elastophagocytosis: underlying mechanisms and associated cutaneous entities
TRANSCRIPT

REVIEW
Elastophagocytosis: Underlying mechanisms andassociated cutaneous entities
Jinane El-Khoury, MD, Mazen Kurban, MD, and Ossama Abbas, MDBeirut, Lebanon
From
M
Fund
Conf
Acce
Repr
A
934
Elastophagocytosis is the phagocytosis of elastic fibers that can microscopically be seen in the cytoplasm ofhistiocytes, multinucleated giant cells, or both. Generally believed to be a characteristic feature of certaingranulomatous disorders such as annular elastolytic giant cell granuloma or elastolytic disorders such asmid-dermal elastolysis, this feature has also been described in other cutaneous inflammatory conditions,cutaneous malignancies, infectious entities, and secondary to certain medications. The list of diseases thatcan exhibit this peculiar finding on histopathology is long. In this review we attempt to shed light on theavailable literature concerning the pathogenesis of this phenomenon and the plethora of skin conditionsthat exhibit elastophagocytosis. ( J Am Acad Dermatol 2014;70:934-44.)
Key words: elastolysis; elastophagocytosis.
Abbreviations used:
AEGCG: annular elastolytic giant cell granulomaGA: granuloma annulareGMF: granulomatous mycosis fungoidesGSS: granulomatous slack skinIGD: interstitial granulomatous dermatitisMDE: mid-dermal elastolysisMF: mycosis fungoidesMMP: matrix metalloproteinase
Elastophagocytosis is the phagocytosis ofelastic fibers that can microscopically beseen in the cytoplasm of histiocytes, multi-
nucleated giant cells, or both (Fig 1).1-3 This phe-nomenon may be primary or secondary and we willreview the available literature concerning pathogen-esis and diagnostic value of this phenomenon(Table I).
ETIOPATHOGENESISVery few studies have looked at the phenomenon
of elastophagocytosis with an aim at elucidating itsetiopathogenesis.1
Elastic fibers in elastophagocytosisElastic fibers, which are made up of an inner core
of cross-linked elastin proteins surrounded by fibril-lin microfibrils, form an architecturally distinct mesh-work that confers to the skin its elastic recoilproperties.4 The turnover of elastin in an adult isvery low with its half-life probably exceeding thelifespan of the individual.5 This has clinical implica-tions; once these fibers are lost, the skin losesdefinitively its elasticity. In elastophagocytosis,several studies have looked at the ultrastructuralstate of the phagocytosed elastic fibers by trans-mission electron microscopy.1-6 Some studies
the Dermatology Department, American University of Beirut
edical Center.
ing sources: None.
licts of interest: None declared.
pted for publication December 5, 2013.
int requests: Ossama Abbas, MD, Dermatology Department,
merican University of Beirut Medical Center, PO Box 11-0236,
demonstrated that both normal and degeneratedelastin fibers can be seen being actively phagocy-tosed by macrophages in MDE.7-9 This indicates thatelastophagocytosis can be directed against bothnormal and abnormal fibers (Fig 2).
Several factors may contribute to elastic fiberdamage leading to a proinflammatory cascade andelastophagocytosis.9 One possibility may be thatdefective elastic tissue synthesis may lead to elastol-ysis such as seen in x-linked recessive cutis laxa.10
Defective copper metabolism has also been linked toelastolysis in acquired cutis laxa.11 Other implicatedprocesses include autoimmunity and postinflamma-tory elastolysis, in which elastin degradation occursas a result of elastinolytic enzymes.12-14 Elastinolyticenzymes, which include aspartic, cysteine, metallo-,and serine proteinases, can be found in various
Riad El Solh/Beirut 1107 2020, Lebanon. E-mail:
Published online January 21, 2014.
0190-9622/$36.00
� 2014 by the American Academy of Dermatology, Inc.
http://dx.doi.org/10.1016/j.jaad.2013.12.012

J AM ACAD DERMATOL
VOLUME 70, NUMBER 5El-Khoury, Kurban, and Abbas 935
micro-organisms and in snake venom, macrophages,trophoblasts, and pancreatic, polymorphonuclear,and tumor cells. Elastases found in granulocytes areserine proteinases packaged in azurophilic gran-ules.14 Their role in skin disease is not very welldescribed although they may contribute to elastol-ysis and elastophagocytosis that accompanies
CAPSULE SUMMARY
d Elastophagocytosis is the phagocytosisof elastic fibers by histiocytes. It canoccur with various conditions.
d The possible underlying mechanismsleading to elastophagocytosis arediscussed.
d In this review, the different genetic oracquired conditions whereelastophagocytosis may be encounteredare described.
intense neutrophilic inflam-mation in Sweet syndrome.15
Macrophage elastases arematrix metalloproteinases(MMPs) with lower affinityto elastin.14 MMP-12, pro-duced by macrophages, isincreased in skin aging, con-tributes to photo-aged hu-man skin through thecleavage of elastin and otherextracellular matrix compo-nents, and its expression isalso increased in areasdevoid of elastic fibers ingranulomatous skin dis-
eases.16,17 Other types of MMPs, especially MMP-9,have also been implicated in skin disease.18,19However, elastin degradation does not neces-sarily lead to phagocytosis. For instance, photo-aged and chronologically aged skin, which exhibitsdegenerative elastin changes, is seldom associatedwith elastophagocytosis.20 In immunoreactivitystudies of patients with MDE, many have shownthat elastin, but not fibrillin-1, immunoreactivity isreduced in lesional skin.18,19,21,22 The phagocyticactivity against elastic fibers appears then to bedirected against the elastin component and not thefibrillin component in MDE.
It is also well known that several elastin-derivedpeptides have a biologically active role. For instancethe hexapeptide Val-Gly-Val-Ala-Pro-Gly hasbeen shown to exhibit a chemotactic effect onfibroblasts and monocytes,23 whereas kappa-elastinhas marked biological effects on human polymor-phonuclear leurkocytes.24 However, it is notknown whether they specifically triggerelastophagocytosis.
