ems: the tools we use
TRANSCRIPT
AND HOW NOT TO GET USED BY THEM….
The Tools we use
RULE No. 1
Tools supplement clinical thinking and details subjective and objective assessments, they do not replace them.
AKA: Treat the patient, NOT THE MONITOR (or the glucometer, or the pulse ox…)
RULE No. 2
Tools fail if you: Don’t take care of them Don’t check them out EVERY SHIFT Don’t know how to use them Don’t know how to NOT use them Don’t read about the technology behind them…
AKA: Murphy is a son of a bitch waiting to screw with you and your equipment….
What we will cover…
StethoscopeSphygmomanometerGlucometerSPO2/SPCOEKGETCO2
Stethoscope
Stethoscope
Prior to the advent of the stethoscope, there were no reliable, non-invasive (and therefore non-lethal) methods to assess certain parts of the human anatomy.
A Stethoscope is used by Auscultation (listening) Sound is simply interpretation of vibrations by the
specialized nervous system structures that send data to the brain.
Therefore any method that limits outside vibration and noise will increase the fidelity of auscultation… Position to the patent Length and thickness of tubing on stethoscope Heels off ground in moving ambulance Environmental factors
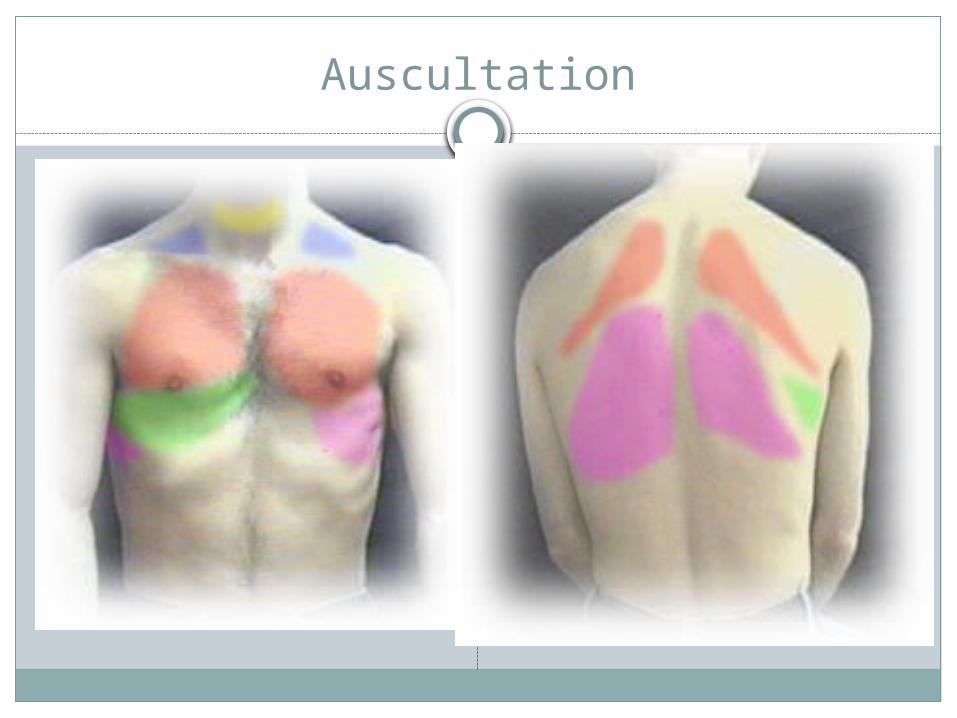
Auscultation
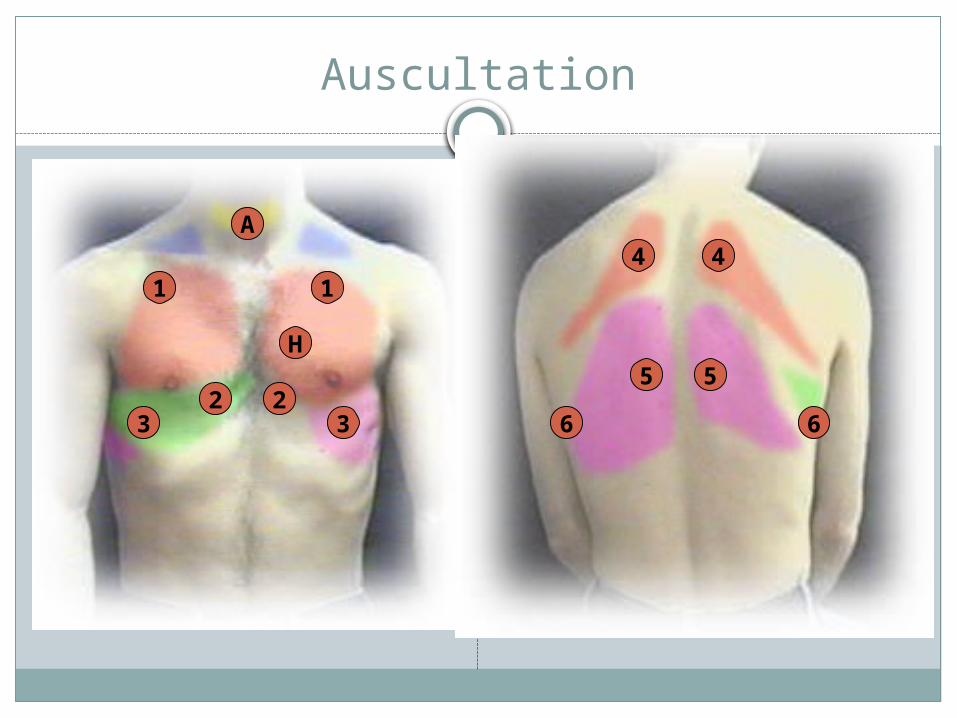
Auscultation
1 1
2 23 3
A4 4
5 5
6 6
H
Variations
ElectronicRecordingDuo-stethascope (for
teaching)Fetoscope, AKA A
Pinard Horn
Sphygmomanometer
Rev. Stephen Hale's experiments to determine the blood pressure of a horse. Circa 1733
Sphygmomanometer
When we talk about blood pressure, we are usually speaking of Non-Invasive Blood Pressure (NIBP).
This is used to estimate the Mean Arterial Pressure (MAP) and thus estimate Aortic Pressure.
Key Point: Blood Pressure (NIBP) is an indirect estimate of central
perfusion pressures
Blood Pressure (NIBP)
Two basic types Manual
Mercury Aneroid
Automatic
Blood Pressure (NIBP)
Systolic Diastolic Mm HgPulse pressureMAP
Pulse Pressure
Generally speaking it is the pressure that produces a pulse that we can feel.
Specifically it is pulse pressure is calculated by subtracting the diastolic pressure from the systolic pressure. SBP – DPB = Pulse Pressure
