ellis w. laderdownload.e-bookshelf.de/download/0004/0223/09/l-g...field guide to the arrhythmias...
TRANSCRIPT

Field Guide to the ArrhythmiAsEllis W. ladEr


F IELD GUIDE TO THE
Arrhythmias

To my family

FIELD GUIDE TO THE
Arrhythmias
ELLIS W. LADER, MD, FACC, FAHA, FACPMid Valley Cardiology, Kingston, and
Adjunct Assistant Professor of Clinical Medicine
New York University School of Medicine
New York, NY, USA
A John Wiley & Sons, Ltd., Publication

This edition first published 2013 C© 2013 by John Wiley & Sons Limited
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientific, Technical andMedical business with Blackwell Publishing.
Registered office: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester,West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to apply forpermission to reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with the UKCopyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, inany form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by theUK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names andproduct names used in this book are trade names, service marks, trademarks or registered trademarks of theirrespective owners. The publisher is not associated with any product or vendor mentioned in this book. Thispublication is designed to provide accurate and authoritative information in regard to the subject matter covered. Itis sold on the understanding that the publisher is not engaged in rendering professional services. If professionaladvice or other expert assistance is required, the services of a competent professional should be sought.
The contents of this work are intended to further general scientific research, understanding, and discussion only andare not intended and should not be relied upon as recommending or promoting a specific method, diagnosis, ortreatment by physicians for any particular patient. The publisher and the author make no representations orwarranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim allwarranties, including without limitation any implied warranties of fitness for a particular purpose. In view ofongoing research, equipment modifications, changes in governmental regulations, and the constant flow ofinformation relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate theinformation provided in the package insert or instructions for each medicine, equipment, or device for, amongother things, any changes in the instructions or indication of usage and for added warnings and precautions. Readersshould consult with a specialist where appropriate. The fact that an organization or Website is referred to in thiswork as a citation and/or a potential source of further information does not mean that the author or the publisherendorses the information the organization or Website may provide or recommendations it may make. Further,readers should be aware that Internet Websites listed in this work may have changed or disappeared between whenthis work was written and when it is read. No warranty may be created or extended by any promotional statementsfor this work. Neither the publisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication Data
Lader, Ellis W.Field guide to the arrhythmias / Ellis W. Lader, MD, FACC, FAHA, FACP, Mid Valley Cardiology, adjunct
assistant professor of clinical medicine, New York University School of Medicine, New York, NY, USA.pages cm
Includes bibliographical references and index.ISBN 978-1-118-38609-5 (pbk. : alk. paper) 1. Arrhythmia. I. Title.RC685.A65L33 2013616.1′28–dc23
2012047266
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not beavailable in electronic books.
Cover image and cartoons: Jane FallowsCover design by Andy Meaden
Set in 9.5/11.5pt Minion by Aptara Inc., New Delhi, India
1 2013

Contents
Key to the Arrhythmias, inside front/back covers
Preface, vi
Acknowledgments, viii
Abbreviations, ix
PART 1: THE RHYTHMS, 1
Normal Sinus Rhythm, 3
Preexcitation, 4
Sinus Bradycardia, 6
Sinus Tachycardia, 7
Sinus Arrhythmia, 8
Wandering Atrial Pacemaker, 9
Multifocal Atrial Tachycardia, 10
Junctional Rhythm, 12
Asystole, 14
Heart Block: First Degree, Second Degree (Mobitz I and II), and ThirdDegree (Complete), 16
Premature Beats (Blocked and Otherwise), 20
Atrial Fibrillation, 23
Atrial Flutter, 25
Supraventricular (Paroxysmal Atrial) Tachycardia, 28
Pacemaker Rhythms, 30
Ventricular Tachycardia, 33
Accelerated Idioventricular Rhythm, 36
Prolonged QT/Torsades de Pointes, 38
Ventricular Fibrillation, 41
PART 2: MULTIPLE CHOICE QUESTIONS, 43
v

Preface
If the innocent or uninitiated were to wander through the cardiac unit, telemetryunit, or in fact through any unit where ECG monitoring is in use (we will stickwith the English ElectroCardioGram spelling), he or she would likely encounterrhythms which were unfamiliar. It is even possible such rhythms might be rudelythrust into one’s face with a request to evaluate them or even take drastic action:“Should I shock him?” or “Do you think this is Mobitz I second degree SAexit block?” In fact, traveling through a unit in such fashion may be likenedto a wanderer strolling through a forest, unsure of the names of the trees orwildflowers, or the significance of certain tracks (see below figure).
Track of Brotozoum giganteum, generally best avoided (with size 11 human footprints, forscale)
When one is in the woods it greatly increases the pleasure and possibly thesafety of the trip if the hiker has a Field Guide which enables the wanderer tosafely identify the various flora and fauna encountered along the way. It shouldthen take the reader just a moment to realize, carrying the metaphor only a littlefurther, the need for a similar Field Guide to the Arrhythmias, as one navigatesthe various hazards of the typical cardiac unit. Hence this work.
This Guide is intended for the student, the casual explorer, making his orher first forays into the Realm of the Cardiac Monitor.1 A trained cardiologistwon’t need it, being able to identify an arrhythmia using only a fragment of a
1We assume, gentle reader, that you have mastered the very basics of the ECG: i.e., you can
tell which side of the rhythm strip or ECG is up, know that the rhythm is recorded from left
to right, can identify the P, QRS, and T waves, and know their normal widths and intervals.
Otherwise, I have included two of my favorite references below, or you can go ask the Head
Nurse politely. Dubin D. Rapid Interpretation of EKGs: An Interactive Course, 6th edn. Tampa,
FL: Cover Publishing Co., 2000. Wagner GS. Marriott’s Practical Electrocardiography, 11th edn.
Philadelphia, PA: Lippincott Williams & Wilkins, 2007.
vi