Sun exposure and elastophagocytosisAlthough many studies have shown changes and
degradation in elastic tissue from sun exposure,25-28
the role of sun exposure in triggering elastophago-cytosis is still unclear. There is only circumstantialevidence linking sun exposure and elastophagocy-tosis. For instance, Abbas et al29 demonstratedelastophagocytosis in 5 cases of extragenital lichensclerosus, 4 of which were on sun-exposed areas.
Patroi et al18 suggested that ultraviolet radiationexposure induced MMP-9 expression by fibroblast-like cells that in turn could lead to elastic fiberdegeneration in MDE. In addition, in a study on 21granuloma annulare (GA) cases on sun-exposedskin, elastophagocytosis and elastic fiber loss wasnoted in all cases.1 However, elastophagocytosis is
not indubitably directedagainst sun-damaged elasticfibers as it has beendescribed in several entitiesthat are not always associ-ated with sun expo-sure.2,21,30-32 This possiblyindicates that sun exposureis not the only factor leadingto elastophagocytosis butthat there are other environ-mental and host factors thatmay play a role in its etiopa-thogenesis. In conceptual-izing elastophagocytosis, wecan distinguish: a substrate,
in this case elastic fibers, and an action (phagocy-tosis) carried out by an effecter cell brought on by 1or several triggers leading to elastic fiber loss andexpression of a specific disease (Fig 3).
ENTITIES CONSISTENTLY EXHIBITINGELASTOPHAGOCYTOSISMid-dermal elastolysis
Although many question its existence as adistinct entity, MDE is generally considered to bean acquired disorder of elastic tissue characterizedon histology by selective mid-dermal loss of retic-ular elastic fibers. In 50% of cases, lesions arepreceded by erythema, burning, and urticarialplaques that resolve, leaving a well-demarcatedpatch of fine wrinkling.21 Three types of MDEhave been described: type I (classic type) ischaracterized by well-demarcated patches of finewrinkling; type II features perifollicular papularprotrusions with elastic tissue loss; and type III ischaracterized by reticular erythema andwrinkling.21
In a study of 79 MDE cases, elastophagocytosiswas reported in 29.1% of cases.21 On electronmicroscopy, elastophagocytosis was identified evenwhen it is not always evident on light micro-scopy.7,8,33 It was observed that inflammation degreeon histology parallels the presence of multinucleatedgiant cells and elastophagocytosis, and this is linkedto lesion age: the earlier the biopsy, the more likely itis to find elastophagocytosis.18 In addition, it appearsfrom several reports on type III MDE that focal

Table I. Differential diagnosis of cutaneous lesions with elastophagocytosis
Entities exhibiting elastophagocytosis on microscopy
Entities consistently exhibiting
elastophagocytosis
Entities inconsistently
exhibiting elastophagocytosis
Entities rarely exhibiting
elastophagocytosis
Elastolytic disorders Inflammatory Elastolytic disordersMid-dermal elastolysis GA AnetodermaPapillary-dermal elastolysis LS Acquired cutis laxa
Sarcoidosis PXEInflammatory Linear elastosisActinic granuloma Neoplastic
GMF InflammatoryNeoplastic NXGGranulomatous slack skin Neoplastic Sweet
AFX Morphea
InfectionsCutaneous leishmaniasisBlastomycosisLeprosy
NeoplasticEruptive vellus cystDFKABCC
Medications (CSF, nicorandil)
AFX, Atypical fibroxanthoma; BCC, basal cell carcinoma; CSF, colony-stimulating factor; DF, dermatofibroma; GA, granuloma annulare; GMF,
granulomatous mycosis fungoides; KA, keratoacanthoma; LS, lichen sclerosis; NXG, necrobiotic xanthogranuloma; PXE, pseudoxanthoma
elasticum.
J AM ACAD DERMATOL
MAY 2014936 El-Khoury, Kurban, and Abbas
elastophagocytosis is more frequently observed withmost instances showing the presence of inflamma-tion on histology.34-40
Similar to MDE, Hashimoto and Tye9 describedthe sole case of papillary-dermal elastolysis, which ischaracterized by complete loss of papillary-dermalelastin with elastophagocytosis.
Annular elastolytic giant cell granulomaFirst proposed by Hanke et al,41 the term ‘‘annular
elastolytic giant cell granuloma’’ was proposed forcutaneous annular lesions with the histologic back-ground of multinucleated giant cell infiltrate, elastol-ysis, and elastophagocytosis localized mainly in themid dermis (Fig 4). Thus, AEGCG includes actinicgranuloma, which shares similar clinical and histo-pathological features.6,42 Although some investiga-tors maintain that AEGCG is a variant of GA, manyothers believe that the absence of connective tissuenecrobiosis and the quantitatively dominant elastictissue changes microscopically distinguish AEGCGfrom GA.43 Consequently, although elastophagocy-tosis is a consistent feature of AEGCG detected inevery case, it is not as common in GA cases.42-46
Other microscopic features of AEGCG include a
granulomatous component consisting of multinucle-ated giant cells typically distributed peripherally to acentral zone that lacks elastic tissue. The granulo-matous area often contains fragmented elastic fiberswith easily identifiable elastophagocytosis. A pali-sading arrangement of histiocytes is usually not afeature. Typical solar elastosis in the surroundingtissue is not a consistent feature.42
Granulomatous slack skin diseaseGranulomatous slack skin (GSS), unlike granulo-
matous mycosis fungoides (GMF), is currently recog-nized as a distinct rare variant of mycosis fungoides(MF).47-50 It usually presents initially as asymptomatic,erythematous papules and plaques that progress,with elastic tissue loss, to boggy pendulous folds ofredundant skin commonly on inguinal and axillaryregions of Caucasian men in their third to fifthdecades of life.47-50 Lesions may grow de novo orless commonly manifest within a background ofpatch- or plaque-stage MF. Classic histologic featuresinclude dense diffuse dermal infiltrate of atypical,irregular, and convoluted lymphocytes that mayextend to the subcutaneous tissue (Fig 5).Numerous histiocytes and multinucleate giant cells

Fig 1. Elastophagocytosis: phagocytosis of elasticfibers that microscopically appear in the cytoplasm ofhistiocytes, multinucleated giant cells, or both. (Hematox-ylin-eosin stain; original magnification: 340. Inset,Verhoeff-van Gieson stain; original magnification: 340.)
