embedding the vision of future in mind and the five year forward view for mental health in our...
TRANSCRIPT

www.england.nhs.uk
Embedding
Future in mind in
our communities
Peter Fonagy, National Clinical Lead for CYP
IAPT
Kathryn Pugh, Children and Young People’s
Programme Lead
Anne O’Herlihy, Project Manager CYP IAPT
and the Children and Young People’s Team,
NHS England
www.england.nhs.uk
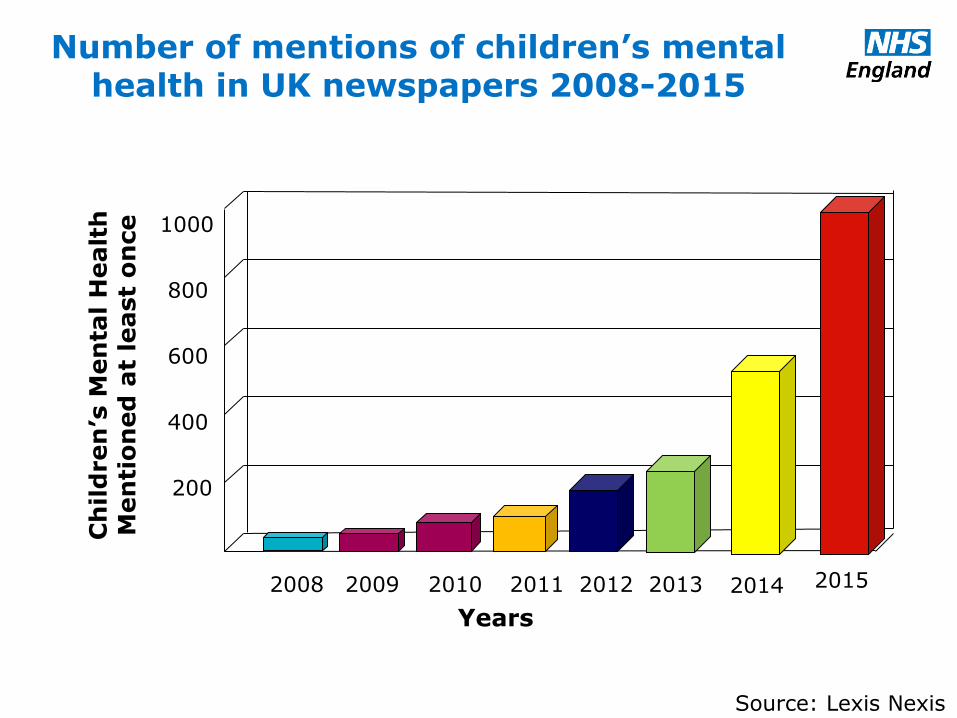
Number of mentions of children’s mental health in UK newspapers 2008-2015
Years
Source: Lexis Nexis
Ch
ild
ren
’s M
en
tal H
ealt
h
Men
tio
ned
at
least
on
ce
2008 2009 2011 2010 2012 2013
200
400
600
800
1000
2015 2014

www.england.nhs.uk
Mentions of Child and Adolescent Mental Health Services or CAMHS in UK Newspapers
Source: Lexis Nexis
Logarith
mic
scale
(ln
)
0
20
50
150
1000
Quinquennial rates
2015 2010 2005 2000
400
N=640
N=74
N=24
N=3
www.england.nhs.uk

www.england.nhs.uk

www.england.nhs.uk
Future in Mind and the Five Year Forward View
Key Themes
• Sets direction of travel across health,
education, children’s social care and
youth justice
• Consensus across the whole system
built on principles of CYP IAPT, EBP,
including the core need for participation
from children, young people, families and
carers, outcomes focused.
• A clear steer and some key principles
about how to make it easier for children
and young people to access high quality
mental health care when they need it.
• Five year strategy designed for and with the NHS and health ALBs.
• For people of all ages and it sets out priorities to improve mental health care across the whole NHS
• Reiterates that by 2020/21, at least 70,000 (30%) more children and young people should have access to high-quality mental health care when they need it.
• Also focused on improving the workforce, and addressing inequalities promoting better leadership across mental health
Published March 2015 Published February 2016

