efficacy of black cohosh-containing preparations on
TRANSCRIPT

ORIGINAL KESEARCH
EFFICACY OF BLACK COHOSH-CONTAININGPREPARATIONS ON MENOPAUSAL SYMPTOMS
A META-ANALYSISTaghreed Shams, MD, FRCSC; Maninder Singh Setia. M[). MPH; Robert Hemmings, MD, FRCSC; Jane McCusker, MD, DrPH;
Maida Sewitch, PhD; Antonio Ciampi. PhD
This study aimed to review the evidence on the efficacy of herbalpreparations containing black cohosh for the treatment of meno-paiisal symptoms. A systematic search of three databases(PuhMed. Embase, and Cochrane library) was conducted toidentify relevant literature. Two reviewers independentlyabstracted the data from the eligible studies. Of the 288 Englishlanguage citations screened, nine randomized placebo-ton trolledtrials were included. Among these trials, six demonstrated a sig-nificant improvement in the black cohosh group compared with
the placebo group. Using data from seven trials, we calculated acombined estimate tor the change in menopausal vasomotorsymptoms. Preparations containing black cohosh improvedthese symptoms overall by 26% (95% confidence intervalll%-40%); there was, however, significant heterogeneity betweenthese trials. Given that black cohosh is one of the most frequentlyused herbal medications tor menopausal vasomotor symptomsin North America, more data are warranted on its effectivenessand safety. {Altem Tlwr Health Med. 2010:]6(l):36-44.)
Taghreed Shams, MD, FRCSC, at the time of the study was a fellowin the Departments of Obstetrics and GjTiecology, St Mary'sHospital and McGill University, Montreal, Canada. ManinderSingh Setia. Ml), MPH, is a doctoral candidate in the DepartmentofClinical Bpidemiolog}' and Community Studies, St Mar>'sHospital, and the Department of Epidemiology, Biostatistics andOcajpational Health, McGill University. Robert Ilemmings, MD,FRCSC, is head of the Departments of Obstetrics and Gynecology,St Mary's Hospital. Jane McCusker, MD. DrPH, is head of theDepartment ofClinical Epidemiology and Community Studies,St Mary's Hospital, and professor in the Department ofEpidemiology, Biostatistics and Occupational Health, McGillUniversity. Maida Sewitch, PhD, is an associate member of theDepartment ofClinical Epidemiolog)' and Community Studies.St Mary's Hospital, and assistant professor in the Department ofMedicine, McGill University. Antonio Ciampi, PhD, is an associ-ate memlwr of the Department of Clhiical Epidemiology andCommunity Studies, St Mary's Hospital, and associate professorin the Department of Epidemiology, Biostatistics andOccupational Health, McGill University.
Corresponding author: Jane McCuskerE-mail: [email protected]
M enopause is defined as loss of ovarian follicularactivity associated with 12 consecutive monthsof anienorrhea not explained by other obviouspathological or physiological causes. The mostcommon symptoms are vasomotor.' Fort}' per-
cent of perimenopausal women and up to 80% of postmen opa usaiwomen complain of moderate to severe vasomotor symptomsthat affect their quality of life to varying degrees.- These symp-toms may lead to insomnia and irritability and can persist inmore than 40% of women 2 years after cessation of menses.'
Multiple treatment modalities have been used to relieve thesymptoms of menopause, including hormonal treatments (eg,estrogens, progesterone, or a combination of both); antidepres-sants (eg. serotonin reuptake inhibitors): complementary andalternative medicine (CAM); and lifestyle modifications."" Arecent survey showed that more than 50% of menopausal womenused a CAM product during the previous year to alleviate meno-pausal symptoms": black cohosh {Actea racemosa or Gmifuga rac-emos(i) is one of the most widely used,' In 2000, black cohosh wasapproved in Ciennany as a nonprescription drug for the treat-ment of hot flashes." Two previous literature reviews on the treat-ment of vasomotor symptoms with CAM have included blackcohosh studies'""; however, these reviews included short durationstudies, a maximum of four randomized controlled trials (RCTs),and neither performed a quantitative synthesis.
Because several additional RCTs have since been pub-lished, we undertook a systematic review and meta-analysis ofthe published literature of the efficacy of preparations contain-ing black cohosh on reduction of vasomotor symptoms associ-ated with menopause.
MATERIALS AND METHODSThis study was exempt from Institutional Review Board
review as there were no human participants involved.
36 ALTERNATIVE THERAPIES, lAN/FEB 2010, VOL 16, NO, 1 Black Cohosh for Menopausal Symptoms

•>« n « .
Data SourcesWe performed a comprehensive literature search of PubMed
(1950 to January 2008), Embase (1980 to January 2008), and theCochrane Library (1950 to January 2008) to identify all the stud-ies on black cohosh and menopause, We used the phrases "blackcohosh and menopause," "Cimicipga riwemosa and menopause,"and "Actaea racemosa and menopause" to identify the studies. Inaddition, we scanned the reference lists of all the identified stud-ies and reviews for any otiier studies not identified by the elec-tronic search. We included only English language studies for thepresent review.
Study FJigibilityThe inclusion and exclusion criteria were established in
advance to minimize the bias in selection of the studies for review.Studies that met the following criteria were included: the studydesign was an RCT, the population comprised perimeniipausal/postmenopausal women, the ititervention was a preparation con-taining black cohosh, at least one of the control groups was placebo,and at least one of the outcomes was the frequency of vasomotorsymptoms. Studies that were conducted exclusively in women witha history of breast cancer were excluded. If a study had more thanone published report, we included the latest published report withthe maximum number of patients, although we reviewed the priorones for study design and patient selection criteria.
Data AbstractionTwo authors (TS and MSS) independently reviewed the
studies to assess inclusion criteria and abstracted data using astandardized data abstraction sheet. Abstracted data includedthe names of authors; the place and time of publication; theinclusion and exclusion criteria; the number of patients random-ized in the intervention and the control group(s); the type anddose of black cohosh used; the type of control; the method ofrandomization; patient characteristics at baseline (age, bodymass index, time since menopause, and smoking status); themethods of sample size calculation; statistical analyses (includ-ing handling of missing data); the measurement of the primaryand secondary outcomes in the intervention and the controlgroup(s); and the change in outcomes at follow-up. For addition-al information, we contacted the authors and did hear back fromone of the article's corresponding authors."
