electronic fetal heart rate monitoring in intra-partum ...hums.ac.ir/uploads/fhr.pdf ·...
TRANSCRIPT

Cardio-Toco-Graphy (CTG)
• Electronic Fetal Heart rate monitoring in intra-partum period.
• With stress (contractions, during labour)
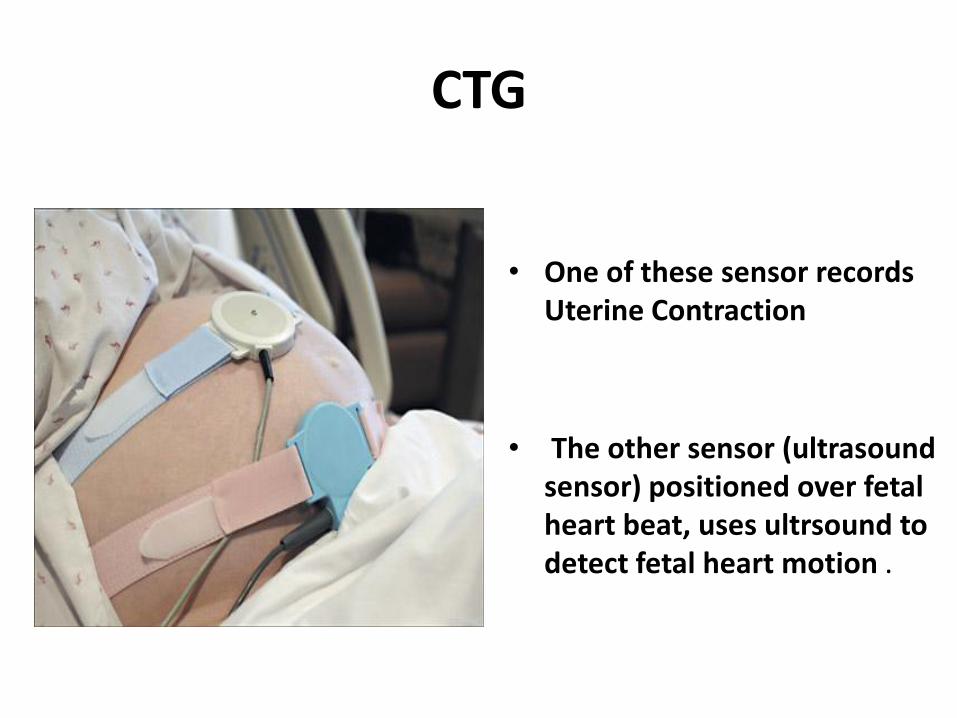
• Two probes are used one for FHR & another at fundus for uterine contractility.
CTG
• One of these sensor records Uterine Contraction
• The other sensor (ultrasound sensor) positioned over fetal heart beat, uses ultrsound to detect fetal heart motion .

CTG
• The typical fetal monitor strip consists of two rows of graphs;
– Upper graph charting the fetal heart rate (in beats per minute) and
– Lower graph charting the mother's contractions (in mm of Hg).
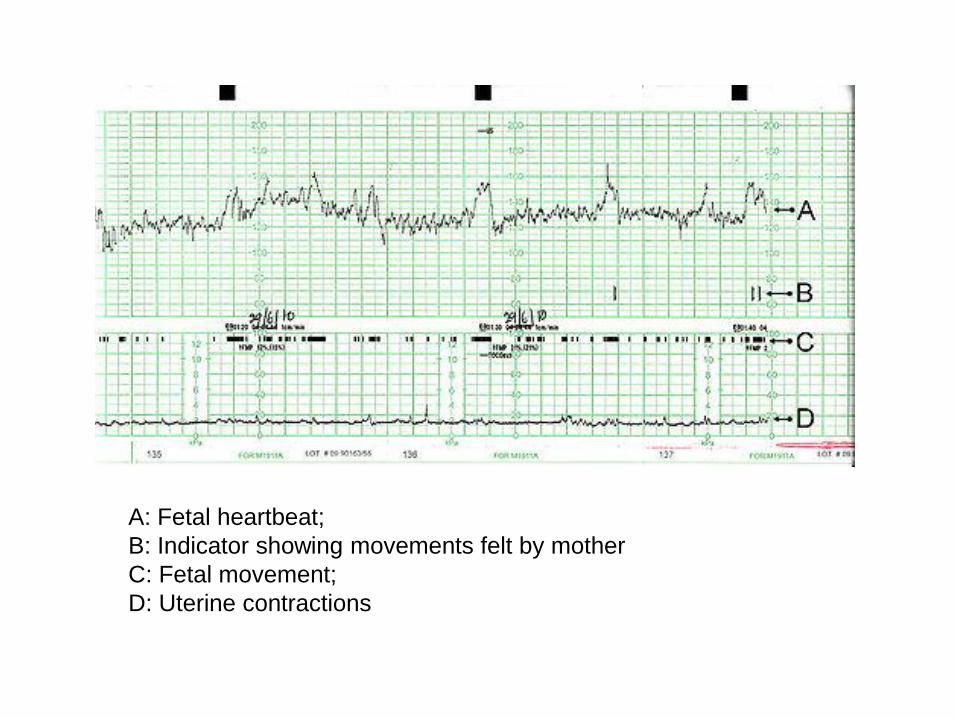
A: Fetal heartbeat;
B: Indicator showing movements felt by mother
C: Fetal movement;
D: Uterine contractions

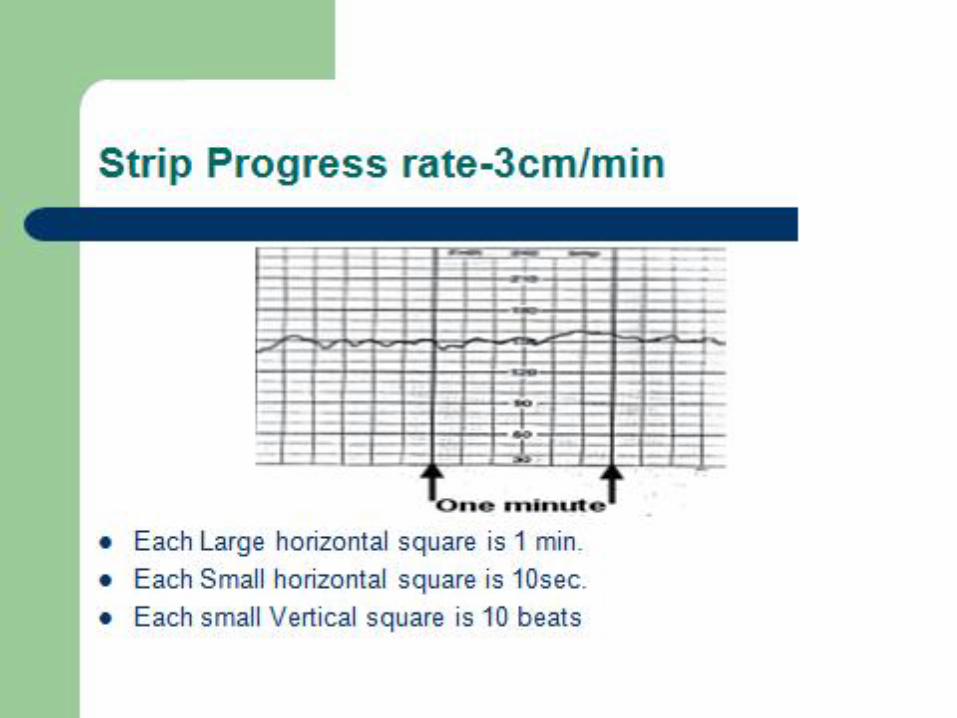
CTG • Strip moves at the
definitive rate of 3cm / minute .
• Each small horizontal square of graph represents the span of 10 – 15 seconds.
. Each small vetical square is 5 - 10 beats
• Test usually lasts for 20 to 40 minutes.
اجزاء اساسی نمودار قلب جنین
• What is the baseline rate?
• Describe the variability
• Are there accelerations present?
• Are there decelerations present?
• Are contractions present?
• What category is this tracing?
• Is this fetal tracing reassuring?

Baseline FHR - Definition
• The mean level of the FHR when this is stable, excluding accelerations and decelerations. It is determined over a time period 10 minutes and expressed in bpm.
• The normal baseline FHR varies between 110-160 bpm (slightly quicker for preterm).
• A baseline FHR of 100-109 bpm or 161-180 bpm is non-reassuring.
• A baseline FHR of <100 or >180 bpm is classified as an abnormal feature.
Intrapartum care: NICE guideline
CG190 (December 2014).


Variabllity
سیکل یا بیشتر 2نوسانات خط پایه ضربان قلب جنین به •
در دقیقه
.از نظر ارتفاع و تناوب متغیر هستند•
.نوساناتی که دامنه و تعداد نامنظمی دارند•
توجه به فاصله تغییرپذیری بر حسب ضربان در دقیقه و با •
.محاسبه می شود موج یک سیکل( ارتفاع )قله تا دامنه

