endometriosis & cancer association yong... · endometriosis & cancer association paul yong,...
TRANSCRIPT
Endometriosis & Cancer Association
Paul Yong, MD, PhD, FRCSC Gynaecologist, VGH/UBC Hospital and BC Women’s Hospital Assistant Professor, UBC Dept of Obstetrics & Gynaecology Research Director, Centre for Pelvic Pain and Endometriosis
Member, Ovarian Cancer Research team (OVCARE)
Disclosures
• None

Learning objectives
• Identify the epidemiology and classification of endometriosis
• State the impact of atypical endometriosis on malignant gynecologic tumours
• Discuss potential ways to prevent future ovarian cancer in women with endometriosis

Learning objectives
• Identify the epidemiology and classification of endometriosis
• State the impact of atypical endometriosis on malignant gynecologic tumours
• Discuss potential ways to prevent future ovarian cancer in women with endometriosis
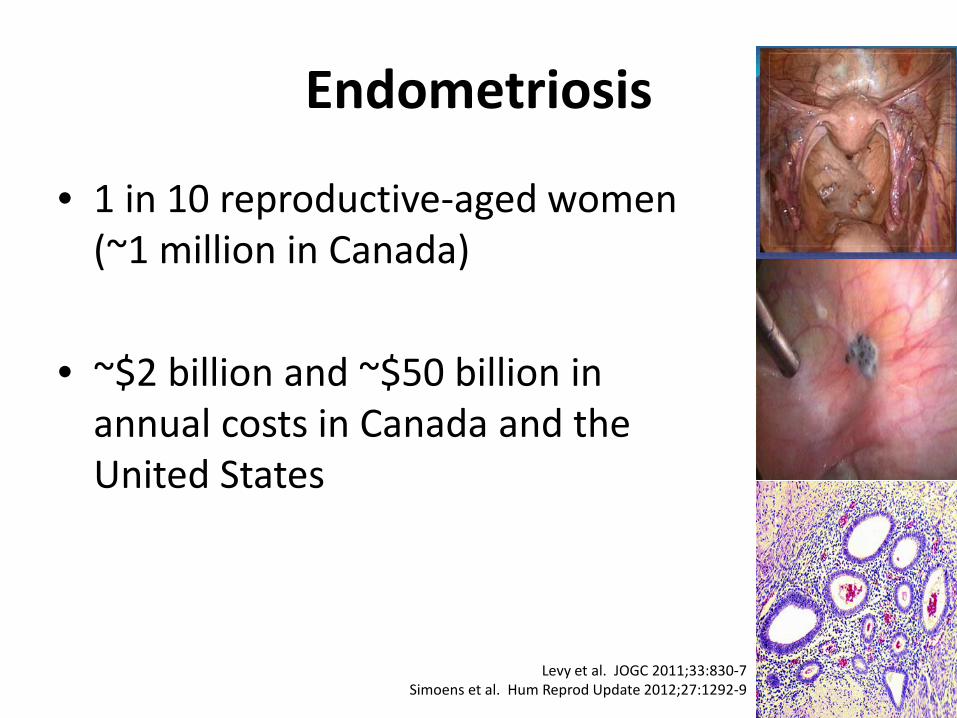
Endometriosis
• 1 in 10 reproductive-aged women (~1 million in Canada)
• ~$2 billion and ~$50 billion in annual costs in Canada and the United States
Levy et al. JOGC 2011;33:830-7 Simoens et al. Hum Reprod Update 2012;27:1292-9

