elevated expression of carcinoembryonic antigen-related cell adhesion molecule 1 (ceacam-1) is...
TRANSCRIPT

L
Ea(al
SCK
a
b
R
H
0d
ung Cancer (2008) 60, 426—433
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / lungcan
levated expression of carcinoembryonicntigen-related cell adhesion molecule 1CEACAM-1) is associated with increasedngiogenic potential in non-small-cellung cancer
ebastian Dangoa,1, Wulf Sienela,∗,1, Moritz Schreibera,hristian Stremmela, Andreas Kirschbauma,laus Pantelb, Bernward Passlicka
Department of Thoracic Surgery, Albert-Ludwigs-University Freiburg, 79106 Freiburg, GermanyInstitute of Tumor Biology, University Medical Center Hamburg-Eppendorf, 20246 Hamburg, Germany
eceived 29 June 2007; received in revised form 20 November 2007; accepted 29 November 2007
KEYWORDSCarcinoembryonicantigen-related celladhesion molecule;Non-small-cell lungcarcinoma;Microvessel density
Summary Recent studies have challenged the previously postulated concept of a tumor-suppressive effect of carcinoembryonic antigen-related cell adhesion molecule 1 (CEACAM-1).A possible angiogenic influence of CEACAM-1 in non-small-cell lung cancer (NSCLC) has not beeninvestigated so far. Therefore, we examined microvessel density (MVD) and CEACAM-1 expres-sion in primary NSCLC and analyzed their possible correlations under consideration of theirprognostic effects. Specimens from 82 consecutive patients with completely resected NSCLCwere stained immunohistochemically using the monoclonal anti-CEACAM-1 antibody 4D1/C2 andthe monoclonal anti-CD31 antibody JC70A. The prognostic relevance of CEACAM-1 expressionand MVD was evaluated by univariate Kaplan—Meier and multivariate Cox regression analy-
sis. The median follow-up period was 75 months (range 10—156 months). A high MVD (i.e.,≥31 microvessels/400× microscopic field) was observed more frequently in tumors with highCEACAM-1 expression (i.e., ≥66% stained tumor cells) than in tumors with low CEACAM-1 expres-sion (61.8% vs. 33.3%, respectively; p = 0.01). In univariate survival analyses, high CEACAM-1expression and high MVD were associated with development of distant metastasis (p = 0.011 and0.022, respectively) and decreased cancer-related survival (p = 0.046 and 0.006, respectively).Multivariate Cox regression analysis demonstrated that the prognostic impact of CEACAM-1∗ Corresponding author at: Department of Thoracic Surgery, University Hospital Freiburg, Albert-Ludwigs-University Freiburg,ugstetter Strasse 55, 79106 Freiburg, Germany. Tel.: +49 761 2702457; fax: +49 761 2702499.
E-mail address: [email protected] (W. Sienel).1 The authorship is shared equally by these authors, and their names are listed in alphabetical order.
169-5002/$ — see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.lungcan.2007.11.015

Elevated expression of CEACAM-1 427
depended on the prognostic influence of MVD, while MVD itself represented an independentprognosticator for unfavorable cancer-related survival (p = 0.021; relative risk 2.1; 95% confidenceinterval, 1.1—4.0). Here we show for the first time that high CEACAM-1 expression is associatedwith an increased angiogenic activity in NSCLC, and that the prognostic influence of CEACAM-1
ssociAll ri
p(tImmpTrcrnrt
1iaadtd
2t
MaaWbmCBsG2iaabbatnaAssociates Inc., Birmingham, USA). Immunohistochemicalstaining was continued by incubating the slides with biotiny-
might be derived from this a© 2007 Elsevier Ireland Ltd.
1. Introduction
Lung cancer remains the most common cause of cancer-related death in Europe and in the United States [1].Non-small-cell lung cancer (NSCLC) affects approximately80% of all lung cancer patients [2]. The 5-year survival forearly stage NSCLC is only 50—60% in stages I and II [3].Patients with the same stage of disease have markedly dif-ferent rates of disease progression. Thus, there is an urgentneed for a better understanding of the molecular mech-anisms of lung cancer progression to reveal new optionsaccording to diagnosis, prediction of survival or selection oftherapy in order to enable a more personalized lung cancertreatment.
Cell adhesions play a key role in tumor invasion andmetastasis [4]. A number of adhesion molecules belongto the immunoglobulin superfamily [5]. One interestingmember of the immunoglobulin superfamily is the car-cinoembryonic antigen-related cell adhesion molecule 1(CEACAM-1), formerly known as biliary glycoprotein I orCD66a [6]. CEACAM-1 is the major antigen of the CD66 clus-ter of granulocyte differentiation antigens. It is expressed inepithelium, endothelium, and myeloid cells in a wide rangeof normal human tissues [7]. Previously, CEACAM-1 expres-sion was analyzed in various malignant epithelial tumors,such as colon [8] and prostate carcinoma [9] as well as ade-nocarcinoma of the lung [10] and malignant melanoma [11].Different functions were described for CEACAM-1 in thosetumors. Recently, it has been shown that high CEACAM-1expression is associated with an unfavorable outcome inadenocarcinoma of the lung [10] and in advanced stagesof all kind of NSCLC histologies [12]. Since larger tumorsmay particularly depend on angiogenesis [13], one expla-nation for the prognostic effect of CEACAM-1 in advancedNSCLC could be an angiogenic effect of CEACAM-1 that hasbeen observed in vitro [14]. However, a possible angiogeniceffect of CEACAM-1 has not been examined in patients withNSCLC so far. Thus, we analyzed a possible angiogenic roleof CEACAM-1 by comparing microvessel density (MVD) andCEACAM-1 expression in primary NSCLC under considerationof their prognostic effects.