www.england.nhs.uk
Future in Mind and the Five Year Forward View
Some key common themes
• Promoting resilience, prevention
and early intervention
• Improving access to effective
support
• Care for the most vulnerable
• Accountability and transparency
• Developing the workforce
• Promoting good mental health and
preventing poor mental health
• A 7 day NHS – right care, right time,
right quality
• Complex need services nationally from
2016
• ‘Hard-wiring’ mental health across the
NHS
www.england.nhs.uk
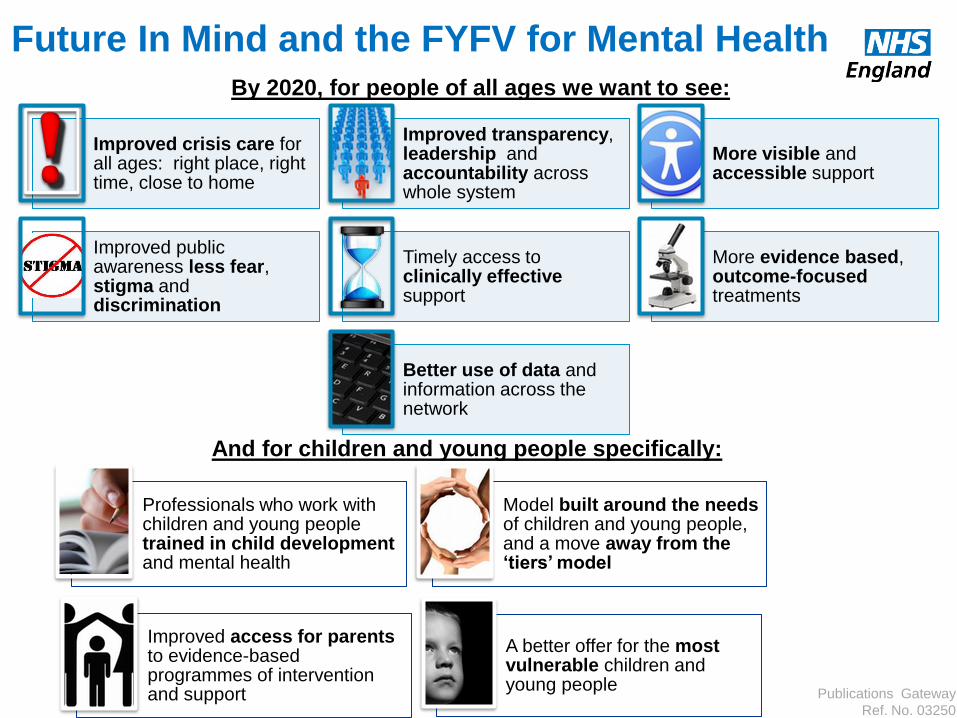
Future In Mind and the FYFV for Mental Health
By 2020, for people of all ages we want to see:
Publications Gateway
Ref. No. 03250
And for children and young people specifically:
Improved crisis care for all ages: right place, right time, close to home
Improved transparency, leadership and accountability across whole system
More visible and accessible support
Improved public awareness less fear, stigma and discrimination
Timely access to clinically effective support
More evidence based, outcome-focused treatments
Better use of data and information across the network
Professionals who work with children and young people trained in child development and mental health
Model built around the needs of children and young people, and a move away from the ‘tiers’ model
Improved access for parents to evidence-based programmes of intervention and support
A better offer for the most vulnerable children and young people

www.england.nhs.uk
Local Transformation Plans
All CCGs submitted Local Transformation Plans (LTPs) on time
123 plans covering 209 CCG areas
Assurance determined monies going out to all CCGs by End December
Spend to be tracked in Q3 and Q4
Plans in user friendly format on web by 31st December 15 – had to include baseline data
Continuous tracking of use of funds in further years to be part of routine assessment process
LTPs should be refreshed, republished each year and included in Sustainability and Transformation plans

www.england.nhs.uk
Transformation plans should
Be Transparent – publishing:
• Baseline investment by local commissioners
• What services are provided including workforce information
• Referrals received, accepted, waiting times
Demonstrate Service transformation in line with principles covering
• Range and choice of treatments and interventions available;
• Collaborative practice with children, young people and families and involving schools;
• Use of evidence-based interventions; and regular feedback of outcome monitoring to children, young people and families and in supervision.
Monitor improvement
• Development of a shared action plan and a commitment to monitor, track and review improvements with appropriate governance structures.

