emerging non-traditional biomarkers for assessing
TRANSCRIPT

EMERGING NON-TRADITIONAL BIOMARKERS FOR
ASSESSING LONG TERM RISK IN RENAL
TRANSPLANT RECIPIENTS
Hege K Pihlstrøm
Faculty of Medicine
University of Oslo
Section of Nephrology, Department of Transplant Medicine.
Oslo University Hospital Rikshospitalet
May 2015

© Hege K Pihlstrøm, 2016 Series of dissertations submitted to the Faculty of Medicine, University of Oslo ISBN 978-82-8333-176-9 ISSN 1501-8962 All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without permission. Cover: Hanne Baadsgaard Utigard Printed in Norway: 07 Media AS – www.07.no

3
Table of Contents
Acknowledgements
4
List of papers
6
Abbreviations
7
General introduction
9
Renal replacement therapy in Norway 9
Comorbidities in renal transplant recipients; short- and long term prognosis
12
Traditional /established risk factors
15
Emerging risk factors
18
Risk markers, risk factors and the concept of causality
18
Systemic inflammation and the macrophage activation marker neopterin
19
Endothelial dysfunction and the dimethylarginines, ADMA and SDMA
21
Hyperparathyroidism and bone- and mineral balance
24
The Alert Trial
27
Aims / Research questions
30
Patients and methods
31
Laboratory measurements and study population 31
Statistical analyses
33
Results
35
Discussion
41
Clinical implications and future perspectives
53
Reference list
56
Appendix: Paper 1-3
67

4
Acknowledgements
This thesis is based on studies which were carried out in the period 2013-2015 during my
position as a full time research fellow associated with the section of Nephrology, Department
of Organ Transplantation, Oslo University Hospital Rikshospitalet HF. I am most grateful for
the financial support of Helse Sør-Øst granting me three years of funding for my research,
which has led to the production and publication of the articles that this thesis is based on, as
well as the conduction of a randomized controlled trial (The ZEAL-study) comparing vitamin
D-agonist with placebo given to newly transplanted renal allograft recipients (the data
collection phase is now complete). Additionally, I want to thank The Norwegian Kidney
Association for their financial support in the form of a research grant. I am also grateful to the
University of Oslo for accepting me on the PhD program, and to Anna Varberg Reisæter and
Anders Åsberg for their highly qualified leadership as heads of the Department of Transplant
Medicine and the Laboratory of Renal Physiology, respectively.
My one-of-a-kind primary supervisor Hallvard Holdaas has to be considered the main
success factor for these studies. He has challenged me and given me the necessary “push”
now and then, while at the same time underscoring the importance of taking care of family
and personal life during valuable parenting years. His genuine enthusiasm for research and
scientific discussion is combined with an extraordinary ability to separate important caveats
and pitfalls from less important “noice”. He has taught me how to communicate a main
message in a structured way without posing too many speculative questions. I am deeply
grateful for his style of mentoring, which involves humor, care and immense support during
moments of stress and nervousness for the candidate.
All three papers are based on data from the ever-so-valuable ALERT –trial. Thanks to all
patients who participated in the study! They have made it possible, not only to investigate the
association between statin use and long term outcomes in this patient group, but to set the
stage for numerous publications looking at different aspects of patient and graft prognosis in
renal transplantation. Furthermore I want to thank all researchers, nurses, coordinators and
laboratory staff taking part in the ALERT trial for assembling such a great amount of data in a
very structured way. When intervention trial data are collected with precision and care for
completeness, it makes it possible for researchers like me to conduct well-designed
observational studies many years later. Several of the main investigators of the ALERT trial
are coauthors of the papers discussed in this thesis, namely Alan Jardine, Bengt Fellström,
Winfried März and Ingar Holme. I want to thank them for their positive attitude and valuable
insights which helped me prepare these manuscripts.

5
Also, a special thank s to Stefan Pilz, whom I have never met in person, but who as a
coauthor has played an important role during the revision process of all three manuscripts,
helping me getting them accepted for publication. Furthermore, my highly valued research
colleagues and friends, Dag-Olav Dahle and Geir Mjøen, have shown a great deal of
patience in the process of teaching a beginner the basic do´s and don´ts in epidemiology and
survival analysis. They have also been of great help in the writing process.
Futhermore, I want to express great gratitude to my additional supervisors, Anders
Hartmann, Karsten Midtvedt and My Svensson. Prof. Hartmann has been constantly
supportive, even though the proximity of his office to the renal lab made him subject to a
constant stream of clinical as well as scientific questions from PhD students. The feedback of
Dr Midtvedt has been invaluable, especially in the process of writing the paper on SDMA.
The way he makes time for questions and discussions, even in the middle of a busy clinical
schedule, is astonishing. Thank you, My, for constructive feedback on my presentations at
scientific congresses and for taking interest in my projects in spite of the physical distance.
I also have to thank my fellow PhD-student Ivar Eide for helping me get started with the
ZEAL-trial. He was the main architect behind the Case Report Files (CRFs) and, like Dag
Olav Dahle and Thea Anine Halden, he helped me take care of some study patients when I
had to stay home with sick kids (or husband). My gratitude goes to Elisabeth Størset for
creating beautiful figures in R for two of my manuscripts! Last, but not least, I want to thank
the medical staff at the Laboratory of Renal Physiology, Kirsten Lund, May-Ellen Lauritzen,
Els Breistein and Sebastian Müller for their great help in conducting the ZEAL-trial. You
made my days in the lab a lot easier, and the social aspect has been invaluable. Sorry for
having eaten at least 50% of the chocolate and biscuits that were brought to the lab….
Finally, I want to express my gratitude to my family, particularly to my husband Håvard. He
has been very flexible and supportive during the last three years. He has also been of great
help in the academic process by giving constructive feedback, “the outsider perspective”, on
presentations and manuscripts.
6
List of Papers
I. Hege Pihlstrøm, Geir Mjøen, Winfried März, Dag Olav Dahle, Sadollah Abedini, Ingar
Holme, Bengt Fellström, Alan Jardine, Stefan Pilz, Hallvard Holdaas
Neopterin is associated with cardiovascular events and all-cause mortality in renal
transplant patients
Clin Transplant 2014; 28(1):111-9.
II. Hege Pihlstrøm, Geir Mjøen, Dag Olav Dahle, Stefan Pilz, Karsten Midtvedt, Winfried
März, Sadollah Abedini, Ingar Holme, Bengt Fellström, Alan Jardine, Hallvard Holdaas
Symmetric Dimethylarginine as Predictor of Graft loss and All-Cause Mortality in
Renal Transplant Recipients.
Transplantation 2014; 98(11):1219-25.
III. Hege Pihlstrøm, Dag Olav Dahle, Geir Mjøen, Stefan Pilz, Winfried März, Sadollah
Abedini, Ingar Holme, Bengt Fellström, Alan G Jardine, Hallvard Holdaas
Increased risk of all-cause mortality and renal graft loss in stable renal transplant
recipients with hyperparathyroidism.
Transplantation 2015;99(2):351-9

7
Abbreviations
ADMA asymmetric dimethylarginine
ALERT Assessment of LEscol in Renal Transplantation
AZA azathioprine
CaR calcium-sensing receptor
CI confidence interval
CKD chronic kidney disease
CHD coronary heart disease
CNI calcineurin inhibitor
CKD chronic kidney disease
CRP C-reactive protein
CV cardiovascular
CVD cardiovascular disease
DD deceased donor
ED endothelial dysfunction
ECD expanded criteria donor
ESRD end stage renal disease
FGF-23 fibroblast growth factor-23
GFR glomerular filtration rate
HD hemodialysis
HLA human leucocyte antigen
HPT hyperparathyroidism
HR hazard ratio
IL-6 interleukine 6
IFN-γ interferon gamma
LD living donor
LDL low-density lipoprotein
MACE major cardiovascular events
MI myocardial infarction
MMF mycophenolate mofetil
NO nitric oxide
NOS nitric oxide synthase
NRI net reclassification improvement
PD peritoneal dialysis
PTH parathyroid hormone
PTHr1 PTH-receptor 1

8
ROS reactive oxygen species
ROC receiver operating curve
RCT randomized controlled trial
RRT renal replacement therapy
RTRs renal transplant recipients
SD standard deviation
SDMA symmetric dimethylarginine
TGFβ transforming growth factor beta
TNFα tumor necrosis factor alpha

9
General introduction
Transplantation in Norway
The first kidney transplantation in the Nordic countries was performed in 1956 at the
National Hospital by a team led by Leif Efskind(1). The patient survived one month
after the transplantation, but died of a heart attack during another surgical procedure.
The next four patients who underwent kidney transplantation in Norway (1960-1962)
all died within 40 days after the procedure, due to either acute rejection or
septicaemia. At Ullevål Hospital, in the year of 1963, the American surgeon R.E.
Wilson performed Norway´s first transplantation resulting in a long-term functioning
graft, introducing immunosuppressive treatment with Azathioprine (AZA)(2).
Scandiatransplant was established in 1969, an organisation for organ exchange
between the Scandinavian countries. A Norwegian renal transplant program was
launched, and its continuing success is dependent on co-operation between regional
and central hospitals and The Transplant Centre at the National Hospital. The
National Hospital (Rikshospitalet) has since 1983 been responsible for all solid organ
transplantations in Norway (3).
Since 1980, The Norwegian Renal Association has collected national data on renal
replacement therapy (RRT), and a formal registry (The Norwegian Renal Registry)
was constituted in 1994. Annual reports are published, containing updated
information on patients waitlisted for, or already receiving, RRT.
Given that kidney transplantation has been shown to improve both survival and
quality of life in patients with end-stage renal disease (ESRD) (4, 5), Norway is
aiming towards offering the option of kidney transplantation to all eligible uremic
patients within a reasonable time frame, and there is no upper age limit(6). In 2014, a
total of 16% of the patients on the waiting list were older than 70 years.
A total of 274 renal transplants were performed at The Transplant Centre at Oslo
University Hospital Rikshospitalet in 2014. In 68 (25%) of them the allograft came
from a living donor (Figure 1). In Norway, like in most other western societies, the
number of individuals in need of RRT is increasing steadily. The overall number of
transplants performed each year is varying between 50 and 60 per million of
population, which is among the highest frequencies in Europe (Figure 2).

10
By the end of 2014, 296 patients were on the active waiting list for a deceased donor
(DD) renal graft, a number that represented an 11% increase since 2013. Since the
end of 2012, the prevalent number of waitlisted patients has increased by more than
45%. Median time on the waiting list for patients who received a DD-graft in 2013
was 9 months, while for the 2014 - cohort of recipients, median time in waiting had
increased to 12 months. A steady high rate of living donation over the last decades is
one of the main reasons that DD-transplant recipients in Norway are spending
relatively short time in waiting for a suitable renal graft. However, we have seen a
slight tendency towards lower rates of living donations during the last couple of years.
Hence, to meet the enhanced demand for kidney transplants, we have been
encouraging the increased use of very old (>75 years) donors and expanded criteria
donors (ECD). This policy is supported by the rather satisfying results of a
retrospective quality control study evaluating the outcomes of single kidney
transplantations from donors older than 75 years(7).
Renal transplantations performed at Rikshospitalet 1969-2014
0
50
100
150
200
250
300
69 72 75 78 81 84 87 90 93 96 99 02 05 08 11 14
LD (n=2838)
DD (n=5011)
TL 01.15
Figure 1. Renal transplantations performed in Norway since 1969. Stratification by
type of kidney donor. LD= living donor, DD= deceased donor. Data from the
Norwegian Renal Registry.

11
Renal transplantation in 2013Graft sources and waiting lists ( ) pr. mill. pop.
0 25 50 75 100 125 150
USA
Australia
UK
Spain
France
Switzerl.
Netherl.
Belgium
Germany
Austria
Sweden
Finland
Denmark
Norway
DD LD
191
167
Figure 2. Renal transplantations performed in Norway in 2013 and patients on the
kidney transplant waiting list (per million population). Comparison with other western
countries. Data from the Norwegian Renal Registry.
Out of the total prevalent patient population on RRT in Norway, more that 70% are
transplant recipients. This is in contrast to other European countries like e.g.Italy,
where the frequency of transplantation per million inhabitants is about half that of
Norway(8). In our opinion, this large fraction of transplant recipients puts Norway in a
position where we have a particular responsibility: Continuing research efforts should
be made in this field, with the goal of optimizing patient- and graft survival.
Transplant medicine in Norway is centralized to the extent that only one hospital is
performing the surgery and taking care of the recipients during the first three months
of follow-up. Patients are then transferred back to their local nephrologists, but 12
months after transplantation they return to the Transplant Centre for a final routine
evaluation including a clinical examination, a complete laboratory work-up as well as
a protocol transplant biopsy. This centralized approach gives us unique opportunities
12
for standardizing the postoperative care of these patients, creating valuable
databases for future research as well conducting representative intervention trials.
Like in most other developed countries, the standard post transplant
immunosuppressive regimen in Norway has for several decades consisted of AZA,
one of the calcineurine inhibitors (CNIs), cyclosporine or tacrolimus, and low-doses of
oral steroids. A marked decrease in the incidence of acute rejection was achieved
world wide when mycophenolate mofetil (MMF) replaced AZA in the standard
regimen in 2001(9). Treatment with CNIs is associated with potentially harmful side
effects, including nephrotoxicity, but in lack of reliable evidence for the superiority of
newer drugs, the vast majority of patients globally are still on an immunosuppressive
regimen containing a CNI.
Comorbidities in renal transplant recipients; short- and long term prognosis
Though the main causes of renal failure are similar around the world, what is
etiologically most important in each society will vary somewhat according to
demographical factors like ethnicity/ genetic background of the population, age
distribution, lifestyle/ health behaviour as well as the quality of the health care
system. Type 2 diabetes is now the most prevalent cause of chronic kidney disease
globally(10). In the USA, much due to the increasing challenge of obesity in the
population, diabetic nephropathy is now responsible for 40.4% of newly developed
ESRD(11). In Norway, the scenario is slightly different, with diabetes nephropathy
being responsible for only 19% of patients starting RRT in 2013.The main change
over time has been an increase in vascular/hypertensive nephropathy (34%) and a
relative reduction of glomerulonephritis (16%) as primary cause of stage 5 CKD in
Norway, but one cannot rule out that this is merely a reflection of changes in coding
practice. Figure 3 depicts the main causes of ESRD for patients in Norway starting
RRT, illustrating the pattern of change in the dominating diagnoses over time (Data
from The Norwegian Renal Registry).

13
0
5
10
15
20
25
30
35
4080
-84
85-8
9
90-9
4
95-9
9
00-0
4
05-0
9
10-1
2Time period
Per
cen
t o
f in
cid
ent
case
s
Glomerulonephritis
Hypertension
Diabetes
Pyelo- /InterstitialnephritisCystic kidney disease
Gen. immunological
Other/Unknown
Primary cause of ESRD in Norway
Figure 3. Main causes of ESRD for patients embarking on RRT, by 5 year periods.
Data from the Norwegian Renal Registry.
In their landmark report, Wolfe et al(4) showed that transplant recipients had a 68%
decrease in mortality compared with those who remained on the wait list. This
survival advantage was also seen in older individuals. Guidelines on transplant
eligibility are now generally supportive of transplantation for older patients with
ESRD. As the mean age of transplant recipients is increasing, renal transplant
recipients (RTRs) today will naturally have more complex medical histories and larger
burden of comorbidity than before(12). Cardiovascular disease is frequent at start of
RRT. The Norwegian data report from 2013 indicates that coronary heart disease is
present in about 29%, anamnestic heart failure in 16%, left-ventricular hypertrophy in
22%, cerebrovascular disease in 17%, peripheral atherosclerotic disease in 15% and
chronic obstructive pulmonary disease in 10% of incident RTRs.
Despite steady improvements in short-term results after kidney transplantation over
the past decades, the global long-term prognosis for graft and patient survival has

14
improved minimally in comparison(13). Figure 4 presents Norwegian results for long-
term first DD-graft survival stratified by era of transplantation. From this figure it
becomes evident that our most recent results are in line with updated calculations for
the rest of Europe showing a 5 year graft survival of 77% and a 10 year survival of
56% (14). Norwegian figures are clearly more favourable than in the USA where the
5- and 10 year graft survival is 67% and 43%, respectively(14).
As a rule of thumb, half of the RTRs die with a functioning allograft, while the other
half lose their graft due to various causes(15). The leading causes of death in RTRs
are fatal cardiovascular events (30-48%), infections (17-30%) and malignancy (8-
18%)(16).
2 4 6 8 10 12 14 16 18 20
10
20
30
40
50
60
70
80
90
Survival of first renal DD graftsBy vintage. Norway 1969-2013
Years TL 02.14
2001-2006 n=707
Gra
ft S
urv
iva
l%
1995-2000 n=598
1989-1994 n=529
1983-1988 n=457
1969-1982 n=587
2007-2013 n=1159100
Figure 4. Long term outcomes among recipients of a first-time deceased donor
kidney transplant by graft vintage. Data from The Norwegian Renal Registry 2014.

15
Traditional / established risk factors
Type of kidney donor (LD,DD or ECD), donor and recipient age, number of human
leukocyte antigen (HLA) mismatches, presence of donor-specific antibodies, cold
ischemia time, ethnicity, and delayed graft function are the main pre- or perioperative
factors determining long term graft survival. In addition, stable glomerular filtration
rate (GFR) at 3-12 months after transplantation, degree of proteinuria, development
of chronic allograft dysfunction and factors related to the immuno-suppressive
regimen are important predictors(17). Chronic allograft dysfunction is presumably a
result of many intricate deleterious factors working together. For the individual
patient, there will be a combination of immune factors (clinical and subclinical
rejection, reactivation of dormant viral infections, treatment adherence) and non-
immune factors (hypertension, diabetes, anaemia, dyslipidaemia) potentially
exhibiting harmful influences on the allograft. Nephrotoxic effects of
immunosuppressive drugs have for the last 20-30 years been considered the major
cause of late allograft loss(18), though several recent review articles have claimed
that the role of CNIs in causing chronic graft dysfunction is exaggerated(19, 20).
Recurrence of native kidney disease, e.g. glomerulonephritis, will also pose a threat
to the graft.
The reduced patient survival in RTRs compared with other populations, might be
explained by interaction effects between a heavy burden of cardiovascular disease
(CVD) and infectious and neoplastic processes(21). Important cardiovascular (CV)
risk factors like diabetes, arterial hypertension and dyslipidemia are frequently
present in RTRs. However, these traditional risk factors cannot fully explain the
heightened CV mortality. Kasiske et al has shown that the Framingham risk score
underestimated risk in the transplanted population(22). In fact, about 40% of
transplanted patients experience one or more CV events during the first 10 years
after TX (23). Decreased GFR and proteinuria have both been independently
associated with coronary artery disease and all-cause mortality in community-based
studies(24-26). Some reduction in kidney function is usually present in RTRs, even
when the treatment course is judged otherwise satisfactory. Reduced GFR can
probably account for some of the increased CV-risk, as shown in a post-hoc analysis
from the Favorit Trial(27).Furthermore, immunosuppressive drugs are thought to

16
exaggerate the negative effects of CV risk factors(22). Using the Assessment of
Lescol in Renal Transplantation (ALERT) trial population, a formula for 7-year CVD
and mortality risk calculation for prevalent RTRs was developed(28). A seven-
variable model including age, previous coronary heart disease, diabetes, low-density
lipoprotein, creatinine, number of transplants, and smoking could predict the
occurrence of major adverse cardiac events. Total mortality could be predicted by the
six variables: age, coronary heart disease, diabetes, creatinine, total time on renal
replacement therapy, and smoking.
Figure 5 gives a summary of the main predictors of transplant and graft survival.
Figure 5. Early predictors of long-term transplant and patient survival.
Variables are listed in order of descending association with long-term survival.
Adaption from Bottomley M J , and Harden P N Br Med Bull 2013;106:117-134
The transplant community is continuously striving to further improve long term graft-
and patient survival in RTRs. The appropriate selection and matching of organ
recipients and donors, the optimization of peri- and postoperative care, the
Age
Comorbidities
Donor status (LD/DD/ECD)
Cause of death (traumatic or not)
S-creatinine from 3 mo after tx
Graft - recipient weight ratio
Donor-specific antibodies
Cold ischaemia time
Delayed graft function
Rejection episodes first y after tx
S-creatinine from 3 mo after tx
Proteinuria from 3 mo after tx
Age
Ethnicity
Comorbidities
Smoking
Time on dialysis
HLA mismatches
Prior transplantation
Panel reactive antibodies
Recipient - donor weight ratio
17
individualization of the immunosuppressive regimens, as well as the attentive
management of the relatively large burden of comorbidity are amongst possible
strategies to achieve better long-term results. Worldwide, use of living kidney donors
varies widely, from less than 10% to more than 75%(29). Most developed countries
encourage the use of living donors, as it is associated with a considerably better
short- and long time prognosis for the recipient(30). Even so, a decline in living
kidney donation has been observed recently, at least in the USA(31). One of the
strategies to combat organ shortage, is the increased use of more marginal organ
donors (ECD)(32). This shift might have an undesirable impact on outcome, but there
is reason to believe that if given to the right recipients, kidneys from older donors or
from donors suffering a cardiac death could serve as a means for expanding the
donor pool without affecting clinical outcomes significantly(33). Furthermore, it has
been shown that recipients of kidney allografts from elderly deceased donors (>65
years) have better survival than their paired counterparts remaining on dialysis(34).
The pursuit of efficient and tolerable CNI-free immunosuppressive regimens
continues to be a stimulus in drug development programs by the pharmaceutical
industry, much due to their presumed side effect of chronic nephrotoxicity, but also
due to their tendency to induce or aggravate diabetes and arterial hypertension.
Although the most important donor and recipient risk factors as well as peri- and
postoperative prognostic factors have been established, a full mapping of causes for
graft failure, CVD and premature death in RTRs remains to be completed. There is
an ongoing search for new and possibly modifiable risk factors in the hope of further
improving long term prognosis in these patients. The research process often begins
with the investigation of novel biomarkers for possible association with long term
outcomes, then the application of predictive statistical models, and consequently the
clinical intervention in causal factors. Important areas of focus include systemic
inflammation, endothelial dysfunction, oxidative stress, bone and mineral disease as
well as hormonal balance.

18
Emerging risk factors
Risk markers, risk factors and the concept of causality.
A risk marker refers to a measurable variable which shows statistically significant
associations with the subsequent clinical outcome of interest. An independent risk
marker should retain its statistical association with the outcome despite controlling for
other risk factors in a multivariate statistical model. Strictly speaking, a risk marker
cannot be considered a risk factor unless intervention to modulate this factor results
in parallel modulation of risk, given that possible confounding factors are taken into
account in the analysis.
Causality is (in science) defined as a relationship between one phenomenon or event
(A) and another (B) in which A precedes and causes B. The direction of influence and
the nature of the effect are predictable and reproducible and may be empirically
observed. Causality is difficult to prove, maybe even impossible, as seems to be the
opinion of some social scientists. Whether a variable could be considered a causal
risk factor, is not really a statistical question, but rather a matter of clinical and
biological knowledge acquired experimentally. A statistical association is necessary,
but not sufficient.
A well designed randomized controlled trial (RCT) is the optimal way to test causality
(e.g. intervention with a drug that is know to reduce the risk marker), but this
approach is not always feasible. Novel statistical methods for causal inference are
being developed for observational data, and a common denominator for such
methods is that datasets are transformed and weighted in order to mimic the
interventional trial setting, where there is exchangeability between treatment groups.
Such strategies include controlling for selection bias using propensity scores(35) and
inverse probability weighting(36), and dealing with multiple treatment times using
structural marginal models(37).
However, the establishment of an independent risk association from observational
data is often necessary before a successful RCT can be designed and conducted.
This thesis presents three such investigations of risk associations, the strengths of
which include a well defined-patient cohort, an extensive time of follow-up as well as
validated clinical end-points. Before summarizing and discussing the results of our

19
papers, I would like to give an overview of three important research areas, all
particularly relevant for RTRs, and show how the biomarkers we are studying place
themselves in this wider context.
Systemic inflammation and the macrophage activation marker neopterin
Chronic systemic inflammation is the result of release of pro-inflammatory molecules
(cytokines) from immune-related cells and the chronic activation of the innate
immune system. C-reactive protein (CRP), an established marker of systemic
inflammation, has been identified as an independent risk factor for CV disease and
CV death in several populations(38). At an early stage in chronic kidney disease
(CKD), a link between CRP and renal function is established(39), and in ESRD, the
association between CRP and risk of death and CV events is shown to be particularly
strong(40). The pro-inflammatory milieu in ESRD is probably due to increased
oxidative stress and chronic activation of various cell subsets belonging to the
immune system, and these phenomena are strongly inter-related(41). Renal
transplantation will ameliorate some of these imbalances, but some changes in
immune function are likely to persist. There is, in fact, evidence for enhanced
systemic inflammation in stable RTRs, even among those with low Framingham risk
scores(42).
There is evidence to suggest that systemic inflammation favours vascular
calcification(43, 44). The presence of calcification in the aorta has been associated
with coronary artery disease, stroke and heart failure in RTRs(45). Osteoprotegrin, a
glycoprotein involved in the regulation of vascular calcification processes, is
associated with mortality as well as renal and CV events in RTRs(46), and our group
has recently shown serum calcification propensity to be a strong and independent
determinant of cardiac and all-cause mortality in kidney transplant recipients (Dahle
et al, manuscript in press)
Inflammation is also a strong promoter in the atherosclerotic process. A central
inflammatory molecule, interleukine 6 (IL-6), triggers the synthesis of fibrinogen and
stimulates a pathway leading to thrombosis. In a stable renal transplant population
high sensitive CRP, as well as IL-6, was shown to be associated with major

20
cardiovascular events (MACE) and all-cause mortality(47) independent of traditional
risk factors, including measures of kidney function. An inflammatory glycoprotein,
TKL-40, which is expressed by macrophages in the earliest atherosclerotic lesions,
was shown to be elevated in RTRs(48). Another study has investigated the impact of
inflammatory cytokine polymorphisms on posttransplant CV-disease(49), concluding
that tumor necrosis factor-α (TNF-α) and interleukine -10 genotypes might represent
cardiovascular risk markers.
Neopterin (D-erythro-1-2-3-trihydroxypropylpterin), a rather specific marker of
macrophage activation, was hot in transplant research in the 1980s as a possible
predictor of acute rejections and viral infections in the postoperative setting, but has
since been somewhat “forgotten”(50). Neopterin is produced from guanosine
triphosphate (51) by activated human monocytes, monocyte-derived dendritic cells
and macrophages. During the cellular immune response, activated Th1-lymphocytes
release interferon-γ (IFN-γ), which again is the main stimulus for neopterin production
and release(52). IFN-γ will quickly bind to target structures or become neutralized by
soluble receptors, but neopterin is biochemical inert, and its serum concentration is
closely linked to the activity of the cellular immune system(53).
Neopterin is shown to be a marker of disease in a variety of conditions like viral
infections, inflammatory diseases, autoimmune diseases, neurodegenerative
diseases and certain forms of cancer (54), and elevated serum neopterin has
previously been associated with CV events and mortality in non-transplant
populations (50, 55). As a marker of cellular immune response activation depending
on IFN-γ release, neopterin may better reflect uremia-associated changes in the
immune system prevailing in kidney transplant recipients, than less specific markers
of inflammation. Neopterin level corresponds to the degree of cellular immune
activation, but also to the extent of oxidative stress involving production of reactive
oxygen species (ROS)(56). Neopterin may excert pro-oxidant properties itself, e.g. by
being able to intensify the effects of ROS (57). Though neopterin measured early
post transplant in kidney allograft recipients has been associated with subsequent
adverse events, in particular acute immunological and infectious complications(57,
58), the predictive value of neopterin for clinical outcomes in stable RTRs has not
been previously investigated.