2. Patients and methods
2.1. Patients
The study was activated in January 1992 after approval bythe ethical committee of the University of Munich. Since
then, 82 patients who gave written informed consent weresubmitted to this study consecutively. The latest follow-up was updated in October 2005. Tumors were classifiedaccording to the international union against cancer (UICC)TNM-classification [15]. The preoperative staging of alll(fpe
ation.ghts reserved.
atients had resulted in the diagnosis of resectable tumorsT1—T4) without evident distant metastasis (M1) or con-ralateral or supraclavicular lymph node involvement (N3).n general, a lobectomy or pneumonectomy with systematicediastinal lymphadenectomy was performed in the Depart-ent of Thoracic Surgery. Only patients with confirmedostoperative R0 stage were eligible for further evaluations.he median age at the time of surgery was 60 years with aange of 37—80 years. Patients whose primary tumors werelassified as pT3 or pT4 received adjuvant percutaneousadiotherapy of the tumor bed and patients with mediasti-al lymph node involvement (pN2) received percutaneousadiotherapy of the entire mediastinum. Systemic adjuvantherapy was not performed.
The median follow-up duration was 75 months (range0—156 months). Follow-up studies included physical exam-nation, chest X-ray and blood tests in a 3-month intervalnd an additional thoracic CT scan, abdominal ultrasoundnd bronchoscopy in a 6-month interval. Close follow-up wasocumented by contacting family practitioners with ques-ionnaires concerning local relapse, distant metastasis andeath.
.2. Immunohistochemical staining of primaryumors
VD was analyzed by immunohistochemical staining usingn avidine—biotin technique with the monoclonal anti-CD31ntibody JC70A (DAKO Cytomation, Hamburg, Germany).e used an anti-CD31 antibody for microvessel stainingecause the first international consensus statement on theethods for assessment of angiogenesis suggested that anti-D31 antibodies might be superior on paraffin sections [16].riefly, paraffin sections were dewaxed, rehydrated and sub-equently incubated with proteinase K (Sigma, Taufkirchen,ermany) at a final concentration of 0.05% for 10 min at5 ◦C. Endogenous peroxidase activity was blocked by treat-ng the specimens with 3% periodate solution. Non-specificntibody binding was prevented with avidine—biotin serumt a final concentration of 1% for 10 min at 25 ◦C. Excesslocking agent was drained, and the sections were incu-ated overnight at 25 ◦C with the primary monoclonal mousenti-human CD-31 antibody. The antibody was used at a dilu-ion of 1:50 in phosphate buffered saline (PBS). For theegative controls the primary antibody was replaced withnon-immune rabbit IgG antibody (Southern Biotechnology
ated peroxidase mouse IgG secondary antibody solutionABC-Kit Vectastatin, Vector Laboratories, Burlingame, USA)or 1 h at 25 ◦C. Peroxidase was introduced using an AB Com-lex (Biotest, Berlin, Germany) for 30 min at 25 ◦C. Betweenach step of the procedure the specimens were thoroughly

4
rvoatem
wfi(wbCbwttaksv
2C
IicevaioasoaeTtlncm
iotowsiitcgcssc
dcatatnabo
2
SscPyuwwservtwpT
3
3
NsircuioIaoPtdei(t
3
M
28
insed with PBS buffer pH 6.8. Peroxidase reactivity wasisualized using aminoethyl carbazole (AEC) (Zymed Lab-ratories, South San Francisco, USA) for 20 min creatingred-brown staining with 30% hydrogen peroxide. Finally,
he sections were counterstained with haemalaun (May-rs Haemalaun solution, Merck, Hamburg, Germany) andounted in Kaiser’s glycerol gelatine (Merck).Immunohistochemical analysis of CEACAM-1 expression
as performed as described previously [12]. Briefly, paraf-n sections were dewaxed and incubated with PronaseSigma). The sections were incubated overnight at 25 ◦Cith the monoclonal CEACAM-1 antibody 4D1/C2. The anti-ody was kindly provided by C. Wagener (Institute of Clinicalhemistry, University Hospital Hamburg-Eppendorf, Ham-urg, Germany). The antibody is produced continuously andill be provide to the scientific community upon request
o C. Wagener. 4D1/C2 was used at a final concentra-ion of 1 �g/ml. Subsequent to incubation with biotinylatednti-mouse/anti-rabbit secondary antibody solution (LSAB-it, DAKO Cytomation), peroxidase was introduced using atreptavidine conjugate (LSAB-kit, DAKO Cytomation) andisualized using aminoethyl carbazole (AEC) (Sigma).