www.england.nhs.uk
LTP = a good CYP MH Strategy Cover the spectrum of services
Including community eating disorder services
Focus on prevention interventions, for existing or emerging mental health problems
Transitions between services.
Include local leadership and governance arrangements
To secure a whole system approach to delivery at local level
Demonstrate collaborative commissioning within and across sectors
To promote effective joint working and establish clear pathways.
This includes working with collaborative commissioning groups in place between NHS England specialised commissioning teams and CCGs
Demonstrate that schools are given the opportunity
To contribute to the development of Transformation Plans.
Be coherent with local priorities
And with the child mental health requirements in the existing joint planning guidance.

www.england.nhs.uk
Complete focus from many local areas with clear leadership
Joined up approach
Understanding of importance of EBP and authentic participation
Focus of strategic players supporting local areas
Raised profile of CYP MH locally and nationally
Creative ideas and energy
Things to celebrate from the LTPs

www.england.nhs.uk
Key challenges for us all
Workforce planning and capacity - across all sectors
Variable leadership, commissioning and collaboration
Joint commissioning – how rather than why
IT planning - need to comply with requirements to be able to flow data and use outcomes in the room
Anxiety about spending the money in the best possible way

www.england.nhs.uk
Delivery of
evidence-
based
practices
Building on what we know works
Improving access
& engagement
Increasing MH
awareness &
decreasing
stigmatisation
Improving
outcomes
accountability
Enhancing youth, carer and community
participation

www.england.nhs.uk
CYP IAPT: expansion (NHS England & HEE)
Continued commitment to embedding evidence based, outcome focussed collaborative service transformation with full participation
Model of delivery is through a collaborative and mentoring scheme between learning collaboratives (HEI) that work in partnership with local providers
Increased geographical coverage of service transformation programme to100 % by 2018
Offer training across partnerships (NHS, LA, Vol sect): CBT, SFP, IPT-A, Parenting, Supervision, Service Transformational Leadership, EEBP, outreach service development, outreach enhanced supervision.
•Children and young people with learning disabilities or autistic spectrum disorder
•Working with 0-5s
•Counselling
•Combination - Prescribing and therapy
• Inpatient CAMHS
New curricula – evidence based interventions for
National Accreditation Council – assure quality of training and embedding of principles

www.england.nhs.uk
CYP IAPT
Partnerships Map
Following recruitment of
6th collaborative,
programme on target to
work with services
covering 80% of 0-19
population by March
2016.
This goes up to 87%
when including ‘light
touch’ outreach and
service leadership work
to prepare partnerships
for full modality training

www.england.nhs.uk
• Young people seen more quickly-time
between referral and assessment
decreased by 73%
• YP achieved significant clinical
improvement over fewer sessions -
number of days between assessment
and discharge decreased by 21%
Is it working?
239
299
64
235
Days between referral andassessment
Days between assessmentand discharge
Pre CYP-IAPT With CYP-IAPT
Improved access through self-referral routes, single point of
access, outreach services, evening and weekend
appointments.