21
Endothelial dysfunction and the dimethylarginines, ADMA and SDMA
The vascular endothelium carries far more biological functions than simply serving as
a barrier between the blood constituents and the tissues. Important functions include
modifying the coagulation process, assisting the immune response in the face of
antigen, controlling the exchange of fluid and molecules between the blood stream
and the tissues, as well as regulating vasoconstriction and vasodilatation. If one or
more of these tasks cannot be performed adequately, endothelial dysfunction (ED) is
present. However, when this concept is used in the literature, it almost invariably
refers to the establishment of an imbalance between dilating and constricting factors
produced in the endothelium(59, 60). Among these factors nitric oxide (NO), one of
the most potent dilators in the vasculature, is considered the most clinically important.
ED is believed to be the first initiating step in the process of atherosclerosis(61, 62)
and has been called the “risk of risk factors”, reflecting that it may be seen as a
common pathway through which much of the CV risk associated with other risk
factors is mediated(63). Conditions associated with an increased level of oxidative
stress(64) such as the traditional CV-risk mediators: diabetes, hypertension,
dyslipidemia, smoking and high age are all predisposing factors for ED. Furthermore,
a close relationship between inflammation and endothelial dysfunction has been
demonstrated in healthy volunteers, patients at risk, and patients with established CV
disease, thus providing a link between these two concepts(62).
When ED is established, the vasculature is predisposed to suffering repeated lesions
followed by remodelling, continuing inflammation, vasoconstriction, thrombotic events
as well as plaque rupture and erosion(65) (Figure 6). The presence of ED is
associated with a less favourable prognosis in patients with established CV
disease(66-68), and in the renal transplant setting, associations between clinical
measures of ED and long term outcomes have recently been demonstrated(69, 70).
The gold standard for measuring ED is angiographic estimation of the coronary artery
response to acetylcholine, given as the change in vessel diameter(71), though less
invasive methods are gaining acceptance(60). However, if endothelial function could
be easily assessed via blood tests, the value of ED as a risk stratification tool would
increase markedly. As a consequence, among the new molecules currently under

22
investigation as possible serum biomarkers for CV disease, we find several markers
potentially reflecting endothelial function(72).
.
Figure 6. Endothelial dysfunction as the “risk of the risk factors.” The endothelium
represents a mechanical and biological barrier between the blood and the vascular
wall. ´Endothelial Dysfunction- A Marker of Atherosclerotic Risk´ Bonetti et.al.,
Arterioscler Thromb Vasc Biol.2003, 23(2):168-75.
The dimethylarginine siblings, asymmetric dimethylarginine (ADMA) and symmetric
dimethylarginine (SDMA), are products of the process of protein turnover in the cells,
formed when constituent methylated arginine residues are released from intracellular
proteins. There is increasing evidence for a role of these molecules in ED as they
may interfere with NO-production. Asymmetric dimethylarginine (ADMA) has the
potential to reduce the levels of NO by inhibiting the enzyme nitric oxide synthase
(NOS) and limiting the uptake of L-arginine, the substrate for NOS, into endothelial
cells(73). ADMA has become an established risk factor for CV events and mortality in
different populations(74). The structural isomer symmetric dimethylarginine (SDMA)
has largely been overlooked in research, as it was believed to be a by-product of

23
metabolism without any biological activity. It has now become clear that though
SDMA does not directly inhibit NOS, it might indirectly reduce the activity of the
enzyme by limiting L-arginine supply (75, 76). In a very recent study of 64 CKD-
patients and 52 RTRs, a strong and predictable association was demonstrated
between hsCRP, SDMA and endothelial dysfunction (77). Figure 7 shows a simplified
overview of the pathways in which the dimethylarginines seem to be involved.
Interestingly, in addition to being involved in pathways central to endothelial function,
SDMA seems also to partake in inflammatory pathways. Mechanisms include
activation of nuclear factor kappa B (NF-κB) and increased expression of IL-6 and
TNF-α (78).
Figure 7. From ”The role of asymmetric and symmetric dimethylarginines in renal
disease” Schwedhelm et al.(79). CAT = cationic amino acid transporter.
Figure shown with permission from the author
Consequently, interest in this novel biomarker is on the rise, and SDMA has recently
been associated with mortality in several populations, including patients referred for
angiography (44, 80),patients having suffered an ischaemic stroke(81) and stable

24
patients with coronary heart disease(82). SDMA was found to independently predict
mortality in a large (n=3523) multi-ethnic cohort representative of the general
population(83).
Abedini et al conducted a post-hoc analysis from the ALERT trial(80) showing that
ADMA is associated with renal and cardiovascular outcomes as well as all-cause
mortality in renal transplant recipients. However, up until now the potential
association between SDMA level and long term outcomes in RTRs has not been
investigated separately. Busch et al studied a heterogenous population of CKD
patients, including 37 renal transplant recipients(84) for associations between the
dimethylarginines and long term outcomes. Their results pointed in the direction of an
association between elevated SDMA and progression to ESRD.
Hyperparathyroidism and bone- and mineral balance
Chronic kidney disease has a strong impact on the mineral and bone metabolism.
In ESRD, long lasting stimulation of the parathyroid gland by low serum calcium, low
levels of active vitamin D and high serum levels of phosphate will initially lead to
polyclonal hyperplasia(85). If uremia persists, these generalized diffuse changes will
frequently be followed by monoclonal nodular hyperplasia resulting in autonomous
hormone production (86). If such a state of autonomy is established, the condition is
less likely to resolve after renal transplantation(87).
Typically, by 6 months after transplantation, the parathyroid functional mass will be
markedly reduced, and parathyroid hormone (PTH) levels will have dropped by
approximately 50%(88). A more gradual decline is to be expected thereafter, but
complete normalization cannot be assured. In fact, hyperparathyroidism (HPT)
beyond 1 year after transplantation has been reported in up to 50% of RTRs (89, 90)
The main predisposing factors for such persistent HPT are high levels of serum
calcium, alkaline phosphatases and PTH at the time of transplantation, as well as
poor graft function and a prolonged time course of dialysis treatment before
transplantation(87, 91). Vitamin D-deficiency is very frequent in the post-transplant
setting, and this is also thought to contribute to the persistence of HPT (90, 92).
Recently, a central role for fibroblast growth factor 23 (FGF-23) in the regulation of
phosphate-vitamin D-PTH homeostasis has also been confirmed (93).

25
In addition to being acknowledged for its involvement in bone disease in different
populations, PTH has recently been launched as a novel CV risk marker(94). There
are receptors for PTH present in cardiomyocytes and the vessel walls(95), and this
might implicate direct effects of the hormone outside bone and kidney(96, 97).
Elevated PTH-levels are associated with reduced survival and increased CV
morbidity in patients with mild primary HPT (98), in the general population (99, 100),
and in patients referred for cardiac angiography(101). Furthermore, there is evidence
that both HPT and an altered vitamin D status contribute to the pattern of CV
pathology and excess mortality from CV causes seen in CKD-patients (102-104).
When it comes to RTRs, data on the possible effect of HPT on clinical outcomes are
limited. Associations between high levels of PTH and decreased bone mineral
density(105), as well as increased rate of fractures(106) have recently been
demonstrated in the transplant setting. Severe persistent HPT is frequently
associated with a chronically elevated level of serum calcium(107). There is evidence
for a detrimental effect of hypercalcemia, not only on bone metabolism, but also on
other tissues and organs, including the allograft(108, 109).
Potential effects of chronically elevated PTH in renal transplantation have been
suggested in a recent review by Evenepoel(110), from which Figure 8 is borrowed.
However, independent relationships between serum PTH and long term renal and
cardiovascular outcomes in renal transplantation have not been described previously.

26
Figure 8. In persistent HPT, inappropriately high PTH levels, along with high FGF23
levels, may cause allograft dysfunction and contribute
to the high burden of fractures and cardiovascular disease in renal transplant
recipients. NODAT, new-onset diabetes after transplantation; pHPT, persistent
hyperparathyroidism.
27
The Alert Trial
The ALERT trial (Assessment of LEscol in Renal Transplantation)(111) was a
double-blind randomized placebo-controlled study designed to evaluate the effect of
treatment with fluvastatin on long term CV outcomes in renal allograft recipients. Prior
to this study, the role of dyslipidemia and the effect of lipid lowering drugs had not
been fully established in RTRs(22, 112). Fluvastatin was the drug of choice in order
to minimize interactions with immunosuppressive therapy(113). The ALERT trial was
a multicenter study initiated and coordinated by The Section of Nephrology at Oslo
University Hospital, Rikshospitalet. 2102 clinically stable RTRs between the age of 30
and 75 were randomized to daily treatment with either fluvastatin or placebo, and
participants were followed for 5-6 years. All events (primary or secondary endpoints)
were registered and validated by an independent critical events committee consisting
of two nephrologists and two cardiologists blinded to treatment assignment. The
primary endpoint of the study was MACE (major cardiovascular events), and the
conclusions from the core trial was a 17% reduction in these events in the treatment
arm, though the result was statistically non-significant. Low density lipoprotein (LDL)-
cholesterol was significantly reduced, and the treatment was found to be safe and
well tolerated by the majority of participants. Secondary endpoints included individual
cardiac events, combined cardiac death or non-fatal myocardial infarction (MI),
combined cerebrovascular events, non-cardiovascular death; all-cause mortality, and
the composite renal endpoint of graft loss or doubling of serum creatinine. There was
a significant 35% reduction in combined cardiac deaths and non-fatal MI´s, an effect
size comparable to the beneficial effects of lipid lowering treatment in other
populations, while for the other secondary endpoints no significant treatment effect
was detected. Of course, in lack of a statistically significant primary efficacy analysis,
effect estimates for secondary endpoints will have to be interpreted with caution.
Available survey data from the year 1994 indicated a yearly 5% rate of MACE in
RTRs, and the power calculation for the ALERT trial was based on this assumption
and the suggestion of a 25% size effect of fluvastatin. However, the rate of events
turned out to be much lower than expected, probably due to the fact that the recruited
study population turned out to be stable RTRs with a rather moderate CV risk profile.
Most patients with pre-existing coronary heart disease were excluded, as the majority
28
of them were already using statins, and patients with a large burden of comorbidity
were probably not included due to complex therapeutic regimens. As the
investigators realized this early in the course of the trial, the number of patients
enrolled was increased. In order to maximize the potential value of the trial, the
dosage of fluvastatin was doubled about two years into the study period, mainly
because of emerging safety data and results from large clinical outcome trials, which
were not available at the time point when the ALERT was planned and designed.
These changes to the protocol was recommended by the Data Safety and Monitoring
board and implemented by the Steering Committee.
The lack of significant treatment effect in the primary efficacy analysis, despite the
above mentioned efforts, was most likely due to a combination of a low event rate in
the selected study population and the fact that as many as 32% of the patients in the
placebo group were actually using statins in the last year of the core trial follow-up.
This figure includes patients who at scheduled study visits presented with lipid levels
above protocol thresholds, as well as patients who were prescribed statins outside
the study by non-participating physicians.
In 2002, based on the findings of two large RCTs in the general population
demonstrating effective long-term prevention of CV events with lipid lowering
treatment, the Steering Committee decided to extend the ALERT trial another two
years, now offering treatment with fluvastatin 80 mg to all participants. Ninety-two
percent of the original study participants took part in the extension trial, and the
conclusion was a significant 21% reduction of MACE and a 29% reduction in the
composite endpoint “cardiac death or non-fatal myocardial infarction”(114). Hence,
the extension study established a cardioprotective effect of statin therapy in RTRs.
Soon after publication of these results, recommendations for statin therapy was
implemented into international guidelines and has now become mainstay as part of
the standard treatment protocol for this patient group(115, 116).
Several examples exist of larger interventional trials having provided extensive
datasets for further epidemiological research on risk factors and clinical outcomes in
the field of CKD and renal transplantation. The Aurora Study(117), the Favorit
Trial(118), and the 4D study (119) are amongst them. The LURIC trial, a prospective
29
cohort study of individuals with and without CV disease at baseline is an example of
a well designed trial aiming to provide a thoroughly characterized cohort for the study
of environmental and genetic risk factors, functional genomics and
pharmacogenomics(120). Likewise, in addition to seeking answers to the main
research question concerning the effectiveness of statins, the ALERT trial
established a valuable database for post-hoc research. Blood and urine was frozen at
time of inclusion, opening up the possibility of studying associations between
baseline levels of potential risk factors and the occurrence of validated cardiac and
renal end points up to 8 years later. Over the last decade, the ALERT cohort has
been the source of numerous investigations concerning statin safety and
effectiveness(121-126), risk prediction and stratification in RTRs (127-134), as well
as the identification of novel risk factors associated with long term outcomes(46, 47).
The papers presented in this thesis are, for now, the latest additions to this
substantial list of research.

30
Aims / Research questions
Considering that long term patient and graft survival in RTRs has shown only very
modest improvements over the last decades, there is an unmet need to identify new,
and possibly modifiable, risk factors for adverse outcomes. The general aim of this
thesis was to explore the possible value of a few such novel biomarkers in transplant
recipients. Causal inference is seldom possible based on observational studies like
these, but establishing associations between the level of a biomarker and future
outcomes in a population at risk, is often a necessary prerequisite for designing a
successful interventional trial where concepts of causality can be tested.
This thesis addresses the following questions, all of which have not been sufficiently
answered by previous research in the field:
I. Is neopterin, an inflammatory marker released from activated macrophages and
monocytes, an independent predictor of long term survival or cardiovascular / renal
outcomes in clinically stable RTRs?
II. Is SDMA, a novel marker of endothelial function and possibly a partaker in
inflammatory pathways, associated with long term outcomes (mortality or
cardiovascular / renal adverse events) in clinically stable RTRs?
III. Is persistent hyperparathyroidism after kidney transplantation associated with
poorer long term outcomes in RTRs?
31
Patients and methods
Laboratory measurements and study population.
For all three studies we used the ALERT database, and all baseline information was
available for each patient(135). The original participants were 2102 male and
female RTRs aged 30–75 years, included from June 1996 to October 1997. They had
received a renal transplant more than six months previously, had a stable graft
function and a total serum cholesterol concentration between 4.0–9.0 mmol/L (155–
348 mg/dL). Patients with familial hypercholesterolemia, a recent acute rejection
episode, or a predicted life expectancy of less than one year were excluded. Patients
already receiving statin therapy were not eligible for randomization.
For the ALERT trial, lipids, serum creatinine, creatine kinase and hepatic enzymes
were measured at a central laboratory (Eurofins Medinet) which has a solid
reputation and many years of experience in analyzing samples for clinical trials.
Several national and international agencies have previously evaluated their
performance, and so the ALERT Steering Committee did not independently supervise
the analytic process or validate the data. At baseline, samples of serum, plasma and
full blood were obtained from the majority of participants and frozen at minus 70° C.
Several pre-specified biomarkers were selected to be measured at a later time point,
and neopterin, SDMA and PTH were amongst these. At the end of the study, the
frozen samples were analysed at a central laboratory in Germany (Synlab
laboratories, Heidelberg) under the direction of Prof. Winfried März. Synlab
specializes in measuring a wide range of biomarkers in frozen samples, and again
the ALERT steering committee did not perform independent validation of
measurements. The methodology for measurement of neopterin, SDMA and PTH is
described in the individual papers.
For the studies described in paper I and III we used the whole ALERT cohort for
statistical analysis, and events registered in the extension trial period were also
included in the follow-up data. This choice of study population seemed justified by the
fact that initial statistical analyses revealed no heterogeneity between treatment arms
regarding the associations between the biomarkers and risk of outcomes.

32
However, for the study on SDMA we used the placebo group alone, analysing the
core trial follow-up data only. We made this choice because of evidence in the
literature supporting a possible effect of statins on endothelial function(136, 137), and
we wanted a `clean approach`. Moreover, initial statistical analyses revealed that the
association between high SDMA and adverse outcomes were markedly stronger in
the placebo arm than in the treatment arm, thus suggesting the presence of an
interaction between dimethylarginines and lipid lowering treatment(138).
Common for all three studies is that measurements of the serum levels of the
biomarkers, as well as the registration of relevant confounding variables, were
conducted at baseline only. Ideally one would like to have repeated measurements
throughout the follow up-period, but for such a large study cohort it was not possible
due to financial restrictions. We have to accept that the baseline value of a risk
marker might not reflect the mean exposure during follow up! There is also a
possibility of bias when risk estimation is confined to “single measurements”, this
being due to the possibility of measurement errors as well as the within-person
variability in the serum levels of the biomarkers. Regression dilution bias is a
statistical phenomenon which has been discussed in several methodological
publications(139, 140).
We are, however, somewhat reassured by the fact that mean levels of SDMA and
neopterin in the ALERT cohort seem in line with levels reported by other publications
in the field of renal transplantation(141-143). We acknowledge that PTH-values in
our cohort were substantially lower than what is reported in most observational
studies of RTRs(144, 145). Patients with the highest burden of comorbidity were not
included the ALERT, which might explain some of the discrepancy in PTH levels.
Also, mean time since last transplantation was longer than in most studies (>5 years),
allowing for parathyroid hyperplasia regression to have occurred.

33
Statistical analysis
The three studies presented in this thesis are methodologically fairly similar. After
having assessed baseline demographics and identified possible confounding
covariates, survival analyses were performed using MACE, all-cause mortality and
renal graft loss as the major clinical outcomes of interest.
Trends or variations in baseline demographics, risk factors and standard laboratory
measurements across categories of the exposure variables (quartiles/quintiles of
neopterin-to-creatinine ratio, SDMA and PTH) were analysed by ANOVA and χ2-
statistics. Results of unadjusted survival analyses were presented as Kaplan Meyer
curves or as Nelson-Aalen cumulative hazard plots, and Log Rank test was used to
compare survival distributions of groups.
In all of the three studies presented we performed Cox proportional hazard
regression; univariate calculations followed by multivariate analyses. The choice of
covariates to enter into the multivariate regression models was based on available
literature and clinical knowledge, but also the presence of significant associations
with the clinical outcomes in initial statistical analyses or significantly skewed
distributions across levels of the biomarker at interest. We chose not to apply
automatic model building procedures such as forward- or backward stepwise
inclusion of covariates, a decision made on the basis that they can be misleading, as
they do not consider the real-world importance of each predictor.
Correlations between biomarkers and other variables were calculated using
Spearman´s correlation test. This non-parametric correlation test was chosen since
biomarker levels did not show normal distributions in our population.
Levels of different biomarkers may to a varying extent reflect the same biological
pathways. Furthermore, if the molecules of interest are not metabolized in the body,
as is the case for SDMA and neopterin, serum levels may be strongly dependant on
the efficacy of renal elimination. In situations like these, correlation analyses will allow
for the evaluation of potential collinearity issues.
Collinearity (sometimes termed multicollinearity) is a statistical phenomenon in which
two or more predictor variables in a multiple regression model are highly correlated,

34
meaning that one can be linearly predicted from the others with a fair degree of
precision. In a Cox regression model this means that the hazard ratio (HR) estimates
may become unstable and change erratically in response to small changes in the
model or the data. If collinearity is present in a model, the affected coefficients will
tend to have large standard errors, and a type 2 error is more likely to be made. We
therefore made careful considerations before entering variables that showed a high
degree of statistical correlation together into our final regression models.
In all three studies, there were no obvious violations of the proportional hazard
assumption, judged by testing of Schoenenfeld residuals. Hazard ratios (HR) were
calculated with a 95% confidence interval (CI), both when comparing groups and
when using continuous exposure variables.
Increasing bias and variability, unreliable confidence interval coverage, and problems
with model convergency become the case if too many variables are included in the
regression model. Also the problem with missing data generally increases with the
number of covariates analysed. For the current studies, in the few cases where the
“rule” of at least ten events per adjusting variable(146) was relaxed, we chose to
seek expert statistical advice concerning the validity of the calculated HRs.
For the purpose of this thesis, we examined correlations between neopterin, SDMA
and PTH. Also, a multivariable regression model was constructed using all the three
biomarkers in focus, as well as the main traditional CV risk factors.
In the study of PTH, to guide our subsequent choice of statistical model, we applied a
restricted cubic spline method(147) for assessing if there was significant non-linearity
in the relationship between the exposure variable and clinical outcomes.
In the study of SDMA as a risk marker, possible competing risks between MACE (as
study endpoint) and all-cause mortality (as competing risk endpoint) were examined
by sensitivity analysis(148), including the sub-distribution hazards method described
by Fine and Gray(149).
Statistical analyses were performed mostly using SPSS version 18.0 (IBM, New
York,USA), but also STATA version 11 (StataCorp, College Station,Texas,USA) and
R Project for Statistical Computing (Free Software Foundation.Inc, Boston, MA).

35
Results
Paper 1: Neopterin is associated with cardiovascular events and all-cause mortality in
renal transplant patients.
This study used the ALERT cohort to investigate the association between serum level
of neopterin at time of inclusion and subsequent MACE, all-cause mortality and death
censored renal graft loss.
Neopterin values were available for 629 patients at baseline. Initial statistical analysis
revealed no relevant difference between trial participants with- or without available
neopterin measurements. The correlation coefficient between neopterin and
creatinine was 0.61, between neopterin and IL-6 was 0.26, while for neopterin and
CRP it was 0.14. All correlations were highly significant.
As has been done in the majority of previous studies on neopterin in populations with
compromised renal function, we calculated the neopterin-to-creatinine ratios for all
patients. Levels ranged from 33 to 325 μmol/mol, mean 96 (SD 42) μmol/mol. The
incidence of MACE and all-cause death was significantly higher in the fourth
neopterin/creatinine quartile compared with the first. For renal graft loss the event
rate was higher in quartile 4 than in quartile 1, but the difference was not statistically
significant.
Neopterin-to-creatinine ratio as a continuous variable was highly significantly
associated with all endpoints in the univariate Cox regression analysis. After
multivariate adjustments for established and potentially important risk factors, a
positive associated was found with all-cause of death (HR 1,06 per 10 units,
p=0.002,95% CI 1.02-1.09) and MACE (HR 1.06 per 10 units, p=0.009,95% CI 1.01-
1.10). We found no independent predictive value for graft loss, the association
between neopterin-to-creatinine ratio and outcome becoming markedly attenuated by
the inclusion of level of proteinuria in the multivariate model.
In this sub-cohort of ALERT, while neopterin was significantly associated with
outcomes, results were weaker for other markers of inflammation. Neither high

36
sensitive CRP nor IL-6 was independently associated with any of the study endpoints
in the multivariable analyses.
To our knowledge, this is the first study conducted in clinically stable RTRs
demonstrating an independent association between serum neopterin concentration
and the long-term clinical outcomes of MACE and all-cause mortality.

37
Paper 2: Symmetric Dimethylarginine as Predictor of Graft loss and All-Cause
Mortality in Renal Transplant Recipients.
Again the ALERT cohort provided a valuable database. We investigated the
association between serum level of SDMA at time of inclusion and subsequent long
term outcomes: MACE, renal graft loss and all-cause death. Sub-analyses also
explored the effect of having a high SDMA level on the three most important causes
of mortality. The study population consisted of ALERT participants in the placebo
group, and we used core trial data with a mean follow up of 5.1 years. 925 of the
1052 participants had available SDMA measurements at baseline (mean 1.20 (SD
0.48) μmol/L; range 0.46-4.41 μmol/L).
Correlations with SDMA had a coefficient of 0.77 for creatinine and -0.72 for
estimated GFR. Significant correlations were also found between SDMA and ADMA
(r=0.40). Correlations between SDMA and inflammatory markers were weak.
Due to apparent non-linear associations between the exposure variable and risk of
outcome, we split patients into quartiles based on their SDMA-values. SDMA showed
a positive association with all study outcomes in univariate analysis. After adjustment
for important possible confounders there was significantly increased risk of death (HR
4.56, 95% CI 2.15-9.71, p<0.001) and graft loss (HR 5.51, 95% CI 1.95-15.57,
p=0.001) in the highest SDMA quartile compared with the first. There was a non-
significant trend indicating increased risk of MACE with higher SDMA-values.
A surprisingly strong association was seen between SDMA and non-cardiovascular
death (HR 7.54, 95% CI 2.54-22.40, p<0.001). Compared with the first quartile there
was a more than nine-fold increase in the risk of dying from cancer and a more than
seven-fold increased risk of death by infection in the 4th SDMA quartile. Both
associations were highly statistically significant.
This study is the first to report that increased serum levels of SDMA, adjusted for
traditional and nontraditional risk factors, are associated with reduced long-term graft
and patient survival in RTRs; the reduced survival driven mainly by non-
cardiovascular causes.