PREFACE vii
P wave, akin to a botanist who only needs a petal and a few stamens to iden-tify a subspecies of goldenrod. A few cardiologists, surprisingly, have expresseddispleasure with this Guide. They claimed it was too offbeat and irreverent fortheir serious tastes. Personally, I suspect they secretly fear the Guide may do awaywith the need for their services! Actually, except for the few remaining clinicalcardiologists, many of them might actually need a basic guide themselves. Someof the interventionalists I know haven’t looked at an ECG in years.
But seriously, the cardiac unit is a jungle, inhabited by fierce nurses, killerintensivists, marauding attendings, various flesh-eating specialists, sick patients,and lots of arrhythmias. Being able to quickly and easily identify the arrhythmiasone is likely to encounter there (or anywhere else) is likely to make one’s travelsthere more enjoyable and probably safer. So gather up your Guide, bring alongyour butterfly net, magnifying glass, calipers, and an extra pair of socks, and let’sget started!

Acknowledgments
I would like to acknowledge the invaluable electrocardiographic teaching Ireceived early in my training from Dr. Bertha Rader, the Queen of Electro-cardiography at Bellevue Hospital, New York. I must also thank Alice Lopez andPat Curtis, the giants of our practice’s and Benedictine Hospital’s arrhythmiaservices, along with our ICU and step-down unit nurses, and monitor techs inthe “war room,” all of whom helped supply the rhythm strips and inspire someof the scenarios that made this work possible.
viii

Abbreviations
AIVR Accelerated idioventricular rhythmAV AtrioventricularCCU Coronary Care UnitCPR Cardiopulmonary resuscitationCT Computed tomographyECG ElectrocardiogramICU Intensive Care UnitPAC Premature atrial complexPVC Premature ventricular complexSVT Supraventricular tachycardiaVT Ventricular tachycardia
ix


PART 1
The Rhythms

Field Guide to the Arrhythmias, First Edition. Ellis W. Lader.C© 2013 John Wiley & Sons, Ltd. Published 2013 by Blackwell Publishing Ltd.

Normal Sinus Rhythm
DESCRIPTIONThis, technically, isn’t an arrhythmia at all, but needs to be included simplybecause it’s very important to be able to call something “normal” if it really is!
The key is that it’s regular, that it’s between a rate of 60 and 100, and mostimportantly, that every QRS is preceded by a P wave at the proper interval. Thecomplexes may be wide or narrow, but they must have a preceding P wave.
The rhythm is regular, nice P waves, not too fast, not too slow, and asDr. Goldilocks1 would say, “Just right!”
HABITATThis rhythm may be found anywhere, and actually may be seen inhabitingmost cardiac monitors, which might make one wonder why that patient isbeing monitored in the first place. It usually means the patient is in some kindof equilibrium with the world: not too hot, not frightened, not in pain, notsuffering from bad heart failure, breathing comfortably … in short, at least bythe monitor, doing all right.
CALL“Can I take this patient off telemetry?”
RESEMBLANCE TO OTHER ARRHYTHMIASIt’s regular, so it could be confused with any other rhythm that’s regular, butthe key is that there’s a P wave in front of every QRS and the rate is 60–100. Ajunctional rhythm is regular but has no P waves.
CARE AND FEEDINGJust keep up what you’re doing! We don’t want to speed things up or slow thingsdown. So avoid excitement, avoid pain, don’t burn your tongue on hot coffee –in short, just do what your mother told you to do.
1Dr. Goldilocks was a famous electrophysiologist at New York University in the late 1980s.
3
Preexcitation
0.10 sec
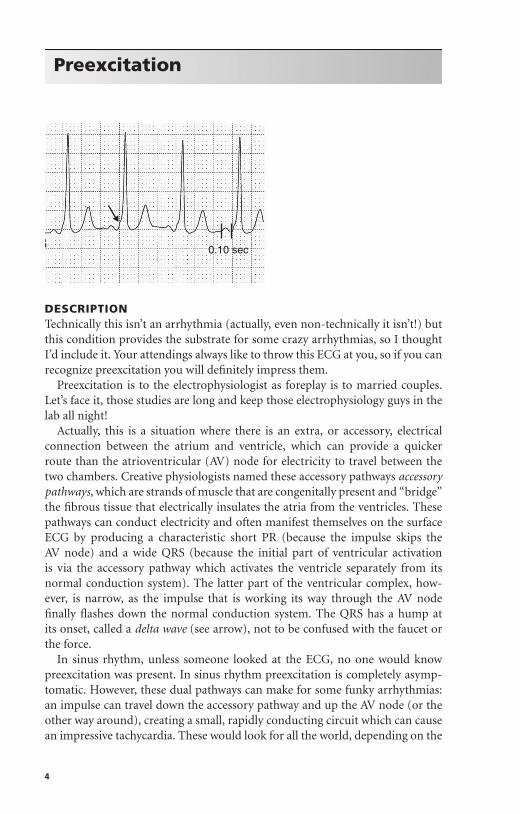
DESCRIPTIONTechnically this isn’t an arrhythmia (actually, even non-technically it isn’t!) butthis condition provides the substrate for some crazy arrhythmias, so I thoughtI’d include it. Your attendings always like to throw this ECG at you, so if you canrecognize preexcitation you will definitely impress them.
Preexcitation is to the electrophysiologist as foreplay is to married couples.Let’s face it, those studies are long and keep those electrophysiology guys in thelab all night!
Actually, this is a situation where there is an extra, or accessory, electricalconnection between the atrium and ventricle, which can provide a quickerroute than the atrioventricular (AV) node for electricity to travel between thetwo chambers. Creative physiologists named these accessory pathways accessorypathways, which are strands of muscle that are congenitally present and “bridge”the fibrous tissue that electrically insulates the atria from the ventricles. Thesepathways can conduct electricity and often manifest themselves on the surfaceECG by producing a characteristic short PR (because the impulse skips theAV node) and a wide QRS (because the initial part of ventricular activationis via the accessory pathway which activates the ventricle separately from itsnormal conduction system). The latter part of the ventricular complex, how-ever, is narrow, as the impulse that is working its way through the AV nodefinally flashes down the normal conduction system. The QRS has a hump atits onset, called a delta wave (see arrow), not to be confused with the faucet orthe force.
In sinus rhythm, unless someone looked at the ECG, no one would knowpreexcitation was present. In sinus rhythm preexcitation is completely asymp-tomatic. However, these dual pathways can make for some funky arrhythmias:an impulse can travel down the accessory pathway and up the AV node (or theother way around), creating a small, rapidly conducting circuit which can causean impressive tachycardia. These would look for all the world, depending on the
4