Variabllity
• Absent = undetectable
• Minimal = 5≥ bpm
• Moderate = 6 to 25 bpm
• Marked = over 25 bpm
• Measured in a 10 minute window
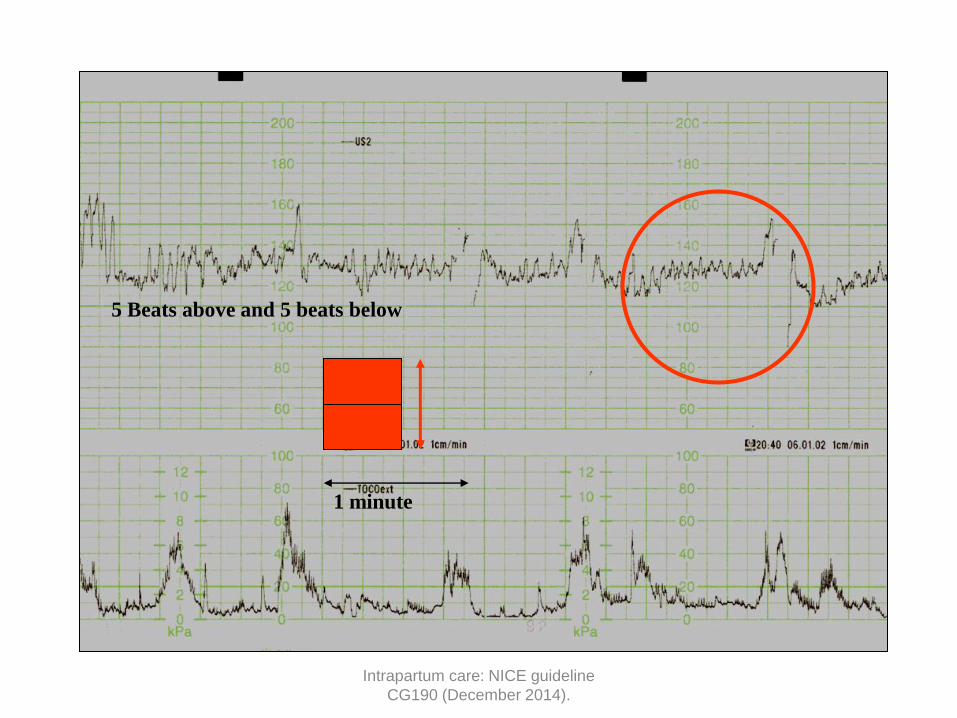
5 Beats above and 5 beats below
1 minute
Intrapartum care: NICE guideline
CG190 (December 2014).
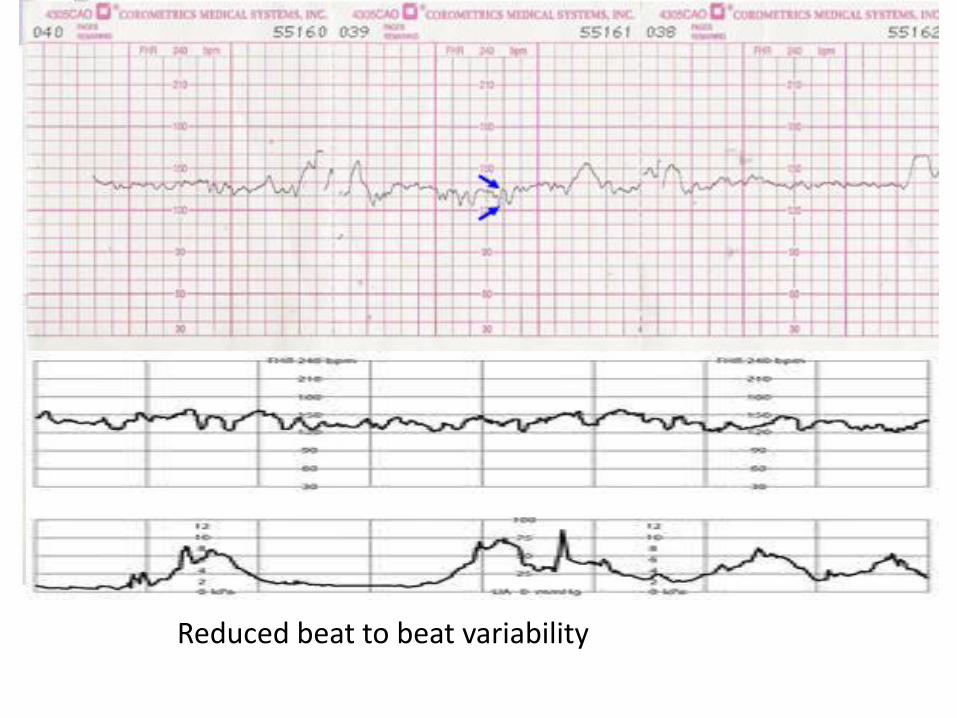
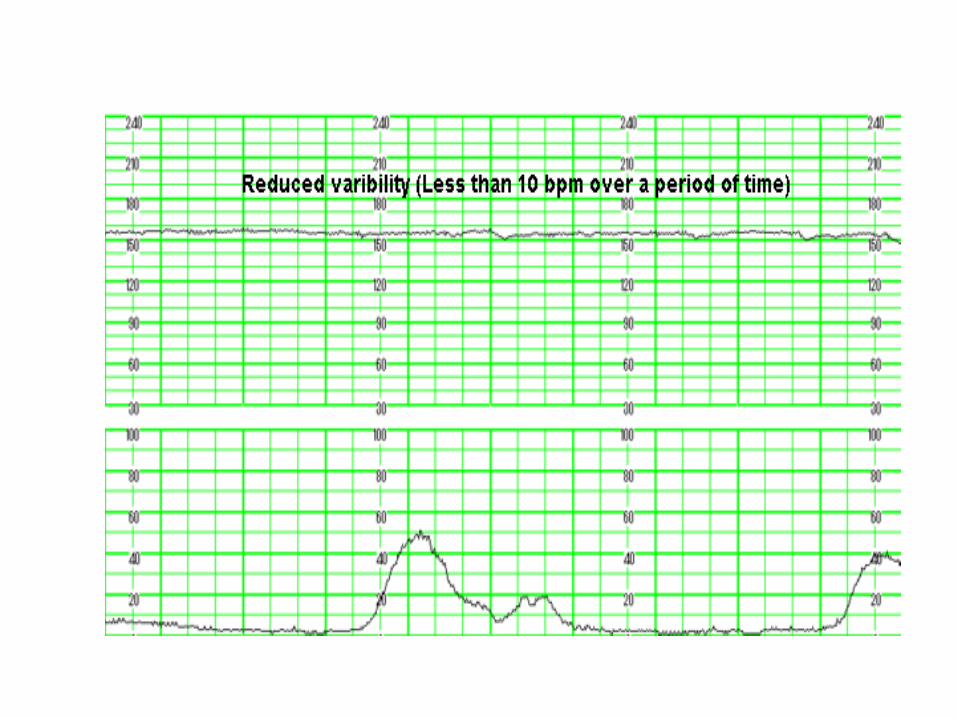
Reduced beat to beat variability
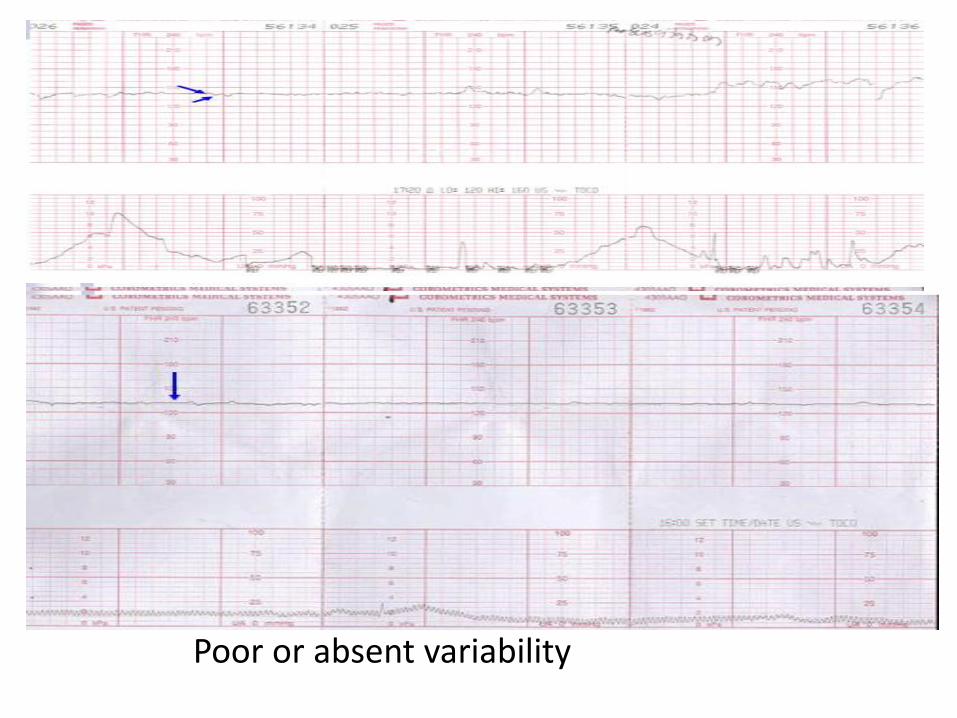
Poor or absent variability

Intrapartum care: NICE guideline
CG190 (December 2014).

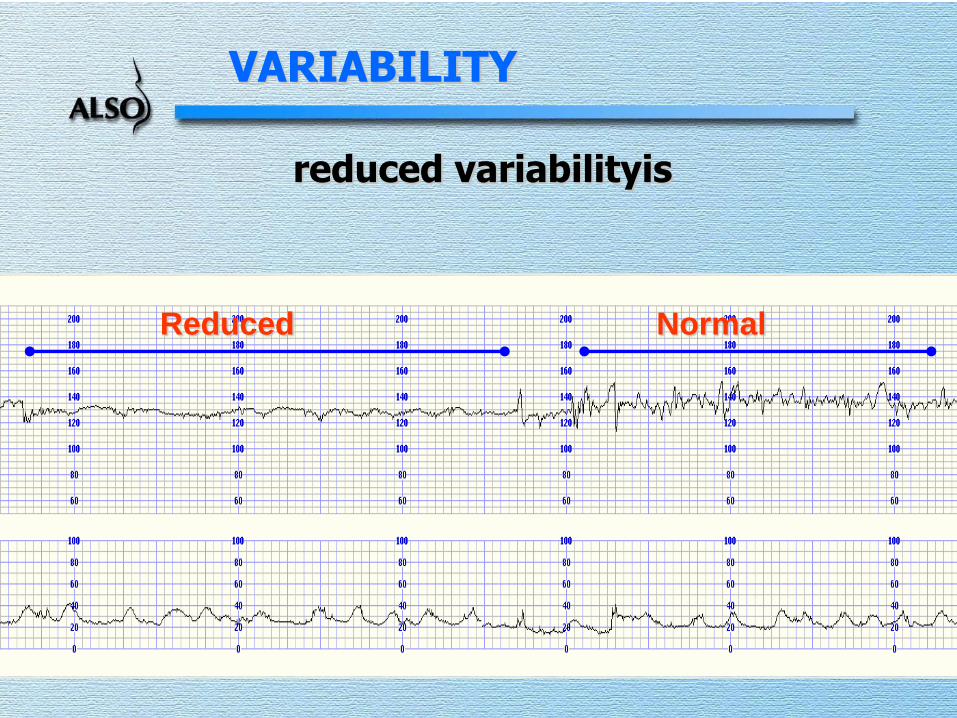
VARIABILITY
reduced variabilityis
Reduced Normal

