electronic surveillance of healthcare-associated ... · electronic surveillance of...
TRANSCRIPT
Electronic Surveillance of Healthcare-Associated Infections – Is it worth it?
Walter Kollera, Alexander Blackya, Harald Mandlb, Klaus-Peter Adlassnigb,c
a Clinical Institute of Hospital Hygiene, Medical University of Vienna (MUV) and Vienna General Hospital (VGH), Austria
b Medexter Healthcare GmbH, Vienna, Austriac Section for Medical Expert and Knowledge-Based Systems, Center for
Medical Statistics, Informatics, and Intelligent Systems, MUV, Austria
SF2H Congress Lille, 6 June 2012
For good reasons, healthcare authorities demand installation and regular application of HAI surveillance as part of quality management in hospitals
Dilemma of conventional surveillance of HAIs: HAI surveillance is a time-consuming task for highly trained experts. Unavailability of a suitable workforce meets with increasing financial constraints
Challenge: Obtain reliable surveillance results without urging or relying on doctor‘s or nurse‘s sparse time resources for documentation of surveillance data
2SF2H Congress Lille, 6 June 2012 Koller
Background
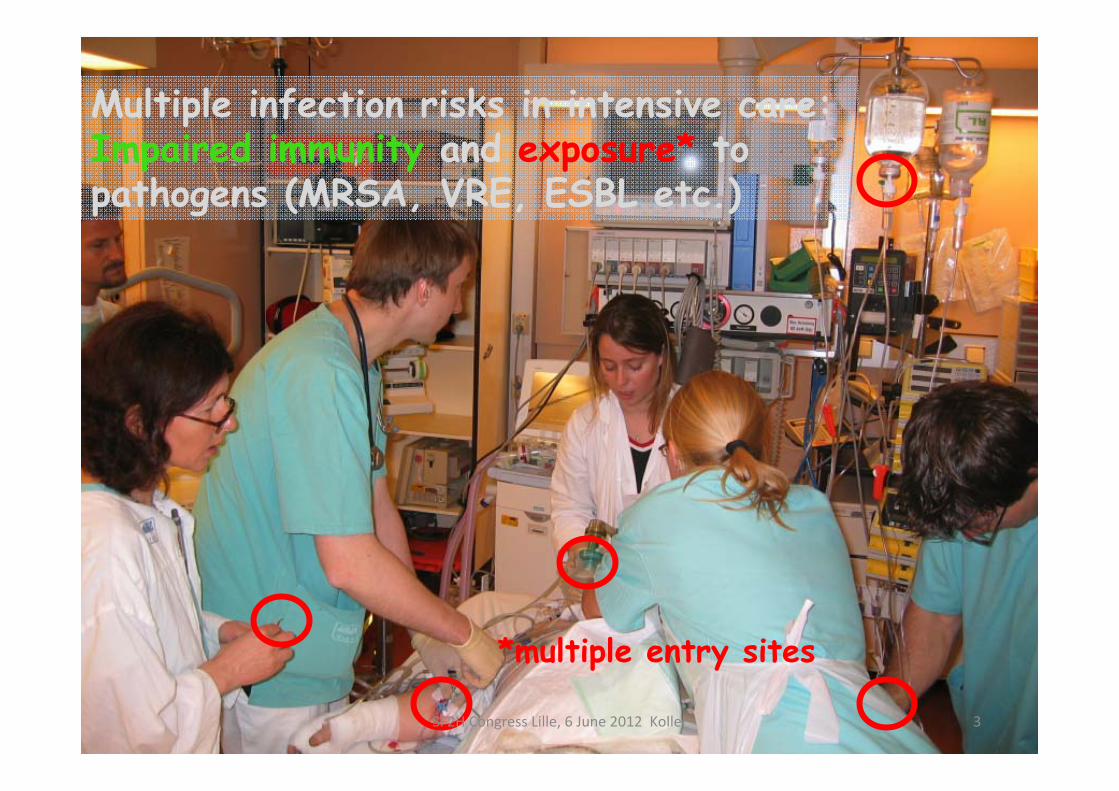
Multiple infection risks in intensive care: Impaired immunity and exposure* to pathogens (MRSA, VRE, ESBL etc.)
*multiple entry sites
3SF2H Congress Lille, 6 June 2012 Koller
Electronic patient data management systems (PDMS): • are installed and in use in many ICUs, • receive continuous automated input from monitoring
equipment (vital parameters) and from laboratories (incl. microbiology).
• ICU caregivers are familiar with documentation of patient-related clinical information into PDMS
PDMS hold structured clinical data relevant for infection surveillance
4SF2H Congress Lille, 6 June 2012 Koller
In ICUs specific features support IT-based HAI surveillance:
Develop and implement intelligent software which can extract and analyze HAI-related surveillance information from structured clinical data held in PDMS
5SF2H Congress Lille, 6 June 2012 Koller
Our target:
