emergency pediatric group department … · 2010-03-29 · admission/transfer guidelines ... rapid...
TRANSCRIPT

EMERGENCY PEDIATRIC GROUP
DEPARTMENT MEETINGJuly 11, 2007

2
Announcements
New fellowsNew Hires• Parmi Suchdev - start date July 1, 2007• Tracy Merrill - August 14, 2007• Tiffany McKinnie - August 14, 2007• Susan Goldberg - October 1, 2007
PEM candidate• Amita Schroff - Long Island Jewish• Sephora Morrison - Children’s Memorial-
Graduating June 2008Salmonella Wandsworth outbreak• Veggie booty bags implicated
Education on medical photographyDr Cornish will present faculty productivity

Volume Indicators

4
Census: 3 year CHOA-HS
2500300035004000450050005500
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 data
Census: 3 years: CHOA-ECH
2,0002,5003,0003,5004,0004,5005,0005,500
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 data

5
Admissions: CHO
0
50
100
150
200
250
300
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 da
Admissions: CHOA-ECH
0100200300400500600
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 data

6
Walkouts: CHOA-H
0
50
100
150
200
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 data
Walkouts: CHOA-ECH
0.0%0.5%1.0%1.5%2.0%2.5%3.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2005 data 2006 data 2007 data
Hughes Spalding

8
Hughes Spalding
Staffing – 2 nurses and 2 techs have been hiredIssues with transfers –• No ortho transfers will be accepted at HS• If CHOA does not give priority to a transfer, let Dr.
Khan knowQuestions about changes slated over the next monthsNew VP: Julia JonesPAC moonlighting• Looking for volunteers
9a-3pSeeing fast track patients
Alert• New interns: provide close supervision• Do not leave the ED/ UC without informing the senior
resident and charge nurse (even for a few minutes)• Prehospital medications cannot be given to patients
once they arrive in the ED

Division of Pediatric Emergency Medicine
Physician education: changes at Hughes Spalding
June 23, 2007July 11, 2007

10
HSOC Patient Safety Charge
Develop a plan which ensures safe implementation of the inpatient service plan recommendations for Hughes Spalding
which meets the quality and safety standards of Children’s and is within the financial constraints of the organization.

11
Working Team Goals
IP Working Team
Goal: To develop a detailed plan for the stabilization of children who are too sick to be admitted to HS and to identify the plan for their transportation to Egleston or Scottish Rite.
ED Working Team
Goal: To identify admission/transfer guidelines for HS inpatients and develop the details of a hospitalist program to support the patients who are admitted. To define guidelines and procedures for potential critical inpatient clinical scenarios.

12
IP Working Team MembersWorking Team Leads:Dr. PettignanoDr. Graham
Working Team Members:Dr. FlowersDr. TaylorDr. KeyesDr. Kohrt
Others Consulted:Dr. MillerDr. DelgadoDr. MooreDr. DunstonDr. PettitDr. StollDr. Tyler-Hill)

13
ED Working Team MembersWorking Team Leads:Dr. KhanDr. McCrory
Working Team Members:Dr. FortenberryLinda Cole
Consulting Members:Dr. PetrilloDr. KingDr. GooDr. SpizmanCyndie RobersonKevin Wall

Recommendations
15
Admission and transfer guidelines
16
Basis for decisions
No ICU
Ability to safely care for the patient
On-going evaluation to expand or contract guidelines
Implementation of these guidelines may initially decrease admissions
Centralized dispatch can offload less acute patients from other campuses to Hughes Spalding where appropriate

ED patients who do not meet criteria for admission to HS and would
require transfer

18
General
Patients who require a higher level of care (medications or resource needs) in excess of that provided in the general patient care unitat Hughes Spalding• Patients who require one-on-one nursing
care• Patients who require specialty care not
provided at Hughes Spalding

19
SpecificRespiratory• O2 requirement ≥ 50%, to maintain SpO2 ≥ 92% at the
time of ED disposition• More than one reported or witnessed apnea with color
change• Intubated patients• BiPaP / CPAP requiring ≥50% O2 and/or more then one
dose of sedation• Patients with immature tracheotomy (≤ 2weeks)• Asthma patients requiring ketamine infusion
Neurological• Acute onset altered mental status requiring continuous
monitoring and/or > q2hr neuro-checks• Intracranial bleeds, masses, CVA’s, increased ICP• Ventricular shunt patients with shunt related problems• Post-op neurosurgical complications