38
Paper 3: Increased risk of all-cause mortality and renal graft loss in stable renal
transplant recipients with hyperparathyroidism.
The majority of patients in the ALERT cohort had available PTH-measurements at
time of inclusion, and in this study we explored the possible association between
persistent HPT and long term graft and patient survival, as well as MACE. Mean
follow up was 6.7 years. Mean serum PTH was 51.9 (SD 67.6) pg/mL,ranging as
wide as from 1.20 to 1007 pg/mL. All patients with HPT, as defined by the upper
reference level (65 pg/mL), were located in the fifth quintile. There were no clinically
significant differences in baseline variables between patients with available PTH-level
(n=1840) and the rest of the ALERT participants (n=262).
The correlation coefficient between PTH and creatinine was 0.28 (p<0.001), and
correspondingly for estimated GFR it was -0.28 (p<0.001). CRP was not significantly
correlated with PTH. Furthermore, there was no overall correlation between PTH and
serum calcium or serum phosphate.
Taking into account the possible non-linearity in associations between PTH and risk
of outcomes, we created univariate restricted cubic splines for serum PTH as a risk
factor for all-cause mortality and graft loss. While univariate analyses might indicate
non-linearity, in the multivariate analyses the tests for non-linear trend were non-
significant. Based on these initial statistical analyses we chose to evaluate serum
PTH both as a continuous variable and a categorical variable in the final Cox
Proportional Hazard Regression models.
In univariate analyses we found significant associations between continuous PTH
and all study outcomes. In multivariate analyses, there were still significant
associations with all-cause mortality (HR 1.042 (1.014-1.071), p=0.004) and graft loss
(HR 1.055 (1.030-1.081), p<0.001), though the risk was somewhat attenuated. For
MACE, the association was weak and far from significant (HR 1.014 (0.982-1.047)
p=0.393), but associations between PTH and fatal cardiovascular, cerebrovascular or
vascular events remained of comparable magnitude as for total mortality (HR 1.039
(1.000-1.079), p=0.050). We then compared patients with serum PTH > 65pg/ml to
those with normal/low values, finding a HR of 1.85 (1.41-2.42; p<0.001) for graft loss,

39
and a HR of 1.46 (1.12-1.92; p=0.006) for all-cause death. Similar results were seen
in quintile analyses.
In contrast to PTH, serum calcium and serum phosphate were not significant
predictors of mortality in the fully adjusted model. Higher phosphate levels and lower
calcium levels were associated with higher risk of graft loss.
Supplementary Risk marker comparison
Pathways of inflammation, endothelial function and bone-mineral disturbances are
intertwined. We were tempted, for the sake of this thesis, to assess the three
biomarkers relationship with each other. We found a strong correlation of 0.65
(p<0.001) between neopterin and SDMA, and correlation of 0.27 (p<0.001) between
neopterin and PTH. Between SDMA and PTH, the correlation was 0.31 (p<0.001).
Now using both treatment arms, analysing patients with available measurements of
all three markers (n= 595), we constructed a multivariate model which included the
most important cardiovascular risk factors: age, gender, diabetes mellitus, coronary
artery disease, systolic blood pressure (BP), estimated GFR and LDL. ADMA and
high sensitive CRP was also included for comparison (Tables 1 and 2).For all-cause
death we found that one standard deviation (SD) increase in neopterin was
associated with 30% increased risk, while one SD increase in SDMA increased the
risk by 35%. Both results were statistically significant.
For graft loss there were significant independent associations for SDMA (40%
increasd risk per SD) and PTH (14% increased risk per SD).

40
1 All-cause death
Exposure variables HR p-value
Risk relationships
per SD
95,0% CI for HR
Lower Upper
Age (years) 1,064 ,000 - 1,044 1,085
Gender ,897 ,602 - ,595 1,351
Diabetes mellitus 2,195 ,000 - 1,481 3,252
Coronary heart dis. 1,861 ,009 - 1,171 2,959
SystolicBP (mmHG) 1,002 ,654 4% incr risk per SD ,992 1,013
LDL (mmol/L) ,983 ,850 1% red risk per SD ,819 1,179
GFR (ml/min) 1,003 ,760 5% incr risk per SD ,984 1,022
Neopterin (nmol/L) 1,033 ,001 30% incr risk per SD 1,014 1,053
ADMA (μmol/L) 3,157 ,158 41% incr risk per SD ,641 15,558
SDMA (μmol/L) 1,727 ,022 35% incr. risk per SD 1,081 2,758
PTH (pg/mL) 1,001 ,449 7% incr risk per SD ,999 1,003
hsCRP (mg/L) 1,010 ,415 67% incr risk per SD ,987 1,033
2 Renal graft loss
Exposure variables HR p-value
Risk relationships
per SD
95,0% CI for HR
Lower Upper
Age (years) ,965 ,001 - ,945 ,986
Gender 1,451 ,109 - ,920 2,287
Diabetes mellitus 1,779 ,007 - 1,168 2,710
Coronary heart dis. 1,147 ,704 - ,566 2,327
SystolicBP (mmHG) 1,013 ,018 25% incr risk per SD 1,002 1,024
LDL (mmol/L) 1,074 ,439 8% incr risk per SD ,896 1,288
GFR (ml/min) ,949 ,000 83% red risk per SD ,928 ,971
Neopterin (nmol/L) 1,022 ,062 20% incr risk per SD ,999 1,045
ADMA (μmol/L) ,767 ,748 3% red risk per SD ,153 3,850
SDMA (μmol/L) 1,825 ,011 40% incr. risk per SD 1,151 2,896
PTH (pg/mL) 1,002 ,025 14% incr risk per SD 1,000 1,003
hsCRP (mg/L) 1,001 ,956 1% incr risk per SD ,977 1,025
Tables 1 and 2. Risk marker comparison; associations with patient and graft survival
expressed as HR per unit and per SD. HR; hazard ratio, SD; standard deviation,
CI;confidence interval.

41
Discussion
The current view on emerging cardiovascular risk markers seems to be that in the
low-risk general population, the contribution of novel markers to the total CV risk
estimation is quite modest. The “old” traditional risk factors are still the ones that
explain most of the variation in prognosis between individuals(150)
Even so, the scenario might be rather different in intermediate- to high risk
populations. The transplant recipient is frequently in a state of low-grade systemic
inflammation, will quite often have some degree of endothelial dysfunction and may
experience persistent derangements in parameters associated with bone- mineral
balance. Consequently, the renal transplant population is a patient group in which
there is frequent elevation of a number of emerging risk factors at the same time.
Based on this, there is a larger potential for new biomarkers to become of clinical
value.
In this thesis we have explored three rather promising emerging risk factors that
might eventually prove of clinical value in RTRs for risk estimation, and possibly risk
reduction. Most of the novel biomarkers being examined in CKD populations are
evaluated in a thorough and comprehensive review by Fassett et al(151). The most
promising novel risk markers in CKD seem to be the inflammation markers CRP and
IL-6, pro brain natriuretic peptide (proBNP) and troponin as markers of cardiac
dysfunction, ADMA as a marker of endothelial function, transforming growth factor -
β1 (TGF-β1) as a mediator of fibrosis and FGF-23 as mediator of fibrosis as well as
of cardiovascular disease(152) (Table 3) . Additionally, vitamin D seems to be of
importance in various functions including immune modulation, cardiac contractility
and bone health. Of these markers, reliable assays are available in clinical practice
for proBNP, CRP and troponin only.

42
Biomarker
Native kidney cohorts Transplant kidney cohorts
IL-6
All-cause and CV-mortality
MACE, all-cause mortality, doubling of serum creatinine and graft loss
CRP All-cause mortality and vascular stiffness
MACE and all-cause mortality
ProBNP All-cause mortality, progression of ESRD
Mortality
Troponin All-cause mortality, progression to ESRD
MACE and mortality
ADMA Endothelial dysfunction, vascular stiffness, progression of CKD
MACE and all-cause mortality
TGF-β Left ventricular hypertrophy in CKD, development of CKD.
Studied in CNI-toxicity and fibrosis.
FGF-23 Vascular calcification, CV-outcomes, progression to ESRD, mortality
Mortality, graft loss
1,25-OH Vit D 25-OH Vit D
Excess: arterial stiffness and vascular damage in CKD. Deficiency: hypertension/cardiac contractility, immune dysfunction
Deficiency: Post-tx malignancy.
IL-6, interleukine-6; MACE, major cardiovascular events; BNP, brain natriuretic peptide; CKD, chronic kidney disease; CRP, C-reactive protein; CNI, calcineurin inhibitor; ESRD, end stage renal disease; FGF, fibroblast growth factor, TGF; transforming growth factor.
Table 3. Promising novel biomarkers in CKD and their association with clinical
endpoints. (Adaption from DeSerres et al.(143)).
When it comes to renal transplant patients, so far most research efforts in biomarkers
have focused on the identification of rejection among recipients with graft
dysfunction. Though a substantial number of publications have described significant
associations of these markers with outcome, descriptions of formal evaluations of the
diagnostic performance of the proposed markers are rare.
Studies evaluating emerging biomarkers of CV-events and mortality in the transplant
setting are scarce. To summarize a few of the investigations, Abedini et al
demonstrated that ADMA was independently associated with long term
outcomes(80). IL-6 and CRP were also associated with major cardiovascular events

43
and all-cause mortality in the ALERT cohort (47), but the associations were markedly
weaker than for ADMA. Recently, FGF-23 was shown to be significantly and
independently associated with death and graft loss in RTRs(144). The work
presented in this thesis adds the investigations of three novel biomarkers to the
relatively short list of association studies conducted in this field. I will continue this
discussion by focusing on each paper individually.
Paper 1
In this study, we have shown that the inflammatory marker neopterin is significantly
associated with cardiovascular events and all-cause mortality in a large cohort of
RTRs from the ALERT trial. The increment in risk associated with higher neoterin-to-
creatinine ratio remained statistically significant after adjustment for conventional and
new risk factors.
Inflammation represents a non-traditional risk factor which is potentially important and
modifiable(153). In CKD-populations, chronically elevated levels of inflammatory
markers like IL-6 and CRP are predictive of increased CV risk (32, 154). Much of the
attention in the research area of systemic inflammation has been focused on these
two biomarkers. In a comprehensive review(152), DeSerres et al argue that it is
unlikely that the combined analyses of a broad spectre of inflammatory markers
(including a large range of cytokines) for estimating CV risk will prove more useful
that a selected, limited number of markers, due to the issues of collinearity and the
fact that they represent multiple facets of the same biological process.
However, in the uremic state, reduction in the number and function of lymphoid cells,
combined with normal or increased activity in the myeloid cell lines, is a frequent
feature. It has been shown that the cellular composition of the immune system does
not normalize after kidney transplantation, even if the level of systemic inflammation
and oxidative stress is markedly reduced(155). Levels of pro-inflammatory CD16+
monocytes are shown to remain high in RTRs independent of the type of
immunosuppression used or how long time has passed since the
transplantation(156). They preferentially produce proinflammatory cytokines,
including IFN-γ, and have been associated with subclinical aterosclerosis in
RTRs(157). This evidence suggests that persistent low-grade macrophage activation

44
and cytokine release might be a specific feature of the immune system in renal
transplant recipients, and that the degree of such activation is related to long term
CV- prognosis. The fact that baseline neopterin values were substantially higher in
our cohort compared to the general population(158)as well as patients with known
CV disease(159), is in harmony with this theory. Levels in our cohort are in line with
findings in clinically stable RTRs in other studies (160, 161).
We find it interesting that neopterin, a marker of macrophage activation, performs this
well in our multivariate analysis despite adjustments for both Il-6 and CRP, and that
the correlations between neopterin and the other markers of inflammation were
relatively weak. In the field of inflammation research, the utility of different biomarker
panels is under active investigation. Our results suggest that neopterin might be
evaluated for inclusion in such panels, especially if developed for the transplant
setting. We nevertheless acknowledge the challenge in establishing reference levels
and specific thresholds for these emerging inflammatory markers, including
neopterin, in the CKD/transplant setting.
According to our findings, neopterin does not seem independently associated with
renal graft loss. This might appear as contradictory to the findings of several groups
who have demonstrated significant associations between early post transplant
neopterin and subsequent adverse renal outcome(57, 162, 163). However, there are
differences in the design and conduction of these studies that could explain the
variation in conclusions. Our study population consisted of clinically stable recipients
with a reasonably good renal function, while the above mentioned publications
investigated neopterin measured in the immediate posttransplant period.
Furthermore, we chose to include level of proteinuria, an established risk marker for
poor patient and graft survival, as a plausible confounder in our final multivariate
regression model. This means that if some of the negative effect of having high
serum neopterin is mediated through pathways which increase urinary excretion of
protein, we will not be able to account for this in our risk estimates. Weimer et al
(142) reported significant associations between neopterin concentration one year
after transplantation and the subsequent development of chronic rejection and
chronic allograft dysfunction, but proteinuria was not included in their multivariable
analysis. Interestingly, if proteinuria is removed from our regression model, there is a

45
significant association between neopterin and graft loss after all with a 5% increase in
risk per 10 units increase in neopterin-to-creatinine ratio (HR 1.05, p=0.013). Whether
proteinuria is a confounder or a mediator in this clinical context is not fully known. Our
results should thus be interpreted as a suggestion that in RTRs neopterin does not
add significantly to the prognostic information given by the degree of proteinuria.
When investigating biomarkers whose elimination is highly dependant on GFR, how
to correctly adjust for the confounding effect of renal function, will necessarily be an
important issue in the statistical analysis. As neopterin is chemically inert and its
elimination is solely through the kidneys, compromised renal function leads to a rise
in serum neopterin that is not caused by increased inflammatory activity (164). As our
main interest lay in the fraction of the serum neopterin concentration determined by
degree of macrophage activation, we chose to express neopterin levels relative to the
level of serum creatinine. This is an approach used by most authors investigating this
biomarker in populations with compromised kidney function. Additionally, we included
serum creatinine as a separate covariate in the regression model to allow for
estimation of the independent association between renal function and endpoints.
Whether this represents a statistical over-correction could be discussed, but
collinearity in the model did not appear to be a problem, judging by the size of the
standard errors.
Diminished monocyte activity has been demonstrated in long-term stable kidney
transplant recipients (25). Measuring neopterin in a stable clinical post transplant
setting might actually be helpful in determining the intensity of immunosuppression,
as a low level of neopterin might be a reflection of sufficient suppression of the
immune response directed against the allograft. Several groups have proposed the
usage of neopterin measurements in clinical practice to guide dosage decisions. This
is an interesting aspect when discussing the possible practical value of neopterin as
a risk marker. We, however, did not have the necessary data to examine the possible
correlation between neopterin level and intensity of immunosuppressive treatment in
the ALERT cohort.

46
Paper 2
This study is the first in renal transplant recipients documenting an association
between increased serum levels of SDMA and reduced long-term graft and patient
survival after adjusting for traditional and novel cardiovascular risk factors. The
association with all-cause death seemed primarily driven by non-cardiovascular
causes.
SDMA has been shown to accumulate in the serum of patients with CKD(79). This is
mainly a result of impaired renal clearance, as the molecule is almost exclusively
eliminated by renal filtration. Claes et al (141) showed recently that patients with
ESRD generally have high serum SDMA, and after renal transplantation, the level
falls quickly until it is stabilized at levels similar to non-transplanted CKD patients
( matched for age, gender, estimated GFR and diabetic status). ADMA displayed a
more biphasic pattern in this study, and the metabolism of ADMA is different from
SDMA with only 20% being excreted through the kidney.
Before implying that a high SDMA level is in fact negatively associated with clinical
outcomes, one has to consider the possible confounding role of kidney function, as
was the case for neopterin. Our analyses is in line with the available literature,
reporting correlation coefficients ranging from - 0.70 to - 0,80 between SDMA and
various GFR estimates(165). Even though estimated GFR was included in our
multivariate regression model, we cannot claim to have made an optimal adjustment
for renal function. This is due to the fact that estimated GFR itself is less than perfect
as a measure of the true glomerular filtration rate. There is an ongoing attempt to
identify new and better markers of organ function for laboratory diagnostics. Some
authors have actually launched SDMA as a potentially better marker of renal function
than serum creatinine(166, 167). Hence residual confounding may be one of the
reasons for the associations we have demonstrated between SDMA and outcomes,
particularly when it comes to graft loss. We believe, however, that the degree of
association and the level of significance makes it unlikely that all statistical significant
results in our analyses should be explained by variations in unmeasured
confounders. Moreover, even if SDMA elevation in RTRs is mainly a reflection of

47
decreased renal elimination, the molecule may still play a part in biochemical
pathways or exert biological actions.
Novel biomarkers reflecting endothelial function are under investigation in many
patient populations, including patients with reduced kidney function. Given the
general interest in ADMA as a novel risk marker, and the previous findings of
associations between ADMA and long term outcomes in the ALERT cohort(80),
results of the current study are intriguing: When entering SDMA into our regression
model together with ADMA, the association of ADMA with graft loss and mortality
became markedly attenuated, even non-significant. SDMA thus seems to be an even
stronger predictor of adverse events than ADMA in our cohort. In the study of a
heterogenous population of CKD-patients(84), an increasing SDMA level could be
identified as a predictor for renal outcome whereas ADMA level could not, a
conclusion consistent with our findings. SDMA is still characterized by some authors
as a biochemically inactive substance, though there is increasing evidence pointing
towards the existence of biological effects. Suggested mechanisms include an
indirect influence on NO-synthesis, as well as a possible participation in inflammatory
pathways, as mentioned previously(79).
We have demonstrated an association between SDMA and mortality in RTRs,
This is in line with findings in several other populations (44, 80-82). While SDMA was
found to independently predict mortality in a large (n=3523) multiethnic cohort
representative of the general population; the associations for ADMA were less robust
in this material (83).
However, contrary to our expectations, SDMA seemed to be more convincingly
associated with death from cancer and infections, than from CV causes.
Furthermore, we were not able to demonstrate a significant association between
SDMA and MACE, a composite CV endpoint which included the “softer” events:
myocardial infarction and performance of a coronary artery revascularization
procedure. One interpretation of these findings is that the involvement of SDMA in
alternative biochemical pathways (e.g. pathways of inflammation or cell turnover) is
more important for long term outcomes than the proposed effect on NO availability
and endothelial function, which has invariably been linked with cardiovascular health.

48
Consistent with this theory, in a study of the role of dimethylarginines in patients with
stable coronary artery disease(82), the authors demonstrated significant
associations between SDMA and secondary CV events as well as mortality, but they
could not find clear association to outcomes for L-arginine (the substrate for NO-
production) or L-arginine/SDMA ratio. Furthermore, associations between ADMA
and study outcomes were generally weaker than for SDMA. The authors concluded
that mechanisms besides those involved in the synthesis of NO should be considered
for both dimethylarginines.
Though not fully elucidated at present, the molecular processes that regulate ADMA
and SDMA, and the pathways that transduce their biological function, might become
targets for intervention in renal disease. We agree with Paroni et al(168) who already
10 years ago suggested the determination of both dimethylarginines in the design of
future clinical trials in this field.
Paper 3
In the last paper we show persistent HPT after renal transplantation to be significantly
associated with all-cause mortality and adverse renal outcome. When looking at
cardiovascular, cerebrovascular, and vascular deaths combined, there was also a
borderline significant association to increased PTH, but there was no evidence for an
association between PTH and non-fatal manifestations of coronary heart disease.
When held up against the few other studies looking at PTH and hard endpoints in
RTRs, results are somewhat conflicting. In the study of 984 stable RTRs(144), whose
main focus was on the value of FGF-23 in predicting clinical outcomes, an
association between PTH and a composite endpoint of death and graft loss was
significant only in univariate analyses, disappearing after adjustment for GFR.
Features of their study population, which might explain some of this discrepancy,
include a cohort half the size of ours and a median serum-PTH almost twice the
value of that in our cohort.
In the study of Bleskestad et al(169), looking at RTRs with GFR >60ml/min 10 weeks
after transplantation, there was a significant association between PTH-level and a
composite clinical endpoint consisting of CV events, graft loss, and all-cause death..

49
While a J-shaped risk pattern for PTH was seen in this population, like in studies of
ESKD-patients(103), we, in our study, could not find significant increase in mortality
associated with PTH-values below reference. In evaluating these differences it is of
note that PTH levels in the cohort of Bleskestad to a large extent reflected pre-
transplantation values, PTH being measured rather early post transplant. Further
regression of parathyroid hyperplasia and reduction of tissue PTH resistance would
be expected in the majority of patients in the months to follow. In dialysis patients,
PTH-levels are almost invariably elevated, and modest increases in PTH (150-300
pg/ml) seem not associated with increased mortality(103, 170). In contrast, in RTRs
we find an increased risk of mortality already at the upper reference level of PTH,
65pg/mL. We believe our findings suggest that stable RTRs are more in line with the
general population(171, 172)as in contrast to dialysis populations, when it comes to
the risk profile for PTH and the level at which risk increases.
There is, as previously mentioned, evidence for an association between PTH-level
and mortality in several populations(98, 101, 170, 171) We consider our results to be
in concert with these studies. More surprising is the weaker association between PTH
and MACE in our data. High levels of PTH have been associated with
hypertension(173), left ventricular hypertrophy(174), clinical heart failure(175), as well
as coronary heart disease(100), and much of the negative effect of high PTH on
survival in different patient groups have been thought to involve the heart muscle and
the vessel walls via changes in the expression and function of both the PTH/ PTHrP-
receptor (PTHR1) and the calcium-sensing receptor (CaR)(176-179).
We postulate in our paper that in the transplant population persistent PTH elevation
might be less associated with the early traditional manifestations of coronary artery
disease than with arterial calcification, key processes of cardiac remodelling and the
development of cardiomyopathy. There are animal studies to support the involvement
of PTH in these pathways(180, 181), and if this theory holds true, it provides an
explanation for the stronger association of PTH to fatal than to non-fatal
cardiovascular events. Acute coronary syndrome is thought to account for
approximately half of the CV-deaths in RTRs(182), but in this patient group as well as
in dialysis patients(183, 184), increased incidence of cardiac dysfunction such as
heart failure and arrhythmias are important causes of heightened cardiovascular

50
mortality compared with the general population. Intriguingly, a recent study has
shown associations between elevated PTH and sudden cardiac death in older adults
without established CV disease(185).
Through the propensity for persistent HPT to induce chronic hypercalcemia(186) and
nephrocalcinosis(187, 188), an association between disturbances in bone- and
mineral balance and unfavourable graft outcome has been established previously. An
elevated calcium phosphate product six months after transplantation has been
associated with subsequent renal graft loss(108).
We are, however, the first group to show significant associations between PTH and
long term renal outcome independent of levels of serum minerals. Whether there is,
in fact, a causal pathway by which PTH may cause damage to the allograft is
unknown, but we allow ourselves to speculate that effects of PTH on the vasculature
supplying the graft may be involved(189, 190).
In the context of the general aim of this thesis, which is to address the value of
different novel biomarkers associated with clinical outcomes in RTRs, it is of interest
also to report the independent value of serum minerals as potential risk markers.
Previous studies have provided inconsistent results as to whether higher serum
phosphate and calcium levels are associated with increased all-cause mortality in
RTRs(191, 192). Our results are in concert with the study of Schaeffner et al, finding
no significant associations.
However, increasing levels of phosphate were independently associated with
increased risk of graft loss in our analyses (J-shaped risk curve), whilst a higher
serum calcium seemed protective of graft loss. Others have also encountered this
rather contradict association for calcium(192).Since we cannot claim to have the
optimal adjustment for kidney function in our multivariate analyses, the mechanism
for such a finding might be that the vitamin D deficiency accompanying loss of GFR
most often leads to reductions in serum calcium.
In conclusion, we dare to suggest that PTH is a novel risk marker for adverse patient
and graft survival in the renal transplant population. PTH levels might be of value for
risk stratification in this patient group.

51
Supplementary analyses
When examining possible novel risk markers, one has to take into account that there
is most likely a complex interplay between pathways involving inflammation,
endothelial dysfunction and mineral balance. Knowledge about the relative
contribution of these pathways to the total burden of risk is limited. Our
supplementary analyses revealed a strong correlation between SDMA and neopterin,
a finding which is rather expected, since both of these parameters are closely
dependant on GFR. More interestingly, in a multivariate Cox regression analysis with
GFR and other important traditional risk factors included as covariates, the hazard
ratios for each of the three biomarkers examined was to some extent affected by
including one or both of the other markers in the model.
This supplemental analysis is not meant to be prognostic and must be interpreted
with causion. Nevertheless, in this smaller sub-cohort of ALERT participants, it
seems like all three biomarkers retain independent assossiations with outcomes,
neopterin possibly showing the strongest association with all-cause mortality and
SDMA seeming the most important for graft loss. PTH seems convincingly
associated with renal graft loss, but no independent association was seen for
mortality when the other novel risk markers were included in the model.
However, the following aspect is important: Available treatment options for HPT
exists, both in the form of surgery and calcimimetic drugs. Furthermore, techniques
for measurement are validated and reference values are somewhat established.
Also, when evaluating the clinical effect of PTH-lowering treatments, it is the total
biological effect mediated through PTH, not just the possible independent pathways
that will be of interest.
In any case, while making comparisons between multiple markers is tempting, results
should be interpreted with caution, as conclusions will be of a speculative nature!
Causality in risk factor comparison should be addressed properly in a prognostic
paper using appropriate models for prediction.