We assessed the quality of the studies based on the follow-ing criteria as proposed by Jadad: method of randomization,blinding procedure, and description of the withdrawals." Eachstudy received a score of 1 for discussion of each of these criteriaand an additional point if randomization and blinding proce-dures were appropriate. Good quality was defined as a score ofmore than 3 out of 5. Both reviewers (TS and MSS) comparedtheir results, and discrepancies were resolved by discussion witha third author (JM).
Data AnalysisThe numbers of participants in the black cohosh arm (N , )
and the placebo arm (N ) were abstracted. For each study, wecalculated the change in the proportion of subjects with symp-toms from baseline (d^) to 12 weeks {á^^ in the black cohosh(Dj P and placebo (D ) groups. (For one study, we had informa-tion for only 16 weeks, and we included that in the analysis.) Ifthese data were not reported in a study, they were calculated as((d,^ - a^/áQ • 100. The rate difference (D.) was then calculatedas the difference between the proportions between black cohoshand the placebo groups (D, ^ - D ). Additionally, we calculatedthe standard error (SE) of the rate difference by the followingmethod; square root {[D,, (1 - D|^p/N,,J -h [D ^ (1 - D|,)/N 11.
The rate differences were combined using the general prin-ciples of fixed effects model,'' The weight (Wp for each study wascalculated as (1/SE'')." The summary measure was calculated bymultiplying the weight with the rate difference (W. • D¡). Thepooled summary was calculated by dividing the sum of summarymeasures by the sum of weights (2 Wj - 0 ^ / 2 W¡)."Homogeneity between studies was assessed by using a chi-squarestatistic with a degree of freedom equal to the number of studiesminus 1.'' If the studies were not found to be statistically homo-geneous, then an extravariation parameter (between-studies vari-ance) was incorporated into the analysis by using a randomeffects model." The fixed effects model takes Into account thewithin-study variance and hence weighs the study according tothe study size and precision. The random effects model, however.additionally accounts for the interstudy variation, the underlyingassumption being that the studies are a random sample from ahypothetical population and that the Interstudy variance can berepresented by a single estimate."
We performed a sensitivity analysis by separating the RCTsinto two groups: those that used black cohosh in conjunctionwith other products and those that had used black cohosh alonein the intervention group.
RESULTSDetails of the literature search are shown in Figure 1. We
scanned 223 abstracts initially and identified 31 potential studiesfor review, of which nine were not RCTs (three studies discussedthe adverse effects of black cohosh,''''' one was a nonrandomizedstudy,''' one an observational study,'" one a pilot study,'"and tbreewere reviews^ "'^')- Of the remaining 22 RCTs. 13 did not meet ourinclusion criteria (three included subjects with a history of breastcancer,"-^ one evaluated the effect of black cohosh on menstrualmigraine only,-' two assessed the role of black cohosh on changesin cardiovascular disease markers, '' '' four lacked a placebo con-trol group,'-''" and three were additional reports of studies alreadyincluded in the current review' "). We scanned the reference listsof these articles for any RCTs not identified by the electronicsearch but did not identify any new studies. Thus, nine RCTs wereretained for the present review and meta-analysis.
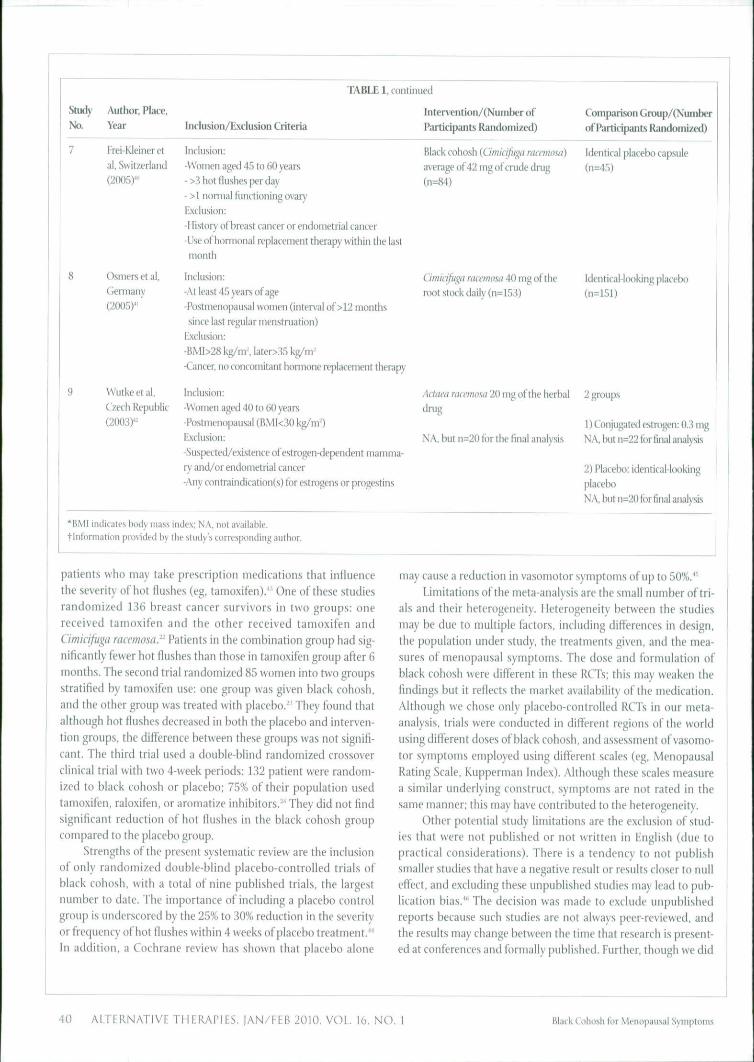
The characteristics of the sample, inclusion, and exclusioncriteria of these RCTs are presented in Table 1, ordered by publi-cation date, starting with the most recent. Of the nine RCTs, sixwere conducted in Europe, one in the United States, one in Israel,
Black Cohosh for Meiiopausal Symptoms ALTERNATIVE THERAFIES, lAN/FEB 2010. VOL. 16. NO.

