empyema due to klebsiella pneumoniae
TRANSCRIPT
Thorax (1967), 22, 170.
Empyema due to Klebsiella pneumoniaeJ. M. REID, R. S. BARCLAY, J. G. STEVENSON,
T. M. WELSH, AND N. McSWAN
From thle Cardio-thoracic Unit, Mearnskirk Hospital, Renifrewshire
Three cases of post-pneumonic empyema due to infection with Klebsiella pneuinoniae arereported. All were men considerably debilitated by complicating factors. The presence of persistentfistulae and of lung necrosis makes eradication of this infection very difficult and tedious, andin the management of these cases the objective is to secure adequate removal of necrotic tissue,effective drainage, and finally a satisfactory deroofing procedure to obliterate the empyemacavity.
The causal organism Klebsiella pneumoniae wasfirst isolated in 1882 by Friedlander. Recent re-ports of infection with the pathogen have all,without exception, stressed the gravity and veryappreciable mortality associated with this typeof pneumonia (Gill, 1951 ; Erasmus, 1956;Holmes, 1956; Limson, Romansky, and Shea,1956; Oswald, Simon, and Shooter, 1961; andLampe, 1964). In a disease which is notorious forproducing destruction of lung tissue with abscessformation, one would expect to encounter a highincidence of complications, particularly withextension of the infection to implicate the pleura.The advent of effective chemotherapy hascertainly reduced the mortality, the recommendedregimen being streptomycin either alone or incombination with chloramphenicol (Lampe,1964); but empyema may still occur in somecases.We wish to present in this communication three
patients with K. pneumoniae infection who,despite apparently adequate antibiotic treatment,developed empyema. All presented difficult prob-lems of management, and their convalescence wasunduly protracted, due in two instances to anaccompanying bronchopleural fistula.
CASE REPORTS
CASE 1 W. M., aged 45 years, was admitted to hos-pital on 8 November 1965 with a history ofproductive cough, right-sided chest pain, and feverof one week's duration. He was subject to inter-mittent bouts of depression and admitted that he wasaddicted to alcohol. On clinical examination signs ofconsolidation at the base of the right lung wereelicited, and this was confirmed by chest radiography.Initially, ampicillin therapy was administered, but as
there was no improvemznt, chloramphenicol wassubstituted. This, in turn, had to be discontinuedafter several days as the patient had developed ageneralized bullous skin eruption. Bacteriologicalexamination of the sputum confirmed the presence ofa heavy growth of K. pnteumontiae which was sensitiveto chloramphenicol, ampicillin, and cephaloridine, andthe patient was then given a course of cephaloridineby intramuscular injection. However, at this juncturethere was evidence of a pleural effusion, and asaspiration yielded a substantial quantity of darkbrown pus, he was transferred to this unit for surgicaltreatment.At operation on 9 December 1965 rib resection
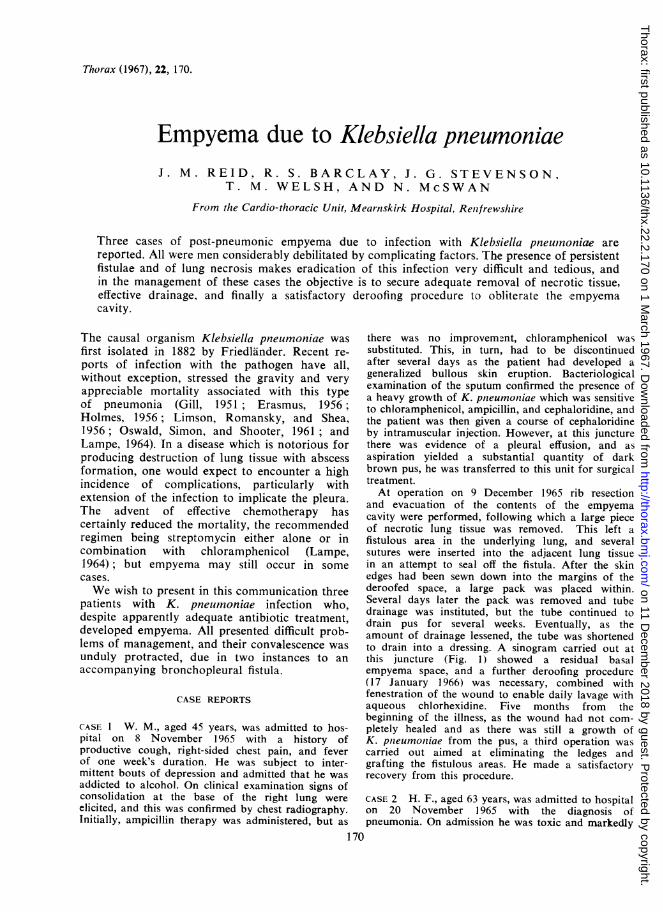
and evacuation of the contents of the empyemacavity were performed, following which a large pieceof necrotic lung tissue was removed. This left afistulous area in the underlying lung, and severalsutures were inserted into the adjacent lung tissuein an attempt to seal off the fistula. After the skinedges had been sewn down into the margins of thederoofed space, a large pack was placed within.Several days later the pack was removed and tubedrainage was instituted, but the tube continued todrain pus for several weeks. Eventually, as theamount of drainage lessened, the tube was shortenedto drain into a dressing. A sinogram carried out atthis juncture (Fig. 1) showed a residual basalempyema space, and a further deroofing procedure(17 January 1966) was necessary, combined withfenestration of the wound to enable daily lavage withaqueous chlorhexidine. Five months from thebeginning of the illness, as the wound had not com-pletely healed and as there was still a growth ofK. pnieumontiae from the pus, a third operation wascarried out aimed at eliminating the ledges andgrafting the fistulous areas. He made a satisfactorvrecovery from this procedure.
