effects of treatment of chronic hbv infection on patient
TRANSCRIPT

Accepted Manuscript
Effects of Treatment of Chronic HBV Infection on Patient-reported Outcomes
Zobair M. Younossi, Maria Stepanova, Harry L.A. Janssen, Kosh Agarwal, MindieH. Nguyen, Ed Gane, Naoky Tsai, Issah Younossi, Andrei Racila
PII: S1542-3565(18)30225-8DOI: 10.1016/j.cgh.2018.02.037Reference: YJCGH 55725
To appear in: Clinical Gastroenterology and HepatologyAccepted Date: 25 February 2018
Please cite this article as: Younossi ZM, Stepanova M, Janssen HLA, Agarwal K, Nguyen MH, GaneE, Tsai N, Younossi I, Racila A, Effects of Treatment of Chronic HBV Infection on Patient-reportedOutcomes, Clinical Gastroenterology and Hepatology (2018), doi: 10.1016/j.cgh.2018.02.037.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Effects of Treatment of Chronic HBV Infection on Patient-reported Outcomes
Zobair M. Younossi* 1, 2, Maria Stepanova3, Harry L. A. Janssen4, Kosh Agarwal5, Mindie H.
Nguyen6, Ed Gane7, Naoky Tsai8, Issah Younossi3, Andrei Racila3
1Center for Liver Diseases, Department of Medicine, Inova Fairfax Hospital,
2Betty and Guy Beatty Center for Integrated Research, Inova Health System, Falls Church, VA,
USA
3Center for Outcomes Research in Liver Disease, Washington DC, USA,
4Toronto Centre for Liver Disease, University Health Network, Canada,
5Institute of Liver Studies, Kings College Hospital, London, United Kingdom,
6Stanford University Medical Center, Palo Alto, California, USA
7Auckland Clinical Studies, Auckland, New Zealand
8Queens Medical Center, University of Hawaii, USA
* Corresponding Author:
Zobair M. Younossi, MD, MPH
Betty and Guy Beatty Center for Integrated Research
Claude Moore Health Education and Research Building
3300 Gallows Road, Falls Church, VA 22042
Phone: (703) 776-2540
Fax: (703) 776-4386
Email: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Word Count: 3589
Tables and Figures: 1+5
Funding Source: Gilead Sciences
Conflicts of Interest: ZY, HJ, KA, EG, NT have received research support or consultant fees
from Gilead. Otherwise no conflict
Author’s Contributions:
Zobair M. Younossi: study guarantor, study design, data interpretation, manuscript development
and critical review of the manuscript.
Maria Stepanova: statistical analysis, data interpretation, manuscript development and critical
review of the manuscript
Harry L. A. Janssen: critical review and editing of the manuscript
Kosh Agarwal: critical review and editing of the manuscript
Mindie H. Nguyen: critical review and editing of the manuscript
Ed Gane: critical review and editing of the manuscript
Naoky Tsai: critical review and editing of the manuscript
Issah Younossi: data management and critical review of the manuscript
Andrei Racila: data management and critical review of the manuscript
Abbreviations:
BMI - body mass index; BP - Bodily Pain; CLDQ - Chronic Liver Disease Questionnaire; CHB -

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
chronic hepatitis B; DNA - deoxyribonucleic acid; GH - General Health; HBV - hepatitis B
virus; MCS - Mental Component Summary; MH - Mental Health; OAV - oral antiviral; PCS -
physical component summary; PF - Physical Functioning; PRO – patient-reported outcomes; RE
- Role Emotional; RP - Role Physical; SF-36 - Short Form 36; SF - Social Functioning; TDF-
tenofovir disoproxil fumarate; VT – Vitality; WPAI - Work Productivity and Activity
Impairment.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
ABSTRACT
Background and aim: Chronic infection with hepatitis B virus (HBV) causes liver disease and
cirrhosis. It is not clear how treatment of chronic HBV infection affects patient-reported
outcomes (PROs). We aimed to assess changes in PROs in patients treated for chronic HBV
infection.
Methods: We collected and analyzed PRO data from 242 patients with chronic HBV infection
(without advanced fibrosis or cirrhosis) enrolled in 2 international phase 2 blinded controlled
clinical trials from 2015 through 2017. In these trials, patients were treated with an approved oral
antiviral regimen (tenofovir, entecavir, adefovir, lamivudine, or telbivudine) and then randomly
assigned to groups given vesatolimod (an oral agonist of toll like receptor 7) or placebo. PROs
were collected using the Short Form-36, the Chronic Liver Disease Questionnaire, and the Work
Productivity and Activity Impairment: Specific Health Problem scoring system before treatment,
on treatment weeks 12, 24, and 48.
Results: We did not observe significant differences in PROs between patients receiving
vesatolimod vs placebo. At baseline, patients with viral suppression (level of HBV DNA <20
IU/mL) had higher PRO scores (by up to +10.6% of a PRO range size). During treatment, there
were significant increases in scores for some domains of Chronic Liver Disease Questionnaire
and in General Health scores of Short Form-36 (increases of up to 4.9%; P<.05). Patients with a
decrease of at least 2.7 log10 IU/mL in level of HBV DNA had substantially larger increases in
PRO scores (mean increases of up to 7.2% by week 48; P<.05 for 10 of 22 studied PROs). In
multivariate analysis, a reduction in viral load was independently associated with increases in
PROs (betas values up to 1.6% per log10 IU/mL decrease; P<.05).