52
Limitations
The limitations which have to be considered are basically the same for all three
papers in this thesis. Despite efforts to include an extensive number of potential
confounding variables in the multivariate analyses, we are not able to rule out
residual confounding. In practice, unmeasured confounders will always be an issue in
observational studies. In paper 3, for example, one would have liked to have
available measurements of other relevant biomarkers, such as FGF-23 and vitamin
D. Biomarkers like neopterin and SDMA, which are mainly eliminated from the body
by renal excretion, will naturally be strongly correlated with serum creatinine and
estimated GFR, Attempts to adjust for glomerular filtration rate in our multivariate
analyses will not be perfect, though, since estimated GFR and creatinine themselves
are not ideal markers of kidney function. Also, missing data for one or more important
covariates led to some patients having to be excluded from multivariate analyses in
all three studies.
Statistical associations between biomarkers and clinical outcomes cannot be
interpreted as representing causal relationships. The conduction of properly designed
interventional trials is necessary before one can arrive at conclusions about which
risk markers are truly causal risk factors.
Furthermore, the study population, a cohort from an RCT investigating the effect of
statin treatment in RTRs, is not necessarily representative of the general transplant
population. In particular, patients with the highest CV risk might have been excluded
due to knowledge emerging in the late 1990´s concerning benefits of lipid lowering
treatment in populations at risk. As mentioned before, the biomarker levels were only
measured once, at baseline. This prevents us from knowing, e.g. if high biomarker
levels in a patient were a constant feature during follow up, corresponding to the
mean “exposure”, or simply representative of the levels at that particular moment.
Due to the above mentioned concerns, and to the retrospective origin of the studies
presented, one should be careful before translating our findings into
recommendations for daily clinical practice.

53
Clinical implications and future perspectives
In this thesis I have analysed three different novel, or non-traditional, biomarkers for a
possible relationship with long term outcomes in renal transplant recipients. The main
goal of association-studies like these is to get closer to establishing whether the
biomarker of interest could be a useful target for intervention in order to modify risk in
the patient population. The next step after showing associations between the
biomarkers and outcomes would be writing a prognostic paper, along the lines of the
paper by Holme et al(121)who used the ALERT cohort to evaluate the predictive
ability of lipoprotein components to that of traditional risk factors. Analytical strategies
like receiver operating statistics (ROC) and net reclassification improvement (NRI)
could determine how well our biomarkers perform in the prediction of clinical events.
Paper 1
The findings in paper 1 led us to believe that neopterin could be an important marker
for risk stratification in RTRs. Others have suggested the use of neopterin as a
possible marker to guide immunosuppressive treatment intensity. No drug currently
on the market will reduce neopterin levels specifically, though a general increase in
the level of immunosuppression is associated with lower serum neopterin.
As previously mentioned, there are indications of an effector role for neopterin in
amplifying the effects of reactive oxygen species. It is unknown, however, whether a
therapeutic strategy of increasing the elimination of neopterin or inhibiting neopterin
production and release would prove fruitful in clinical practice. Clinical trials are
needed in order to determine if this biomarker should be considered a true causal
factor and not merely a risk marker.
Eventually, more research would also be needed in order to establish a target level
for neopterin in interventional settings. If calculating the neopterin-to-creatinine ratio
is the way to go in adjusting for compromised renal function, will also have to be
evaluated further.

54
Paper 2
In paper 2 we found a strong link between SDMA, a marker of endothelial function
and patient and graft survival in RTRs. This new risk marker may prove useful for risk
stratification in this high-risk population. As for most novel biomarkers, there is a
demand for both basic research and clinical trials before one can conclude that
knowing a patient ´s SDMA level would be of practical value in the clinical
management of the individual.
The somewhat surprising finding that SDMA was less associated with CV events and
more so with non-CV fatal events, has led us to believe that this molecule is indeed
more than an indirect inhibitor of NO-production. Inflammatory pathways and possibly
viral replication activity could be involved. However, whether the relationship between
elevated SDMA and unfavourable clinical outcomes is a causal one, has yet to be
elucidated.
Hopefully, future research will establish if an association with cancer and severe
infections holds true also in other patient groups. What are the levels of SDMA in
active malignancy or ongoing systemic infections, and how does it vary with the
intensity of the disease? SDMA might turn out to be an interesting marker for
malignancy or even for low-grade infectious activity in transplanted patients, and
possibly also other patient groups at risk.
In conclusion, RCTs are required in order to find out whether SDMA-lowering
therapeutic strategies actually may reduce the risk of graft loss and mortality in
RTRs. As previously proposed, both dimethylarginines should be measured and
evaluated in the course of such studies, in order to determine which marker might be
most useful in the different clinical settings.

55
Paper 3
In paper 3 we have investigated the value of PTH as a risk marker for long term
events in RTRs. Of the tree papers in the thesis, this is the one that in our opinion
may carry the most important clinical implications at present. Intervention trials with
PTH-lowering drugs are being conducted in the transplant population(193). The goal
of these trials has been mainly to establish the efficacy and safety of drugs like
cinacalcet for lowering of PTH..
Hopefully, RCTs designed to investigate long-term outcomes after PTH-lowering
treatment will follow the initial trials mentioned above. Judging from the study by
Evenepoel et al., the effects of calcimimetica on serum calcium and PTH seem
temporary, as values quickly reverted back to pre-treatment level after the treatment
was stopped. Economical issues might thus limit the possibilities of studying the
effect of drugs like cinacalcet on long term clinical outcomes in RTRs.
As for now, PTH has yet to be established as a definite causal risk factor for reduced
graft- and patient survival. This is reflected in the fact that despite an increased
interest in PTH as a potential multi-faceted risk factor, we still lack guidelines for the
prevention and treatment of persistent HPT in RTRs. Likewise, there is no
consensus on how to handle severe secondary HPT in ESRD patients being
considered for kidney transplantation.
We humbly suggest that our research adds to the notion that persistent HPT should
be actively treated, not only due to the risk of persistent hypercalcemia and
bone/mineral disturbances, but also due to the proposed negative effect of HPT on
long term graft and patient survival. Persistent hyperparathyroidism should be
recognized in this patient group, and the decision on whether or not to embark on
PTH-lowering treatment should probably be based on more than the levels of serum
minerals.

56
References
1. Thorsby E. [Transplantation medicine in Norway through 50 years]. Tidsskr Nor Laegeforen 2006;126:3305-10.
2. Enger E, Bergan F, Hoeg K, Malm OJ, Thorsby E. [Kidney transplantation at Ulleval hospital. A 7 year
material]. Tidsskr Nor Laegeforen 1971;91:1113-31. 3. Reisaeter AV. [Kidney transplantation in Norway--a historical perspective]. Tidsskr Nor Laegeforen 1999;119:3163-6. 4. Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on
dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999;341:1725-30.
5. Fujisawa M, Ichikawa Y, Yoshiya K, et al. Assessment of health-related quality of life in renal
transplant and hemodialysis patients using the SF-36 health survey. Urology 2000;56:201-6. 6. Reisaeter AV, Foss A, Hartmann A, Leivestad T, Midtvedt K. The kidney transplantation program in
Norway since 2000. Clin Transpl 2011:111-8. 7. Foss A, Heldal K, Scott H, et al. Kidneys from deceased donors more than 75 years perform acceptably
after transplantation. Transplantation 2009;87:1437-41. 8. International figures on Donation and Transplantation - 2010. Council of Europe. Newsletter Transplant
2011.
9. Pretagostini R, Rossi M, Berloco P, et al. Mofetil mycophenolate in renal transplantation. Transplant Proc 2001;33:1082-3.
10. Park CW. Diabetic kidney disease: from epidemiology to clinical perspectives. Diabetes Metab J
2014;38:252-60. 11. United States Renal Data System: USRDS Annual Data Report. National Institute of Diabetes and
Digestive and Kidney Diseases, 2013. 12. Knoll GA. Kidney transplantation in the older adult. Am J Kidney Dis 2013;61:790-7. 13. Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograft survival in the United States: a
critical reappraisal. Am J Transplant 2011;11:450-62. 14. Gondos A, Dohler B, Brenner H, Opelz G. Kidney graft survival in Europe and the United States:
strikingly different long-term outcomes. Transplantation 2013;95:267-74. 15. El-Zoghby ZM, Stegall MD, Lager DJ, et al. Identifying specific causes of kidney allograft loss. Am J
Transplant 2009;9:527-35. 16. Marcen R. Immunosuppressive drugs in kidney transplantation: impact on patient survival, and
incidence of cardiovascular disease, malignancy and infection. Drugs 2009;69:2227-43. 17. Legendre C, Canaud G, Martinez F. Factors influencing long-term outcome after kidney transplantation.
Transpl Int 2013;27:19-27. 18. Casey MJ, Meier-Kriesche HU. Calcineurin inhibitors in kidney transplantation: friend or foe? Curr
Opin Nephrol Hypertens 2011;20:610-5. 19. Rush D. The impact of calcineurin inhibitors on graft survival. Transplant Rev (Orlando) 2013;27:93-5.

57
20. Issa N, Kukla A, Ibrahim HN. Calcineurin inhibitor nephrotoxicity: a review and perspective of the evidence. Am J Nephrol 2013;37:602-12.
21. Hernandez D, Moreso F. Has patient survival following renal transplantation improved in the era of
modern immunosuppression? Nefrologia 2013;33:171-80. 22. Kasiske BL, Chakkera HA, Roel J. Explained and unexplained ischemic heart disease risk after renal
transplantation. J Am Soc Nephrol 2000;11:1735-43. 23. Aalten J, Hoogeveen EK, Roodnat JI, et al. Associations between pre-kidney-transplant risk factors and
post-transplant cardiovascular events and death. Transpl Int 2008;21:985-91. 24. Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting
from cardiovascular disease in the United States. J Am Soc Nephrol 2002;13:745-53. 25. Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal
replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol 2005;16:489-95.
26. Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of
cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003;108:2154-69.
27. Weiner DE, Carpenter MA, Levey AS, et al. Kidney function and risk of cardiovascular disease and
mortality in kidney transplant recipients: the FAVORIT trial. Am J Transplant 2012;12:2437-45. 28. Soveri I, Holme I, Holdaas H, Budde K, Jardine AG, Fellstrom B. A cardiovascular risk calculator for
renal transplant recipients. Transplantation 2012;94:57-62. 29. Salvadori M, Bertoni E. What's new in clinical solid organ transplantation by 2013. World J Transplant
2014;4:243-66. 30. Tarantino A. Why should we implement living donation in renal transplantation? Clin Nephrol
2000;53:suppl 55-63. 31. Salvadori M, Bertoni E. What's new in clinical solid organ transplantation by 2013. World J Transplant
2013;4:243-66. 32. Panichi V, Maggiore U, Taccola D, et al. Interleukin-6 is a stronger predictor of total and cardiovascular
mortality than C-reactive protein in haemodialysis patients. Nephrol Dial Transplant 2004;19:1154-60. 33. Singh SK, Kim SJ. Does expanded criteria donor status modify the outcomes of kidney transplantation
from donors after cardiac death? Am J Transplant 2013;13:329-36. 34. Lloveras J, Arcos E, Comas J, Crespo M, Pascual J. A Paired Survival Analysis Comparing
Hemodialysis and Kidney Transplantation From Deceased Elderly Donors Older Than 65 Years. Transplantation 2014.
35. Cotton CA, Cuerden MS, Cook RJ. Causal inference in nonrandomized studies via propensity score
methods. Transfusion 2011;51:2536-9. 36. Shen C, Li X, Li L, Were MC. Sensitivity analysis for causal inference using inverse probability
weighting. Biom J 2011;53:822-37. 37. McCulloch CE. Observational studies, time-dependent confounding, and marginal structural models.
Arthritis Rheumatol 2014. 38. Ridker PM. Clinical application of C-reactive protein for cardiovascular disease detection and
prevention. Circulation 2003;107:363-9.

58
39. Stuveling EM, Hillege HL, Bakker SJ, Gans RO, De Jong PE, De Zeeuw D. C-reactive protein is
associated with renal function abnormalities in a non-diabetic population. Kidney Int 2003;63:654-61. 40. Yeun JY, Levine RA, Mantadilok V, Kaysen GA. C-Reactive protein predicts all-cause and
cardiovascular mortality in hemodialysis patients. Am J Kidney Dis 2000;35:469-76. 41. Vaziri ND. Oxidative stress in uremia: nature, mechanisms, and potential consequences. Semin Nephrol
2004;24:469-73. 42. Mansell H, Rosaasen N, Dean J, Shoker A. Evidence of enhanced systemic inflammation in stable
kidney transplant recipients with low Framingham risk scores. Clin Transplant 2013;27:E391-9. 43. Tintut Y, Patel J, Territo M, Saini T, Parhami F, Demer LL. Monocyte/macrophage regulation of
vascular calcification in vitro. Circulation 2002;105:650-5. 44. Wang AY, Wang M, Woo J, et al. Cardiac valve calcification as an important predictor for all-cause
mortality and cardiovascular mortality in long-term peritoneal dialysis patients: a prospective study. J Am Soc Nephrol 2003;14:159-68.
45. DeLoach SS, Joffe MM, Mai X, Goral S, Rosas SE. Aortic calcification predicts cardiovascular events
and all-cause mortality in renal transplantation. Nephrol Dial Transplant 2009;24:1314-9. 46. Svensson M, Dahle DO, Mjoen G, et al. Osteoprotegerin as a predictor of renal and cardiovascular
outcomes in renal transplant recipients: follow-up data from the ALERT study. Nephrol Dial Transplant 2012;27:2571-5.
47. Abedini S, Holme I, Marz W, et al. Inflammation in renal transplantation. Clin J Am Soc Nephrol
2009;4:1246-54. 48. Malyszko J, Koc-Zorawska E, Malyszko J. YKL-40, a marker of cardiovascular disease and endothelial
dysfunction, in kidney transplant recipients. Transplant Proc 2014;46:2651-3. 49. La Manna G, Cappuccilli ML, Cianciolo G, et al. Cardiovascular disease in kidney transplant recipients:
the prognostic value of inflammatory cytokine genotypes. Transplantation 2010;89:1001-8. 50. De Rosa S, Cirillo P, Pacileo M, et al. Neopterin: from forgotten biomarker to leading actor in
cardiovascular pathophysiology. Curr Vasc Pharmacol 2011;9:188-99. 51. Reynolds JJ, Brown GM. The Biosynthesis of Folic Acid. Iv. Enzymatic Synthesis of Dihydrofolic Acid
from Guanine and Ribose Compounds. J Biol Chem 1964;239:317-25. 52. Gostner JM, Becker K, Fuchs D, Sucher R. Redox regulation of the immune response. Redox Rep 2013
18:88-94.
53. Huber C, Batchelor JR, Fuchs D, et al. Immune response-associated production of neopterin. Release from macrophages primarily under control of interferon-gamma. J Exp Med 1984;160:310-6.
54. Hoffmann G, Wirleitner B, Fuchs D. Potential role of immune system activation-associated production
of neopterin derivatives in humans. Inflamm Res 2003;52:313-21. 55. Mangge H, Almer G, Truschnig-Wilders M, Schmidt A, Gasser R, Fuchs D. Inflammation, adiponectin,
obesity and cardiovascular risk. Curr Med Chem 2010;17:4511-20. 56. Murr C, Widner B, Wirleitner B, Fuchs D. Neopterin as a marker for immune system activation. Curr
Drug Metab 2002;3:175-87. 57. Weiss G, Fuchs D, Hausen A, et al. Neopterin modulates toxicity mediated by reactive oxygen and
chloride species. FEBS Lett 1993;321:89-92.

59
58. Margreiter R, Fuchs D, Hausen A, et al. Neopterin as a new biochemical marker for diagnosis of allograft rejection. Experience based upon evaluation of 100 consecutive cases. Transplantation 1983;36:650-3.
59. Lerman A, Burnett JC, Jr. Intact and altered endothelium in regulation of vasomotion. Circulation
1992;86:III12-19. 60. Poredos P, Jezovnik MK. Testing endothelial function and its clinical relevance. J Atheroscler Thromb
2013;20:1-8. 61. Vanhoutte PM. Endothelial dysfunction: the first step toward coronary arteriosclerosis. Circ J
2009;73:595-601. 62. Trepels T, Zeiher AM, Fichtlscherer S. The endothelium and inflammation. Endothelium 2006;13:423-
9. 63. Bonetti PO, Lerman LO, Lerman A. Endothelial dysfunction: a marker of atherosclerotic risk.
Arterioscler Thromb Vasc Biol 2003;23:168-75. 64. Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ
Res 2000;87:840-4. 65. McGorisk GM, Treasure CB. Endothelial dysfunction in coronary heart disease. Curr Opin Cardiol
1996;11:341-50. 66. Munk PS, Butt N, Larsen AI. Endothelial dysfunction predicts clinical restenosis after percutaneous
coronary intervention. Scand Cardiovasc J 2011;45:139-45. 67. Schachinger V, Britten MB, Zeiher AM. Prognostic impact of coronary vasodilator dysfunction on
adverse long-term outcome of coronary heart disease. Circulation 2000;101:1899-906. 68. Heitzer T, Schlinzig T, Krohn K, Meinertz T, Munzel T. Endothelial dysfunction, oxidative stress, and
risk of cardiovascular events in patients with coronary artery disease. Circulation 2001;104:2673-8. 69. Dahle DO, Midtvedt K, Hartmann A, et al. Endothelial dysfunction is associated with graft loss in renal
transplant recipients. Transplantation 2013;95:733-9. 70. Dahle DO, Jenssen T, Holdaas H, et al. Uric acid and clinical correlates of endothelial function in
kidney transplant recipients. Clin Transplant 2014;28:1167-76. 71. Hasdai D, Lerman A. The assessment of endothelial function in the cardiac catheterization laboratory in
patients with risk factors for atherosclerotic coronary artery disease. Herz 1999;24:544-7. 72. Badimon L, Romero JC, Cubedo J, Borrell-Pages M. Circulating biomarkers. Thromb Res 2012;130
Suppl 1:S12-5. 73. Vallance P, Leone A, Calver A, Collier J, Moncada S. Endogenous dimethylarginine as an inhibitor of
nitric oxide synthesis. J Cardiovasc Pharmacol 1992;20 Suppl 12:S60-2. 74. Bouras G, Deftereos S, Tousoulis D, et al. Asymmetric Dimethylarginine (ADMA): a promising
biomarker for cardiovascular disease? Curr Top Med Chem 2013;13:180-200. 75. Closs EI, Basha FZ, Habermeier A, Forstermann U. Interference of L-arginine analogues with L-
arginine transport mediated by the y+ carrier hCAT-2B. Nitric Oxide 1997;1:65-73. 76. Bogle RG, MacAllister RJ, Whitley GS, Vallance P. Induction of NG-monomethyl-L-arginine uptake: a
mechanism for differential inhibition of NO synthases? Am J Physiol 1995;269:C750-6.

60
77. Memon L, Spasojevic-Kalimanovska V, Bogavac-Stanojevic N, et al. Assessment of endothelial dysfunction: the role of symmetrical dimethylarginine and proinflammatory markers in chronic kidney disease and renal transplant recipients. Dis Markers 2013;35:173-80.
78. Schepers E, Barreto DV, Liabeuf S, et al. Symmetric dimethylarginine as a proinflammatory agent in
chronic kidney disease. Clin J Am Soc Nephrol 2011;6:2374-83. 79. Schwedhelm E, Boger RH. The role of asymmetric and symmetric dimethylarginines in renal disease.
Nat Rev Nephrol 2011;7:275-85. 80. Abedini S, Meinitzer A, Holme I, et al. Asymmetrical dimethylarginine is associated with renal and
cardiovascular outcomes and all-cause mortality in renal transplant recipients. Kidney Int 2010;77:44-50.
81. Schulze F, Carter AM, Schwedhelm E, et al. Symmetric dimethylarginine predicts all-cause mortality
following ischemic stroke. Atherosclerosis 2010;208:518-23. 82. Siegerink B, Maas R, Vossen CY, et al. Asymmetric and symmetric dimethylarginine and risk of
secondary cardiovascular disease events and mortality in patients with stable coronary heart disease: the KAROLA follow-up study. Clin Res Cardiol 2013;102:193-202.
83. Gore MO, Luneburg N, Schwedhelm E, et al. Symmetrical Dimethylarginine Predicts Mortality in the
General Population: Observations From the Dallas Heart Study. Arterioscler Thromb Vasc Biol 2013 84. Busch M, Fleck C, Wolf G, Stein G. Asymmetrical (ADMA) and symmetrical dimethylarginine
(SDMA) as potential risk factors for cardiovascular and renal outcome in chronic kidney disease - possible candidates for paradoxical epidemiology? Amino Acids 2006;30:225-32.
85. Cunningham J, Locatelli F, Rodriguez M. Secondary hyperparathyroidism: pathogenesis, disease
progression, and therapeutic options. Clin J Am Soc Nephrol 2011;6:913-21. 86. Gioviale MC, Bellavia M, Damiano G, Lo Monte AI. Post-transplantation tertiary hyperparathyroidism.
Ann Transplant 2012;17:111-9. 87. Koch Nogueira PC, David L, Cochat P. Evolution of secondary hyperparathyroidism after renal
transplantation. Pediatr Nephrol 2000;14:342-6. 88. Bonarek H, Merville P, Bonarek M, et al. Reduced parathyroid functional mass after successful kidney
transplantation. Kidney Int 1999;56:642-9. 89. Bleskestad IH, Bergrem H, Leivestad T, Goransson LG. Intact parathyroid hormone levels in renal
transplant patients with normal transplant function. Clin Transplant 2011;25:E566-70. 90. Giannini S, Sella S, Silva Netto F, et al. Persistent secondary hyperparathyroidism and vertebral
fractures in kidney transplantation: role of calcium-sensing receptor polymorphisms and vitamin D deficiency. J Bone Miner Res 2010;25:841-8.
91. Torres A, Rodriguez AP, Concepcion MT, et al. Parathyroid function in long-term renal transplant
patients: importance of pre-transplant PTH concentrations. Nephrol Dial Transplant 1998;13 Suppl 3:94-7.
92. Lobo PI, Cortez MS, Stevenson W, Pruett TL. Normocalcemic hyperparathyroidism associated with
relatively low 1:25 vitamin D levels post-renal transplant can be successfully treated with oral calcitriol. Clin Transplant 1995;9:277-81.
93. Lafage-Proust MH. Does the downregulation of the FGF23 signaling pathway in hyperplastic
parathyroid glands contribute to refractory secondary hyperparathyroidism in CKD patients? Kidney Int 2010;77:390-2.

61
94. van Ballegooijen AJ, Reinders I, Visser M, Brouwer IA. Parathyroid hormone and cardiovascular disease events: A systematic review and meta-analysis of prospective studies. Am Heart J 2013;165:655-64, 664 e1-5.
95. Fitzpatrick LA, Bilezikian JP, Silverberg SJ. Parathyroid hormone and the cardiovascular system. Curr
Osteoporos Rep 2008;6:77-83. 96. Smogorzewski M, Zayed M, Zhang YB, Roe J, Massry SG. Parathyroid hormone increases cytosolic
calcium concentration in adult rat cardiac myocytes. Am J Physiol 1993;264:H1998-2006. 97. Schluter KD, Piper HM. Cardiovascular actions of parathyroid hormone and parathyroid hormone-
related peptide. Cardiovasc Res 1998;37:34-41. 98. Yu N, Donnan PT, Flynn RW, et al. Increased mortality and morbidity in mild primary
hyperparathyroid patients. The Parathyroid Epidemiology and Audit Research Study (PEARS). Clin Endocrinol (Oxf) 2010;73:30-4.
99. Hagstrom E, Hellman P, Larsson TE, et al. Plasma parathyroid hormone and the risk of cardiovascular
mortality in the community. Circulation 2009;119:2765-71. 100. Kamycheva E, Sundsfjord J, Jorde R. Serum parathyroid hormone levels predict coronary heart disease:
the Tromso Study. Eur J Cardiovasc Prev Rehabil 2004;11:69-74. 101. Pilz S, Tomaschitz A, Drechsler C, et al. Parathyroid hormone level is associated with mortality and
cardiovascular events in patients undergoing coronary angiography. Eur Heart J 2010;31:1591-8. 102. Rostand SG, Drueke TB. Parathyroid hormone, vitamin D, and cardiovascular disease in chronic renal
failure. Kidney Int 1999;56:383-92. 103. Floege J, Kim J, Ireland E, et al. Serum iPTH, calcium and phosphate, and the risk of mortality in a
European haemodialysis population. Nephrol Dial Transplant 2011;26:1948-55. 104. Natoli JL, Boer R, Nathanson BH, et al. Is there an association between elevated or low serum levels of
phosphorus, parathyroid hormone, and calcium and mortality in patients with end stage renal disease? A meta-analysis. BMC Nephrol 2013;14:88.
105. Heaf J, Tvedegaard E, Kanstrup IL, Fogh-Andersen N. Hyperparathyroidism and long-term bone loss
after renal transplantation. Clin Transplant 2003;17:268-74. 106. Perrin P, Caillard S, Javier RM, et al. Persistent hyperparathyroidism is a major risk factor for fractures
in the five years after kidney transplantation. Am J Transplant 2013;13:2653-63. 107. Torregrosa JV, Barros X. Management of hypercalcemia after renal transplantation. Nefrologia
2013;33:751-7. 108. Egbuna OI, Taylor JG, Bushinsky DA, Zand MS. Elevated calcium phosphate product after renal
transplantation is a risk factor for graft failure. Clin Transplant 2007;21:558-66. 109. Ozdemir NF, Elsurer R, Ibis A, Arat Z, Haberal M. Serum C-reactive protein surge in renal transplant
recipients: link with allograft survival. Transplant Proc 2007;39:934-7. 110. Evenepoel P. Recovery versus persistence of disordered mineral metabolism in kidney transplant
recipients. Semin Nephrol 2013;33:191-203. 111. Holdaas H, Fellstrom B, Jardine AG, et al. Effect of fluvastatin on cardiac outcomes in renal transplant
recipients: a multicentre, randomised, placebo-controlled trial. Lancet 2003;361:2024-31. 112. Bumgardner GL, Wilson GA, Tso PL, et al. Impact of serum lipids on long-term graft and patient
survival after renal transplantation. Transplantation 1995;60:1418-21.

