emergency department senior house officers' consultation difficulties: implications for...
TRANSCRIPT
E D U C A T I O N / O R I G I N A L C O N T R I B U T I O N
3 5 8 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 3 M A R C H 1 9 9 8
Emergency Department Senior House Officers’
Consultation Difficulties: Implications for Training
Susan Williams, MSc*
Jeremy Dale, MA, MRCGP*‡
Edward Glucksman, FRCP, FFAEM§
Study objective: We investigated the types of patient presen-tations that cause senior house officers (SHOs) most difficultyduring their tenure in emergency departments and report theextent to which such difficulties are related to SHOs’ communi-cation problems, stress, or perceived lack of skills or knowledge.
Methods: We conducted a questionnaire survey of 171 newlyappointed SHOs employed in 27 EDs in the South Thames regionof England. Subjects were asked to describe the presentationthat gave them greatest difficulty during three subsequent shiftsat the end of the first and fourth months of their ED appointment.
Results: A total of 132 (77%) and 110 (64%) respondents re-turned questionnaires at the end of the first and fourth months,respectively; 61% (105) responded to both questionnaires. Therespondents described 537 of a possible total of 726 cases (74%).Communication problems caused difficulty in 406 (76%) cases,SHOs’ experience of stress in 352 (66%) cases, and a perceivedlack of knowledge or skills in 281 (52%) cases. Communicationproblems and the experience of stress occurred in 141 (26%) cases.Patients presenting with mental or behavioral disorders and symp-toms most frequently gave rise to communication problems, per-ceived lack of skills, and the experience of stress. The difficultiesdescribed at the two time periods were very similar indicating thatexperience alone had little effect on these problems.
Conclusion: ED SHOs may benefit from communication skillstraining, the opportunity to review difficult case presentations,and the alleviation of organizational stress factors.
[Williams S, Dale J, Glucksman E: Emergency department seniorhouse officers’ consultation difficulties: Implications for training.Ann Emerg Med March 1998;31:358-363.]
From the Department of GeneralPractice and Primary Care, King’sCollege School of Medicine andDentistry, Weston Education Centre,London,* the School of PostgraduateMedical Education, University ofWarwick, Coventry,‡ and the Depart-ment of Accident and EmergencyMedicine, King’s College Hospital,London,§ England.
Received for publication March 24, 1997. Revision receivedAugust 12, 1997. Accepted for publication August 15, 1997.
Supported by the Primary CareDevelopment Fund, South ThamesRegion, NHSE, London.
Copyright © 1998 by the AmericanCollege of Emergency Physicians.

I N T R O D U C T I O N
In the United Kingdom, senior house officers (SHOs) arethe largest group of physicians employed within emergencydepartments. The appointment as an SHO is the first postafter working as a house officer (intern); SHOs are gener-ally employed in EDs on 6-month attachments. AlthoughSHOs in the United Kingdom are authorized to assess anddischarge patients independently, the ED is a particularlydemanding area of hospital practice in the United Kingdomand SHOs frequently work long shifts with varying levelsof direct supervision. It has been reported that their trainingneeds to be improved.1,2 Criticisms have included an absenceof a clearly defined structure for teaching, induction pro-grams, and insufficient time allocated to learning.
Guidelines on a core curriculum for physicians who wishto specialize in emergency medicine have been produced inthe United Kingdom,3 but there is no core curriculum toguide SHO teaching. Whereas a core curriculum for trainingin emergency medicine exists in the United States,4 guide-lines on how topics should be taught are lacking. Despitethe wealth of literature on the importance of communicationskills, little attention has been given to this topic in the con-text of ED training in either country.5 Effective physician-patient communication is important not only for improvedpatient satisfaction and compliance,6-8 but also may be bene-ficial for the well-being of the physician.9
Few studies have attempted to gain SHOs’ assessmentsof their training needs and the skills or knowledge that theythemselves perceive to be lacking during their tenure in theED. A detailed regional survey was set up to investigate EDSHOs’ training needs as part of a larger study of SHOs’ expe-rience of working in EDs.10 The first aim was to describepatient presentations that cause SHOs greatest difficulty dur-ing their ED assignments. The second aim was to determinethe extent to which difficulties were the result of communi-cation problems, lack of skills or knowledge, or the expe-
rience of stress during consulting. The results are discussedin relation to the need for further training and support.