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Conclusions: In an analysis of data from phase 2 trials, we associated active treatment of chronic
HBV infection with increased PRO scores. These findings support inclusion of PRO endpoints in
assessments of efficacy and safety in clinical trials of treatments for HBV infection.
Keywords: CLDQ, SF-36, health-related quality of life, fatigue, utility.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
INTRODUCTION
Chronic hepatitis B (CHB) infection is a major cause of chronic liver disease and hepatocellular
carcinoma (HCC) worldwide [1]. Although the medical burden of CHB (cirrhosis, HCC, and
mortality) has been well described [2-3], there is little data on the impact of HBV to patient-
reported outcomes (PROs) which are, by definition, the outcomes directly reported by patients
without any modification [4].
Over the past decade, treatment of CHB has seen tremendous advancements. In fact, there are
now a number of regimens that can effectively suppress HBV replication [5-6], and this
sustained viral suppression of HBV has been convincingly shown to improve hepatic fibrosis [7-
8] and complications of HBV-related cirrhosis [9]. On the other hand, the effect of HBV viral
suppression on PROs has been studied less extensively [10]. Therefore, the aim of this study was
to systematically assess PROs in patients with chronic HBV infection with and without viral
suppression using the data collected from participants of multinational studies who are treated
with oral antiviral (OAV) regimens for HBV.
METHODS
In this study, we used PROs collected as exploratory endpoints in two multinational,
randomized, double-blind, placebo-controlled phase 2 clinical trials of vesatolimod, an oral toll-
like receptor 7 agonist (GS-US-283-1059 and GS-US-283-1062, clinicaltrials.gov
#NCT02166047, #NCT02579382). All authors had access to the study data and reviewed and
approved the final manuscript.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
In GS-US-283-1059, prior to enrollment, patients were required to have been treated with an
approved HBV OAV (tenofovir, entecavir, adefovir, lamivudine or telbivudine, either as single
agents or in combination) for at least a year, with no change in the regimen for 3 months prior to
screening, and to have HBV DNA level below the lower limit of quantification measured at least
once in 6 months prior to screening followed by HBV DNA <20 IU/ml at screening. Enrolled
participants were randomized 3:3:3:1 to receive 1, 2, or 4 mg of vesatolimod once a week for 11
weeks (12 doses) or a matching blinded placebo in addition to their OAV.
In GS-US-283-1062, enrolled patients were required to be not on treatment for at least 3 months
prior to screening and to have HBV DNA ≥2,000 IU/mL at screening. All patients were then
started on tenofovir disoproxil fumarate (TDF) and were randomized to receive either 1, 2, or 4
mg of vesatolimod once a week for 11 weeks (12 doses) or a matching placebo in addition to
TDF; after discontinuation of vesatolimod at 11 weeks, patients continued TDF for 37 more
weeks with a total duration of treatment of 48 weeks.
The trials were conducted in 2015-2017 in the United States, Canada, United Kingdom, Italy,
New Zealand, Hong Kong, South Korea, and Taiwan. In both trials, patients with extensive
bridging fibrosis or cirrhosis (defined by a liver biopsy with Metavir ≥ 3, Ishak ≥ 4, or FibroTest
score of > 0.58 and APRI > 1, or FibroScan > 9 kPa within 6 months of enrollment, or evidence
of cirrhosis by imaging or clinical presentation such as ascites, varices etc.), hepatocellular
carcinoma, coinfection with HIV, HCV or HDV, or any other major comorbidity were excluded.
Complete details of the primary and secondary safety and efficacy outcomes of those trials have
been published elsewhere [11-12].

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
Patient-reported outcomes
Patient-reported outcomes were prospectively collected using 3 validated instruments: the Short
Form-36 (SF-36), the Chronic Liver Disease Questionnaire (CLDQ), and the Work Productivity
and Activity Impairment: Specific Health Problem (WPAI:SHP) [13-16]. The instruments were
self-administered by patients at baseline (day 1 of treatment), treatment week 12, 24, and 48
visits while blinded to their most recent laboratory test results and before initiation of any other
study-related activities for those visits.
The SF-36 is a generic HRQL instrument which includes 8 domains: Physical Functioning (PF),
Role Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning
(SF), Role Emotional (RE), and Mental Health (MH) (all range 0-100). The domain scores are
used to calculate two summary scores: Physical Component Summary (PCS) and Mental
Component Summary (MCS) scores. Additionally, preference-based SF-6D health utility scores
were calculated using SF-36 responses and a previously published non-parametric Bayesian
algorithm [13-14].
The CLDQ is a disease-specific PRO instrument which assesses HRQL in patients with chronic
liver disease. The instrument has six domains: Abdominal Symptoms, Activity/Energy,
Emotional, Fatigue, Worry, and Systemic Symptoms (all range 1-7), and a total score which is an
average of the domain scores [15].
The WPAI:SHP instrument is used to assess impairment in daily activities and work productivity

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
associated with a specific health problem (in this study, HBV infection). It includes Work
Productivity Impairment domain, which is a sum of Absenteeism and Presenteeism domains, and
Activity Impairment domain (all range 0-1). Unlike other instruments, greater scores indicate
more impairment [16].