Endometriosis
• Definition: – Uterine endometrial tissue, present
ectopically elsewhere in the pelvis (or elsewhere)
• Etiology
– Retrograde menstruation/Immune – Metaplasia – Blood/lymphatic dissemination
www.bcwomens.ca
Levy et al. JOGC 2011;33:830-7 Simoens et al. Hum Reprod Update 2012;27:1292-9
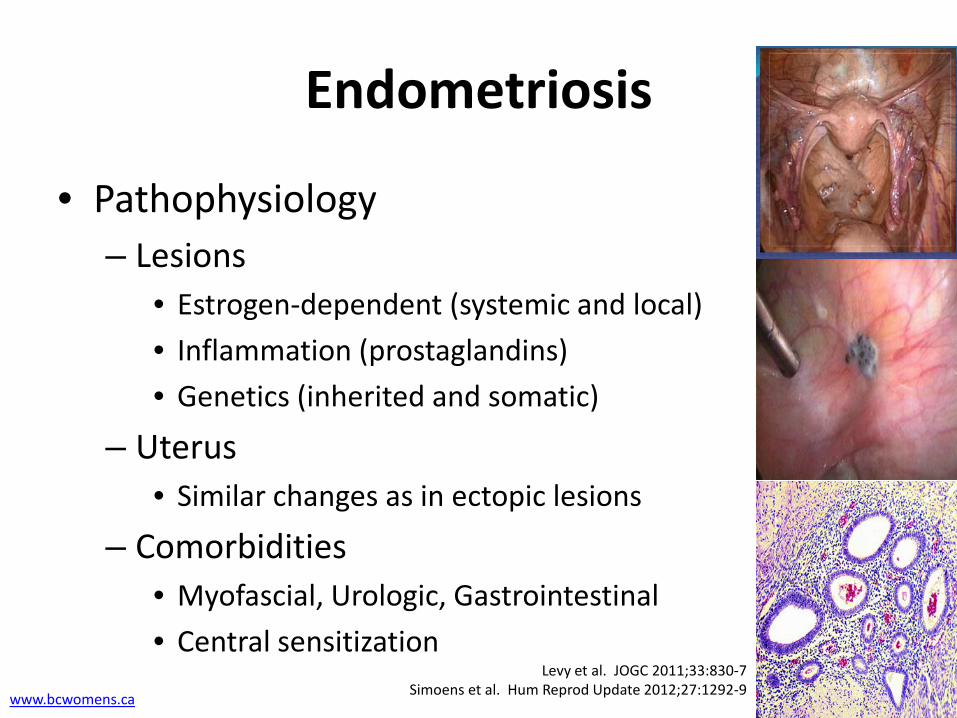
Endometriosis
• Pathophysiology – Lesions
• Estrogen-dependent (systemic and local) • Inflammation (prostaglandins) • Genetics (inherited and somatic)
– Uterus • Similar changes as in ectopic lesions
– Comorbidities • Myofascial, Urologic, Gastrointestinal • Central sensitization
www.bcwomens.ca
Levy et al. JOGC 2011;33:830-7 Simoens et al. Hum Reprod Update 2012;27:1292-9

Symptoms
• Pelvic pain – Menstrual cramps – Painful intercourse (deep) – Painful bowel movements – Cyclical or chronic pelvic pain
• Infertility • Asymptomatic

Classification
• Anatomic subtype: – Superficial – Ovarian – Deep
• Stage
– I/II: minimal-mild – III/IV: moderate-severe

Superficial endometriosis
• Superficially attached to peritoneum
• Classically pigmented • Can have other appearances
– Red – White – Increased vascularity

Ovarian endometriomas
• Chocolate cysts
• Virtually pathognomonic at ultrasound and surgery

Deep endometriosis
• Invasive > 5mm
• Forms “nodules”
• Can “obliterate” the pouch of Douglas

American Society of Reproductive Medicine: Surgical staging of endometriosis
13 1 If the fimbriated end of the fallopian tube is completely enclosed, change the point assignment to 16. Staging: Stage I (minimal): 1-5; stage II (mild): 6-15; stage III (moderate): 16-40; stage IV (severe): >40. Revised ASRM Classification. Fertil Steril 1997; 67: 819.
ENDOMETRIOSIS <1 cm 1-3 cm >3 cm
Peritoneum Superficial 1 2 4
Deep 2 4 6
Ovary Right Superficial 1 2 4
Deep 4 16 20
Left superficial 1 2 4
Deep 4 16 20
POSTERIOR CUL-DE-SAC OBLITERATION Partial Complete
4 40
ADHESIONS <1/3 Enclosure
1/3 - 2/3 Enclosure
>2/3 Enclosure
Ovary R Filmy 1 2 4
Dense 4 8 16
L filmy 1 2 4
Dense 4 8 16
Tube R Filmy 1 2 4
Dense 41 81 16
L Filmy 1 2 4
Dense 41 81 16

American Society of Reproductive Medicine: Surgical staging of endometriosis
Scoring system for Stages: Poorly correlated to symptoms (and malignancy?)
14 Revised ASRM Classification. Fertil Steril 1997; 67: 819.
Stage Description Scoring Range Stage I minimal 1-5 Stage II mild 6-15 Stage III moderate 16-40 Stage IV severe >40

Diagnosis
• Can be suspected based on history and exam – Symptoms and/or infertility – Tenderness on pelvic exam
• Diagnosis made by surgery and pathology; or – Nodularity on pelvic examination – Routine or specialized ultrasound – MRI
• CA-125 can be elevated; but not a diagnostic or screening tool