o Bridge the gap between international standard HAI case definitions and the clinicians perception of his/her actual “case” Reliability and accuracy in clinical terms and Timeliness of surveillance results
o Achieve full technical and organizational feasibility of IT surveillance
o Get indepenent from day to day data input of clinical specialists and documentation staff Reduce infection rates and costs by (almost) real-time
IT monitoring
(Our) main challenges when starting and propagating intelligent IT surveillance:
6SF2H Congress Lille, 6 June 2012 Koller
MONI-ICU
Knowledge-based recognition and automated monitoring of nosocomial infections for adult ICUs at
Medical University of Vienna and Vienna General Hospital
7SF2H Congress Lille, 6 June 2012 Koller
(1) Electronic data sources providing structured medical data; (2) Medical knowledge base with computerized knowledge about all relevant clinical entities; (3) Processing algorithm that evaluates, aggregates, and interprets medical data in a stepwise manner until it can be mapped into the given HAI definitions (ECDC/HELICS or NHSN*)
MONI-ICU components in terms of METHOD and PRACTICE
8SF2H Congress Lille, 6 June 2012 Koller
* NHSN = National Healthcare Safety Network, former NNIS of CDC, Atlanta, USA
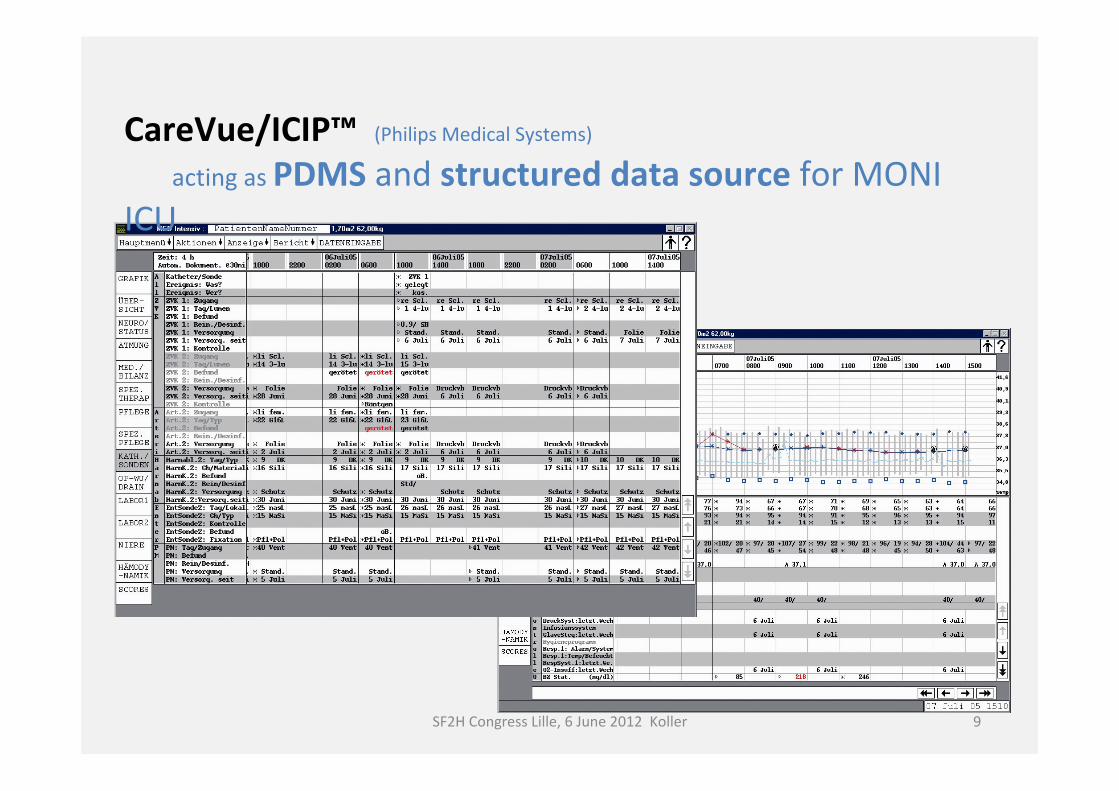
CareVue/ICIP™ (Philips Medical Systems)
acting as PDMS and structured data source for MONI ICU
9SF2H Congress Lille, 6 June 2012 Koller
o Clinical signs/symptoms (e.g., fever, chills, cough, rales, pain, …)
o Laboratory findings (e.g., elevated WBC-counts, elevated CRP)
o Microbiology findings
o Radiology findings (e.g., positive chest-RX)
Constituents of HAI case definitions
10SF2H Congress Lille, 6 June 2012 Koller
Medical Knowledge Base and data processing
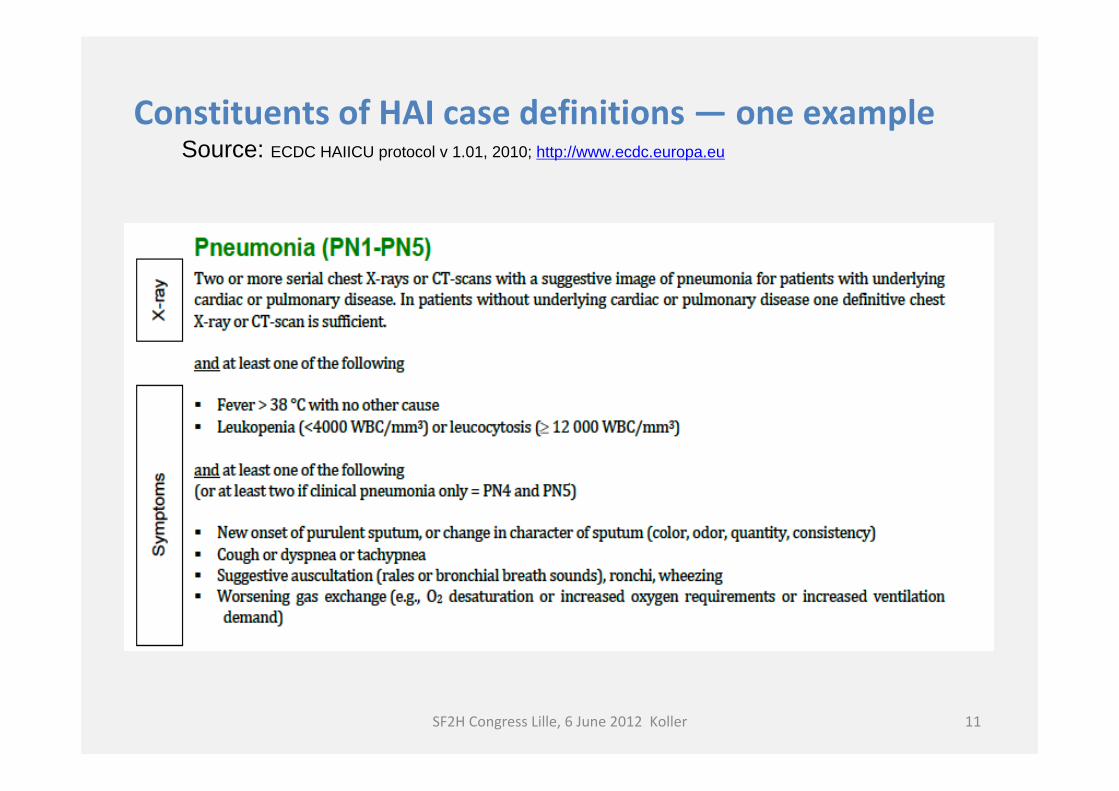
Constituents of HAI case definitions — one exampleSource: ECDC HAIICU protocol v 1.01, 2010; http://www.ecdc.europa.eu
11SF2H Congress Lille, 6 June 2012 Koller
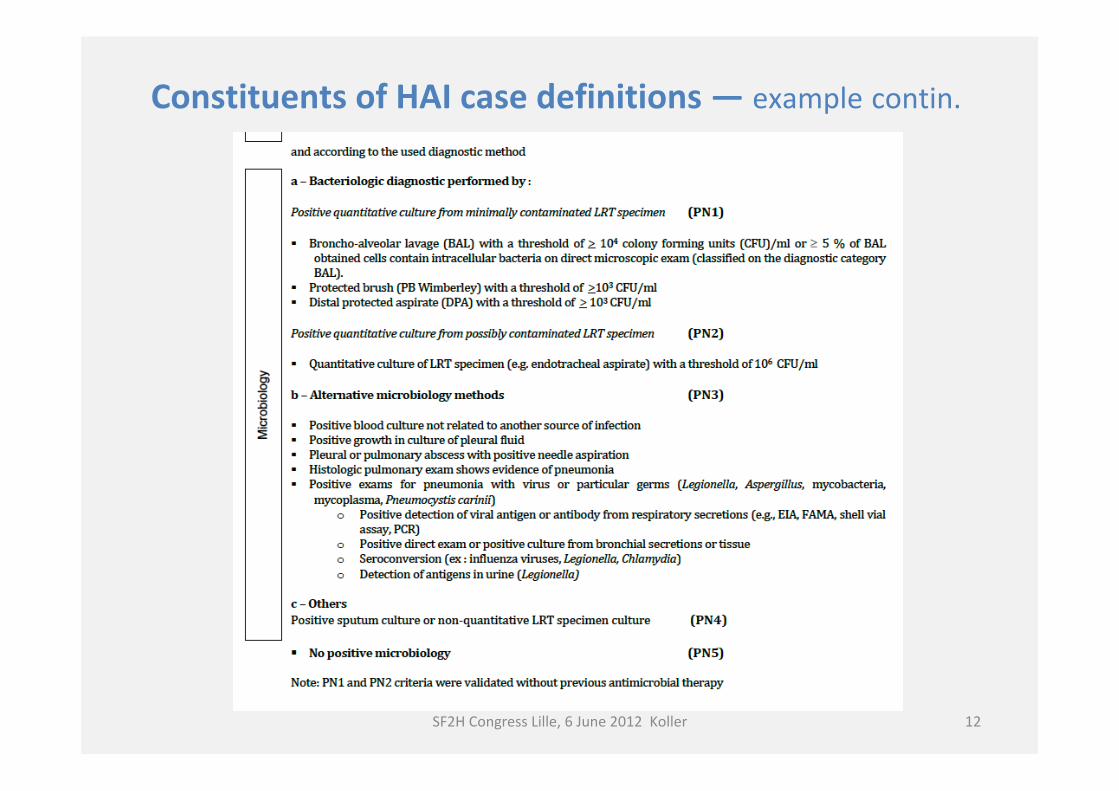
Constituents of HAI case definitions — example contin.