www.england.nhs.uk
Greater involvement of children,
young people and
their parents or carers:
Throughout treatment and every aspect of their care
Recruitment and interview
panels
Staff appraisal and
training
Website and information
design
Planning and delivery of
mental health awareness
Mystery shopped service
evaluation
Environ-mental changes
Speaking with clinical
directors
New feedback systems ‘you said, we did’
Increased agentive CYP involvement
56%
34%
Pre CYP-IAPT2 With CYP-IAPT
CYP agreed they had
recovered sufficiently to be
discharged - percentage of
closed cases by mutual
agreement increased

www.england.nhs.uk
Building on what we know - LTP
baseline
Abi Childs and Rahul Agarwal
NEL Healthcare Consulting, NEL CSU

www.england.nhs.uk
Referrals per 1000 CYP
Abi Childs and Rahul Agarwal
NEL Healthcare Consulting, NEL CSU
www.england.nhs.uk
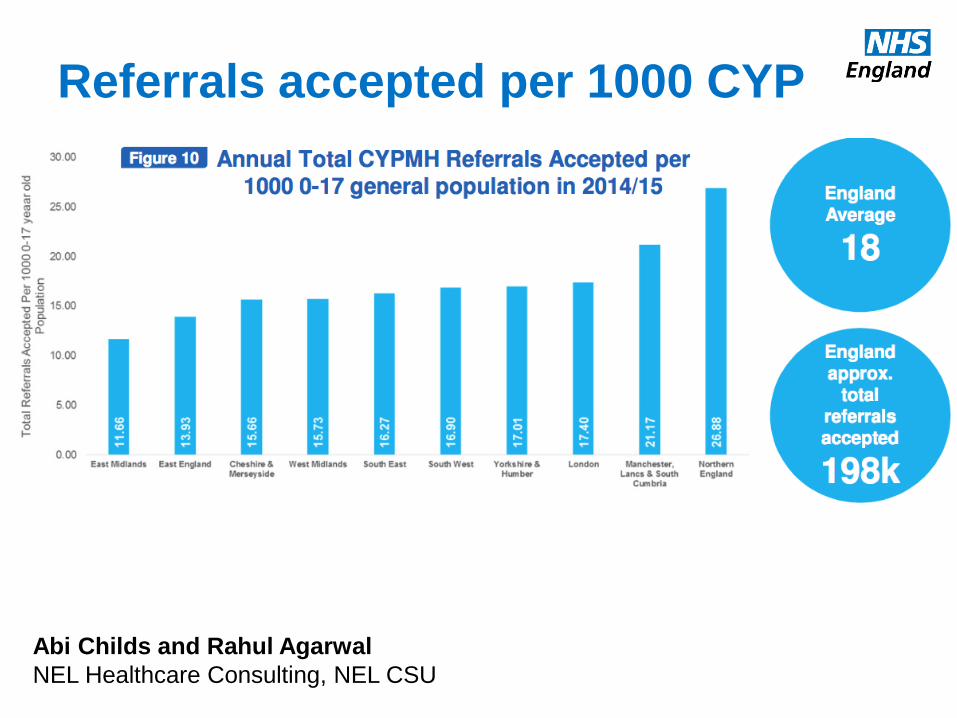
Referrals accepted per 1000 CYP
Abi Childs and Rahul Agarwal
NEL Healthcare Consulting, NEL CSU