288 citations identified for screening• 114 froiTi Medline• 159 from Embase
• 15 from Cochrane Library
65 duplicate, abstracts excluded
223 abstracts retrieved
31 potential studies retrieved
192 abstracts
not relevant
22 randomized trials retrieved
9 studies werenot randomizedcontrolled trials
Did not meet inclusion criteria (13)3 history ot breast cancer3 witbout outcome ot interest3 additional reports of included studies4 without a placebo arm
9 randomized controlled trials
included in the iiieta-analysis
FIGURE 1 Details of Literalure Review and Study Identification fur
the Systematic Review
and one in Korfy. The mean age of women ranged between 50.5and 59 years. All of the RCTs excluded subjects with a history ofhormone-dependent cancer and/or previous use of hormonesunless followed by a washout period.
The outcomes, measures, results, quality scores, and fundingsotirces for the trials are presented in Table 2. Tivo trials'' did notdemonstrate a significant improvement in the intensity of vasomo-tor symptoms in the black cohosh group when compared with tbeplacebo group. Of these, the study by Newton et al had multiplecomparison groups (multibotanical products, multibotanical withsoy. conjugated equine estrogen, and placebo) and the longest fol-low-up period (12 months). In this trial, only the group treatedwith estrogens had a significant change in the frequency of vaso-motor symptoms. Of the other seven trials demonstrating a signifi-cant improvement, one used a combination of black cohosh,ligans, and isoflavones''; one used black cohosh in combinationwith dong quai, milk thistle, red clover, American ginseng, andchastetree berry"; two used a combination of black cohosh and StJohn's wort'" ''; and the others used black cohosh alone.'"'-
Some of the commonly reported side effects in the blackcohosh group were gastrointestinal symptoms (0.7%-15%), mus-
culoskeletal atid connective tissue conditions (4%-9.8%). andinfections and infestations (8..S%-ll.it"i,). Breast discomfort wasnot seen in the intervention group in tivo trials,''-'" and in anoth-er study, the intervention and control groups reported similarproportions of breast complaints.'^ None of the RCTs reportedincreased occurrence of side effects in the intervention groupcompared with the placebo group.
Oí the nine RCTs, six received a quality score of more than3 and were, therefore, considered good quality.'""'*""" Two ofthese trials' ' •" did not demonstrate a significan! improvement invasomotor symptoms. Three RCTs received scores of 3 becauseappropriateness of randomization and blinding could not bedetermined.'"*^-' The trials were financed by the privateflinders *' '"'' and government research organizations.''- Onestudy just mentioned that the intervention tablets were fundedby a private funden'' Three of the RCTs did not report the sourceof funding.''^"^'
The results of seven RCTs" '''" were used to calculate I he com-bined estimate of the rate difference; data tor calculation of the effectsize for the other two RCTs could not be obtained." '- The combinedestimate of the rate différence for improvement of vasomotor svinp-toms in the black cohosh group compared with placebo using thefixed eifects model was 24% (95% CI: 18V29%). The hypothesis ofhomogeneit)' bet veen the studies was rejected (7'<.005). The com-bined estimate of the rate difference calculated with the randomeffects model was 26% (95% CI: 11%-4Û%; Figure 2).
Five trials'' '"'''' had used black cohosh in combination withother products; the combined estimate of these trials using therandom effects model was 41% (95%CI: 20%-62%). The combinedestimate of the two RCTs"" that used a combination of blackcohosh and St John's wort in the intervention group was 33%(95% CI: 24%-42%); the results of these two studies were homoge-nous and the fixed effects model was used. Two RCTs~"' " had usedonly black cohosh in the inter\'t'ntion group; the combined esti-mate using a fixed effects model was 11% (95% CI: l%-20%). asthese RCTs were homogeneous.
COMMENT
We report a systematic review of nine placebo-controlledRCTs of preparations containing black cohosh in healthy peri-menopausal women between the ages of 40 and 60 years. Wewere able to perform a meta-analysis with data from seven ofthese trials. Overall, black cohosh-containing preparations werefound to be efficacious in reducing the symptoms of menopausein comparison to placebo, although the trials were significantlyheterogeneous. Notably, the trial with the longest follow-up (12months) and the highest dose of black cohosh (ltiO mg) did notdemonstrate significant improvement in the black cohosh groupcompared with the placebo group. " Black cohosh in combinationwith other muitibotanicals and St John's wort appeared to bemore efficacious in treating menopausal symptoms comparedwith black cohosh alone. Side etiects in the black cohosh groupwere similar to those in the placebo group.
We excluded three RCTs conducted on breast cancer
38 ALTERNATIVE THERAPIES, |AN/FEB 2010, VOL. 16, NO. 1 Black Coinisli lor XU'inijmusal S\rii|iU)iiis

TABLE 1 Description of the Studies. Inclusion and Exclusion Criteria. Inten'ention and Control Groups, and Outcome for Studies Included in the Review*
Stijd\' Author. Place, lntervention/(NunilHT of Comparison Group/(Number
Na Year
1 Chung et al,Korea, (2007)^
Rotem et a!,
Israel, (2007)'
Sammartino et
al. Italy (2006r
Uebelhack etal. Germany
(2006)'
Newton et al.
United States
(2006)'-
Inclusion/Exclusion Criteria Participants Randuini/ed)
Verhoeven et
al. Netheriands(2005)"
Inclusion:-Perimenopausal women (specific agt not disiiissed)-Women with typical climacteric s)Tnptoms
Exclusion;-Patients w ith history of breast cancer
Inclusion:-Pre- and pitstmenopausal women aged A^-6S years
-Amenorrhea for at least 6 months-Elevated follicle-stiiTiulating hormone le -fl {>^0 pg/rnl.)