J AM ACAD DERMATOL
VOLUME 70, NUMBER 5El-Khoury, Kurban, and Abbas 937
are present diffusely in the dermis and display prom-inent elastophagocytosis and lymphophagocytosis.Loss of elastic fibers is a universal finding in GSS andusually correlates with the extent of the granuloma-tous infiltrate. Elastophagocytosis is a very consistentfeature that has been described in more than half ofthe cases reported and usually contributes to thewidespread dermal elastic tissue loss. An ultrastruc-tural study showed that the majority of the elasticfibers that undergo elastophagocytosis in GSS weremorphologically abnormal or degenerated, and werein contact with multinucleate giant cells by coatedvesicles.50 Based on these results, it seems thatmultinucleated giant cells actively phagocytoseddegenerated elastic fibers by receptor-mediated pino-cytosis. Noncaseating granulomas may even benoted. Epidermotropism andPautrier microabscessesmay be present but are not commonly prominent.
ENTITIES INCONSISTENTLY EXHIBITINGELASTOPHAGOCYTOSISGranuloma annulare
Histologically, GA is essentially characterized byeither a palisading granulomatous pattern (granu-lomas surrounding areas of degenerated collagen) orinterstitial granulomatous pattern with increasedmucin deposition (Fig 6). The presence of elasto-phagocytosis in GA varied in different studies. In 1study,31 18 of 50 (36%) GA cases exhibited elasto-phagocytosis, including 11 of 13 (84.6%) generalizedGA cases. In another study of localized GA, 6 of 32(18.75%) cases exhibited elastophagocytosis. As pre-viously mentioned, Ragaz and Ackerman1 reported21 GA cases on sun-exposed skin exhibiting elasto-phagocytosis. Hanna et al44 reported elastophago-cytosis in 2 of 10 (20%) cases whereas it was seen in 4of 10 cases on electron microscopy. In another study
on 38 GA biopsy specimens, elastic tissue changeswere noted in 100% of cases whereas only 2exhibited elastophagocytosis.2 On the other hand,elastophagocytosis was not described in 2 largeseries comprising together more than 400 biopsyspecimens of GA.45,46
Granulomatous MFGMF is a rare histopathological MF variant that
shares overlapping histologic features with GSS(Fig 7) and differs only clinically from it by thedevelopment of bulky skin folds in GSS.48,49,51
Histologically, prominent granulomatous compo-nent may obscure the atypical lymphoid infiltrate inGMF leading to delayed diagnosis. Epidermotropiclymphocytesmaynot always beprominent. Althoughnot as prominent as GSS, elastic fiber changes andelastophagocytosis may also be encountered inGMF.48,49,51 In a recent study, although multinucle-ated giant cells were seen in 22 of 27 GMF biopsyspecimens, elastophagocytosis was only present in5.51 In another study, although elastic fiber loss wasobserved in all 12 GMF cases, only 1 (8%) demon-strated elastophagocytosis.49 In both GMF and GSS,the cytokines released by neoplastic T cellsmay cause activation of histiocytes with subsequentelastolysis and elastophagocytosis.48
SarcoidosisHistologically, sarcoidosis classically exhibits
naked sarcoidal granulomas.52 However, additionalhistologic findings including elastophagocytosis maybe seen. In a study by Ball et al52 the authorsreviewed 28 biopsy specimens of sarcoidosis andnoted elastophagocytosis in 11 (39%) cases with noassociated solar elastosis.
Lichen sclerosusElastophagocytosis has recently been described in
7 of 35 (20%) cases of lichen sclerosis, all of whichwere extragenital.29 Moreover 4 of the 5 cases werelocated on sun-exposed skin. Elastophagocytosismay thus be contributing to the elastic fiber lossclassically seen in the dermal homogenized zone oflichen sclerosis, which may also be mediated byother factors such as inflammatory cell-mediatedelastase enzymatic digestion.
Atypical fibroxanthomaAtypical fibroxanthoma is a rare cutaneous
neoplasm that primarily occurs in older individualson sun-exposed skin. Histopathologically, thisnonencapsulated dermal tumor is composed oflarge, spindle-shaped and anaplastic cells arrangedin fascicles. Elastophagocytosis has been shown to

Fig 2. Scenarios explaining the phagocytosis of ultrastructurally normal elastic fibers. Scenario1: Activated macrophages phagocytose ultrastructurally normal elastic fibers leading to theirdegradation. Scenario 2: Secondary alteration of ultrastructurally normal elastic fibers leading toactivation of macrophages and elastophagocytosis. Scenario 3: Primary alteration of elasticfibers leading to activation of macrophages and elastophagocytosis. UV, Ultraviolet.
J AM ACAD DERMATOL
MAY 2014938 El-Khoury, Kurban, and Abbas
occur more frequently in association with the in-flammatory infiltrate surrounding this tumor whencompared with other epithelial neoplasms.3 In fact adermal granulomatous inflammation was seen in 7 of9 atypical fibroxanthoma biopsy specimens of which5 exhibited elastophagocytosis.3
ENTITIES RARELY/INCIDENTALLYEXHIBITING ELASTOPHAGOCYTOSISCutaneous infections associated withelastophagocytosis
Probably owing to the granulomatous inflamma-tion associated with some cutaneous infections, andthe ability of neutrophils and several types of micro-organisms to secrete elastases andmodify the dermalelastic fiber network,14 elastophagocytosis has been
associated with numerous infections includingleprosy,53 granulomatous syphilis,1 North-Americanblastomycosis,30 bacterial folliculitis, and cutaneousleishmaniasis.54
Drug-induced elastophagocytosisNicorandil is an antianginal vasodilator that has
been associated with ulcerations of the ocularepithelium, gastrointestinal tract, and skin that may,at times, be life-threatening.55-58 A recent reportdescribes a 78-year-old patient with flexural psoriasiswho developed ulceration while on nicorandil.59 Onbiopsy specimen, 1 of the lesions exhibited an ulcerwith prominent elastophagocytosis in the surround-ing dermis. The ulcers eventually healed spontane-ously after discontinuation of the medication.
