emergency medical services 1 - ylo.moph.go.th · •state-based centers in malaysia –hospital...
TRANSCRIPT

1
2
3
4
Emergency Medical Services –
the service and components within
Malaysia perspective
MECC ORGANIZATION STRUCTURE
MECC SERVICE OBJECTIVE
MECC PERAK STATISTIC
LECTURE 0UTLINES
CHALLENGES AND SUMMARY5
Understand the
various components
of EMS
Understand the
function of
MECC
Introduce the role of PED
LECTURE OBJECTIVES

WE TEACH PUBLIC DURING EMERGENCY….
DO THESE…

• 994 – Fire and Rescue Department
• 991 – Civil Defence Department
• 995 – gas-related emergencies.
• 112 – if use cell phone
WHEN TRYING TO GET HELPTHEY FACE THIS…..
WHO DO I CALL
FIRST?
EMERGENCY NUMBERS
COORDINATED PRE HOSPITAL EMERGENCY
RESPONSE – MECC
• Developed as part of MERS 999 system
• October 2007 (Perak officially started Jan 2015)
• Regionalization of Pre Hospital Emergency Response
• State-based centers in Malaysia – hospital based
• Emergency Physician as Medical Director
• Communications hub for multi-agency ambulance
network
• Medical Direction help for interagency network

MECC
ONE STOP CENTER
FOR ALL
MEDICAL
EMERGENCIES

MECC: ORGANIZATIONAL STRUCTURE
MEDICAL
STANDBY
HEAD OF EMERGENCY AND
TRAUMA DEPARTMENT
STATE
DIRECTOR
HOSPITAL
DIRECTOR
CLINICAL
EMERGENCY CARE
AREA
PRE-HOSPITAL
CARE
DISASTER
MANAGEMEN
T
AMBULAN
CE
SERVICE
MECC

MECCSERVICE OBJECTIVES
• Answer all calls requesting for emergency
ambulance service
• Public
• Health facilities
• Dispatch appropriate response team in
accordance to triage category and protocol
• Responder service level – BLS, ALS
• Mode of response – ambulance, motorcycle,
bicycle, doctor’s care

MECCSERVICE OBJECTIVES
• Information monitoring hub for all major emergency
incidents
• Coordination and communication centre for all
ambulance movement
• 999 ambulance, interfacility and retrieval
• Monitor various phases of response
• Interagency activation and coordination
• Maintain communication with responding team
• Receives reports from teams at regular interval
• Facilitate Medical Direction

EMERGENCY CALL MANAGEMENT STRUCTURE
TM 999
Call Centre
Caller
Medical
Call Centre
21
MECC
PreHospital Care
District Hosp
(One Line)
AmbulanceNGOs Ambulance
Incident Site
10s
10s
10s Call Mx
1Min Call Mx
Health Clinics
Ambulance
EMERGENC
Y CALL
TAKER
AND
OPERATOR
S
EMERGENC
Y
DISPATCHER
S

930 931974
927 933
822
909938 957
902 913
975
874854
957
907
993
850
999
921 932965
906
1014
652 649
700666 658 658
711679
719
647
593
771
0
200
400
600
800
1000
1200
JUMLAH RESPON KECEMASAN AMBULAN HRPB 2016
PAGI PETANG MALAM

0
500
1000
1500
2000
2500
3000
JUMLAH RESPON KECEMASAN AMBULAN HRPB
2015- 2016
2015 2016

13671278
13581432 1393 1439
13251438
13721470 1523 1531
2111 2057
2334
2110 2161 2181
23602293
21752251
2172
24392439 2419
26192494
2579
2316
26062533
25982510
2403
27502815
2640
3057
2732
2959
2596
2833 28812735
30452924
3085
JAN FEB MAC APRIL MEI JUN JUL OGOS SEP OKT NOV DIS
2014 2015 2016 2017
TOTAL 999 CALL IN MECC PERAK 2014-2017

