efficacy of the self-adjusting file system on cleaning and ... · efficacy of the self-adjusting...
TRANSCRIPT

Basic Research—Technology
Efficacy of the Self-Adjusting File System on Cleaningand Shaping Oval Canals: A Microbiologicaland Microscopic EvaluationAvina Paranjpe, BDS, MS, MSD, PhD,* Cesar de Gregorio, DDS, MS,† Ana Maria Gonzalez, PhD,‡
Arianna Gomez, DDS, MS,‡ Daniel Silva Herzog, PhD,‡ Antonio Arag�on Pi~na, MS, PhD (Eng),§
and Nestor Cohenca, DDS*k
Abstract
Introduction: The shaping ability of root canal instru-ments is determined by a complex interrelationship ofparameters such as cross-sectional design and theability to remove debris and the smear layer. The self-adjusting file (SAF) consists of a hollow, flexible instru-ment in the form of a compressible, thin-walled, pointedcylinder. The aim of this study was to compare the SAFwith the ProTaper rotary file system, evaluating debrisand smear layer removal and the presence of bacteriaby using microbiological and scanning electron micros-copy (SEM) evaluation.Methods: Fifty maxillary premo-lars were inoculated with Enterococcus faecalis for30 days and then randomly distributed into 2 groups.Group 1 was prepared with ProTaper rotary instrumentsand irrigated with 30-gauge side-vented needles. Group2 was prepared by using the SAF system with contin-uous irrigation. Bacteriologic samples were taken beforeand after preparation. All samples were then longitudi-nally split and analyzed under scanning electron micros-copy. The scoring was carried out by 3 blindedevaluators. Results: In group 1, 40% of samples hadnegative cultures with postinstrumentation samplestaken with paper points (S2a) and 45% with postinstru-mentation dentin samples (S2b). In group 2, 20% ofsamples had negative cultures with S2a and 15% withS2b. Intragroup analyses evaluating the reduction inthe number of colony-forming units (CFUs) from S1 toS2a and S2b demonstrated both preparation techniqueswere highly effective (P < .01). Further reduction ofCFUs was observed when comparing S2a and S2b ingroup 1 (P < .05), whereas no difference was observedin group 2. Intergroup analysis demonstrated a statisti-cally significant difference of CFUs at S2a and S2b(P < .05). SEM scores were consistent with the microbi-ology findings. Conclusions: The SAF system does notFrom the *Department of Endodontics and kDepartment of Pedof Advanced Endodontics, Universidad Europea de Madrid, Spain; aM�exico.
Address requests for reprints to Dr Avina Paranjpe, [email protected]/$ - see front matter
Copyright ª 2012 American Association of Endodontists.doi:10.1016/j.joen.2011.10.014
226 Paranjpe et al.
allow control of the apical enlargement, thus limiting the ability of the irrigants toachieve effective and predictable disinfection. (J Endod 2012;38:226–231)
Key WordsBacteria, cleaning efficacy, ProTaper, root canal disinfection, SAF, SEM
Successful endodontic treatment depends on the effectiveness of the cleaning andshaping of the root canal system (1, 2). Any remaining tissue, bacteria, or debris
can contribute to endodontic failure (2). Nickel-titanium (NiTi) rotary instrumenta-tion and the associated files have been studied extensively and are significant adjunctsresponsible for shaping the root canal system (3). Shaping with rotary instruments,however, produces a significant amount of debris and creates a smear layer withinthe root canal system (4). Metzger et al (5) have shown that a 5-mm-thick smearlayer creates a potential gap between the root canal filling and the wall of the rootcanal that is be capable of accommodating approximately 5 layers of bacteria.Many studies have also shown that failure to eliminate the smear layer could affectobturation, which in turn could lead to the failure of treatment (6). In addition,many root canal systems are not round but oval in cross section. Hence, the cylin-drically shaped tapered rotary file systems currently available might not be capable ofremoving the infected dentin of oval-shaped canals, thus hindering the ability toadequately clean and shape the root canal system. Therefore, the ability of the fileto adequately clean and shape the root canal system is influenced by a complex inter-relationship of parameters such as cross-sectional file design, flute design, thesurface treatment of the instrument, and the capacity of the instrument to removedebris and enhance the smear layer removal (3).