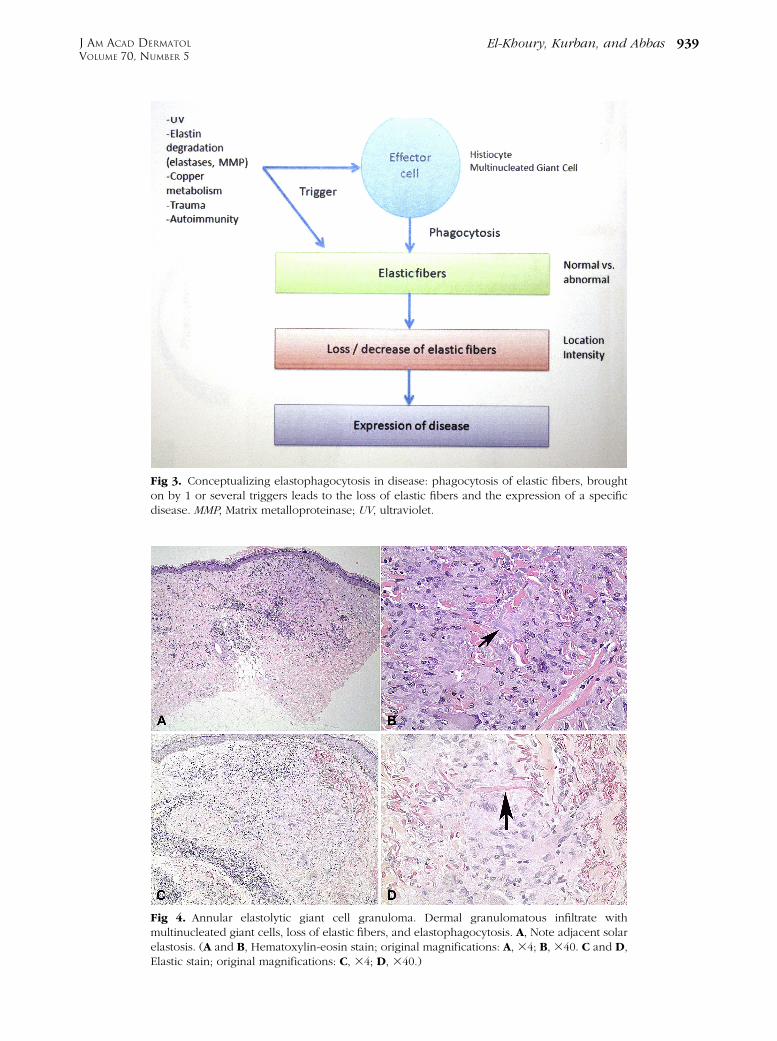
Fig 4. Annular elastolytic giant cell granuloma. Dermal granulomatous infiltrate withmultinucleated giant cells, loss of elastic fibers, and elastophagocytosis. A, Note adjacent solarelastosis. (A and B, Hematoxylin-eosin stain; original magnifications: A, 34; B, 340. C and D,Elastic stain; original magnifications: C, 34; D, 340.)
Fig 3. Conceptualizing elastophagocytosis in disease: phagocytosis of elastic fibers, broughton by 1 or several triggers leads to the loss of elastic fibers and the expression of a specificdisease. MMP, Matrix metalloproteinase; UV, ultraviolet.
J AM ACAD DERMATOL
VOLUME 70, NUMBER 5El-Khoury, Kurban, and Abbas 939

Fig 5. Granulomatous slack skin. Dense diffuse dermal infiltrate of atypical convolutedlymphocytes that extend to subcutaneous tissue with epidermotropism. Numerous histiocytesand multinucleate giant cells are present and display prominent elastophagocytosis. (A to D,Hematoxylin-eosin stain; original magnifications: A, 34; B, 310; C and D, 340.)
J AM ACAD DERMATOL
MAY 2014940 El-Khoury, Kurban, and Abbas
Granulocyte colony-stimulating factor is a cyto-kine that stimulates the proliferation and differenti-ation of the granulocytic progenitor cells. Interstitialgranulomatous dermatitis (IGD) has been reportedto occur with granulocyte colony-stimulating factortreatment and elastophagocytosis was noted in 3cases of granulocyte colony-stimulating factoreas-sociated IGD.60,61 The authors postulate that
elastophagocytosis is more likely to be linked tothe IGD that to the drug itself.61
Penicillamine is a copper chelator used in thetreatment of Wilson disease. At high doses, it has theability to distort elastic fibers leading topenicillamine-associated dermopathies.62 In 1 casereport, a 36-year-old man with Wilson disease onhigh-dose penicillamine developed lesions of
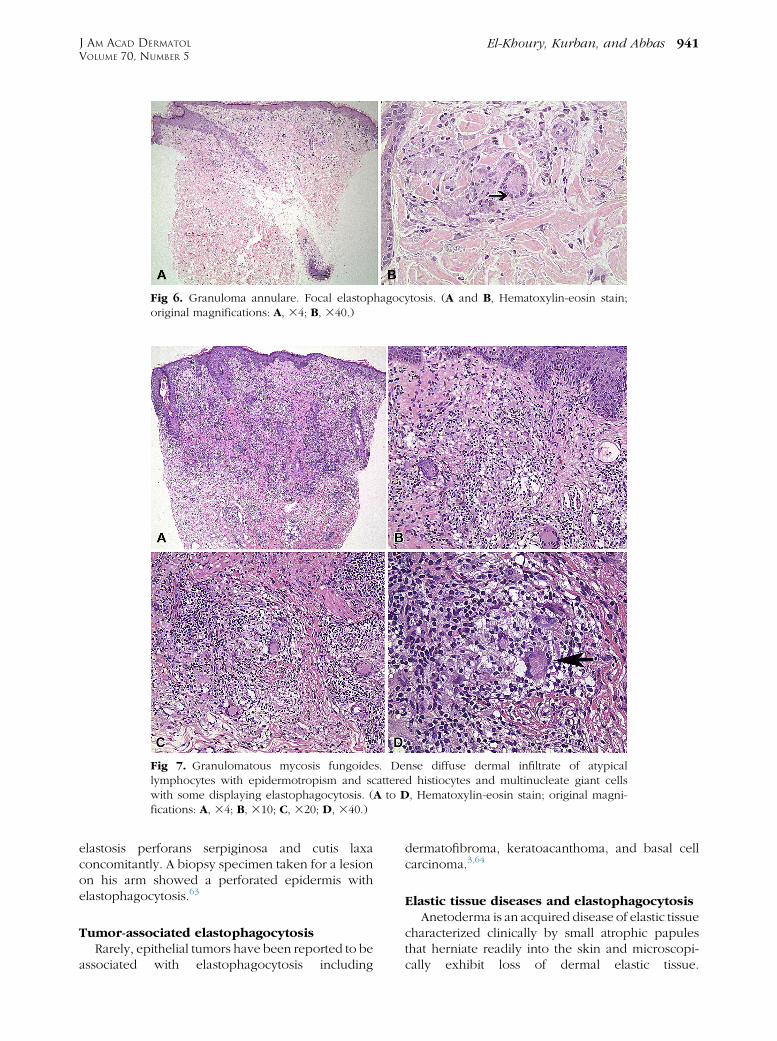
Fig 7. Granulomatous mycosis fungoides. Dense diffuse dermal infiltrate of atypicallymphocytes with epidermotropism and scattered histiocytes and multinucleate giant cellswith some displaying elastophagocytosis. (A to D, Hematoxylin-eosin stain; original magni-fications: A, 34; B, 310; C, 320; D, 340.)