Combined together, these PRO instruments return 22 domain and summary scores (8 domain + 2
summary + 1 utility score from SF-36, 6 domain + 1 summary score from CLDQ, and 4 domain
scores from WPAI:SHP). Where stated explicitly, for presentation purposes, PRO scores were
transformed from their original scales to a universal 0-100 scale.
Statistical Analysis
Clinico-demographic parameters, baseline and on-treatment PRO scores were compared between
patients with and without baseline viremia, and between patients receiving different regimens
using chi-square or non-parametric Mann-Whitney test. Changes (improvements or decrements)
in PRO scores were calculated at weeks 12, 24, and 48 with reference to patients’ own baseline
levels, and were compared to zero (which would indicate no significant change) using a signed-
rank test. Spearman’s correlation of the changes in HBV viremia and ALT with the changes in
PROs were calculated. A threshold for a drop in viremia which would return the greatest
association with the changes in PROs (quantified as the number of significantly different
changes in PROs with the highest average effect size) was selected.
Independent predictors of baseline PROs in patients with HBV were assessed using generalized
linear models; the presence of HBV viremia (as opposed to baseline virologic suppression with

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
OAVs), age, gender, race, location, BMI, history of type 2 diabetes, psychiatric disorders, and
clinically overt fatigue were tested as potential PRO predictors. In addition, independent
predictors of on-treatment PROs were assessed using generalized linear models with adjustment
for repeated measures; the models included potential PRO predictors listed above, baseline PRO
levels, and changes in treatment-emergent HBV viremia. Only predictors with p<0.05 were left
in the models after bidirectional stepwise selection of significant predictors.
All analyses were run using SAS 9.4 (SAS Institute, Cary, NC). The study was approved by each
site’s Institutional Review Board.
RESULTS
A total of 242 patients with chronic HBV infection were included. Of these, there were 50 HBV
patients with PRO data who were enrolled in GS-US-283-1059 (virally suppressed at baseline; 5
treated with OAV+placebo and 45 with OAV+vesatolimod). Additionally, 192 HBV patients
with PRO data were enrolled in GS-US-283-1062 (viremic at baseline, started on TDF; 28
treated with TDF+placebo and 164 with TDF+vesatolimod). In viremic subjects, the mean HBV
DNA at baseline was 5.8±1.8 log10 IU/mL. Other clinico-demographic parameters of the study
participants are summarized in Table 1. Briefly, virally suppressed subjects were older, mainly
male and white, predominantly enrolled in Italy, less employed, and had substantially longer
duration of infection (p<0.05). They also had lower prevalence of hepatitis B e antigen and
antibody positivity, lower HBV surface antigen (HBsAg), aspartate aminotransferase (AST) and
alanine aminotransferase (ALT) levels, but higher Fibrotest scores, and lower platelet levels. The
prevalence rates of psychiatric comorbidities (depression, anxiety), sleep disorders, and clinically

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
overt fatigue were less than 4% (Table 1).
Patient-reported outcomes in patients with HBV
At baseline, non-viremic subjects had significantly higher PRO scores in a number of disease-
specific and some generic domains (by, on average, 6.5 to 10.5 points on a 0-100 PRO scale;
p<0.05 for General Health and Mental Health of SF-36, and all but one of the CLDQ domains)
(Figure 1, Supplementary Figure 1). Furthermore, even when adjusted for the baseline
demographics, significant independent association of HBV viremia with PRO impairment was
observed (betas range from -5.7 to -10.1 points, p<0.05) (Figure 2). Other predictors of baseline
PRO impairment include gender, country of enrollment, race, BMI, history of psychiatric
comorbidities, sleep disorders, and clinically overt fatigue (Supplementary Table 2).
During treatment, there was no difference in treatment-emergent changes in PROs in patients
receiving OAV+placebo and OAV+vesatolimod in both studies (all p>0.05) (Supplementary
Figure 1). Given that the addition of vesatolimod had no impact on PROs, the subjects were
merged into one cohort regardless of the treatment arm. In the combined cohort receiving active
antiviral suppressive treatment with OAV, significant increases in the scores of General Health-
SF-36 were observed during treatment (average +3.2 by week 24, +3.2 by week 48), Fatigue,
Worry, and total CLDQ (average +1.2 to +4.9 by weeks 24 and 48) (all p<0.05).
Association of a decrease in HBV DNA viremia with improvement in PROs
Of patients who started treatment non-viremic, 100% maintained their viral suppression during
the duration of the study. Of patients who were enrolled while viremic, 100% had at least 1.7
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
log10 decrease in HBV DNA levels by treatment week 12, and the average (± standard
deviation.) decrease in HBV DNA level was -3.7±1.0 log10 IU/mL by week 12, -4.1±1.4 log10
IU/mL by week 24, and -4.2±1.7 log10 IU/mL by week 48. Furthermore, of patients who
remained viremic by week 48 (N=56), 86% had HBV DNA below 2000 IU/mL despite starting
from substantially higher baseline levels (4.1±2.1 log10 IU/mL in patients with HBV DNA <20
IU/mL by week 48 vs. 7.4±1.6 log10 IU/mL in those with week 48 HBV DNA ≥ 20 IU/mL,
p<0.0001). In turn, a decrease in viremia correlated with a decrease in ALT, especially after 24
weeks of treatment (Rho=0.34 at week 12, 0.48 at week 24, 0.47 at week 48; all p<0.0001).