A Normal Antenatal CTG

Baseline Rate
• 110 to 160 bpm at term
• Faster in early pregnancy
• Below 110 bpm= baseline bradycardia
• Below 80 bpm = severe bradycardia
• Over 160 bpm = Tachycardia
• Tachycardia common with maternal fever
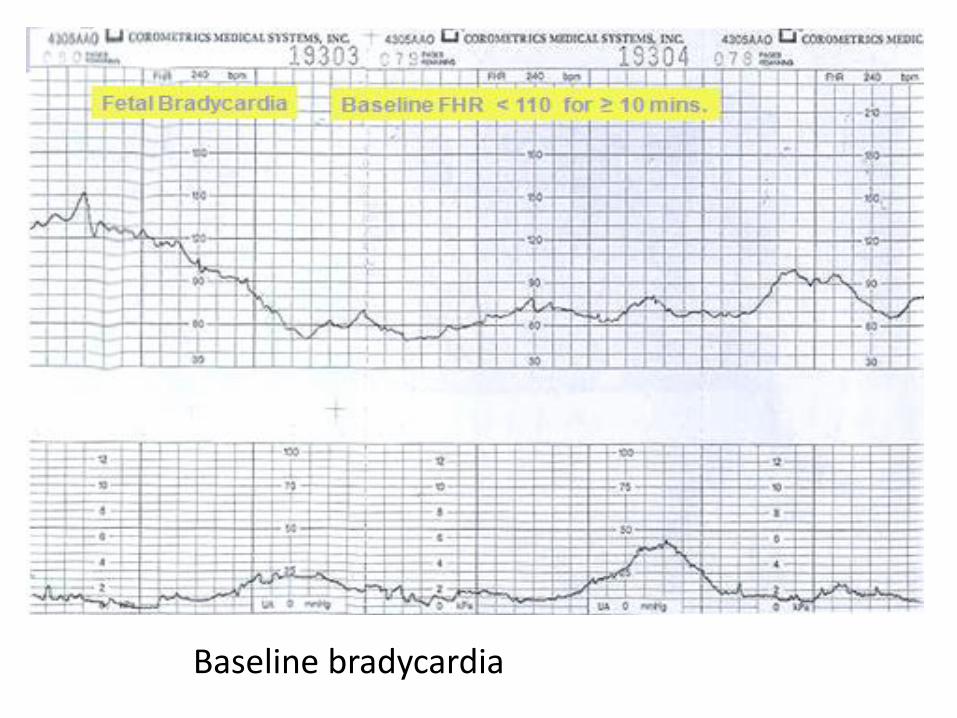
Baseline bradycardia

Baseline tachycardia

Accelerations
• Must be ≥15 bpm and ≥15 sec above baseline (32w)
• Always reassuring when present
• May not occur when fetus is “sleeping”
• Should occur in response to fetal movements or fetal stimulation
• Non reactive periods usually do not exceed 40 min • (>90 min and no accelerations is worrying)
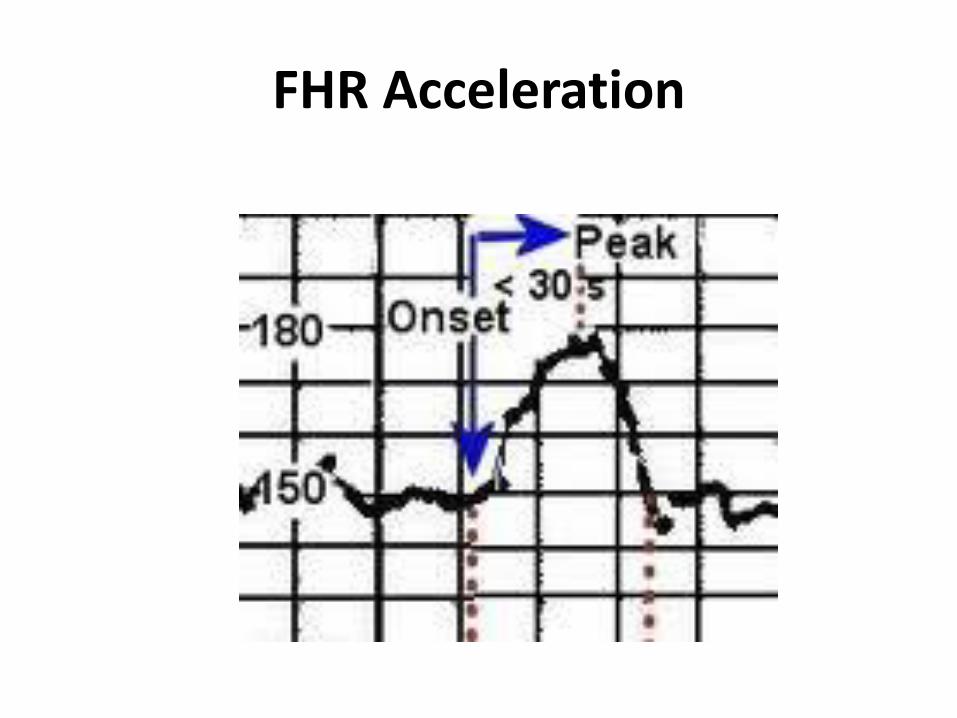
FHR Acceleration
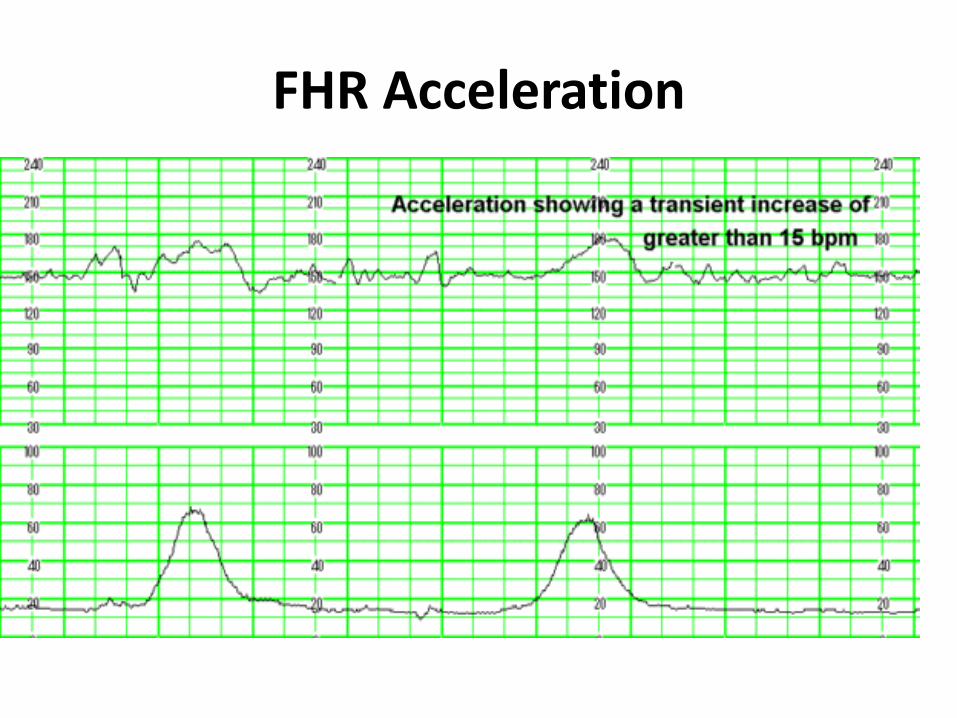
FHR Acceleration

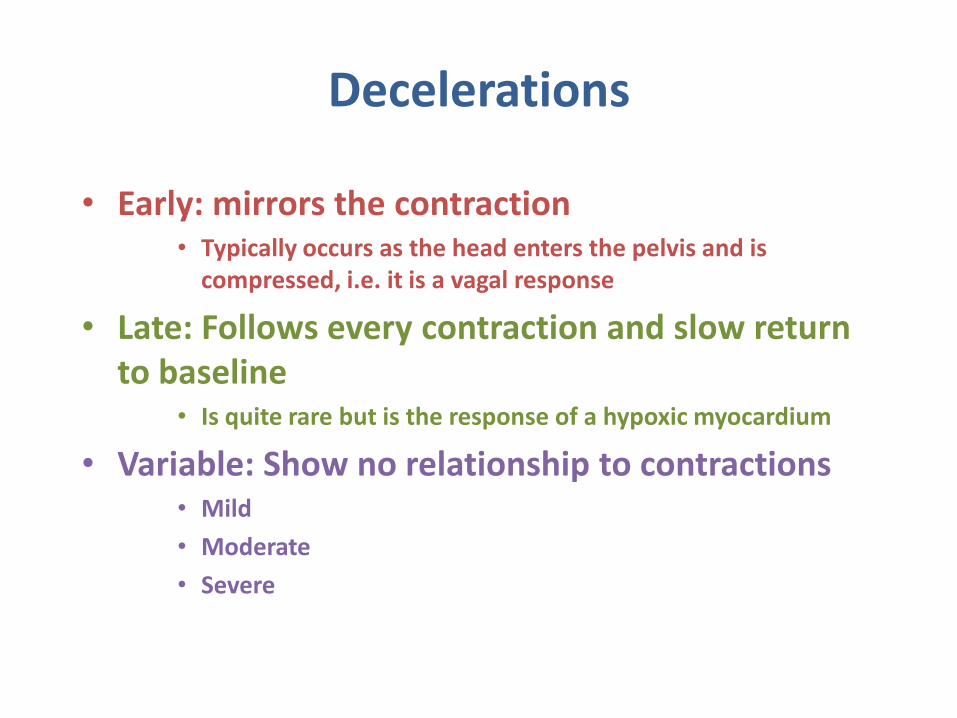
Decelerations
• Early: mirrors the contraction • Typically occurs as the head enters the pelvis and is
compressed, i.e. it is a vagal response
• Late: Follows every contraction and slow return to baseline
• Is quite rare but is the response of a hypoxic myocardium
• Variable: Show no relationship to contractions • Mild
• Moderate
• Severe