Fig 6. Granuloma annulare. Focal elastophagocytosis. (A and B, Hematoxylin-eosin stain;original magnifications: A, 34; B, 340.)
J AM ACAD DERMATOL
VOLUME 70, NUMBER 5El-Khoury, Kurban, and Abbas 941
elastosis perforans serpiginosa and cutis laxaconcomitantly. A biopsy specimen taken for a lesionon his arm showed a perforated epidermis withelastophagocytosis.63
Tumor-associated elastophagocytosisRarely, epithelial tumors have been reported to be
associated with elastophagocytosis including
dermatofibroma, keratoacanthoma, and basal cellcarcinoma.3,64
Elastic tissue diseases and elastophagocytosisAnetoderma is an acquired disease of elastic tissue
characterized clinically by small atrophic papulesthat herniate readily into the skin and microscopi-cally exhibit loss of dermal elastic tissue.
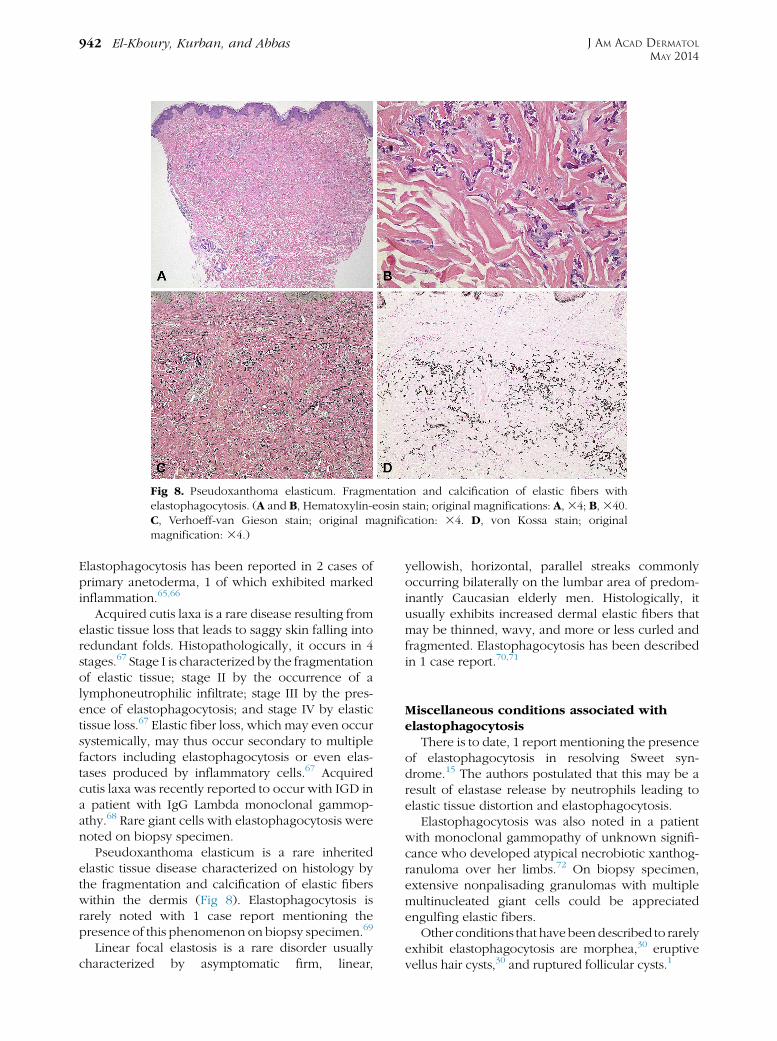
Fig 8. Pseudoxanthoma elasticum. Fragmentation and calcification of elastic fibers withelastophagocytosis. (A and B, Hematoxylin-eosin stain; original magnifications: A,34; B,340.C, Verhoeff-van Gieson stain; original magnification: 34. D, von Kossa stain; originalmagnification: 34.)
J AM ACAD DERMATOL
MAY 2014942 El-Khoury, Kurban, and Abbas
Elastophagocytosis has been reported in 2 cases ofprimary anetoderma, 1 of which exhibited markedinflammation.65,66
Acquired cutis laxa is a rare disease resulting fromelastic tissue loss that leads to saggy skin falling intoredundant folds. Histopathologically, it occurs in 4stages.67 Stage I is characterized by the fragmentationof elastic tissue; stage II by the occurrence of alymphoneutrophilic infiltrate; stage III by the pres-ence of elastophagocytosis; and stage IV by elastictissue loss.67 Elastic fiber loss, which may even occursystemically, may thus occur secondary to multiplefactors including elastophagocytosis or even elas-tases produced by inflammatory cells.67 Acquiredcutis laxa was recently reported to occur with IGD ina patient with IgG Lambda monoclonal gammop-athy.68 Rare giant cells with elastophagocytosis werenoted on biopsy specimen.