.3. Assessment of microvessel density andEACAM-1 expression
mmunohistochemical reactions for CD-31 were examinedndependently by two observers who were unaware of thelinical data. The slides with discrepant evaluations were re-valuated and a consensus was reached (n = 4). The two mostascularized areas within tumors (hot spots) were chosent low magnification (25×) and microvessels were countedn a representative high magnification (400×) field in eachf these two areas as described previously by Weidner etl. [16,17]. The MVD was the mean of countable microves-el in these two areas. Any brown stained endothelial cellr endothelial cell cluster that was clearly separate fromdjacent vessels, tumor cells, and other connective tissuelements was considered a single countable microvessel.he presence of vessel lumens was not necessary for a struc-ure to be defined as a vessel [16]. Endothelial staining inarge vessels with tunica media, and non-specific staining ofon-endothelial structures were disregarded in microvesselounts. MVD was divided into two groups according to theedian as suggested previously [16].Immunohistochemical CEACAM-1 staining was also exam-
ned by two independent observers who were unawaref the clinical data. CEACAM-1 staining was assessed inhe same tumor areas which were chosen for analysisf MVD. Discrepant evaluations occurred six times andere re-evaluated and a consensus was reached. The
lides were examined at 200× magnification. CEACAM-1mmunoreactivity of tumor cells was compared to themmunoreactivity of normal lung tissue and granulocytes inhe sections. CEACAM-1 is the major antigen of the CD66luster of granulocyte differentiation antigens. Therefore,
ranulocytes are suitable to serve as an internal positiveontrol of CEACAM-1 immunoreactivity. CEACAM-1 expres-ion rate was categorized according to the percentage oftained tumor cells into ‘‘low’’ (i.e., <66% positive tumorells) and ‘‘high’’ (i.e., ≥66% positive tumor cells) asleivs
S. Dango et al.
escribed previously [12]. The method for choosing theut-point for differentiation between patients at high-nd low-risk based on previous results and knowledge ofhe measurement technique [12]. Staining specificity wasssessed by evaluation of the negative controls in whichhe primary antibody had been replaced with normal rabbiton-immune IgG. Staining intensity was not consideredparameter for the assessment of CEACAM-1 expression
ecause staining intensity varied between different batchesf immunohistochemical staining.
.4. Statistical analyses
tatistical analysis was performed using SPSS software Ver-ion 14.0 for PC (SPSS Inc., Chicago). All variables wereompared statistically using cross-tables and two-tailedearson’s Chi-square test or Fisher’s exact test. For anal-sis of follow-up data, life table curves were calculatedsing the Kaplan—Meier method and survival distributionsere compared by log-rank statistics. The primary end pointas cancer-related death, as measured from the date of
urgery to death. Data of patients who were still alive at thend of the study were censored. Joint effects with alreadyecognized prognostically relevant variables were examinedia Cox proportional hazards analysis: pT-status, pN-status,umor histology and patient age were entered stepwise for-ard into the model to test these covariables for possiblerognostic joint effects with MVD and CEACAM-1 expression.he threshold for statistical significance was p < 0.05.
. Results
.1. CEACAM-1 expression of primary tumors
ormal lung tissue, normal bronchiolar epithelium andtromal cells of all sections exhibited no CEACAM-1mmunostaining. The staining intensity of tumor cellsanged between no staining and high staining intensityomparable to the immunoreactivity of granulocytes. Gran-locytes served as an internal positive control for CEACAM-1mmunoreactivity because CEACAM-1 is the major antigenf the CD66 cluster of granulocyte differentiation antigens.mmunohistochemically stained granulocytes were found onll CEACAM-1 negative tumors. Therefore, the possibilityf false-negative results could be excluded for all slides.rimary tumors were divided into two groups according tohe number of stained tumor cells in the tumor center asescribed previously [12]. Tumors of 48 patients (58.5%)xhibited a low CEACAM-1 expression rate (i.e., <66% pos-tive tumor cells) (Fig. 1A) and specimens of 34 patients41.5%) showed a high expression rate (i.e., ≥66% positiveumor cells) (Fig. 1B) (Table 1).
.2. Microvessel density of primary tumors
VD was quantified using CD-31 as a marker for vascu-
ar endothelium (Fig. 1C and D). The staining intensity ofndothelial cells ranged between no staining and high stain-ng intensity comparable to the immunoreactivity of largeressels with tunica media. The median MVD was 31 microves-els per 400× magnification field (range 4—75). The MVD
Elevated expression of CEACAM-1 429
Fig. 1 Immunohistochemical staining of CEACAM-1 and of microvessels in primary NSCLC. (A) The tumor shown here was judgedto express CEACAM-1 at a low level (i.e., positive staining in <66% tumor cells). (B) This tumor shows positive staining in ≥66% tumor
EACAtum
3s
T14oapoMtt1(Naa
cells and was classified as exhibiting a high expression rate of Ca low MVD (<31 microvessels/400× microscopic field). (D) Thisfield).
was divided into two groups according to the median assuggested previously [16]. Tumors of 45 patients (54.9%)exhibited a low MVD (i.e., <31 microvessels/400× micro-scopic field) (Fig. 1C) and specimens of 37 patients (45.1%)showed a high MVD (i.e., ≥ 31 microvessels/400× micro-scopic field) (Fig. 1D) (Table 1).
