endodontic emergenciesjrdindia.org/ver2/app/upload/review article 87.pdf · endodontic emergencies...
TRANSCRIPT
Khaly Bane IJRD ISSUE 1, 2019
1 Downloaded from www.jrdindia.org
Review Article
ENDODONTIC EMERGENCIES
Khaly Banea*, Mouhamed Sarra, Koffi Yolande Gnagneb, Babacar Fayea, Babacar Touréa.
aDepartment of Conservative Dentistry and Endodontics, Faculty of Medicine, Pharmacy and
Odontology-Stomatology, Cheikh Anta Diop University of Dakar, Senegal.
bDepartment of Conservative Dentistry and Endodontics, Félix Houphouet Boigny University,
Abidjan, Ivory Cost.
BANE Khaly, Associate Professor, Department of Conservative Dentistry and Endodontics, Cheikh Anta Diop University of Dakar. P.O.Box 5005, Dakar-Fann, Dakar, Senegal.
E-mail address: [email protected]
SARR Mouhamed, Associate Professor, Department of Conservative Dentistry and Endodontics, Cheikh Anta Diop University of Dakar. P.O.Box 5005, Dakar-Fann, Dakar, Senegal.
E-mail address: [email protected]
GNAGNE Koffi Yolande, Associate Professor, Department of Conservative Dentistry and Endodontics, Félix Houphouët Boigny University - Abidjan. BP: 612 Abidjan 22, Ivory Cost.
E-mail address: [email protected]
FAYE Babacar, Full Professor, Department of Conservative Dentistry and Endodontics, Cheikh Anta Diop University of Dakar. P.O.Box 5005, Dakar-Fann, Dakar, Senegal.
E-mail address: [email protected]
TOURÉ Babacar, Full Professor, Department of Conservative Dentistry and Endodontics, Cheikh Anta Diop University of Dakar. P.O.Box 5005, Dakar-Fann, Dakar, Senegal.
E-mail address: [email protected]
Corresponding author: Khaly Bane, Department of Conservative Dentistry and Endodontics, Cheikh Anta Diop University of Dakar. P.O.Box 5005, Dakar-Fann, Dakar, Senegal.
Tel: +221 77550 63 21
E-mail: [email protected]

Khaly Bane IJRD ISSUE 1, 2019
2 Downloaded from www.jrdindia.org
ABSTRACT
Endodontic emergencies represent approximately 90% of the emergency consultation reasons. In
particular, they are characterized by violent or disabling pain. In the absence of adequate emergency
treatment, there is a risk of infectious complication. The management of these emergencies in the
dental office requires to be effective the achievement of a precise diagnosis and an emergency act
with or without a prescription.
The objective of this article is to present, according to the data of the current endodontic literature,
the diagnostic and therapeutic elements which make it possible to face effectively all emergency
situations in endodontics.
KEY WORDS: Acute apical abscess, Acute apical periodontitis, Flare up, Pain, Pulpitis
Introduction:
Endodontic emergencies account for
approximately 90% of emergency consultation
reasons1. In particular, they are characterized
by violent or disabling pain. In the absence of
adequate emergency treatment, there is a risk
of infectious complication. While some of them
are vital emergencies (diffuse cellulitis), which
may be hospitalization in intensive care, the
management of the vast majority of endodontic
emergencies is the responsibility of the
odontologist and relies mainly on symptomatic
treatment2. Management of endodontic pain is
one of the challenging aspects in endodontics3.
The aim of this article is to present, according
to the data of the current endodontic literature,
the diagnostic and therapeutic elements which
make it possible to face effectively all
emergency situations in endodontics.
I. PAIN IN ENDODONTICS
1.1. Peripheral mechanisms
involved in the nociception of the
trigeminal sphere
The orofacial region is strongly innervated and
very varied. Pain receptors are located in most
superficial and deep tissues4. The dental and
periodontal sensibility is ensured by the
maxillary nerve (V2, branch of the trigeminal
nerve) which innervates the middle third of the
face and the mandibular nerve (V3, third
branch of the trigeminal nerve) which
innervates the lower stage of the face; the
ophthalmic nerve (V1, first branch of the
trigeminal nerve) innervating the upper stage
of the face. The endings of these three
branches are found in almost all of the
orofacial territories, especially at the dental
level. They are grouped together to constitute
the peripheral ramifications of amyelinic C
fibers and myelinic of Aδ type and also Aβ4.
