eit to deliver mechanical ventilation - critical care … · eit - basic principles •electrode...
TRANSCRIPT

EIT to deliver mechanicalventilation
Claude Guérin MD PhDRéanimation MédicaleHôpital de la Croix RousseUniversité de LyonLyon, France
CCF 2
012
1
CCCF October 2012

Disclosure
• Carefusion
2
CCF 2
012

Outline
•Introduction
•Technique
•Applications
•Conclusions
CCF 2
012
3

EIT: an attractive tool
• Non invasive
• Radiation free
• Available at bedside
• Monitoring
• Regional assessment of lung ventilation
CCF 2
012
4
Introduction
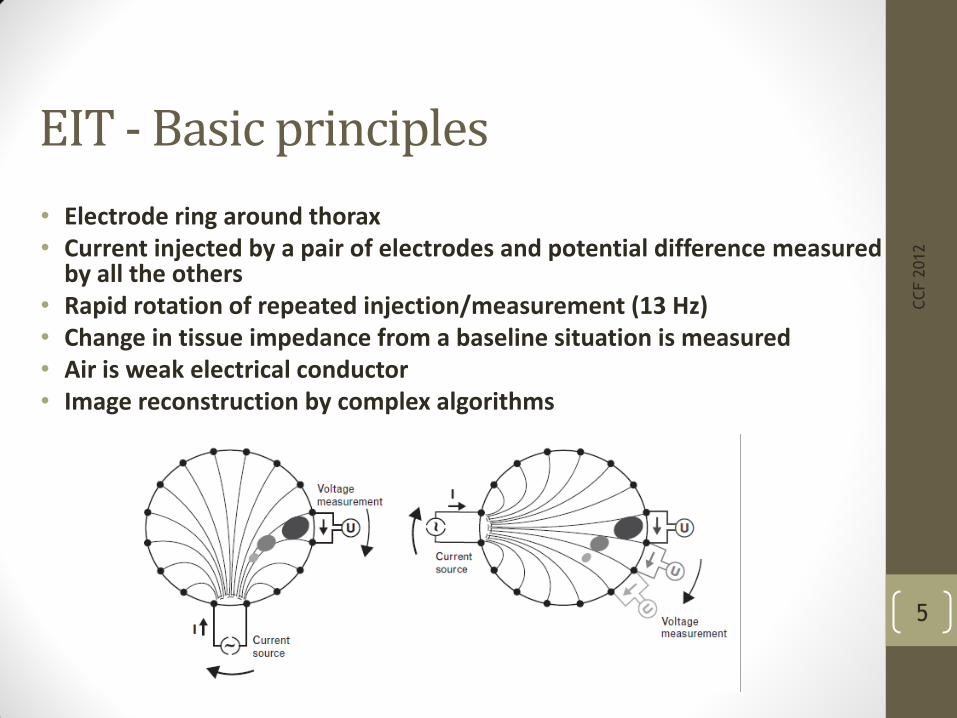
EIT - Basic principles
• Electrode ring around thorax• Current injected by a pair of electrodes and potential difference measured
by all the others• Rapid rotation of repeated injection/measurement (13 Hz)• Change in tissue impedance from a baseline situation is measured • Air is weak electrical conductor • Image reconstruction by complex algorithms
CCF 2
012
5

Low spatial resolution
CCF 2
012
6
Matrix 32 x 32
pixels

High temporal resolution: Impedance-time curves
CCF 2
012
7
Flow (L/min)
Right
Ventral
Dorsal
Left
Ventral
Dorsal
Overall

Impedance-time curves
CCF 2
012
8
flow
ventral
dorsal
R L
1
2
3
4

Validation of Lung Ventilation measurement
9
CCF 2
012
Richard et al. CC 2009
EIT
PET
EIT
PET

Impedance-time curves
CCF 2
012
10
VTeit
EELI
flow
S.I. 40 cm H2O x 40 sec

Functionnal image (fEIT)
CCF 2
012
11

Functionnal image (fEIT)
CCF 2
012
12
Local change
Overall change

Technical issues
Individual calibration attractive and feasible but not
standardized across subjects
Impedance-lung volume relationship depends on patient
morphology
Impedance depends on intracellularand extracellular liquid volume and
pulmonary blood volume
Sampled volume by EIT is limited and sois calibration by using global signal, i.e.
spirometer at the airway opening
Gas cranio-caudal redistribution duringcalibration induces error in local
calibration of impedance change in the plane of the electrode
Relative lung volumes
EIT measures change in impedance relative to reference
(DZ)
Absolute volume is not measured
If reference has changed between tested conditions, same lung volume change may promote
different EIT data
CCF 2
012
13