A high MVD was observed more frequently in tumors withhigh CEACAM-1 expression than in tumors with low CEACAM-1 expression (61.8% vs. 33.3%, respectively; p = 0.01, Chi-square test; Table 2).
3.3. Correlation with clinicopathologicalparameters
Counter to one’s expectations neither MVD nor CEACAM-1 expression level was associated with the presence oflymph node metastasis, tumor extension or tumor grad-ing (Table 1). Furthermore, there was no correlation withpatient sex or age (Table 1). Interestingly, high CEACAM-1
expression was more frequently observed in adenocarci-noma of the lung (56%) and in miscellaneous histologies (46%)comprising of large cell carcinomas and mixed histologiesthan in squamous carcinomas (27%) (p = 0.046; Chi-squaretest).CycC(
M-1 protein. (C) The tumor shown here was judged to containor exhibited a high MVD (≥31 microvessels/400× microscopic
.4. Correlation with recurrence, metastasis andurvival
he median follow-up duration was 75 months (range0—156 months). Within the observation period a total of3 patients (52%) developed a relapse. Local recurrenceccurred in 12 patients, distant metastasis in 12 patientsnd both local recurrence and distant metastasis in 19atients. Kaplan—Meier analyses of local recurrence andccurrence of distant metastases demonstrated that highVD and high CEACAM-1 expression were associated with dis-
ant metastasis (p = 0.022 and 0.011, respectively; log-rankest) (Table 3). However, no influence of MVD and CEACAM-expression concerning local recurrence became apparent
p = 0.06 and 0.74, respectively; log-rank test) (Table 3).evertheless, high MVD and high CEACAM-1 expression weressociated with a shortened relapse-free survival (p = 0.006nd 0.05, respectively; log-rank test) (Table 3).
All patients with relapse died of cancer-related causes.
omparable with relapse-free survival, Kaplan—Meier anal-sis of cancer-related survival demonstrated a decreasedancer-related survival in patients with high MVD or highEACAM-1 (p = 0.006 and 0.046, respectively; log-rank test)Figs. 2 and 3). In detail, cancer-related death was observed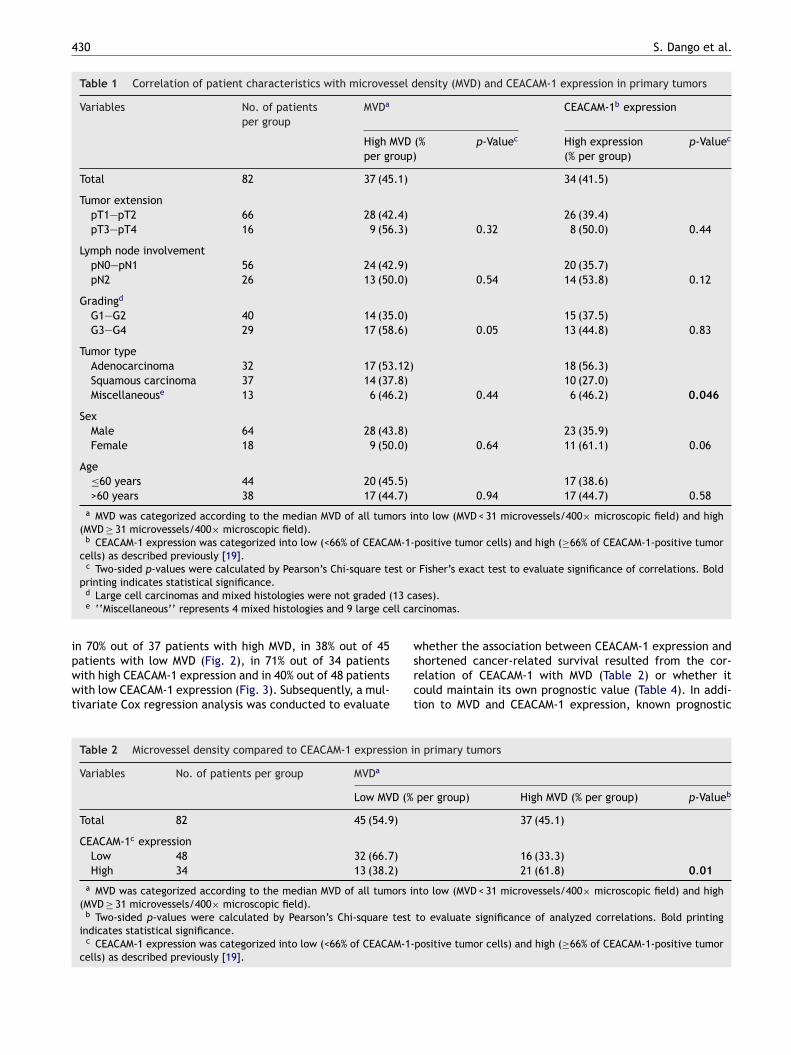