Significant for: A PP is considered LOW if it is less than 25% of the SBP. A narrowing PP is significant for progressing cardiac
tapenade, blood loss, or Tension Pneumothorax A high PP is significant for cardiac disease, HTN, and cor
pulmonale
Mean Arterial Pressure
The MAP is an mathmatical estimate of the current perfusion pressure. A minimum MAP of 50-60 mmHg is needed for most perfusion
sensitive organs.
Two main methods of calculation:Diastolic pressure + one third of the patients pulse
pressure: diastolic blood pressure + (pulse pressure/3).
Diastolic pressure times 2 plus the systolic pressure and then divide that number by 3: (diastolic pressure x 2) + systolic pressure] / 3
“Normal MAP” is between 70—110 mmHg A normal MAP does not preclude a serious condition
Orthostatic Blood Pressure
Procedure:Assess the need for orthostatics.Obtain patient’s pulse and blood pressure while supine.Have the patient sit up for one minute; Obtain the patient's blood pressure and pulse while
sitting. If positive orthostatic changes occur while sitting, DO NOT continue
to the standing position. Have patient stand for one minute.
Free standing, not leaning. Obtain patient’s pulse and blood pressure while
standing. Have someone stand on each side of the patient in case of
orthostatic syncope
Orthostatic Blood Pressure
Orthostatics are considered POSITIVE if: The patient was unable to tolerate standing and became severely
symptomatic. If pulse has increased by 20 BPM OR systolic blood pressure
decreased by 20 mmHg, the orthostatics are considered positive. As an alternative, an increase of 10 BPM AND a decrease of 10
mmHg may also be considered positive if symptomatic. Document the time and vital signs for supine and
standing positions on/with the patient care report (PCR).KEY Points:
You need both PULSE and BLOOD PRESSURE You need the patient to be in each position for a full minute. If they cant complete the test, it is considered positive.
Monitoring Blood Glucose
Source: Accu-Chek® Aviva used with permission of Roche Diagnostics.
Blood glucose monitoring kit
Monitoring Blood Glucose
Perhaps the single most important factor in a diabetics health is how well they monitor their own BG.
Severity of diabetic complications depends on patient’s average blood glucose level.