CASE 2 H. F., aged 63 years, was admitted to hospitalon 20 November 1965 with the diagnosis ofpneumonia. On admission he was toxic and markedly
170
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from
Empyema due to Klebsiella pneumoniae
:0~~~:
FIG. 1. Case 1. Shows the size of the residual empyema cavity outlined bylipiodol injected through the drainage tube.
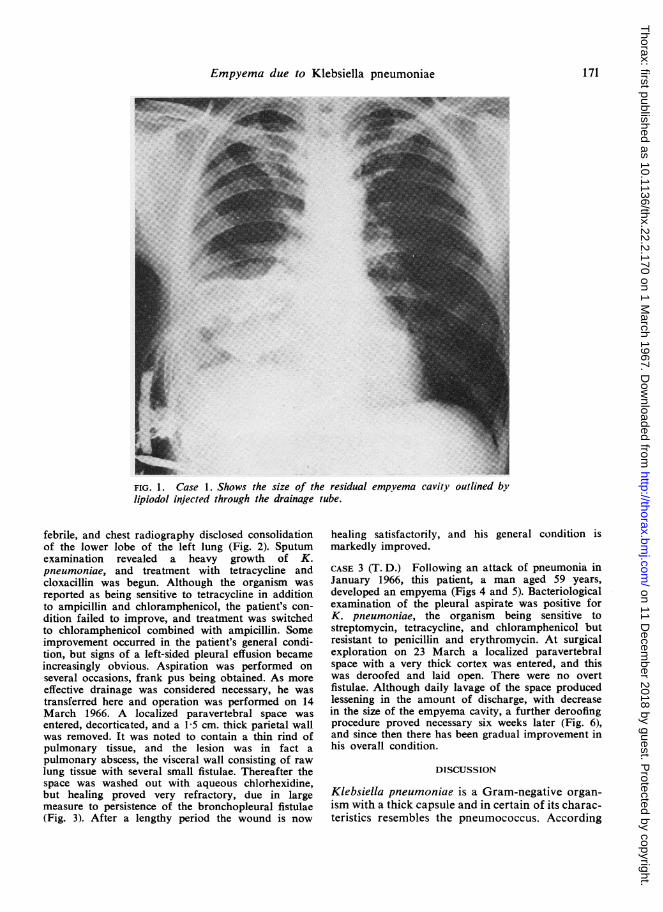
febrile, and chest radiography disclosed consolidationof the lower lobe of the left lung (Fig. 2). Sputumexamination revealed a heavy growth of K.pneumoniae, and treatment with tetracycline andcloxacillin was begun. Although the organism wasreported as being sensitive to tetracycline in additionto ampicillin and chloramphenicol, the patient's con-dition failed to improve, and treatment was switchedto chloramphenicol combined with ampicillin. Someimprovement occurred in the patient's general condi-tion, but signs of a left-sided pleural effusion becameincreasingly obvious. Aspiration was performed onseveral occasions, frank pus being obtained. As moreeffective drainage was considered necessary, he wastransferred here and operation was performed on 14March 1966. A localized paravertebral space wasentered, decorticated, and a 1-5 cm. thick parietal wallwas removed. It was noted to contain a thin rind ofpulmonary tissue, and the lesion was in fact a
pulmonary abscess, the visceral wall consisting of raw
lung tissue with several small fistulae. Thereafter thespace was washed out with aqueous chlorhexidine,but healing proved very refractory, due in largemeasure to persistence of the bronchopleural fistulae(Fig. 3). After a lengthy period the wound is now
healing satisfactorily, and his general condition ismarkedly improved.