The fibers found at the level of the dental pulp
consist of 80% of two major types: C fibers,
amyelinic, low conduction velocity (less than
5m / s) and small diameter (less than 1.5μm),
and fibers slightly myelinic, diameter (1 to 5μm)
and conduction velocity (less than 15 - 35m /
s) slightly higher than the first. Aδ fibers differ

Khaly Bane IJRD ISSUE 1, 2019
3 Downloaded from www.jrdindia.org
from other myelinic fibers in the body due to
the absence of perineural connective sheath5.
All the pulp fibers give fine collateral branches
in the center of the pulp and end with a rich
plexus in the acellular zone under the
odontoblasts, Rashkow's Plexus. Various
external agents (mechanical, chemical,
thermal, electrical) or internal (pro-
inflammatory molecules such as
prostaglandins or neuropeptides) can
stimulate these fibers and give rise to two
different kinds of sensation6. The short and
sharp pain is due to activation of the A fibers
while the dull pain is due to the C fibers. The
action potentials from the peripheral endings
are transmitted to the central ends where they
will cause the release of neurotransmitters
such as the glutamate. Transmission is rapid in
the A fibers (acute pain), slower in the C fibers
(torpid pain) 5.
1.2. Diagnostic tools
In an emergency, the practitioner is required to
perform a quick and effective gesture to relieve
the patient. The nature of this intervention is
dictated by the diagnosis, which as for any
medical treatment is an indispensable and
decisive step. A set of elements are taken into
consideration and make it possible to
determine the nature of the pathology and also
to perform a differential diagnosis.
a. Anamnesis
The reason for the consultation will very
quickly guide the interview of the patient. In
endodontics, the pain is usually concerned and
simple and short questions allow to determine
the origin, nature and characteristics of the
pain. The spontaneous or provoked nature of
pain, triggering factors, duration, persistence,
location, and nature are all necessary
elements to consider7,8.
Medical and surgical history and criteria such
as fatigue, fever, and excessive self-
medication should also be taken into
consideration for the management of the
patient9.
b. Tests
Depending on the patient's grievances,
performing test (s) may be necessary. Among
the many tests at our disposal, the most
appropriate and relevant to confirm or
invalidate a diagnosis should be selected10.
Exobuccal examination allows to highlight
the possible swelling of the mouth, the
presence of fistula or trauma. Careful
palpation of the integuments makes it
possible to detect the presence of
adenopathies.
The intra-oral examination makes it
possible to observe the teeth of the sector
concerned in every detail. The use of
magnifying elements such as magnifying
glass or microscope optimizes the
diagnosis.
Intraoral palpation of the gingiva is often
painful compared to the apices of teeth with
acute apical periodontitis or acute apical
abscess. Axial or vertical percussion with
the handle of an instrument is used to
determine the presence of acute
periodontal or periapical inflammation.
Khaly Bane IJRD ISSUE 1, 2019
4 Downloaded from www.jrdindia.org
The periodontal survey should be
systematic. The probing of the suspect
tooth allows to establish a differential
diagnosis between an endodontic problem,
a periodontal problem, or the presence of a
fracture.
Pulp vitality tests (hot, cold and electrical)
are always done in comparison with a
healthy tooth and provide information on
the pulp state. They are particularly useful
for establishing a differential diagnosis
between an endodontic problem and a
periodontal problem.
The bite test involves biting the patient,
cuspid by cusp, on a wet cotton swab or a
sheet of dike wrapped around a cement
spatula. A sharp pain on loosening and
occlusion can lead to the diagnosis of
cracking8, 9.
c. Radiographic examination
The panoramic X-ray is a good element for the
emergency clinical examination. It gives a
global vision of the oral cavity and in the
context of the search for a pathology, it makes
it possible to highlight the dental fractures, the
carious attacks and the apical lesions. In
endodontics, the area of interest will be
systematically controlled by a retroalveolar
radiograph8, 9.
