Optional accessories:9826 SF Pedestal, for monitor 9826 NB9626 SF Pedestal, for monitor 9619 NB
26"
9826 NB
l
–
l
l
l
l
l
–
l
–
l
l
l
l
l
l
19"
9619 NB
l
–
–
l
l
l
l
l
l
l
–
l
l
l
l
l
KARL STORZ HD and FULL HD Monitors
Wall-mounted with VESA 100 adaption
Inputs:
DVI-D
Fibre Optic
3G-SDI
RGBS (VGA)
S-Video
Composite/FBAS
Outputs:
DVI-D
S-Video
Composite/FBAS
RGBS (VGA)
3G-SDI
Signal Format Display:
4:3
5:4
16:9
Picture-in-Picture
PAL/NTSC compatible
19"
optional
9619 NB
200 cd/m2 (typ)
178° vertical
0.29 mm
5 ms
700:1
100 mm VESA
7.6 kg
28 W
0 – 40°C
-20 – 60°C
max. 85%
469.5 x 416 x 75.5 mm
100 – 240 VAC
EN 60601-1, protection class IPX0
Specifications:
KARL STORZ HD and FULL HD Monitors
Desktop with pedestal
Product no.
Brightness
Max. viewing angle
Pixel distance
Reaction time
Contrast ratio
Mount
Weight
Rated power
Operating conditions
Storage
Rel. humidity
Dimensions w x h x d
Power supply
Certified to
26"
optional
9826 NB
500 cd/m2 (typ)
178° vertical
0.3 mm
8 ms
1400:1
100 mm VESA
7.7 kg
72 W
5 – 35°C
-20 – 60°C
max. 85%
643 x 396 x 87 mm
100 – 240 VAC
EN 60601-1, UL 60601-1, MDD93/42/EEC, protection class IPX2
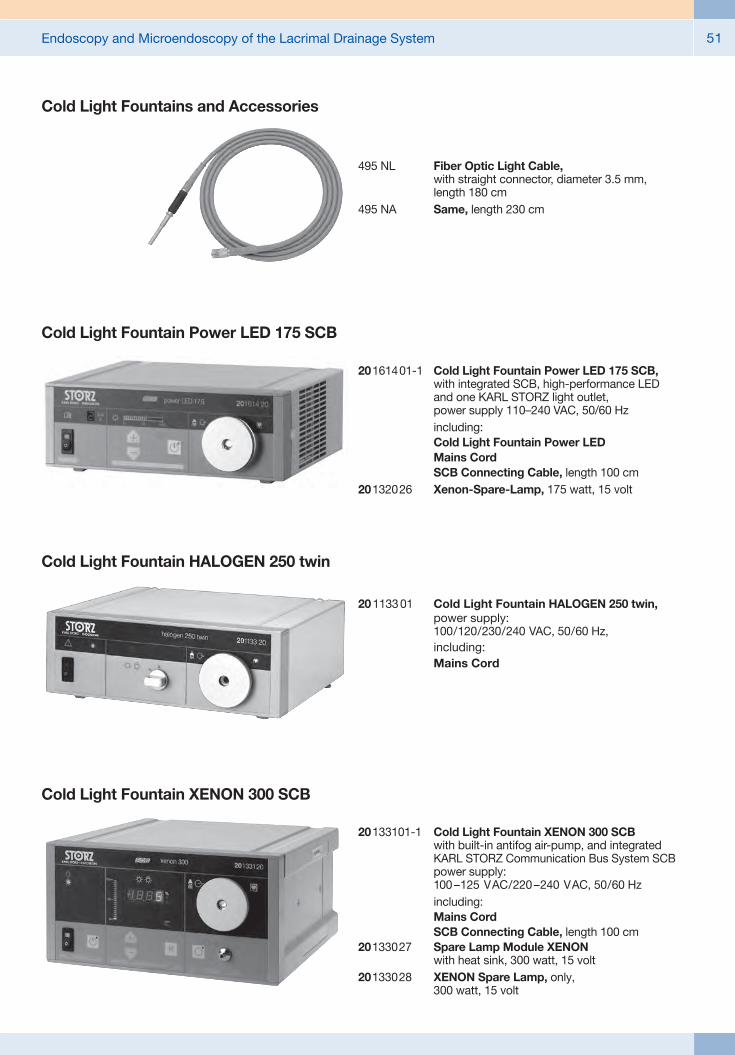
Endoscopy and Microendoscopy of the Lacrimal Drainage System 51
Cold Light Fountains and Accessories
495 NL Fiber Optic Light Cable, with straight connector, diameter 3.5 mm, length 180 cm
495 NA Same, length 230 cm
20 1133 01 Cold Light Fountain HALOGEN 250 twin, power supply: 100/120/230/240 VAC, 50/60 Hz,
including: Mains Cord
Cold Light Fountain HALOGEN 250 twin
20 1614 01-1 Cold Light Fountain Power LED 175 SCB, with integrated SCB, high-performance LED and one KARL STORZ light outlet, power supply 110–240 VAC, 50/60 Hz
including: Cold Light Fountain Power LED Mains Cord SCB Connecting Cable, length 100 cm20 1320 26 Xenon-Spare-Lamp, 175 watt, 15 volt
Cold Light Fountain Power LED 175 SCB
Cold Light Fountain XENON 300 SCB
20 133101-1 Cold Light Fountain XENON 300 SCB
with built-in antifog air-pump, and integrated KARL STORZ Communication Bus System SCB power supply: 100 –125 VAC/220 –240 VAC, 50/60 Hz
including: Mains Cord SCB Connecting Cable, length 100 cm20133027 Spare Lamp Module XENON
with heat sink, 300 watt, 15 volt20133028 XENON Spare Lamp, only,
300 watt, 15 volt