The self-adjusting file (SAF) is a fairly new concept in endodontics. The SAF isa hollow and flexible instrument in the form of a compressible, thin-walled, pointedcylinder composed of 120-mm-thick NiTi lattice. Metzger et al (7) mention thatwhen the file is inserted into the root canal, the instrument adapts 3-dimensionallyto the root canal’s longitudinal and cross-sectional shape. The surface of the latticeis slightly abrasive, and the system removes dentin with a vibrating, back-and-forthgrinding motion. In addition, it has an inherent irrigation system in which the irrigantcirculates through the hollow cylinder, enhancing the flow of irrigant that passesthrough the file. Previous research has shown that the SAF is effective in disinfectingoval-shaped root canals (8) and also in the overall removal of debris and smear
iatric Dentistry, University of Washington School of Dentistry, Seattle, Washington; †Departmentnd ‡Faculty of Dentistry and §Faculty of Engineering, University of San Luis Potos�ı, San Luis Potos�ı,
of Endodontics, University of Washington, Box 357448, Seattle, WA 98195-7448. E-mail address:
JOE — Volume 38, Number 2, February 2012
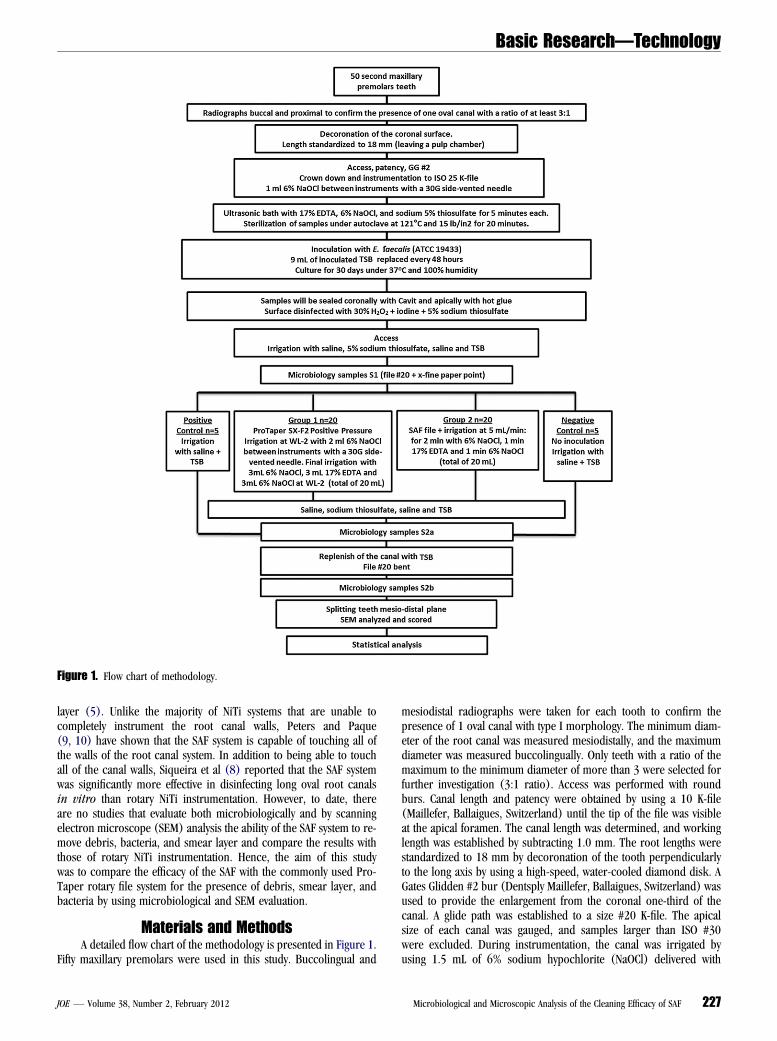
Figure 1. Flow chart of methodology.