Glucose Monitors Facts
Personal use: Calibrated Monthly (rare)For EMS use: Calibrated WEEKLYMost have a chip which need to be changed
with EVRY BOTTLE OF NEW STRIPS Affected by tempAffected by time (samples must be applied
w/in 30 –60 seconds)
Blood Glucose Monitoring
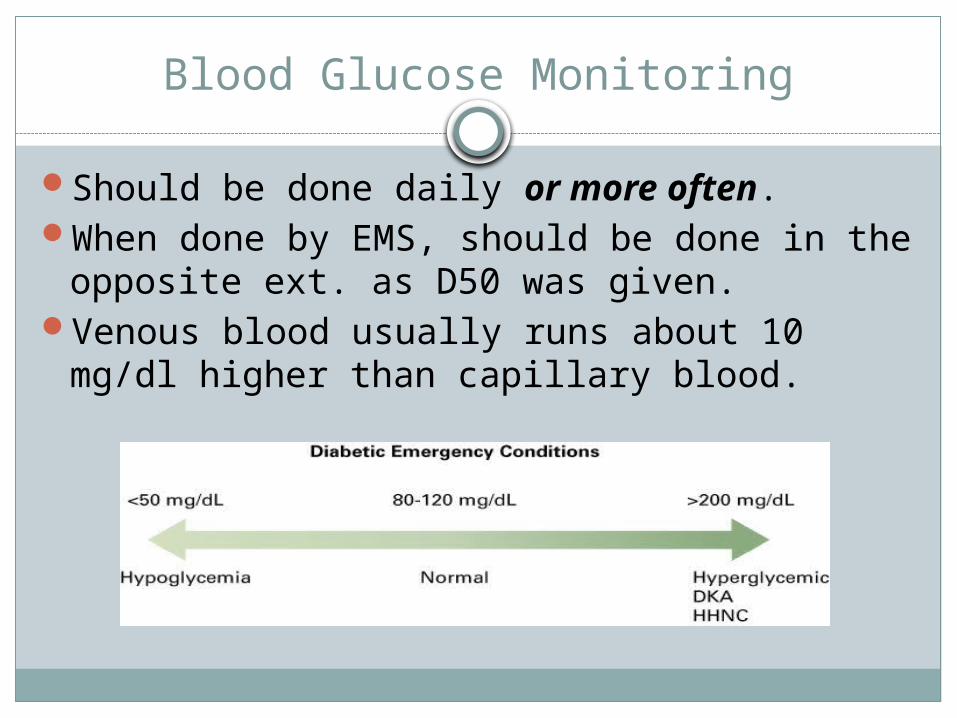
Should be done daily or more often.When done by EMS, should be done in the
opposite ext. as D50 was given.Venous blood usually runs about 10 mg/dl
higher than capillary blood.
Checking the Blood Glucose Level (BG)
Glucometers are commonly found on EMS units.
Determines the amount of glucose in the blood, the sample usually coming from a finger stick.
Glucose is measured in milligrams per deciliter (mg/dl).
A normal range is 80-120 mg/dl. Hypoglycemia is a BGL <60 mg/dl. Hyperglycemia is a BGL >150 mg/dl.
Typically not significant until greater than 250. Often not symptomatic until greater than 400 (not always true)
What are the numbers?
Low: <60mg/dl (<3.0 mmol/L)Normal: 60-150mg/dl (3.0-8.0 mmol/L)
Some recommend 120 mg/dlHyperglycemic: >150 (>8.0 mmol/L)DKA usually seen at 250-500mg/dl
mmol/L vs. mg/dl
What is an MMOL?It is a unit of measurement commonly used in
chemistry based on the molecular weight of the substance it pertains to.
To convert mmol/l of glucose to mg/dl, multiply by 18. To convert mg/dl of glucose to mmol/l, divide by 18 or multiply by 0.055.
SPO2
Pulse oximetry is a non-invasive method allowing the monitoring of the saturation of a patient's hemoglobin.
Originally invented in the 1930’s, it expaded into Ors in the 1980;s, and ER,s ICU’s, and EMS Units in the early 1990’s. Early models were unreliable.
Current technology is not only reliable, but leading into other assessment parameters , including SPCO, SPMet, and Fluid hydration status. There are still things that can “Spoof” common SPO2
devices.
SPO2
It shines infrared light across the blood flow in the capillary beds. The sensor then reads the light reflected back. The color of the light is representative of the state of the hemoglobin (hgb) that is bound up with O2.
Each hemoglobin molecule can be bound (carry) by up to four oxygen molecules.
The SPO2 is an expression of the percentage (%) of hemoglobin that is bound.