-Hot flushes and/(ir night sweats at least 3x/iiExclusion:
-Women with a history of any cancer »ere excludedfrom the study!
Inclusion:- I^ t menses at least 6 months before inclusion and no
more than 24 months
-Minimum number of 7 moderate-to-severe hot flush-
es (including night sweats) per 24-hour period
Exclusion:
-Neoplastic, metabolic, and infectious diseases
-Past or otncomitant use of estrogeri/progesterone
replacement therap)' or other drugs used to treat cli-macteric s)Tnptoms
Inclusion:
-Women aged 45 to 60 years
-Menopausal Rating Scale of 0.4 or more in at least
3 items
Exclusion:-Did not specifically mention exclusion of breast
cancer cases
Inclusion:
-Women aged 45 to 55 years
-Two or more vasomotor symptoms per day
Exclusion:-History of breast cancer-Contrai ndifation(s) to homnone therapy
Inclusion:-Women aged 45 to 65 years
-Amenorrhoeic for at least 6 monthsExclusion:-History of hormone-dependent cancer
-Women on honiione therapy required a washoutperiod of at least 6 months
Black cohosh and Si John's wort(264 mg tablet, 0.0:tB4 mi. ofextract from Cîmicifùga mcemosa)
(n=47)
Black cohosh (Gtmqfuga racanosa)
100 mg, dong tjuiil rixjt extract 75mg, milk thistle herb extract 75 mg,red clover flov\'er extract ÍÍO mg,
American ginseng 59 nig, chaste-tree berrv fruit extract SO nig {n=19)
Cimicifiiga mcemosa {50 mg) withisoflavones and lignans
Black cohosh and Si lolm's wort(22.5-41.2ii mg of rootstiKk of
black cohosh)(n=]51)
Black cohosh 160 mg daily
(n=80)
100 mg of black COIKISII extract(Additionally: 125 mg soy extract.
1500 mgprimro.se oil. 1.25 figvitamin D. 200 nig calcium, and
10IU\itaminE)(n=60)
of Participants Randomized)
Placebo preparation (n=42)
Placebo capsules outwardly
idenrical to the study prepara-
tion (n=16)
Calcium supplements (n=40)
Placebo preparation (n=150)
4 groups:
1) Muitibotanical groups:black cohosh, alfalfa, boron,chaste tree, doiig qiiaj. falseuniconi. licorice, oats, ¡xime-granat*', Siberian ginseng:(n=76)
2) Muitibotanical ;iiid soycounselling (M-79)
3) 0,625 mg oí conjugatedequine estrogen tor w omenwith uterus and 2.5 mg otmedroxj-progesteronc acetate4)Placeix>(ii=84)
Placebiï preparation (2fK)(Jmgoli\'eoil)(n=(>4)
Black Cohosh for Meiiopausal Symptoms ALTERNATIVE THERAPIES, IAN/FEIÍ 2010, VOL. lo, NO.
StiK ' Author. Place,
Nd Year
7 Frei-Kleiner etal, Switzerland
(2(K)5)*'
8 Osmers et al,
Ciermany(2005) '
9 Wutkeetal,
Czech Republic
(2003) -
TABLE 1, continued
inclusion/Exclusion Criteria
Inclusion:
-Women aged 45 to 60 years- >3 hot flushes per day
- >1 normal functioning ovaryExclusion:
-History of breast cancer or endometrial cancer-Use of hormonal replacement therapy within the lastmonth
Inclusion:
-At least 45 years of age
-Postmenopausal women (interval of >12 monthssince last regular menstruation)
Exclusion:
-BMI>28 kg/ni% Iater>35 kg/m'-Cancer, no concomitant hormone replacement therapy
Inclusion:
-Women aged 40 to 60 years
-Postmenopausal (BMI<30 kg/nr)Exclusion:
-Suspected/existence of estrogen-dependent mainnia-ry and/or endometrial cancer
-Any contraindication(s) for estrogens or progestins
•BMI indicates body mass index; NA. not available.tInformation provided by the study's corresponding author.
lntervention/(Number ofParticipants Randomized)
Black cohosh {Cimicifuga mcenumi)
average of 42 mg of crude drug(n=84)
Cimicifuga racemosa 40 mg of theroot stock daily (n=153)
Actaea racemasa 20 mg of the herbal
drug
N A, but n=20 for the final analysis
Comparison Group/(Nuniberof Participants Randomized)
Identical placebo capsule
(n=45)
IdenticaHooking placebo(n=151)
2 groups
1) Conjugated estrogen: 0.3 mg
NA, but n=22 for final analysis
2) Placebo: identical-lookingplacebo
NA, but n=2() for final analysis
patients who may take prescription medications that influencethe severity of hot flushes (eg, tamoxifen).'()ne of these studiesrandomized 136 breast cancer survivors in two groups: onereceived tamoxifen and the other received tamoxifen atuiCimkijuga mcemosar Patients in the combination group had sig-nificantly fewer hot flushes than those in tamoxifen group after 6months. The second trial randomized 85 women into two groupsstratified by tamoxifen use: one group was given black cohosh,and the other group was treated with placebo.^' They found thatalthough hot flushes decreased in both the placebo and interven-tion groups, the difference between these groups was not signifi-cant. The third trial used a double-blind randomized crossoverclinical trial with two 4-week periods: 132 patient were random-ized to black cohosh or placebo; 75% of their population usedtamoxifen. raloxifen, or aromatize inhibitors.-^ They did not findsignificant reduction of hot Hushes in the black cohosh groupcompared to the placebo group.