131
106 110121
100
160 163
123117
188 187
89
122
95
120125
116124
96
116 119 118123
110102 105
114106
101
65
80
111104
96105
118
0
20
40
60
80
100
120
140
160
180
200
JUMLAH KES RUJUKAN INTERFASILITI
AMBULAN HRPB TAHUN 2015-2017
2015 2016 เชงิเสน้ (2015)

7975
81
7168
46
5861
7470
58
75
10
2529 30
27
15 16
44
2320
40 38
15
5 4 5 6 4 6 6 7 6 7 5
JUMLAH KES RUJUKAN INTERFASILITI
AMBULAN HRPB TAHUN 2017
PAGI PETANG MALAM

0
50
100
150
200
250
300
JAN FEB MAC APRIL MEI JUN JUL OGOS SEP OKT NOV DIS
NUMBER OF DIRECT CALL TO HOSPITAL IN PERAK
2014 2015 2016

20…
20…
0
200
400
600
800
1000
1200
JAN FEB MAC APRIL MEI JUN JUL OGOS SEP OKT NOV DIS
319 321361
450 437
352300
350314
370 362413
713 700736 723 744
710
856786
716778
708
795780
834
929885
916
776
951 9481009
949
863
10581012 995
11371076
1128
947989
1088 1071
11601104
1185
2014 2015 2016 2017
AMBULANCE RESPONS FOR DISTRICT HOSPITAL IN PERAK
2014 - 2016

19.5
20
20.5
21
21.5
22
22.5
23
23.5
JAN FEB MAC APRIL MEI JUN JUL OGOS SEP OKT NOV DIS
PHC AMBULANCE RESPONSE TIME
2015 - 2016
2015
2016

MECC
ORGANIZATION,
STRUCTURE, PROCESS
AND TECHNOLOGY

MECC: STRUCTURE LAY-OUT

ORGANIZATIONAL STRUCTURE IN MECC
Emergency
physician in-
charge
MECC Supervisor
on-site PPP U32
Emergency Call
Takers
(PPP, JT)
Emergency
Dispatchers
MECC Supervisor
PPP U36
MECC Care Taker
PPP U41/42/44
STAFF QUALIFICATION

MECCTELECOMMUNICATIONS STRUCTURE
• System network infrastructure
• Data server
• Interagency network
• Communications structure
• Telephone – independent from hospital
• Cellular and fixed
• Radio devices – primary and secondary
• Data transfer capability
• Voice communication capture capability

MECCTOOLS TO FACILITATE SERVICE
• Computer Aided Dispatch
• Emergency Call Management Protocols
• Standard Time - synchronisation
• Response Monitoring Display
• Individual Response Monitoring Sheet
• Resource Monitoring Display
• Individual Resource Assignment Sheet
• Map of area
• Street map of locations
• Street map of location and facilities