1.3. Importance of differential
diagnosis
Before undertaking any emergency
endodontic treatment, it is important to make a
differential diagnosis.
a. Endodontic lesion mimicking a
periodontal lesion
The diagnosis of an endodontic problem is
often easy, its evolution respects the integrity
of the epithelial attachment11. In some cases,
especially in the mandible, an alveolar abscess
of endodontic origin may have a submucosal
or subperiosteal drainage path and lead into
the gingival sulcus of the affected tooth,
reminiscent of periodontal abscess. The
fistular route is established at the expense of
one of the bone tables and may appear in the
form of radiolucency radiography. In this case,
the periodontal sounding is deep and narrow,
located at the level of the fistula, and the pulpal
vitality test is negative. The patient consults
especially because of purulent discharge, and
not for painful symptomatology. These lesions
can sometimes be associated with an acute
inflammatory episode. Emergency treatment is
purely endodontic11, 12.
b. Periodontal lesion mimicking an
endodontic lesion
This situation is quite rare. However, confusion
may exist when there is an abscess of
periodontal origin localized to a single tooth.
The pain is accompanied or not by swelling of
the vestibular portion of the mucosa in the
vicinity of a tooth showing no sign of
endodontic pathology. The tooth can be
sensitive to axial percussion and apical
palpation and normally responds to thermal
sensitivity tests (hot or cold)11, 12.
Khaly Bane IJRD ISSUE 1, 2019
5 Downloaded from www.jrdindia.org
c. Syndrome septum and endodontic
lesions
The septum syndrome results from a food
settling between two teeth whose point of
contact is deficient. The pain is very severe,
especially after the meal, and the presence of
decay or coronary restoration may suggest an
endodontic origin. The papillary gingiva bleeds
at the slightest touch and the X-ray can show
horizontal bone lysis in the interproximal
space. The simple suppression of food intake
relieves the patient9.
d. Radicular crack/fracture and
endodontic lesions
Radicular cracks and fractures are often
difficult to highlight. The clinical picture may
resemble that of a pulpitis if it occurs on a vital
tooth, and a desmodontitis if it occurs on a
tooth already treated endodontically. The most
reliable way to make an emergency diagnosis
is the bite test8, 9.
II. EMERGENCIES BEFORE
TREATMENT
2.1. Pulpitis
Pulpitis is a result of a bacterial attack most
often related to tooth decay. The aggression
can be triggered also by mechanical irritations,
chemical. The inflammatory reaction of the
pulp is similar to that which occurs in other
connective tissues; the fact that it is enclosed
in a cavity with inextensible walls explains the
local increase in pressure13. The first stage of
inflammation is associated with pulpal
hyperemia, which can evolve either acutely or
chronically to pulpal necrosis with the
possibility of periapex contamination4.
a. Reversible pulpitis
The reversible pulpitis corresponds to an
alteration stage of an inflamed but vital pulp.
External stimuli (hot, cold, sugar ...) cause
painful response but disappears immediately
after stopping the stimulus. The pains are
always provoked and not spontaneous. In
most cases, a carious lesion or recent
obstruction appears to be the cause of the
condition14, 15.
Urgent treatment consists of removing cavities
and providing a tight temporary seal to protect
the underlying pulp and provide sedative
function10, 15. In cases of proven pulpal
proximity, the use of other materials such as
calcium hydroxide or even MTA may be
indicated.
b. Irreversible pulpitis
The irreversible pulpitis corresponds to a
severe inflammation that does not regress,
even if the cause is suppressed; the pulp is
therefore condemned to be eliminated. The
symptomatology associated with irreversible
acute pulpitis is spontaneous, violent and
radiating pain. Pain can also be triggered by
hot, cold and acid and exacerbated by physical
activity and decubitus16. In the most advanced
stages of inflammation, ligament thickening
may be observed on X-ray. Given the extent of
such pain symptomatology, emergency
treatment is required after completion of a
deep anesthesia. The tooth to be treated is
isolated from the rest of the oral cavity, the

Khaly Bane IJRD ISSUE 1, 2019
6 Downloaded from www.jrdindia.org
decayed dentin completely removed before
seeking access to the pulp, and the access
cavity made.
For multi-rooted teeth, only the cameral
pulp is removed with a bur or excavator.
The pulp is frankly sectioned at the
entrance of each canal. Hemostasis is
performed by compression with a cotton
pellet, previously decontaminated with
sodium hypochlorite. If stopping bleeding is
not achieved, pulpectomy of the bleeding
canal is indicated9.