Strengths of the present systematic review are the inclusionof only randomized double-blind placebo-controlled trials ofblack cohosh, with a tolal of nine published trials, the largestnumber to date. The importance of including a placebo controlgroup is underscored by the 25% to 30% reduction in the severityor frequency of hot flushes within 4 weeks of placebo treatment."In addition, a Cochrane review has shown that placebo alone
may cause a reduction in vasomotor symptoms of up to 50%.*''Limitations of the meta-analysis are the small number of tri-
als and their heterogeneity. Heterogeneity between the studiesmay be due to multiple factors, including differences in design,the population under study, the treatments given, and the mea-sures of menopausal symptoms. The dose and formulation ofblack cohosh were different in these RCTs; this may weaken thefindings but it reflects the market availability of the medication.Although we chose only placebo-controlled RCTs in our meta-analysis, trials were conducted in different regions of the worldusing different doses of black cohosh, and assessment of vasomo-tor symptoms employed using different scales (eg, MenopausalRating Scale, Kupperman Index). Although these scales tiieasurea similar underlying construct, symptoms are not rated in thesame manner; this may have contributed lo the heterogeneity.
Other potential study limitations are the exclusioti of stud-ies that were not published or not written in English (due topractical considerations). There is a tendency to not publishsmaller studies that have a negative result or results closer to nulleffect, and excluding these unpublished studies may lead to pub-lication bias.'" The decision was made to exclude unpublishedreports because such studies are not always peer-reviewed, andthe results may change between the time that research is present-ed at conferences and formally published. Further, though we did
40 ALTERNATIVE THERAPIES. |AN/FEB 2010, VOL. 16, NO. Bîai'k Coliosli for Mcnopausal Symptoms

Study
No.
1'»
2"
3"
4»
Principal
Outcome
Kupperman
Index
Number of hot
flushes
Kupperman
Index
Menopausal
Rating Scale
Mean change
in intensity' of
vasomotorsymptoms
TABLE 2 Outcome, Quality Score, and Funding Sources for Studies included in the Review
Measurement of the Outcome
Intervention group:Baseline: 2(i.46±10.64
4weeks:12.46±6.9612weeks:6.37±4.16
Change: 20.09±4.16
Control group:Baseline: 2538±10.16
4 weeks: 19.63111.0912 weeks: ]7,14±11,61
Change: 8.24±7,57
Intervention group:Baseline: 5.57+2.57 (mean number of hot flushes)4 weeks: 43±3 {percentage change from baseline)
12 weeks: 73±5 (percentage change frotii baseline)
Control group:Baseline: 5.06±2.98 (mean number of hot flushes)
4 weeks: 18±4 (percentage change from baseline)
12 weeks: 38±5 (percentage change from baseline)
Intervention group:
Baseline: 30 (24 to 36)
12 weeks: 8 (6 to 10)
Control group:Baseline: 31 (26 to 36)
12 weeks: 26 (23 to 29)
Intei-vention group (change from baseline):
8weeks:-O.16±().i:i16 weeks:-0.23±0,13
Control group (change from baseline):
8weeks:-0.10±0.13
16 weeks:-0.09±0.12
Black coliosli vs placebo
3 months:-0.96 (-2.03toO.U)
6 months:-0.48 (4.63 to 0.66)12 months: -0.80 (-1.30 to 0.93)All:-0.54 (-1,47 to 0.38)MBA vs placebo3montbs:0.41 (-0.67 to 1.50)
6 months: 0.80 (-0,36 to 1,96)12 months: 0.09 (-1.03 to 1.20)All: 0,43 (-0.50 to 1.37)
MBAS vs placebo3 months:-0.53 (-1.60 to 0.54)6montbs:0.32 (-0.83 lo 1.47)
12 months: 0.49 (-0.62 to 1.60)
All: 0.09 (-0.83 to 1.02)CEE vs placebo3 months:-4.55 (-6.51 to-2.59)
6 months:-3.86 (-5.73 to-2,00)12 months:-.176 (-5.76 to-1,76)All:-4.06 (-5,93 to-2.19)
Significance
.002t
<.ooit<.ooit
,026t
<,05t
<,ooit<.ooit
Quality Score
3
3
5
4
5
Funding Source
Private funding
The intervention capsules
were donated by a private
company
Not mentioned
Private frinding
Government funding
Black Cohosh for Menopausal Symptoms ALTERNATIVE THERAPIES, ¡AN/FEB 2010, VOL 16, NO, 41

Study Principal
No. Outcome
6^ Modified
KuppemianIndex Scale,changeât 12
weeks com-
pared withbaseline
7" Hot flashes.
weekly weight-ed scores.
Kupperman
Index
8*' Meiiopausa!
Rating Score 1
(MRS)
9« Vaüdated
MenstrualRating Score
(MRS)
TABLE 2
Measurement of the Outcome
Intervention group:
Baseline; 28.1±5,73 weeks; 23.8±6.9
12 weeks; 20.7±8.9Percentage change from baseline
-26 (-33 to -18)Controls:
Baseline: 27.9±5.8
3 weeks: 22.5±8.2
12 weeb: 20.6±8.8Percentage change from baseline
-26 (-35 to -18)
Intervention group:
12 weeks37% reduction in hot flashes
26% reduction in Kuppennan Index
Controls:
12 weeks
30% reduction in hot flashes
17% reduction in Kupperman Index
, continued
Significance Quality Score Funding Source
4 Private fiinding
904.,OOf
4 Not mentioned
Beta coefficient of the regression model (Including 5 Not mentionedinteraction terms, medically relevant model)12 weeks
Treatment: -0,0788 (-0.12 to -0.0374)
MRS at baseline: -0.301 (-0,395 to -0.207)
Durationf treatment:
.00387 (.000801 to .000694)
(Data extracted from graphs)Intervention group:
12 weeks
Change from baseline:
-1.8 (-1.7 to-2.0)
Controls;
12 weeks
Change from baseline for CE:-1.78 (-1.7 to-1.9)
Change in baseline for placebo group:-1.5 (-1.35 to-1.6)
<.001§
<.001§
.002§
3 Government funding
.0506t
.0513t
*MBA indicates multibotanical groups; MBAS, muitihoianical groups with soy and counselling; CEE, conjugated equine estrogen; CE. conjugated estrogen.fP value is the comparison between intervention and control group,tp\'alue for chiinEe,§P value for coefficient.
scan the references of the reviewed studies, we may have missedother articles not captured by these three databases. It also hasbeen shown that fewer CAM trials with positive outcomes arepublished in high-impact mainstream medical journals,^' andmedical journals in the United States are less likely to report pos-itive outcomes of CAM trials than are European journals.*"' This,potentially, may have resulted in some publication bias in ourmeta-analysis.