Pseudoxanthoma elasticum is a rare inheritedelastic tissue disease characterized on histology bythe fragmentation and calcification of elastic fiberswithin the dermis (Fig 8). Elastophagocytosis israrely noted with 1 case report mentioning thepresence of this phenomenon on biopsy specimen.69
Linear focal elastosis is a rare disorder usuallycharacterized by asymptomatic firm, linear,
yellowish, horizontal, parallel streaks commonlyoccurring bilaterally on the lumbar area of predom-inantly Caucasian elderly men. Histologically, itusually exhibits increased dermal elastic fibers thatmay be thinned, wavy, and more or less curled andfragmented. Elastophagocytosis has been describedin 1 case report.70,71
Miscellaneous conditions associated withelastophagocytosis
There is to date, 1 report mentioning the presenceof elastophagocytosis in resolving Sweet syn-drome.15 The authors postulated that this may be aresult of elastase release by neutrophils leading toelastic tissue distortion and elastophagocytosis.
Elastophagocytosis was also noted in a patientwith monoclonal gammopathy of unknown signifi-cance who developed atypical necrobiotic xanthog-ranuloma over her limbs.72 On biopsy specimen,extensive nonpalisading granulomas with multiplemultinucleated giant cells could be appreciatedengulfing elastic fibers.
Other conditions that havebeendescribed to rarelyexhibit elastophagocytosis are morphea,30 eruptivevellus hair cysts,30 and ruptured follicular cysts.1

J AM ACAD DERMATOL
VOLUME 70, NUMBER 5El-Khoury, Kurban, and Abbas 943
ConclusionAlthough elastophagocytosis may represent a
nonspecific incidental process seen in various dis-eases, this phenomenon appears to be a character-istic reproducible feature of distinctive entities suchas MDE, AEGCG, or GSS, and may thus serve as ahelpful clue to their diagnosis. As for etiopatho-genesis, elastophagocytosis may result from diverseinitiating events that reveal the antigenicity of elasticfibers and trigger a cascade of events that lead to acellular immune response and eventually phagocy-tosis of elastin. However, there are still manyquestions that remain unanswered and need furtherclarification in future studies: what triggers thephagocytosis of normal and abnormal elastic tissue?What is the role of ultraviolet light? What are theintrinsic factors that render elastin antigenic?
REFERENCES
1. Ragaz A, Ackerman AB. Is actinic granuloma a specific
condition? Am J Dermatopathol 1979;1:43-50.
2. Gunes P, Goktay F, Mansur AT, Koker F, Erfan G. Collagen-e-
lastic tissue changes and vascular involvement in granuloma
annulare: a review of 35 cases. J Cutan Pathol 2009;36:838-44.
3. Sweeney EC, McDermott M. Tumor-related cutaneous elas-
tophagocytosis. J Clin Pathol 1996;49:81-3.
4. Baldwin AK, Simpson A, Steer R, Cain SA, Kielty CM. Elastic
fibers in health and disease. Expert Rev Mol Med 2013;15:e8.
5. Sandberg LB, Soskel NT, Wolt TB. Structure of the elastic fiber:
an overview. J Invest Dermatol 1982;79:128s-32s.
6. O’Brien JP. Actinic granuloma: an annular connective tissue
disorder affecting sun- and heat-damaged (elastotic) skin.
Arch Dermatol 1975;111:460-6.
7. Harmon CB, Su WP, Gagne EJ, Fransway AF, Zelickson BD.
Ultrastructural evaluation of mid-dermal elastolysis. J Cutan
Pathol 1994;21:233-8.
8. Fimiani M, Mazzatenta C, Alessandrini C, Paola M, Paola C,
Andreassi L. Mid-dermal elastolysis: an ultrastructural and
biochemical study. Arch Dermatol Res 1995;287:152-7.
9. Hashimoto K, Tye MJ. Upper dermal elastolysis: a compara-
tive study with mid-dermal elastolysis. J Cutan Pathol 1994;
21:533-40.
10. Byers PH, Narayanan AS, Bornstein P, Hall JG. An X-linked
form of cutis laxa due to deficiency of lysyl oxidase. Birth
Defects Orig Artic Ser 1976;12:293-8.
11. Reed WB, Horowitz RE, Beighton P. Acquired cutis laxa:
primary generalized elastolysis. Arch Dermatol 1971;103:
661-9.
12. Gambichler T, Linhart C, Wolter M. Mid-dermal elastolysis
associated with Hashimoto’s thyroiditis. J Eur Acad Dermatol
Venereol 1999;12:245-9.
13. Kirsner RS, Falanga V. Features of an autoimmune process in
mid-dermal elastolysis. J Am Acad Dermatol 1992;27:832-4.
14. Werb Z, Banda MJ, McKerrow JH, Sandhaus RA. Elastases and
elastin degradation. J Invest Dermatol 1982;79:154s-9s.
15. Loo WJ, Rytina E, Banfield C. Elastophagocytosis: a feature of
resolving Sweet’s syndrome. J Eur Acad Dermatol Venereol
2004;18:471-3.
16. Taddese S, Weiss AS, Neubert RH, Schmelzer CE. Mapping of
macrophage elastase cleavage sites in insoluble human skin
elastin. Matrix Biol 2008;27:420-8.
17. Vaalamo M, Kariniemi AL, Shapiro SD, Saarialho-Kere U.
Enhanced expression of human metalloelastase (MMP-12)
in cutaneous granulomas and macrophage migration.
J Invest Dermatol 1999;112:499-505.
18. Patroi I, Annessi G, Girolomoni G. Mid-dermal elastolysis: a
clinical, histologic, and immunohistochemical study of 11
patients. J Am Acad Dermatol 2003;48:846-51.