The magnitude of a decrease in both HBV viremia and ALT significantly correlated with
increases in a number of PROs although the correlations with ALT decrease were weaker
(p<0.05 for 8/22 PRO domain scores with HBV DNA, 4/22 for with ALT) (Supplementary
Table 3). In a round of dynamic search, it was found that the threshold of -2.7 log10 IU/mL for
the change in HBV viral load was associated with the greatest number of significant changes in
PRO scores (Supplementary Figure 2A). Again, a similarly defined threshold for ALT change
(-12 IU/L) returned weaker association with PRO improvement (Supplementary Figure 2B).
Given that, we considered patients with a decrease in HBV DNA of at least 2.7 log10 IU/mL by a
given time point to be viral responders, as opposed to viral non-responders (i.e., patients who had
their HBV DNA decreased by less than 2.7 log10 IU/mL by that time point).
By treatment week 12, there was a minimal difference in treatment-emergent changes in PRO
scores between viral responders and non-responders (145 vs. 91, p<0.05 for Worry of CLDQ
only) although significant PRO improvements in some domains (on average, +2.1 to +6.0 points,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
p<0.05 in General Health of SF-36, Emotional, Worry and total of CLDQ) were noted in
responders but not in non-responders. However, by treatment weeks 24 and 48, significantly
greater PRO improvements were noted in responders in contrast to no improvement or
significant decrements in PRO scores in non-responders: +2.9 to +7.0 vs. -2.9 to -6.7, p<0.05 for
10/22 PROs, by treatment week 24 (N=149 vs. 88); +1.9 to +7.2 vs. -5.1 to -9.8, p<0.05 for
10/22 PROs, by treatment week 48 (N=144 vs. 92) (Figure 3, Figure 4). Similar findings,
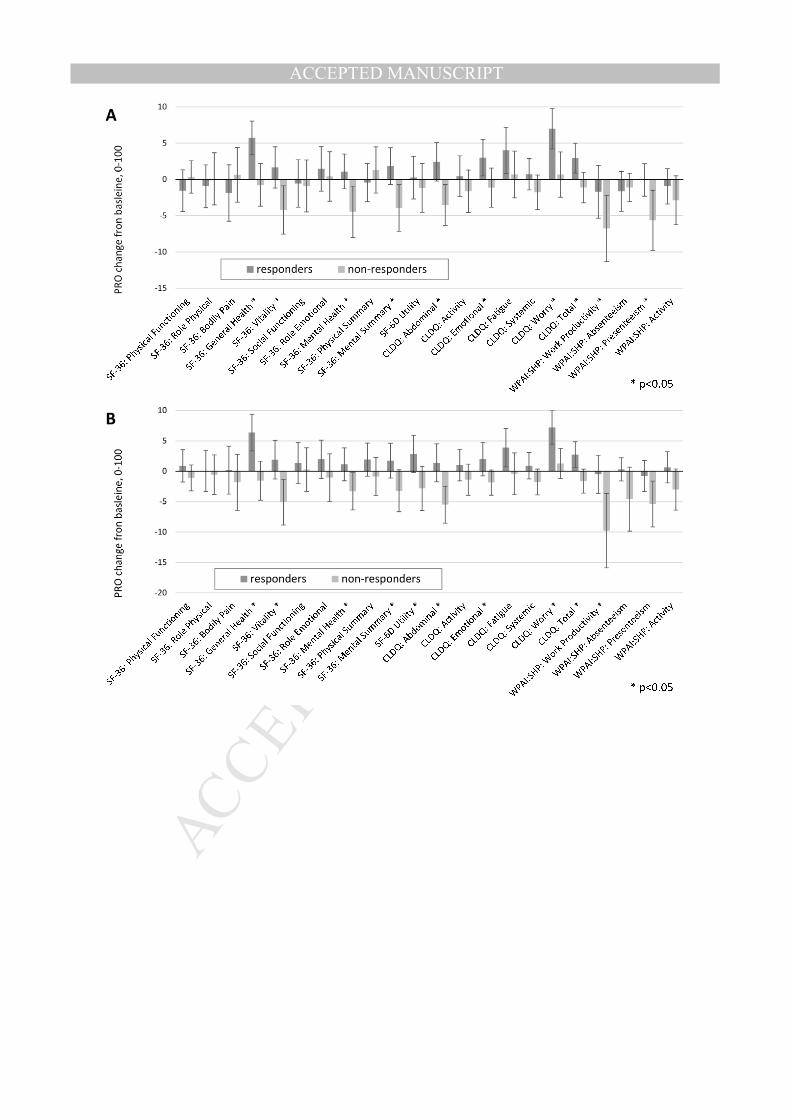
including substantially superior PRO scores in viral responders in comparison to non-responders
(+2.9 to +7.0 vs. -4.9 to -7.5, p<0.05 for 8/22 PROs, by treatment week 12; +1.9 to +7.2 vs. -4.9
to -8.0, p<0.05 for 12/22 PROs, by treatment week 48) were also observed in a subgroup
analysis of patients with baseline viremia (Supplementary Figure 3).
In multivariate analysis with adjustment for the baseline PRO levels, repeated measures, the type
of treatment received, and for clinico-demographic factors, the magnitude of a decrease in HBV
DNA was found to be significantly predictive of an increase in some generic and most disease-
specific PRO scores: betas from +0.5 to +1.6 points per each additional -1 log10 IU/mL (Figure
5); notably, that would yield between +1.9 and +6.9 points to PRO scores in patients with a
decrease in HBV DNA equal to the average observed in this study (-4.2 log10 IU/mL). In
contrast, there was no independent association of PRO improvement with achieving HBV DNA
<20 IU/mL during treatment (all p≥0.05).