Overall, our results are consistent with those of previousreviews that suggested a benefit of black cohosh in reducing thefrequency of vasomotor symptoms.""*" The present studyadvances the literature on the efficacy of black cohosh in reduc-ing the vasomotor symptoms in menopause because we haveincluded more RCTs and performed a quantitative nieta-analysisof these trials.
Additionally, our finding that St John's wort, an herbal
42 ALTERNATIVE THERATIES, |AN/FEL^ 2010. VOL. 16, NO, I Black Cohosh for Menopausal Symptoms

i r II'
1 -
-30 -20 -10 20 30
Rate Difference
40 50 60 70 80
FIGURE 2 Forest Plot of the Seven Randomized Trials Included in the Meta-analysis*
Shown are the point estimates with confidence limits of each trial and the random eifects combined estimate with confidence limits. The size of each box repre-sents the weight of the study in the random effects model. The rate difference is defined as the difference between the change in proportion of the menopausalsymptoms between 12 weeks and baseline in the black cohosh and placebo groups.•Study 1, Chung el al (2007)"; 2, Rotem et al (2007)": 3, Sammartino et al (2006)''; 4, üebelhack et al (2006)'•; 5, Newton et al (2006)''; 6, Verhoeven et al (2005)": 7,Frei-Kleiner et al (aoos)."'
antidepressant, in combination with black cohosh may increasethe efficacy of black cohosh lias not been reported in previoussystematic reviews. This finding should be interpreted cautious-ly, however, as it was based on only two RCTs. A recent Cochranereview concluded that St John's wort is superior to placebo forthe treatment of major depression and has similar effectivenessto standard antidepressants but with fewer side effects. " Furtherclinical controlled trials to assess the role of St John's wort andblack cohosh vs each herbal medication alone may also be war-ranted to tease apart the independent contribution of each tothe reduction of vasomotor symptoms.
Although an essay discussing the effectiveness of Cimiafugawas published in Germany as early as I960," clinical trials werenot conducted until 1982. Despite the paucity of quality evi-dence to date, black cohosh is considered by some to be one ofthe three most effective CAM products used by perimenopasualwomen.-' The mechanism of action of black cohosh in the reduc-tion of menopausal symptoms is controversial. Whereas somestudies suggest that black cohosh has estrogenic properties onvaginal cytology and bone markers,*^ others found no effect onvaginal cytology or on gynecologicatly relevant hormones.^'"Other authors suggest that black cohosh has antiestrogenicproperties and augments the effects of tamoxifen in vivo as well
as in vitro." Though the exact mechanism is not known, it issuggested that the combined effects of essential fatty acids, vita-mins, minerals, betacarotenes, and other chemical componentsmay play a role in the observed physiological effects of blackcohosh." Since the publication of the Women's Health Initiativestudy in 2002/* the use of hormone replacement therapy hasdrastically decreased. Fear of breast cancer, stroke, and myocar-dial infarct associated with HRT has led many menopausalwomen experiencing vasomotor symptoms to seek nonhormon-al treatment.
We did not find significant differences in side effects in theblack cohosh and placebo groups. However, two previousreviews reported serious side effects including hepatic sideeffects (hepatotoxocity, hepatic failure, and hepatic enzyme ele-vation) and cardiovascular side effects (arrhythmias and bleed-ing and coagulation disorders)/^^^ Given that black cohosh isone of the most frequently used herbal medications for vasomo-tor symptoms in North America and Europe, more researchabout its effectiveness and safety is warranted.*
AcknowledgmentThe study was condurtctl with the assistance of staff of the I>[iarlmeiil ot Clínica!Epidprniojogv' and Community Studies. St Mary's Hospilal, and funded by the St Mary sHo.spita) Toundation.
Black Cohosh for Menopausal Symptoms ALTERNATIVE THERAPIES, |AN/FEB 2010, VOL. 16, NO. I 43
Rödstriim K. Bengtüsoii C, üssner L, MiLsom 1, Sundh V, Björkelund C. A longitudinalslvidy of the treatment of hot flushes: ihe |)opulation study of women in Gothenburgduring a quarter ot a i'eniur\\ Menopause. 2{M)2:!)(;i):15fi.lfil.
MashchakC. Lobo R. Dozono-TakanoR.ctal. Comparison of pharmacodynamii'propenies of various estrogen ftirmulations. Am) Ohslel Gynecot. 1982;]44(5):5U-518.Loprinzi C, Sloan J. Perez E, et ai. Phase !lf evaluation oldugxetine for treatment iif hotfla.shes./aínOHí,i/,2002;20(fi):1578-1583.
Newton KM, Bui.sl DS. Keenan NL. Anderson LA. l.a(>i)u \Z. Use of alternative thera-pies for menopause symptoms: results of a population-based survey. Olulfl Gynecol.
( l ( '
REFERENCES1. Rowc T. Rlake J, Belisle S. IntroUvKiJcin: Cunfert'cice Canadienne dp lüiisensiis sur la
menopause, mi.se à jour 2006: Chapitre l . /Ofa/f íGiwro ' í ümiJ(i,200t!;S13-S21.2. Bachmann G. Vasomotor flushes in menopausal women. Am J Obxiti Cynecol.
l ! ) 9 9 8 ( : F S
20.
21,
22,
23.
24.
2ri,
26.
28.
KeenanNL. Mark S, Fugh-Berman A. Browne I), Kaczmarezyk), Hunter C. Severit)'ofmenopausa! symptoms and use of both conventional and CDniplpmentary/alternatlvetherapies. Menopuuse. 20():i; 10(ti):507-f>15.