12SF2H Congress Lille, 6 June 2012 Koller
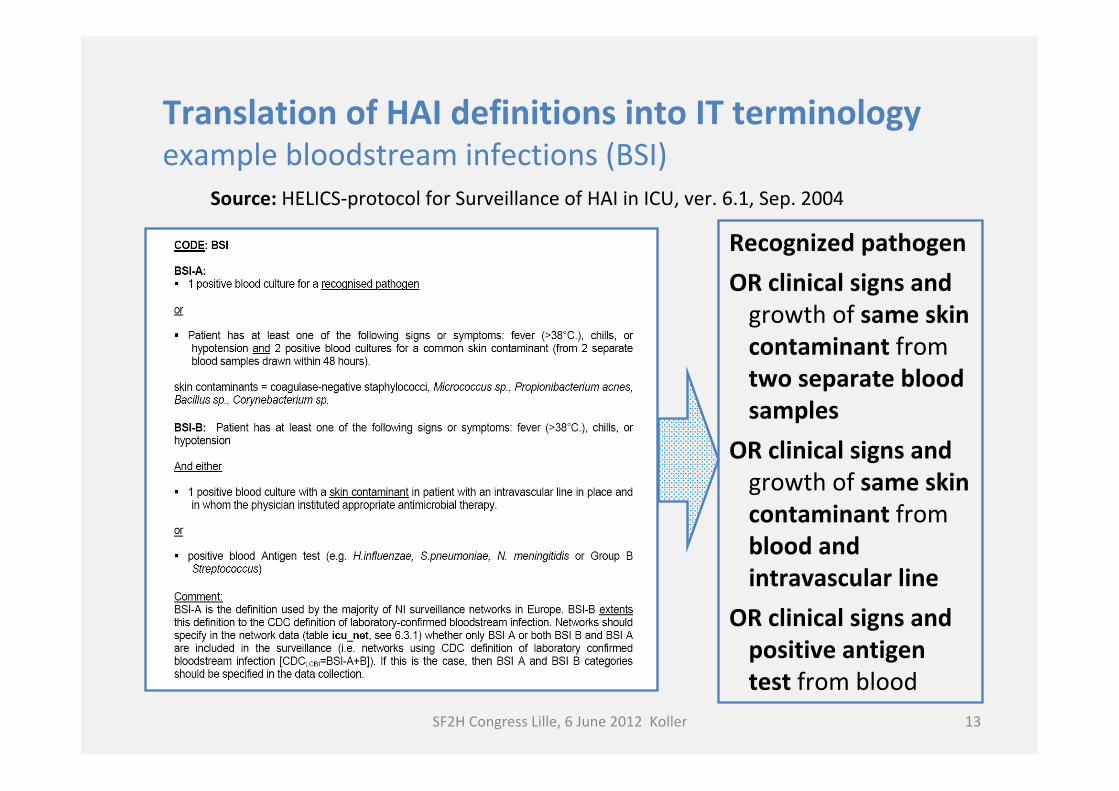
Translation of HAI definitions into IT terminologyexample bloodstream infections (BSI)
Source: HELICS-protocol for Surveillance of HAI in ICU, ver. 6.1, Sep. 2004
Recognized pathogenOR clinical signs and
growth of same skin contaminant from two separate blood samples
OR clinical signs and growth of same skin contaminant from blood and intravascular line
OR clinical signs and positive antigen test from blood
SF2H Congress Lille, 6 June 2012 Koller 13
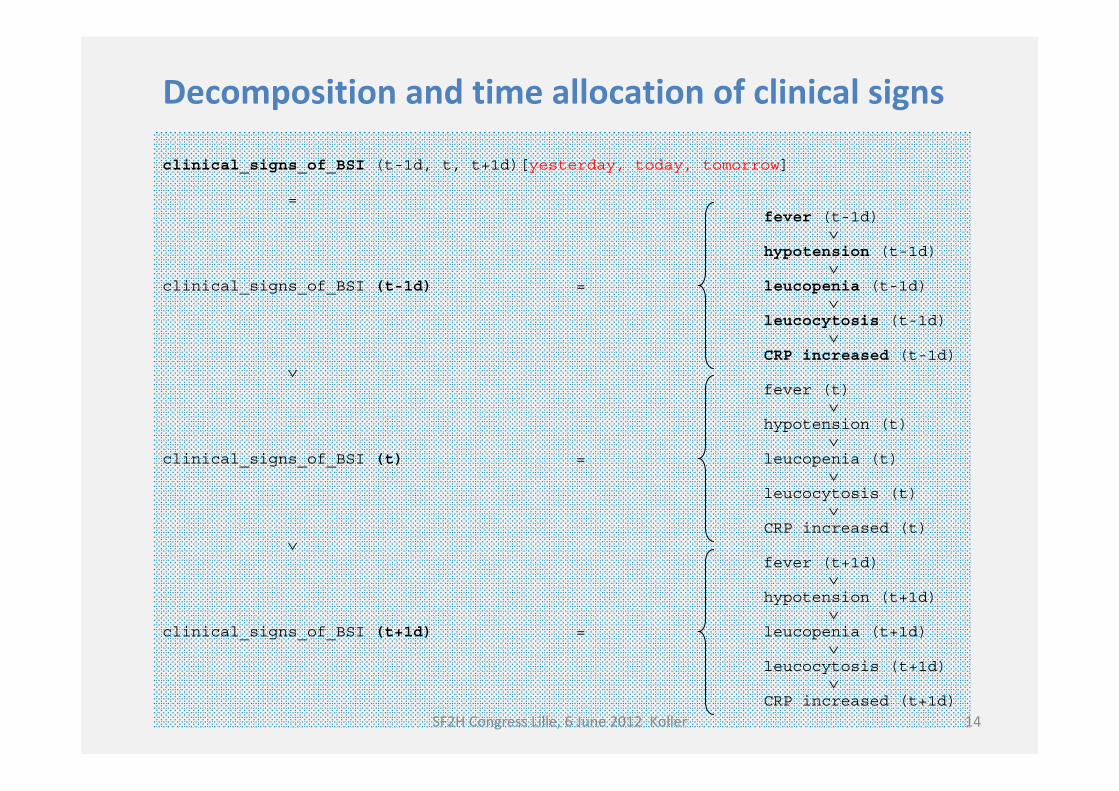
clinical_signs_of_BSI (t-1d, t, t+1d)[yesterday, today, tomorrow]
= fever (t-1d)
∨hypotension (t-1d)
∨clinical_signs_of_BSI (t-1d) = leucopenia (t-1d)
∨leucocytosis (t-1d)
∨CRP increased (t-1d)
∨fever (t)
∨hypotension (t)
∨clinical_signs_of_BSI (t) = leucopenia (t)
∨leucocytosis (t)
∨CRP increased (t)
∨fever (t+1d)
∨hypotension (t+1d)
∨clinical_signs_of_BSI (t+1d) = leucopenia (t+1d)
∨leucocytosis (t+1d)
∨CRP increased (t+1d)
Decomposition and time allocation of clinical signs
14SF2H Congress Lille, 6 June 2012 Koller
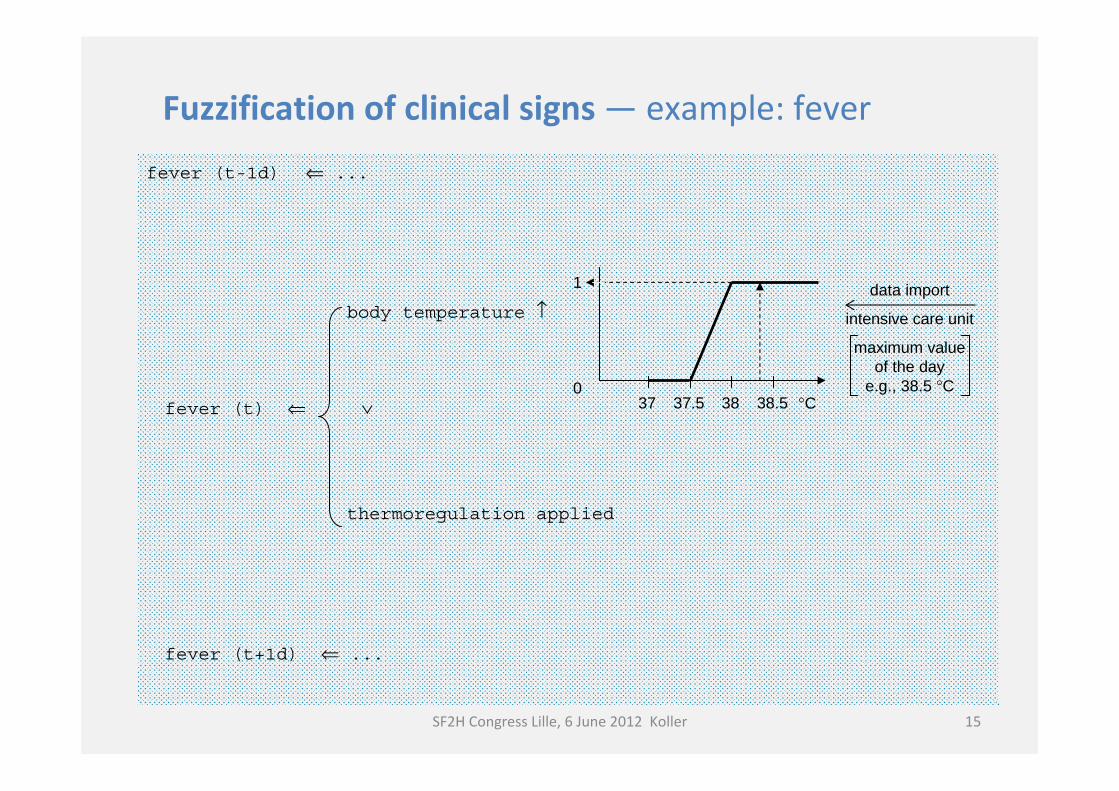
fever (t-1d) ⇐ ...
body temperature ↑
fever (t) ⇐ ∨
thermoregulation applied
fever (t+1d) ⇐ ...
data import