For monoradiculates, complete
pulpectomy is indicated. It can be
performed with a nerve-puller whose
length and diameter selected according to
the radiological indications. Ideally a first
instrument is put in place, then a second
one is inserted. By simultaneously rotating
the two instruments, the instruments wind
up the connective bundle, which can be
removed from the canal without difficulty.
In all cases, a sterile cotton pellet alone is
placed in the pulp chamber. This dressing is
then covered with a temporary waterproof
cement. In some cases, especially in the most
advanced stages of periodontal inflammation,
the tooth should be placed under occlusion.
The treatment is accompanied by a
prescription of nonsteroidal anti-inflammatory
to block the synthesis of prostaglandins which
are algogenic factors.
All recent endodontic manuals advocate this
emergency treatment to relieve patients with
acute pulpitis17, 18, 19, 20. In addition, a large
number of authors have shown that a tooth
thus treated may remain asymptomatic for a
period of at least one month, and may exceed
6 months21, 22, 23, 24, 25. However, all of them
mention the difficulty of emergency
implementation and poor initial management
can strongly influence the definitive treatment
(accidental bacterial contamination of the
canals during the emergency procedure can
promote or lead to an infection of the
endodontic system which will very often lead to
formation of an inflammatory apical bone
lesion that may progress to abscess.) More
recently, different protocols for the
management of this type of pain syndromes
have been proposed, consisting of a
periradicular intra-osseous injection of
synthetic glucocorticoid26, 27. The anti-
inflammatory action on the inflamed pulp has
been demonstrated by a biochemical
approach28.
Anesthesia of the concerned tooth is
performed. The site of transcortical perforation
is determined after clinical and radiographic
examination: it should ideally be located in the
attached vestibular gingiva, about 5 mm below
the line of the necks, avoiding the dental roots.
The cortical bone is perforated using a sterile
disposable device designed for intra-bone
injection of anesthetic, mounted on a counter-
angle rotating at 10,000 rpm (Dentsply-
Maillefer X-Tip® Needle). The perforator is then
removed leaving in place a catheter for
injection into the medullary bone space. The
methyl-prednisolone acetate (Dépo-Médrol®),
previously conditioned, is injected slowly (1 ml
in 1 to 2 minutes) via a needle placed in the
catheter. The injection site is monitored for
Khaly Bane IJRD ISSUE 1, 2019
7 Downloaded from www.jrdindia.org
evidence of possible reflux that would lead to
treatment failure. After injection, the guide is
removed using a hemostatic forceps, and if
necessary, hemostasis obtained by
compression. No endodontic procedure or
prescription is required and final endodontic
treatment can be performed later in a single
session to avoid the risk of contamination27.
2.2. Acute apical periodontitis
In the absence of treatment, the bacteria that
cause pulpitis can develop, cause pulp
necrosis and eventually cause bacterial
contamination of the endodontic space10. The
development of this infection usually leads to
the development of an inflammatory bone
lesion in the periapical region of the concerned
root. In most cases the periodontal ligament is
also affected by the inflammation and a
thickening is clearly visible on the X-ray.
Clinically, the pains are dull, continuous,
exacerbated by occlusal contact. The pulpal
vitality tests are negative and the percussion is
very painful9. In extreme cases the contact of
the tongue is unbearable thus putting the
patient in a situation of discomfort.
Emergency treatment is done under
anesthesia because there may still be nerve
fibers in the canals. The canals are rid of all
their contents and the shaping carried out
under abundant irrigation with sodium
hypochlorite. An endodontic medication with
calcium hydroxide is put in place and the tooth
is then closed and imperatively placed under
occlusion. A prescription of ibuprofen
completes the surgical procedure14, 15.
2.3. Acute apical abscess
Acute alveolar abscess results from the
passage of bacteria beyond the endodontic
system with diffusion of infection between the
alveolar bone and the periosteum. In some
cases too, it may follow a chronic inflammatory
reaction of the apical periodontium which, for
various reasons, passes into the acute phase.
In clinical terms, the pains are spontaneous,
continuous and very intense9, 14. The causal
tooth is sensitive to contact and percussion.