19. Suda T, Hara H, Yoshitake M, Ohbayashi T, Nakamura T, Terui
T. Immunohistochemical investigation of mid-dermal elastol-
ysis with a history of erythema. Am J Dermatopathol 2008;30:
477-80.
20. Suwabe H, Serizawa A, Kajiwara H, Ohkido M, Tsutsumi Y.
Degenerative processes of elastic fibers in sun-protected and
sun-exposed skin: immunoelectron microscopic observation
of elastin, fibrillin-1, amyloid P component, lysozyme and
alpha1-antitrypsin. Pathol Int 1999;49:391-402.
21. Gambichler T. Mid-dermal elastolysis revisited. Arch Dermatol
Res 2010;302:85-93.
22. Thorneby K, Sakai L, Dahlback K. Middermal elastolysis:
report of a case and immunohistochemical studies on the
dermal distribution of fibrillin, vitronectin and amyloid P
component. Acta Derm Venereol 1991;71:1-5.
23. Senior RM, Griffin GL, Mecham RP, Wrenn DS, Prasad KU, Urry
DW. Val-Gly-Val-Ala-Pro-Gly, a repeating peptide in elastin, is
chemotactic for fibroblasts and monocytes. J Cell Biol 1984;
99:870-4.
24. Hauck M, Seres I, Kiss I, Saulnier J, Mohacsi A, Wallach J, et al.
Effects of synthesized elastin peptides on human leukocytes.
Biochem Mol Biol Int 1995;37:45-55.
25. Bernstein EF, Underhill CB, Hahn PJ, Brown DB, Uitto J. Chronic
sun exposure alters both the content and distribution of
dermal glycosaminoglycans. Br J Dermatol 1996;135:255-62.
26. Cavarra E, Fimiani M, Lungarella G, Andreassi L, de Santi M,
Mazzatenta C, et al. UVA light stimulates the production of
cathepsin G and elastase-like enzymes by dermal fibroblasts:
a possible contribution to the remodeling of elastotic areas
in sun-damaged skin. Biol Chem 2002;383:199-206.
27. BrennanM, Bhatti H, Nerusu KC, Bhagavathula N, Kang S, Fisher
GJ, et al. Matrix metalloproteinase-1 is the major collagenolytic
enzyme responsible for collagen damage in UV-irradiated
human skin. Photochem Photobiol 2003;78:43-8.
28. Seite S, Zucchi H, Septier D, Igondjo-Tchen S, Senni K,
Godeau G. Elastin changes during chronological and
photo-ageing: the important role of lysozyme. J Eur Acad
Dermatol Venereol 2006;20:980-7.
29. Abbas O, Chatrath V, Goldberg LJ. Elastophagocytosis in
extragenital lichen sclerosus. J Cutan Pathol 2010;37:1032-7.
30. Barnhill RL, Goldenhersh MA. Elastophagocytosis: a
non-specific reaction pattern associated with inflammatory
processes in sun-protected skin. J Cutan Pathol 1989;16:
199-202.
31. Burket JM, Zelickson AS. Intracellular elastin in generalized
granuloma annulare. J Am Acad Dermatol 1986;14:975-81.
32. Friedman-Birnbaum R, Weltfriend S, Kerner H, Lichtig C.
Elastic tissue changes in generalized granuloma annulare.
Am J Dermatopathol 1989;11:429-33.
33. Neri I, Patrizi A, Fanti PA, Passarini B, Badiali-De Giorgi L,
Varotti C. Mid-dermal elastolysis: a pathological and ultra-
structural study of five cases. J Cutan Pathol 1996;23:165-9.
34. Bannister MJ, Rubel DM, Kossard S. Mid-dermal elastopha-
gocytosis presenting as a persistent reticulate erythema.
Australas J Dermatol 2001;42:50-4.
35. Cutillas E, Ferrando FJ, Marti ME, Mateu A, Rausell N. Reticular
variant of mid-dermal elastolysis after insertion of a pace-
maker. Clin Exp Dermatol 2010;35:498-500.
J AM ACAD DERMATOL
MAY 2014944 El-Khoury, Kurban, and Abbas
36. Gambichler T, Lubbe J. Reticular variant of mid-dermal
elastolysis accompanied by persistent urticarial lesions.
J Dermatol 2012;39:963-5.
37. Hillen U. Reticular erythema with focal mid-dermal elasto-
phagocytosis (REMDE). J Dtsch Dermatol Ges 2008;6:857-9.
38. Martin LK, Kossard S, Murrell DF. Reticular variant of
mid-dermal elastolysis. Am J Dermatopathol 2008;30:287-90.
39. Meyer A, Aaron D, Perry A, Guill M III. Erythematous reticular
patches: a rare presentation of mid-dermal elastolysis. J Am
Acad Dermatol 2012;67:e216-7.
40. Posada C, No N, De La Torre C, Florez A. Reticular variant of
mid-dermal elastolysis. Australas J Dermatol 2013;54:69-71.
41. Hanke CW, Bailin PL, Roenigk HH Jr. Annular elastolytic giant
cell granuloma: a clinicopathologic study of five cases and a
review of similar entities. J Am Acad Dermatol 1979;1:413-21.
42. Limas C. The spectrum of primary cutaneous elastolytic
granulomas and their distinction from granuloma annulare:
a clinicopathological analysis. Histopathology 2004;44:277-82.
43. Al-Hoqail IA, Al-Ghamdi AM, Martinka M, Crawford RI. Actinic
granuloma is a unique and distinct entity: a comparative
study with granuloma annulare. Am J Dermatopathol 2002;
24:209-12.
44. Hanna WM, Moreno-Merlo F, Andrighetti L. Granuloma
annulare: an elastic tissue disease? Case report and literature
review. Ultrastruct Pathol 1999;23:33-8.
45. Dabski K, Winkelmann RK. Generalized granuloma annulare:
histopathology and immunopathology. Systematic review of
100 cases and comparison with localized granuloma annu-
lare. J Am Acad Dermatol 1989;20:28-39.