Basic Research—Technology
layer (5). Unlike the majority of NiTi systems that are unable tocompletely instrument the root canal walls, Peters and Paque(9, 10) have shown that the SAF system is capable of touching all ofthe walls of the root canal system. In addition to being able to touchall of the canal walls, Siqueira et al (8) reported that the SAF systemwas significantly more effective in disinfecting long oval root canalsin vitro than rotary NiTi instrumentation. However, to date, thereare no studies that evaluate both microbiologically and by scanningelectron microscope (SEM) analysis the ability of the SAF system to re-move debris, bacteria, and smear layer and compare the results withthose of rotary NiTi instrumentation. Hence, the aim of this studywas to compare the efficacy of the SAF with the commonly used Pro-Taper rotary file system for the presence of debris, smear layer, andbacteria by using microbiological and SEM evaluation.
Materials and MethodsA detailed flow chart of the methodology is presented in Figure 1.
Fifty maxillary premolars were used in this study. Buccolingual and
JOE — Volume 38, Number 2, February 2012
mesiodistal radiographs were taken for each tooth to confirm thepresence of 1 oval canal with type I morphology. The minimum diam-eter of the root canal was measured mesiodistally, and the maximumdiameter was measured buccolingually. Only teeth with a ratio of themaximum to the minimum diameter of more than 3 were selected forfurther investigation (3:1 ratio). Access was performed with roundburs. Canal length and patency were obtained by using a 10 K-file(Maillefer, Ballaigues, Switzerland) until the tip of the file was visibleat the apical foramen. The canal length was determined, and workinglength was established by subtracting 1.0 mm. The root lengths werestandardized to 18 mm by decoronation of the tooth perpendicularlyto the long axis by using a high-speed, water-cooled diamond disk. AGates Glidden #2 bur (Dentsply Maillefer, Ballaigues, Switzerland) wasused to provide the enlargement from the coronal one-third of thecanal. A glide path was established to a size #20 K-file. The apicalsize of each canal was gauged, and samples larger than ISO #30were excluded. During instrumentation, the canal was irrigated byusing 1.5 mL of 6% sodium hypochlorite (NaOCl) delivered with
Microbiological and Microscopic Analysis of the Cleaning Efficacy of SAF 227

Basic Research—Technology
a 30-gauge Max-I-Probe side-vented needle (Dentsply/Tulsa Dental,York, PA).All samples were instrumented by using a crown-down technique;the apical third was prepared to ISO #20 K-file by using 1 mL of 6%NaOCl between instruments. All teeth were then placed in an ultrasonicbath of 17% ethylenediaminetetraacetic acid (EDTA), 6% NaOCl, and5% sodium thiosulfate for 5 minutes each to ensure the removal ofdebris and smear layer.
Specimen SterilizationAll samples were kept in sterile saline. Moisture was removed from
the canals with sterile paper points, and the teeth were air dried for8 hours before sterilization. Sterilization was accomplished by usingan autoclave at 121�C and 15 lb/in2 for 20 minutes.
Cultivation of Enterococcus faecalis and SpecimenInoculation
Pure isolated 24-hour colonies of E. faecalis (American TypeCulture Collection 19433) grown on sheep blood agar plates weresuspended in 15 mL trypticase soy broth (TSB) (Becton, Dickinson,Lomas de Chapultepec M�exico, D.F.) for 8 hours. Five drops of thisbacteria culture medium were inoculated in a new 15 mL TSB for 4hours. The bacteria suspensions were adjusted to match the turbidityof 1.5 � 108 colony-forming units (CFUs)/mL (equivalent to 0.5McFarland standard). The glass tubes containing the specimenswere opened, and sterile pipettes were used to add 9 mL of thebacterial inoculums to the vials containing the teeth suspended inthe sterile culture medium.
The tubes were sealed and kept at 37�C for 30 days with 100%humidity. Eighty percent of the broth was replaced with 24 mL of freshsterile culture medium every 2 days to avoid culture medium satura-tion. The turbidity of the culture medium during the incubation indi-cated bacterial growth. The purity of the cultures was confirmed byGram staining after 30 days and later verified in the positive controlsample under SEM. Time of inoculation was set at 30 days to developa mature biofilm because they are more resistant to disinfecting agents(11, 12).