early deceleration
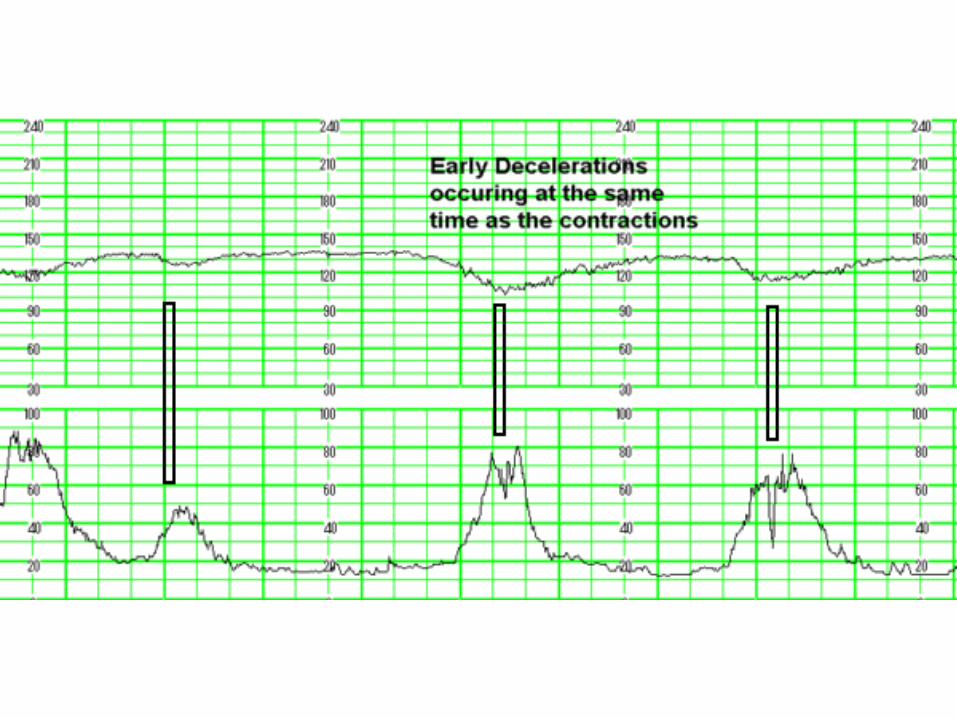


• Begin after onset of contraction
• Nadir (or trough) after peak of contraction
• Return to baseline after end of contraction
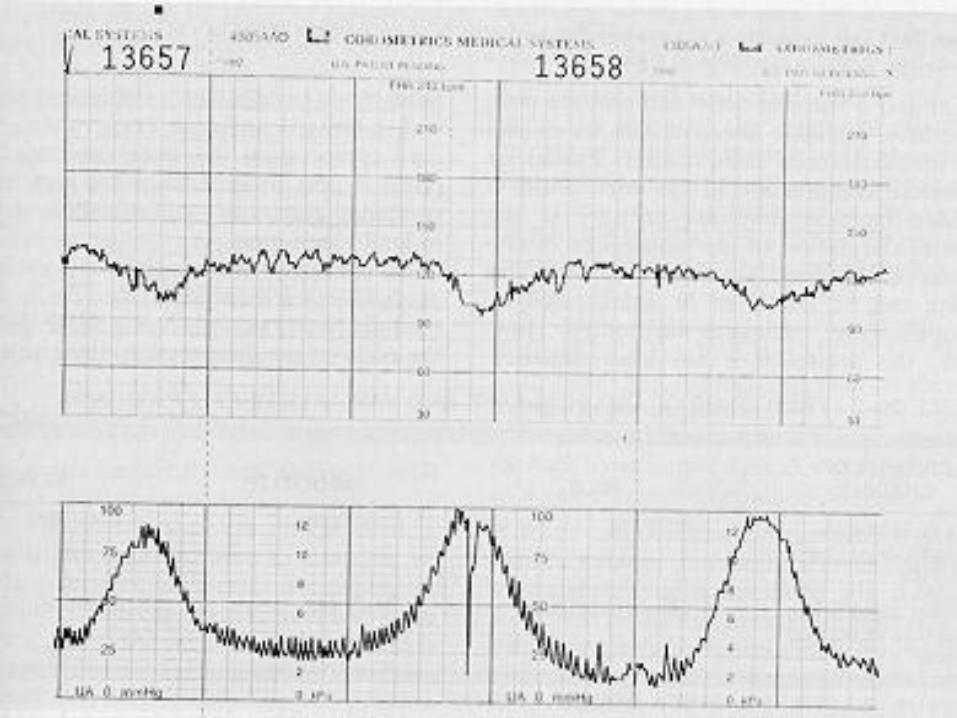
LATE DECELERATIONS