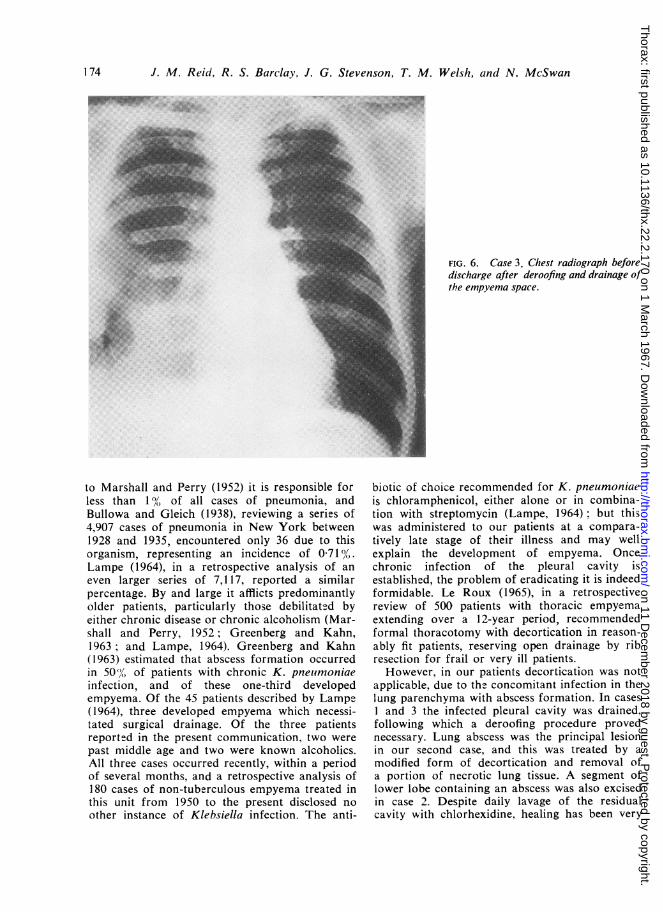
CASE 3 (T. D.) Following an attack of pneumonia inJanuary 1966, this patient, a man aged 59 years,developed an empyema (Figs 4 and 5). Bacteriologicalexamination of the pleural aspirate was positive forK. pneumoniae, the organism being sensitive tostreptomycin, tetracycline, and chloramphenicol butresistant to penicillin and erythromycin. At surgicalexploration on 23 March a localized paravertebralspace with a very thick cortex was entered, and thiswas deroofed and laid open. There were no overtfistulae. Although daily lavage of the space producedlessening in the amount of discharge, with decreasein the size of the empyema cavity, a further deroofingprocedure proved necessary six weeks later (Fig. 6),and since then there has been gradual improvement inhis overall condition.
DISCUSSION
Klebsiella pneumoniae is a Gram-negative organ-ism with a thick capsule and in certain of its charac-teristics resembles the pneumococcus. According
171
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from
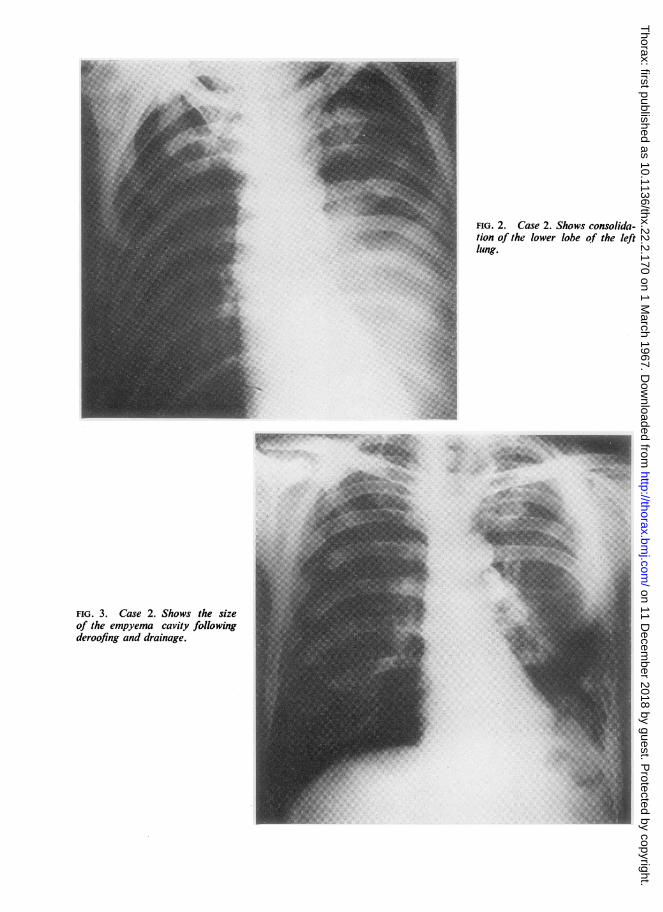
FIG. 2. Case 2. Shows consolida-tion of the lower lobe of the leftlung.