Endoscopy and Microendoscopy of the Lacrimal Drainage System52
Data Management and DocumentationKARL STORZ AIDA® – Exceptional documentation
The name AIDA stands for the comprehensive implementation of all documentation requirements arising in surgical procedures: A tailored solution that flexibly adapts to the needs of every specialty and thereby allows for the greatest degree of customization.
This customization is achieved in accordance with existing clinical standards to guarantee a reliable and safe solution. Proven functionalities merge with the latest trends and developments in medicine to create a fully new documentation experience – AIDA.
AIDA seamlessly integrates into existing infrastructures and exchanges data with other systems using common standard interfaces.
WD 200-XX* AIDA Documentation System, for recording still images and videos, dual channel up to FULL HD, 2D/3D, power supply 100-240 VAC, 50/60 Hz
including: USB Silicone Keyboard, with touchpad ACC Connecting Cable DVI Connecting Cable, length 200 cm HDMI-DVI Cable, length 200 cm Mains Cord, length 300 cm
WD 250-XX* AIDA Documentation System, for recording still images and videos, dual channel up to FULL HD, 2D/3D, including SMARTSCREEN® (touch screen), power supply 100-240 VAC, 50/60 Hz
including: USB Silicone Keyboard, with touchpad ACC Connecting Cable DVI Connecting Cable, length 200 cm HDMI-DVI Cable, length 200 cm Mains Cord, length 300 cm
*XX Please indicate the relevant country code (DE, EN, ES, FR, IT, PT, RU) when placing your order.