M A T E R I A L S A N D M E T H O D S
Surveys were sent to 171 newly appointed SHOs employedon 6-month assignments in 27 EDs between August 1994and February 1995 in the South Thames region; question-naires were sent at the end of the first and fourth monthsof their assignment.
Questionnaires sent at the end of the first and fourthmonths asked, “At the end of your next three shifts, pleasecomplete a case report on the patient who gave you mostdifficulty.” The SHOs were asked to report the age, gender,and medical symptoms or injury presented. The SHOs werethen asked, “When considering the main difficulties in thisconsultation, were these due to: … communication difficul-ties, … lack of skills, … lack of knowledge, … stress and/orworry cause by the consultation, … other factors.” For each“yes” response, SHOs were asked to describe exactly whatcaused the given difficulty. In a separate section of the ques-tionnaire sent at the end of the fourth month, they were askedto describe the types of patients that they were “having thegreatest difficulty in dealing with” in the ED.
All quantitative data were entered into a mainframe com-puter and statistical analysis was done with the StatisticalPackage for the Social Sciences (SSPS Inc, Chicago, IL). The“grounded” approach11 was used in the analysis of the quali-tative data from the case study descriptions. The diseases/symptoms described in the difficult case presentations bythe SHOs were classified according to International Classifi-cation of Diseases-10 nomenclature.12
R E S U L T S
The response rates were 77% (132) and 66% (110) to ques-tionnaires sent at the end of the first and fourth months,
E D S E N I O R H O U S E O F F I C E R S ’ C O N S U L T A T I O N D I F F I C U L T I E SWilliams, Dale & Glucksman
M A R C H 1 9 9 8 3 1 : 3 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 5 9
Table 1.Results of χ2 tests on the percentages of cases related to communication difficulties, a perceived lack of knowledge or skills, or stress at theend of months 1 and 4.
Difficulties Month 1 (% cases) Month 4 (% cases) χ2 df P value
Communication 17 18 .057 1 NSStress 4 4 .13 1 NSSkills/knowledge 10 8 .28 1 NSCommunication + stress 9 7 .31 1 NSSkills/knowledge + stress 11 11 .045 1 NSStress + communication 23 30 .94 1 NSCommunication + stress + skills/knowledge 26 22 .35 1 NS
respectively; 61% (105) SHOs completed both. Demographicdetails were obtained for 82% (140) of the sample (76 men,64 women). The mean age of the sample was 26.5 years(range 23.7 to 36.3 years; interquartile range 24.9 years,27.1 years).
Responding SHOs completed a total of 319 (81%) of apossible 396 difficult case descriptions at the end of the firstmonth. A total of 267 (81%) of a possible 330 difficult casedescriptions were completed at the end of the fourth month.
The results of χ2 tests of the percentage of cases thatpresented difficulties related to communication problems,lack of skills or knowledge, or stress are presented in Table 1.These were not significant; therefore the data from the twosampling periods were grouped together (Figure).
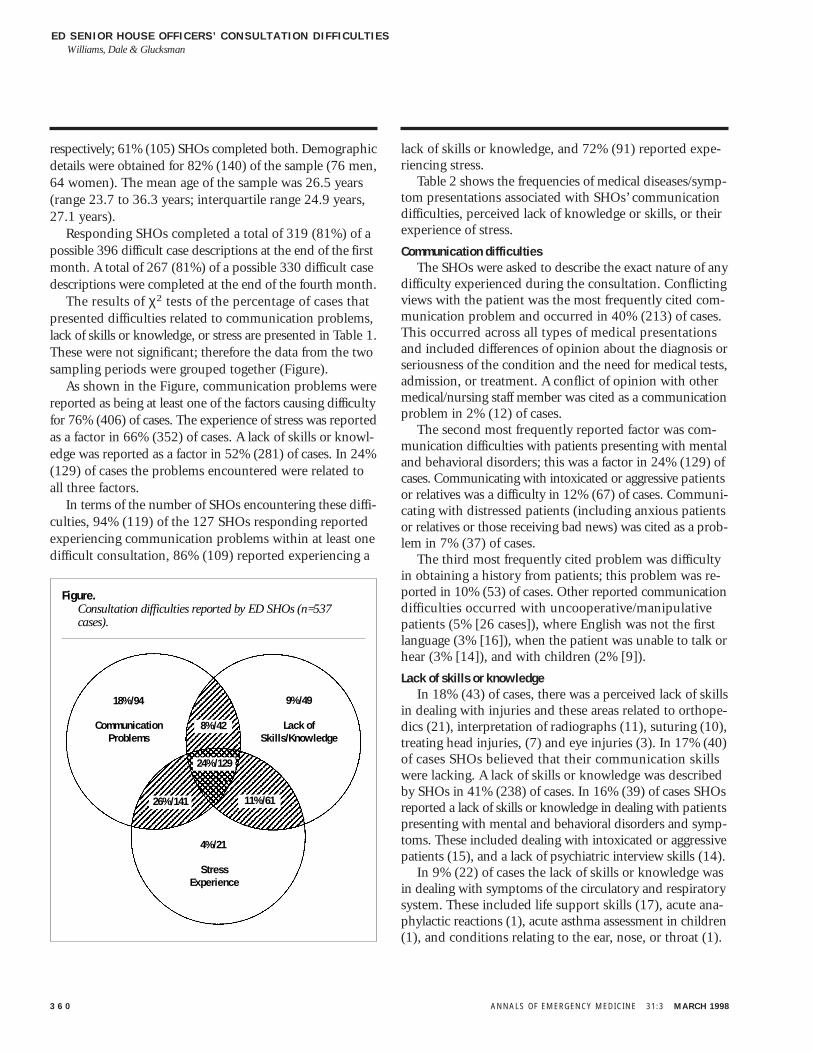