Preparation for Bacterial SamplingAfter 30 days of inoculation with E. faecalis, teeth were taken
out of the culture medium and rinsed with sterile saline. A sterilecotton pellet was placed into the chamber, and the access cavitywas sealed with Cavit (3M ESPE, St Paul, MN) to avoid furthercontamination. To simulate a clinical situation, the apical foraminawere sealed with hot-melt glue (Stanley Hand Tools, Cuajimalpa,Mexico, D.F.). The teeth were placed along the long axis into1-inch segments of surgical tubing (Sullivan-Schein, Melville, NY),and polyvinylsiloxane impression material (3M Health Care, StPaul, MN) was injected into the tubes, leaving the crown of the toothuncovered. A rubber dam was used to isolate the tooth, and thecrown of each tooth was disinfected with 30% hydrogen peroxide(H2O2); all surfaces were then coated with 10% tincture of iodineand allowed to dry. The surface of the tooth was swabbed witha 5% sodium thiosulfate solution to inactivate the iodine tincture.The Cavit and cotton pellet were removed, the chamber was flushedwith 2 mL sterile saline, and the canals were then dried with sterilecotton pellets and paper points. For control purposes, the coronalsurface of the teeth, the rubber dam, and the associated clampswere all swabbed with a sterile cotton pellet and inoculated in bloodagar plates at 37�C for 48 hours.
228 Paranjpe et al.
Initial Sample (S1)By using a sterile tuberculin syringe, 0.5 mL of TSB was inserted
into the canals. To collect dentin shavings, an ISO #20 K-file (Kerr,Romulus, MI) was inserted to working length (WL), rotated clockwiseuntil resistance was met, and then removed from the canal. The file wasremoved, and the fluted part of the file was cut off with a sterile wirecutter and allowed to fall into the opened bottle of TSB. Sterile paperpoints (x-fine) were introduced toWL for 1minute and then transferredto the TSB bottle. All samples were processed immediately.
Teeth were randomly divided into 2 experimental and 2 controlgroups: (1) ProTaper group (20 samples), instrumented to anF3 and irrigated with side-vented needle irrigation; (2) SAF group(20 samples), instrumented with the SAF according the manufacturer’sinstructions; (3) positive control (5 samples), irrigation with sterilesaline; and (4) negative control (5 samples), not inoculated.
All groups were instrumented by the same trained endodontist(A.P.) with no commercial affiliation to any of the systems. The unbiasedoperator (A.P.) was trained by a representative of ReDent on the use ofSAF and was present throughout the experimental phase of the study.This particular approach is critical to avoid variables and biases.
Group 1: ProTaperProTaper NiTi files (Dentsply/Tulsa Dental, Tulsa, OK) were used
to instrument the canals by using a crown-down technique to a size F3 at300 rpm. During instrumentation all samples received 5 mL of 6%NaOCl between each instrument by using a side-vented 30-gaugeMax-I-Probe needle 2 mm short of WL. A total of 20 mL of NaOClwas used during 4 minutes of instrumentation.
Group 2: SAFCleaning and shaping of all samples were carried out by using the
SAF system (ReDent-Nova, Raanana, Israel) following the manufac-turer’s recommendations that were given by the representative fromReDent. A Kavo Gentle power low-speed handpiece (Kaltenbach & VoigtGmbH, Biberach, Germany) was connected to the RDT3 head (ReDent-Nova) at a frequency of 5000 movements per minute and amplitude of0.4 mm. The SAF was inserted into the canals while vibrating and for-warded apically until it reached WL. Duration of instrumentation was4 minutes. Continuous irrigation with 6% NaOCl was carried out byusing an irrigation device (VATEA; ReDent-Nova) set at 5mL/min. A totalof 20 mL of NaOCl was used during the 4 minutes of instrumentation.
Final irrigation was completed in both experimental groups asfollows: 3 mL of 6% NaOCl, followed by 3 mL of 17% EDTA, and finally3 mL of 6% NaOCl at 2 mm short of WL.