Endoscopy and Microendoscopy of the Lacrimal Drainage System 53
Workflow-oriented use
Patient
Entering patient data has never been this easy. AIDA seamlessly integrates into the existing infrastructure such as HIS and PACS. Data can be entered manually or via a DICOM worklist. ll important patient information is just a click away.
Checklist
Central administration and documentation of time-out. The checklist simplifies the documentation of all critical steps in accordance with clinical standards. All checklists can be adapted to individual needs for sustainably increasing patient safety.
Record
High-quality documentation, with still images and videos being recorded in FULL HD and 3D. The Dual Capture function allows for the parallel (synchronous or independent) recording of two sources. All recorded media can be marked for further processing with just one click.
Edit
With the Edit module, simple adjustments to recorded still images and videos can be very rapidly completed. Recordings can be quickly optimized and then directly placed in the report. In addition, freeze frames can be cut out of videos and edited and saved. Existing markings from the Record module can be used for quick selection.
Complete
Completing a procedure has never been easier. AIDA offers a large selection of storage locations. The data exported to each storage location can be defined. The Intelligent Export Manager (IEM) then carries out the export in the background. To prevent data loss, the system keeps the data until they have been successfully exported.
Reference
All important patient information is always available and easy to access. Completed procedures including all information, still images, videos, and the checklist report can be easily retrieved from the Reference module.
Endoscopy and Microendoscopy of the Lacrimal Drainage System54
UG 540 Monitor Swifel Arm, height and side adjustable, can be turned to the left or the right side, swivel range 180°, overhang 780 mm, overhang from centre 1170 mm, load capacity max. 15 kg, with monitor fixation VESA 5/100, for usage with equipment carts UG xxx
UG 540
Equipment Cart
UG 220
UG 220 Equipment Cart wide, high, rides on 4 antistatic dual wheels equipped with locking brakes 3 shelves, mains switch on top cover, central beam with integrated electrical subdistributors with 12 sockets, holder for power supplies, potential earth connectors and cable winding on the outside,
Dimensions: Equipment cart: 830 x 1474 x 730 mm (w x h x d), shelf: 630 x 510 mm (w x d), caster diameter: 150 mm
inluding: Base module equipment cart, wide Cover equipment, equipment cart wide Beam package equipment, equipment cart high 3x Shelf, wide Drawer unit with lock, wide 2x Equipment rail, long Camera holder

Endoscopy and Microendoscopy of the Lacrimal Drainage System 55
Recommended Accessories for Equipment Cart
UG 310 Isolation Transformer, 200 V – 240 V; 2000 VA with 3 special mains socket, expulsion fuses, 3 grounding plugs, dimensions: 330 x 90 x 495 mm (w x h x d), for usage with equipment carts UG xxx
UG 310
UG 410 Earth Leakage Monitor, 200 V – 240 V, for mounting at equipment cart, control panel dimensions: 44 x 80 x 29 mm (w x h x d), for usage with isolation transformer UG 310
UG 410
UG 510 Monitor Holding Arm, height adjustable, inclinable, mountable on left or right, turning radius approx. 320°, overhang 530 mm, load capacity max. 15 kg, monitor fixation VESA 75/100, for usage with equipment carts UG xxx
UG 510
Endoscopy and Microendoscopy of the Lacrimal Drainage System56
Special features:## Luminous field can be focused – adjustable from 20 to 80 mm at a working distance of 40 cm – resulting in brightness of over 175,000 lux
## Double lens system provides outstanding illumination in the depths of the operating field
## Precise delineation and no luminous field color margins
## Homogeneous illumination of the luminous field without shadows
## Newly designed, lightweight headband provides improved comfort, also suitable for a small head size, can be adjusted both horizontally and vertically
## Sterilizable handle allows adjustment under sterile conditions, moveable and height adjustable
## Light cable is divided in the head area, ensuring even distribution of weight
## Extremely robust and flexible light cable due to special protective casing
## Convenient light cable length of 290 cm provides greater freedom of movement
310060 Headlight KS60, with double lens system and Y-fiber optic light cable, >175,000 lux, illuminated area adjustable from 20 – 80 mm in diameter with 40 cm working distance
including: Headlight KS60, with removeable and sterilizable Focus Handle 310065 Headband, fully adjustable, with Forehead Cushion 078511,
with cross band, including holder for Headlight 310060/310063 Y-Fiber Optic Light Cable, with special protective casing for
Headlight 310063, length 290 cm Clip with Band, for attaching the fiber optic light cable to OR clothing
310060 / 310061
310061 Same, including: Headlight KS60 Headband Y-Fiber Optic Light Cable, with special protective casing for
Headlight 310063, with 90º deflection to the light source, length 290 cm Clip with Band
Headlight KS60with Cold Light Illumination

Endoscopy and Microendoscopy of the Lacrimal Drainage System 57
Notes:

Endoscopy and Microendoscopy of the Lacrimal Drainage System58
Notes:

with the compliments of
KARL STORZ — ENDOSKOPE