elective mutism in immigrant families
TRANSCRIPT
Elective Mutism in Immigrant Families
Susan Bradley, M.D. and Leon Sloman, M.R.C.S., L.R.C.P.
When we found ourselves faced with three cases of elective mutismin children of recent immigrant parents to Canada in a clinic population in which elective mutism is relatively rare, we were forced towonder about the following: are these children more prone to specific kinds of psychoneurotic disorder than a similar population ofEnglish-speaking children? If so, what might be the underlyingreasons for this development?
The recent literature on elective mutism defines the problemdynamically as resulting from a hostile dependent relationship between mother and child, to which a number of factors such as marital disharmony and traumatic experiences contribute (Parker etal., 1960; Reed, 1963; Wright, 1968; Browne et al., 1963; Morris,1953).
Cultural factors in the development of childhood disturbance arenot well defined in the literature. However, it is known thatmembers of immigrant families may undergo considerable stressfollowing arrival in the new country. The lack of familiar clues in anew environment leads to "culture shock," which is characterizedby anxiety and depression, hostility to the inhabitants, and stereotyping of the culture (Wallen, 19(7). Because wives and childrentend to be involuntary immigrants, they are more likely to developa negative attitude toward the host country (Tyhurst, 1951). A variety of factors may influence the family's emotional adjustment,such as mother's acceptance of mobility (Kantor, 19(5), the extentof closeness of relationship system in family of origin (Wittkowerand Fried, 1958; Fried and Lindemann, 1961; Bennis and Slater,19(8), and support networks in the new environment.
In an effort to obtain statistical validation of our clinical impres-
Dr. Bradley is a Lecturer of Psychiatr», and Dr. Sloman Assistant Professor of P~ychiatry, Faculty ofMedicine, University of Toronto. Dr. Bradley is ~tafI psychiatri,t. and Dr. Sloman senior psychiatrist,Clarke lnstitute of Psychiatry. The authors unsh to thank the Toronto Board of Education for their encouragement, help, and cooperation, and Dr. C. D. Websterfor hi, helpful comments.
Reprints may be requestedfrom Dr. L. Sloman, 250 College Street, Toronto M5T I R8, Ontario.
510

Electroe Mutism in Immigrant Families 511
sion of an increased occurrence of electively mute behavior in children from immigrant families, we undertook a school survey.
METHOD
From a predominantly immigrant. non-English-speaking population, six schools were selected. five covering junior kindergarten toGrade 6, and one grades 4, 5, and 6. The percentage of immigrantor non-English-speaking children in these schools ranged from 64to 76 percent. The total number of children in this group was3,777.
In English-speaking areas, there were five other schools, fourcovering junior kindergarten to Grade 6. and one kindergarten toGrade 8. Although the exact percentage of immigrants and nonEnglish-speaking children in these schools was not known, theschool principals estimated that:") percent or fewer came from immigrant or non-English-speaking families. This estimate has beenused throughout our calculations. The total number of children inthis group was 3,088.
Questionnaires were sent to all of the teachers in the elevenschools. requesting the following information on any child whohad. in the preceding year. exhibited "persistent refusal to speak inclass, while speaking at home": (I) his initials, (2) age, (3) grade, (4)country of origin, (5) language spoken in the home. (6) length oftime mute (whole year or part thereof). and (7) date of entry toCanada. if known. Sex was omitted because the literature showedno sex bias in the incidence of elective mutism. Attempts weremade to clarify the definition through discussions with the principals, who relayed information to the teachers. These talks werealso used to exclude doubtful cases, most principals being acquainted with the mute children in their school. Simple non-
familiarity with English as a cause o] mutism was excluded through theinstructions conveyed to the teachers that, although mute, the children understood English and responded nonuerballs to English.