62
113. Jardine A, Holdaas H. Fluvastatin in combination with cyclosporin in renal transplant recipients: a review of clinical and safety experience. J Clin Pharm Ther 1999;24:397-408.
114. Holdaas H, Fellstrom B, Cole E, et al. Long-term cardiac outcomes in renal transplant recipients
receiving fluvastatin: the ALERT extension study. Am J Transplant 2005;5:2929-36. 115. Maharjan N, Bedi U, Arora R, Bhandari S, Dahal P, Khosla S. Impact of statins on cardiovascular
outcomes in renal transplant recipients: a systematic review. Am J Ther 2011;18:e48-54. 116. Kasiske B, Cosio FG, Beto J, et al. Clinical practice guidelines for managing dyslipidemias in kidney
transplant patients: a report from the Managing Dyslipidemias in Chronic Kidney Disease Work Group of the National Kidney Foundation Kidney Disease Outcomes Quality Initiative. Am J Transplant 2004;4 Suppl 7:13-53.
117. Fellstrom BC, Jardine AG, Schmieder RE, et al. Rosuvastatin and cardiovascular events in patients
undergoing hemodialysis. N Engl J Med 2009;360:1395-407. 118. Bostom AG, Carpenter MA, Kusek JW, et al. Rationale and design of the Folic Acid for Vascular
Outcome Reduction In Transplantation (FAVORIT) trial. Am Heart J 2006;152:448 e1-7. 119. Wanner C, Krane V, Marz W, et al. Atorvastatin in patients with type 2 diabetes mellitus undergoing
hemodialysis. N Engl J Med 2005;353:238-48. 120. Winkelmann BR, Marz W, Boehm BO, et al. Rationale and design of the LURIC study--a resource for
functional genomics, pharmacogenomics and long-term prognosis of cardiovascular disease. Pharmacogenomics 2001;2:S1-73.
121. Holme I, Fellstrom B, Jardine A, Holdaas H. Comparison of predictive ability of lipoprotein
components to that of traditional risk factors of coronary events in renal transplant recipients. Atherosclerosis 2009;208:234-9.
122. Fellstrom B, Abedini S, Holdaas H, Jardine AG, Staffler B, Gimpelewicz C. No detrimental effect on
renal function during long-term use of fluvastatin in renal transplant recipients in the Assessment of Lescol in Renal Transplantation (ALERT) study. Clin Transplant 2006;20:732-9.
123. Fellstrom B, Holdaas H, Jardine AG, et al. Effect of fluvastatin on renal end points in the Assessment of
Lescol in Renal Transplant (ALERT) trial. Kidney Int 2004;66:1549-55. 124. Jardine AG, Holdaas H, Fellstrom B, et al. Fluvastatin prevents cardiac death and myocardial infarction
in renal transplant recipients: post-hoc subgroup analyses of the ALERT Study. Am J Transplant 2004;4:988-95.
125. Singer JB, Holdaas H, Jardine AG, et al. Genetic analysis of fluvastatin response and dyslipidemia in
renal transplant recipients. J Lipid Res 2007;48:2072-8. 126. Holdaas H, Fellstrom B, Jardine AG, et al. Beneficial effect of early initiation of lipid-lowering therapy
following renal transplantation. Nephrol Dial Transplant 2005;20:974-80. 127. Abedini S, Holme I, Fellstrom B, et al. Cerebrovascular events in renal transplant recipients.
Transplantation 2009;87:112-7. 128. Fellstrom B, Holdaas H, Jardine AG, et al. Risk factors for reaching renal endpoints in the assessment
of Lescol in renal transplantation (ALERT) trial. Transplantation 2005;79:205-12. 129. Fellstrom B, Jardine AG, Soveri I, et al. Renal dysfunction is a strong and independent risk factor for
mortality and cardiovascular complications in renal transplantation. Am J Transplant 2005;5:1986-91. 130. Jardine AG, Fellstrom B, Logan JO, et al. Cardiovascular risk and renal transplantation: post hoc
analyses of the Assessment of Lescol in Renal Transplantation (ALERT) Study. Am J Kidney Dis 2005;46:529-36.

63
131. Soveri I, Abedini S, Holdaas H, Jardine A, Eriksson N, Fellstrom B. Graft loss risk in renal transplant
recipients with metabolic syndrome: subgroup analyses of the ALERT trial. J Nephrol 2012;25:245-54. 132. Oien CM, Reisaeter AV, Os I, Jardine A, Fellstrom B, Holdaas H. Gender-associated risk factors for
cardiac end points and total mortality after renal transplantation: post hoc analysis of the ALERT study. Clin Transplant 2006;20:374-82.
133. Schjelderup P, Dahle DO, Holdaas H, et al. Anemia is a predictor of graft loss but not cardiovascular
events and all-cause mortality in renal transplant recipients: follow-up data from the ALERT study. Clin Transplant 2013;27:E636-43.
134. Soveri I, Holdaas H, Jardine A, Gimpelewicz C, Staffler B, Fellstrom B. Renal transplant dysfunction--
importance quantified in comparison with traditional risk factors for cardiovascular disease and mortality. Nephrol Dial Transplant 2006;21:2282-9.
135. Holdaas H, Fellstrom B, Holme I, et al. Effects of fluvastatin on cardiac events in renal transplant
patients: ALERT (Assessment of Lescol in Renal Transplantation) study design and baseline data. J Cardiovasc Risk 2001;8:63-71.
136. Asberg A, Hartmann A, Fjeldsa E, Holdaas H. Atorvastatin improves endothelial function in renal-
transplant recipients. Nephrol Dial Transplant 2001;16:1920-4. 137. Reriani MK, Dunlay SM, Gupta B, et al. Effects of statins on coronary and peripheral endothelial
function in humans: a systematic review and meta-analysis of randomized controlled trials. Eur J Cardiovasc Prev Rehabil 2011;18:704-16.
138. Vladimirova-Kitova LG, Deneva-Koycheva TI. The effect of simvastatin on asymmetric
dimethylarginine and flow-mediated vasodilation after optimizing the LDL level: a randomized, placebo-controlled study. Vascul Pharmacol 2012;56:122-30.
139. Wood AM, White I, Thompson SG, Lewington S, Danesh J. Regression dilution methods for meta-
analysis: assessing long-term variability in plasma fibrinogen among 27,247 adults in 15 prospective studies. Int J Epidemiol 2006;35:1570-8.
140. Hutcheon JA, Chiolero A, Hanley JA. Random measurement error and regression dilution bias. Bmj
2010;340:c2289. 141. Claes KJ, Bammens B, Kuypers DR, et al. Time course of asymmetric dimethylarginine and symmetric
dimethylarginine levels after successful renal transplantation. Nephrol Dial Transplant 2014;29:1965-72.
142. Weimer R, Susal C, Yildiz S, et al. Post-transplant sCD30 and neopterin as predictors of chronic
allograft nephropathy: impact of different immunosuppressive regimens. Am J Transplant 2006;6:1865-74.
143. Lee PH, Huang MT, Chung YC, et al. Monitoring of serum neopterin in renal transplant recipients. J
Formos Med Assoc 1992;91:1209-12. 144. Wolf M, Molnar MZ, Amaral AP, et al. Elevated fibroblast growth factor 23 is a risk factor for kidney
transplant loss and mortality. J Am Soc Nephrol 2011;22:956-66. 145. Sanchez Fructuoso AI, Maestro ML, Perez-Flores I, et al. Serum level of fibroblast growth factor 23 in
maintenance renal transplant patients. Nephrol Dial Transplant 2012;27:4227-35. 146. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox
regression. Am J Epidemiol 2007;165:710-8. 147. Desquilbet L, Mariotti F. Dose-response analyses using restricted cubic spline functions in public health
research. Stat Med 2010;29:1037-57.
64
148. Thabane L, Mbuagbaw L, Zhang S, et al. A tutorial on sensitivity analyses in clinical trials: the what,
why, when and how. BMC Med Res Methodol 2013;13:92. 149. Fine J, Gray R. A proportional hazards model for the subdistribution of a competing risk. J Am Stat
Assoc. 1999;94:496-509. 150. De Backer GG. New risk markers for cardiovascular prevention. Curr Atheroscler Rep 2014;16:427. 151. Fassett RG, Venuthurupalli SK, Gobe GC, Coombes JS, Cooper MA, Hoy WE. Biomarkers in chronic
kidney disease: a review. Kidney Int 2011;80:806-21. 152. De Serres SA, Varghese JC, Levin A. Biomarkers in native and transplant kidneys: opportunities to
improve prediction of outcomes in chronic kidney disease. Curr Opin Nephrol Hypertens 2012;21:619-27.
153. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women
with elevated C-reactive protein. N Engl J Med 2008;359:2195-207. 154. Barreto DV, Barreto FC, Liabeuf S, et al. Plasma interleukin-6 is independently associated with
mortality in both hemodialysis and pre-dialysis patients with chronic kidney disease. Kidney Int 2010;77:550-6.
155. Betjes MG. Immune cell dysfunction and inflammation in end-stage renal disease. Nat Rev Nephrol
2013;9:255-65. 156. Scherberich JE, Estner H, Segerer W. Impact of different immunosuppressive regimens on antigen-
presenting blood cells in kidney transplant patients. Kidney Blood Press Res 2004;27:177-80. 157. Ulrich C, Heine GH, Gerhart MK, Kohler H, Girndt M. Proinflammatory CD14+CD16+ monocytes are
associated with subclinical atherosclerosis in renal transplant patients. Am J Transplant 2008;8:103-10. 158. Schennach H, Murr C, Gachter E, Mayersbach P, Schonitzer D, Fuchs D. Factors influencing serum
neopterin concentrations in a population of blood donors. Clin Chem 2002;48:643-5. 159. Ray KK, Morrow DA, Sabatine MS, et al. Long-term prognostic value of neopterin: a novel marker of
monocyte activation in patients with acute coronary syndrome. Circulation 2007;115:3071-8. 160. Wolf J, Musch E, Neuss H, Klehr U. [Neopterin in the serum and urine in the differential diagnosis of
disorders of kidney function following kidney transplantation]. Klin Wochenschr 1987;65:225-31. 161. Kameoka H, Takahara S, Takano Y, et al. Serum and urinary neopterin as markers in renal transplant
patients. Int Urol Nephrol 1994;26:107-15. 162. Grebe SO, Kuhlmann U, Fogl D, Luyckx VA, Mueller TF. Macrophage activation is associated with
poorer long-term outcomes in renal transplant patients. Clin Transplant 2011;25:744-54. 163. Carey BS, Jain R, Adams CL, et al. Serum neopterin as an indicator of increased risk of renal allograft
rejection. Transpl Immunol 2013;28:81-5. 164. Aulitzky WE, Tilg H, Niederwieser D, et al. Comparison of serum neopterin levels and urinary
neopterin excretion in renal allograft recipients. Clin Nephrol 1988;29:248-52. 165. Kielstein JT, Salpeter SR, Bode-Boeger SM, Cooke JP, Fliser D. Symmetric dimethylarginine (SDMA)
as endogenous marker of renal function--a meta-analysis. Nephrol Dial Transplant 2006;21:2446-51. 166. Bode-Boger SM, Scalera F, Kielstein JT, et al. Symmetrical dimethylarginine: a new combined
parameter for renal function and extent of coronary artery disease. J Am Soc Nephrol 2006;17:1128-34.
65
167. Fliser D, Kronenberg F, Kielstein JT, et al. Asymmetric dimethylarginine and progression of chronic kidney disease: the mild to moderate kidney disease study. J Am Soc Nephrol 2005;16:2456-61.
168. Paroni R, Fermo I, Fiorina P, Cighetti G. Determination of asymmetric and symmetric
dimethylarginines in plasma of hyperhomocysteinemic subjects. Amino Acids 2005;28:389-94. 169. Bleskestad IH, Bergrem H, Leivestad T, Hartmann A, Goransson LG. Parathyroid hormone and clinical
outcome in kidney transplant patients with optimal transplant function. Clin Transplant 2014;28:479-86. 170. Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism,
mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol 2004;15:2208-18. 171. van Ballegooijen AJ, Reinders I, Visser M, et al. Serum parathyroid hormone in relation to all-cause
and cardiovascular mortality: the Hoorn study. J Clin Endocrinol Metab 2013;98:E638-45. 172. Bjorkman MP, Sorva AJ, Tilvis RS. Elevated serum parathyroid hormone predicts impaired survival
prognosis in a general aged population. Eur J Endocrinol 2008;158:749-53. 173. Snijder MB, Lips P, Seidell JC, et al. Vitamin D status and parathyroid hormone levels in relation to
blood pressure: a population-based study in older men and women. J Intern Med 2007;261:558-65. 174. Saleh FN, Schirmer H, Sundsfjord J, Jorde R. Parathyroid hormone and left ventricular hypertrophy.
Eur Heart J 2003;24:2054-60. 175. Khouzam RN, Dishmon DA, Farah V, Flax SD, Carbone LD, Weber KT. Secondary
hyperparathyroidism in patients with untreated and treated congestive heart failure. Am J Med Sci 2006;331:30-4.
176. Huang Z, Li J, Jiang Z, Qi Y, Tang C, Du J. Effects of adrenomedullin, C-type natriuretic peptide, and
parathyroid hormone-related peptide on calcification in cultured rat vascular smooth muscle cells. J Cardiovasc Pharmacol 2003;42:89-97.
177. Torres PA, De Broe M. Calcium-sensing receptor, calcimimetics, and cardiovascular calcifications in
chronic kidney disease. Kidney Int 2012;82:19-25. 178. Alam MU, Kirton JP, Wilkinson FL, et al. Calcification is associated with loss of functional calcium-
sensing receptor in vascular smooth muscle cells. Cardiovasc Res 2009;81:260-8. 179. Fritsch S, Lindner V, Welsch S, et al. Intravenous delivery of PTH/PTHrP type 1 receptor cDNA to rats
decreases heart rate, blood pressure, renal tone, renin angiotensin system, and stress-induced cardiovascular responses. J Am Soc Nephrol 2004;15:2588-600.
180. Custodio MR, Koike MK, Neves KR, et al. Parathyroid hormone and phosphorus overload in uremia:
impact on cardiovascular system. Nephrol Dial Transplant 2012;27:1437-45. 181. Bogin E, Massry SG, Harary I. Effect of parathyroid hormone on rat heart cells. J Clin Invest
1981;67:1215-27. 182. Ojo AO. Cardiovascular complications after renal transplantation and their prevention. Transplantation
2006;82:603-11. 183. Herzog CA, Mangrum JM, Passman R. Sudden cardiac death and dialysis patients. Semin Dial
2008;21:300-7. 184. Ghanta M, Kozicky M, Jim B. Pathophysiologic and Treatment Strategies for Cardiovascular Disease in
End Stage Renal Disease and Kidney Transplantation. Cardiol Rev 2014. 185. Deo R, Katz R, Shlipak MG, et al. Vitamin D, parathyroid hormone, and sudden cardiac death: results
from the Cardiovascular Health Study. Hypertension 2011;58:1021-8.

66
186. Messa P, Cafforio C, Alfieri C. Clinical impact of hypercalcemia in kidney transplant. Int J Nephrol 2011;2011:906832.
187. Schwarz A, Mengel M, Gwinner W, et al. Risk factors for chronic allograft nephropathy after renal
transplantation: a protocol biopsy study. Kidney Int 2005;67:341-8. 188. Gwinner W, Suppa S, Mengel M, et al. Early calcification of renal allografts detected by protocol
biopsies: causes and clinical implications. Am J Transplant 2005;5:1934-41. 189. Suwelack B, Gerhardt U, Witta J, Hillebrandt U, Hohage H. Effect of parathyroid hormone levels on
carotid intima-media thickness after renal transplantation. Am J Hypertens 2001;14:1012-8. 190. Barenbrock M, Hausberg M, Kosch M, Kisters K, Hoeks AP, Rahn KH. Effect of hyperparathyroidism
on arterial distensibility in renal transplant recipients. Kidney Int 1998;54:210-5. 191. Moore J, Tomson CR, Tessa Savage M, Borrows R, Ferro CJ. Serum phosphate and calcium
concentrations are associated with reduced patient survival following kidney transplantation. Clin Transplant 2011;25:406-16.
192. Schaeffner ES, Fodinger M, Kramar R, Sunder-Plassmann G, Winkelmayer WC. Prognostic
associations of serum calcium, phosphate and calcium phosphate concentration product with outcomes in kidney transplant recipients. Transpl Int 2007;20:247-55.
193. Evenepoel P, Cooper K, Holdaas H, et al. A randomized study evaluating cinacalcet to treat
hypercalcemia in renal transplant recipients with persistent hyperparathyroidism. Am J Transplant 2014;14:2545-55.

67
Appendix
Paper 1-3


I

Neopterin is associated with cardiovascularevents and all-cause mortality in renaltransplant patients
Pihlstrøm H, Mjøen G, M€arz W, Dahle DO, Abedini S, Holme I,Fellstr€om B, Jardine A, Pilz S, Holdaas H. Neopterin is associatedwith cardiovascular events and all-cause mortality in renal transplantpatients.
Abstract: Background: Inflammatory markers show significantassociations with cardiovascular events and all-cause mortality afterkidney transplantation. Neopterin, reflecting interferon-c-release, maybetter reflect the proinflammatory state of recipients than less specificmarkers.Methods: Kidney transplant recipients in the Assessment of LEscol inRenal Transplant (ALERT) trial were examined and investigated for anassociation between serum neopterin and subsequent clinical events: graftloss, major cardiovascular events (MACE) and all-cause mortality.Results: After adjustment for established and emerging risk factorsneopterin expressed as neopterin-to-creatinine ratio was significantlyassociated with MACE (p = 0.009) and all-cause mortality (p = 0.002).Endpoints were more frequent with increasing quartiles of neopterin-to-creatinine ratio. The incidence rates of MACE and all-cause mortalitywere significantly increased in the upper quartiles compared with the first.Conclusions: This long-term prospective analysis in stable kidneyallograft recipients suggests that neopterin is associated with long-termrisk of cardiovascular events and all-cause mortality, but not renaloutcomes.
Hege Pihlstrøma, Geir Mjøenb,Winfried M€arzc,d,e, Dag OlavDahlea, Sadollah Abedinif, IngarHolmeg, Bengt Fellstr€omh, AlanJardinei, Stefan Pilzj,k and HallvardHoldaasa
aDepartment of Organ Transplantation, OsloUniversity Hospital Rikshospitalet, Oslo,Norway, bDivision of Nephrology, Departmentof Medicine, Oslo University Hospital Ullev"al,Oslo, Norway, cClinical Institute of Medical andChemical Laboratory Diagnostics, MedicalUniversity of Graz, Graz, Austria, dSynlabCenter of Laboratory Diagnostics, Heidelberg,Germany, eMedical Faculty Mannheim,Mannheim Institute of Public Health, Socialand Preventive Medicine, University ofHeidelberg, Mannheim, Germany, fDivision ofNephrology, Department of Medicine,Sykehuset i Vestfold, Tønsberg, Norway,gDepartment of Research and Development,Oslo University Hospital Ullev"al, Oslo, Norway,hDivision of Nephrology, Department ofInternal Medicine, Uppsala UniversityHospital, Uppsala, Sweden, iBritish HeartFoundation, Glasgow Cardiovascular ResearhCentre, Glasgow, UK, jDivision ofEndocrinology and Metabolism, Department ofInternal Medicine, Medical University of Graz,Graz, Austria and kDepartment ofEpidemiology and Biostatistics, EMGOInstitute for Health and Care Research, VUUniversity Medical Centre, Amsterdam, theNetherlands
Key words: inflammatory marker – kidney
transplantation – long-term – neopterin –
outcomes
Corresponding author: Hege Pihlstrøm,
Department of Organ Transplantation, Division
of Nephrology, Oslo University Hospital
Rikshospitalet, P.B. 4950 Nydalen, 0424 Oslo,
Norway.
Tel.: +47 92 214585;
fax: +47 23 073928;
e-mail: [email protected]
Conflict of interest: The authors have no
conflicts of interest to declare. The results
presented in this article have not been
published previously in whole or part, except
in abstract format.
111
© 2013 The Authors Clinical Transplantation Published by John Wiley & Sons Ltd
Clin Transplant 2014: 28: 111–119 DOI: 10.1111/ctr.12285 Clinical Transplantation

This is an open access article under the terms
of the Creative Commons
Attribution-NonCommercial License, which
permits use, distribution and reproduction in
any medium, provided the original work is
properly cited and is not used for commercial
purposes.
Accepted for publication 30 October 2013
Cardiovascular (CV) events and premature deathsare significantly more frequent in kidney transplantrecipients (KTR) compared with the general popu-lation, even when adjusting for the higher preva-lence of traditional risk factors such as diabetesmellitus, hypercholesterolemia, and hypertension(1). Although long-term statin therapy reduces theincidence of major cardiovascular events (MACE)in this population, there is significant residual riskfor both cardiac events and all-cause mortality (2).Several non-traditional risk factors, both modifi-able and non-modifiable, have been proposed tocontribute to this excessive risk (3). We have previ-ously demonstrated in KTR with stable graft func-tion that the inflammatory markers interleukin 6(IL-6) and C-reactive protein (CRP) show signifi-cant associations with CV events and all-causemortality (4). In this study, we explored the possi-bility that neopterin may be a more appropriateinflammatory marker for patients undergoing renaltransplantation (5).Neopterin (D-erythro-1-2-3-trihydroxypropyl-
pterin) is produced from guanosine triphosphate(6) by activated human monocytes, monocyte-derived dendritic cells, and macrophages. Releaseand production of neopterin is stimulated mainlyby interferon-c (IFN-c) released by activated Th1-lymphocytes during the cellular immune response(7). In contrast to IFN-c, which quickly binds totarget structures or is neutralized by soluble recep-tors, neopterin is biochemical inert, and its serumconcentrations were closely linked to the activityof the cellular immune system (8). Neopterin isshown to be a marker of disease in a variety of con-ditions (9) and has previously been associated withCV events and mortality in non-transplant popula-tions (10, 11). As a marker of cellular immuneresponse activation depending on IFN-c release,neopterin may better reflect the proinflammatorystate of KTR than less specific markers of inflam-mation, but the predictive value of neopterin forclinical outcomes in stable KTR is unknown.In the current analysis, long-term data from the
randomized Assessment of LEscol in RenalTransplant (ALERT) trial (1) were examined toinvestigate the association between serum neopter-
in level and subsequent adverse clinical outcomesin a population of KTR.
Patients and methods
Study design
The study design and baseline data of the ALERTtrial have been described previously (12). In brief,ALERT was a randomized, double-blind,placebo-controlled study of the effect of fluvastatin(40–80 mg/d vs. placebo) on cardiac and renal out-comes in 2102 male and female KTR aged 30–75 yr, included from June 1996 to October 1997.Patients had received a renal transplant more thansix months previously, had a stable graft functionand a total serum cholesterol between 4.0 and9.0 mM (155–348 mg/dL). Exclusion criteria werefamilial hypercholesterolemia, recent acute rejec-tion episodes, predicted life expectancy of less thanone yr or ongoing statin therapy. Follow-up was5–6 yr in the core study, after which trial partici-pants were offered open-label fluvastatin 80 mg/din a two-yr extension trial. Mean total follow-uptime for the extension study was 6.7 yr. Prior tounblinding the ALERT study, neopterin was cho-sen as one of the pre-specified cardiovascular riskfactors to be analyzed. Serum neopterin concentra-tion was measured in 30% of patients (randomlychosen) by radioimmunoassay (IBL Diagnostics,Hamburg, Germany) in samples taken at the timeof study entry (baseline), a mean of 5.4 yr aftertransplantation.
The study adhered to the International Confer-ence on Harmonization guidelines for Good Clini-cal Practice and was conducted in accordance withthe Declaration of Helsinki Principles. All partici-pants provided written informed consent, and theethics committee at each participating centerapproved the trial.
Outcome definitions
Renal endpoint was the time to graft loss (RGL),defined as return to dialysis or retransplantation.Cardiac endpoint was the occurrence of a MACE,
112
Pihlstrøm et al.

