emergence of infectious diseases after flood-related ... · pdf filetyphoid fever •...
TRANSCRIPT

Gastrointestinal Infections
Eric J. Stern, MD
Pediatric infectious diseases
2011

WHO <5y mortality
• Diarrhea – 19%
• PNA/URI – 19% (in a/w malnutrition)
• Measles – 7%
• Malaria – 5%
• Malnutrition (direct cause) – 21%
• One or more of these 5 – 71%
Oxford Handbook of Trop Med
Climate Change and
Infectious Diseases• Temps expected to increase 1.8°C - 5.8°C
by end of century
• Will alter hydrologic cycle -->more rainfall, more drought, more severe weather (hurricanes, floods, tsunamis)– Waterborne diseases, diarrheal diseases,
runoff, contamination of water by livestock
– WHO: 10% increase in diarrheal disease by 2030
• Insect vectors more active at higher temperatures

Climate Change and
Infectious Diseases (2)
• Kyoto protocol (2005) - not signed by
US, set to expire in 2012
• Copenhagen (2009) - no binding
resolution
• Developing countries
disproportionately affected

Post-disaster Infections:
Day 3-7• Wound infections
• Diarrheal disease (crowding, DPs)
• Pneumonia
• Vaccine-preventable diseases (crowding, displaced persons camps, disruption of healthcare system)– measles
– Diphtheria
– Tetanus
– Hep A

Post-disaster Infections:
>4 weeks• Gastrointestinal infections
• Wound infections (ie, Vibrio spp.)
• Sepsis
• Mosquito-borne illness - malaria, dengue
• TB (crowding, disrupted med supply, disrupted public health)
• HIV (blood transfusions, disrupted med compliance)

Long-Term Infectious
Disease Concerns
• Local public health concerns remain long after natural disaster…
• Disruption of public health system, chronic care facilities
• Increasing incidence of vaccine-preventable diseases
• Ecological impact on wildlife
• Climate change

Water
• Diarrheal disease
• Contaminated baby
formula
• Where does
purification take
place? Point of origin
vs consumption?
• Bottles
• Tankers
• Filters
• Aluminum, chlorine
• “Bladders,” “onion
tanks”

Port-au-Prince, 2010
Plans for Controlling
Infectious Diseases after
Natural Disasters1. Ensure access to safe drinking water
and sanitation
2. Provide access to primary care facilities
3. Implement surveillance system for potential outbreaks
4. Promote measles vaccination and vitamin A supplementation
5. Prevent epidemics of malaria and dengue


Traveler’s diarrhea
• Affects 20-60% of traveler’s to low-income countries
• So. Asia > Sub-Saharan Africa > Cent. and So. America
• Pathogens: Enterotoxigenic E. coli, Salmonella spp., Shigella, Campylobacter, viral gastro– Emergence of Enterotoxigenic Bacteroides
• Rx: azithromycin due to FQ-R Campylobacter (SE Asia) + metronidazole

Diarrheal Diseases:
Pathogens– Viral gastroenteritis
(Norovirus, Rotavirus, enteric Adeno ST 41, 43)
– V. cholera
– Enterotoxigenic E. coli
– Salmonella
– Shigella
– Campylobacter
– Yersinia
– C. difficile
– Cryptosporidiium, Isospora, Cyclospora
– Giardia
– Parasitic: ascariasis, strongyloides, hookworm, whipworm
– Other: food poisoning (Staph, Bacillus cereus)

Case 1
• 25 year old female migrant worker returned for 2.5 weeks to S.D. after family visit to Nicaragua
• 3 days of fever to 105F (>41C), constipation, vomiting, H/A, abdominal pain, myalgias
• Took no malaria prophylaxis, was bitten by mosquitoes
• Reportedly ate no unpasteurized dairy products
• No known ill contacts
• Helped with family shopping, foods bought in local street markets…


Case 1 (cont.)
• PE ill-appearing
• T103.4 P68 R24 BP112/78 cor, lungs nl abd - RUQ tenderness with mild rebound ext - no rash
• WBC 4.8 36S 34B Hct 36 Plts 170K
• Malaria smear negative x1