PREEXCITATION 5
direction the arrhythmia took, like a supraventricular tachycardia or a ventric-ular tachycardia. Worse yet, patients with preexcitation are prone to developingatrial fibrillation which can be particularly rapid since the accessory pathwaymay not slow the impulses the way the normal AV node does.
HABITATThese can be found anywhere, but most are found accidentally when somebodyhas an ECG done for another reason.
CALL“Is Wolff–Parkinson–White a sausage company or a law firm?”
RESEMBLANCE TO OTHER ARRHYTHMIASIn sinus rhythm, preexcitation can be confused with sinus rhythm with a bundlebranch block. With preexcitation, the key is the short PR and the delta wave,with the terminal part of the QRS being narrow. During a tachycardia all betsare off; in atrial fibrillation your only clue to the presence of preexcitation maybe that it is particularly rapid, with a mix of narrow and wide beats, dependingon which pathway conducts the impulse. During other tachycardias it may bevery hard to tell if there is underlying preexcitation.
CARE AND FEEDINGIf the patient is in sinus rhythm, you don’t have to do anything except maybe makean appointment for him or her to see an electrophysiologist, since some of thesepatients are actually at risk for sudden death from their rhythm disturbances,especially rapid atrial fibrillation. If the patient is known to have preexcitationand is actually in a tachycardia, especially atrial fibrillation, like Siberian tigersor polar bears it is best left to the experts to care for. Many of the responsesto pharmacology are paradoxic; if there was an emergency and the patient wasunstable, probably the safest thing to do is just to cardiovert the rhythm back tosinus rhythm without getting sucked into the murk of odd drug reactions.

Sinus Bradycardia
DESCRIPTIONJust like sinus rhythm, but slower; it is defined as sinus rhythm (every QRSpreceded by a proper P wave) with a rate under 60.
HABITATBoring lectures, a Kenny G concert, inferior infarcts, sleep apnea, or too much�-blocker.
CALL“Why is everyone running into in my room and looking at me?”
RESEMBLANCE TO OTHER ARRHYTHMIASThis looks like sinus rhythm, only slower. When it’s really slow (rates into the30s) you might think it’s a junctional rhythm, but the presence of P waves withthe proper PR interval would indicate it’s definitely a sinus rhythm.
CARE AND FEEDINGProbably here more than anywhere else, it’s a question of “when in doubt, checkthe patient”! If the heart rate is 30 but the patient is fine, don’t do anything. If theheart rate is slow and the patient is dizzy or hypotensive, then intervene. Herea little atropine might help in the short term. Often withdrawal or reducing thedose of “slower-downers” (such as �-blockers, diltiazem, digoxin, verapamil, orsome antiarrhythmics) over time would allow the heart rate to increase. Shoutingor showing the patient his or her bill might help also, but if the heart rate stayslow and the patient is symptomatic, a pacemaker might be in order.
6