defined as cardiac death, non-fatal myocardialinfarction verified by hospital records, or coronaryrevascularization procedure, including coronaryartery bypass graft or percutaneous coronary inter-vention. Death by any cause was also chosen asstudy outcome. All endpoints were validated by anindependent clinical end point committee blindedto study randomization.
Statistical analysis
Since treatment and placebo arms of the originalstudy showed no significant heterogeneity in rela-tion to demographics, known cardiovascular orrenal risk factors or levels of inflammatory markers(12), the current analysis was based on the pooledpatient population.
In comparing baseline characteristics betweengroups, independent samples t-test and Mann–Whitney U-test for continuous variables and chi-square test for associations between categoricalvariables were used. Spearman’s rank correlationwas used in checking for statistical associationsbetween neopterin and creatinine, as well as theinflammatory markers IL-6 and CRP.
Univariable and multivariable Cox proportionalhazard models were used to evaluate the influenceof possible prognostic variables, including conven-tional cardiovascular risk factors, other inflamma-tory markers and factors associated with graftsurvival. These models were used to examine theassociation between neopterin and MACE, all-cause mortality and graft loss. Since high sensitivityCRP (hsCRP) and IL-6 are closely linked etiologi-cally and considered to be mutual confounders, theywere included as covariates in separate multivari-able regression models, the other variables remain-ing the same. Covariates were examined usingSchoenenfeld residuals and found to fulfill theassumptions of proportionality. Hazard ratios (HR)were estimated with 95% confidence intervals.
Neopterin estimates
As neopterin is chemically inert and its eliminationis solely through the kidneys, compromised renalfunction leads to a rise in serum neopterin that isnot caused by increased inflammatory activity (13).We found a high degree of correlation betweenneopterin and creatinine. Therefore, as done in themajority of previous studies on neopterin in popu-lations with compromised renal function, neopter-in levels were calculated relative to the serumconcentration of creatinine, thus adjusting for kid-ney function. Values are expressed in lmol/mol ofcreatinine.
SPSS version 18 (IBM Corp., Armonk, NY,USA) was used for all statistical analyses except forgeneration of Figs. 1 and 2 where we used Stataversion 11 (StataCorp, College Station, TX, USA).
Results
Baseline characteristics
Table 1 lists baseline characteristics for theALERT participants, comparing those with andwithout available baseline neopterin data. Demo-graphics, risk factors, and neopterin levels weresimilar in the fluvastatin and placebo arms (notshown). Since there were no clinically importantdifferences, neither between the two treatmentarms nor between the overall study population andthose for whom neopterin levels were available –subsequent analysis was performed on the pooledpopulation with available neopterin measurements(4, 14).
Fig. 1. Cumulative all-cause mortality according to quartilesof neopterin-to-creatinine ratio.
Fig. 2. Cumulative major cardiovascular events (MACE)according to quartiles of neopterin-to-creatinine ratio.
113
Neopterin in renal transplant recipients

The correlation coefficient between neopterinand creatinine was 0.61. For purposes of survivalanalysis, we categorized patients into quartilesaccording to their neopterin-to-creatinine ratios atbaseline. Levels ranged from 33 to 325 lmol/mol.In Table 2, demographic data and background riskfactors are presented for each quartile of neopter-in/creatinine. There was a tendency towards higherproportions of patients with hypertension, chronicheart disease, panel reactive antibodies, delayedgraft function (DGF), longer time on dialysis priorto transplantation and treatment for CMV-infec-tion/reactivation in the highest or the two highestquartiles. IL-6 and hsCRP increased progressivelyacross the quartiles, as did age.
Outcomes
The proportions of patients reaching the renal, car-diac and mortality endpoints in each quartile forneopterin-to-creatinine ratio are listed in Table 3.Log-rank tests were used to check the significance
of differences between each of the three upperquartiles compared with the lowest.
The rate of death from all causes increased inhigher neopterin/creatinine quartiles, and the dif-ferences were statistically significant between allthree upper quartiles and the first quartile. Thenumber of events more than trebled from the firstto the fourth quartile (9.5–33.6%). For MACE,the incidence rate was more than twice as high(11.1–25.0%) in the fourth neopterin/creatininequartile compared with the first one, and the differ-ence was statistically significant. For renal graftloss the incidence rates was slightly higher in thefourth quartile, but no statistical significance wasreached.
Figs. 1 and 2 presents the Kaplan–Meier failureestimates plots for all-cause mortality and MACEshowing time to event, or end of follow-up, byneopterin/creatinine quartile.
Multiple risk factor analysis
Table 4 shows risk factor evaluation using univari-able and multivariable models of Cox regressionanalyses. For all study outcomes we present HRwith 95% confidence intervals (95% CI) and theirrespective p-Values. In the univariable model,baseline neopterin expressed as neopterin-to-creati-nine ratio, as well as potential risk factors andbaseline demographics, is examined separatelyagainst the study outcomes. The multivariablemodel is adjusted for the following baseline covari-ates: age, gender, smoking habit, diagnosis of coro-nary heart disease, LDL-cholesterol, systolic bloodpressure, diabetes mellitus, serum creatinine, andproteinuria. IL-6 and hsCRP were included in sep-arate models, as they are part of the same etiologi-cal inflammatory pathway and thus have a highcolinearity. Results are shown only for the analysisincluding hsCRP, as the hazard ratio for neopterinwas virtually identical in the two models.
In the univariable model, neopterin was highlysignificantly associated with all endpoints in ourstudy. After adjustment for other established andpotentially important risk factors, we found neop-terin (in lmol/mol creatinine) to have a significantpositive association with all-cause of death (HR1.06 per 10 units, p = 0.002, 95% CI 1.02–1.09)and MACE (HR 1.06 per 10 units, p = 0.009, 95%CI 1.01–1.10) but no independent predictive valuefor graft loss. HR and p-Values for neopterinremained the same for all endpoints when random-ization group was included in the multivariatemodel (not shown). Though reaching significancefor MACE in the univariable analyses, HsCRPwas not independently associated with any of the
Table 1. Demographic and baseline data for patients with or withoutmeasurement of neopterin
VariablesAvailabledata (n)
Neopterinmeasured(n = 629)
Neopterin notmeasured(n = 1473)
Age at baseline, yr 2102 49.9 (10.9) 49.6 (10.9)Male gender 2102 420 (66.8) 967 (65.6)Current smoker 2100 133 (21.1) 256 (17.4)Body massindex, kg/m2
2051 25.5 (4.3) 25.9 (4.6)
Diabetes mellitus 2101 133 (21.1) 263 (17.9)Hypertension 2102 483 (76.8) 1092 (74.1)Systolic bloodpressure, mmHg
2094 142.6 (19.0) 144.5 (18.8)
Diastolic bloodpressure, mmHg
2093 85.5 (9.3) 85.7 (10.4)
Coronary heart disease 2101 58 (9.2) 143 (9.7)Serum creatinine, lM 2028 146.2 (51.6) 145.0 (53.6)Proteinuria, g/24 h 1981 0.40 (0.76) 0.45 (1.11)HDL cholesterol, mM 2017 1.33 (0.46) 1.34 (0.45)LDL cholesterol, mM 2001 4.19 (1.01) 4.12 (1.02)Triglycerides, mM 2028 2.26 (1.24) 2.19 (1.42)hsCRP, mg/L 1910 3.70 (6.82) 3.85 (6.66)IL-6, pg/mL 1751 3.05 (1.92) 2.85 (1.84)Time since lasttransplant, yr
2101 5.4 (3.5) 5.0 (3.4)
Time on dialysis, yr 2092 2.2 (3.6) 2.3 (3.4)Cold ischemiatime, hours
1520 17.9 (7.3) 20.5 (7.8)
Panel reactive antibodies 1845 117 (20.4) 210 (16.5)Delayed graft function 2063 93 (15.0) 272 (18.8)Treatment forcytomegalovirus
2030 86 (14.1) 200 (14.1)
Continuous variables are shown as mean (SD); categorical variables as n(%).HDL, high-density lipoprotein; LDL, low-density lipoprotein; hsCRP, highsensitivity CRP; IL-6, interleukin-6.
114
Pihlstrøm et al.
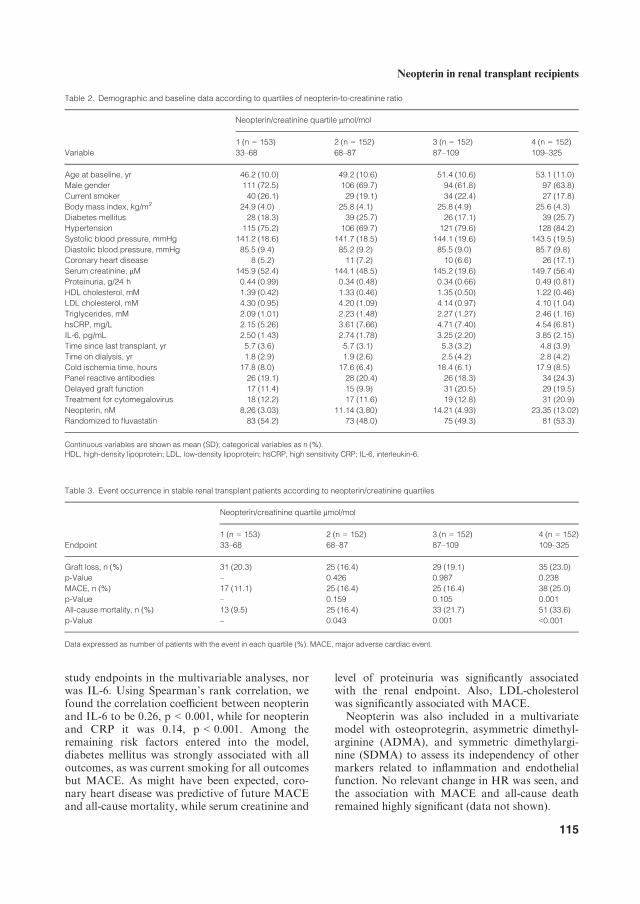
study endpoints in the multivariable analyses, norwas IL-6. Using Spearman’s rank correlation, wefound the correlation coefficient between neopterinand IL-6 to be 0.26, p < 0.001, while for neopterinand CRP it was 0.14, p < 0.001. Among theremaining risk factors entered into the model,diabetes mellitus was strongly associated with alloutcomes, as was current smoking for all outcomesbut MACE. As might have been expected, coro-nary heart disease was predictive of future MACEand all-cause mortality, while serum creatinine and
level of proteinuria was significantly associatedwith the renal endpoint. Also, LDL-cholesterolwas significantly associated with MACE.Neopterin was also included in a multivariate
model with osteoprotegrin, asymmetric dimethyl-arginine (ADMA), and symmetric dimethylargi-nine (SDMA) to assess its independency of othermarkers related to inflammation and endothelialfunction. No relevant change in HR was seen, andthe association with MACE and all-cause deathremained highly significant (data not shown).
Table 2. Demographic and baseline data according to quartiles of neopterin-to-creatinine ratio
Variable
Neopterin/creatinine quartile lmol/mol
1 (n = 153)33–68
2 (n = 152)68–87
3 (n = 152)87–109
4 (n = 152)109–325
Age at baseline, yr 46.2 (10.0) 49.2 (10.6) 51.4 (10.6) 53.1 (11.0)Male gender 111 (72.5) 106 (69.7) 94 (61.8) 97 (63.8)Current smoker 40 (26.1) 29 (19.1) 34 (22.4) 27 (17.8)Body mass index, kg/m2 24.9 (4.0) 25.8 (4.1) 25.8 (4.9) 25.6 (4.3)Diabetes mellitus 28 (18.3) 39 (25.7) 26 (17.1) 39 (25.7)Hypertension 115 (75.2) 106 (69.7) 121 (79.6) 128 (84.2)Systolic blood pressure, mmHg 141.2 (18.6) 141.7 (18.5) 144.1 (19.6) 143.5 (19.5)Diastolic blood pressure, mmHg 85.5 (9.4) 85.2 (9.2) 85.5 (9.0) 85.7 (9.8)Coronary heart disease 8 (5.2) 11 (7.2) 10 (6.6) 26 (17.1)Serum creatinine, lM 145.9 (52.4) 144.1 (48.5) 145.2 (19.6) 149.7 (56.4)Proteinuria, g/24 h 0.44 (0.99) 0.34 (0.48) 0.34 (0.66) 0.49 (0.81)HDL cholesterol, mM 1.39 (0.42) 1.33 (0.46) 1.35 (0.50) 1.22 (0.46)LDL cholesterol, mM 4.30 (0.95) 4.20 (1.09) 4.14 (0.97) 4.10 (1.04)Triglycerides, mM 2.09 (1.01) 2.23 (1.48) 2.27 (1.27) 2.46 (1.16)hsCRP, mg/L 2.15 (5.26) 3.61 (7.66) 4.71 (7.40) 4.54 (6.81)IL-6, pg/mL 2.50 (1.43) 2.74 (1.78) 3.25 (2.20) 3.85 (2.15)Time since last transplant, yr 5.7 (3.6) 5.7 (3.1) 5.3 (3.2) 4.8 (3.9)Time on dialysis, yr 1.8 (2.9) 1.9 (2.6) 2.5 (4.2) 2.8 (4.2)Cold ischemia time, hours 17.8 (8.0) 17.6 (6.4) 18.4 (6.1) 17.9 (8.5)Panel reactive antibodies 26 (19.1) 28 (20.4) 26 (18.3) 34 (24.3)Delayed graft function 17 (11.4) 15 (9.9) 31 (20.5) 29 (19.5)Treatment for cytomegalovirus 18 (12.2) 17 (11.6) 19 (12.8) 31 (20.9)Neopterin, nM 8.26 (3.03) 11.14 (3.80) 14.21 (4.93) 23.35 (13.02)Randomized to fluvastatin 83 (54.2) 73 (48.0) 75 (49.3) 81 (53.3)
Continuous variables are shown as mean (SD); categorical variables as n (%).HDL, high-density lipoprotein; LDL, low-density lipoprotein; hsCRP, high sensitivity CRP; IL-6, interleukin-6.
Table 3. Event occurrence in stable renal transplant patients according to neopterin/creatinine quartiles
Endpoint
Neopterin/creatinine quartile lmol/mol
1 (n = 153)33–68
2 (n = 152)68–87
3 (n = 152)87–109
4 (n = 152)109–325
Graft loss, n (%) 31 (20.3) 25 (16.4) 29 (19.1) 35 (23.0)p-Value – 0.426 0.987 0.238MACE, n (%) 17 (11.1) 25 (16.4) 25 (16.4) 38 (25.0)p-Value – 0.159 0.105 0.001All-cause mortality, n (%) 13 (9.5) 25 (16.4) 33 (21.7) 51 (33.6)p-Value – 0.043 0.001 <0.001
Data expressed as number of patients with the event in each quartile (%). MACE, major adverse cardiac event.
115
Neopterin in renal transplant recipients

Discussion
In this analysis of a large cohort of KTR from theALERT study, we have shown that the inflamma-tory marker neopterin is significantly associatedwith cardiovascular events and all cause mortalityin KTR, even after adjustment for conventionaland new risk factors.In patients with pre-dialysis chronic kidney
disease (CKD), serum neopterin is elevated andsignificantly correlated with markers of inflamma-tion including hsCRP, IL-6, and IFN-c. (15). Wehave shown previously that levels of IL-6 andhsCRP are associated with cardiovascular end-points and all-cause mortality following kidneytransplantation (4, 16). However, and of centralimportance, this study shows that in KTR thepredictive power of neopterin was maintained afteradjustment for hsCRP and IL-6. In the multivari-able analyses including neopterin, CRP and IL-6
failed to reach significance as independent predic-tors of long-term outcomes. In addition, thoughstatistically significant, the correlations betweenneopterin and these two inflammation markerswere weak ones. Our epidemiological data on thepredictive value of neopterin are in line with previ-ous literature showing that neopterin rises quicklyafter macrophage activation (17), is an excellentmarker for longer term activation of cellularimmunity during the maintenance phase, andappear to remain relatively stable over time (18).
Inflammation is a key element of the develop-ment of atherosclerosis, with T-lymphocytes andmonocyte-derived macrophages being detected inatherosclerotic lesions. In accordance with ourresults, studies have highlighted neopterin as auseful marker for long-term risk of all-cause andcardiovascular death in patients from diversepopulations, including individuals undergoingcoronary angiography (19), patients with stable
Table 4. Hazard ratios for neopterin-to-creatinine ratio (per 10 units in lmol/mol) with covariates in relation to outcomes in 628 stable renal trans-plant patients by univariable and multivariable Cox regression analysis
Risk factors
MACE 106/628 All-cause mortality 122/628Graft loss (death-censored)124/628
Univariable analysis HR (95% CI) p-Value HR (95% CI) p-Value HR (95% CI) p-Value
Age 1.03 (1.01–1.05) 0.002 1.07 (1.05–1.09) <0.001 0.98 (0.96–0.99) 0.008Male gender 1.51 (0.98–2.34) 0.064 1.05 (0.72–1.54) 0.792 1.42 (0.96–2.12) 0.083Current smoking 1.03 (0.64–1.64) 0.917 1.55 (1.04–2.30) 0.030 2.02 (1.39–2.94) <0.001Coronary heart disease 4.00 (2.55–6.27) <0.001 3.22 (2.09–4.99) <0.001 1.00 (0.52–1.90) 0.994LDL-cholesterol 1.42 (1.18–1.69) <0.001 1.06 (0.88–1.26) 0.552 1.11 (0.92–1.32) 0.273Systolic blood pressure 1.01 (1.00–1.02) 0.202 1.01 (1.01–1.02) 0.001 1.02 (1.01–1.02) 0.001Diabetes mellitus 1.99 (1.32–2.99) 0.001 2.17 (1.49–3.16) <0.001 1.64 (1.11–2.43) 0.013Creatinine 1.01 (1.00–1.01) 0.002 1.01 (1.00–1.01) <0.001 1.02 (1.02–1.02) <0.001Proteinuria 1.22 (1.02–1.45) 0.030 1.23 (1.04–1.45) 0.015 2.23 (1.96–2.54) <0.001hsCRP 1.03 (1.01–1.05) 0.004 1.02 (1.00–1.04) 0.062 1.01 (0.99–1.03) 0.331Neopterin/creatinine 1.08 (1.04–1.12) <0.001 1.11 (1.07–1.14) <0.001 1.05 (1.01–1.09) 0.020
Risk factors
MACE 100/585 All-cause mortality 117/583Graft loss (death-censored)114/583
Multivariable analysis HR (95% CI) p-Value HR (95% CI) p-Value HR (95% CI) p-Value
Age 1.02 (1.00–1.04) 0.057 1.07 (1.05–1.09) <0.001 0.98 (0.96–1.00) 0.097Male gender 1.54 (0.96–2.45) 0.073 0.90 (0.59–1.35) 0.596 0.92 (0.59–1.44) 0.723Current smoking 1.00 (0.60–1.65) 0.990 1.75 (1.16–2.65) 0.008 1.71 (1.14–2.58) 0.010Coronary heart disease 3.35 (2.06–5.46) <0.001 2.02 (1.27–3.19) 0.003 1.04 (0.51–2.11) 0.921LDL-cholesterol 1.47 (1.22–1.77) <0.001 0.99 (0.83–1.19) 0.940 1.07 (0.89–1.28) 0.498Systolic blood pressure 1.00 (0.99–1.01) 0.503 1.00 (0.99–1.01) 0.893 1.00 (0.99–1.01) 0.979Diabetes mellitus 2.01 (1.31–3.10) 0.002 2.38 (1.60–3.55) <0.001 1.82 (1.20–2.79) 0.005Creatinine 1.00 (1.00–1.01) 0.056 1.01 (1.00–1.01) <0.001 1.02 (1.01–1.02) <0.001Proteinuria 1.08 (0.87–1.34) 0.508 1.09 (0.87–1.35) 0.456 1.88 (1.60–2.21) <0.001hsCRP 1.02 (1.00–1.04) 0.127 1.01 (0.99–1.03) 0.343 1.01 (0.99–1.03) 0.526Neopterin/creatinine 1.06 (1.01–1.10) 0.009 1.06 (1.02–1.09) 0.002 1.03 (1.00–1.08) 0.152
The multivariable analysis adjusts for relevant demographic covariates (age, gender), known renal/cardiovascular risk factors (smoking, coronary heart dis-ease, LDL-cholesterol, systolic blood pressure, diabetes mellitus, creatinine, level of proteinuria), and the inflammation marker hsCRP.CI, confidence interval; HDL, high-density lipoprotein; HR, hazard ration; hsCRP, high sensitivity CRP; LDL, low-density lipoprotein; MACE, major adversecardiac event.
116
Pihlstrøm et al.

coronary artery disease (20), newly diagnosed dia-betics (21), and dialysis-dependent CKD patients(22). Furthermore, it has recently been shown thatelevated neopterin, but not CRP level, predicts leftventricular dysfunction in patients with chronicstable angina pectoris (23). A recent report fromthe Hordaland study demonstrated that in elderlypatients, without pre-existing coronary heart dis-ease, higher levels of neopterin are associated withan increased risk of subsequent coronary events(24). Chronic low-grade inflammation is one of themain conditions associated with increased cardio-vascular morbidity and mortality in patients withCKD, especially those on dialysis (25). Thus, it isnot surprising that persistent inflammation, endo-thelial dysfunction, and associated oxidative stressin KTR (26) is reflected in progression of athero-sclerosis (27) and adversely affects cardiovascularoutcomes (4). The significant association betweenneopterin and outcomes was maintained even afteradjustment for markers of endothelial function(SDMA, ADMA).
Immunologic responses to allografts involvehumoral and cellular components of both theadaptive and innate immune system, the T-cellplaying a pivotal role in the initial recognition ofanti-self (28). The stronger association that wefound between neopterin and the clinical endpointsthan for other inflammatory markers may possiblyreflect the dominance of T-cell and macrophageactivation in the ongoing inflammatory status ofallograft recipients. Consistent with this, baselineneopterin values were substantially higher in ourcohort compared with the general population (29)and patients with known CV disease (18). This is inharmony with earlier findings on clinically stableKTR (30, 31).
In one of the earliest publications to assess levelsof neopterin in KTR (32), Margreiter et al. mea-sured urinary neopterin daily during the earlypost-operative period and found that acute rejec-tion and early viral infection were preceded by arising or high level of urinary neopterin in 95%and 100% of cases, respectively. They laterextended their data to include urinary neopterinmeasurements in 294 kidney allograft recipients(33). Subsequent studies by others have confirmedthat elevation of serum or urinary neopterin pre-cedes the rise in creatinine by up to several days inpatients with acute early complications (34, 35),and routine daily post-operative neopterin mea-surements have been suggested for the early detec-tion of immunologic complications in kidneyallograft recipients (36).
In the trial (33) conducted by Reibnegger andcolleagues, a high neopterin level in the early
post-transplant period was associated with ahigher risk of graft failure in the long term. In asmaller cohort of patients, Grebe et al. (37)observed that elevated neopterin levels followingtransplantation were associated with inferior graftand patient survival, while a recent prospectivestudy in 216 KTR showed an association betweenhigher levels of neopterin and acute rejection in thefirst year of follow-up (38). Our population wasrecruited five yr after transplantation and was clin-ically stable with a reasonably good renal function.Elevated neopterin was not significantly associatedwith renal graft loss after adjusting for level of pro-teinuria. While Grebe et al. (37) were primarilyinterested in early post-transplant macrophageactivation associated with elevated neopterin, ourstudy suggests that in clinically stable allograftrecipients, serum neopterin is not independentlyassociated with renal graft failure and does notadd significantly to the prognostic informationgiven by the degree of proteinuria. Weimer et al.(39, 40) reported significant associations betweenneopterin concentration at one yr post-transplantand the development of chronic rejection andchronic allograft dysfunction within two yr, butproteinuria was not included in their multivariableanalysis, possibly explaining this discrepancy.A small study on children with primary nephro-
tic syndrome (41) showed a positive correlationbetween serum neopterin levels and proteinuria inpatients with active disease. A link between neop-terin levels and the progression rate in proteinuricdiabetic nephropathy has been demonstrated (42),and one group (43) observed marked differences inserum and urine neopterin levels among diabeticpatients with and without microalbuminuria. Weare not proposing that enhanced macrophageactivity is not an important factor in the develop-ment of a dysfunctional renal allograft, but thepotential clinical value of neopterin with respect tograft function may be limited as long as protein-uria is considered a well established risk factor forpoorer long-term renal outcomes in kidney allo-graft recipients (44, 45).Reference ranges for neopterin are higher in the
healthy elderly population (>75 yr). Several studiesreport rising neopterin levels from the age of 60–70(46) or even earlier (47), probably reflecting theinvolvement of cellular immunity in the aging pro-cess, as well as the presence of low-grade inflam-matory processes such as atherosclerosis,neurodegeneration, or unrecognized evolving dis-ease (autoimmunity or malignancy) (29). However,we did not find significant differences in baselineneopterin between different age groups, perhapsbecause kidney transplants are not performed for
117
Neopterin in renal transplant recipients