430 S. Dango et al.
Table 1 Correlation of patient characteristics with microvessel density (MVD) and CEACAM-1 expression in primary tumors
Variables No. of patientsper group
MVDa CEACAM-1b expression
High MVD (%per group)
p-Valuec High expression(% per group)
p-Valuec
Total 82 37 (45.1) 34 (41.5)
Tumor extensionpT1—pT2 66 28 (42.4) 26 (39.4)pT3—pT4 16 9 (56.3) 0.32 8 (50.0) 0.44
Lymph node involvementpN0—pN1 56 24 (42.9) 20 (35.7)pN2 26 13 (50.0) 0.54 14 (53.8) 0.12
Gradingd
G1—G2 40 14 (35.0) 15 (37.5)G3—G4 29 17 (58.6) 0.05 13 (44.8) 0.83
Tumor typeAdenocarcinoma 32 17 (53.12) 18 (56.3)Squamous carcinoma 37 14 (37.8) 10 (27.0)Miscellaneouse 13 6 (46.2) 0.44 6 (46.2) 0.046
SexMale 64 28 (43.8) 23 (35.9)Female 18 9 (50.0) 0.64 11 (61.1) 0.06
Age≤60 years 44 20 (45.5) 17 (38.6)>60 years 38 17 (44.7) 0.94 17 (44.7) 0.58
a MVD was categorized according to the median MVD of all tumors into low (MVD < 31 microvessels/400× microscopic field) and high(MVD ≥ 31 microvessels/400× microscopic field).
b CEACAM-1 expression was categorized into low (<66% of CEACAM-1-positive tumor cells) and high (≥66% of CEACAM-1-positive tumorcells) as described previously [19].
c Two-sided p-values were calculated by Pearson’s Chi-square test or Fisher’s exact test to evaluate significance of correlations. Bold
13 call ca
ipwwt
printing indicates statistical significance.d Large cell carcinomas and mixed histologies were not graded (e ‘‘Miscellaneous’’ represents 4 mixed histologies and 9 large ce
n 70% out of 37 patients with high MVD, in 38% out of 45atients with low MVD (Fig. 2), in 71% out of 34 patientsith high CEACAM-1 expression and in 40% out of 48 patientsith low CEACAM-1 expression (Fig. 3). Subsequently, a mul-
ivariate Cox regression analysis was conducted to evaluate
wsrct
Table 2 Microvessel density compared to CEACAM-1 expression i
Variables No. of patients per group MVDa
Low MVD (%
Total 82 45 (54.9)
CEACAM-1c expressionLow 48 32 (66.7)High 34 13 (38.2)
a MVD was categorized according to the median MVD of all tumors in(MVD ≥ 31 microvessels/400× microscopic field).
b Two-sided p-values were calculated by Pearson’s Chi-square testindicates statistical significance.
c CEACAM-1 expression was categorized into low (<66% of CEACAM-1-cells) as described previously [19].
ses).rcinomas.
hether the association between CEACAM-1 expression andhortened cancer-related survival resulted from the cor-elation of CEACAM-1 with MVD (Table 2) or whether itould maintain its own prognostic value (Table 4). In addi-ion to MVD and CEACAM-1 expression, known prognostic
n primary tumors
per group) High MVD (% per group) p-Valueb
37 (45.1)
16 (33.3)21 (61.8) 0.01
to low (MVD < 31 microvessels/400× microscopic field) and high
to evaluate significance of analyzed correlations. Bold printing
positive tumor cells) and high (≥66% of CEACAM-1-positive tumor

Elevated expression of CEACAM-1 431
Table 3 Correlation of microvessel density (MVD) and CEACAM-1 expression with local recurrence, metastasis, relapse-freesurvival and cancer-related survival
Local recurrencep-valuea
Distant metastasisp-valuea
Relapse-freesurvival p-valuea
Cancer-relatedsurvival p-valuea
MVDb 0.060 0.022 0.006 0.006CEACAM-1c expression 0.740 0.011 0.050 0.046
a p-Values of follow-up analyses were determined by log-rank test. Bold printing indicates statistical significance.b MVD was categorized according to the median MVD of all tumors into low (MVD < 31 microvessels/400× microscopic field) and high
(MVD ≥ 31 microvessels/400× microscopic field).c CEACAM-1 expression was categorized into low (<66% of CEACAM-1-positive tumor cells) and high (≥66% of CEACAM-1-positive tumor
cells) as described previously [19].
parameters such as tumor extension, lymph-node involve-ment, tumor histology and patient age at the time ofoperation were tested for possible prognostic joint-effects.This multivariate regression analysis demonstrated that theprognostic impact of CEACAM-1 depended on the prognosticinfluence of MVD because the significance of the prognosticeffect of CEACAM-1 expression observed by univariate anal-ysis disappeared when CEACAM-1 expression was enteredtogether with MVD into multivariate analysis, while MVDitself remained a significant prognosticator for unfavor-able cancer-related survival (p = 0.021). The relative risk forcancer-related death was 2.1-fold increase in the case ofhigh MVD (95% confidence interval, 1.1—4.0).