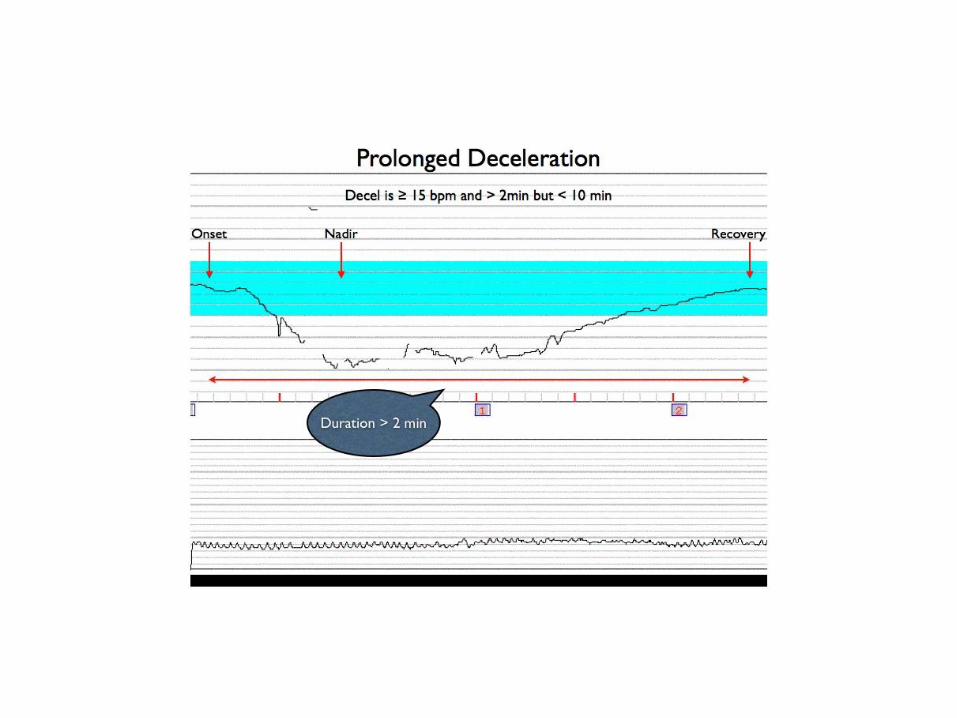

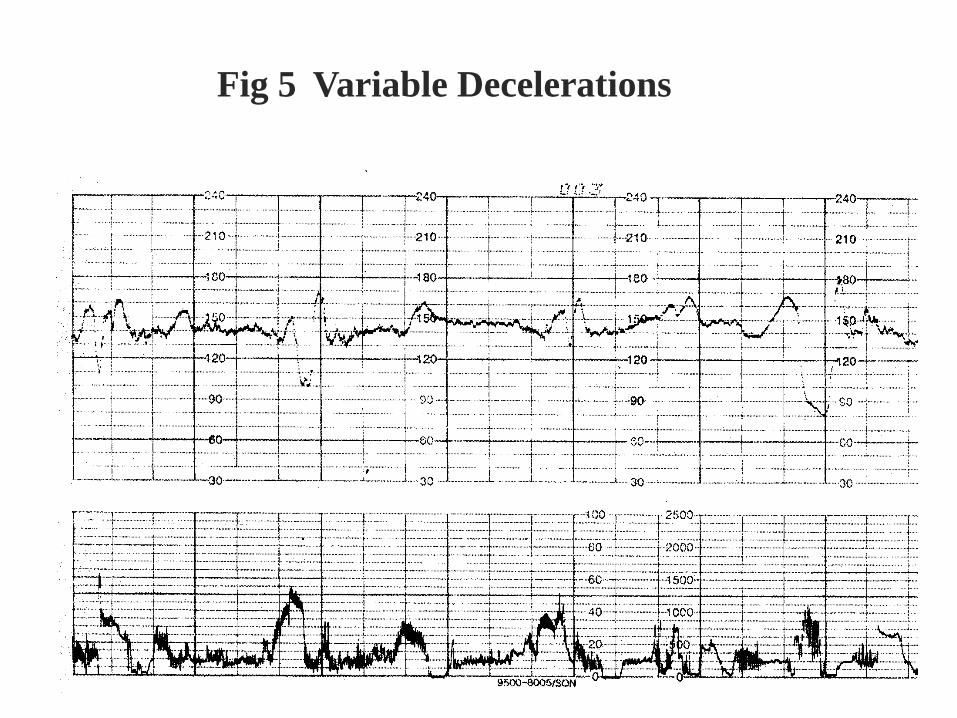
Fig 5 Variable Decelerations


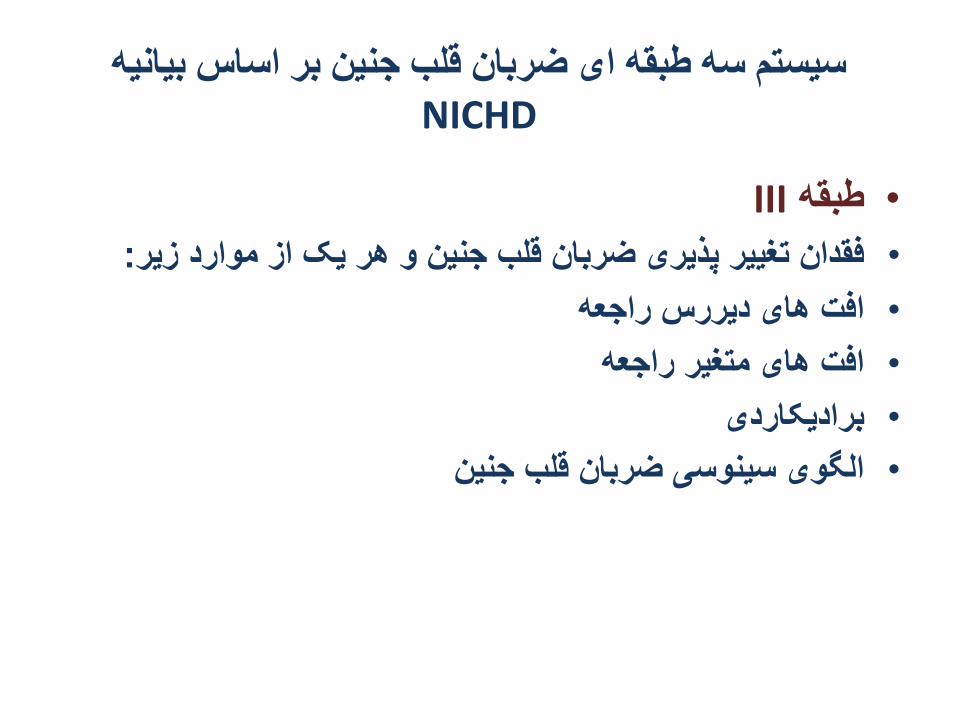
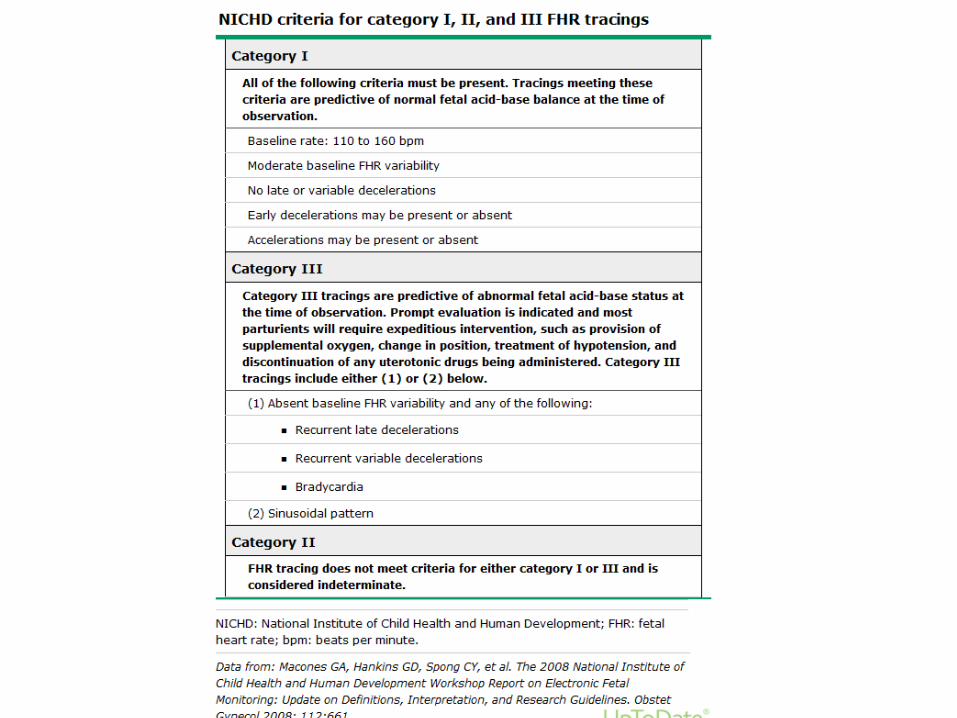
سیستم سه طبقه ای ضربان قلب جنین بر اساس بیانیه
NICHD
Iطبقه
ضربه در دقیقه 110-160خط پایه ضربان قلب جنین •
تغییر پذیری متوسط ضربان قلب جنین•
فقدان افت های دیررس یا متغیر•
وجود یا فقدان افت زودرس•
وجود یا فقدان تسریع ها •
سیستم سه طبقه ای ضربان قلب جنین بر اساس بیانیه
NICHD
IIIطبقه •
:فقدان تغییر پذیری ضربان قلب جنین و هر یک از موارد زیر•
افت های دیررس راجعه•
افت های متغیر راجعه•
برادیکاردی•
الگوی سینوسی ضربان قلب جنین•

سیستم سه طبقه ای ضربان قلب جنین بر اساس بیانیه
NICHD
IIطبقه •
تاکیکاردی –برادی کاردی : خط پایه •
تغییر پذیری کم یا تغییر پذیری قابل توجه ، : تغییر پذیری خط پایه •
فقدان تغییر پذیری بدون همراهی با افت راجعه
فقدان تسریع بعد از تحریک جنین: تسریع ها •
افت های متغیر راجعه همراه با تغییر پذیری : افت های پریودیک •
کم یا متوسط خط پایه، افت دیررس راجعه با تغییر پذیری متوسط
خط پایه

الگوی سینوسی
ضربه در 120 -160خط پایه ثابت ضربان قلب جنین بین •
دقیقه با امواج منظم
ضربه در دقیقه 5- 25ارتفاع موج بین •
سیکل در دقیقه 2 -5تناوب •
شکل امواج منظم باال و پایین خط پایه•
فقدان تسریع ها•


NICHDالگوهای تعریف نشده در سیستم
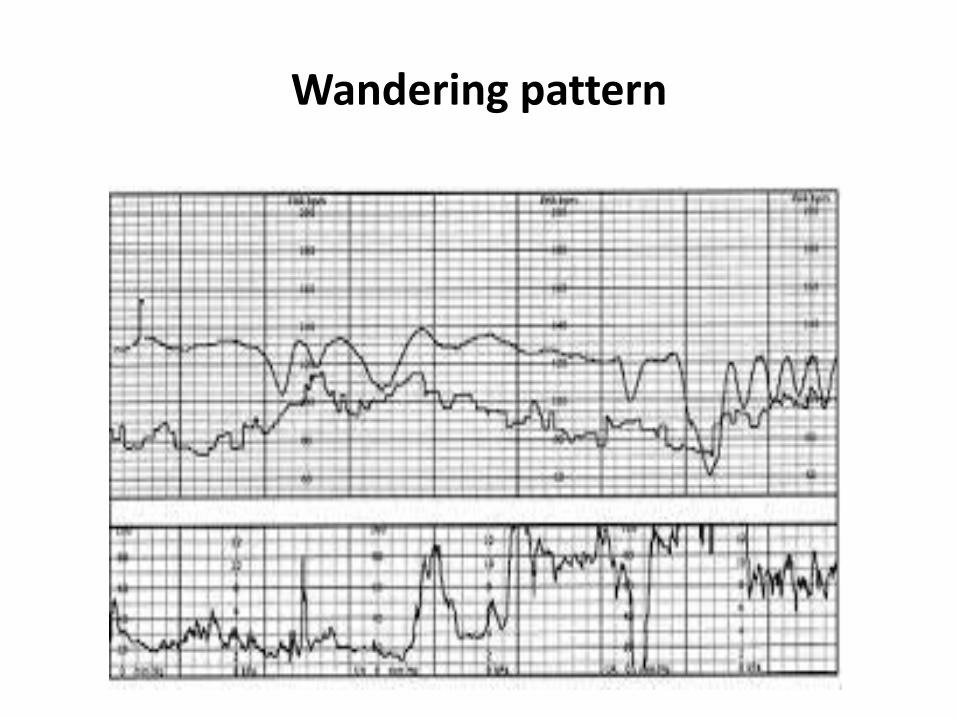
خط پایه در محدوده نرمال است، اما : خط پایه نوسان دار
میزان ثابت پایداری برای یک دوره زمانی طوالنی ندارد تا
( Wandering baseline.)بتوان متوسط آن را بیان کرد
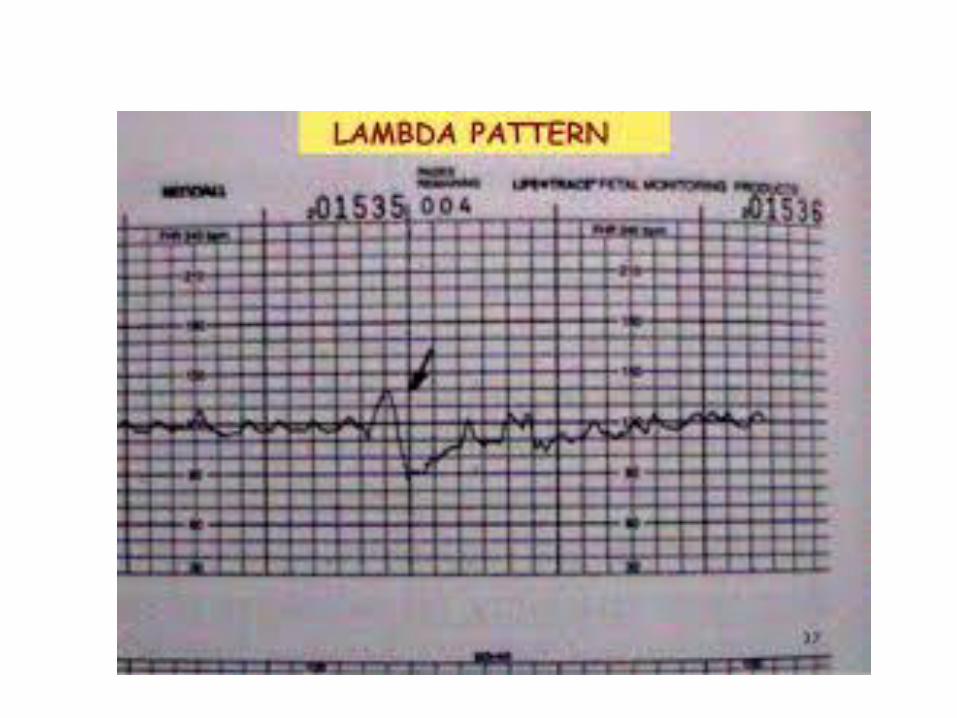
ضربان قلب جنین به صورت یک تسریع : الگوی المبدا
مختصر و به دنبال آن یک افت کوچک، در مراحل اولیه
.لیبر، شایع است و اهمیت بالینی ندارد
تغییرات سریع در ضربان قلب جنین : Saltattory الگوی
25سیکل در دقیقه و در محدوده بیش از 3-6با تناوب ضربه در دقیقه
Wandering pattern

Saltattory pattern

Non stress test
*Done using the cardiotocometry with the patient in left lateral position
**Record for 20 minutes