No distinction has been made in the sample between childrenborn in Canada who arc from immigrant families, and those whoimmigrated to Canada with their families. "Immigrant," in thisstudy, includes all children from non-English-speaking families. aswell as those who have come from the Caribbean islands, for whomit is felt the cultural change might be significant enough to producesome effects of culture shock (Nicol. 1971), Children of familiesfrom U.S.A., U.K., Australia, etc., have not been included ill the
512 S usan B radley and Leon Sloman
immigran t sam pie, as the effect of cultu ral ch anges in I he se situalions was felt to be less sign ifica nt.
RES ULTS
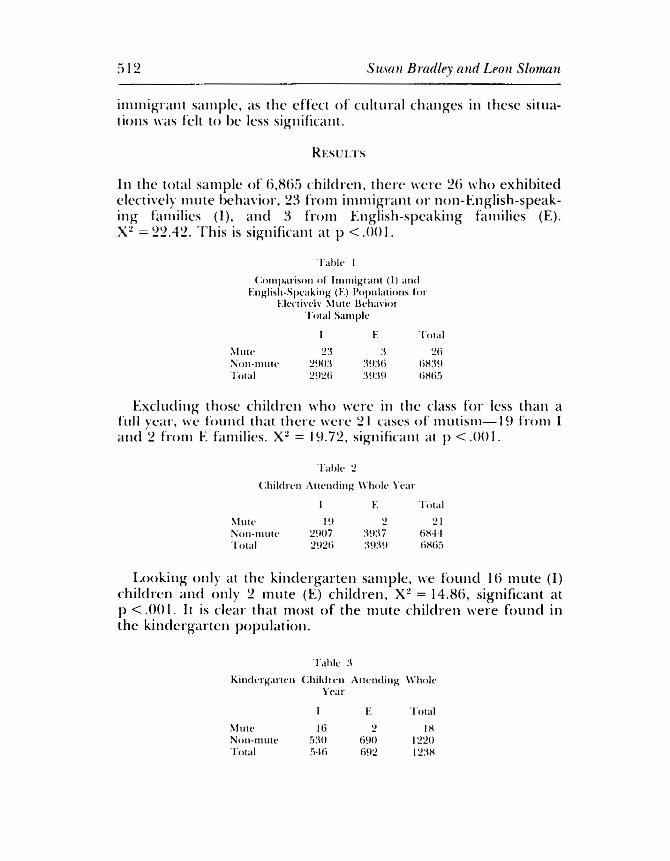
In the total sa m p le of 6,H65 children . th ere were 26 who exhibitedelectively mute behavior , 2 :~ from immigrant or non-English-speaking families (I ), a nd 3 from English -speaking families (E).X~ = 22.42 . This is sign ifir a n t a t P < .00 I.
T ahle I
Co m pa rison of lnunigrant (I) andEngl ish -Speaking (E) Populat ions for
Ekxtivelv Mute Beh aviorT,;tal Sample
E T ot al
~Iute 2:\ :\ 26:'\i oll-lllllt e 2'10 :\ :\ !l:\ l i l iH:HITota l 2~ J2 f ; :\ !I:\ !1 liHli 5
Excluding th ose ch ild re n who were in th e class for less than afull yea I ' , we fou nd that there were ~ I cases or mUlism-19 Irom Iand 2 from E families. X~ = 19.72. sign ifica nt at P < .00 I.
T ahl e 2
Chi ld re n Att ending \\ 'h ole Year
E Tota l
~Iut e
Nnn- murcTOla l
I !I2!IOi2!12(i
:\!l:1i:\!I:\!l
2 16H'j.JliHli :J
Looking only at the kindergarten sample. we found I() mute (I)children and only 2 mute (E) children, X~ = 14.H6. significant a tp < .00 I, It is clear that most of the mute ch ild ren were found inthe kindergarten population.