www.england.nhs.uk
CYPMH expenditure per 1000 CYP
Abi Childs and Rahul Agarwal
NEL Healthcare Consulting, NEL CSU
www.england.nhs.uk
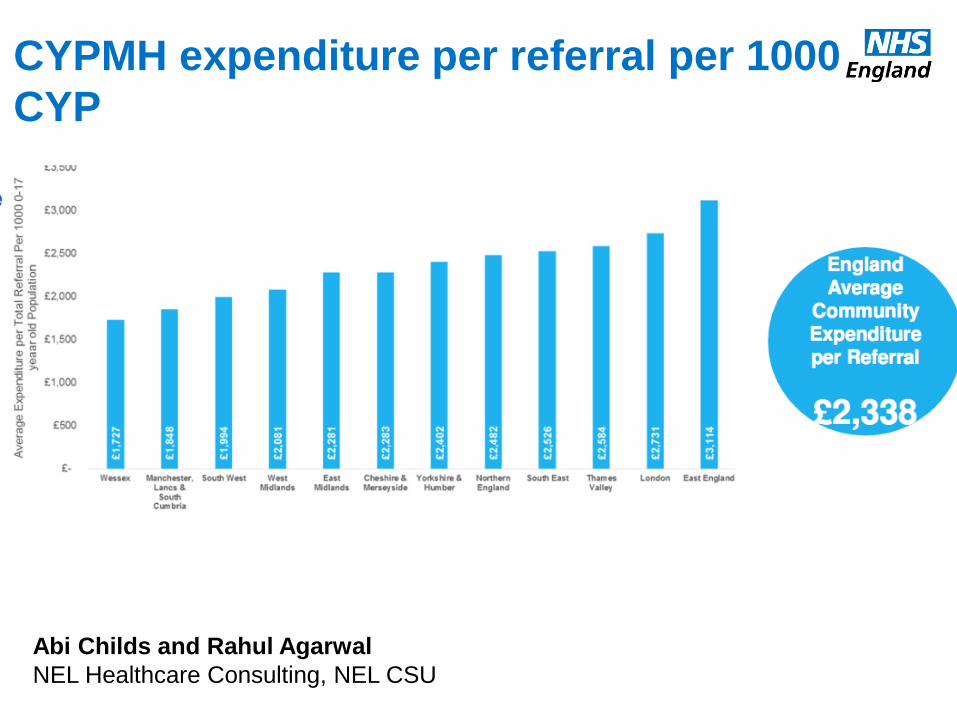
CYPMH expenditure per referral per 1000
CYP
Abi Childs and Rahul Agarwal
NEL Healthcare Consulting, NEL CSU

www.england.nhs.uk
Predicting referral acceptance Not an obvious relationship
TOTAL EXPENDITURE WORKFORCE
p > 0.05 p > 0.05

www.england.nhs.uk
Teams working together: The AMBIT approach
Mentalizing
© Bevington & Fuggle
How does AMBIT make people work collaboratively?