Case 1 (cont.)
• Blood culture: positive for S. typhi
• Bone marrow aspirate culture also
positive S. typhi
• Treatment: IV ceftriaxone, fever continued
for 4 days on appropriate therapy
• Stool culture: negative x1, positive x2,
became negative 2 weeks later

Typhoid fever (“Enteric fever”)
• Salmonella typhi
– Enterobacteriaceae
family
• Gram-negative rod
with flagellae
• Paratyphoid
– S. paratyphi A
emerging…no vaccine
– usually milder, but two
not clinically
distinguishable
Typhoid fever
• Fecal-oral transmission in areas with poor hygiene, unsafe water
• Average incubation: 10-20 days (range 3-60)
• Epidemic and endemic foci: India, Southeast Asia ,Philippines, eastern Europe
• Intermediate risk: Mexico, C. America
Typhoid Fever
• Clinical manifestations: fever, headache, malaise, splenomegaly, rash (transient), constipation followed by diarrhea
• Severe outcome due to ileal perforation
– 10% mortality if untreated
• Serologic tests (Widal antibodies, febrile agglutinins) usually not helpful
• Treatment: ceftriaxone/cefixime, azithromycin, ciprofloxacin
– Nalidixic acid/FQ-R in SE Asia
• Vaccine only ~60-75% effective, no coverage for S. paratyphi
• Uncomplicated Salmonella AGE – consider Abx for <1y

Typhoid vaccines
CDCLong. Principles and Practices of Ped Inf Dis
Campylobacter
• Motile, comma-shaped GNR
• Grows @ 42ºC
• Foodborne or waterborne
– Unpasteurized dairy, poultry
• Fever, abd pain, colitis bloody diarrhea
• “pseudoappendicitis” syndrome –
mesenteric lymphadenitis
• C. jejuni Guillaun-Barre Syndrome

Shigella
• Highly infectious (low inoculum – as few as 10 organisms)
• Shigella sonnei most common
• Clinical: watery -> bloody...Seizures
• 2009 – Kansas City outbreak >250 cases
• Treatment recommended for confirmed cases to decrease transmission and decrease duration of illness
• Rx: ceftriaxone, cipro, azithro
• TMP-SMX resistance 47% in 1999-2003 89% in 2006
MMWR 2006;55: 1068-71

Yersinia
• Short GNR
• Y. enterocolitica, Y. pseudotuberculosis
• Y. pestis (plague)– septicemic vs pneumonic vs bubonic
– transmitted by rat fleas, domestic + feral cats
• US SW
• Tropism for intraabdominal lymphoid tissue --> pseudoappendicitis
• Disseminated infection
• increased risk in iron-overload states
• Reactive arthritis late
Case 2
• 16 yo healthy female from Imperial County, CA traveled to Panama for three weeks on a church mission trip
• Took malaria meds, had 2 Hep A doses, typhoid Vi CPS vaccine, and routine immunizations up-to-date
• Stayed with local family; numerous mosquito bites
• Upon return, febrile illness with headaches, muscle/joint/bone pain, mild transient rash

Case 2 (cont)
• WBC 3.2 with mild neutropenia; plt’s 115k
• Malaria screen negative
• Dengue serologies IgM positive
• Continued fatigue, malaise, gradually worsening GI symptoms, 4 kg weight loss (weeks)
• Bloating, decreased appetite, constipation alternating with diarrhea
• Unable to bring stool sample to laboratory
• Thoughts? Next steps?


Case 2 – Giardia lamblia
• Empiric
metronidazole x
10d significant
improvement
over first week of
Rx
Case 2 (cont)
• Dx’s: 1. Dengue 2. Presumed giardiasis
• Principles: “ticks and fleas”
– Immigrants and travelers may present with multiple infections and/or complications, e.g., anemia
– Empiric outpatient therapy sometimes warranted (as in tropics): confirmation ideal but not always practical
Giardia lamblia
• Rx: metronidazole, Nitazoxanide
(Alinia)
• Retreatment occasionally necessary
– Ongoing household reinfection?
– Immune deficiency (CVID)?
– Other? (ie, IBD)

Case 3: Haiti
• 23 yo aide worker, airlifted from rural mountainous Haiti after 6 weeks of non-bloody watery diarrhea
• Cipro/flagyl x 5 days
• Stool fecal leuks neg, Cx neg
• Med-evaced to GUH for severe dehydration
• Cholera???