intensive care unit
maximum value of the day
e.g., 38.5 °C°C
1
037 37.5 38 38.5
Fuzzification of clinical signs — example: fever
15SF2H Congress Lille, 6 June 2012 Koller
a) Standard Reporting Tool: aggregates results in tables and graphs for periodic epidemiology reporting
b) Advanced Reporting Tool: Graphical user interfaces display daily “infection pattern” and allow for deep insight at the level of vital parameters and basic clinical indicators
c) Option: automated reminders (alerts) for HAI-related conditions may be installed
MONI-ICU components in terms of OUTPUT
16SF2H Congress Lille, 6 June 2012 Koller
Preformatted tables and graphs:− Overview of 12 ICUs for the Institute of Hospital
Hygiene− Separate report for each ICU
MONI-ICU data are exported into a specially designed EXCEL tool whichdisplays tables and graphs
a) MONI-ICU “standard” reporting
17SF2H Congress Lille, 6 June 2012 Koller
SF2H Congress Lille, 6 June 2012 Koller 18
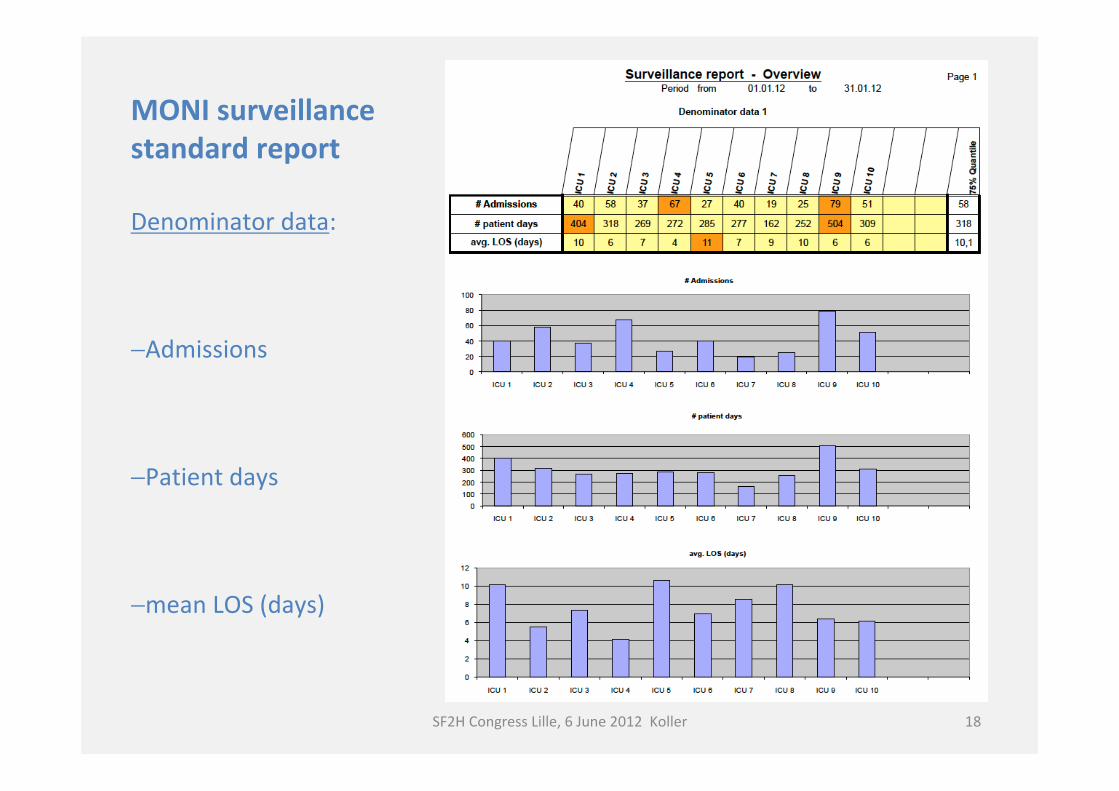
MONI surveillancestandard report
Denominator data:
−Admissions
−Patient days
−mean LOS (days)
SF2H Congress Lille, 6 June 2012 Koller 19
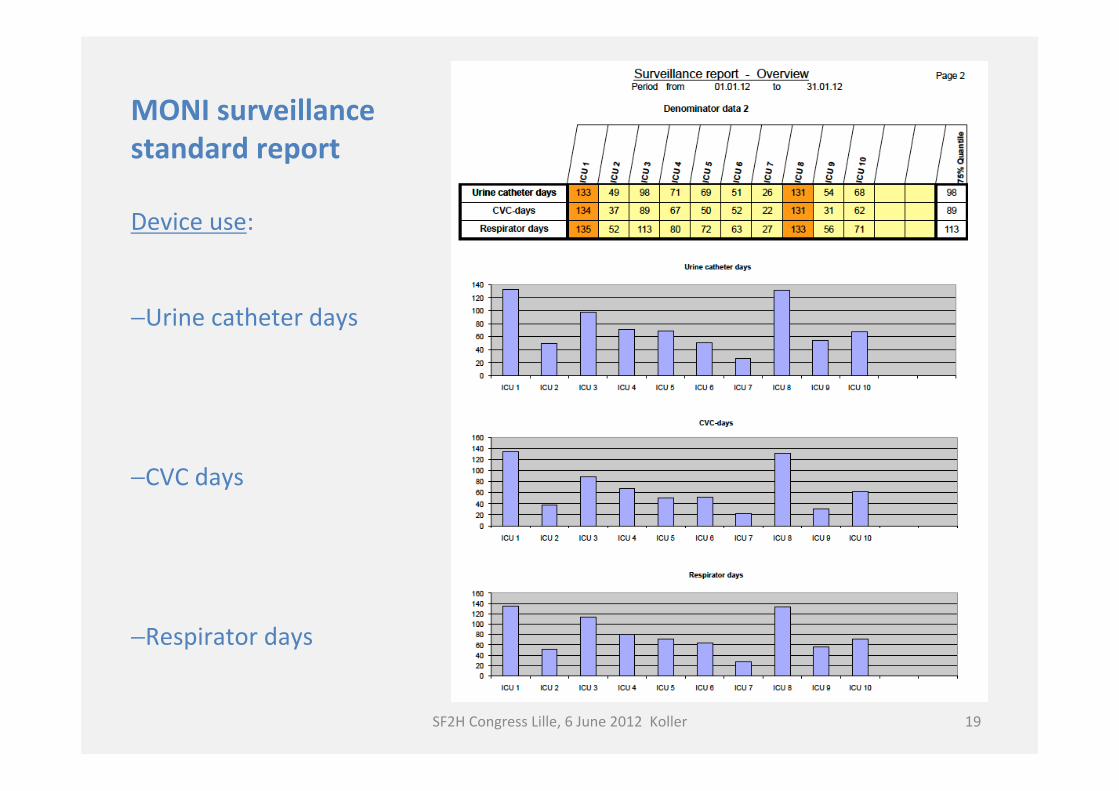
MONI surveillancestandard report
Device use:
−Urine catheter days
−CVC days
−Respirator days