As shown in the Figure, communication problems werereported as being at least one of the factors causing difficultyfor 76% (406) of cases. The experience of stress was reportedas a factor in 66% (352) of cases. A lack of skills or knowl-edge was reported as a factor in 52% (281) of cases. In 24%(129) of cases the problems encountered were related toall three factors.
In terms of the number of SHOs encountering these diffi-culties, 94% (119) of the 127 SHOs responding reportedexperiencing communication problems within at least onedifficult consultation, 86% (109) reported experiencing a
lack of skills or knowledge, and 72% (91) reported expe-riencing stress.
Table 2 shows the frequencies of medical diseases/symp-tom presentations associated with SHOs’ communicationdifficulties, perceived lack of knowledge or skills, or theirexperience of stress.
Communication difficulties The SHOs were asked to describe the exact nature of any
difficulty experienced during the consultation. Conflictingviews with the patient was the most frequently cited com-munication problem and occurred in 40% (213) of cases.This occurred across all types of medical presentationsand included differences of opinion about the diagnosis orseriousness of the condition and the need for medical tests,admission, or treatment. A conflict of opinion with othermedical/nursing staff member was cited as a communicationproblem in 2% (12) of cases.
The second most frequently reported factor was com-munication difficulties with patients presenting with mentaland behavioral disorders; this was a factor in 24% (129) ofcases. Communicating with intoxicated or aggressive patientsor relatives was a difficulty in 12% (67) of cases. Communi-cating with distressed patients (including anxious patientsor relatives or those receiving bad news) was cited as a prob-lem in 7% (37) of cases.
The third most frequently cited problem was difficultyin obtaining a history from patients; this problem was re-ported in 10% (53) of cases. Other reported communicationdifficulties occurred with uncooperative/manipulativepatients (5% [26 cases]), where English was not the firstlanguage (3% [16]), when the patient was unable to talk orhear (3% [14]), and with children (2% [9]).
Lack of skills or knowledge In 18% (43) of cases, there was a perceived lack of skills
in dealing with injuries and these areas related to orthope-dics (21), interpretation of radiographs (11), suturing (10),treating head injuries, (7) and eye injuries (3). In 17% (40)of cases SHOs believed that their communication skillswere lacking. A lack of skills or knowledge was describedby SHOs in 41% (238) of cases. In 16% (39) of cases SHOsreported a lack of skills or knowledge in dealing with patientspresenting with mental and behavioral disorders and symp-toms. These included dealing with intoxicated or aggressivepatients (15), and a lack of psychiatric interview skills (14).
In 9% (22) of cases the lack of skills or knowledge wasin dealing with symptoms of the circulatory and respiratorysystem. These included life support skills (17), acute ana-phylactic reactions (1), acute asthma assessment in children(1), and conditions relating to the ear, nose, or throat (1).
E D S E N I O R H O U S E O F F I C E R S ’ C O N S U L T A T I O N D I F F I C U L T I E SWilliams, Dale & Glucksman
3 6 0 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 3 M A R C H 1 9 9 8
Figure.Consultation difficulties reported by ED SHOs (n=537cases).