Vestibular palpation triggers an exacerbation
of pain. Pulpal vitality tests are negative,
important element for differential diagnosis
with periodontal abscess. In the emergency
treatment of acute alveolar abscess, three
situations are always described1, 9, 14.
- Drainage can be obtained by the canal
After setting up the rubber dam, the access
cavity is made. As soon as access to the pulp
chamber is reached, the pus flows and the
patient feels immediate relief. Once this flow
has dried up, the access cavity is finalized, and
abundantly rinsed with sodium hypochlorite. If
this spontaneous drainage is not obtained
immediately after the creation of the access
cavity, it must be caused by the use of a file
(08 to 15) exceeding controlled beyond the
apical constriction. After rinsing the canals, the
tooth is left open and placed under occlusion
for a maximum of 48 hours. A second
appointment is given to achieve the root canal
shaping and disinfection.
- A fluctuating abscess is present

Khaly Bane IJRD ISSUE 1, 2019
8 Downloaded from www.jrdindia.org
If trans-canal drainage has not been achieved
and fluctuating abscess is present, the
drainage required to achieve patient relief can
be achieved by open incision to the
periosteum. After performing a superficial
anesthesia of the mucous membrane, a frank
incision until the periosteum is performed with
a scalpel blade n ° 11. The drainage
immediately relieves the patient. The canals
are thoroughly rinsed with sodium hypochlorite
and the tooth is closed and placed under
occlusion. As in the previous case, an
appointment is scheduled as soon as possible
to initiate endodontic treatment.
- Drainage is not obtained
1. If drainage has not been achieved after
the access cavity and instrumental
maneuver and the abscess is not yet
collected, the tooth should be left open
and placed under occlusion. The
patient is also advised to perform hot
and salty mouthwash by focusing on
the affected tooth. The prescription of
antibiotics is essential; it is here an
association of amoxicillin and
metronidazole. The prescription of a
strong analgesic or corticosteroid must
also be done. As soon as the clinical
signs disappear, the patient must be
reviewed and the endodontic treatment
performed14.
III. EMERGENCIES AFTER TREATMENT
3.1. Recent conservative treatment of the pulp
Following a conservative treatment of the pulp,
a post-operative pain can occur in three
situations:
- Biological cause: Exposure of the pulp to
bacteria is the most virulent irritant and the
most likely to cause pulpal reactions. The
virulence of bacterial aggression, the duration
of contamination and the tightness of the teeth
/ obturation are the parameters most frequently
involved in this cause.
- Physical cause: pulpal pain is associated with
excessive heat-up during milling or polishing,
or abnormal mechanical stimulation of the
tooth due to, for example, iatrogenic occlusal
overload.
Chemical cause: it is directly related to the
toxicity of drug products and materials used in
conservative dentistry29.
3.2. Flare up
a. Infectious outbreak
The peculiarity of this type of emergency is that
it occurs in a patient who before his endodontic
treatment did not suffer. It is after the canal
cleaning session that the pain occurs, which
contributes to the frustration of the patient14, 30.
Three hypotheses can explain the appearance
of this pain:
- The presence of debris, bacteria or
endotoxins beyond the apical foramen

Khaly Bane IJRD ISSUE 1, 2019
9 Downloaded from www.jrdindia.org
propelled into this region during
instrumentation.
- A modification of the intraductal bacterial flora
due to the non-respect of the asepsis-
antisepsis chain.
- A lasting or temporary immunodeficiency of
the patient. The emergency treatment is the
same as that of acute apical periodontitis with
imperatively a prescription of the amoxicillin
and metronidazole combination14, 30.
b. Inflammatory outbreak
The peculiarity of this type of emergency is that
it occurs in a patient who before his endodontic
treatment did not suffer. It is after the canal
cleaning session that the pain occurs, which
contributes to the frustration of the patient14, 31.
Three hypotheses can explain the appearance
of this pain:
- The presence of debris, bacteria or
endotoxins beyond the apical foramen
propelled into this region during
instrumentation.
- A modification of the intraductal bacterial flora
due to the non-respect of the asepsis-
antisepsis chain.
- A lasting or temporary immunodeficiency of
the patient. The emergency treatment is the
same as that of acute apical periodontitis with
imperatively a prescription of the amoxicillin
and metronidazole combination14.