Non stress test
حرکات جنینجنین در پاسخ به ضربان قلب تعداد تسریع•
.استوضعیت جنین این تست بررسي •
سالمت جنینساده ترین و پر كاربردترین تست ارزیابي •
ضربان قلب جنین به علت تاثیرات اتونوم افزایش یا کاهش پیدا •
می کند، و تغییر پذیري ضربه به ضربه نیز تحت كنترل دستگاه
.قرار دارد( اتونوم )عصبي خودكار
کاهش تسریع ممکن است با کاهش تغییر پذیری ضربه به ضربه •
.ضربان قلب همراه باشد

Non stress test
به طور شایع كاهش از بین رفتن واكنشي جنین تحت •
، تضعیف مركزي به علت تاثیرسیکلهای خواب جنین رخ می دهد
.دارو و استعمال دخانیات و اسیدوز هم اتفاق می افتد
، تسریع و یا واکنش پذیری ضربان قلب جنین را سن حاملگی•
.تحت تاثیر قرار می دهدبا باال رفتن سن حاملگی تعداد حرکات بدنی همراه با تسریع •
.ضربان و دامنه تسریعها افزایش می یابد

Non stress test
باالی bpm 15،اوج تسریع هفته یا بیشتر 32جنین های در • .ثانیه یا بیشتر طول می کشد 15تعداد پایه و تسریع به مدت
یا bpm 10،تسریع به صورت حداکثرحاملگی 32قبل از هفته • ثانیه یا بیشتر 10بیشتر از حد پایه به مدت
دقیقه 20دو یا بیش از دو تسریع در عرض : نتایج طبیعی •

Non stress test
*The base line 110-160 beats/minute
*Reactive
At least two accelerations from base line of 15 bpm for at least 15 sec within 20 minutes
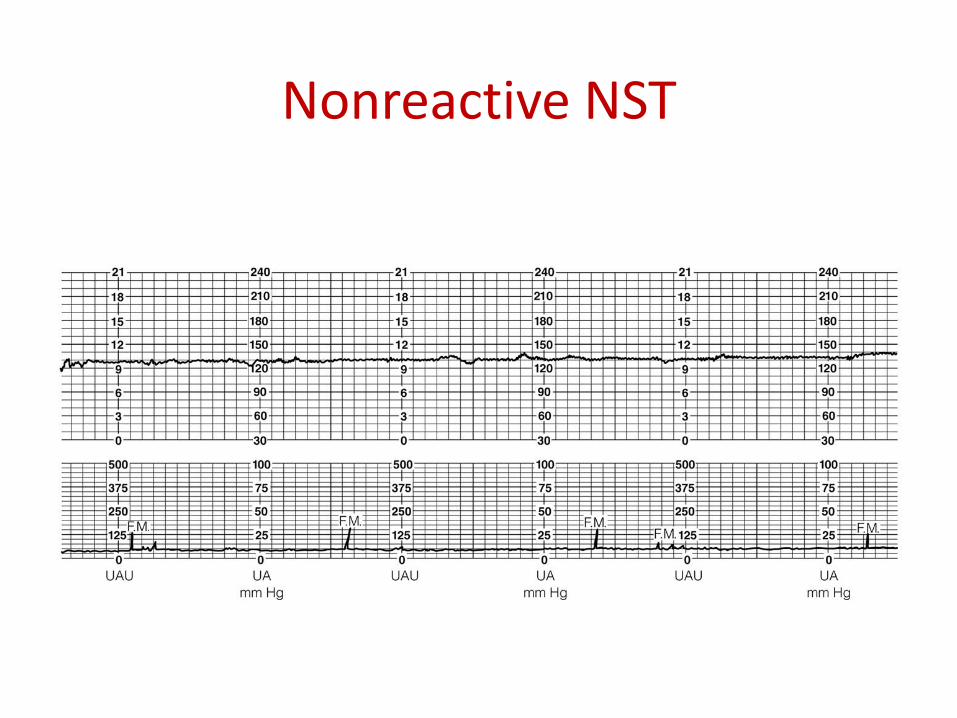
* Non reactive
No acceleration after 20 minutes- proceed for another 20 minutes

Non stress test
If non reactive in 90 minutes---proceed for contraction stress test or biophysical profile
The positive predictive value of NST to predict fetal acidosis at birth is 44%

Reactive NST
Nonreactive NST

Contraction stress test
Fetal response to induced stress of uterine contraction and relative placental insufficiency
Should not be used in patients at risk of preterm labor or placenta previa
Should be proceeded by NST

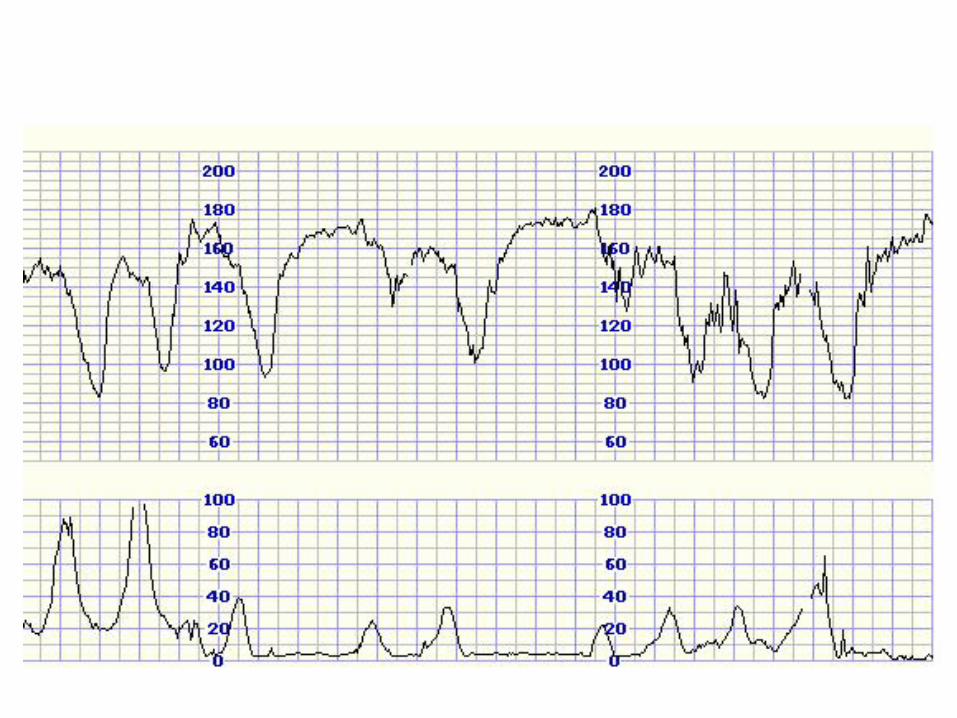
جفتی -اختالل رحمی افت دیررس ضربان قلب جنین
Contraction stress test
•Contraction is initiated by nipple stimulation or by oxytocin I.V.
•
•The objective is 3 contractions in 10 minutes
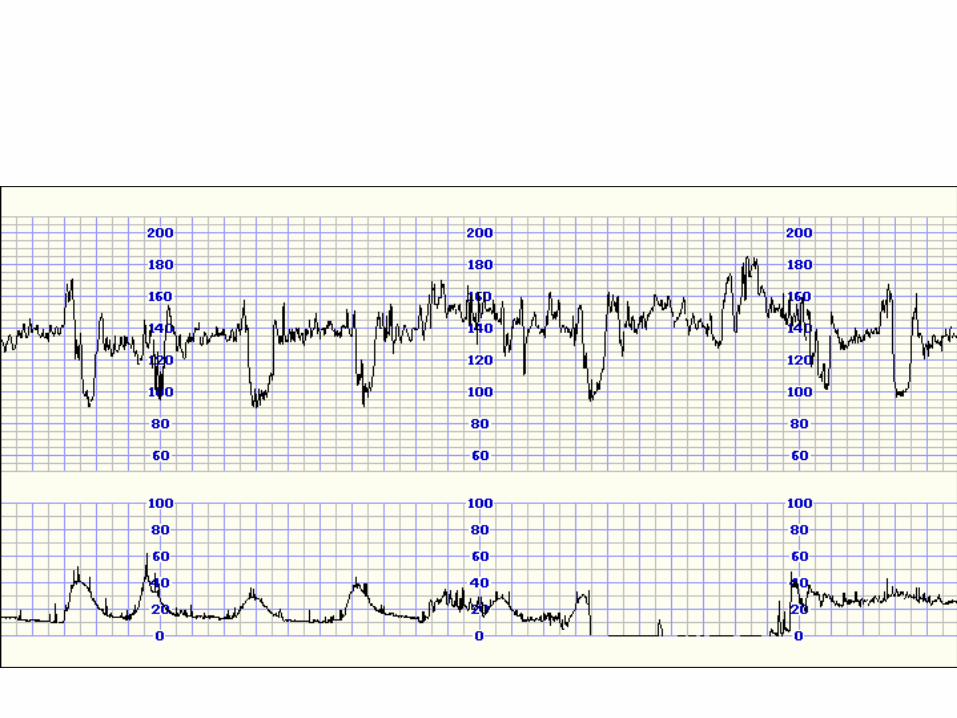
•If late deceleration occur-----positive CST
Contraction stress test
فقدان افت دیررس یا افت متغیر قابل توجه: منفي•
درصد 50درصد یا بیش از 50وقوع افت دیررس به دنبال : مثبت•
دقیقه 10انقباض در 3حتي اگر تعداد انقباض كمتر از ) انقباضات
(باشد
افت دیررس متناوب یا افت متغیر قابل توجه: مشكوك-مبهم•
افت تعداد ضربان قلب جنین كه در حضور : تحریك مفرط: مبهم•
دقیقه رخ مي دهدو به مدت 2انقباضات، بیش از یك بار در هر
.ثانیه طول مي كشد 90بیش از
دقیقه و یا نوار غیر 10انقباض در 3كمتر از : غیر رضایت بخش•
قابل تفسیر