DISCUSSION
In this study, we reported PRO assessment in patients with chronic HBV infection according to
their viremia status before and after treatment with OAV regimens. The most important finding

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
of the study is that the level of a decline in HBV DNA seems to predict PRO improvement, and,
expectedly, disease-specific PROs are affected more than generic.
There are a number of other clinically relevant observations made in this study. First, we noted
that patients with HBV rarely reported neuro-psychiatric comorbidities (such as depression or
anxiety) and clinically overt fatigue. This is in contrast to chronic HCV infection where a large
proportion of patients report these comorbidities [17-21]. Second, on-treatment PROs did not
differ between patients treated with placebo and vesatolimod regardless of the dosage,
suggesting that vesatolimod may have few side effects that could negatively impact PROs. Third,
the baseline level of HBV DNA predicted PRO impairment which primarily manifested via
lower CLDQ domain scores. Fourth, we demonstrated that a decline in HBV DNA viral load was
associated with improvement of some PROs. In this context, a decline of at least 2.7 log10 IU/mL
from the baseline seems to produce the most significant improvement of PRO scores when
compared to patients who did not experience a similar decline. Finally, our multivariate analysis
showed that the magnitude of the decrease in HBV DNA level was an independent predictor of
PRO gains, again primarily captured by the disease-specific domains of CLDQ.
Interestingly, we found that achieving complete viral suppression (HBV DNA <20 IU/mL) alone
or with adjustment for a treatment-emergent decline in HBV DNA was not necessarily
associated with improvement of PROs. This finding is likely related to the fact that even though
some patients may not achieve complete viral suppression with OAV treatment, they still
experience HBV DNA declines to relatively low levels (of those with >20 IU/mL by week 48,
86% had it <2000 IU/mL) which were probably low enough not to cause any residual negative

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
effect on PROs. These data are consistent with a prior report from a large cohort study of patients
with HBV enrolled to be treated with OAVs in South Korea [10]. In that study, achieving post-
treatment HBV DNA level of or below 4 log10 IU/mL was associated with pronounced PRO
improvement. Since in this study, 97.9% patients achieved that level after 48 weeks of treatment,
we were unable to validate that report beyond demonstration that significant PRO impairment
does not seem to manifest with mere presence of detectable viremia. In this context, it is also
important to note that patients included in this study were enrolled in 8 countries, including
North America, Europe, Southeast Asia, and New Zealand, and from multiple racial/ethnic
groups which may result in better generalizability of our findings.
The mechanisms behind the reported association of HBV DNA decline with changes in PROs
are not clear and need to be studied. Nevertheless, previous reports regarding similar effects in
successfully treated patients with HCV have suggested that a decrease in systemic inflammation
may be responsible for PRO improvement [22-23]; this may also play a role in patients with
HBV suppression. It is, however, important to note that improvements in PROs seen in patients
with HBV are generally smaller than PRO improvements reported in patients with HCV who
achieve sustained virologic response [24-25]. Although the exact reasons are unclear, these
differences could be related to the fact that HCV infection tends to cause a greater impairment in
quality of life, more depression, fatigue, and other systemic sequelae in infected patients [17-21].
The implications of this study are clinically pertinent. In the context of comprehensive
assessment of HBV, our data support the notion that HBV viremia has a negative impact not
only on clinical outcomes of HBV-infected patients but also on their patient-reported outcomes.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
In contrast, viral suppression with antiviral agents for HBV can improve patients’ quality of life
and other PROs, and this enhances the value of anti-viral treatments to HBV-infected patients.
Limitations of the study include limited sample size, the lack of independent validation of the
viral responder definition, and clinical trial setting of the studies which might have biased both
the sample of patients and their PROs. Given that, the findings need to be validated in larger
studies involving more diverse patient populations from real-world settings.
In summary, our data show that HBV viremia is associated with PRO impairment while a 2-3
log10 drop in HBV DNA level may result in improvement of PROs. A comprehensive approach
to outcomes assessment in HBV can capture the total burden of HBV infection on patients’ lives
and determine the comprehensive benefit of treatment. This information should inform patients,
healthcare providers, payers, and policy makers to make decisions to maximize value to our
patients and the society.
REFERENCES
1. World Health Organization (WHO). Facts on HBV- July 2017.
http://www.who.int/mediacentre/factsheets/fs204/en/. Last accessed on 9/12/2017.
2. Wu JF, Chang MH. Natural history of chronic hepatitis B virus infection from infancy to adult
life - the mechanism of inflammation triggering and long-term impacts. J Biomed Sci. 2015 Oct
20;22:92.
3. Chen CJ, Yang HI. Natural history of chronic hepatitis B REVEALed. J Gastroenterol
Hepatol. 2011 Apr;26(4):628-38.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
4. Centers for Disease Control- Health Related Quality of Life.
http://www.cdc.gov/HRQoL/concept.htm. Last accessed on 31 August 2017.
5. Gish RG, Given BD, Lai CL, Locarnini SA, Lau JY, Lewis DL, et al. Chronic hepatitis B:
Virology, natural history, current management and a glimpse at future opportunities. Antiviral
Res. 2015 Sep;121:47-58.