CommunicationProblems
Lack ofSkills/Knowledge
StressExperience
18%/94
4%/21
9%/49
8%/42
26%/141 11%/61
24%/129

Other areas where skills or knowledge were perceived to belacking were in dealing with external causes of morbidityand mortality (7), diseases of the musculoskeletal systemand connective tissue (7), and obstetrics and gynecology(7). Other areas with a reported lack of skills were in rela-tion to diseases of the nervous system (4), diseases of theskin and subcutaneous tissue (3), examination of the ear(2), dental and oral medicine (1), urinary tract infections(1), ophthalmology (1), and diabetes (1).
In 21% (51) of cases the lack of skills or knowledge wasrelated to symptoms, signs, and abnormal clinical and labora-tory findings not classifiable by International Classificationof Diseases-10.12 These included pediatrics (27) (diagnosis,examination for fever, headache, diarrhea, and vomiting).Pediatric patients were also listed as the types of patientswho caused most difficulty overall. Other lacking in skillsor knowledge included diagnosis of chest pain (8), diagnosisof abdominal pain (7), and assessment of headaches (5).
When asked to list the types of patients they were “havingthe greatest difficulty in dealing with in the ED,” 50% (54)of 107 SHOs responding, stated that intoxicated and/oraggressive patients caused them greatest difficulty. Otherareas where SHOs reported a lack of skills were dealing withdrug abusers (6), demented patients (2), special-needspatients (1), and overdose victims (1).
Stress factors A broad range of personal and organizational factors were
reported as causing stress during difficult consultations. The
most frequently cited organizational factors were concernsor uncertainty about the discharge or referral of patients,which occurred in 13% (74) of difficult cases. Departmentalissues were factors causing stress in 6% (33) of cases, anddifficulties with medical or nursing colleagues were stressfulin 4% (20) of cases. Concern over medicolegal issues wasdescribed as a cause of stress in 3% (15) of cases. A moredetailed account of these stress factors has been reportedelsewhere.10
D I S C U S S I O N
The most striking finding from this survey is that communi-cation problems were the most frequently reported factorcausing difficulty during SHOs’ consultations. The com-munication problems were in relation to a broad range ofclinical presentations, and a lack of communication skillswas frequently cited as a cause of stress. A large proportionof the cases causing difficulty appeared to relate to problemsof a primary care type, which is in keeping with other find-ings.10 The most frequently cited communication problemswere having a conflict of view with the patient about thediagnosis or seriousness of the condition, need for medicaltests, need for treatment, or need for admission. Other com-mon communication problems occurred with patients pre-senting with mental or behavioral disorders or symptomsand intoxicated or aggressive patients.
E D S E N I O R H O U S E O F F I C E R S ’ C O N S U L T A T I O N D I F F I C U L T I E SWilliams, Dale & Glucksman
M A R C H 1 9 9 8 3 1 : 3 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 6 1
Table 2.Percentages of cases by medical diseases/symptom presentations leading to communication difficulties, lack of knowledge/skills, and stress.
Medical diseases/symptoms Communication No. (%) Knowledge/Skills No. (%) Stress No. (%)
Mental and behavioral disorders/symptoms 209 (36) 113 (19) 146 (25)Injury, poisoning, and certain other consequences of external causes 118 (20) 105 (18) 75 (13)Diseases/symptoms of circulatory and respiratory system 117 (20) 86 (15) 90 (15)Diseases/symptoms of digestive system 107 (18) 69 (12) 57 (10)Symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere 104 (18) 86 (15) 88 (15)
classifiedExternal causes of morbidity and mortality 75 (13) 51 (9) 53 (9)Diseases/symptoms of musculoskeletal system and connective tissue 72 (12) 37 (6) 57 (10)Diseases of genitourinary system 31 (5) 31 (5) 23 (4)Diseases/symptoms of skin and subcutaneous tissue 15 (3) 9 (2) 12 (2)Diseases of nervous system 15 (3) 11 (2) 13 (2)Pregnancy, childbirth, and puerperium 15 (3) 10 (2) 8 (1)Diseases of blood and blood-forming organs and certain disorders involving 8 (1) 7 (1) 5 (1)
immune mechanisms/symptomsDiseases of ear and mastoid process 5 (1) 5 (1) 2 (.3)Certain infectious and parasitic diseases 5 (1) 5 (1) 5 (1)Endocrine, nutritional, and metabolic disease 5 (1) 2 (.3) 2 (.3)Diseases of the eye 1 (.2) 3 (.3) 3 (.3)Neoplasms 1 (.2) 0 0

Communication difficulties described at the end of thefirst month of employment in the ED tended to be the sameas those difficulties at the end of the fourth month indicat-ing that experience alone had little impact on these problems.This suggests that ED SHOs may benefit from communica-tion skills training. Further studies are needed to determinewhether this also applies to American training. In a surveyof 76 directors of emergency medicine residency trainingprograms in America, Rozenzweig5 reported that 98% agreed(35% strongly agreed) that communication skills should bestudied and taught. Although the “Core Content for Emer-gency Medicine”4 includes the topic of interpersonal skills,there remain no published guidelines for teaching these skillswithin an ED residency in the United States.