Applications
CCF 2
012
14

1. EELV measurement
CCF 2
012
15
Bikker ICM 2009 Hinz ICM 2003
Biais 194 ml
Biais 0 ml

2. Regional lung inflation patterns
CCF 2
012
16Hinz EJA 2006
global
regio
nal
VT EIT variation

3. Alveolar recruitment
CCF 2
012
17
AUC
‘slope’: parameter ‘b’ in equation
y = axb + c
RVD: Time to reach a threshold value (10%
of maximum value)
Wrigge CCM 2008
ventral dorsal

CT-assessed recruitment
CCF 2
012
18
Wrigge CCM 2008
r2 = 0.79 indirect ALI
r2 =0.15 direct ALI
AUC
slope
RVD

4. Intra-tidal recruitment
CCF 2
012
19Dargaville
ICM 2010
16 piglets surfactant
depletion
PCV DP=10 cm H2O

VT amplitude and homogeneity
CCF 2
012
20
Dargaville
ICM 2010
Right L
Lavaged Lung
CCF 2
012
21
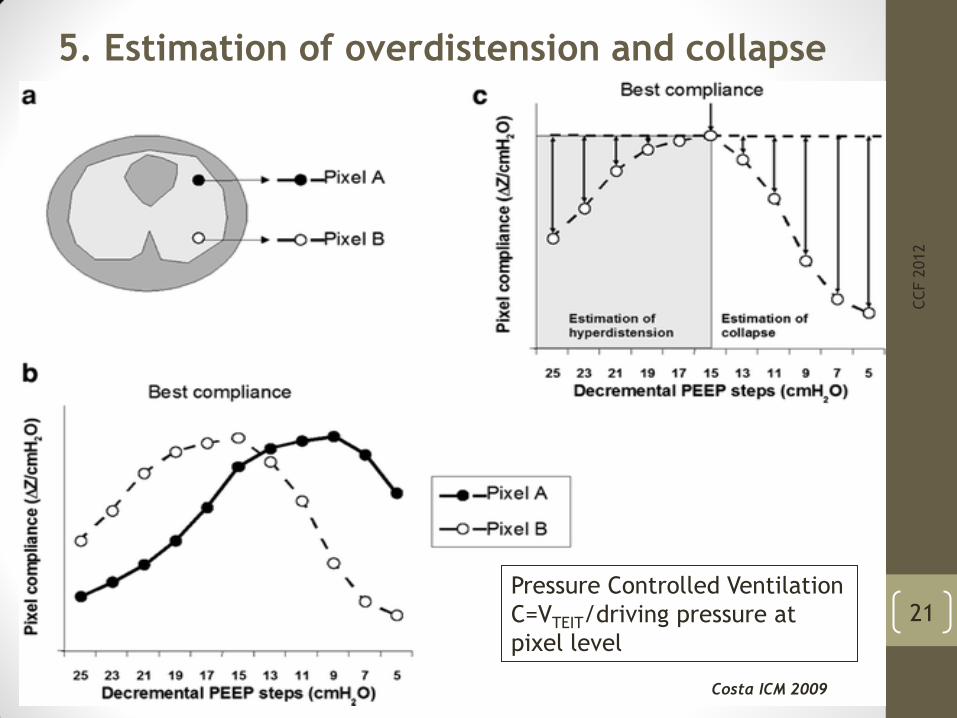
5. Estimation of overdistension and collapse
Costa ICM 2009
Pressure Controlled Ventilation
C=VTEIT/driving pressure at
pixel level

CCF 2
012
22
Costa ICM 2009
5. Estimation of overdistension and collapse

6. Potential for recruitment
CCF 2
012
23Lowhagen 2010

Potential for recruitment
CCF 2
012
24Lowhagen 2010

Potential for recruitment
CCF 2
012
25
Optimal PEEP
PEEP at potential of
recruitment ≤ 10%
Lowhagen 2010

Conclusions
• EIT now available at bedside
• Monitoring tool
• Should allow optimizing ventilator settings and interventions
CCF 2
012
26