6. Russo FP, Rodríguez-Castro K, Scribano L, Gottardo G, Vanin V, Farinati F. Role of antiviral
therapy in the natural history of hepatitis B virus-related chronic liver disease. World J Hepatol.
2015 May 18;7(8):1097-104.
7. Liaw YF. Impact of therapy on the outcome of chronic hepatitis B. Liver Int 2013; 33 Suppl 1:
111-115
8. Shim JJ. Long-Term Suppression of Viral Replication in Chronic Hepatitis B: Outcomes and
Future Directions. Gut Liver. 2015 May; 9(3): 265–266.
9. Kim CH, Um SH, Seo YS, Jung JY, Kim JD, Yim HJ, et al. Prognosis of hepatitis B-related
liver cirrhosis in the era of oral nucleos(t)ide analog antiviral agents. J Gastroenterol Hepatol.
2012 Oct;27(10):1589-95.
10. Kim JH, Kwon SY, Lee YS, Lee JH, Lee YS, Lee CH. Virologic response to therapy
increases health-related quality of life for patients with chronic hepatitis B. Clin Gastroenterol
Hepatol. 2012 Mar;10(3):291-6.
11. Janssen HLA, Brunetto MR, Kim YJ, Ferrari C, Massetto B, Nguyen AH, et al. Safety,
Efficacy and Pharmacodynamics of Vesatolimod (GS-9620) in Virally-Suppressed Patients with
Chronic Hepatitis B. J Hepatol. 2017 Nov 2. doi: 10.1016/j.jhep.2017.10.027. [Epub ahead of
print]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
12. Gilead Sciences US-283-1062. A Study of the Safety, Tolerability, and Efficacy of
Vesatolimod in Combination With Tenofovir Disoproxil Fumarate (TDF) in Adults With
Chronic Hepatitis B (CHB) Infection Who Are Currently Not Being Treated.
https://clinicaltrials.gov/ct2/show/NCT02579382. Last accessed on 11/19/2017.
13. Ware JE, Kosinski M. Interpreting SF-36 summary health measures: a response. Qual Life
Res. 2001;10(5):405-13; discussion 415-20.
14. Kharroubi SA, Brazier JE, Roberts J, O'Hagan A. Modelling SF-6D health state preference
data using a nonparametric Bayesian method. J Health Econ. 2007 May 1;26(3):597-612.
15. Younossi Z M, Guyatt G, Kiwia M, Boparai N, King D. Development of a disease specific
questionnaire to measure health related quality of life in patients with chronic liver disease. Gut
1999;45:295-300.
16. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity
and activity impairment instrument. PharmacoEconomics 1993;4:353-65.
17. Kallman J, O'Neil MM, Larive B, Boparai N, Calabrese L, Younossi ZM. Fatigue and health-
related quality of life (HRQL) in chronic hepatitis C virus infection. Dig Dis Sci. 2007
Oct;52(10):2531-9.
18. Weinstein AA, Kallman Price J, Stepanova M, Poms LW, Fang Y, Moon J, et al. Depression
in patients with nonalcoholic fatty liver disease and chronic viral hepatitis B and C.
Psychosomatics. 2011 Mar-Apr;52(2):127-32.
19. Adinolfi LE, Nevola R, Rinaldi L, Romano C, Giordano M. Chronic Hepatitis C Virus
Infection and Depression. Clin Liver Dis. 2017 Aug;21(3):517-534.
20. Iriana S, Curry MP, Afdhal NH. Neurologic Manifestations of Hepatitis C Virus Infection.
Clin Liver Dis. 2017 Aug;21(3):535-542.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
21. Younossi Z, Park H, Henry L, Adeyemi A, Stepanova M. Extrahepatic Manifestations of
Hepatitis C: A Meta-analysis of Prevalence, Quality of Life, and Economic Burden.
Gastroenterology. 2016 Jun;150(7):1599-1608.
22. Gerber L, Estep M, Stepanova M, Escheik C, Weinstein A, Younossi ZM. Effects of Viral
Eradication With Ledipasvir and Sofosbuvir, With or Without Ribavirin, on Measures of Fatigue
in Patients With Chronic Hepatitis C Virus Infection. Clin Gastroenterol Hepatol. 2016
Jan;14(1):156-64.e3.
23. Villani R, Facciorusso A, Bellanti F, Tamborra R, Piscazzi A, Landriscina M, et al. DAAs
Rapidly Reduce Inflammation but Increase Serum VEGF Level: A Rationale for Tumor Risk
during Anti-HCV Treatment. PLoS One. 2016 Dec 20;11(12):e0167934.
24. Younossi ZM, Stepanova M, Henry L, Nader F, Hunt S. An In-Depth Analysis of Patient-
Reported Outcomes in Patients With Chronic Hepatitis C Treated With Different Anti-Viral
Regimens. Am J Gastroenterol. 2016 Jun;111(6):808-16.
25. Younossi ZM, Stepanova M, Nader F, Lam B, Hunt S. The patient's journey with chronic
hepatitis C from interferon plus ribavirin to interferon- and ribavirin-free regimens: a study of
health-related quality of life. Aliment Pharmacol Ther. 2015 Aug;42(3):286-95.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
Table 1. Baseline clinico-demographic characteristics of subjects.