20
Specific
Cardiovascular• Hemodynamic instability not improved with fluids
alone• Patients requiring inotropes, vasodilators, anti-
arrhythmics, cardioversion• High risk cardiac patients with complex
congenital conditions, shunts, pacemakers, open thoracotomy
• Patients with acute myocardial/ pericardial disease
Hematologic/Oncologic Diseases• All active oncology patients• All unstable hematology patients
21
Specific
Gastrointestinal Diseases
• Acute GI bleed with hemodynamic or respiratory instability
• Patients requiring endoscopy for FB removalSurgical
• All patients requiring acute surgical intervention• All major trauma patients with unstable and/or life
threatening injuriesRenal
• Patients with signs of acute renal failure• Patients requiring hemodialysis, peritoneal dialysis

22
To be developed:
Clinical Guidelines• To be developed by the ED physicians• Include permissible length of stay and extent of
interventions prior to assigning disposition• Including but not limited to the following disease
processesAsthmaBronchiolitisDKADehydration with acidosis and/or hypotensionIngestionsAcute abdomenIntussusceptionAltered mental statusApnea with color change
23
Approach to a patient deteriorating on the floor

24
Approach to Clinically Worsening Patient
P a t i e n t a d m i t t e d t o G e n e r a l P e d ia t r ic s F lo o r
C h a n g e in p a t ie n t s t a tu s
C l in ic a l c h a n g e b u t n o t u n s ta b le C a r d io p u lm o n a r y i n s ta b i l i t y N o t i f y s e n io r r e s id e n t C o d e b lu e U n a b le to r e s p o n d R e s p o n d s o r C o d e t e a m * * r e s p o n d s n e e d f o r p r e l im in a r y e v a lu a t io n e v a lu a t io n R R T * e v a lu a t i o n P a t i e n t s t a b i l i z e d i n te r v e n t io n p r n R a p id r e s p o n s e t e a m * H o s p i t a l i s t n o t i f i e d N o t i f y C o d e b lu e H o s p i t a l i s t E v a lu a t io n T r a n s f e r b a s e d o n D i s c u s s io n o f g u id e l in e s f u r th e r C o d e T e a m * * i n t e r v e n t io n /d i s p o s i t io n C a l l r e s id e n t S u g g e s t s i n t e r v e n t io n
F u r th e r In te r v e n t io n T r a n s f e r o r c o n t in u e d c a r e b a s e d o n g u id e l in e s N o t i f y h o s p i t a l i s t o f r e c o r d o r h o s p i ta l i s t o n c a l l
T r a n s f e r o r c o n t in u e d c a r e b a s e d o n g u id e l in e s

25
A dedicated hospitalist group at HS
26
Why a hospitalist program at HS?Dedicated patient care Expertise in disease managementComfort with identified patient populationImproved quality, error reductionImproved patient satisfaction
Critical components needed at HS:Board Eligible/Certified in Pediatrics or a Pediatric Sub-SpecialtyDedicated hospitalist 24/7
• (i.e. when assigned to hospital, they do not have any other clinical responsibilities).
Minimum of 3 months of clinical service per yearCall from home, return when needed

27
Hospitalist Program
Key components still to be determined:
Hospitalist job descriptionNumber of teamsMedical school representationNumber of FTE’sAcceptable call scheduleDetermine core competencies in
Disease managementProcedures
Develop education componentDevelop Q/I program
28
Critical Success Factors
Keeping the best interest of the patient as our driving forceCreative thinking and flexibilityProvider buy-in (MD’s, nurses, respiratory others)Ensuring provider training and competency on an ongoing basisFlexible nursing/RRT model to accommodate children needing a greater nurse/RRT to patient ratioContinued reevaluation of admission and transfer guidelinesSuccessful QI program