SF2H Congress Lille, 6 June 2012 Koller 20
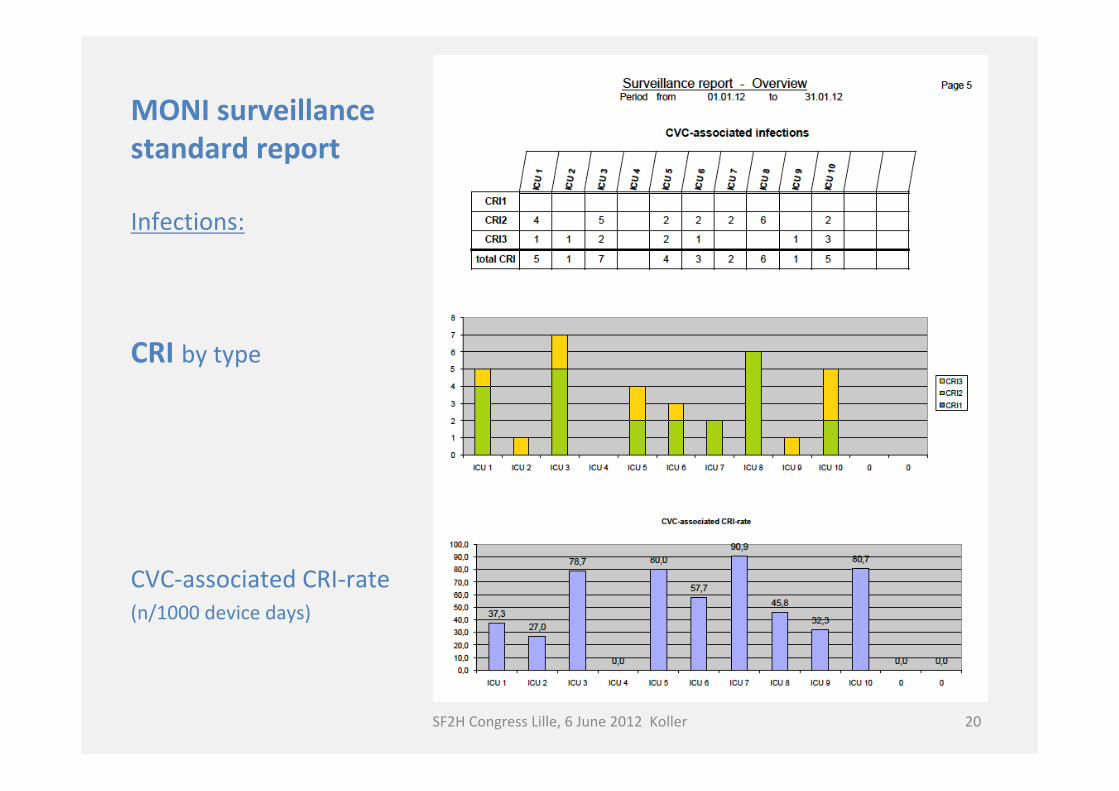
MONI surveillancestandard report
Infections:
CRI by type
CVC-associated CRI-rate (n/1000 device days)
SF2H Congress Lille, 6 June 2012 Koller 21
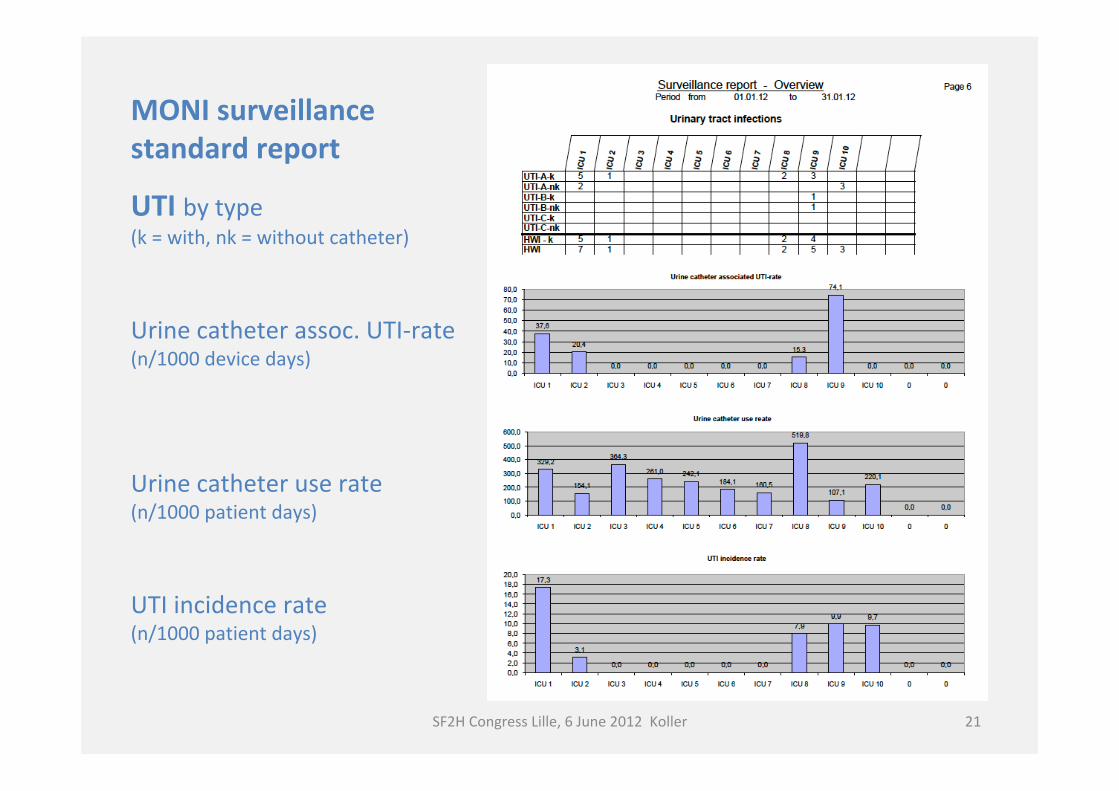
MONI surveillancestandard report
UTI by type(k = with, nk = without catheter)
Urine catheter assoc. UTI-rate(n/1000 device days)
Urine catheter use rate(n/1000 patient days)
UTI incidence rate(n/1000 patient days)
• Detailed insight into day-to-day patient data• Tool for infection control staff and for ICU staff
b) MONI-ICU “advanced” tool for detailed analyses
22SF2H Congress Lille, 6 June 2012 Koller
23SF2H Congress Lille, 6 June 2012 Koller
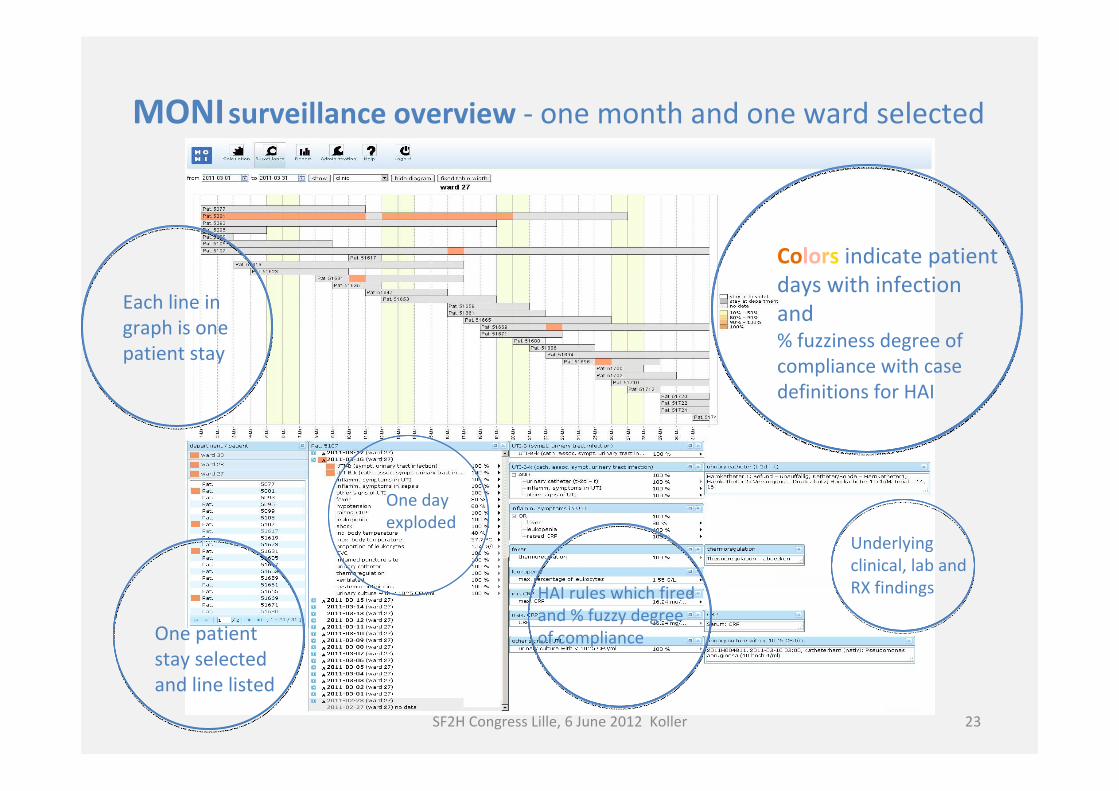
MONIsurveillance overview - one month and one ward selected
Colors indicate patient days with infection and % fuzziness degree of compliance with case definitions for HAI
Each line in graph is one patient stay
One patient stay selected and line listed
One day exploded
HAI rules which fired and % fuzzy degree of compliance
Underlying clinical, lab and RX findings