Baseline non-viremic
Baseline viremic p All
N 50 192 242 Age, years 48.0 ± 10.3 42.3 ± 10.1 0.0006 43.5 ± 10.4 Male gender 40 (80.0%) 123 (64.1%) 0.0323 163 (67.4%) Race: white 27 (54.0%) 25 (13.0%) <0.0001 52 (21.5%) Race: black 1 (2.0%) 9 (4.7%) 0.39 10 (4.1%) Race: Asian 22 (44.0%) 155 (80.7%) <0.0001 177 (73.1%) Country: Canada 7 (14.0%) 23 (12.0%) 0.70 30 (12.4%) Country: Italy 27 (54.0%) 32 (16.7%) <0.0001 59 (24.4%) Country: South Korea 5 (10.0%) 51 (26.6%) 0.0134 56 (23.1%) Country: USA 6 (12.0%) 43 (22.4%) 0.10 49 (20.2%) Country: other 0 (0.0%) 43 (22.4%) 0.0002 43 (17.8%) Employed at baseline 37 (74.0%) 192 (100.0%) <0.0001 229 (94.6%) History of anxiety 3 (6.0%) 4 (2.1%) 0.14 7 (2.9%) History of depression 1 (2.0%) 7 (3.6%) 0.56 8 (3.3%) History of clinically overt fatigue
1 (2.0%) 2 (1.0%) 0.59 3 (1.2%)
History of sleep disorders 1 (2.0%) 8 (4.2%) 0.47 9 (3.7%) History of type 2 diabetes 2 (4.0%) 12 (6.3%) 0.54 14 (5.8%) BMI, kg/m2 24.7 ± 4.2 24.6 ± 4.8 0.68 24.6 ± 4.7 Duration of HBV-positivity, years
22.4 ± 11.8 8.6 ± 8.3 <0.0001 11.4 ± 10.7
Baseline HBV DNA, log10 IU/mL
1.28 ± 0.00 5.81 ± 1.82 <0.0001 4.87 ± 2.4
HBV e antibody 37 (74.0%) 118 (100.0%) <0.0001 155 (92.3%) HBV e antigen 10 (20.0%) 75 (39.1%) 0.0119 85 (35.1%) HBV surface antigen, log10 IU/mL
3.09 ± 0.55 3.59 ± 0.80 <0.0001 3.49 ± 0.78
ALT, U/L 25.1 ± 21.2 54.5 ± 63.7 <0.0001 48.4 ± 58.7 AST, U/L 23.0 ± 9.9 36.5 ± 30.7 <0.0001 33.7 ± 28.2 Platelets, 103/uL 191.1 ± 45.7 210.3 ± 50.2 0.0118 206.3 ± 49.8 Total bilirubin, mg/dL 0.64 ± 0.26 0.59 ± 0.25 0.22 0.60 ± 0.25 Albumin, g/dL 4.40 ± 0.27 4.48 ± 0.26 0.08 4.46 ± 0.26 Alkaline phosphatase, U/L 67.5 ± 14.2 66.1 ± 20.2 0.20 66.4 ± 19.1 Fibrotest score 0.405 ± 0.194 0.267 ± 0.190 <0.0001 0.295 ± 0.199

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
FIGURE LEGENDS
Figure 1. Baseline PROs in HBV patients with and without viremia. The exact numbers are
included in Supplementary Table 1.
Figure 2. Independent association of HBV viremia with baseline PROs in HBV patients
(adjusted for clinico-demographic confounders). The complete list of baseline PRO predictors is
included in Supplementary Table 2.
Figure 3. Treatment-emergent PRO changes from the baseline level (mean w/95% CI) in
patients with HBV who had (responders) and did not have (non-responders) their HBV viremia
decreased by at least -2.7 log10 IU/mL by (A) week 24, (B) week 48. Similar changes in patients
with baseline viremia only are shown in Supplementary Figure 3.
Figure 4. Mean PROs in patient with HBV who had (responders) and did not have (non-
responders) their HBV viremia decreased by at least -2.7 log10 IU/mL. Dashed horizontal lines
represent projections of the mean baseline levels.