Hlumeiilhal M. Goldberg A, lirinikmarni ]. eds. Hcriml Medicine: Expanded CommissionE Miiiii'iiraph. Newton, MA: Integrative Medicine Communications: 2000.I'hilp ! lA. Hot flashes—a review of the literature on alternative and complementaryfreatmentapproaches./1//crnMf(/Ro', 20Ü3:8(3):284-302.
Kronenberg F. Fugh-Bennan A. Complementary' and alternative medicine fur meno-pausal symptoms: a review of randomized, conirolled trials. Ann liiltrn Mi-d.2O02;!37(lü):8Or,-8B.
Rotem r , Kaplan 8. l'hyto-Femaie Complex for the relief of hot Hushes, night .sweatsand cjiiality of sleep: randomized, controlled, double-blind pilot study. GyneinlEiidocriiwl. 2m7;2H2):ll7-lT2.
Jadad AR, Moore RA. C arroll D, el al. Assessing the quality of reports of randomizeddinical trials: is blinding necessary? C(mfrii/tïi>(7>i'fl/i. 1996; 17(1): 1-12.Cooper ft. Hedges LV. eds. The Haiidboak of Research Synthms. '^ew \QTk, N\: RusxWSage Foundation: 1994.
DerSimonian R, Laird N, Mefa-analysis in clinical trials. Contrtil Clin Trials.1986;7(3): 177-188.Ciurley B. Hubbard MA. Williams [IK. et al. Assessing the clinical significance ofbotanical supplementation on liuman i-jtochrome P4r)0 3A activity: comparison of amilk thistle and black cohosh product to dfampin and rlarithromyt i n j Clin Pharmacol2OO6:46(2):2tll-2i:i. '
tlurley BJ. Barone f.W. Williams DK, et al. Effet of milk thistle (Silybum marianum)and black cohosh iCimicißigu racemaia) supplementation on digoxin pliamiarokineticsin humans, Dru^Melah ilispiK. 2O(W:34(l):69-74.
Haas K. Bnicker C, Gorkow (.. Wuttke W. First-time proof of endometrial wfet)' of thespecial black cohosh extract (Actaeo or Cimidßiga racemosa extract) CR BNÓ 1055.Maluritas. 2(«fi; B(4):678-fi91.
Vermes G, Bánhidy F, Acs N. The efîects of Remifemin on subjective symptoms ofmenopause. Adv Ther 2005;22(2): 14K-l54.Briese V. Slamniwitz U. Friede M, Henneicke-vim Zepelin HH. Black cohosh with orwithout Si. John's wort tor symptom-specific climacteric treattnent: results of a largescale, controlled, obser\ational study. Maturilax. 2O07:57(4):405-414.Pockaj BA, l.oprinzi CL Sloan )A. et al. Pilot evaluation of black cohosh lor the treat-ment of hot flashes in women. Cmctr liiml. 2004;22(4):51&-521.I.ieberman S, A review oí the ellectiveness nfCimirífiiga racanosa (black cohosh) fiir thesyit\j)tomsofinenopause.ytViim™iWi(i///i, 1998;7(5):525-529.Hernández Muñoz G, Pluchino S, Cimirifuga racemosii fbr the treatnienf of lioi flushesin women surviving breast cancer. Maluriiiu. 2003:44(Suppl I):S59-5i)5.Jacohwm JS, Tro\el AB, Evans J, el al. RandomÍ7,ed triai of black cohosh fbr the treat-ment of hot flashes among women with a history of breast tamer. / Clin Oncol.2OO1;I9(1O);2739'2745, ' '
Pockaj BA. Gallagher JG, ljipriii/,i Ct,, et al. Phase III double-blind, random i zed, place-bo-controlled crossover trial of black cohosh in the management of hoi flashes: NCCTGTrial NO]CCl,y Clin Onrol. 2()(W:24(18):2836-2841.
Burke BE. Olson R|l, ( usack BJ. Randomized. conlmlleiJ trial of phytoestrogen in theprophylactic treatment of menstrual migraine. Biiimfil Pliannmother. 2Ó02;5f)(li):28;í-288.Spangler L, fvewioti KM. Grothaus LC, Heed SD, Ehrlich K, LaCroix A2. The eßects ofblack rohosh therapies on lipids, fibrinogen, glucose and insulin. Maturitas.2007:57{2):l 95-204.
Verhoeven MO, Teerlink T. Keneiiians P, Zuijdgeesi-van Leeuwen SD, van der MoorenMJ. EfTects ufa supplement containing isoflavones and Aclaea racemom L on asymmet-ric di methyl a I gin in e, lipids, and C-reactive protein in menopausal women, fértil Steril.2007;84(4):84H-857.
Bai W. Henneicke-\'on Zepelin HH. Wang S, et al. Efficacy and tolerability of a medici-nal product containing an isopropanolir black cohosh extract in Chinese women withmenopausal symptoms: a randomized, double blind, paraliei-controlled study versustibolone. Maturilas. 2007;58(l):31-41.¡.iske E. Hänggi W, Henneicke-von Zepelin HH. Boblitz N, Wüstenberg P, itahtfs VW.Physiological investigation of unique extract of black cohosh iCimiciJiigae racemtisiurhitomii): a 6-monih clinical study demonstrates no systemic estrogenic efFect.yWomentiHealth GeiidBasedMed.2im:\\(2).\m-\7^-
Nappi RE, Malavasi B. Bruttdu B. lacchinelti E. Etficacy oí Cimicifiiga racemosa on cli-macteric complaints: a randomized study versus low-dose Iransdermal estradiol.
37.
Oktem M, Eroglu D, Karahan HR. Taskintuna N', Kuscu E, Zeyneloglu I IB. Black cohoshand fiuoxeiine in the treatment of postmenopausal symptoms: a prospective, rand<Jm-ized irial, Adv Ther. 2007;24(2):44a-461.