Comparison of: Surveillance results generated automatically by MONI-ICU with conventionally generated - in parallel by trained surveillance staff and attending clinical experts using patient chart reviews and other available information (“gold standard”) Time expenditure for manual analysis of patient charts vs. time expenditure when applying MONI-ICU for presentation and analysis of surveillance results
COMPARATIVE CLINICAL STUDY with MONI ICU
24SF2H Congress Lille, 6 June 2012 Koller
Blacky A, Mandl H, Adlassnig K-P, Koller W. Fully automated surveillance of healthcare-associated infections with MONI-ICU – A breakthrough in clinical infection surveillance. Appl Clin Inf 2011; 2: 365–372
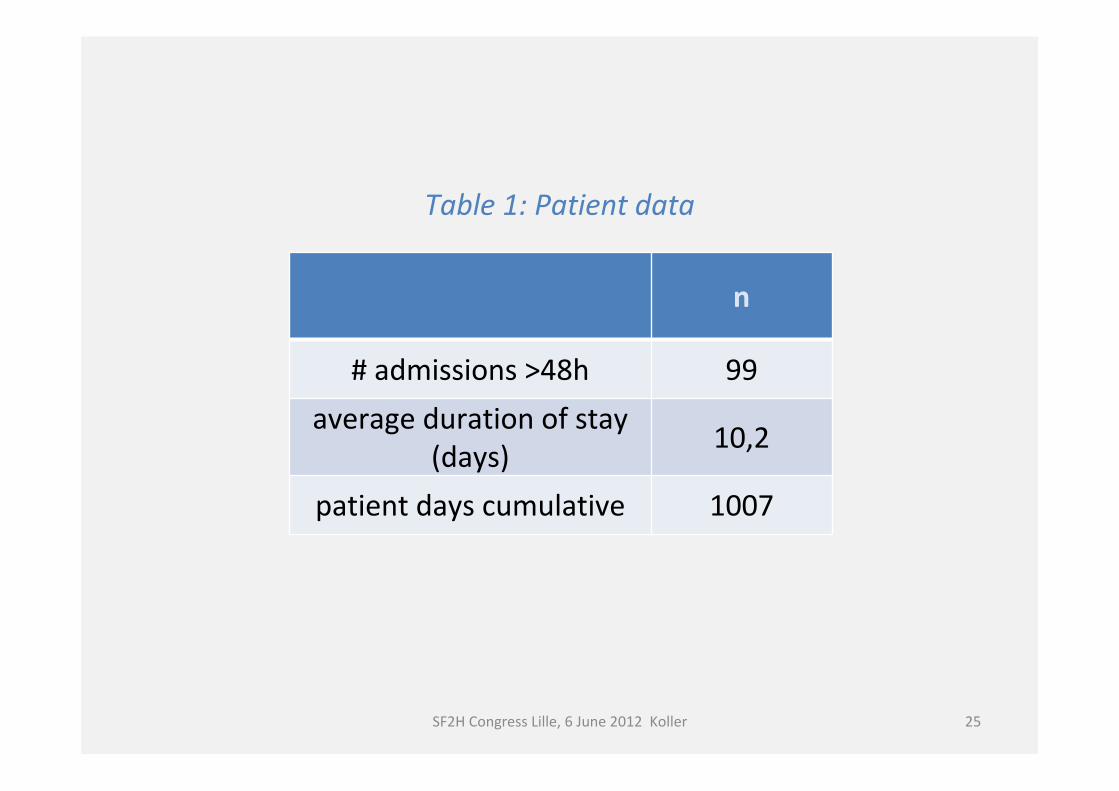
n
# admissions >48h 99average duration of stay
(days) 10,2
patient days cumulative 1007
25SF2H Congress Lille, 6 June 2012 Koller
Table 1: Patient data
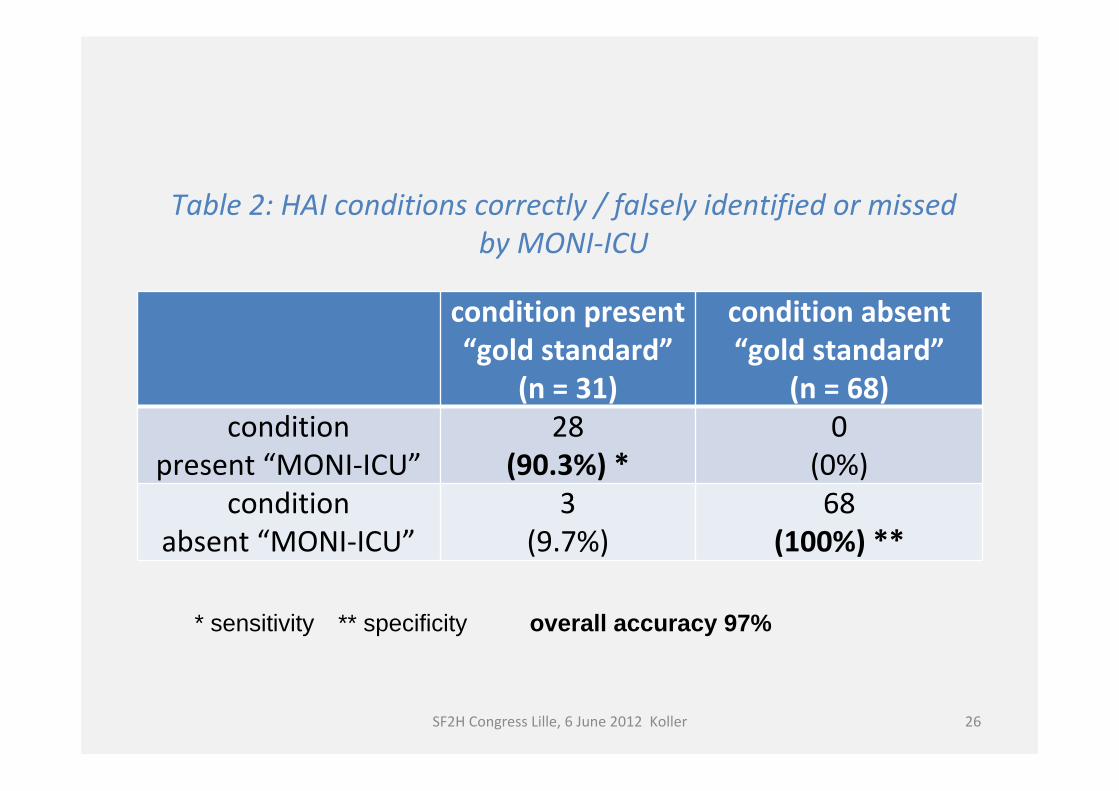
condition present“gold standard”
(n = 31)
condition absent“gold standard”
(n = 68)condition
present “MONI-ICU”28
(90.3%) *0
(0%)condition
absent “MONI-ICU”3
(9.7%)68
(100%) **
Table 2: HAI conditions correctly / falsely identified or missedby MONI-ICU
26SF2H Congress Lille, 6 June 2012 Koller
* sensitivity ** specificity overall accuracy 97%
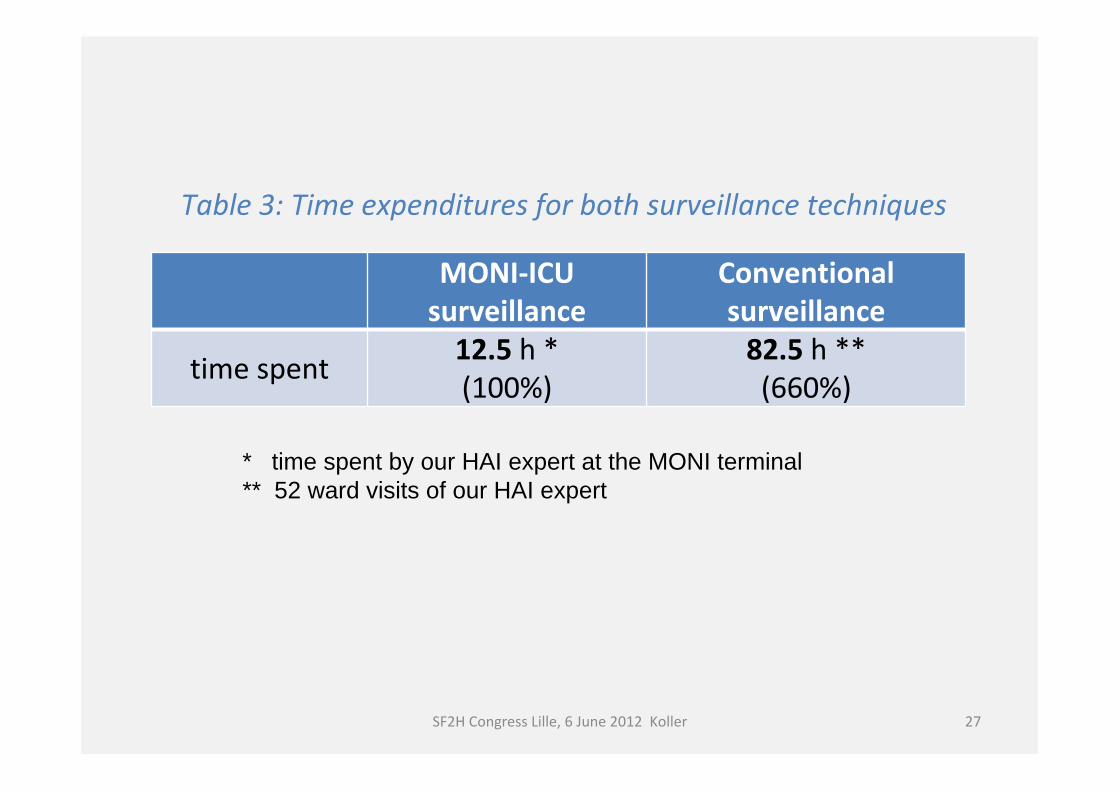
MONI-ICU surveillance
Conventional surveillance
