embracing technology is dumb . embracing well-designed technology is smart
DESCRIPTION
Embracing Technology is DUMB . Embracing Well-Designed Technology is Smart. Dr. Ben-Tzion (Bentzi) Karsh Associate Professor Industrial and Systems Engineering Department Systems Engineering Initiative for Patient Safety University of Wisconsin-Madison (AHRQ: R01 HS013610 (PI-Karsh)) - PowerPoint PPT PresentationTRANSCRIPT
1
Embracing Technology is DUMB.
Embracing Well-Designed Technology is Smart
Dr. Ben-Tzion (Bentzi) KarshAssociate ProfessorIndustrial and Systems Engineering DepartmentSystems Engineering Initiative for Patient SafetyUniversity of Wisconsin-Madison
(AHRQ: R01 HS013610 (PI-Karsh))(NIH 1R01LM008923-01A1 (PI-Karsh))
2
Take Away Messages…
• We know that patient safety problems are the result of the interaction between people, the technology they use, and the system in which they work…SO LEARN HOW TO UNDERSTAND YOUR SYSTEM (don’t focus on technology)
• There is a science devoted to understanding how to design technology to support human performance (physical and cognitive). It’s called human factors engineering (HFE)…LEARN ABOUT IT!
• Technology needs to be designed to be a team player…ANYTHING LESS IN UNACCEPTABLE
• HFE research makes clear that technologies are NOT solutions; they should be ASSISTIVE DEVICES!
3
Main Take Away MessageTHE ROAD TO PATIENT SAFETY AND HIGH
QUALITY PATIENT CARE RUNS THROUGH THE PERFORMANCE OF YOU
AND YOUR STAFF
So if your technology is bad, your performance will be bad. If your performance is bad,
quality and safety suffer
4
Is there evidence HIT improves patient safety or quality?
• CPOE and CDSS?– Yes: (Kaushal & Bates, 2001; Kaushal, Shojania, & Bates, 2003; Mekhjian et al., 2002; King, Paice,
Rangrej, Forestell, & Swartz, 2003; Potts, Barr, Gregory, Wright, & Patel, 2004)
• Bar coding?– Yes: (Poon et al. 2006; Kaushal, Barker, & Bates, 2001; Puckett, 1995; Wald & Shojania, 2001)
• EMRs?– Yes: (Mitchell and Sullivan 2001; Gill et al. 2001; Legler and Oates 1993, Ornstein and Bearden
1994, Solomon and Dechter 1995, Mitchell and Sullivan 2001, Garrison et al. 2002)
5
But something isn’t right…
• EMR– Concerns related to cost, a lack of tested systems,
number of steps to complete tasks, problems with data entry, inexperienced vendors, confidentiality, and security found (Ornstein and Bearden 1994, Wager et al. 2000, Mitchell and Sullivan 2001)
– Entire systems have been abandoned because of problems with poor reliability, poor credibility, poor consistency, and problematic user interface design (Lawler
et al. 1996)
6
But….
• CPOE– Systems have been abandoned (Prabhu, 2003)
– CPOE can increase the incidence rate of errors, adverse events and mortality (Koppel et al. 2005, Nebeker et al. 2005, Thompson et al. 2005, Han et al. 2005)
• Bar coding– Nurse don’t use it as “they are supposed to”
and mistakes can still be made (McDonald 2006; Patterson et al. 2002, 2006)
7
But….
• Smart IV pumps– “We found no measurable impact on the
serious medication error rate… technological and nursing behavioral factors must be addressed if these pumps are to achieve their potential for improving medication safety” (Rothschild et al. 2005)
• CDSS in CPOE– Physicians override up to 90% of drug alerts
(Weingart et al., 2003)
8
Oh my
9
Confession
• We don’t know to what extent technology DESIGN has caused patient safety problems.
• In existing studies, it is nearly impossible to determine what was related to design, to implementation, to new workflow….
10
What’s the Problem? The Prevailing Paradigm
for healthcare technology?