3.3. Accidental injection of
sodium hypochlorite
This type of rare accident occurs when sodium
hypochlorite has been injected into the
periradicular tissues. The reaction is
immediate and violent. The pain is unbearable
and a swelling appears within minutes. At the
level of the canal concerned, prolonged
bleeding appears14. This type of accident often
causes significant necrosis of the surrounding
tissues. The action to take is the following32:
• Stay calm and inform the patient about the
cause and nature of the complication,
• Perform local anesthesia for initial control of
acute pain,
• Rinse immediately with saline to decrease
soft tissue irritation by dilution of sodium
hypochlorite,
• Apply cold compresses immediately to the
facial area to relieve the pain and burning
sensation felt by the patient,
• Leave the tooth open to optimize drainage,
• Recommend that the patient apply an ice
pack for 24 h (15 min intervals) to minimize
edema,
• Recommend that the patient apply warm,
moist compresses after 24 h (15 min intervals)
and rinse with saline for 1 week to improve
circulation in the affected area,
• Control pain with painkillers,
• Avoid nonsteroidal anti-inflammatory drugs,
• Control the inflammatory reaction with the
steroids in the form of tablets at a rate of 1 mg
/ kg or intramuscularly for 3 days,
• Prevent over-infection by prescribing
antibiotics: penicillin is the molecule of choice.
In case of allergy prefer Metronidazole for 7
days,

Khaly Bane IJRD ISSUE 1, 2019
10 Downloaded from www.jrdindia.org
• Schedule follow-up appointments at regular
intervals: Clinical control is required until
symptoms are resolved,
• In severe cases: hospital care is necessary.
To avoid this type of incident, simply avoid
blocking the needle in the canal during
irrigation. To do this, the needle is lowered into
the canal until it locks, then withdrawn by one
millimeter; the injection of sodium hypochlorite
can then begin14.
CONCLUSION
Emergency consultations are unanimously
described as the last resort for patients who
have given up their care, particularly for socio-
economic reasons. Their consultation is
motivated by pain, which explains the large
number of endodontic emergencies in daily
practice. The dental surgeon must have a
therapeutic arsenal to deal with all these
emergencies. A medicalized approach to our
profession based on a preventive and
ultraconservative odontology would certainly
help to reduce endodontic emergencies in
general and those that occur during treatments
in particular.
REFERENCES
1. Carrotte P. Endodontics, part 3: treatment
of endodontic emergencies. Br Dent J
2004;197:299-305.
2. Eleazer PD, Rosenberg PD. Les urgences
et leur thérapeutique en endodontie. In:
Torabinejad M, Walton RE, Fouad AF,
Lévy G, éditeurs. Endodontie: Principes et
pratiques. 5ème édition. Paris : Elsevier
Masson; 2016.p.172-182.
3. Jenarthanan S, Subbarao C. Comparative
evaluation of the efficacy of diclofenac
sodium administered using different
delivery routes in the management of
endodontic pain: A randomized controlled
clinical trial. J Conserv Dent
2018;21(3):297-301.
4. Boucher Y, Pionchon P. Douleurs
orofaciales, diagnostic et traitement. Paris :
CDP; 2006.
5. Lafont J, Lasfargues JJ. Les médiateurs
de l’inflammation pulpaire. Real Clin
1995;6: 193-213.
6. Le Bars D, Willer J C. Physiologie de la
douleur. EMC-Anesthésie réanimation
2004; 1:227-266.
7. Walton RE, Fouad AF. Diagnostic, plan de
traitement et considerations systémiques.
In: Torabinejad M, Walton RE, Fouad AF,
Lévy G, éditeurs. Endodontie: Principes et
pratiques. 5ème édition. Paris : Elsevier
Masson; 2016.p.73-100.
8. Simon S. Endodontie, Volume 1:
traitements. Paris : CDP; 2008.
9. Haas M. Managing endodontic
emergencies. Dent Today 2017; 36(5):80-
83.
10. Ahossi V., Perrot G., Thery L., Potard G.,
Perrin D. Urgences Odontologiques EMC
(Elsevier Masson SAS, Paris), Médecine
d’urgence, 25-170-A-10, 2007.
11. Machtou P, Cohen A. Diagnostic
differentiel des lesions endo-parodontales.
J Parodont 1988;7:155-166.