the oldest CKD patients (recipients in our cohortwere aged 23.6–74.8 yr), and because comorbidity,the immunological consequences of long-standinguremia and the anti-allograft immune responsemay overshadow the component of neopterin pro-duction related to aging.The strengths of this analysis are the prospective
controlled design, the long follow-up time, thelarge patient cohort and the independent adjudica-tion of all clinical endpoints. Potential limitationsof our study, however, merit consideration.Although the results show a strong associationbetween neopterin and clinical outcomes, the datado not prove a causal relationship. Residual con-founding cannot be ruled out, though we havecarefully adjusted for a wide range of covariates inour statistical models. Although neopterin may, atpresent, not be a clinically useful single parameterfor risk prediction in KTR, it is conceivable thatneopterin could be valuable for multi-marker riskprediction or for the evaluation of the clinical effi-cacy of established treatments in this patientgroup.As in most large prospective trials, serum samples
were obtained at inclusion and not followed consec-utively. The study population, a cohort selected forentry into a clinical trial, is not necessarily fully rep-resentative of the general renal transplant popula-tion, although the qualitative relationships betweenneopterin and the specified clinical outcomes arelikely to apply, at least for Caucasians. Mean neop-terin values were not different for the two randomi-zation groups, and there was no significant skewingin the proportion of patients receiving fluvastatin ineach quartile of neopterin-to-creatinine ratio.Entering treatment group as a covariate in the mul-tiple regression analysis did not change the hazardratio for neopterin.In conclusion, in clinically stable renal trans-
plant recipients there appears to be an independentassociation between serum neopterin concentrationand long-term clinical outcomes of MACE and all-cause mortality.
Acknowledgements
The ALERT study was funded by Novartis Pharma AG.IBL Diagnostics provided the neopterin assays free ofcharge, but did not assume an active role in the statisticalevaluation or interpretation of data. There was no otherexternal funding.
Authors’ contributions
Hege Pihlstrøm: Data collection, data analysis/interpretation, statistics, drafting the article. Hall-vard Holdaas: Concept/design, study protocol,
data collection, drafting and critical revision of thearticle. Bengt Fellstr€om and Alan Jardine: Con-cept/design, study protocol, data collection, criticalrevision of the article. Geir Mjøen, Ingar Holme,Sadollah Abedini, and Dag Olav Dahle: Dataanalysis/interpretation, statistics, critical revisionof the article. Winfried M€arz and Stephan Pilz:Data analysis/interpretation, drafting and criticalrevision of the article.
References
1. HOLDAAS H, FELLSTROM B, JARDINE AG et al. Effect of flu-vastatin on cardiac outcomes in renal transplant recipients:a multicentre, randomised, placebo-controlled trial. Lan-cet 2003: 361: 2024.
2. HOLDAAS H, FELLSTROM B, COLE E et al. Long-term car-diac outcomes in renal transplant recipients receiving flu-vastatin: the ALERT extension study. Am J Transplant2005: 5: 2929.
3. JARDINE AG, GASTON RS, FELLSTROM BC, HOLDAAS H.Prevention of cardiovascular disease in adult recipients ofkidney transplants. Lancet 2011: 378: 1419.
4. ABEDINI S, HOLME I, MARZ W et al. Inflammation in renaltransplantation. Clin J Am Soc Nephrol 2009: 4: 1246.
5. GREBE SO, MUELLER TF. Immune monitoring in organtransplantation using neopterin. Curr Drug Metab 2002:3: 189.
6. REYNOLDS JJ, BROWN GM. The biosynthesis of folic acid.IV. Enzymatic synthesis of dihydrofolic acid from guanineand ribose compounds. J Biol Chem 1964: 239: 317.
7. GOSTNER JM, BECKER K, FUCHS D, SUCHER R. Redox regu-lation of the immune response. Redox Rep 2013: 18: 88.
8. HUBER C, BATCHELOR JR, FUCHS D et al. Immuneresponse-associated production of neopterin. Release frommacrophages primarily under control of interferon-gamma. J Exp Med 1984: 160: 310.
9. HOFFMANN G, WIRLEITNER B, FUCHS D. Potential role ofimmune system activation-associated production of neop-terin derivatives in humans. Inflamm Res 2003: 52: 313.
10. DE ROSA S, CIRILLO P, PACILEO M et al. Neopterin: fromforgotten biomarker to leading actor in cardiovascularpathophysiology. Curr Vasc Pharmacol 2011: 9: 188.
11. MANGGE H, ALMER G, TRUSCHNIG-WILDERS M, SCHMIDT A,GASSER R, FUCHS D. Inflammation, adiponectin, obesityand cardiovascular risk. Curr Med Chem 2010: 17: 4511.
12. HOLDAAS H, FELLSTROM B, HOLME I et al. Effects of flu-vastatin on cardiac events in renal transplant patients:ALERT (Assessment of Lescol in Renal Transplantation)study design and baseline data. J Cardiovasc Risk 2001: 8:63.
13. AULITZKY WE, TILG H, NIEDERWIESER D et al. Compari-son of serum neopterin levels and urinary neopterin excre-tion in renal allograft recipients. Clin Nephrol 1988: 29:248.
14. SVENSSON M, DAHLE DO, MJOEN G et al. Osteoprotegerinas a predictor of renal and cardiovascular outcomes inrenal transplant recipients: follow-up data from theALERT study. Nephrol Dial Transplant 2012: 27: 2571.
15. YADAV AK, SHARMA V, JHA V. Association between serumneopterin and inflammatory activation in chronic kidneydisease. Mediators Inflamm 2012: 2012: 476979.
16. DAHLE DO, MJOEN G, OQVIST B et al. Inflammation-asso-ciated graft loss in renal transplant recipients. NephrolDial Transplant 2011: 26: 3756.
118
Pihlstrøm et al.

17. TROPPMAIR J, NACHBAUR K, HEROLD M et al. In-vitro andin-vivo studies on the induction of neopterin biosynthesisby cytokines, alloantigens and lipopolysaccharide (LPS).Clin Exp Immunol 1988: 74: 392.
18. RAY KK, MORROW DA, SABATINE MS et al. Long-termprognostic value of neopterin: a novel marker of monocyteactivation in patients with acute coronary syndrome. Cir-culation 2007: 115: 3071.
19. GRAMMER TB, FUCHS D, BOEHM BO, WINKELMANN BR,MAERZ W. Neopterin as a predictor of total and cardiovas-cular mortality in individuals undergoing angiography inthe Ludwigshafen Risk and Cardiovascular Health study.Clin Chem 2009: 55: 1135.
20. FUCHS D, AVANZAS P, ARROYO-ESPLIGUERO R, JENNY M,CONSUEGRA-SANCHEZ L, KASKI JC. The role of neopterin inatherogenesis and cardiovascular risk assessment. CurrMed Chem 2009: 16: 4644.
21. VENGEN IT, DALE AC, WISETH R, MIDTHJELL K, VIDEM V.Neopterin predicts the risk for fatal ischemic heart diseasein type 2 diabetes mellitus: long-term follow-up of theHUNT 1 study. Atherosclerosis 2009: 207: 239.
22. AVCI E, COSKUN S, CAKIR E, KURT Y, OZGUR AKGUL E,BILGI C. Relations between concentrations of asymmetricdimethylarginine and neopterin as potential risk factorsfor cardiovascular diseases in haemodialysis-treatedpatients. Ren Fail 2008: 30: 784.
23. ESTEVEZ-LOUREIRO R, RECIO-MAYORAL A, SIEIRA-RODRI-
GUEZ-MORET JA, TRALLERO-ARAGUAS E, KASKI JC. Neop-terin levels and left ventricular dysfunction in patientswith chronic stable angina pectoris. Atherosclerosis 2009:207: 514.
24. SULO G, VOLLSET SE, NYGARD O et al. Neopterin and ky-nurenine-tryptophan ratio as predictors of coronary eventsin older adults, the Hordaland Health Study. Int J Cardiol2013: 168: 1435.
25. STENVINKEL P, BARANY P. Dialysis in 2011: can cardiovas-cular risk in dialysis patients be decreased? Nat Rev Neph-rol 2011: 8: 72.
26. NAFAR M, SAHRAEI Z, SALAMZADEH J, SAMAVAT S, VAZIRI
ND. Oxidative stress in kidney transplantation: causes,consequences, and potential treatment. Iran J Kidney Dis2011: 5: 357.
27. TURKMEN K, TONBUL HZ, TOKER A et al. The relationshipbetween oxidative stress, inflammation, and atherosclero-sis in renal transplant and end-stage renal disease patients.Ren Fail 2012: 34: 1229.
28. HEEGER PS, DINAVAHI R. Transplant immunology fornon-immunologist. Mt Sinai J Med 2012: 79: 376.
29. SCHENNACH H, MURR C, GACHTER E, MAYERSBACH P,SCHONITZER D, FUCHS D. Factors influencing serum neop-terin concentrations in a population of blood donors. ClinChem 2002: 48: 643.
30. WOLF J, MUSCH E, NEUSS H, KLEHR U. Neopterin in theserum and urine in the differential diagnosis of disordersof kidney function following kidney transplantation. KlinWochenschr 1987: 65: 225.
31. KAMEOKA H, TAKAHARA S, TAKANO Y et al. Serum andurinary neopterin as markers in renal transplant patients.Int Urol Nephrol 1994: 26: 107.
32. MARGREITER R, FUCHS D, HAUSEN A et al. Neopterin as anew biochemical marker for diagnosis of allograft rejec-
tion. Experience based upon evaluation of 100 consecutivecases. Transplantation 1983: 36: 650.
33. REIBNEGGER G, AICHBERGER C, FUCHS D et al. Posttrans-plant neopterin excretion in renal allograft recipients–areliable diagnostic aid for acute rejection and a predictivemarker of long-term graft survival. Transplantation 1991:52: 58.
34. CHIN GK, ADAMS CL, CAREY BS, SHAW S, TSE WY,KAMINSKI ER. The value of serum neopterin, interferon-gamma levels and interleukin-12B polymorphisms in pre-dicting acute renal allograft rejection. Clin Exp Immunol2008: 152: 239.
35. SCHAFER AJ, DANIEL V, DREIKORN K, OPELZ G. Assess-ment of plasma neopterin in clinical kidney transplanta-tion. Transplantation 1986: 41: 454.
36. LEE PH, HUANG MT, CHUNG YC et al. Monitoring ofserum neopterin in renal transplant recipients. J FormosMed Assoc 1992: 91: 1209.
37. GREBE SO, KUHLMANN U, FOGL D, LUYCKX VA, MUELLER
TF. Macrophage activation is associated with poorerlong-term outcomes in renal transplant patients. ClinTransplant 2011: 25: 744.
38. CAREY BS, JAIN R, ADAMS CL et al. Serum neopterin as anindicator of increased risk of renal allograft rejection.Transpl Immunol 2013: 28: 81.
39. WEIMER R, SUSAL C, YILDIZ S et al. sCD30 and neopterinas risk factors of chronic renal transplant rejection: impactof cyclosporine A, tacrolimus, and mycophenolate mofetil.Transplant Proc 2005: 37: 1776.
40. WEIMER R, SUSAL C, YILDIZ S et al. Post-transplantsCD30 and neopterin as predictors of chronic allograftnephropathy: impact of different immunosuppressive regi-mens. Am J Transplant 1865: 2006: 6.
41. BAKR A, RAGEH I, EL-AZOUNY M, DEYAB S, LOTFY H.Serum neopterin levels in children with primary nephroticsyndrome. Acta Paediatr 2006: 95: 854.
42. WEISS MF, RODBY RA, JUSTICE AC, HRICIK DE. Freepentosidine and neopterin as markers of progression ratein diabetic nephropathy. Collaborative Study Group. Kid-ney Int 1998: 54: 193.
43. BARIS N, ERDOGAN M, SEZER E et al. Alterations in L-argi-nine and inflammatory markers in type 2 diabetic patientswith and without microalbuminuria. Acta Diabetol 2009:46: 309.
44. ROODNAT JI, MULDER PG, RISCHEN-VOS J et al. Protein-uria after renal transplantation affects not only graft sur-vival but also patient survival. Transplantation 2001: 72:438.
45. FERNANDEZ-FRESNEDO G, PLAZA JJ, SANCHEZ-PLUMED J,SANZ-GUAJARDO A, PALOMAR-FONTANET R, ARIAS M. Pro-teinuria: a new marker of long-term graft and patient sur-vival in kidney transplantation. Nephrol Dial Transplant2004: 19(Suppl. 3): iii47.
46. FRICK B, SCHROECKSNADEL K, NEURAUTER G, LEBLHUBER
F, FUCHS D. Increasing production of homocysteine andneopterin and degradation of tryptophan with older age.Clin Biochem 2004: 37: 684.
47. SPENCER ME, JAIN A, MATTEINI A et al. Serum levels ofthe immune activation marker neopterin change with ageand gender and are modified by race, BMI, and percentageof body fat. J Gerontol A Biol Sci Med Sci 2010: 65: 858.
119
Neopterin in renal transplant recipients


II


Symmetric Dimethylarginine as Predictor of Graft lossand All-Cause Mortality in Renal Transplant RecipientsHege Pihlstrøm,1,12 Geir Mjøen,2 Dag Olav Dahle,1 Stefan Pilz,3,4 Karsten Midtvedt,1 Winfried Marz,5,6,7
Sadollah Abedini,8 Ingar Holme,9 Bengt Fellstrom,10 Alan Jardine,11 and Hallvard Holdaas1
Background. Elevated symmetric dimethylarginine (SDMA) has been shown to predict cardiovascular events and allcause mortality in diverse populations. The potential role of SDMA as a risk marker in renal transplant recipients(RTR) has not been investigated.Methods. We analyzed SDMA in the placebo arm of the Assessment of Lescol in Renal Transplantation study, arandomized controlled trial of fluvastatin in RTR. Mean follow-up was 5.1 years. Patients were grouped into quartilesbased on SDMA levels at study inclusion. Relationships between SDMA and traditional risk factors for graft functionand all-cause mortality were analyzed in 925 RTR using univariate and multivariate survival analyses.Results. In univariate analysis, SDMA was significantly associated with renal graft loss, all-cause death, and majorcardiovascular events. After adjustment for established risk factors including estimated glomerular filtration rate, anelevated SDMA-level (4th quartile, 91.38 Kmol/L) was associated with renal graft loss; hazard ratio (HR), 5.51; 95%confidence interval (CI), 1.95Y15.57; P=0.001, compared to the 1st quartile. Similarly, SDMA in the 4th quartile wasindependently associated with all-cause mortality (HR, 4.56; 95% CI, 2.15Y9.71; PG0.001), and there was a strongborderline significant trend for an association with cardiovascular mortality (HR, 2.86; 95% CI, 0.99Y8.21; P=0.051).Conclusion. In stable RTR, an elevated SDMA level is independently associated with increased risk of all-causemortality and renal graft loss.
Keywords: Symmetric dimethylarginine, Renal transplantation, Survival, Graft loss.
(Transplantation 2014;98: 1219Y1225)
Increased risk of cardiovascular (CV) disease and prematuredeath in renal transplant recipients (RTR) cannot fully be
explained by traditional risk factors (1). In addition to es-tablished predictors of CV disease, numerous modifiable andnonmodifiable emerging risk factors have been proposedto contribute to the excessive incidence of CV events inRTR. Increased symmetric dimethylarginine (SDMA), which
is an established risk factor for CV events and all-causemortality in other populations, has not been investigated intransplant patients.
The introduction of new and more efficient immuno-suppressive agents has significantly reduced the incidence ofacute rejection episodes. However, less has been achieved forlong-term allograft survival, and chronic allograft dysfunctionremains a major clinical challenge (2). To improve risk strat-ification and to identify potential treatment targets for this
CLINICAL AND TRANSLATIONAL RESEARCH
Transplantation & Volume 98, Number 11, December 15, 2014 www.transplantjournal.com 1219
The ALERT study was funded by Novartis Pharma AG.The authors declare no conflicts of interest.1 Division of Nephrology, Department of Organ Transplantation, Oslo
University Hospital Rikshospitalet, Oslo, Norway.2 Division of Nephrology, Department of Medicine, Oslo University
Hospital Ulleval, Oslo, Norway.3 Division of Endocrinology and Metabolism, Department of Internal
Medicine, Medical University of Graz, Graz, Austria.4 Department of Epidemiology and Biostatistics, EMGO Institute for
Health and Care Research, VU University Medical Centre, Amsterdam,the Netherlands.
5 Clinical Institute of Medical and Chemical Laboratory Diagnostics,Medical University of Graz, Graz, Austria.
6 Synlab Center of Laboratory Diagnostics, Heidelberg, Germany.7 Medical Faculty Mannheim, Mannheim Institute of Public Health, Social
and Preventive Medicine, University of Heidelberg, Mannheim, Germany.8 Department of Medicine, Division of Nephrology, Vestfold Hospital,
Tønsberg, Norway.9 Department of Preventive Medicine and Unit of Biostatistics and Epi-
demiology, Oslo University Hospital Ulleval, Oslo, Norway.10 Division of Nephrology, Department of Internal Medicine, Uppsala
University Hospital, Uppsala, Sweden.11 British Heart Foundation, Glasgow Cardiovascular Research Centre,
Glasgow, Scotland, United Kingdom.
12 Address correspondence to: Hege Pihlstrøm, M.D., Department ofOrgan Transplantation, Division of Nephrology, Oslo UniversityHospital, Rikshospitalet, P.B. 4950 Nydalen, 0424 Oslo, Norway.
E-mail: [email protected] digital content (SDC) is available for this article. Direct URL
citations appear in the printed text, and links to the digital files areprovided in the HTML text of this article on the journal’s Web site(www.transplantjournal.com).
All authors participated in the research design and performance of the re-search. H.P., G.M., D.O.D., K.M., S.A., and H.H. participated in thewriting of the article. W.M. contributed new reagents or analysis tools.H.P., G.M., D.O.D., S.A., I.H., and H.H. participated in data analysis.
Received 30 January 2014. Revision requested 17 February 2014.Accepted 25 March 2014.This is an open-access article distributed under the terms of the Creative
Commons Attribution-NonCommercial-NoDerivatives 3.0 License, whereit is permissible to download and share the work provided it is properlycited. The work cannot be changed in any way or used commercially.http://creativecommons.org/licenses/by-nc-nd/3.0.
Copyright * 2014 by Lippincott Williams & WilkinsISSN: 0041-1337/14/9811-1219DOI: 10.1097/TP.0000000000000205
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

patient group, further investigations on novel risk factorsfor allograft loss are of importance.
We and others have shown that markers of inflam-mation are associated with impaired long-term patient andgraft outcome (3Y5). Inflammation seems to correlate withendothelial dysfunction and early atherosclerotic changes inpatients with chronic kidney disease (CKD) (6). It has beenhypothesized that some of the excessive CV risk associatedwith CKD can be attributed to mechanisms involving oxida-tive stress (7), development of endothelial dysfunction, andreduced bioavailability of nitric oxide (NO). Nitric oxide re-laxes vascular smooth muscle and suppresses processes in-volved in vascular disease, including smooth muscle cellproliferation, leukocyte adhesion, and platelet aggregation (8).Oxidative stress is also believed to be a key element in theprogression of chronic renal disease (9, 10) and chronic allo-graft dysfunction (11, 12).
Methylarginines are formed when constituent methyl-ated arginine residues are released from intracellular proteins.These arginine analogues may interfere with NO production.High levels of asymmetric dimethylarginine (ADMA) mayreduce the levels of NO by inhibiting the enzyme NO synthase(13). Asymmetric dimethylarginine is an established risk fac-tor for CV events and mortality in different populations, and
we have previously shown an association with both renal andCV long-term outcomes in RTR (14). The structural isomer,SDMA, does not directly inhibit NO synthase but might in-directly reduce its activity by limiting arginine supply (15, 16).Furthermore, SDMA seems to participate in the inflamma-tory pathways in CKD by activation of nuclear factor-JBand increased expression of interleukin (IL)-6 and tumornecrosis factor-> (17). Plasma concentrations of ADMA andSDMA are elevated in patients with CKD (18). The role ofendogenous inhibitors of NO in transplantation is not fullyelucidated. We therefore investigated the association betweenSDMA and long-term outcomes in a well-characterized cohortof stable RTR.
RESULTSBaseline Characteristics
Participants in the Assessment of Lescol in Renal Trans-plantation (ALERT) study (19) were kidney allograft recipientswith a stable graft function. Mean time from transplantation torandomization was 5.1 years. Baseline patient data includingpatient demographics, risk factors, and comorbidity have pre-viously been presented (20).
Table 1 shows baseline characteristics for patients ac-cording to quartiles of SDMA. The groups were comparable in
TABLE 1. Demographic and baseline data according to quartiles of SDMA
SDMA quartiles Kmol/L
VariablesQ1 (n=248)
0.46Y0.88 Kmol/LQ2 (n=216)
0.88Y1.08 Kmol/LQ3 (n=232)
1.08Y1.38 Kmol/LQ4 (n=229)
1.38Y4.41 Kmol/L P
Age at baseline, yr 51.7(10.4) 51.1 (11.2) 49.0 (10.7) 47.7 (11.2) G0.001
Male sex 138 (55.6) 138 (63.9) 171 (73.7) 161 (70.3) G0.000
Current smoker 36 (14.5) 29 (13.4) 48 (20.1) 53 (23.2) 0.003
Body mass index, kg/m2 25.9 (4.2) 26.2 (4.3) 25.5 (4.7) 25.1 (4.5) 0.015
Diabetes mellitus 60 (24.2) 32 (14.8) 39 (16.8) 46 (20.1) 0.316
Hypertension 170 (68.5) 150 (69.4) 181 (78.0) 173 (75.5) 0.023
Systolic blood pressure, mm Hg 143.0 (18.8) 143.0 (18.0) 145.2 (18.0) 147.0 (21.2) 0.012
Diastolic blood pressure, mm Hg 85.7 (9.3) 85.6 (8.8) 86.5 (9.5) 85.9 (10.8) 0.548
Coronary heart disease 19 (7.7) 16 (7.4) 22 (9.4) 30 (13.1) 0.033
ADMA, Kmol/L 0.72 (0.10) 0.76 (0.10) 0.80 (0.12) 0.86 (0.16) G0.001
Serum creatinine, Kmol/L 104.1 (17.8) 124.3 (24.2) 146.6 (29.0) 196.2 (60.9) G0.001
eGFR, mL/min 63.2 (12.5) 53.3 (12.0) 45.9 (10.4) 34.6 (11.6) G0.001
Proteinuria, g/24 hr 0.22 (0.37) 0.27 (0.57) 0.42 (0.79) 0.59 (0.99) G0.001
HDL cholesterol, mmol/L 1.42 (0.45) 1.39 (0.46) 1.35 (0.44) 1.20 (0.39) G0.001
LDL cholesterol, mmol/L 4.17 (0.98) 4.24 (1.10) 4.15 (0.96) 4.12 (1.02) 0.441
Triglycerides, mmol/L 2.19 (2.13) 2.14 (1.13) 2.22 (1.39) 2.37 (1.28) G0.001
hsCRP, mg/L 2.80 (4.27) 3.64 (5.75) 3.46 (6.46) 4.23 (8.14) 0.646
IL-6, pg/mL 2.60 (1.52) 2.88 (1.89) 2.83 (1.80) 3.24 (2.02) 0.006
Time since last transplantation, yr 4.9 (3.3) 5.1 (3.3) 4.9 (3.4) 5.6 (3.6) 0.186
Time on dialysis, yr 2.0 (3.6) 2.1 (3.6) 2.5 (3.6) 2.8 (4.0) G0.001
Cold ischemia time, hr 20.0 (7.8) 18.5 (7.8) 20.2 (7.1) 19.9 (7.9) 0.535
Panel reactive antibodies 43 (18.5) 39 (19.5) 30 (14.5) 30 (16.1) 0.305
Delayed graft function 31 (12.6) 31 (14.6) 47 (20.4) 54 (24.3) G0.000
Treatment of cytomegalovirus 23 (9.4) 30 (14.4) 34 (15.5) 30 (13.6) 0.149
Total n=925.Continuous variables are shown as mean (SD); categorical variables as n (% of total).ADMA, asymmetric dimethylarginine; SDMA, symmetric dimethylarginine; HDL, high-density lipoprotein; LDL, low-density lipoprotein; hsCRP, high
sensitivity CRP; IL-6, interleukin-6. P values for linear trends (ANOVA/W2 test) are presented in the rightmost column, SD, standard deviation.
1220 www.transplantjournal.com Transplantation & Volume 98, Number 11, December 15, 2014
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

relation to time since transplantation, cold ischemia time,presence of panel reactive antibodies, and treatment of cyto-megalovirus. There were, however, more patients with delayedgraft function in the higher SDMA quartiles, and they expe-rienced generally longer time on dialysis before transplanta-tion. Symmetric dimethylarginine was positively associatedwith proteinuria and inversely correlated with estimated glo-merular filtration rate (eGFR). Also, patients with elevatedSDMA at baseline were slightly younger, more likely to bemenand smokers, and showed a higher burden of coronary heartdisease, hypertension, and dyslipidemia. Also, IL-6 valueswere significantly higher in the 4th SDMA quartile, whereashigh sensitivity C-reactive protein (hsCRP) showed no suchassociation with SDMA. P values for linear trends (analysisof variance and chi-square test) are presented in the right-most column of Table 1.
Correlation AnalysisCorrelation analyses were performed between SDMA
andmeasures of kidney function as well as ADMA and selectedparameters of inflammation (calculations not shown). Thecorrelation coefficient was 0.77 for creatinine and 0.72 foreGFR. Symmetric dimethylarginine was significantly correlatedwith ADMA (r=0.40) and IL-6 (r=0.09), but not hsCRP(r=0.02, nonsignificant).
Survival AnalysisResults from univariate and multivariate Cox regres-
sion analyses are presented in Table 2. Fifty-two participantshad missing values for one or more of the covariates and wereexcluded from the multivariate model. Hazard ratios (HRs)with corresponding 95% confidence intervals (95% CI) areshown for all study outcomes. The multivariate model is ad-justed for baseline characteristics and potentially importantrisk factors including age, sex, smoking habit, establishedcoronary heart disease, systolic blood pressure, low-densitylipoprotein cholesterol, diabetes mellitus, hsCRP, ADMA,and eGFR split into quartiles.
Symmetric dimethylarginine showed a positive associ-ation with all study outcomes in univariate analysis, whereasafter multivariate adjustment, there was a significant increasedrisk of death (HR, 4.56; 95% CI, 2.15Y9.71; PG0.001) and graftloss (HR, 5.51; 95% CI, 1.95Y15.57; P=0.001) in the highestSDMA quartile. When the mortality variable was furthersubdivided by cause of death, there was a strong associa-tion between SDMA and non-CV death (HR, 7.54; 95% CI,2.54Y22.40; PG0.001). For CV death, the increased risk as-sociated with SDMA in quartile 4 was borderline significant(HR, 2.86; 95% CI, 0.99Y8.21; P=0.051). A higher frequencyof major adverse CV events (MACE) was seen in the4th SDMA quartile, although this trend was not statistically
TABLE 2. Cox Regression Analysis for study outcomes using SDMA quartile 1 (Q1) as reference
SDMA quartiles
Outcome
Q1 0.46Y0.88 Kmol/L Q2 0.88Y1.08 Kmol/L Q3 1.08Y1.38 Kmol/L Q4 1.38Y4.41 Kmol/L
n=248 n=216 n=232 n=229
MACE
Number of events 26 (10.5%) 24 (11.1%) 30 (12.9%) 40 (17.5%)
Univariate HR (95% CI) 1 1.03 (0.59Y1.80) 1.24 (0.73Y2.09) 1.88 (1.15Y3.09)Multivariate HR (95% CI) 1 0.99 (0.54Y1.83) 1.10 (0.56Y2.14) 1.64 (0.75Y3.58)
All-cause mortality
Nr of events 21 (8.5%) 20 (9.3%) 23 (9.9%) 61 (26.6%)
Univariate HR (95%CI) 1 1.04 (0.56Y1.91) 1.15 (0.64Y2.08) 3.53(2.15Y5.79)Multivariate HR (95%CI) 1 1.40 (0.72Y2.71) 1.70 (0.83Y3.47) 4.56 (2.15Y9.71)
Cardiovascular death
Number of events 12 (4.8%) 11 (5.1%) 13 (5.6%) 29 (12.7%)
Univariate HR (95% CI) 1 1.06 (0.48Y2.37) 1.12 (0.51Y2.46) 2.91 (1.48Y5.70)Multivariate HR (95%CI) 1 1.34 (0.56Y3.22) 1.47 (0.56Y3.87) 2.86 (0.99Y8.21)
Noncardiovascular death
Number of events 9 (3.6%) 9 (4.2%) 10 (4.3%) 32 (14.0%)
Univariate HR (95% CI) 1 0.99 (0.38Y2.57) 1.19 (0.48Y2.93) 4.36 (2.08Y9.14)Multivariate HR (95%CI) 1 1.41 (0.51Y3.92) 1.97 (0.68Y5.74) 7.54 (2.54Y22.40)
RGL
Number of events 6 (2.4%) 14 (6.5%) 24 (10.3%) 80 (34.9%)
Univariate HR (95%CI) 1 2.65 (1.02Y6.88) 4.44 (1.82Y10.87) 19.70 (8.59Y45.16)Multivariate HR (95%CI) 1 1.62 (0.59Y4.48) 1.86 (0.68Y5.11) 5.51 (1.95Y15.57)
Number of events (in percentage of total) registered in each SDMA quartile during a mean of 5.1 years of follow-up. Univariate and multivariate hazardratios with 95% confidence intervals (HR, 95% CI) for study outcomes for each SDMA quartile compared with the first quartile. In the multivariate modeladjustments were made for: age, sex, diabetes mellitus, smoking status, systolic blood pressure, LDL cholesterol, coronary artery disease, ADMA, hsCRP andeGFR in quartiles.
MACE, major adverse cardiovascular events; RGL, renal graft loss; cardiovascular death, cardiac, vascular, and cerebrovascular deaths; HR, hazard ratio;9%% CI, 95% confidence interval; hsCRP, high sensitivity C-reactive protein; LDL, low-density lipoprotein.
* 2014 Lippincott Williams & Wilkins Pihlstrøm et al. 1221
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