(stolen from Matt Scanlon, MD)
11
How do we get beyond this state of “technology will save me” and “technological determinism”?
A few propositions…
12
Proposition #1: Stop blaming everything on “human error”!
13
• Human error?
14
If the wrong number is keyed in, is it “human error”?
At the bar code data committee meeting yesterday, we discussed the fact that nurses sometimes need to scan several times before the bar code 'takes'. The nurse educator … said that she teaches nurses that if they don't succeed on the first couple scans, to key in the number from the med bottle.
15
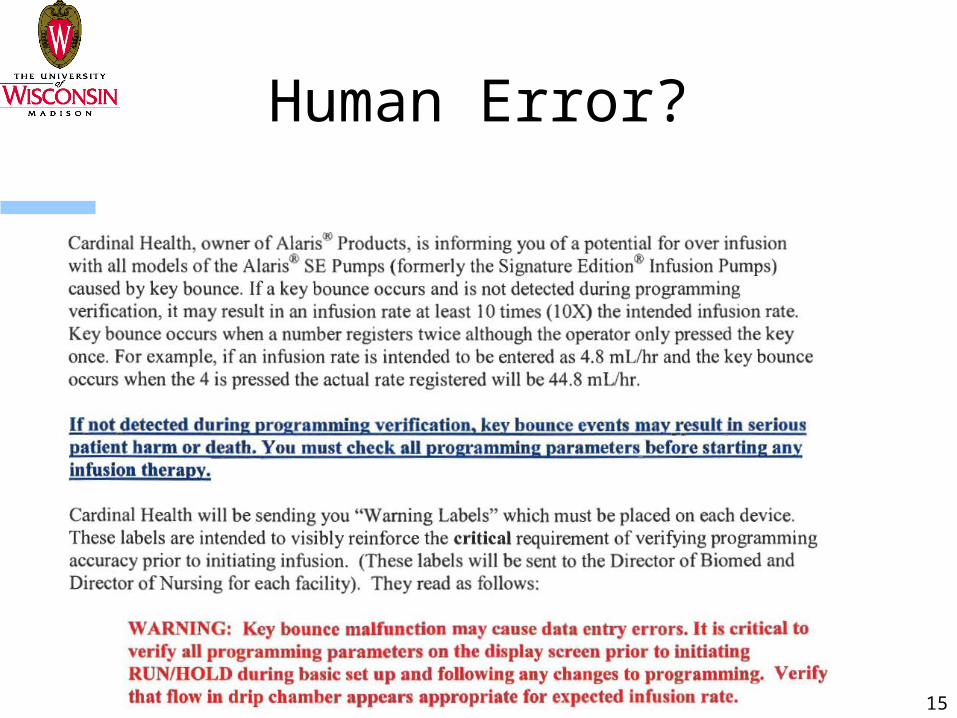
Human Error?