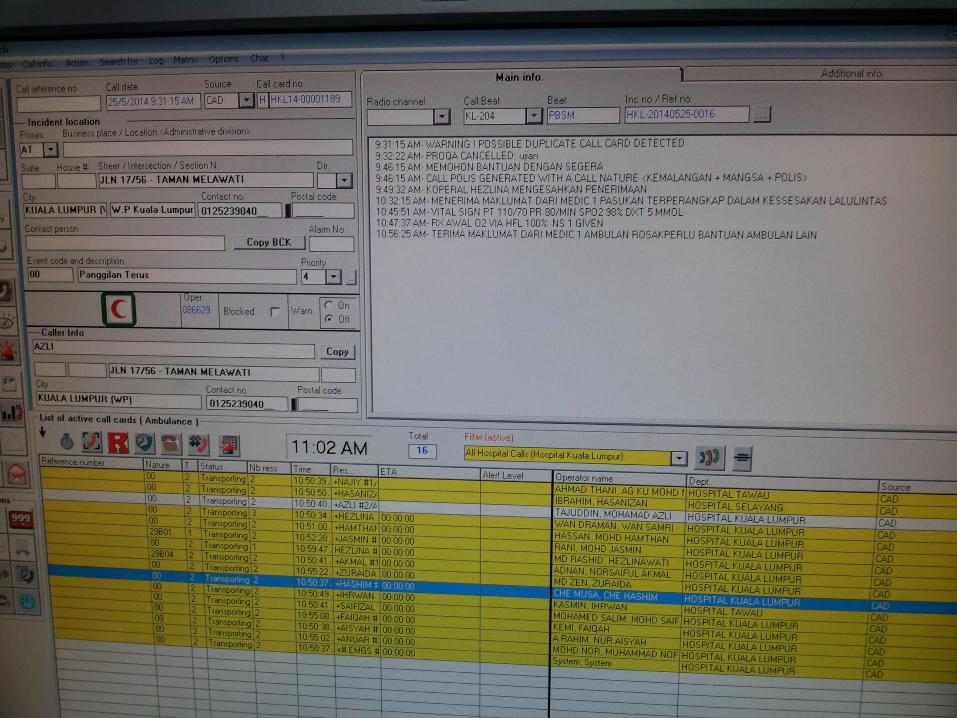
Call Card View
Area MappingDespatch Resources
View
COMPUTER AIDED DISPATCH
STANDARD - WORKSTATION


COMPUTER AIDED DISPATCH (CAD)

EMERGENCY CALL MANAGEMENT PROTOCOLS


INDIVIDUAL RESPONSE DISPLAY
Suggestion of nearest
ambulance to respond
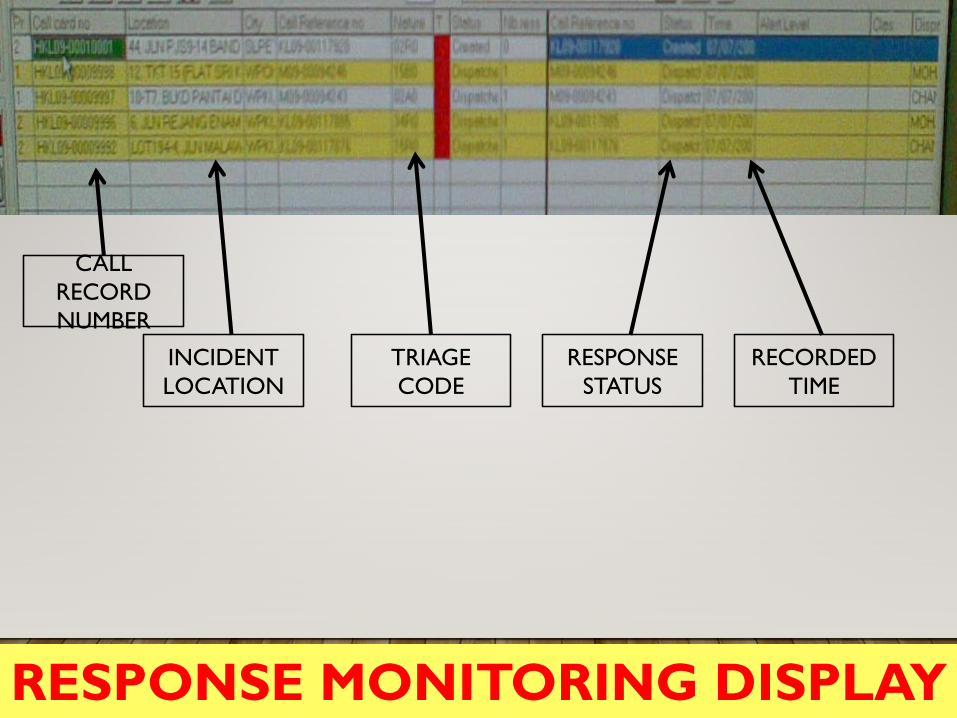
RESPONSE MONITORING DISPLAY
CALL
RECORD
NUMBER
INCIDENT
LOCATION
TRIAGE
CODE
RESPONSE
STATUS
RECORDED
TIME