Positive CST


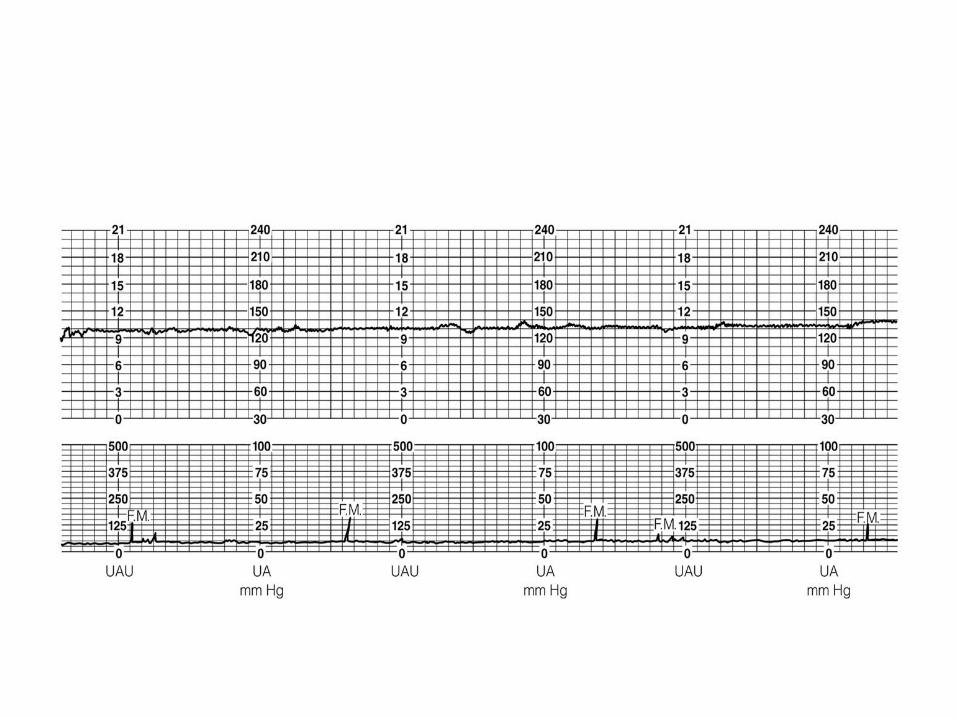
What category is this tracing? Is this fetal tracing reassuring
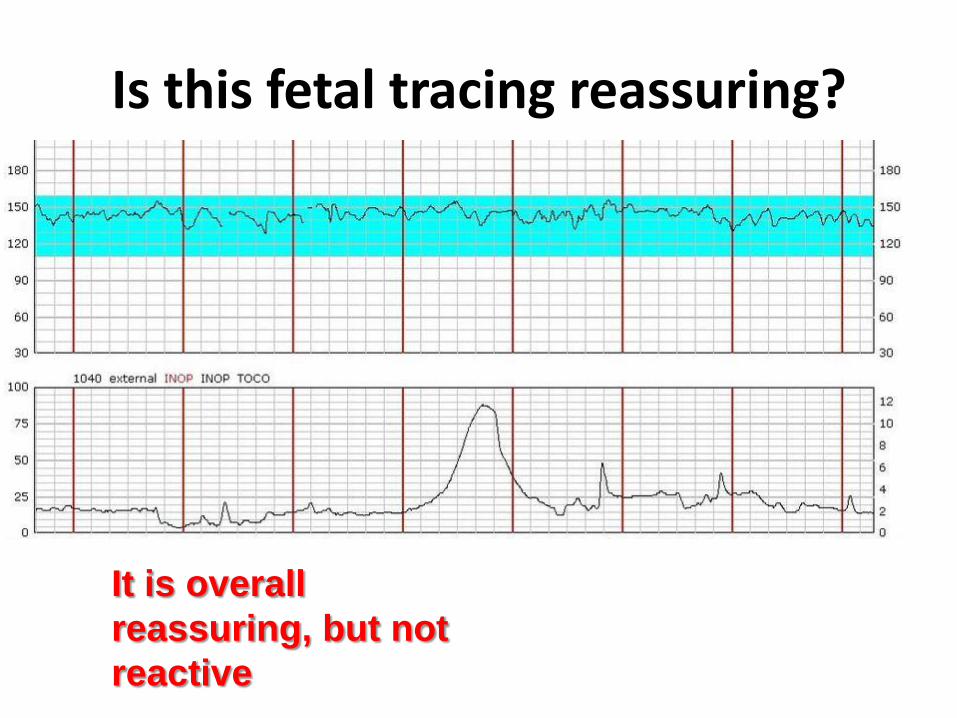
Is this fetal tracing reassuring?
It is overall
reassuring, but not
reactive
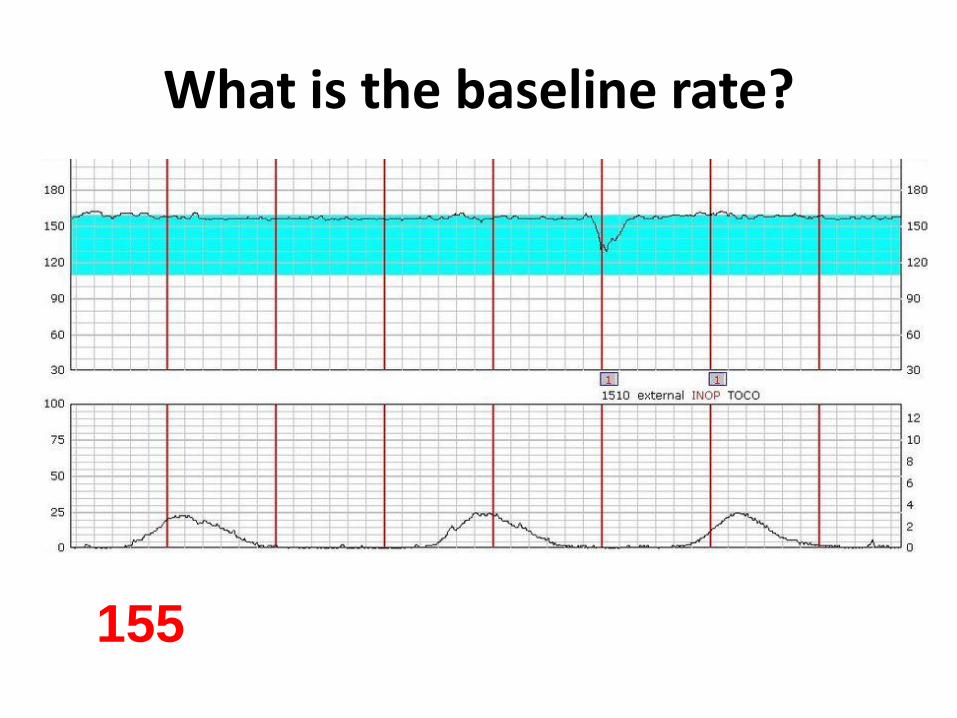
What is the baseline rate?
155

Describe the variability.
Absent

Quiz 1
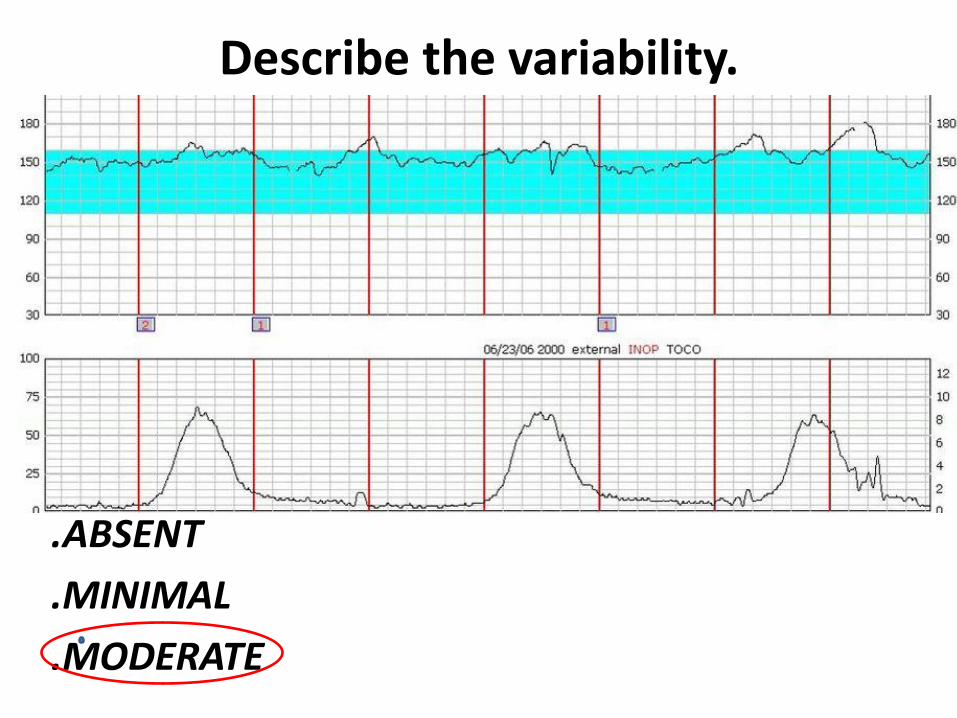
Describe the variability.
.ABSENT
.MINIMAL
.MODERATE

Are there accelerations present?
Answer: yes

Are there decelerations present? Are contractions present?
No regullar



3 examples are highlighted
ACCELERATIONS
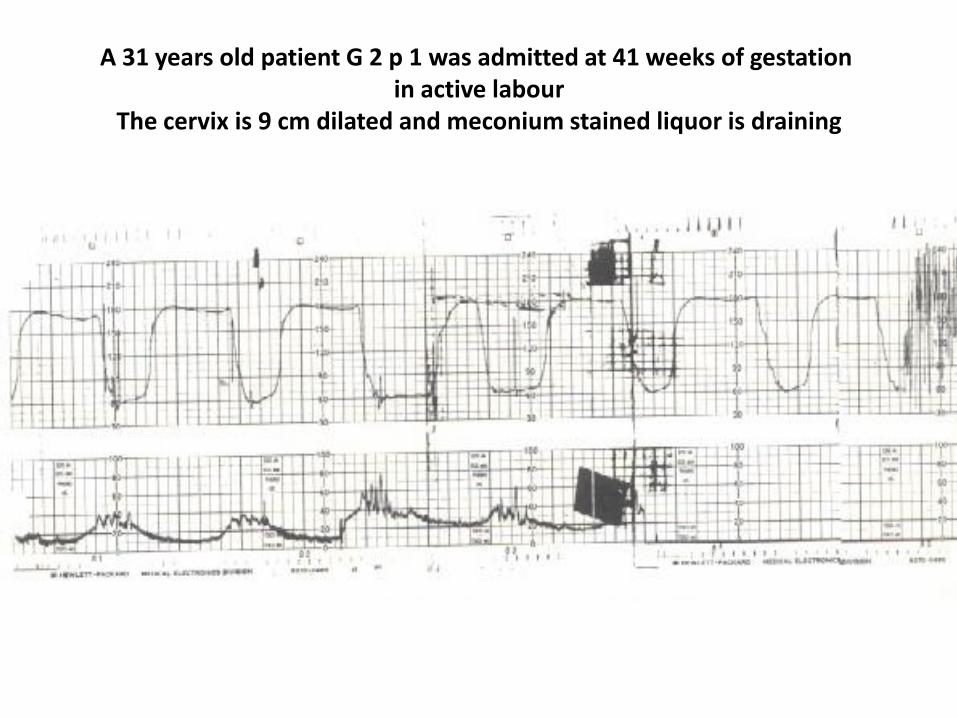
A 31 years old patient G 2 p 1 was admitted at 41 weeks of gestation in active labour
The cervix is 9 cm dilated and meconium stained liquor is draining