4. Discussion
Here we show for the first time that high CEACAM-1 expres-sion is associated with angiogenesis measured as MVD andthat the prognostic influence of CEACAM-1 might be derivedfrom this association. Previously, it has been observed thatadenocarcinoma of the lung [10] and also advanced stagesof all kind of NSCLC histologies [12] are associated with poor
Fig. 2 Kaplan—Meier curves of cancer-related survival inpatients with high MVD compared to patients with low MVD.High MVD was associated with a significant unfavorable outcome(p = 0.006; log-rank test).
survival in case of high CEACAM-1 expression. One possibleexplanation for this prognostic effect of CEACAM-1 could bean angiogenic effect of CEACAM-1 that has been observedin vitro [14]. An angiogenic property of CEACAM-1 had beendescribed in cultured human microvascular endothelial cells[14], but not in primary NSCLC so far. In detail, it hasbeen reported that CEACAM-1 is expressed in microves-sels of proliferating tissues such as endometrium, healingwounds, and solid tumors [14,7]. In microvascular humanendothelial cells, purified native and recombinant CEACAM-1 stimulated proliferation, chemotaxis, and tube formation[14]. Furthermore, it has been shown that the angiogeniceffects of CEACAM-1 are additive to those of the VEGF: Theexpression of CEACAM-1 has been up-regulated by VEGF, andVEGF-induced in vitro tube formation has been completelyblocked by a monoclonal anti-CEACAM-1 antibody [14].
Since high CEACAM-1 expression was significantly associ-ated with a high MVD (p = 0.01), the present work suggeststhat CEACAM-1 might exhibit its tumor-promoting effect[10,12] by induction of angiogenesis. Further research isrequired to clarify how CEACAM-1 expression by tumor cellsmay contribute to formation of new microvessels. One possi-
Fig. 3 Cumulative cancer-related survival of patients with ahigh CEACAM-1 expression compared to patients showing a lowCEACAM-1 expression. High-CEACAM-1 expression was associ-ated with a significant unfavorable outcome (p = 0.046; log-ranktest).

432 S. Dango et al.
Table 4 Univariate and multivariate analysis of cancer-related survival (n = 82)
Risk factor Univariate analysis p-valuea Multivariate analysisb
Relative risk (95% CI) p-Value
MVD low vs. highc 0.006 2.1 (1.1—4.0) 0.021CEACAM-1 expression low vs. highd 0.046 —e 0.44f
pT1-2 vs. pT3-4 0.063 2.4 (1.1—5.1) 0.029pN0-1 vs. pN2 0.049 2.5 (1.3—4.9) 0.007Adenocarcinoma vs. squamous cell
carcinoma vs. miscellaneous0.99 —e 0.72
≤60 years vs. >60 years 0.006 2.4 (1.3—4.4) 0.008a p-Values of univariate analyses were determined by log-rank test. Bold printing indicates statistical significance.b Stepwise multivariate analysis was performed using the Cox proportional-hazard model.c MVD was categorized according to the median MVD of all tumors into low (MVD < 31 microvessels/400× microscopic field) and high
(MVD ≥ 31 microvessels/400× microscopic field).d CEACAM-1 expression was categorized into low (<66% of CEACAM-1-positive tumor cells) and high (≥66% of CEACAM-1-positive tumor
cells) as described previously [19].e No estimate of relative risk is given, since the variable was not significant on multivariate analysis.f tic in
rednost
bi-wIa
crtpmmff[aosamrotpcenwmoamTiait
poi
taf(CCwowttap
mahtnecaoCetid
The prognostic impact of CEACAM-1 depended on the prognosof CEACAM-1 expression observed by univariate analysis disappeamultivariate analysis, while MVD itself remained a significant prog
le mechanism might be that CEACAM-1 expression leads toncreased expression of angiogenic factors like VEGF-A, -B,C and Ang2. These factors have been shown to be increasedhen CEACAM-1 is down-regulated in prostate cancer [18].
n contrast to lung cancer, prostate cancer is associated withpoorer prognosis when CEACAM-1 is down-regulated [9].The prognostic impact of MVD in operable NSCLC is dis-
ussed controversially and remains unclear. Some previouseports investigating angiogenesis by anti-CD31 immunos-aining of primary tumors demonstrated an association withoor outcome in NSCLC [19—21]. Furthermore, a recenteta-analysis of Meert et al. revealed that a high MVD in pri-ary tumors of NSCLC is a statistically significant prognostic
actor for poorer survival independent of the antibodies usedor microvessel visualization (anti-factor VIII, CD34 or CD31)22]. However, a more recent meta-analysis of Trivella etl. showed only weak evidence that high MVD is a markerf poor survival in operable NSCLC [23]. In this latter analy-is, MVD was only of prognostic significance when analyzeds a continuous variable and measured with the Chalkleyethod [23]. Chalkley described a graticule to estimate a
elative area of vasculature. The graticule can be insertedn the microscope while focusing on a hot spot. Rotation ofhe graticule with its 25 random points so that the randomoints touch as many vessels as possible gives a theoreti-al maximum of 25 counted vessels per hot spot. Trivellat al. suggested that MVD should not be regarded a prog-ostic factor in NSCLC because its association with survivalas not consistent with studies that used the ‘‘all vesselsethod’’ firstly described by Weidner et al. [17]. In contrast,
ur data show that even with the ‘‘all vessels method’’, MVDnalyzed by anti-CD31 immunostaining of primary tumorsay have a significant prognostic impact in operable NSCLC.
hus, our study strengthens previous reports demonstrat-ng a prognostic impact of MVD assessment using anti-CD31ntibodies and the ‘‘all vessels method’’ [19,20]. However,t should be noted that the aim of the present study waso investigate a possible angiogenic effect of CEACAM-1 in
5
Ib
fluence of MVD because the significance of the prognostic effectwhen CEACAM-1 expression was entered together with MVD intoicator.
atients with NSCLC and that the level of evidence [24]f meta-analyses is higher than of individual cohort stud-es.