www.england.nhs.uk
Teams working together: The AMBIT approach
How does AMBIT make people work collaboratively?
1. Putting learning at the centre of the team culture
2. Developing a whole team Approach which recognises the interdependence of colleagues within a team
3. Using this team to support the development of strong individual key working relationships
4. Using a systems approach to emphasise interconnectedness and shared intentions across the wider multi-agency network.
www.england.nhs.uk
Empirically supported therapies
(ESTs) adapted to improve outcomes
or engagement in subgroups of
individuals expected to respond poorly
to ESTs.
Parent–Child Interaction Therapy (PCIT), an
EST for disruptive behavior, adapted for
Mexican American families; outperformed
nonadapted PCIT at follow-up (McCabe & Yeh,
2009; McCabe et al., 2005, 2012).
ESTs that alter or leverage environments
(e.g. family, school, peers) thought to
impact youth outcomes; therapists
conduct treatment at least partly within
these environments using formats
tailored to patient needs, based on individualized goals.
Multisystemic Therapy, an EST for
both delinquent and substance-
abusing adolescents that is widely
disseminated (Henggeler, 2011; Henggeler &
Schaeffer, 2010; Schoenwald, 2010).
ESTs organized into self-contained
modules that can be used multiple
times or not at all, and combined as
needed; decision-making flowcharts
guide which modules to use and when
to use them for a particular patient.
Modular Approach to Therapy for Children
with Anxiety, Depression, Trauma, or
Conduct Problems; outperformed standard
ESTs at posttreatment and usual care at
posttreatment and follow-up (Chorpita & Weisz, 2009;
Chorpita et al., 2013; Weisz et al., 2012)
A trial design that randomizes
individuals to a first-stage treatment or
assessment condition, assesses
response, then potentially randomizes
individuals to next-stage treatment
options based on their response;
generates evidence for constructing
decision rules in sequencing treatments.
A SMART of minimally verbal children with autism
found superior outcomes for communication
intervention augmented by a speech-generating
device (vs. nonaugmented intervention), and, for
nonresponders after 3 months, intensified
augmented intervention (vs. intensified
nonaugmented intervention; Kasari et al., 2014).
A system of administrating assessments of
treatment outcomes and progress indicators
that are psychometrically sound, sensitive to
clinical change, brief, and clinically useful;
then storing and displaying the data in
meaningful formats to provide feedback
about how well treatment is working.
The Youth Outcome Questionnaire and
Youth Outcome Questionnaire Self-Report
have identified youths at-risk of treatment
failure; Youth-Clinical Support Tools pinpoint
obstacles and suggest solutions (Burlingame et
al., 2001; Cannon et al., 2010; Ridge et al., 2009; Warren & Lambert,
2012; Warren et al., 2012).
Research syntheses of randomized
trials comparing alternative treatment
strategies or types directly (i.e. within
the same trial) among patients with
specific characteristics.
A meta-analysis compared psychotherapy,
medication, and combination psychotherapy-
medication for subgroups of depressed adults and
found sufficient evidence to recommend
medication for dysthymia and combination
treatment for older adults and outpatients
(Cuijpers et al., 2012).
Models that guide decision-making
based on multiple characteristics of
individuals; developed through data-
mining, an exploratory approach for
detecting and interpreting patterns in
data.
The Distillation and Matching Model mined data
from youth psychotherapy trials to develop a tool to
select efficacious treatments, or their elements,
based on patient characteristics; produced
medium-large pre-post effects as part of a
comprehensive service model (Chorpita & Daleiden, 2013; Chorpita et al., 2005; Southam-Gerow et al.,
2013).
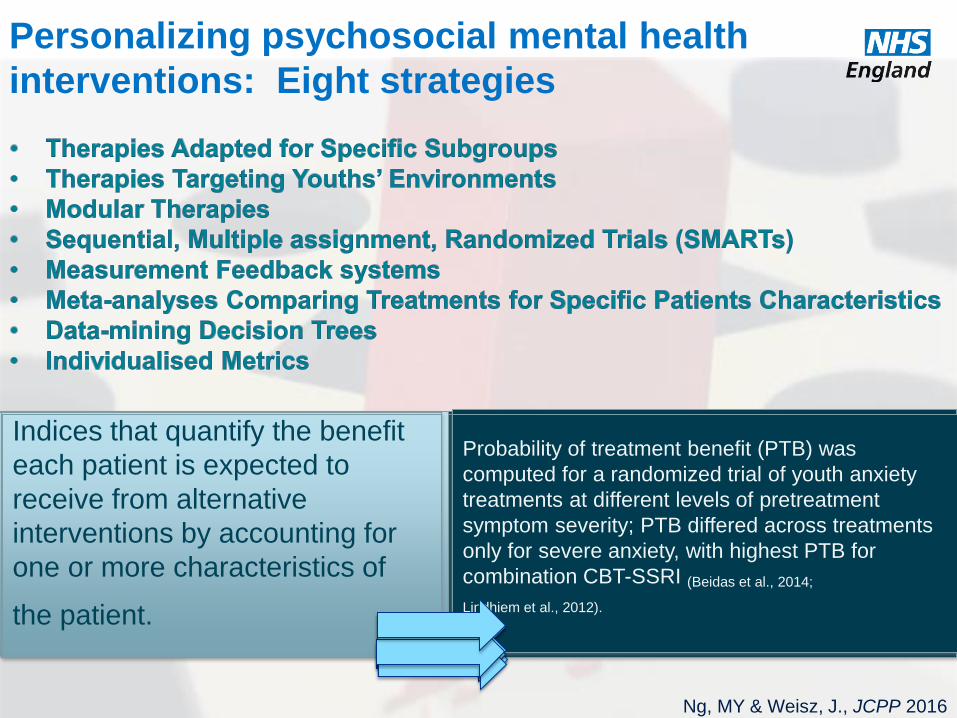
Indices that quantify the benefit
each patient is expected to
receive from alternative
interventions by accounting for
one or more characteristics of
the patient.
Probability of treatment benefit (PTB) was
computed for a randomized trial of youth anxiety
treatments at different levels of pretreatment
symptom severity; PTB differed across treatments
only for severe anxiety, with highest PTB for
combination CBT-SSRI (Beidas et al., 2014;
Lindhiem et al., 2012).
Personalizing psychosocial mental health
interventions: Eight strategies
Ng, MY & Weisz, J., JCPP 2016