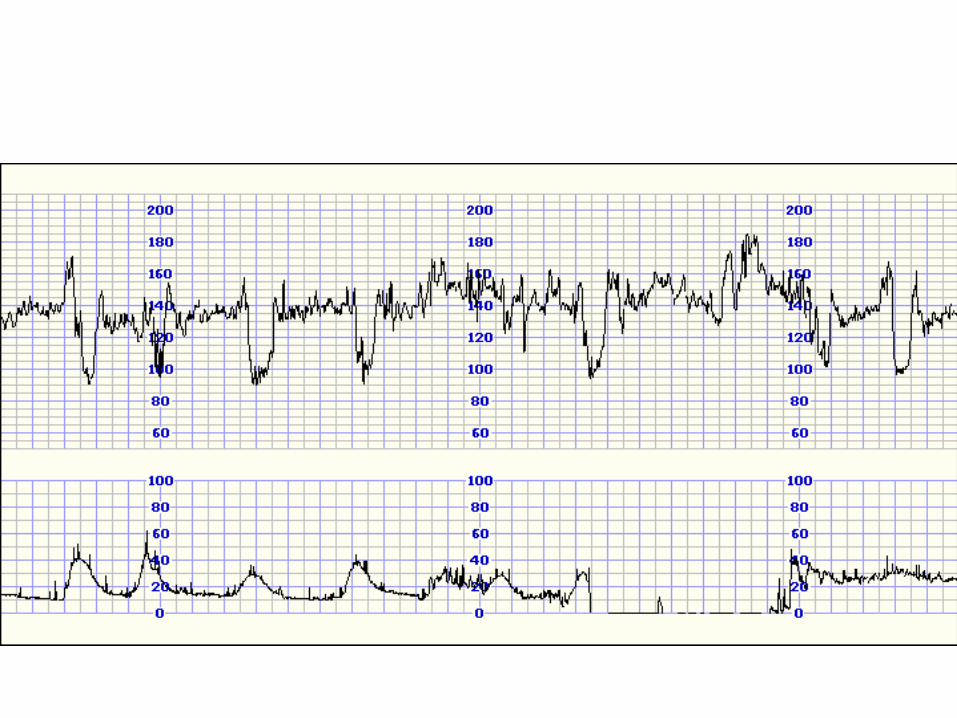
Tachycardia With Deceleration And No Variability: Mixed Pattern
Actions Wait and review after 30 minutes (no) Change the position of the patient (yes) Fetal scalp blood sampling (no) Immediate cesarean section (yes) Explain and reassure the patient (yes) Course and Outcome Cesarean section was carried out. A baby girl weighing 3898 gm was delivered from vertex presentation. Apgar score was 1/5 at one and five minutes. The position of the cord was not noted. The baby had meconium aspiration pneumonitis and was discharged after 10 days.

A 21 years old primigravid patient complaining of reduced fetal
movement at 42 weeks of gestation was admitted for induction of
labour. The cervix was 3cm
dilated, so amniotomy was done and liquor was clear. Syntocinon
infusion was started 30 minutes ago

Increased variability with hypertonic labour Actions Observe and review after 30 minutes (no) Vaginal examination to asses progress (yes) Reduce syntocinon infusion rate (yes) Immediate cesarean section (no) Oxygen by facial mask (yes) Fetal blood sampling for PH (no) Course and Outcome Syntocinon infusion was reduced and fetal heart returned to normal. 3 hours later CTG started to show late and variable decelerations, so cesarean section was performed for fetal distress. Outcome was baby girl weighing 3 kg with 3 tight loops of the cord around the neck. Apgar score was 9/10 at one and five minutes. The infant had normal newborn course.
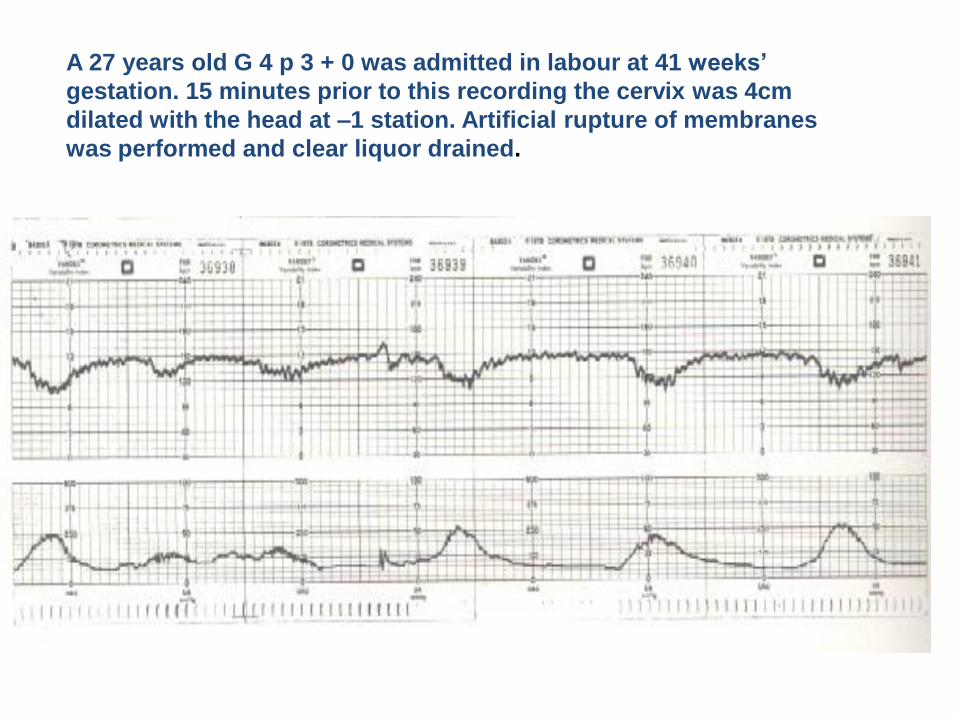
A 27 years old G 4 p 3 + 0 was admitted in labour at 41 weeks’
gestation. 15 minutes prior to this recording the cervix was 4cm
dilated with the head at –1 station. Artificial rupture of membranes
was performed and clear liquor drained.
Early decelerations
Actions Oxygen by facial mask (no)
Change maternal position (no)
Cesarean section (no)
Observe for the development of other types of declarations (yes)
Vaginal examination for progress assessment (no)
Fetal blood sampling (no)
Course and outcome Progressed to normal vaginal delivery of female infant
weighing 3969 gm. Apgar score was 8/9 at one and five
minutes. The infant followed a normal newborn course.
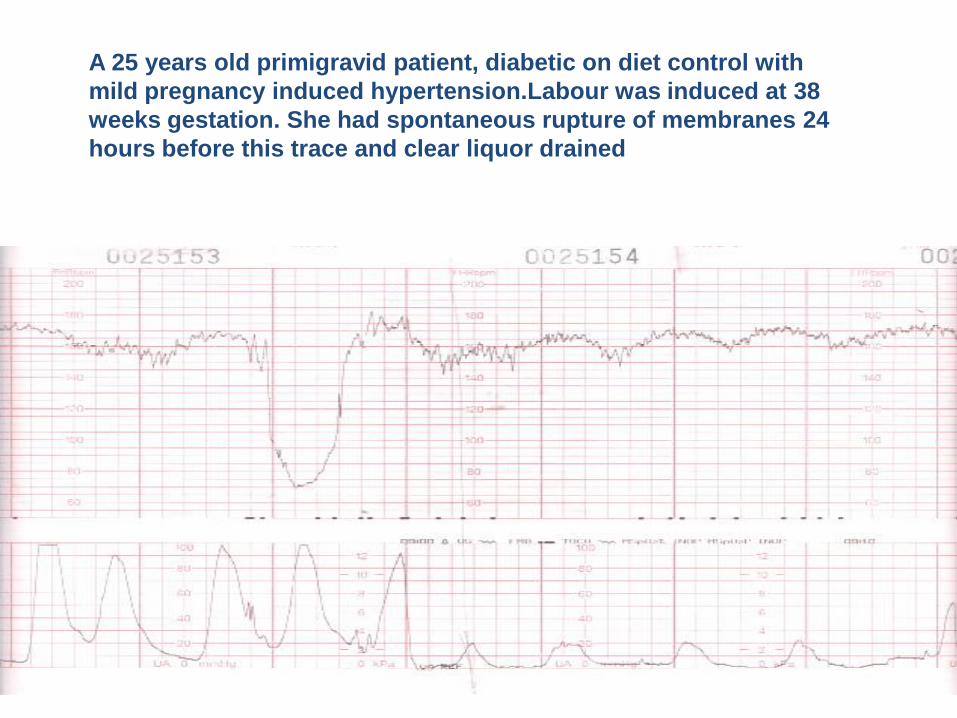
A 25 years old primigravid patient, diabetic on diet control with
mild pregnancy induced hypertension.Labour was induced at 38
weeks gestation. She had spontaneous rupture of membranes 24
hours before this trace and clear liquor drained

Late Deceleration and Severe Variable Deceleration
Actions Change maternal position (yes) Immediate cesarean section (no) Exclude cord prolapse (yes) Wait and review as normal patient (no) Administration of tocolytics if the pattern continues (yes) Course and outcome Cesarean section was performed for failed induction of labour. Outcome was female infant weighing 3200 gm. Apgar score was 9/10 at one and five minutes.
The infant followed normal newborn outcome.