Kaplan—Meier analyses in the present study showedhat both, high MVD and high CEACAM-1 expression weressociated with distant metastasis, shortened relapse-ree survival and a decreased cancer-related survivalFigs. 2 and 3). To verify whether the prognostic impact ofEACAM-1 expression resulted from the association betweenEACAM-1 and MVD, a multivariate Cox regression analysisas conducted, demonstrating that the prognostic impactf CEACAM-1 depended on the prognostic influence of MVD,hile MVD itself represented an independent prognostica-
or for unfavorable cancer-related survival (p = 0.021). Thus,he results of the present work suggest for the first time thatn angiogenic effect of CEACAM-1 [14] could confer to therognostic effect of CEACAM-1.
Like the present study, two recent studies on malignantelanoma that revealed an increased metastatic relapse
nd tumor invasion in CEACAM-1 positive melanomas [11,25]ave challenged the previously postulated concept of aumor-suppressive effect of CEACAM-1 [8]. A possible expla-ation for observing a tumor-promoting effect of CEACAM-1xpression in malignant melanoma and NSCLC, but not inolorectal [8], breast [26] and prostate cancer [9] might betissue dependent restriction of the angiogenic potential
f CEACAM-1. However, a possible correlation of MVD withEACAM-1 has not been investigated in the latter tumorntities so far. Inhibition of CEACAM-1 might be a newherapeutic anti-angiogenic strategy in NSCLC. Previous clin-cal studies investigating angiogenesis inhibitors in NSCLCemonstrated encouraging anti-tumor activity [27,28].
. Conclusion
n summary, CEACAM-1 leads to poor prognosis in NSCLCy induction of angiogenesis, a mechanism that might be

[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Elevated expression of CEACAM-1
noteworthy in future NSCLC therapy. This study may pro-vide a rationale for the preselection of patients to beincluded in possible future trials investigating systemic anti-CEACAM-1 therapy alone or in combination with establishedanti-angiogenic or cytostatic therapies in NSCLC.
Conflict of interest
None.
Acknowledgements
We would like to thank C. Wagener (Institute of Clin-ical Chemistry, University Hospital Hamburg-Eppendorf,Hamburg, Germany), who kindly provided the monoclonalCEACAM-1 antibody 4D1/C2. We also gratefully acknowl-edge the technical assistance of Gabriele Mueller-Buscher.This work was supported by the Deutsche Forschungsgemein-schaft and Deutsche Krebshilfe, Germany.
References
[1] Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al.Cancer statistics, 2006. CA Cancer J Clin 2006;56:106—30.
[2] Wahbah M, Boroumand N, Castro C, el Zeky F, Eltorky M.Changing trends in the distribution of the histologic typesof lung cancer: a review of 4,439 cases. Ann Diagn Pathol2007;11:89—96.
[3] Winton T, Livingston R, Johnson D, Rigas J, Johnston M, ButtsC, et al. Vinorelbine plus cisplatin vs. observation in resectednon-small-cell lung cancer. N Engl J Med 2005;352:2589—97.
[4] Cavallaro U, Christofori G. Cell adhesion in tumor invasion andmetastasis: loss of the glue is not enough. Biochim Biophys Acta2001;1552:39—45.
[5] Rojas M, Fuks A, Stanners CP. Biliary glycoprotein, a mem-ber of the immunoglobulin supergene family, functions in vitroas a Ca2(+)-dependent intercellular adhesion molecule. CellGrowth Differ 1990;1:527—33.
[6] Beauchemin N, Draber P, Dveksler G, Gold P, Gray-OwenS, Grunert F, et al. Redefined nomenclature for mem-bers of the carcinoembryonic antigen family. Exp Cell Res1999;252:243—9.
[7] Prall F, Nollau P, Neumaier M, Haubeck HD, Drzeniek Z, Helm-chen U, et al. CD66a (BGP), an adhesion molecule of thecarcinoembryonic antigen family, is expressed in epithelium,endothelium, and myeloid cells in a wide range of normalhuman tissues. J Histochem Cytochem 1996;44:35—41.
[8] Neumaier M, Paululat S, Chan A, Matthaes P, Wagener C. Bil-iary glycoprotein, a potential human cell adhesion molecule,is down-regulated in colorectal carcinomas. Proc Natl Acad SciUSA 1993;90:10744—8.
[9] Luo W, Tapolsky M, Earley K, Wood CG, Wilson DR, LogothetisCJ, et al. Tumor-suppressive activity of CD66a in prostate can-cer. Cancer Gene Ther 1999;6:313—21.