Positive ControlTeeth were inoculated with E. faecalis. A microbiological sample
was taken to confirm contamination of the canals. ProTaper NiTi fileswere used to instrument the canals by using a crown-down techniqueto a size F3 at 300 rpm. During instrumentation all samples received5 mL saline between each instrument by using a side-vented 30-gaugeMax-I-Probe needle at 2 mm short of WL. A total volume of 20 mL ofsaline was used during the 4 minutes of instrumentation.
Negative ControlTeeth in this group were not inoculated with bacteria. ProTaper
NiTi files were used to instrument the canals by using a crown-downtechnique to a size F3 at 300 rpm. During instrumentation allsamples received 5 mL of 6% NaOCl between each instrument byusing a side-vented 30-gauge Max-I-Probe needle at 2 mm short
JOE — Volume 38, Number 2, February 2012

TABLE 1. Intergroup Comparison of CFU Counts at S1, S2a, and S2b
Groups
S1 S2a
ReductionS1–S2a (%)
S2b
ReductionS2a–S2b (%)Mean SD
Pvalue Mean SD
Pvalue Mean SD
Pvalue
ProTaper 1.59 � 109 3.95 � 108 >.05 4.42 � 108 4.18 � 108 <.5* 72.15 3.29 � 108 3.53 � 108 <.05* 79.24SAF 1.63 � 109 1.65 � 108 9.98 � 108 5.20 � 108 38.84 1.02 � 109 4.64 � 108 37.15
SD, standard deviation.
*P <.5 was considered statistically significant.
Basic Research—Technology
of WL. A total of 20 mL of NaOCl was used during 4 minutes ofinstrumentation.
Postinstrumentation SamplesAfter treatment protocols were completed, the canals were
sampled again (S2) to evaluate for any decrease in bacterial counts.
Postinstrumentation Samples Taken with Paper Points(S2a). Root canals were flushed with 2 mL 5% sodium thiosulfateto neutralize the NaOCl and then 2 mL sterile saline. Canals were dried,0.5 mL of TSB was inserted into the canals, and then a #25 gutta-perchapoint was introduced to WL by using a pumping motion. Sterile paperpoints (x-fine) were introduced toWL for 1minute and then transferredto the TSB bottle.
Postinstrumentation Dentin Samples (S2b). Root canalswere replenished with TSB, and a #25 gutta-percha point was intro-duced to WL by using a pumping motion. Then a bent #20 K-file wasused with pulling strokes on the buccal and lingual surfaces. Thiswas done to resuspend any bacteria, biofilm remnants, and dentindebris from uninstrumented areas within the canal system. Sampleswere taken by using the same procedure as the S1 sample.
Tubes containing S2a and S2b samples were immediately pro-cessed.
SEM ExaminationTeeth were longitudinally grooved and carefully split. Samples
were rinsed in phosphate-buffered saline, soaked in glutaraldehydefor 1 hour, and fixed with ascending concentrations of ethanol, andthen critical point process was performed. Completely processedsamples weremounted separately on SEM disks, coated with gold/palla-dium, and examined with a scanning electron microscope (Philips XL30, EEUU; FEI Company, Eindhoven, Netherlands) operating at 5 kV.Images were taken at 1 and 3 mm from the apical foramen at magnifi-cation of 200�, 1000�, and 5000�.
SEM images were scored blindly and independently by 3 operatorswho were not involved with the experiment. The scores for debris andsmear layer were recorded according to the Hulsmann scoring criteria(13) at 200� and 1000�, respectively. Scoring for bacteria was per-formed under 5000�magnification according to the following criteria:Score 1, no bacteria on the surface of the root canal; Score 2, isolatedbacteria over the surface with no signs of viability/organization (mitosis,
TABLE 2. Intragroup Comparison of CFU Counts at S1, S2a, and S2b
Samples
ProTaper
Mean SD P valu
S2a 4.42 � 108 4.18 � 108 <.05S2b 3.29 � 108 3.53 � 108
SD, standard deviation.
*P <.5 was considered statistically significant.
JOE — Volume 38, Number 2, February 2012
biofilm matrix); Score 3, agglomeration of bacteria with signs ofviability/organization (mitosis, biofilm matrix); Score 4, more than50% of the root canal walls was covered with viable bacteria; Score5, complete or nearly complete root canal wall coverage with viablebacteria.