Khaly Bane IJRD ISSUE 1, 2019
11 Downloaded from www.jrdindia.org
12. Rangé H. Les relations complexes entre
parodonte et endodonte. Rev Odont
Stomat 2007;36:161-178.
13. Vreven J, Noël H. Pulpite et nécrose
pulpaire. In : Piette E, Goldberg M,
éditeurs. La dent normale et pathologique.
1ère Ed. Bruxelles : De Boeck Université ;
2001. p.125-35.
14. Machtou P. Endodontie. Paris: CDP;
1993.
15. Robinson J.-J., Giraud O., Dos Santos S.,
Turlotte S., Fieschi J.-M. Urgences
dentaires dans la pratique quotidienne.
EMC (Elsevier Masson SAS, Paris),
Odontologie, 23-750-A-10, 2001,
Médecine buccale, 28-700-M-10, 2008.
16. Vreven J. Pathologie des dents, section
Pathologie dentaire carieuse. In: Piette E,
Reychler H. Traité de pathologies buccales
et maxillo-faciales. Bruxelles : De Boeck-
Wesmael; 1991.p.1161-1177.
17. Cohen S, Hargreaves KM. Pathways of
the Pulp. 9th Ed. St. Louis: Mosby; 2006.
18. Hülsmann M, Schäfer E. Problems in the
treatment of endodontic emergencies. In:
Hülsmann M, Schäfer E, editors.
Problems in Endodontics. New Malden:
Quintessence Publishing; 2009. p.127-
43.
19. Ingle JI, Bakland LK. Endodontics. 5th Ed.
London: B. C. Decker; 2002.
20. Tronstad L. Clinical Endodontics: A
Textbook. 2nd Ed. New York: Thieme
Medical Publishers; 2003.
21. DeRosa TA. A retrospective evaluation of
pulpotomy as an alternative to extraction.
Gen Dent 2006; 54(1):37-40.
22. Hasselgren G, Reit C. Emergency
pulpotomy: Relieving Effect with and
without the Use of Sedative Dressings. J
Endod 1989;15(6):254-6.
23. McDougal RA, Delano EO, Caplan D,
Sigurdsson A, Trope M. Success of an
alternative for interim management of
irreversible pulpitis. J Am Dent Assoc
2004;135(12):1707-12.
24. Nyerere JW, Matee MI, Simon EN.
Emergency pulpotomy in relieving acute
dental pain among Tanzanian patients.
BMC Oral Health 18 janvier 2008;6:1.
Publication sous forme électronique:
http://www.biomedcentral.com/1472-
6831/6/1.
25. Oguntebi BR, DeSchepper EJ, Taylor TS,
White CL, Pink FE. Postoperative pain
incidence related to the type of emergency
treatment of symptomatic pulpitis. Oral
Surg Oral Med Oral Pathol Oral Radiol
Endod 1992;73(4):479-83.
26. Gallatin E, Nist R, Beck M. Pain
Reduction in Untreated Irreversible Pulpitis
Using an Intraosseous Injection of Depo-
Medrol. J Endod 2000;26(11): 633-8.
27. Bane K, Charpentier E, Bronnec F,
Descroix V, Gaye Ndiaye F, Kane A
W,Toledo R, Machtou P, Azérad J.
Randomized clinical trial of intraosseous
methylprednisolone injection for acute
pulpitis pain. J Endodo 2016;42:2-7.
28. Isett J, Reader A, Gallatin E, Beck
M,Padgett D. Effect of an Intraosseous
Injection of Depo-Medrol on Pulpal
Concentrations of PGE2 and IL-8 in

Khaly Bane IJRD ISSUE 1, 2019
12 Downloaded from www.jrdindia.org
Untreated Irreversible Pulpitis. J Endod
2003;29(4):268-71.
29. Chazel J.-C., Esber S., Kouassi M.,
Pélissier B. Pulpopathies iatrogènes.
Etiologie, prévention et traitements. EMC
(Elsevier Masson SAS, Paris),
Odontologie, 23-008-A-20, 2006,
Médecine buccale, 28-260-V-10, 2008.
30. Gbadebo SO, Sulaiman AO, Anifowose
OO. Endodontic flare up: incidence and
association of possible risks. Afr J Med
Med Sci 2016;45(2):207-2012.