FIG. 3. Case 2. Shows the sizeof the empyema cavity followingderoofing and drainage.
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from
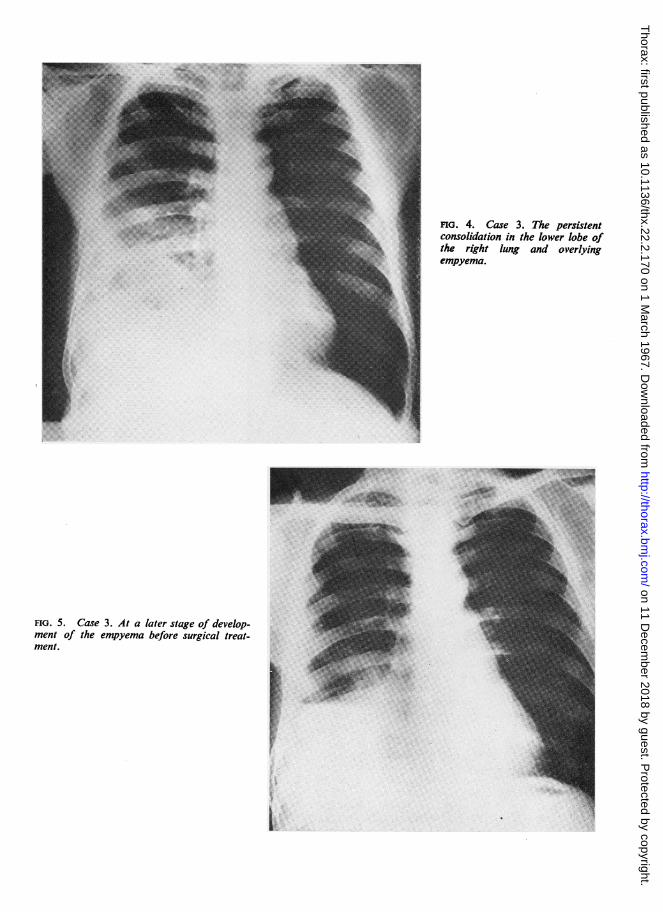
FIG. 4. Case 3. The persistentconsolidation in the lower lobe ofthe right lung and overlyingempyema.
I
FIG. 5. Case 3. At a later stage of develop-ment of the empyema before surgical treat-ment.
L.
pw
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from
174 J. M. Reid, R. S. Barclay, J. G. Stevenson, T. M. Welsh, and N. McSwan
FIG. 6. Case 3. Chest radiograph beforedischarge after deroofing and drainage ofthe empyema space.