Statistical AnalysisThe Mann-Whitney test was used for intragroup analysis that
compared the reduction in the number of CFU counts from S1 to S2aand S2b. The incidence of positive cultures within each group wasanalyzed by using the 2-tailed Fisher exact test and difference betweenthe groups by using the c2 test. Difference between SEM scores wasanalyzed by using the Student t test. Significance level for all analyseswas set at P <.05.
ResultsAll samples taken from the operatory field (coronal structure,
rubber dam, and clamp) were negative for bacterial culture, demon-strating proper disinfection of the field and ruling out possible cross-contamination of the experimental samples. Samples taken on accessand before instrumentation (S1) were all positive for bacteria, exceptfor the samples from the negative control, which remained negativeat S2a and S2b. Samples from the positive control group tested positivefor bacteria at S2a and S2b.
In group 1 (ProTaper), 8 of 20 samples (40%) cultured negativeat S2a and 9 of 20 (45%) at S2b. In group 2 (SAF), 4 of 20 (20%)samples cultured negative at S2a and 3 of 20 (15%) at S2b. A statisticalreduction (P< .01) of bacteria from S1 to S2a and S2b was observed inboth experimental groups. The mean and standard deviation of CFUsobserved for the ProTaper and SAF groups are presented in Table 1.Intergroup analysis demonstrated no statistical difference at S1 (samebacteria load). At S2a and S2b, a statistical significant difference wasobserved between the experimental groups (P < .05) (Table 1). Intra-group analyses evaluating the reduction in the number of CFUs from S1to S2a and S2b demonstrated that both preparation techniques werehighly effective (P < .01). Further reduction of CFUs was observedwhen comparing S2a and S2b in group 1 (P < .05), whereas no statis-tical difference in reduction was observed in group 2 (Table 2).
A representative sample for each experimental group at 1 and3 mm under the SEM is illustrated in Figure 2. For smear layer andbacteria, the SAF group scored statistically higher compared with the
SAF
e Mean SD P value
* 9.98 � 108 5.20 � 108 >.05*1.02 � 109 4.64 � 108
Microbiological and Microscopic Analysis of the Cleaning Efficacy of SAF 229

Figure 2. Representative samples of each experimental group. Debris, original magnification 200�: (A) SAF at 1 mm, (B) SAF at 3 mm, (C) ProTaper at 1 mm,and (D) ProTaper at 3 mm. Smear layer, original magnification 1000�: (E) SAF at 1 mm, (F) SAF at 3 mm, (G) ProTaper at 1 mm, and (H) ProTaper at 3 mm.Bacteria, original magnification 5000�: (I) SAF at 1 mm, (J) SAF at 3 mm, (K) ProTaper at 1 mm, and (L) ProTaper at 3 mm.
Basic Research—Technology
230 Paranjpe et al. JOE — Volume 38, Number 2, February 2012

Figure 3. SEM scores for (A) debris, (B) smear layer, and (C) bacteria.
Basic Research—Technology
ProTaper group at both 1 and 3 mm (Fig. 2). For debris, a statisticaldifference was only found at the 3-mm level (Fig. 3).
DiscussionMany studies have demonstrated the limitations and challenges
related to rotary systems with regard to cleaning the canal complexitiessuch as fins and isthmuses (14). Recent studies have shown that theSAF system is able to touch all the canal walls evenly (9, 10). De-Deuset al (15) histologically compared the debridement efficacy of the SAFsystem with the ProTaper system and demonstrated that the SAF systemwas more efficient in pulpal debridement. However, to date, there havebeen no studies comparing the efficacy of these 2 systems by usinga combined microbiological and microscopic analysis. For this purpose,our research group decided to first evaluate the fluid dynamics for bothsystems and correlate the results to the microbiology and SEM results.
Previous studies have demonstrated that root canal debridement isimproved with progressively larger instrumentation (16) by removingmore contaminated dentin and providing better access for efficient irri-gation and disinfection of the canal system (3). These findings providea logical explanation to the results obtained in the present study fromboth a microbiological and microscopic standpoint. However, theyare not in accordance with the results obtained by Metzger et al (5)and Siqueira et al (8) by using the SAF system.