SPO2
SPO2 is always expressed as a percentage.By contrast, PAO2 (arterial pressure of
oxygen) is NOT expressed as a percentage. Even though the normal PAO2 is 80-100 mmhg it can
be over 400 mmhg.
SPO2
In Order to have a reliable reading, you must have: A good site to sample Adequate perfusion to that site Appropriate sensor A visible waveform to assess quality of reading
SPO2 Spoofs
CO PoisoningCyanide PoisoningHypothermiaLow perfusion statesShockNail PolishHigh Light situationsPoor Placement
KEY POINT
Pulse oximetry measures solely hemoglobin saturation, not ventilation, not perfusion, not inspired FIO2, and not physiologic stress.
SPO2 WORKS BEST when combined with other monitoring tools, such as the EKG and especially ETCO2
Hyperoxemia
New discussions on the use of SPO2 to detect and prevent hyperoxemia often “get it wrong”.
Hyperoxemia is PAO2 in excess of 100 mmHgSPO2 parameters (controversial and
debatable) 94% SPO2 -> give O2 94%-99% SPO2 -> give supplemental O2 only if in
distress. 99-100% SPO2-> consider withholding O2 or titrating
down O2 unless in severe failure
SPCO
CO-Oxometry is the non-invasive measurement of Carbon Monoxide (CO) in the capillary beds.
It is a developmental evolution from SPO2 technology, originally designed for “low flow” states in neonates.
The current technology most commonly in use is the RAD series from masimo.

The Rad Series
Benefits
Uses “Signal Extraction technology” (AKA SET)
This new generation can be potentially used for SPO2, SPCO2, SpHg and SPMET.
SET technology was originally developed to be a “low perfusion state” and “Motion resistant” SPO2, whose technology was expanded to CO-Oxometry
Early device specific research papers focused on neonates, alternative sensing locations, and anesthesia settings.
RAD-57 Operation: Sensor Placement
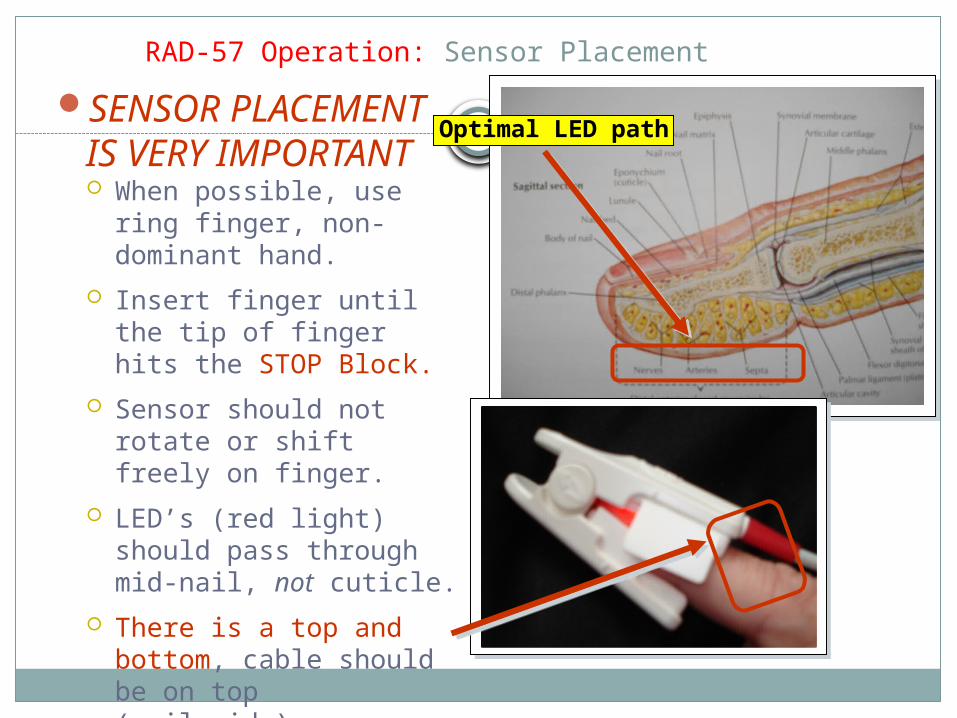
SENSOR PLACEMENT IS VERY IMPORTANT When possible, use ring
finger, non-dominant hand.
Insert finger until the tip of finger hits the STOP Block.
Sensor should not rotate or shift freely on finger.
LED’s (red light) should pass through mid-nail, not cuticle.
There is a top and bottom, cable should be on top (nail side).