to Marshall and Perry (1952) it is responsible forless than 1°/0 of all cases of pneumonia, andBullowa and Gleich (1938), reviewing a series of4,907 cases of pneumonia in New York between1928 and 1935, encountered only 36 due to thisorganism, representing an incidence of 0-710/,%.Lampe (1964), in a retrospective analysis of aneven larger series of 7,117, reported a similarpercentage. By and large it afflicts predominantlyolder patients, particularly those debilitated byeither chronic disease or chronic alcoholism (Mar-shall and Perry, 1952; Greenberg and Kahn,1963; and Lampe, 1964). Greenberg and Kahn(1963) estimated that abscess formation occurredin 50(,y of patients with chronic K. pneumoniaeinfection, and of these one-third developedempyema. Of the 45 patients described by Lampe(1964), three developed empyema which necessi-tated surgical drainage. Of the three patientsreported in the present communication, two werepast middle age and two were known alcoholics.All three cases occurred recently, within a periodof several months, and a retrospective analysis of180 cases of non-tuberculous empyema treated inthis unit from 1950 to the present disclosed noother instance of Klebsiella infection. The anti-
biotic of choice recommended for K. pneumoniaeis chloramphenicol, either alone or in combina-tion with streptomycin (Lampe, 1964); but thiswas administered to our patients at a compara-tively late stage of their illness and may wellexplain the development of empyema. Oncechronic infection of the pleural cavity isestablished, the problem of eradicating it is indeedformidable. Le Roux (1965), in a retrospectivereview of 500 patients with thoracic empyemaextending over a 1 2-year period, recommendedformal thoracotomy with decortication in reason-ably fit patients, reserving open drainage by ribresection for frail or very ill patients.However, in our patients decortication was not
applicable, due to the concomitant infection in thelung parenchyma with abscess formation. In cases1 and 3 the infected pleural cavity was drained,following which a deroofing procedure provednecessary. Lung abscess was the principal lesionin our second case, and this was treated by amodified form of decortication and removal ofa portion of necrotic lung tissue. A segment oflower lobe containing an abscess was also excisedin case 2. Despite daily lavage of the residualcavity with chlorhexidine, healing has been very
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from

Empyema due to Klebsiella pneumoniae
prolonged due to a persistent bronchopleuralfistula in association with areas of necrotic lungtissue. We have successfully used chloramphenicolsuccinate in previous cases of empyema (Steven-son, Reid, McFarlane, and Barrie, 1961), the drugin the form of a suspension being instilleddirectly into the pleural cavity, but it proved ofonly temporary benefit when used in these threepatients. It did not produce any substantial reduc-tion in the size of the empyema cavity, andfurther surgical procedures have been necessary.Our policy in coping with patients suffering
from empyema who require surgical interventionis to carry out rib resection and drainage,decortication, deroofing, or a combination of twoor more of these procedures. These measuressuffice in most patients with non-tuberculousempyema, but empyema caused by K. pneumoniaeis very intractable, due in large measure to theunderlying areas of lung necrosis and to thepresence of persistent bronchopleural fistulae.Despite successive procedures designed to secureadequate drainage, to remove necrotic tissue, andto close the fistulae, the condition has been undulyrecalcitrant in all three. Fairly extensive andmutilating operations on the chest wall have beenimperative, but they have been justified by theoverall improvement in the patients' general con-dition and the slow but steady reduction in the
dimensions of the empyema space. All threepatients are now ambulant and reasonably fit,although admittedly still having daily dressingsto their wounds.
The authors wish to thank the various physiciansin the area who referred their patients for furthertreatment. They are also indebted to Mr. Gray,Department of Medical Illustration, Victoria Infir-mary, for reproducing the radiographs.
REFERENCES
Bullowa, J. G. M., and Gleich, M. (1938). A comparison of theetiology, death rates and bacteremic incidence in the morefrequent primary pneumonias of infants, children, and adults.Amer. J. med. Sci., 196, 709.
Erasmus, L. D. (1956). Friedlander bacillus infection of the lung.Quart. J. Med., 25, 507.
Gill, R. J. (1951). Treatment of Friedlander's pneumonia. Amer. J.med. Sci., 221, 5.
Greenberg, L. F., and Kahn, S. B. (1963). Klebsiella pneumonia withpneumothorax, pneumomediastinum, and pneumoperitoneum.Report of a case. Dis. Chest, 43, 546.
Holmes, R. B. (1956). Friedlander's pneumonia. Amer. J. Roentgenol.,86, 728.
Lampe, W. T. (1964). Klebsiella pneumonia. A review of 45 cases andre-evaluation of the incidence and antibiotic sensitivities. Dis.Chest, 46, 599.
Le Roux, B. T. (1965). Empyema thoracis. Brit. J. Surg., 52, 89.Limson, B. M., Romansky, M. J., and Shea, J. G. (1956). An evalua-
tion of 22 patients with acute and chronic pulmonary infectionwith Friedlander's bacillus. Ann. intern. Med., 44, 1070.
Marshall, G., and Perry, K. M. A. (1952). Diseases of the Chest.vol. I. Butterworth, London.
Oswald, N. C., Simon, G., and Shooter, R. A. (1961). Pneumonia inhospital practice. Brit. J. Dis. Chest, 55, 109.
Stevenson, J. G., Reid, J. M., McFarlane, N., and Barrie, J. D. (1961).The value of chloromycetin succinate used topically in intra-thoracic suppuration. Ibid., 55, 216.
175
on 11 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.22.2.170 on 1 March 1967. D
ownloaded from