Treatment
• Hormonal – NSAID – Estrogen-progestin contraceptive – Progestin (dienogest, norethindrone) – Progestin IUD (treatment efficacy can be < 5 yrs) – GnRH agonists
• Surgical (laparoscopic) – Conservative: ablation or excision – Definitive: hysterectomy +/- BSO

Learning objectives
• Identify the epidemiology and classification of endometriosis
• State the impact of atypical endometriosis on malignant gynecologic tumours
• Discuss potential ways to prevent future ovarian cancer in women with endometriosis

Other clinical implications
• Extra-pelvic endometriosis (e.g. thoracic) • Pregnancy complications (e.g. placenta related) • Autoimmune disease (e.g. MS) • Coronary heart disease • Cancer
– Ovarian: higher – Endometrial and breast: equivocal – Cervical: lower

What’s the risk of ovarian CA?
• Risk estimates for endometriosis and ovarian CA

Ovarian CA subtypes
• Endometriosis is a risk factor for clear cell and endometrioid (and low-grade serous?)

Atypical endometriosis
• Observation of histologically atypical endometriosis contiguous with ovarian CA – Crowding of cells – Increase of nuclear/cytoplasmic ratio
• NOTE: Other meanings of “atypical” endometriosis – “Atypical” ovarian endometriomas on ultrasound – “Atypical” appearance at laparoscopy
Anglesio and Yong, Clin Obstet Gynecol, in press
Atypical endometriosis
• Genomic evidence that atypical endometriosis is the precursor to endometrioid/clear cell ovarian CA: – Shared regions of loss-of-heterozygosity – Shared ARID1A mutations (Weigand et al., NEJM) – Shared up to 98% of somatic mutations (Anglesio
et al., J Path) • Suggests that endometriosis can accumulate
somatic mutations and become atypical, and eventually transform to ovarian CA
Anglesio and Yong, Clin Obstet Gynecol, in press

However…
• Deep endometriosis can also harbour somatic mutations (Anglesio et al., NEJM)
• But extremely rare for deep endometriosis to become atypical and undergo malignant transformation
• Thus, there must be role of ovarian micro-environment
Anglesio and Yong, Clin Obstet Gynecol, in press
Learning objectives
• Identify the epidemiology and classification of endometriosis
• State the impact of atypical endometriosis on malignant gynecologic tumours
• Discuss potential ways to prevent future ovarian cancer in women with endometriosis

What’s the risk of ovarian CA?
• Endometriosis: approx 2 fold increase in risk – May be higher with tissue confirmed ovarian
endometriosis compared to self-reported history
• However, this is average risk and likely to be heterogeneous – e.g. estrogen exposure
• Goal: Identifying the endometriosis patient who is at higher risk for ovarian CA.
Crux of the problem
• Endometriosis Common Time?
• Atypical endometriosis Uncommon Time?
• Clear cell or endometrioid ovarian CA

Gyne oncologist
• What the gyne oncologist is likely to see – Concurrent endometriosis found in 30-40% of
clear cell ovarian cancer – Atypical endometriosis can be seen in this context – Sometimes a continuum is seen consisting of
endometriosis, atypical endometriosis, and frank carcinoma
General gynecologist or family physician
• What we’re more likely to see – Patient with benign ovarian endometrioma 1) What’s the risk of ovarian CA? 2) How can we prevent and who’s at higher risk?
– Atypical endometriosis found on pathology, in
what looked like a benign endometrioma 1) How frequent is this finding? 2) How to manage?

General gynecologist or family physician
• What we’re trying to avoid – Published case report – Age 24: MIS left ovarian cystectomy
endometrioma – Age 29: MIS right ovarian cystectomy
endometrioma with atypical endometriosis – Age 33: MIS bilateral ovarian cystectomies
right endometrioid ovarian CA

General gynecologist or family physician
• What we’re more likely to see – Patient with benign ovarian endometrioma 1) What’s the risk of ovarian CA? 2) How can we prevent and who’s at higher risk?
– Atypical endometriosis found on pathology, in
what looked like a benign endometrioma 1) How frequent is this finding? 2) How to manage?