46. Umbert P, Winkelmann RK. Histologic, ultrastructural and
histochemical studies of granuloma annulare. Arch Dermatol
1977;113:1681-6.
47. Shah A, Safaya A. Granulomatous slack skin disease: a review,
in comparison with mycosis fungoides. J Eur Acad Dermatol
Venereol 2012;26:1472-8.
48. LeBoit PE, Zackheim HS, White CR Jr. Granulomatous variants
of cutaneous T-cell lymphoma: the histopathology of gran-
ulomatous mycosis fungoides and granulomatous slack skin.
Am J Dermatopathol 1988;12:83-95.
49. Kempf W, Ostheeren-Michaelis S, Paulli M, Lucioni M,
Wechsler J, Audring H, et al. Granulomatous mycosis
fungoides and granulomatous slack skin: a multicenter study
of the cutaneous lymphoma histopathology task force croup
of the European Organization For Research and Treatment of
Cancer (EORTC). Arch Dermatol 2008;144:1609-17.
50. Tsuruta D, Kono T, Kutsuna H, Yashiro N, Ishii M. Granulo-
matous slack skin: an ultrastructural study. J Cutan Pathol
2001;28:44-8.
51. Li JY, Pulitzer MP, Myskowski PL, Dusza SW, Horwitz S,
Moskowitz A, et al. A case-control study of clinicopathologic
features, prognosis, and therapeutic responses in patients
with granulomatous mycosis fungoides. J Am Acad Dermatol
2013;69:366-74.
52. Ball NJ, Kho GT, Martinka M. The histologic spectrum of
cutaneous sarcoidosis: a study of twenty-eight cases. J Cutan
Pathol 2004;31:160-8.
53. Barbosa AA Jr, Guimar~aes NS, Follador I, Sarno LS, Pereira CP.
Leprosy combined with elastolytic granuloma. An Bras
Dermatol 2002;77:585-92.
54. Boer A, Blodorn-Schlicht N, Wiebels D, Steinkraus V, Falk TM.
Unusual histopathological features of cutaneous
leishmaniasis identified by polymerase chain reaction specific
for Leishmania on paraffin-embedded skin biopsies. Br J
Dermatol 2006;155:815-9.
55. Fraunfelder FW, Fraunfelder FT. Conjunctival and corneal
ulceration associated with nicorandil. Cutan Ocul Toxicol doi:
10.3109/15569527.2013.811248. Published online July 10,
2013.
56. Carlile A, Sheikh E, Shakeel M, Maini SK. Nicorandil associated
pinna ulceration: a new entity for an otolaryngologist. Am J
Otolaryngol 2013;34:586-8.
57. Robinson A, Baker P, Stevenson H. Nicorandil as a cause of
perineal ulceration. Ulster Med J 2012;81:97.
58. Mosley F, Bhasin N, Davies JB, Ausobsky JR. Life-threatening
hemorrhage secondary to nicorandil-induced severe
peri-anal ulceration. Ann R Coll Surg Engl 2010;92:W39-40.
59. Wong T, Swain F, Calonge E. Nicorandil-associated perianal
ulceration with prominent elastophagocytosis and flexural
ulceration. Br J Dermatol 2005;152:1360-1.
60. Alvarez-Ruiz S, Penas PF, Fernandez-Herrera J, Sanchez-Perez
J, Fraga J, Garcia-Diez A. Maculopapular eruption with
enlarged macrophages in eight patients receiving G-CSF or
GM-CSF. J Eur Acad Dermatol Venereol 2004;18:310-3.
61. Ferran M, Gallardo F, Salar A, Iglesias M, Barranco C, Pujol RM.
Granulomatous dermatitis with enlarged histiocytes: a char-
acteristic pattern of granulocyte colony-stimulating factor.
Report of two cases and review of the literature. Derma-
tology 2006;212:188-93.
62. Ishak R, Abbas O. Penicillamine revisited: historic overview
and review of the clinical uses and cutaneous adverse effects.
Am J Clin Dermatol 2013;14:223-33.
63. Hill VA, Seymour CA, Mortimer PS. Pencillamine-induced
elastosis perforans serpiginosa and cutis laxa in Wilson’s
disease. Br J Dermatol 2000;142:560-1.
64. Kiyohara T, Kumakiri M, Kobayashi H, Ohkawara A, Lao LM.
Atrophic dermatofibroma: elastophagocytosis by the tumor
cells. J Cutan Pathol 2000;27:312-5.
65. Kossard S, Kronman KR, Dicken CH, Schroeter AL. Inflamma-
tory macular atrophy: immunofluorescent and ultrastructural
findings. J Am Acad Dermatol 1979;1:325-34.
66. Zaki I, Scerri L, Nelson H. Primary anetoderma: phagocytosis
of elastic fibers by macrophages. Clin Exp Dermatol 1994;19:
388-90.
67. Lewis KG, Bercovitch L, Dill SW, Robinson-Bostom L. Acquired
disorders of elastic tissue, part II: decreased elastic tissue.
J Am Acad Dermatol 2004;51:165-85.
68. Silveria L, Torres I, Salvino MA, Follador I, Bittencourt AL.
Acquired cutis laxa with an interstitial granulomatous reac-
tion associated with IgG lambda monoclonal gammopathy.
Am J Dermatopathol 2013;35:e67-71.
69. Loche F, Raynal H, Bazex J. Acne-like eruption induced by
pseudoxanthoma elasticum: effectiveness of liquid nitrogen
cryotherapy. Eur J Dermatol 1998;8:63-5.
70. Tamada Y, Yokochi K, Ikeya T, Nakagomi Y, Miyake T, Hara K.
Linear focal elastosis: a review of three cases in young
Japanese men. J Am Acad Dermatol 1997;36:301-3.
71. Kanitakis B, Chouvet M, Dupin A, Flechaire P. Linear focal
elastosis. Eur J Dermatol 1997;7:300-2.
72. Ito Y, Nishimura K, Yamanaka K, Hakamada A, Isoda K,
Kurokawa I, et al. Necrobiotic xanthogranuloma with para-
proteinemia; an atypical case. J Dtsch Dermatol Ges 2008;6:
40-3.