Optimal LED path
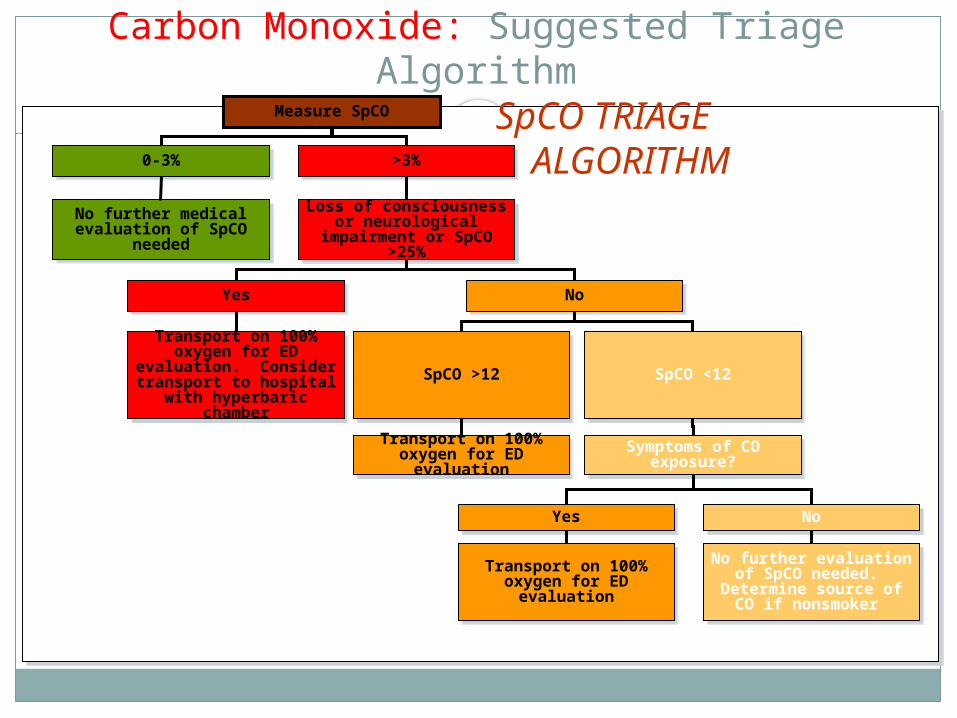
Carbon Monoxide: Suggested Triage Algorithm
Measure SpCO
0-3%0-3% >3%>3%
No further medical evaluation of SpCO
needed
No further medical evaluation of SpCO
needed
Loss of consciousness or neurological
impairment or SpCO >25%
Loss of consciousness or neurological
impairment or SpCO >25%
YesYes NoNo
Transport on 100% oxygen for ED
evaluation. Consider transport to hospital
with hyperbaric chamber
Transport on 100% oxygen for ED
evaluation. Consider transport to hospital
with hyperbaric chamber
SpCO >12SpCO >12 SpCO <12SpCO <12
Transport on 100% oxygen for ED
evaluation
Transport on 100% oxygen for ED
evaluationSymptoms of CO
exposure?Symptoms of CO
exposure?
Transport on 100% oxygen for ED
evaluation
Transport on 100% oxygen for ED
evaluation
No further evaluation of SpCO needed.
Determine source of CO if nonsmoker
No further evaluation of SpCO needed.
Determine source of CO if nonsmoker
YesYes NoNo
SpCO TRIAGE ALGORITHM
How its being used in EMS nationally
Asymptomatic patients – Screening when there is a CO alarm, Hx of
potential exposure, or for rehab situations Asymptomatic Patients with elevated readings
may be screened and reevaluated after 15 minutes of High Flow O2 and Medical Control Consult
Asymptomatic patients without elevated levels may be released on scene. (Controversial)
Symptomatic patients Transport all symptomatic patients
REGARDLESS OF SPCO Screening for severity and diversion to HBO
(Hyperbaric therapy)
SPCO
When used correctly : It is accurate within +/-2% of carboxy-hemoglobin levels to measure CO (the accepted standard)
When not used correctly: It is useless and provide false reassurance.
Downfalls
Very sensitive, can be “spoofed” by strobes and high ambient light. Cover the probe when “Zero”-ing to the patient
Approx. $4,000 retail
Controversy
There is some debate on the accuracy of the technology. Operator error, high light environments, lack of
understanding of the technology all contribute to a high false positive and false negative rate.
Smokers, urban dwellers, and certain occupations have a naturally elevated baseline. Their “Norm” may be in otherwise “elevated CO” ranges.
WHEN WE GET BACK WE WILL BE ON THE ETCO2 PRESENTATION….
Take a Break