29
IP Critical Success Factors..Contd
Dedicated inpatient providers
In depth understanding of:Admission criteriaTransfer criteriaApproach to the worsening patient
Inpatient MD comfort with saying “no” to the ED
Inpatient MD returning to hospital to evaluate the “sick or sicker” childhelp with stabilization and transfer
ED MD comfort with decision to transfer
Acceptance and buy-in of key physicians and leaders at SR and EG with regard to HS’s transfer criteria and policies.
Algorithm for Transfer site selection
Implementation July 1, 2007
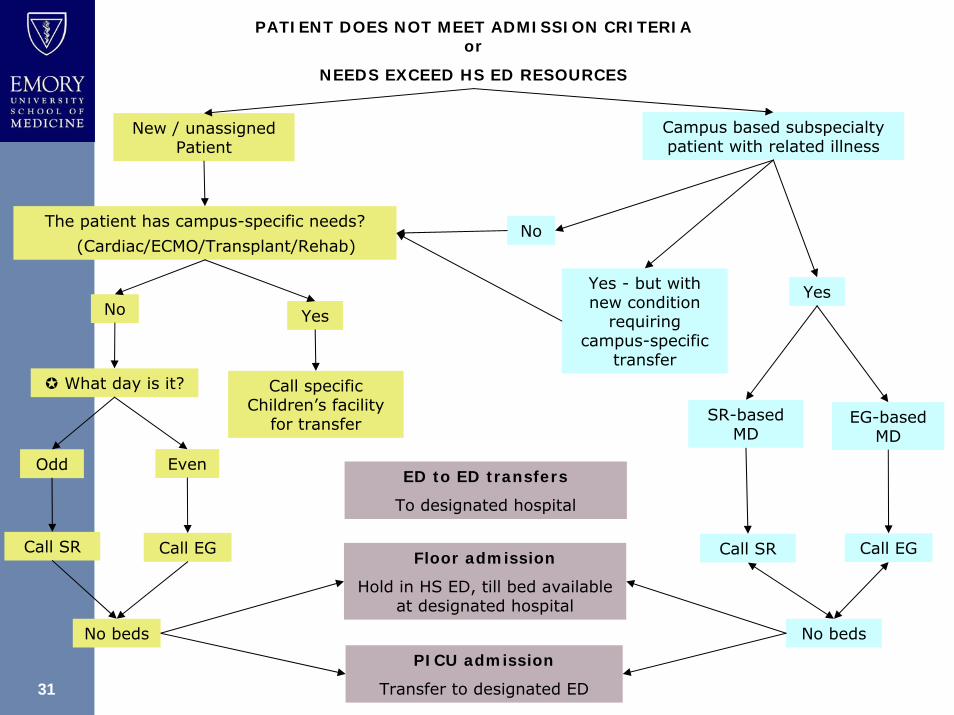
31
PATIENT DOES NOT MEET ADMISSION CRITERIA or
NEEDS EXCEED HS ED RESOURCES
New / unassigned Patient
The patient has campus-specific needs?
(Cardiac/ECMO/Transplant/Rehab)
Campus based subspecialty patient with related illness
No Yes
No
Yes
What day is it?
Odd Even
Call SR Call EG
PICU admission
Transfer to designated ED
Yes - but with new condition
requiring campus-specific
transfer
EG-based MD
Call SR Call EG
Call specific Children’s facility
for transfer SR-based MD
No beds
Floor admission
Hold in HS ED, till bed available at designated hospital
No beds
ED to ED transfers
To designated hospital
32
ED physician and resident staffing

33
ED physician staffing
Current:• BC/BE Pediatric Emergency Medicine coverage 7am to
2am
• Fellow coverage- 2am to 7am
• During peak hours 12-16 hours of coverage with urgent care physician
Physician Staffing under Patient Safety Plan:• Transition to 24-hour coverage with Pediatric Emergency
Physicians
• Reevaluate staffing needs every 4-6 months

34
Other providers
Minimal resident staffing• Four/ shift• One senior pediatric resident
Augmentation of resident staffing with urgent care NP’s or PA’s• Budgeted for 3.4 FTE’s

35
Non-physician Staffing and Skills

36
Staff Skills and Coverage
Nursing• Education focused on stabilization and monitoring of
critical patients
Respiratory therapy• Coverage
Minimum of 1 RT in ED 24/7Float RT during peak times
• Education (slated to be completed by July 2007)IntubationVentilator managementLMA placement

37
HS Hospital-wide response to “Code Blue”

38
Response to “Code Blue”
Development of a team concept
ED physician and ED nurse responds to codes
Hospitalist responds in person andHelps in stabilization on arrivalProvides post-stabilization monitoringUpdates parents/ guardianTalks to accepting physicianArranges transport
Other physicians/ staff to ED to monitor and manage ED patients
39
Screening In-coming Transports to Hughes Spalding