Communication skills training should cover dealing withthe difficult patient.1 In a recent study of ED junior physi-cians in the United Kingdom, 96 of 100 respondents hadexperienced verbal aggression, 50 had received threats, and32 reported that patients had attempted to assault them.13
It was determined that only 11 physicians had received anytraining on how to manage aggressive patients, although 88suggested that such training would be useful. This is con-sistent with a recent survey of 461 American emergencymedicine residents, where 62% of respondents reported thatthey worried about their own safety while working in EDs.14
There is clearly a need for training and support for ED SHOsin dealing with violent or abusive patients.
“Communication lies at the heart of health care delivery,”15
and surveys over the last 30 years have rated poor commu-nication as the major reason for dissatisfaction with healthcare.16-19 There is good evidence that more positive out-comes are obtained when communication is effective.20-22
Communication skills not only need to be taught at theundergraduate level, but need to be taught within an EDcontext if they are to be effectively maintained in posttrain-ing medical practice.23
Organizational factors reported to be stressful includeddifficulties with discharging or referring the patient and feel-ing concerned about future problems for the patient. Otherfactors causing stress were difficulty in treating patients be-cause of lack of on-site treatment and experiencing prob-lems with medical or nursing teams. There is a need to assessand address where possible factors that cause ED SHOs stressas part of the process of managing the quality of care pro-vided by the department.
A broad range of symptoms, signs, and abnormal clinicaland laboratory findings in relation to acute trauma werereported as areas in which SHOs believed they lacked skillsor knowledge. Concern about missed or incorrect diagnoseswas frequently cited as a stress factor. However, the types
of patients who caused the greatest difficulty overall includedelderly patients, pediatric patients, psychiatric patients,patients presenting with minor difficulties, assault victims,and patients with psychosocial problems. Patients with“primary care” problems frequently are seen in EDs, and inthe United Kingdom there have been developments towardmeeting these patients’ needs within this setting.24
The aim of this study was to report on a sample of con-sultations causing greatest difficulty for SHOs from theirown perspective, in terms of communication problems, alack of skills or knowledge, and stress and to discuss theimplications for training. Despite the fact that response rateswere good, the nonrespondents may have resulted in a biasof the findings. Future studies are needed to assess the fre-quency of communication problems, a lack of skills/knowl-edge, or the experience of stress in everyday practice. Thereis also a need to investigate the applicability of these studyfindings to other health services, to investigate the effective-ness of consultations from the perspective of more seniorphysicians and the patients themselves. This may identifyother SHO consultation difficulties not described in thisstudy.
This study has demonstrated the importance of commu-nication problems and specific types of patient presenta-tions as factors causing difficulty during ED consultations.The findings indicate that ED SHOs may benefit from con-sultation skills training in which they are taught communi-cation skills. It has been proposed that an ideal environmentfor learning is one in which “learners play a leading rolein their own education and where learning opportunitiesprovided meet previously identified, individual needs.”25
The methods used in this study suggest a straightforwardmeans of identifying and auditing individual physician train-ing needs in an ED setting, and this could be used to enhanceteaching programs. These methods have been used withina consultation skills training program for ED SHOs that hasbeen successfully operating at King’s College Hospital since1992. This program has been enthusiastically received bySHOs, but its impact on their clinical practice needs furtherevaluation.
R E F E R E N C E S1. Rodenberg H: Education in accident and emergency medicine for senior house officers: Reviewand recommendations. J Accid Emerg Med 1996;13:238-242.
2. Standing Committee on Postgraduate Medical Education: Improving the Experience: GoodPractice in Senior House Officer Training: First Report on Local Initiatives Standing Committee onPostgraduate Medical Education. London: SCOPME, 1991.