Our initial study included a total of 120 teeth from which 90 wereinstrumented with the SAF system for 5 minutes. The results revealed aninsufficient apical preparation and inadequate apical irrigation. It isimportant to mention that the preparation of the samples, the cleaninganalysis, tallying the number of bacterial colonies, and the evaluation ofirrigant penetration in cleared teeth took place in 3 independent labo-ratories from 3 universities located in different countries.
The concept of a 3-dimensional file that adapts to the canalmorphology is encouraging. However, there is no system in whichone size fits all. Root canal anatomy is complex, and variations arethe rule rather than the exception. Apical instrumentation should bedictated and strategically planned on the basis of the anatomy and themicrobiological status of the root canal. Therefore, the type and sizeof instruments should be selected by the clinician on the basis of thetherapeutic goal of the treatment. As demonstrated by the results ofthe present study, the SAF system does not allow control of the apical
JOE — Volume 38, Number 2, February 2012
instrumentation, thus limiting the ability of the irrigants to achieve aneffective and predictable disinfection.
AcknowledgmentsThe authors deny any conflicts of interest related to this study.
References1. Eriksen HM, Kirkevang LL, Petersson K. Endodontic epidemiology and treatment
outcome: general considerations. Endod Topics 2002;1:1–9.2. Friedman S. Considerations and concepts of case selection in the management of
post-treatment endodontic disease. Endod Topics 2002;1:54–78.3. H€ulsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals:
shaping goals, techniques and means. Endod Topics 2005;10:30–76.4. Elmsallati EA, Wadachi R, Ebrahim AK, Suda H. Debris retention and wear in three
different nickel-titanium rotary instruments. Aust Endod J 2006;32:107–11.5. Metzger Z, Teperovich E, Cohen R, Zary R, Paque F, Hulsmann M. The self-adjusting
file (SAF): part 3—removal of debris and smear layer: a scanning electron micro-scope study. J Endod 2010;36:697–702.
6. Taylor JK, Jeansonne BG, Lemon RR. Coronal leakage: effects of smear layer,obturation technique, and sealer. J Endod 1997;23:508–12.
7. Metzger Z, Teperovich E, Zary R, Cohen R, Hof R. The self-adjusting file (SAF):part 1—respecting the root canal anatomy: a new concept of endodontic filesand its implementation. J Endod 2010;36:679–90.
8. Siqueira JF Jr, Alves FR, Almeida BM, de Oliveira JC, Rocas IN. Ability of chemome-chanical preparation with either rotary instruments or self-adjusting file to disinfectoval-shaped root canals. J Endod 2010;36:1860–5.
9. Paque F, Peters OA. Micro-computed tomography evaluation of the preparation oflong oval root canals in mandibular molars with the self-adjusting file. J Endod2011;37:517–21.
10. Peters OA, Paque F. Root canal preparation of maxillary molars with the self-adjusting file: a micro-computed tomography study. J Endod 2011;37:53–7.
11. Hockett JL, Dommisch JK, Johnson JD, Cohenca N. Antimicrobial efficacy of two irri-gation techniques in tapered and nontapered canal preparations: an in vitro study.J Endod 2008;34:1374–7.
12. Shen Y, Stojicic S, Haapasalo M. Antimicrobial efficacy of chlorhexidine againstbacteria in biofilms at different stages of development. J Endod 2011;37:657–61.
13. Hulsmann M, Rummelin C, Schafers F. Root canal cleanliness after preparation withdifferent endodontic handpieces and hand instruments: a comparative SEM investi-gation. J Endod 1997;23:301–6.
14. Peters OA. Current challenges and concepts in the preparation of root canal systems:a review. J Endod 2004;30:559–67.
15. De-Deus G, Souza EM, Barino B, et al. The self-adjusting file optimizes debridementquality in oval-shaped root canals. J Endod 2011;37:701–5.
16. Usman N, Baumgartner JC, Marshall JG. Influence of instrument size on root canaldebridement. J Endod 2004;30:110–2.
Microbiological and Microscopic Analysis of the Cleaning Efficacy of SAF 231