Haiti: current situation
• 1.2 million DPs
• MSF teams treated >41,000 cholera
patients since start of outbreak
• More than 1,800 deaths
• Under reporting
• Crowding, poor sanitation, malnutrition
• Disrupted water system
• Buckets

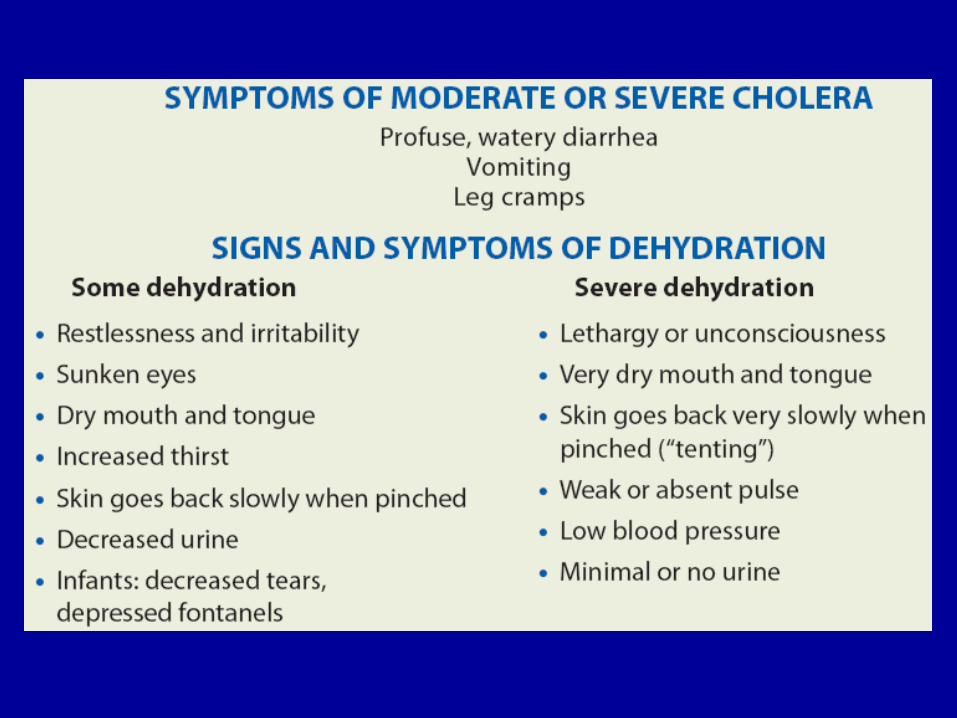
Cholera
• Vibrio cholera 01
• Other non-cholera Vibrio sp. (haemolyticus, parahaemolyticus)
• Low infectious dose
• Rapid environmental spread
– Biofilms in environment increase infectivity to human as better passes through stomach
– Sewage-contaminated drinking water, seafood contaminated with water, food/water contaminated with feces
• Cytokine-producing T-cells
• cGMP transport profuse “rice-water” stools

CDC Nov. 2010

Reactive arthritis
• Reiter’s no longer P.C.
(arthritis/urethritis/uveitis)
• SSYC
• Predilection for lower extremities
• 1-4 wks post-infectious diarrhea
(avg: 2 wks)
• HLA-B27?
Clostridium difficile• 1935 – C. difficile discovered
• 1978 – first associated w/ disease
• 2004 – CDC reports new, more virulent strain
• Epidemiology:
– CDC: 15-30,000 deaths/year
– 1-2.5% fatality
– 13 cases/1,000 hospitalized
• Difficult to eradicate
– Alcohol-based hand sanitizers do not kill spores
– Can live in hospital room up to 40 days
– Contact isolation gown, gloves
– Wash hands!
Clostridium difficile• Almost every antibiotic can cause
– PCN, Clinda, Cephs most common
– Can occur weeks after Abx stopped
• Sx: fever, abd pain, profuse diarrhea +/- blood, elevated WBC/CRP leukemoid rxn
• Dx: stool C. diff toxin (A>B)
• Carriage w/o symptoms common in newborns and <1y
– Intestinal colonization as high as 50% in healthy neonates vs <5% in >2y
– Difficult to interpret toxin assay results in <12mo w/o GI sxs, fever, etc. only order if pre-test probability high