16
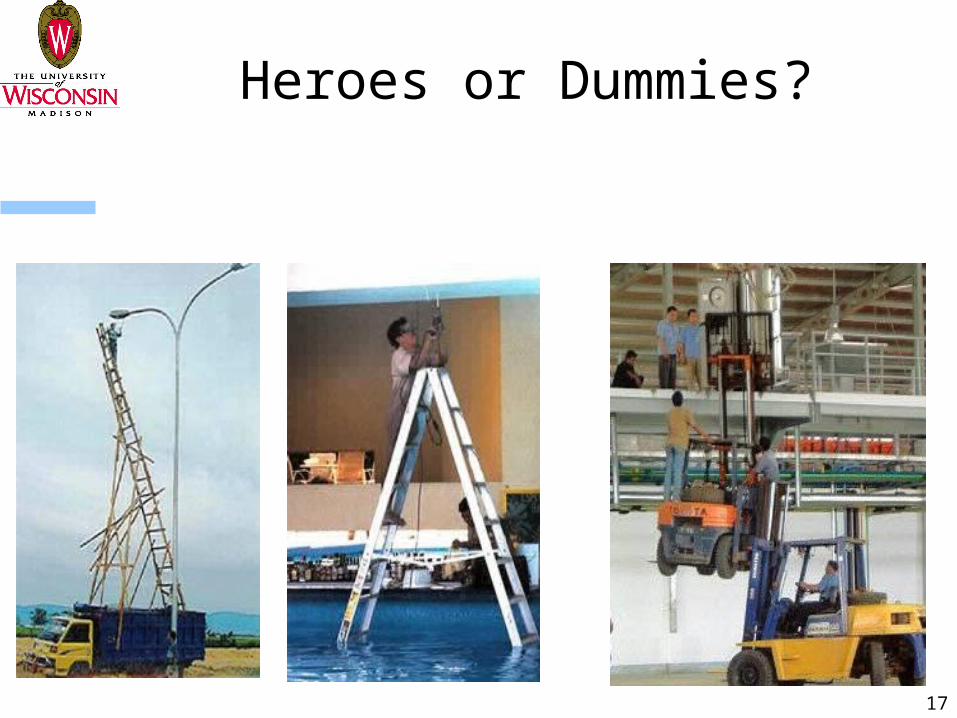
Proposition #2: Workarounds and violations of technology protocols
are GOOD!
When you see them, you should thank the violator!
17
Heroes or Dummies?
18
Heroes or villains?
• Maybe workarounds/violations are the right choice when the technology is not appropriate for the situation?
• Maybe workarounds are responses to poorly designed technologies and are therefore symptoms of the actual problems?
19
Proposition #3: Healthcare professional rejection of technology
is wonderful!
20
• Maybe rejection is a sign that smart people don’t want to be forced to work in ineffective ways
• Maybe the technology is not designed to meet the needs, SIMULTANEOUSLY of– Staff– Patients– Other technologies– Physical layout
21
Proposition #4: Only purchase well-designed technology
22
Technology as Assistive Device
• What is the goal of a walking cane?
• What makes a cane “well-designed” for a particular person?
23
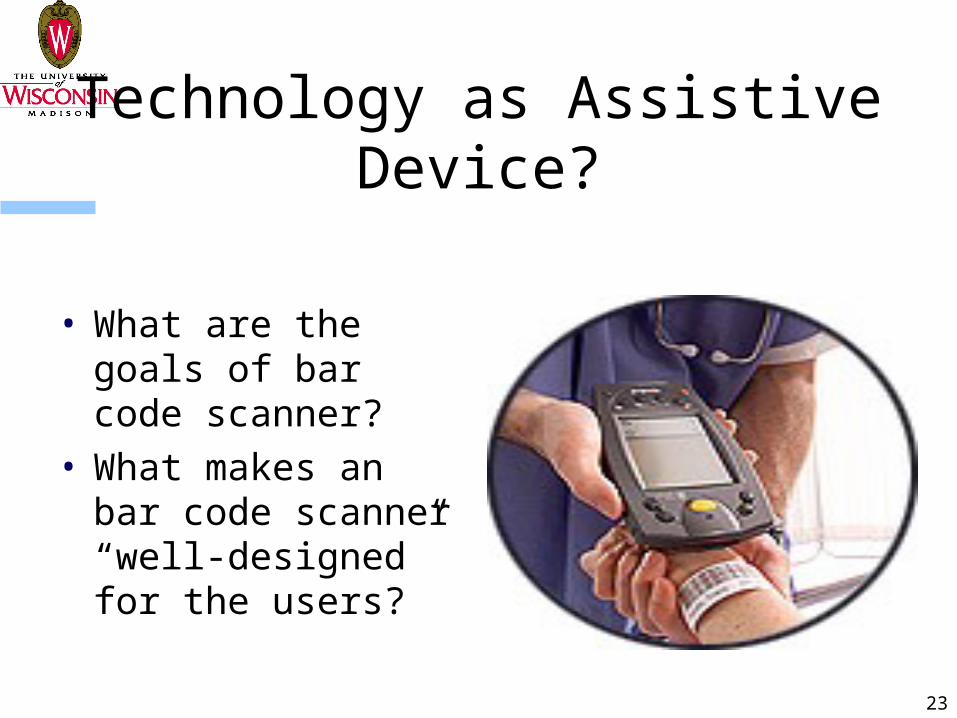
Technology as Assistive Device?