40
Plan
Children’s Central dispatch (once created) to • direct appropriate EMS traffic to HS• Direct inappropriate EMS traffic away from HS
Unstable patients to HS only if • HS is the nearest facility or• BOTH EG and SR are on ED saturation
EMS transports and inter-facility ED transfers• HS will not accept
Unstable patients, unless as aboveIntubated patientsPatients requiring cardiac, neurosurgical, surgical, orthopedic servicesPatients who obviously do not meet admission criteriaPatients meeting major trauma criteria as defined by ACS guidelines

41
Dedicated HS transport team

42
Transport PlanKey Components
Pediatric Transport Team:• RN, RCP & EMT-P
Coverage 24/7/365
Integrated into current Children’s transport system
Unit based at HS
Medical Control: Receiving MD is online Medical Control
Staff, when available, will assist in PEC
Benefits of Plan:• Improves coverage of south and west section of metro area
• More easily accessible for HS transfers
• Will transport patients from HS to CT scanner at Grady when needed

43
ED Plan Critical Success Factors

44
ED/Transport Critical Success Factors
Physicians• Acceptance of HS patients by the physicians at EG and SR• Acceptance of direct admissions to EG and SR by
subspecialists and hospitalists• Development of the hospitalist model at HS
Patients and Families• Availability of non-emergent transportation to EG and SR
for patients and families• Social services at all three sites to meet the needs of this
populationOther• Critical care and floor bed availability at EG and SR• CR machine for copying radiographs for transfer patients• Optimal resident and practitioner staffing to support the
attending physician coverage• Team approach to “code blues”• Cat Scan transport team: composition to be determined• Children’s response gives preference to HS transfers

45
Does plan fit within 2008 budget?
Most of the patient safety plan developed was able to be fit into the financial parameter of the 2008 budget.
In order to transition to 24/7 PEM coverage in the ED, a cost of $200,000 annually will be incurred and will be incremental to the 2008 operating budget.
46
Quality Improvement ProgramThe following indicators will be monitored and closely
reviewed to ensure patient safety and quality;
• ED admissions and transfers
• Adherence to admission criteria and inpatient volumes
• Origin of admissions: ED, direct admit (source)
• Transfers
• Activation of rapid response team
• “Code blue”

47
TimelinesJune 28, 2007• Dr. McCrory resigns
July 1, 2007• Implementation of transfer algorithm• Pediatric orthopedic clinic closes at Grady• Only closed reductions and consultative orthopedic
services provided at HS (these patients will get follow up in the adult orthopedics clinic at Grady)
• PICU beds reduced to 3 beds (low census, insufficient nurses)
• PICU attendings: Drs Pettignano, Paradisis, Stockwell, Hebbar, Petrillo
• Dedicated hospitalists for the general pediatric serviceJuly 16, 2007• free commuter van service for patients and families with
appointments or services at EG or SR

48
Timelines…contdAugust 1, 2007• Children’s response unit based at HS 24/7
September 1, 2007• PICU closes• New admission and transfer guidelines implemented• All admissions will be to the 18 bed 3rd floor• An additional overflow 5 beds will be available on the
2nd floor which will be closed down• ED attending moonlighting shift added 2a-7a
October 1, 2007• 24/7 ED coverage at HS and reorganization of the EG
and HS fellow coverage

Egleston

50
EglestonStaffing – all respiratory positions have been filledTrauma Update – number of traumas were average for JuneFast track report –• We are meeting goals 25% of the time• Compare observational things to see what S.R. does
right so that we can improve and get patients in and out in 90 minutes or less.
• If you have ideas or suggestions, contact Roshni Patel
Calling out physicians – use it wisely

51
Egleston
Master Facilities Building Update• Lab moves this week• Conference center moves June 12• Blood bank moves next week• Morgue moves next week• In-patients will be relocated June 23 and
24.
We will still be responding to codes until further notice. Please check your email for updates.

52
Faculty Issues
Grady privileges MUST be maintained to keep malpracticeTDJ update - use by August 31, 2007Need a PEM and an UC physician to coordinate recruiting

53
Basic Non-Clinical Requirements
<15.1% >15.1%Scholastic Oversight Cttee 4
Req office time 12 8Req. fellows conf 8 12
Req. EPG mtgs 6 6AVU's 92 80
54
Office Day responsibilities
Effective date: July 1, 20079a-3pSelf schedulingED BU Chart reviewsCommittee workAttendance at meetingsSpecial projectsCan schedule teaching activities