FLEET MANAGEMENT

AREA MAPPING
GEOGRAPHICAL INFORMATION SYSTEM

MECCPROTOCOLS OF SERVICE
• Daily Functions And Preparations Of Dispatchers
• Emergency Call Management Protocol
• Primary Response Activation Protocol
• Interagency Activation Protocol
• Multiple Casualty Response Activation Protocol
• Emergency Response Monitoring Protocol
• Secondary Response Activation Protocol
• Medical Direction Facilitation Protocol
MECC
INFORMATION TO FACILITATE COMMUNICATION
• Knowledge and understanding of Ambulance Response
Protocols for each provider
• Primary Response Protocol
• Medical Direction Request Protocol
• Secondary Response Request Protocol
• Discharge against Medical Advice Protocol
• Knowledge and understanding the scope of service for
responders
• Level of service response – BLS, ALS, Intermediate
• Equipment and medication (if any) carried by responder
THE CHALLENGES
• ‘I DON’T WANNA CALL 999 BECAUSE IT WILL DELAY MY
TIME TO BRING MY SON TO HOSPITAL’- FATHER OF
ASPIRATED CHILD WITH CARDIORESPIRATORY ARREST
• ‘I ADVISED THE MOTHER TO BRING HER BABY BY HER
OWN BECAUSE IT WILL BE DELAYED IF WAITING FOR AN
AMBULANCE’-MO FROM KK , 6 MONTH OLD BABY WITH
MULTIPLE APNEIC EPISODE.
• BYSTANDER WITNESS ARREST CALL 999 BUT REFUSED
TO DO CHEST COMPRESSION ONLY CPR.
• MISUSE MECC

SUMMARY
• Regionalization of Pre Hospital Emergency Response
• State-based centers in Malaysia – hospital based
• Emergency Physician as Medical Director
• Communications hub for multi-agency ambulance network
• Medical Direction help for interagency network
• Structure, process and technology to save lives
• Need to increase awareness to Health provider and civillian on
999 and MECC.

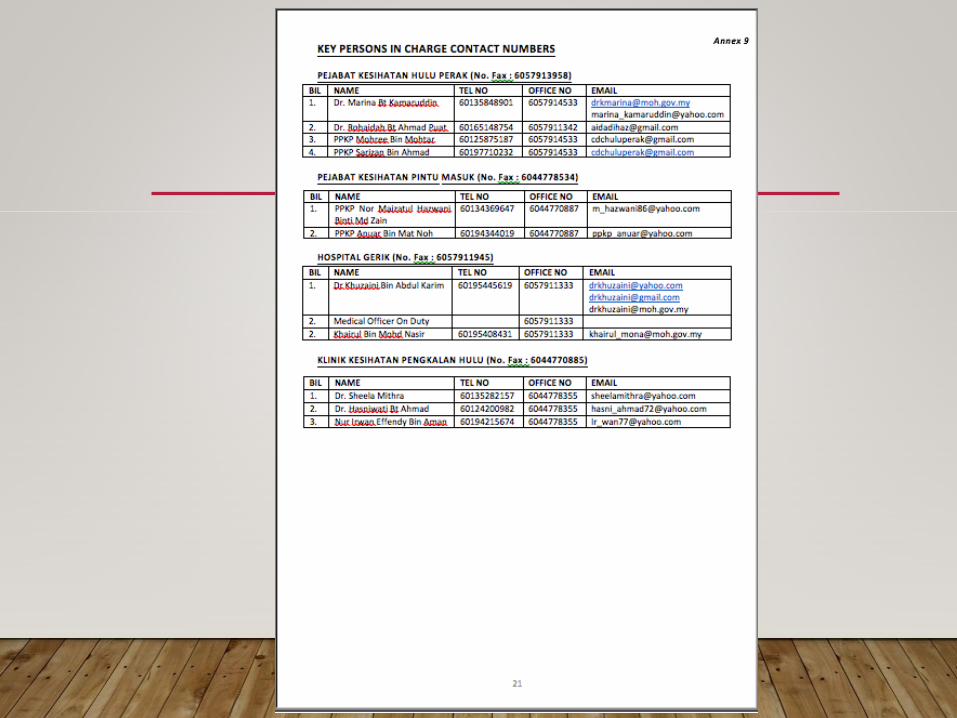
CRITERIA FOR PT TRANSFER
• Inpatient foreigner case who requests to be hospitalized in
their country of origin. Cases which have been discharged are
not to be transferred via ambulance. Patients / relatives will
have to arrange their own transport.
• The in-charge doctor of the respective discipline / department
has agreed to proceed with the transfer request.
• All unstable cases are kept in the current hospital and to be
stabilized before transfer.
• Transfer can only be made upon approval by the receiving
hospital.