Tahle :\
Kind erg urten Children Attend ing Wh okYear
E Total
M Ull ' IIi 2 IHNon-m u te 5:10 6!10 1220Total [',46 692 12:\H

Elective Mutism in Immigrant Families
DISCUSSION
513
The preponderance of mute behavior in the kindergartens mightmake one wonder whether we were in fact dealing with true electively mute behavior. It could be argued that this was simply aform of bashfulness in children who did not understand English.However, discussions with the teachers ruled out simple nonfamiliarity with English, as these children could perform adequately on a nonverbal level in an English-speaking class. Inaddition, the persistence of this behavior for at least one schoolyear in the majority of the children leads us to believe that we aredealing with a continuum-the more resistant and presumablymore pathological cases being the ones referred to psychiatric clinics, while the milder forms usually respond in the school setting. Inspite of the assumption that the child's degree of pathology is animportant variable, we recognize that other factors such as theteacher's ability to communicate with immigrant children may playa major role.
In attempting to understand the above findings, we present dataregarding the characteristics of the four immigrant families withelectively mute children in treatment at our clinic. In these moresevere cases, the hostile dependent relationship between motherand child described in the literature was invariably present. It had,however, been exacerbated by the mother's depression and herloneliness on moving to a foreign country. The hostile dependentrelationship was furthered by the mothers' tendency to remainisolated and indifferent to learning the new language. Fear of theunknown further strengthened the pathological bond betweenmother and child, and interfered with the development of normalindependence skills. In mutism, these children centered upon thearea which best fed into the mothers' dreams of return to their native land, as the parents often threatened to send the children backto their own country, where speaking would be no problem.
The above comparison survey and the study of the four clinicchildren involved the assumption that we were dealing with thesame population, although the children demonstrated differingdegrees of severity in the symptoms. Further study of the familiesof the children in our school sample would be necessary to confirmour impressions. In addition, it would be necessary to explore thedifferences between the children and families of those childrenwho began to speak after fairly brief periods of electively mute behavior, and those in whom this behavior persisted.

514 Susan Bradley and Leon Sloman
These findings highlight the plight of the immigrant family.Community programs which aim at helping the immigrant adaptmore quickly are probably less successful in reaching the very families who need help most. As the latter are likely to reject all initialoffers to become more integrated into the general society, theypose a real challenge.
CONCLUSION
According to our data, elective mutism is more likely to develop inchildren of immigrant families. Both our survey of the literatureon elective mutism and immigration and our individual case studies indicate that parental reactions to immigration will at times contribute to the characteristic dynamics of elective mutism.
REFERENCES
BAGLEY, C. (1969), A comparative study of mental illness among immigrant groups in Britain. Transcul. Psychiat. Res. Reu., 6: 199-202.
BENNIS, w. G. & SLATER, P. E. (1968), The Temporary Society. New York: Harper & Row,p.89.
BROWNE, E., WILSON, V., & LAYBOURNE, P. C. (1963), Diagnosis and treatment of electivemutism in children. This journal, 2:605-617.
FRIED, M. & LINDEMANN, E. (1961), Sociocultural factors in mental health and illness. Amer.I Orthopsychiat., 31:87-101.
KANTOR, M. B., ed. (1965), Mobility and Mental Health. Springfield, III.: Thomas.MORRIS,.J. V. (1953), Cases of elective mutism. Amer.I Ment. Dejic., 57:661-668.NICOl., R. A. (1971), Psychiatric disorder in the children of Caribbean immigrants. I Child
Psychol. Psychuu., 12:273-287.PARKER, E. B., OLSEN, 1'. F., & THROCKMORTON, M. C. (1960), Social casework with elemen-
tary school children who do not talk in school. Social Wk, 5(2):64-70.REED, G. F. (1963), Elective mutism in children.j", Child Psychol. Psychiat., 4:99-107.TYHURST, 1.. (1951), Displacement and migration. A mer.I Psychiat., 107:561-568.WALLEN, V. (1967), Culture shock and the problem of adjustment to a new overseas environ
ment. Milit. Med., 132:722-725.WITTKOWER, E. D. & FRIED, J. (1958), Some problems of transcultural psychiatry. Int. I Soc.
Psychiat., s:245-252.WRIGHT, H. 1.., JR. (1968), A clinical study of children who refuse to talk in school. ThisJour
nal,7:603-617.