time spent 12.5 h * (100%)
82.5 h **(660%)
27SF2H Congress Lille, 6 June 2012 Koller
Table 3: Time expenditures for both surveillance techniques
* time spent by our HAI expert at the MONI terminal** 52 ward visits of our HAI expert
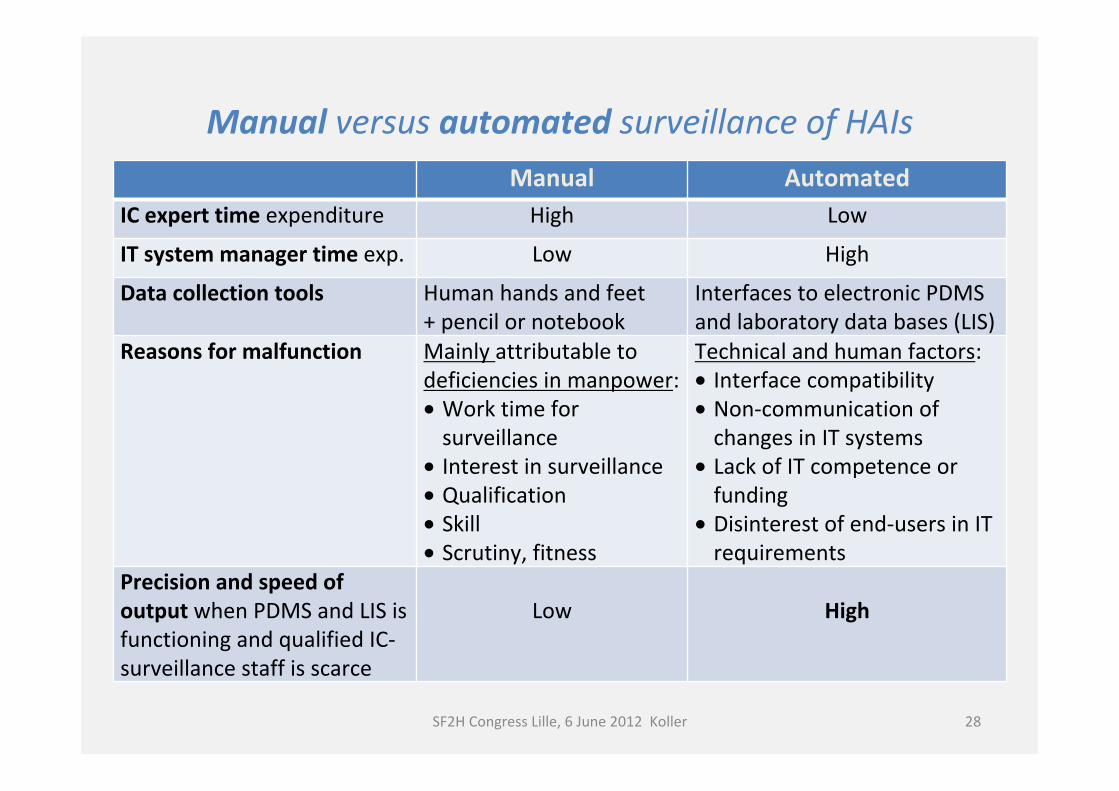
Manual versus automated surveillance of HAIsManual Automated
IC expert time expenditure High Low
IT system manager time exp. Low High
Data collection tools Human hands and feet + pencil or notebook
Interfaces to electronic PDMS and laboratory data bases (LIS)
Reasons for malfunction Mainly attributable to deficiencies in manpower:• Work time for
surveillance• Interest in surveillance• Qualification • Skill• Scrutiny, fitness
Technical and human factors:• Interface compatibility• Non-communication of
changes in IT systems• Lack of IT competence or
funding• Disinterest of end-users in IT
requirementsPrecision and speed of output when PDMS and LIS is functioning and qualified IC-surveillance staff is scarce
Low High
SF2H Congress Lille, 6 June 2012 Koller 28
CONCLUSIONS
• High specificity (= no “false alarms”) with MONI surveillance;cases missed in MONI-ICU surveillance due to rectifiable technical errors
• 85% of doctors’ and nurses’ time saved with MONI-ICU compared to manual/conventional surveillance
• When PDMS and LIS provide an accessible and up-to-date collection of clinical and denominator data, intelligent IT can provide valuable surveillance reports on demand and quickly
• MONI-ICU is also suited for day-to-day follow-up of infections and may – in conjunction with the modules MOAB and MOMO – support clinical decisions in ICUs
• MONI-ICU enhances transparency of infection matters and supports scientific work-up of unresolved questions
29SF2H Congress Lille, 6 June 2012 Koller
Intelligent software helps to ask relevant questions and to get reliable answers from abundant clinical data without a need for time consuming (and often redundant!) manual data management.
Facing a growing lack of skilled manpower, health care institutions are under increasing pressure to comply with quality assurance and patient safety regulations.
We believe that electronic surveillance of HAI with intelligent IT in near future will be indispensible in health care institutions.
30SF2H Congress Lille, 6 June 2012 Koller
Electronic Surveillance of HAI – Is it worth it?
31SF2H Congress Lille, 6 June 2012 Koller
Co-workers:
Prof. Peter ADLASSNIGDr. Alexander BLACKYDr. Harald MANDL
Dr. Claudia HONSIG-BAUER
Thank you for attention!