31. Yang HL, Tang R, Gong Y, Zhang YH.
Clinical evaluation of the presence of
interappointment emergencies during
intracanal medication before and after root
canal preparation. Shanghai Kou Qiang Yi
Xue 2016;25(2):227-230.
32. Ben Rajeb H, douki N. injection
accidentelle d’hypochlorite de sodium au
cours d’un traitement accidentelle : mieux
comprendre pour mieux gérer.
Odontostomatol Trop 2015 ; 38 :50-56.
LISTE OF FIGURES
Figure 1: Emergency treatment of reversible
pulpitis involves removal of decayed tooth tissue
and placement of pulp capping material
.
a. b.
c.
Figure 2 : Opening of the pulpal chamber of a
maxillary molar presenting acute irreversible
pulpitis with significant bleeding (a) which
persisted despite a few minutes of haemostasis
(b); which necessitated the pulpectomy of the
palatal canal (c).
a. b.
Figure 3: Periradicular injection of methyl prednisolone
acetate
a: Transcortical perforation
b: Injection of the product
Khaly Bane IJRD ISSUE 1, 2019
13 Downloaded from www.jrdindia.org
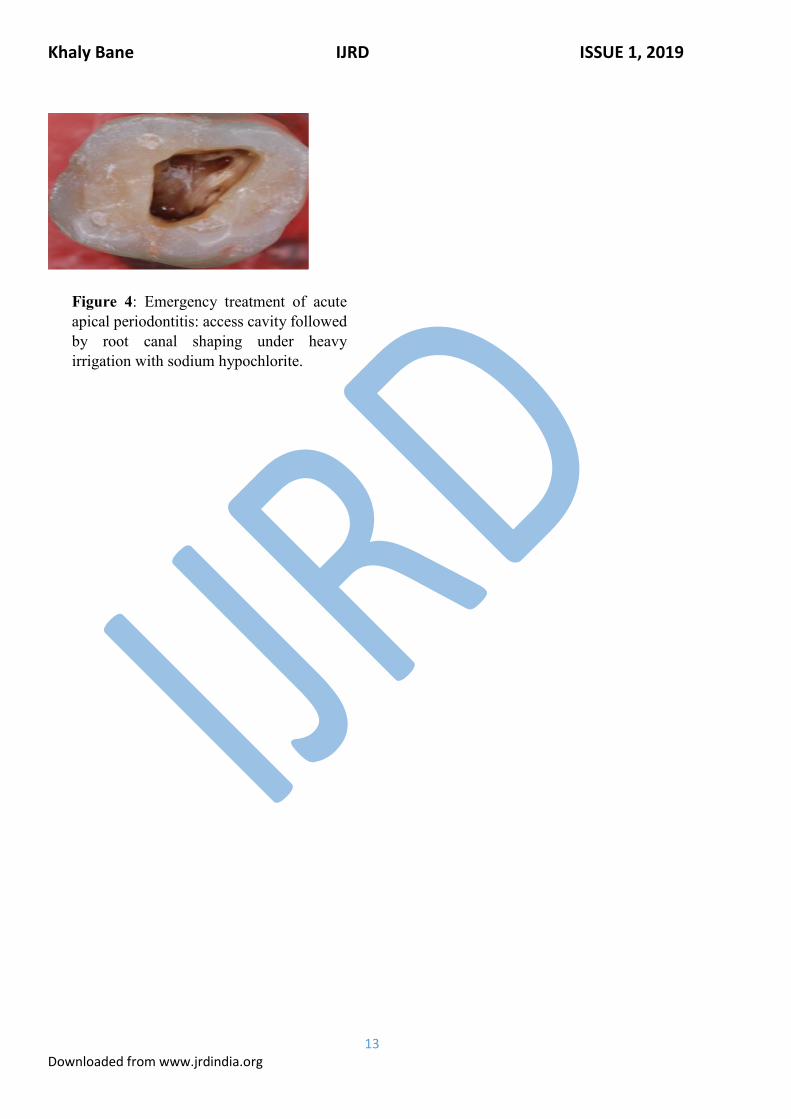
Figure 4: Emergency treatment of acute
apical periodontitis: access cavity followed
by root canal shaping under heavy
irrigation with sodium hypochlorite.