Clostridium difficile
• Rx: metronidazole 30mg/kg/day PO div Q8hrs OR Vanco 40mg/kg/day PO if no response to metronidazole x 10d
– Metronidazole resistance reported
– PO Vanc role in VRE
• Up to 40% relapse - retreatment • Contact precautions: duration of clinical
illness while C.diff pos
• Alcohol-based hand cleansers are not effective in removing C.diff spores
Rotavirus• Reoviridae Family
• 11 segments of
dsRNA
• Strain diversity
• 15 ST; G1-G4, G9
cause majority of
disease
• G1 ST 73% No. Amer.
• Surface antigens VP7
(G protein) and VP4 (P
protein) = immune
response

Rotavirus (cont.)
• #1 cause severe diarrhea children <5 in U.S. and
worldwide
– US: 600,000 outpatient visits, 55-70,000
hospitalizations, 20-60 deaths/yr
– Nearly 100% children infected by 5y
• “Wintertime vomiting disease”
• Fever, vomiting, profuse non-bloody diarrhea
(3 - 9 days)
– Vomiting helps dx vs AGE
• Dehydration
PIDJ – Dec 2010
Rotavirus Vaccine
• 1998 Rotashield - safe and effective in prelicensure testing among 18,000
– Pulled from market due to association with intussusception w/i 14d vaccination
– Decision to pull vaccine made early
– CDC, other health agencies involved in surveillance
– Peak incidence intussusception ages 3-9 mo, when vaccine given…Causal vs coincidental?
– Devastating loss of vaccine to developing countries

Rotavirus Vaccine (2)
• 2006 Rotateq - bovine, pentavalent, reassortant live-attenuated oral
• 2008 Rotarix – monovalent, live-attenuated
• Rotateq:– REST Trial - 6 cases intuss. (n=34,837 Rotateq) in 1st
42d vs 5 cases placebo (n=34,788)
– 3 doses, beginning b/w 6-12 weeks
– All 3 doses by 32 weeks
– 71% VE during 1st and 2nd seasons; 88% VE for severe Rota infections
– recent Bangla and Vietnam study 48% effective vs severe Rota

Norwalk agent 1st virus identified to cause gastro
Occurs year round - cold weather, hospitals, cruise ship
Sx: sudden onset vomiting, nonbloody diarrhea
Duration: 1-3 days…longer in immunocompromised
Immunocompromised may shed virus for up to 56 days

Koo - CID 2009
First case series describing Noro as cause of persistent
gastroenteritis in adult HSCT recipients
Previous reports in children
RT-PCR gold standard - best early in illness
Consider Noro esp. in cases of GVHD diarrhea refractory
to prolonged steroid therapy
Conclusion: Contact
precautions• In general, contact precautions until
diarrhea stops
• Little kids bigger concern for
nosocomial transmissionmay not
wash hands well
• Shigella, E. coli 0157:H7 – no
diarrhea and x2 neg stool Cx
• Salmonella – no diarrhea and x3 neg
stool Cx


References
• Ivers, LC and Edward, TR. Infectious disease of severe weather-related and flood-related natural disasters. Curr Opin Infect Dis 2006, 19:408-14.
• Lignon, BL. Infectious diseases that pose specific challenges after natural disasters: a review. Semin Pediatr Infect Dis 2006; 17:36-45.
• MMWR: Vibrio Illnesses After Hurricane Katrina --- Multiple States, Aug-Sept 2005
• Othman, N, Ismail, I, Yip, R, Zainuddin, Z, Kasim, SM, Isa, R, and Noh, LM. Infections in post-tsunami victims. Pediatr Infect Dis J 2007 Oct; 26(10):960-1.
• Watson, JT, Gayer, M, and Connolly, MA. Epidemics after natural disasters. CDC 2007 January. Available at http://www.cdc.gov/ncidod/EID/13/1/1-appt.htm