ARRANGEMENT FOR PATIENT TRANSFER
• The arrangement shall be made at least 24 hours earlier.
• Adequate info and explanation shall be made to patient &
family members of the potential risks.
• Call centre must be informed of the details of transfer
• Referring institutions shall send all documents via email/fax
to the receiving institution. Receiving states/province health
office shall be informed via phone once agreement on
patient transfer is achieved.

• Receiving district health office shall facilitate and coordinate
the patient trasnfer process with relevent agencies at the
border check point. The agencies include;
• Malaysia-Thailand Border Coordination Office)
• Immigration
• Custom
• DOT (dept of transport)
• AKSEM (Malaysian Border security Agency)
• Police
• Civil defence

TRANSFER PROCESS
• Once transfer request has been approved by receiving institution, all necessary
documents and equipment shall be prepared. The referring institution shall reconfirm
the estimated time of departure, estimated time of arrival at the transfer zone. Any
delay or incidents that occurs during transportation of patient shall be updated to
the receiving side.
• The transfer of patient between ambulances shall take place in the free zone
between immigration checkpoints of Malaysia and Thailand. The designated transfer
area shall be agreed by both bordering state and province. In any event of rain during
transfer process, alternative area (e.g. covered parking bay) shall be identified.
• Pre-transfer notification to other relevant agencies a few hours prior to transfer is to
ensure a coordinated response between agencies and the transfer zone is evacuated
at least 10 meter radius from public passage.

TRANSFER PROCESS
• In the event of infectious disease case transfer, the areas that need to be
evacuated for the transfer process between ambulances is at least 15
meter radius. The area will only be reopened to the public after
disinfection process has been carried out at the transfer area. This
notification will also ensure the use of the Green Lane at the Immigration
and Custom check point and to ensure smooth process of immigration
procedure for the patient and accompanying relative(s).
• During passing over of the case, all documents shall be signed by the
representatives of both referring and receiving teams (Annex 7 and Annex
8). All documents shall be completed in two copies and each referring and
receiving team shall keep a copy for the reference. Any updates / progress
of the patient during the journey shall also be passed over to the receiving
team.

ISSUES
• All notifiable disease cases either discharged against medical advice or
transferred must be informed to the foreign District Health Office.
• In case of death during transfer process, the present transporting
ambulance shall bring patient to nearest health clinic / hospital in the
present state/province for death declaration and documentation.
Death certificate and Burial Permit Certificate shall be produced by
the state/province that death occurred. Foreign Institution Call Centre
should be informed on the event of death. Cross border dead body
transportation should be dealt together according to both countries’
laws.

ISSUES
• Transfer of detainee case shall be dealt with according to
the rules and regulations in the present country.
• In the case of an accident involving the ambulance, the
nearest local emergency medical service of the present
transporting ambulance shall respond.
• In the case of patient being unable to pay their hospital bills,
the embassy of their country of origin shall be referred to.




THANK YOU