3. Board of the Faculty of A&E Medicine: Guidelines for Specialist Training in Accident andEmergency Medicine. Kent: Thanet Press, 1996.
4. American College of Emergency Physicians: Core content for emergency medicine. Ann EmergMed 1991;20:920-934.
E D S E N I O R H O U S E O F F I C E R S ’ C O N S U L T A T I O N D I F F I C U L T I E SWilliams, Dale & Glucksman
3 6 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 3 M A R C H 1 9 9 8

E D S E N I O R H O U S E O F F I C E R S ’ C O N S U L T A T I O N D I F F I C U L T I E SWilliams, Dale & Glucksman
M A R C H 1 9 9 8 3 1 : 3 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 6 3
5. Rosenzweig S: Teaching the art of emergency medicine. Ann Emerg Med 1991;20:71-76.
6. Ley P: Communicating with Patients: Improving Communication Satisfaction and Compliance.London: Chapman and Hall, 1988.
7. Hunt MT, Glucksman E: A review of 7 years of complaints in the inner-city accident and emer-gency department. Arch Emerg Med 1991;8:17-23.
8. Kadzombe EA, Coals J: Complaints against doctors in an accident and emergency department:A 10 year analysis. Arch Emerg Med 1992;9:134-142.
9. Firth-Cozens J: Emotional distress in junior house officers. Br Med J 1987;295:533-535.
10. Williams S, Dale J, Glucksman E, et al: Senior house officers' work-related stressors, psycho-logical distress and confidence in performing clinical tasks in accident and emergency. Br Med J1997;314:713-718.
11. Glaser BG, Strauss AL: The Discovery of Grounded Theory: Strategies for Qualitative Research.Chicago: Aldine, 1967.
12. World Health Organization: International Statistical Classification of Diseases and RelatedHealth Problems, Tenth Revision, vol 1. Geneva: WHO, 1992.
13. Wyatt JP, Wyatt M: Violence towards junior doctors in accident and emergency departments.J Accid Emerg Med 1995;12:40-42.
14. Anglin D, Kyriacou DN, Huston HR: Residents' perspectives on violence and personal safetyin the emergency department. Ann Emerg Med 1994;23:1082-1084.
15. Audit Commission: What Seems to Be the Matter: Communication Between Hospitals andPatients. London: Her Majesty’s Stationary Office, 1993.
16. Ley P: Communicating with the Patient. Liverpool: Staples Press, 1967.
17. Kincey J, Bradshaw P, Ley P: Patients' satisfaction and reported acceptance of advice in gen-eral practice. J R Coll Gen Pract 1975;25:558-566.
18. Hall JA, Roter DL, Katz NR: Meta-analysis of correlates of provider behaviour in medicalencounters. Med Care 1988;26:657-675.
19. Williams S, Weinman J, Dale J, et al: Patient expectations: What do primary care patientswant from the GP and how far does meeting expectations affect patient satisfaction? Fam Pract1995;12:193-201.
20. Stewart M: What is a successful doctor-patient interview? A study of interactions and out-comes. Soc Sci Med 1984;19:167-175.
21. Squier R: A model of empathic understanding and adherence to treatment regimens in practi-tioner-patient relations. Soc Sci Med 1990;30:325-339.
22. Levinson W, Roter D, Mullooly JP, et al: Physician-patient communication: The relationshipwith malpractice claims among primary care physicians and surgeons. JAMA 1997;277:553-559.
23. Sanson-Fisher R, Cockburn J: Effective teaching of communication skills for medical practice:Selecting an appropriate clinical context. Med Educ 1997;31:52-57.
24. Dale J, Lang H, Roberts J, et al: Cost effectiveness of treating primary care patients in acci-dent and emergency: A comparison between general practitioners, senior house officers and reg-istrars. Br Med J 1996;312:1340-1344.
25. Dale J, Davies M, Vasant K, et al: Primary care consultation skills training in an accident andemergency department: Implementing a new training programme. Medical Education 1997;31:243-249.
We thank all the accident and emergency medical, clerical, and secretarial staff whohelped us during the study; Dr Derek Cooper for his statistical advice; and MarilynPeters, Floss Chittenden, Emma Smith, Kate Cowley, and Patsy Dixon for transcribingand coding the data.
Reprint no. 47/1/87769Address for reprints:
Susan Williams, MSc
Kings College
Weston Education Centre
Cutcombe Road
Bessemer Road
London SE5 9PJ
England