[10] Laack E, Nikbakht H, Peters A, Kugler C, Jasiewicz Y, Edler L,et al. Expression of CEACAM1 in adenocarcinoma of the lung:a factor of independent prognostic significance. J Clin Oncol2002;20:4279—84.
[11] Thies A, Moll I, Berger J, Wagener C, Brummer J, Schulze HJ,
et al. CEACAM1 expression in cutaneous malignant melanomapredicts the development of metastatic disease. J Clin Oncol2002;20:2530—6.[12] Sienel W, Dango S, Woelfle U, Morresi-Hauf A, Wagener C,Brummer J, et al. Elevated expression of carcinoembryonic
433
antigen-related cell adhesion molecule 1 promotes progressionof non-small cell lung cancer. Clin Cancer Res 2003;9:2260—6.
13] Bergers G, Benjamin LE. Tumorigenesis and the angiogenicswitch. Nat Rev Cancer 2003;3:401—10.
14] Ergun S, Kilik N, Ziegeler G, Hansen A, Nollau P, Gotze J, et al.CEA-related cell adhesion molecule 1: a potent angiogenic fac-tor and a major effector of vascular endothelial growth factor.Mol Cell 2000;5:311—20.
15] Mountain CF. Revisions in the international system for staginglung cancer. Chest 1997;111:1710—7.
16] Vermeulen PB, Gasparini G, Fox SB, Toi M, Martin L, McCullochP, et al. Quantification of angiogenesis in solid human tumours:an international consensus on the methodology and criteria ofevaluation. Eur J Cancer 1996;32A:2474—84.
17] Weidner N, Folkman J, Pozza F, Bevilacqua P, Allred EN, MooreDH, et al. Tumor angiogenesis: a new significant and indepen-dent prognostic indicator in early-stage breast carcinoma. JNatl Cancer Inst 1992;84:1875—87.
18] Tilki D, Irmak S, Oliveira-Ferrer L, Hauschild J, Miethe K,Atakaya H, et al. CEA-related cell adhesion molecule-1 isinvolved in angiogenic switch in prostate cancer. Oncogene2006;25:4965—74.
19] O’Byrne KJ, Koukourakis MI, Giatromanolaki A, Cox G, Turley H,Steward WP, et al. Vascular endothelial growth factor, platelet-derived endothelial cell growth factor and angiogenesis in non-small-cell lung cancer. Br J Cancer 2000;82:1427—32.
20] Han H, Silverman JF, Santucci TS, Macherey RS, d’Amato TA,Tung MY, et al. Vascular endothelial growth factor expressionin stage I non-small cell lung cancer correlates with neoangio-genesis and a poor prognosis. Ann Surg Oncol 2001;8:72—9.
21] Apolinario RM, van d V, de Jong JS, Deville W, Ark-Otte J, Dinge-mans AM, et al. Prognostic value of the expression of p53,bcl-2, and bax oncoproteins, and neovascularization in patientswith radically resected non-small-cell lung cancer. J Clin Oncol1997;15:2456—66.
22] Meert AP, Paesmans M, Martin B, Delmotte P, Berghmans T,Verdebout JM, et al. The role of microvessel density on the sur-vival of patients with lung cancer: a systematic review of theliterature with meta-analysis. Br J Cancer 2002;87:694—701.
23] Trivella M, Pezzella F, Pastorino U, Harris AL, Altman DG.Microvessel density as a prognostic factor in non-small-cell lungcarcinoma: a meta-analysis of individual patient data. LancetOncol 2007;8:488—99.
24] Graham AJ, Gelfand G, McFadden SD, Grondin SC. Levels ofevidence and grades of recommendations in general thoracicsurgery. Can J Surg 2004;47:461—5.
25] Ebrahimnejad A, Streichert T, Nollau P, Horst AK, WagenerC, Bamberger AM, et al. CEACAM1 enhances invasion andmigration of melanocytic and melanoma cells. Am J Pathol2004;165:1781—7.
26] Bamberger AM, Kappes H, Methner C, Rieck G, Brummer J,Wagener C, et al. Expression of the adhesion molecule CEA-CAM1 (CD66a, BGP, C-CAM) in breast cancer is associated withthe expression of the tumor-suppressor genes Rb, Rb2, and p27.Virchows Arch 2002;440:139—44.
27] Johnson DH, Fehrenbacher L, Novotny WF, Herbst RS, Nemu-naitis JJ, Jablons DM, et al. Randomized phase II trialcomparing bevacizumab plus carboplatin and paclitaxel withcarboplatin and paclitaxel alone in previously untreated locallyadvanced or metastatic non-small-cell lung cancer. J Clin Oncol2004;22:2184—91.
28] Herbst RS, Johnson DH, Mininberg E, Carbone DP, HendersonT, Kim ES, et al. Phase I/II trial evaluating the anti-vascular
endothelial growth factor monoclonal antibody bevacizumabin combination with the HER-1/epidermal growth factorreceptor tyrosine kinase inhibitor erlotinib for patients withrecurrent non-small-cell lung cancer. J Clin Oncol 2005;23:2544—55.