Newton KM, Reed SD, Grolhaus L, el al. The Herbal Alternatives for Menopause(HALT) Study: background and sludy design. Maluritas. 2005;52(2): 134-146.Newton KM, Reed SD. UCroix A, (irothaus LC, Ehrlick K, Guiltinan J, Treatment ofvasomotor symptoms ofmenopause with black cohosh, muitibolanicals, soy, honnonetherapy, or placebo: a randonii/ed trial. Ohstel Gynecol Surv. 2007:62(4):249-250.Wutike VV, Rau K, Gorkow C, Efficacy and lolerability ol'the hIack cohosh {Actaea rac-emnsa) eihnanolic extract BNO 1055 on climacteric complaints: a double-blind, place-bo- and conjugated estrogens-con I rol led study. Maturitas. 2006;55 (Suppl 1):S83-S91.Newton KM, Reed SD. UCroix AZ, Grothaus LC, Ehriich K, Guiltinan (. Treatment ofvast>tnotor symptoms of metiopatise with black cohosh, tnultibotanicals, soy, hormonetherapy, nr placebo: a randomi/ed irial. Ann Intern Med. 2(>l)6; 145(12):869-879.Verlîoeven MO, van der Mooren MJ, vati lie Weijer PI I, el al. Efiect of a combination ofisoflavones and .Actaea racemosa Unnai-iLS on climacteric symptoms ¡n healrh)' symp-tomatic perimenopausal women: a 12-week randomized, placebo-con tro lied, double-blind study. Mmo/wusr, 2005;12(4):412-420.
Sammariino A , Tommasclli GA. Gargano V, di Carlo C. Attianese W, Nappi C. Short-lertn effeds of a combination of Isoftavones, lignans and Cimicifuga racemosa on cli-macteric-related symptoms in postmenopatisal women: a double-blind randomized,placebo-controlled trial. G|wru/£'fli/(Jifjnii/,2006;22(ll):646-6r)0.Chutig DJ, KLm li\ ' . Park KH, et al. Black cohosh and St. John's wort (GVNO-Plus) forclimaderic symptoms. Yonst-iMedj. 2t)07:48(2):289-294,
Debelhack R, Blohmer Jl', Graubaum HJ, Busch R, (iruenwald J, Wernecke KD, Blackcohosh and St. John's worl tor iliinacteric complaints: a ratidotnized trial. ObstetCynecol. 2006:107(2 Pr l):245-255,
Frei-Kleiner S, SchaHrier W. Rahlls VW, Bodmer C, Birkhauser M. Cimicifuga raiermmdried ethanolic estraci in menopausal disorders: a double-blind placebo-controlledclinical trial. Maturitin. 2005:51 (4):397-404.
Osmers R, Friede M, l.iske E. el al, Eflicacy and safety of isopropanolic black cohoshextractforclimactericsiTnploms.Oiiîff/o'imi/, 2005:105(5 Pi 0:1074-1083.Wiiilke W, Seidlová-Wuttke D, tiorkow C. The Cimicifuga preparation BNO 1055 vs.i.i)n;ugated estrogens in a douhle-hlind placebij-contriilled study: efFect,s on menopausesymptoms and bone tnarkers. Maturitas. 2003:44 Supj)! l:S67-577,Mom CH, Buijs C, WQlemse PH, Moiirits MJ, de Vries Eti, Hot flushes in breasl cancerpatients, Cn/An'Onro///email)/. 2006;57il):63-77.
Shatiafell TD, Barton DL. Adjei AA, Loprinzi CL, Pathophysiology and trealment ofhotflashes-MiJiwCi/n/•/•.«:. 2002:77(10:1207-1218,
Macl.ennan A, U'ster S, Moore V. Oral oestrogen replacement therapy versus placebofor hot flushes. Coehrane Datahase ij.ç/ Rir. 2001;(] ):CDI)()2978.Easterbrook PJ, Berlin JA, Gopalan R, Mallhews PR, Publication bias in clinicalresearch. Liiicit. 1991 ::i37(8746):867-872.
Pitlier MH. Abbot NC, Harkness EE, Ernst E. Location bias in controlled clinical trialsofcomplementary/alternativetherapie.s,yC/;n£/))(/miij/. 20(H);5:Í(5):4R5-489.
Sood A, Knutlsen K, Sood R, et al. Publication bias for CAM trials in the highest impactfactor medicine journals is partly due to geographical bias. / Clin Epidemiol.2t»7:60(lO;n23-1126,
Borreili F, ILrnsi E. Cimiafuga racemosa: a systematic review of its clinical efficacy, Eur}Pharmacol. 2002:58(4) :2 35-241,Linde K, Berner MM. Kriston 1,. St John s wort for major depression. CochraneDatabase Syst Ra: 2008 Oct 8:(4):C[XK1O448.
Brücker A. Beitrag zur Phytothérapie hormonaler Störungen der Frau, Merl Welt.1960:44:2331-2333.van der Sluijs CP, Bensoussan A. Liyanage L, Shah S. Women's health during mid-lifesurvey: the use of (omplementary and alternative medicine by symptomatic womeniransitioninglhroughnienopaiiseinSydney.Mrnii/jawf, 2007:14(3 Pt 0:397-403.Nisslein T. Freudenslein J. Concotnitant administration of an isopropanolic extract ofblack cohosh and lamoxifen in the in vivo tumor model of itnplanted RUCA-I rat endo-metrical adenocarcinoma cells. 7(w/cWM/. 2OO4;15O<3):271-275.RossouwJE, Anderson GL, Prentice RL, ei al: Writing Group fbr the Women's HealthInitiative Invesligalors, Risks and benpfits of estrogen plus progestin in heailhy post-menopausal women: principal results From ihe Women's Hvalth Initiative randomizedconirolled inal.JAMA. 2002:288(3):321-33:i,
Mahady GB, Black cohosh {Aciaea/Cmiiaßiga racemosa): review of the clinical data torsafety and efficacy in menopausal symptoms. Treat Endocrino!. 2005:4(3): 177-184.Huntley A, Ernsi L A systematic review of the .safety of black cohosh.2003;10(O:, ' :Í8-64,
44 ALTERNATIVE THERAPIES, lAN/FER 2010, VOL 16, NO. 1 Black Cohosh for Menopausal Symploms

Copyright of Alternative Therapies in Health & Medicine is the property of InnerDoorway Health Media and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.