How can we prevent ovarian CA?
• Factors that may reduce risk: – Hormonal therapy
• Combined oral contraceptives (dose response) • Progestin • Progestin IUD
– Parity (vs. nulliparity or infertility) – Tubal ligation (salpingectomy); Hysterectomy – Oophorectomy and complete surgical removal of
endometriosis

Who’s at higher risk of ovarian CA?
• Examples of women with endometriosis who may be at higher risk for ovarian CA:
• Problem: we don’t know which of our patients are at genetic risk quintile 4-5
*

Case 1
• 50 year old perimenopausal G0 with symptomatic left sided 5 cm endometrioma – Hypertension, Smoker – BMI 40 – Previous laparotomy, left ovarian cystectomy – No previous tubal ligation
• CA-125: 100 • Exam: evidence of Stage IV endometriosis

Case 1
• Management:
• Surveillance until menopause?
• Try hormonal therapy, and surveillance?
• Surgery (oophorectomy)?
Case 1
• Surveillance until menopause? – Advantages
• Avoid surgical risk
– Disadvantages • Will endometrioma resolve, and if so, how long will it
take? • If endometrioma no longer apparent on ultrasound, is
it truly resolved or is there still endometriosis in the ovary that could become atypical?

Case 1
• Hormonal therapy, with surveillance? – Advantages
• Improvement in symptoms and reduce size of cyst • Chemoprevention
– Disadvantages • Clot risk (if combined estrogen-progestin) • If endometrioma no longer apparent on ultrasound, is
it truly resolved or is there still endometriosis in the ovary that could become atypical?

Case 1
• Surgery? (oophorectomy, removal of endometriosis, +/- hysterectomy and bilateral salpingectomy) – Advantages
• Tissue diagnosis • Prevention of future ovarian CA?
– Disadvantages • Surgical risk (Stage IV endometriosis)

Case 1
• Patient opts for surgery: hysterectomy, BSO, complete removal of endometriosis
• 6 week post-op visit: Patient presents with significant hot flushes. What type of HRT? – Estrogen and Progesterone
Hum Reprod Update 23(4):481-500

General gynecologist or family physician
• What we’re more likely to see – Patient with benign ovarian endometrioma 1) What’s the risk of ovarian CA? 2) How can we prevent and who’s at higher risk?
– Atypical endometriosis found on pathology, in
what looked like a benign endometrioma 1) How frequent is this finding? 2) How to manage?

Atypical endometriosis in (benign) endometrioma
• How frequent? – Risk of atypical endometriosis in ovarian
endometriosis approx 1-2% (4/255)
• How to manage?
– No guidelines – Possibilities: Surveillance? Hormonal therapy?
Repeat surgery?
Histopathology 1997;30:249-55
Case 2
• 30 year old, G0, with infertility – History/physical suspicious for endometriosis – AMH = 2.0 ng/mL – Workup shows 5cm right endometrioma – Patient opts for laparoscopy, cystectomy done
• Pathology: right endometrioma with evidence of atypical endometriosis, no malignancy
• Post-operative U/S: 1cm “follicle” in right ovary

Case 2
• Management?
• Expectant and try for pregnancy, re-evaluate postpartum?
• Hormonal therapy and proceed to ART, then re-evaluate postpartum?
• Oophorectomy, then try for pregnancy?

Case 2
• Expectant and try for pregnancy, re-evaluate postpartum? – Advantages
• Preserve fertility, spontaneous conception
– Disadvantages • Residual atypical endometriosis present?
Case 2
• Hormonal therapy and proceed to ART, then reevaluate post-partum? – Advantages
• Chemoprevention • Preserve fertility
– Disadvantages • Residual atypical endometriosis present? • ART required (e.g. cost)

Case 2
• Oophorectomy, then try for pregnancy? – Advantages
• Prevention of ovarian CA?
– Disadvantages • Loss of ovary – but AMH reasonable and could conceive
from other ovary

Case 2
• Patient opts for oophorectomy, conceives spontaneously from remaining ovary
• 6 week post-partum visit: Patient asks about spacing next pregnancy. What type of family planning? – Hormonal (estrogen-progestin or progestin)

Take home points
• Identify the epidemiology and classification of endometriosis
Endometriosis is common, and the ovarian subtype appears to be at risk for malignant transformation
Take home points
• State the impact of atypical endometriosis on malignant gynecologic tumours
Genomic evidence that endometriosis can become atypical, which is a precursor to ovarian CA (clear cell or endometrioid)
Take home points
• Discuss potential ways to prevent future ovarian cancer in women with endometriosis
Possibilities: Hormonal therapy, Parity, Tubal ligation (Salpingectomy), Hysterectomy, Oophorectomy, Complete surgical removal of endometriosis

Questions?
Email: [email protected] or [email protected] BC Women’s Centre for Pelvic Pain and Endometriosis: Http://www.womenspelvicpainendo.com