significant in multivariate analysis (HR, 1.64; 95%CI, 0.75Y3.58;P=0.212). We were not able to reveal any significant com-peting risks between nonfatal MACE and all-cause mortality(data not shown).
Figure 1 presents adjusted HRs with correspondingP values for the three most important causes of death: CVevents, infection, and cancer. Compared with the first quartile,there was amore than ninefold increase in the risk of dying fromcancer and a more than sevenfold increased risk of death byinfection in the fourth SDMA quartile. The occurrence ofdeath from cancer or infection according to SDMA quartilesare shown in Table S1 (SDC, http://links.lww.com/TP/A994).
Figures 2 to 3 show adjusted Cox hazard functions forall-cause death and renal graft loss according to SDMA quar-tiles, illustrating the relationship between SDMA level and therisk of adverse events as a function of time.
In an initial analysis, IL-6 replaced CRP without causingnoticeable changes in HR for any of the study outcomes (datanot shown). Furthermore, we constructed an extended modelfor the prediction of graft loss, adding to the multivariateanalysis the following plausible risk factors for adverse renaloutcome: time since last transplantation, total time on renalreplacement therapy, baseline level of proteinuria, delayedgraft function, and treatment of rejection (before randomi-zation). Importantly, this extensive multivariate adjustmentrendered the HR for SDMA quartile 4 essentially unchanged(HR, 4.02; CI, 1.37Y11.80; P=0.011).
DISCUSSIONThis study is the first to report that increased serum
levels of SDMA, adjusted for traditional and nontraditionalrisk factors, are associated with reduced long-term graft and
patient survival in kidney transplant recipients. The associ-ation between SDMA and clinical outcomes does not appearfully linear, the risk increasing substantially from the third tothe fourth quartile. The increased HR for all-cause mortalityin the fourth quartile was mainly driven by non-CV causes,but there was still borderline significance for an associationbetween SDMA and CV death.
An association between SDMA and mortality has pre-viously been reported in several nontransplanted populations:in patients referred for angiography (21, 22), in patients afteran ischemic stroke (23) and in stable coronary heart diseasepatients(24). Recently, SDMA was found to independentlypredict mortality in a large (n=3523) multiethnic cohort rep-resentative of the general population (25). One study indicatesthat in an older population, plasma levels of SDMA seem pre-dictive of CV events (26). Significant relationships betweenSDMA and development of major CV events have been foundin patients undergoing elective diagnostic cardiac catheteriza-tion (21, 22), patients with stable coronary heart disease (24)
FIGURE 1. Hazard ratios with corresponding P values inthe fourth SDMA quartile (SDMA Q4) stratified by cause ofdeath. Multivariate Cox regression analysis adjusted forage, sex, diabetes mellitus, smoking status, systolic bloodpressure, LDL cholesterol, coronary artery disease, hsCRP,ADMA and eGFR in quartiles. SDMA, symmetric dimethyl-arginine; hsCRP, high sensitivity C-reactive protein; ADMA,asymmetric dimethylarginine; LDL, low-density lipoprotein.
FIGURE 2. Adjusted cumulative hazard curves for all-cause mortality by quartiles of SDMA (SDMAq=1Y4). SDMA,symmetric dimethylarginine.
FIGURE 3. Adjusted cumulative hazard curves for renalgraft loss by quartiles of SDMA (SDMAq=1Y4). SDMA,symmetric dimethylarginine.
1222 www.transplantjournal.com Transplantation & Volume 98, Number 11, December 15, 2014
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and patients with non-ST-elevationmyocardial infarction (27).In patients with CKD (28, 29) and in primary care patientswith and without peripheral arterial disease (30), increasedCV risk was not related to SDMA.
The relationship between high SDMA and increasedrisk of all-cause death seems robust in our cohort of RTR.We identified a trend, but no significant association betweenSDMA levels and the composite endpoint of major CVevents. For CV death, there was an almost threefold higherrisk associated with the highest SDMA-quartile, althoughjust borderline significant. In conclusion, our findings extendand corroborate that SDMA may be a marker for CV eventsand all-cause death (21).
We also showed that a high SDMA level in clinicallystable RTR is independently predictive of renal graft loss.The possibility of SDMA being a separate risk factor foradverse renal outcomes in RTR has not previously beenstudied. Busch et al. (29) looked at the prognostic role ofboth ADMA and SDMA in a heterogeneous populationof 200 CKD-patients including 37 renal transplant patients.Their results indicate that an increased serum level of SDMA(but not ADMA) might be a predictor for the progression toend-stage renal disease.
Compared to the healthy general population, meanSDMA levels were elevated in our RTR cohort (31, 32). OurSDMA values were in concert with a review by Fleck et al.(33) demonstrating high levels of dimethylarginines in end-stage renal disease patients, SMDA levels decreasing afterrenal transplantation, though not reaching reference valuesfor healthy subjects.
Possible mechanisms for the relationship between highSDMA and poor long-term outcomes are not well defined.Symmetric dimethylarginine is believed to be biochemicallyinert and eliminated solely by renal filtration (34, 35). Hence,most of the difference in SDMA concentrations between var-ious populations could be explained by its strong covariancewith kidney function; an association first shown in a study onhypertensive children (36). A meta-analysis by Kielstein et al.(37) reports a correlation coefficient of 0.77 and 0.78 be-tween SDMA and various GFR estimates and insulin clear-ance, respectively. In our study, we found a similar level ofcorrelation between SDMA and eGFR. Even so, after adjustingfor eGFR, SDMAwas still independently associated with graftloss and mortality.
Symmetric dimethylarginine may influence L-arginineavailability (35). Associations between dimethylarginines andCV disease in different patient groups are believed mainly toresult from negative effects of these substances on endothelialfunction (38, 39), although a recent publication by Siegerinket al. (24) questions this, suggesting that alternative mecha-nisms for both dimethylarginines should be considered.
Symmetric dimethylarginine may trigger vascular pa-thology by modulation of store-operated calcium channelsin monocytes (40), thus exerting a proinflammatory effect.Symmetric dimethylarginine is also shown to be involved ininflammatory pathways in CKD patients by activating nuclearfactor-JB, leading to enhanced expression of tumor necrosisfactor-> and IL-6 (17). Hence, a raised SDMA level may con-tribute to increasing the inflammatory burden.
The mean level of SDMAwas significantly higher in ourcohort than inmost populations. A high SDMA level seems to
identify a subpopulation of RTRmore likely do die of infectionsand cancer. There is no known mechanism of action pro-viding a plausible link between high serum levels of SDMAand the development of infection or malignancy in RTR. Ahigh proportion of cancers in RTR are lymphoproliferativeand related to infections with Epstein-Barr virus, humanherpesvirus 8, human papilloma virus or the hepatitis B andC viruses (41). Symmetric dimethylarginine residuals are shownto be important constituents of the Epstein-Barr virusYencodednuclear antigen 2 which is responsible for growth trans-formations in B lymphocytes(42, 43), but whether virus-relatedmalignancy is associated with increased plasma levels ofSDMA is not known. Further studies are needed to elaborateon this as well as to investigate whether associations betweenSDMA and specific non-CV causes of death can be found inother populations.
The main analysis is based on the placebo arm of thestudy. This cohort was selected because we wished to avoidthe risk of interactions with the active intervention (statintherapy), as it is possible that statin use could modify SDMAlevels or the biologic actions of SDMA. Degree ofendothelium-dependent vasodilatation achieved by simva-statin treatment was indeed shown to vary across levels ofADMA (44), pointing in the direction of a possible interac-tion between statins and dimethylarginines. Statin treatmentmight improve endothelial function both in RTR (45) and inthe general population (46). Endothelial NO synthase isupregulated by statins (47). Possibly, some of the beneficialeffects of statins are mediated through pathways involvingdimethylarginines. In our study, SDMA was measured atbaseline only, before the initiation of statin therapy. Hence,speculations on mechanisms involved in the suspected in-teraction between SDMA and statin treatment was beyondthe scope of this article.
The prospective controlled design, the long time offollow-up, the large patient cohort, and the independent ad-judication of all clinical endpoints are major strengths of ourstudy. However, there are potential limitations which meritconsideration. Although the statistics show significant asso-ciations between SDMA and mortality as well as the renalendpoint, the data do not prove a casual relationship. Fur-thermore, the study population, a cohort selected for entryinto a clinical trial, is not necessarily fully representative ofthe general renal transplant population
In conclusion, this is the first study to report that in-creased plasma levels of SDMA in stable RTR are significantlyassociated with future graft loss and all-cause mortality.
MATERIALS AND METHODSStudy Design
A post hoc analysis was performed using the data from RTR includedin the ALERT trial. Study design with baseline data has previously beendescribed (20). In short, this randomized, double-blind, placebo-controlledstudy examined the effect of fluvastatin (40Y80 mg daily) on cardiac and renaloutcomes in 2102 RTR. Inclusion criteria were stable RTRs aged 30Y75 yearshaving received a renal transplant more than 6 months before study start andhaving serum cholesterol in the range of 4.0Y9.0 mmol/L (155Y348 mg/dL).Exclusion criteria were ongoing statin therapy, familial hypercholesterolemia,an acute rejection episode in the last 3 months before inclusion or predictedlife expectancy of less than 1 year. The original trial had a follow-upmean timeof 5.1 years.
* 2014 Lippincott Williams & Wilkins Pihlstrøm et al. 1223
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

The ALERT study adhered to the International Conference on Harmoni-zation guidelines for Good Clinical Practice and was conducted in accordancewith the Declaration of Helsinki Principles. Written informed consent wasobtained from all patients included, and the trial was approved by the localethics committee at each participating center.
Outcome DefinitionsCardiac study outcome was the original primary endpoint in the ALERT
trialVa composite endpoint of MACE, defined as time to cardiac death,non-fatal myocardial infarction or performed coronary revascularizationprocedure. Renal outcome was time to first renal graft loss (death-censored).General survival outcome was time to death from all causes. An independentclinical endpoint committee blinded to study drug allocation validated allendpoints (19, 20).
LaboratoryBaseline laboratory values of the ALERT trial have been reported previ-
ously(20). Symmetric dimethylarginine level was measured at baseline to beassessed as a risk factor at inclusion, a mean 5.1 years after transplantation.Reversed-phased high-performance liquid chromatography was used tomeasure SDMA level in frozen serum (j80-C) obtained from 925 of the 1,052participants in the placebo arm, the last 127 samples missing at random.Estimated GFR (mL/min per 1.73 m2) was calculated by the formula fromthe Modification of Diet in Renal Disease study (48).
Statistical AnalysisIn reviewing the literature before conducting our analyses, we found
evidence of a possible effect of statins on endothelial function. Initial sta-tistical analyses indicated a significant interaction between SDMA and ran-domization group. Consequently, for a clean approach, we used the placeboarm only in subsequent analyses.
Study participants were stratified into quartiles according to SDMAlevels. For comparison of demographics and known risk factors acrossquartiles, P values for continuous variables were calculated using anal-ysis of variance with linear trend, whereas for categorical variables, weused the chi-square linear test for proportions. The variables IL-6,hsCRP, triglycerides, ADMA, creatinine, proteinuria, time since last trans-plantation, and time on dialysis were logarithmically transformed to correctfor skewness.
Survival analyses were performed by Cox proportional hazard models.We calculated HRs with 95% CI by comparing the upper three quartiles tothe first. We did not calculate HRs for SDMA as a continuous vari-able because the association between SDMA and outcomes appeared non-linear when using categorical approach. Crude and multivariate adjustedHRs are presented. The multivariate model was adjusted for plausible con-founders based on clinical knowledge and published literature. Colinearitybetween eGFR and SDMA was not a problem because standard errorsremained of acceptable size when including both parameters in the statis-tics. Because eGFR as a continuous variable did not fully meet the pro-portional hazards assumption, we split this variable into quartiles forinclusion in subsequent statistical analyses. Remaining covariates ful-filled the proportionality assumptions according to the Schoenfeld re-siduals test. Possible competing risks between MACE (as study endpoint)and all-cause mortality (as competing risk endpoint) were examined bysensitivity analysis (49), including the subdistribution hazards method de-scribed by Fine and Gray (50).
All analyses were performed using SPSS version 18.0 (IBM, New York)and STATA version 11 (StataCorp, College Station, TX).
ACKNOWLEDGMENTSThe authors thank all patients who participated in the
ALERT study as well as all investigators, study nurses, andcollaborators involved in the trial.
The authors thank Ph.D. student Elisabeth Størset forthe design and construction of Figure 1.
REFERENCES1. Jardine AG, Gaston RS, Fellstrom BC, et al. Prevention of cardiovas-
cular disease in adult recipients of kidney transplants. Lancet 2011;378: 1419.
2. Lamb KE, Lodhi S, Meier-Kriesche HU. Long-term renal allograftsurvival in the United States: a critical reappraisal. Am J Transplant2011; 11: 450.
3. Abedini S, Holme I, Marz W, et al. Inflammation in renal transplan-tation. Clin J Am Soc Nephrol 2009; 4: 1246.
4. Dahle DO, Mjoen G, Oqvist B, et al. Inflammation-associatedgraft loss in renal transplant recipients. Nephrol Dial Transplant2011; 26: 3756.
5. Jabs WJ, Meier M, Lamprecht P, et al. Local expression of C-reactiveprotein is associated with deteriorating graft function in acute andchronic failure of kidney transplants. Nephron Clin Pract 2011; 117: c390.
6. Recio-Mayoral A, Banerjee D, Streather C, et al. Endothelial dysfunc-tion, inflammation and atherosclerosis in chronic kidney diseaseVacross-sectional study of predialysis, dialysis and kidney-transplantationpatients. Atherosclerosis 2011; 216: 446.
7. Popolo A, Autore G, Pinto A, et al. Oxidative stress in patients withcardiovascular disease and chronic renal failure. Free Radic Res 2013;47: 346.
8. Schafer A, Bauersachs J. Endothelial dysfunction, impaired endogenousplatelet inhibition and platelet activation in diabetes and atherosclerosis.Curr Vasc Pharmacol 2008; 6: 52.
9. Kobayashi M, Sugiyama H, Wang DH, et al. Catalase deficiency ren-ders remnant kidneys more susceptible to oxidant tissue injury andrenal fibrosis in mice. Kidney Int 2005; 68: 1018.
10. Sener G, Paskaloglu K, Satiroglu H, et al. L-carnitine amelioratesoxidative damage due to chronic renal failure in rats. J CardiovascPharmacol 2004; 43: 698.
11. Kedzierska K, Domanski M, Sporniak-Tutak K, et al. Oxidative stressand renal interstitial fibrosis in patients after renal transplantation:current state of knowledge. Transplant Proc 2011; 43: 3577.
12. Djamali A. Oxidative stress as a common pathway to chronic tubu-lointerstitial injury in kidney allografts. Am J Physiol Renal Physiol 2007;293: F445.
13. Vallance P, Leone A, Calver A, et al. Endogenous dimethylarginine asan inhibitor of nitric oxide synthesis. J Cardiovasc Pharmacol 1992;20(Suppl 12): S60.
14. Abedini S, Meinitzer A, Holme I, et al. Asymmetrical dimethylarginineis associated with renal and cardiovascular outcomes and all-causemortality in renal transplant recipients. Kidney Int 2010; 77: 44.
15. Closs EI, Basha FZ, Habermeier A, et al. Interference of L-arginineanalogues with L-arginine transport mediated by the y+ carrier hCAT-2B. Nitric Oxide 1997; 1: 65.
16. Bogle RG, MacAllister RJ, Whitley GS, et al. Induction of NG-monomethyl-L-arginine uptake: a mechanism for differential inhibi-tion of NO synthases? Am J Physiol 1995; 269: C750.
17. Schepers E, Barreto DV, Liabeuf S, et al. Symmetric dimethylarginineas a proinflammatory agent in chronic kidney disease. Clin J Am SocNephrol 2011; 6: 2374.
18. Schwedhelm E, Boger RH. The role of asymmetric and symmetricdimethylarginines in renal disease. Nat Rev Nephrol 2011; 7: 275.
19. Holdaas H, Fellstrom B, Jardine AG, et al. Effect of fluvastatin oncardiac outcomes in renal transplant recipients: a multicentre, ran-domised, placebo-controlled trial. Lancet 2003; 361: 2024.
20. Holdaas H, Fellstrom B, Holme I, et al. Effects of fluvastatin on cardiacevents in renal transplant patients: ALERT (Assessment of Lescol inRenal Transplantation) study design and baseline data. J CardiovascRisk 2001; 8: 63.
21. Meinitzer A, Kielstein JT, Pilz S, et al. Symmetrical and asymmetricaldimethylarginine as predictors for mortality in patients referred forcoronary angiography: the Ludwigshafen Risk and CardiovascularHealth study. Clin Chem 2011; 57: 112.
22. Wang Z, Tang WH, Cho L, et al. Targeted metabolomic evaluation ofarginine methylation and cardiovascular risks: potential mechanismsbeyond nitric oxide synthase inhibition. Arterioscler Thromb Vasc Biol2009; 29: 1383.
23. Schulze F, Carter AM, Schwedhelm E, et al. Symmetric dime-thylarginine predicts all-cause mortality following ischemic stroke.Atherosclerosis 2010; 208: 518.
24. Siegerink B, Maas R, Vossen CY, et al. Asymmetric and symmetricdimethylarginine and risk of secondary cardiovascular disease events
1224 www.transplantjournal.com Transplantation & Volume 98, Number 11, December 15, 2014
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

and mortality in patients with stable coronary heart disease: theKAROLA follow-up study. Clin Res Cardiol 2013; 102: 193.
25. Gore MO, Luneburg N, Schwedhelm E, et al. Symmetrical di-methylarginine predicts mortality in the general population: observa-tions from the Dallas Heart Study. Arterioscler Thromb Vasc Biol 2013;33: 2682.
26. Kiechl S, Lee T, Santer P, et al. Asymmetric and symmetric dimethyl-arginines are of similar predictive value for cardiovascular risk in thegeneral population. Atherosclerosis 2009; 205: 261.
27. Cavalca V, Veglia F, Squellerio I, et al. Circulating levels of dimethyl-arginines, chronic kidney disease and long-term clinical outcome innon-ST-elevation myocardial infarction. PLoS One 2012; 7: e48499.
28. Zoccali C, Bode-Boger S, Mallamaci F, et al. Plasma concentrationof asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: a prospective study. Lancet 2001; 358: 2113.
29. Busch M, Fleck C, Wolf G, et al. Asymmetrical (ADMA) and sym-metrical dimethylarginine (SDMA) as potential risk factors forcardiovascular and renal outcome in chronic kidney diseaseVpossible candidates for paradoxical epidemiology? Amino Acids2006; 30: 225.
30. Boger RH, Endres HG, Schwedhelm E, et al. Asymmetric dimethyl-arginine as an independent risk marker for mortality in ambulatorypatients with peripheral arterial disease. J Intern Med 2011; 269: 349.
31. Schwedhelm E, Xanthakis V, Maas R, et al. Plasma symmetric dimethyl-arginine reference limits from the Framingham offspring cohort. ClinChem Lab Med 2011; 49: 1907.
32. Hov GG, Sagen E, Bigonah A, et al. Health-associated reference valuesfor arginine, asymmetric dimethylarginine (ADMA) and symmetricdimethylarginine (SDMA) measured with high-performance liquidchromatography. Scand J Clin Lab Invest 2007; 67: 868.
33. Fleck C, Schweitzer F, Karge E, et al. Serum concentrations of asym-metric (ADMA) and symmetric (SDMA) dimethylarginine in patientswith chronic kidney diseases. Clin Chim Acta 2003; 336: 1.
34. Fliser D, Kronenberg F, Kielstein JT, et al. Asymmetric dimethylarginineand progression of chronic kidney disease: the mild to moderate kidneydisease study. J Am Soc Nephrol 2005; 16: 2456.
35. Bode-Boger SM, Scalera F, Kielstein JT, et al. Symmetrical dimethyl-arginine: a new combined parameter for renal function and extent ofcoronary artery disease. J Am Soc Nephrol 2006; 17: 1128.
36. Goonasekera CD, Rees DD, Woolard P, et al. Nitric oxide synthaseinhibitors and hypertension in children and adolescents. J Hypertens1997; 15: 901.
37. Kielstein JT, Salpeter SR, Bode-Boeger SM, et al. Symmetric dimethyl-arginine (SDMA) as endogenous marker of renal functionVa meta-analysis. Nephrol Dial Transplant 2006; 21: 2446.
38. Boger RH, Zoccali C. ADMA: a novel risk factor that explains excesscardiovascular event rate in patients with end-stage renal disease.Atheroscler Suppl 2003; 4: 23.
39. Yamagishi S, Ueda S, Nakamura K, et al. Role of asymmetric dimethyl-arginine (ADMA) in diabetic vascular complications. Curr Pharm Des2008; 14: 2613.
40. Schepers E, Glorieux G, Dhondt A, et al. Role of symmetric di-methylarginine in vascular damage by increasing ROS via store-operatedcalcium influx in monocytes. Nephrol Dial Transplant 2009; 24: 1429.
41. Wong G, Chapman JR. Cancers after renal transplantation. TransplantRev (Orlando) 2008; 22: 141.
42. Barth S, Liss M, Voss MD, et al. Epstein-Barr virus nuclear antigen2 binds via its methylated arginine-glycine repeat to the survivalmotor neuron protein. J Virol 2003; 77: 5008.
43. Gross H, Barth S, Palermo RD, et al. Asymmetric arginine dimethyla-tion of Epstein-Barr virus nuclear antigen 2 promotes DNA targeting.Virology 2010; 397: 299.
44. Boger GI, Rudolph TK, Maas R, et al. Asymmetric dimethylargininedetermines the improvement of endothelium-dependent vasodilationby simvastatin: effect of combination with oral L-arginine. J Am CollCardiol 2007; 49: 2274.
45. Asberg A, Hartmann A, Fjeldsa E, et al. Atorvastatin improves endo-thelial function in renal-transplant recipients. Nephrol Dial Transplant2001; 16: 1920.
46. Reriani MK, Dunlay SM, Gupta B, et al. Effects of statins on coronaryand peripheral endothelial function in humans: a systematic reviewand meta-analysis of randomized controlled trials. Eur J CardiovascPrev Rehabil 2011; 18: 704.
47. Laufs U, La Fata V, Plutzky J, et al. Upregulation of endothelial nitricoxide synthase by HMG CoA reductase inhibitors. Circulation 1998;97: 1129.
48. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method toestimate glomerular filtration rate from serum creatinine: a newprediction equation. Modification of Diet in Renal Disease StudyGroup. Ann Intern Med 1999; 130: 461.
49. Thabane L, Mbuagbaw L, Zhang S, et al. A tutorial on sensitivityanalyses in clinical trials: the what, why, when and how. BMC Med ResMethodol 2013; 13: 92.
50. Fine J, Gray R. A proportional hazards model for the subdistributionof a competing risk. J Am Stat Assoc 1999; 94: 496.
* 2014 Lippincott Williams & Wilkins Pihlstrøm et al. 1225
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.


III