• What are the goals of bar code scanner?
• What makes an bar code scanner “well-designed” for the users?
24
Well-designed technology
• Better feedback to the user
• Better cooperation with the user
• Better visibility and transparency of what the technology is doing
• Better matching of designs to mental models of the USER, not the designer and not the purchaser
25
Example• an A300 crashed in Nagoya, Japan, after the pilots
inadvertently engaged the autopilot’s go-around mode. The pilots countered the unexpected pitch-up by making manual inputs, which turned out to be ineffective. Essentially, the pilot attempted to continue the approach by manually deflecting the control column, which in all other aircraft—and in this aircraft in all modes except the approach mode—would normally disconnect the autopilot. However, in this particular aircraft and in this particular mode, the autopilot had to be manually deselected and could not be overridden by control column inputs. Consequently, a power struggle developed between the pilot and the autopilot, with the pilot attempting to push the nose down through elevator control and the autopilot attempting to lift the nose up through trim control. This caused the aircraft to become so far out of trim that it could no longer be controlled.
26
Proposition #5: Use Human Factors Engineering Expertise
27
**Use Human Factors Engineering Design Thinking**
(modified from Sanders and McCormick 1993)
• Technologies need to be designed for and to work with people
• Systems must be designed to accommodate the range of users
• How systems are designed will influence human behavior and therefore system performance
• Design needs to be evidence-based, not “common sense” or designer driven
• All design must take into account the system of use
28
For more information
• Karsh, B. and Scanlon, M. (2007). When is a defibrillator not a defibrillator? When it is like a clock radio…. The challenge of usability and patient safety in the real world. Annals of Emergency Medicine, 50, 433-435.
• Holden, R. J. and Karsh, B. (2007). A theoretical model of health information technology behavior. Behaviour and Information Technology, 1-17. DOI: 10.1080/01449290601138245. URL: http://dx.doi.org/10.1080/01449290601138245
• Karsh, B., Holden, R. J., Alper, S. J., and Or, K. L. (2006). A human factors engineering paradigm for patient safety – designing to support the performance of the health care professional. Quality and Safety in Healthcare, 15(Suppl I), i59-i65.
29
For more information
• Carayon, P. (Ed.) (2007) Handbook of Human Factors in Health Care and Patient Safety. Lawrence Erlbaum Associates: Mahwah, New Jersey.
• Nielsen, J. Usability Engineering. New York: AP Professional, 1993.• Norman, DA. The Design of Everyday Things. New York:
Doubleday. 1998. • Salvendy (Ed.), (2006) Handbook of Human Factors and
Ergonomics (3rd ed). John Wiley and Sons. • Sanders, M. S., & McCormick, E. J. (1993). Human Factors in
Engineering and Design (7th ed). McGraw-Hill, Inc. • Spath (2000). Error Reduction in Health Care: A Systems Approach
to Improving Patient Safety. Jossey Bass Wiley. • Wickens, C. D., Lee, J. D., Liu, Y., & Becker, S. E. G. (2004). An
Introduction to Human Factors Engineering (2nd ed.). Prentice Hall.• Woods and Hollnagel (2006). Joint Cognitive Systems. CRC Press.
30
THANK YOU!
QUESTIONS???
Ben-Tzion Karsh, Ph.D.Associate ProfessorDepartment of Industrial EngineeringUW-Madison
Contact InformationIndustrial EngineeringUniversity of Wisconsin-Madison1513 University Avenue, Room 3218Madison, WI 53706Tel: 608-262-3002Fax: 608-262-8454E-mail: [email protected]/mesh