Figure 5. Independent association of a change in HBV viremia (beta per a 1 log10 IU/mL
decrease from the baseline level) with treatment-emergent PRO changes (adjusted for the PRO
baseline levels and other clinico-demographic PRO predictors).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
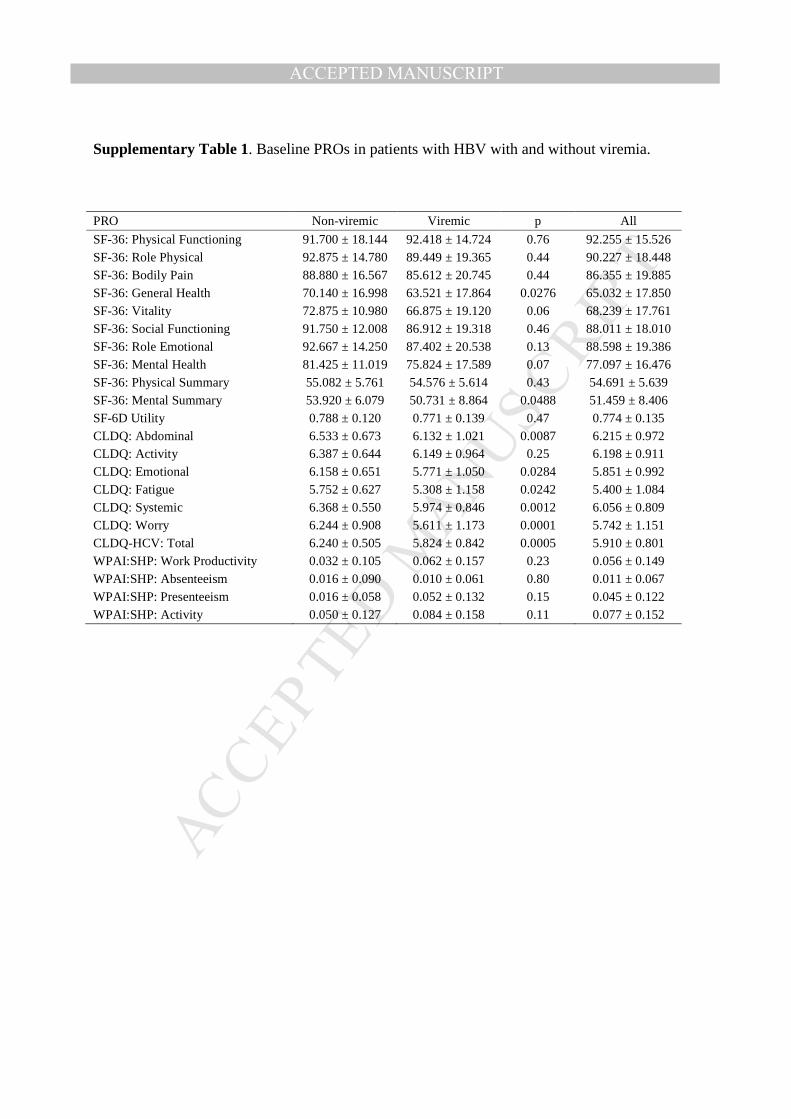
Supplementary Table 1. Baseline PROs in patients with HBV with and without viremia.
PRO Non-viremic Viremic p All
SF-36: Physical Functioning 91.700 ± 18.144 92.418 ± 14.724 0.76 92.255 ± 15.526 SF-36: Role Physical 92.875 ± 14.780 89.449 ± 19.365 0.44 90.227 ± 18.448 SF-36: Bodily Pain 88.880 ± 16.567 85.612 ± 20.745 0.44 86.355 ± 19.885 SF-36: General Health 70.140 ± 16.998 63.521 ± 17.864 0.0276 65.032 ± 17.850 SF-36: Vitality 72.875 ± 10.980 66.875 ± 19.120 0.06 68.239 ± 17.761 SF-36: Social Functioning 91.750 ± 12.008 86.912 ± 19.318 0.46 88.011 ± 18.010 SF-36: Role Emotional 92.667 ± 14.250 87.402 ± 20.538 0.13 88.598 ± 19.386 SF-36: Mental Health 81.425 ± 11.019 75.824 ± 17.589 0.07 77.097 ± 16.476 SF-36: Physical Summary 55.082 ± 5.761 54.576 ± 5.614 0.43 54.691 ± 5.639 SF-36: Mental Summary 53.920 ± 6.079 50.731 ± 8.864 0.0488 51.459 ± 8.406 SF-6D Utility 0.788 ± 0.120 0.771 ± 0.139 0.47 0.774 ± 0.135 CLDQ: Abdominal 6.533 ± 0.673 6.132 ± 1.021 0.0087 6.215 ± 0.972 CLDQ: Activity 6.387 ± 0.644 6.149 ± 0.964 0.25 6.198 ± 0.911 CLDQ: Emotional 6.158 ± 0.651 5.771 ± 1.050 0.0284 5.851 ± 0.992 CLDQ: Fatigue 5.752 ± 0.627 5.308 ± 1.158 0.0242 5.400 ± 1.084 CLDQ: Systemic 6.368 ± 0.550 5.974 ± 0.846 0.0012 6.056 ± 0.809 CLDQ: Worry 6.244 ± 0.908 5.611 ± 1.173 0.0001 5.742 ± 1.151 CLDQ-HCV: Total 6.240 ± 0.505 5.824 ± 0.842 0.0005 5.910 ± 0.801 WPAI:SHP: Work Productivity 0.032 ± 0.105 0.062 ± 0.157 0.23 0.056 ± 0.149 WPAI:SHP: Absenteeism 0.016 ± 0.090 0.010 ± 0.061 0.80 0.011 ± 0.067 WPAI:SHP: Presenteeism 0.016 ± 0.058 0.052 ± 0.132 0.15 0.045 ± 0.122 WPAI:SHP: Activity 0.050 ± 0.127 0.084 ± 0.158 0.11 0.077 ± 0.152

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary Table 2. Independent predictors of baseline PROs in patients with HBV
(viremia included regardless of significance, other predictors only with p<0.05 after stepwise
selection).
Outcome Variable Beta Std.Err. p
SF-36: Physical Functioning
Non-viremic -3.976 2.630 0.1321 Country: Italy 6.613 2.463 0.0078 Male gender 5.654 2.217 0.0114
SF-36: Role Physical
Non-viremic 1.930 2.876 0.5028 Male gender 6.143 2.567 0.0176 Black race -11.695 5.721 0.0421 Depression -21.775 6.357 0.0007 Fatigue -25.624 12.525 0.0420
SF-36: Bodily Pain Non-viremic 3.268 3.199 0.3080
SF-36: General Health
Non-viremic 0.826 2.853 0.7725 Country: Italy 9.358 3.001 0.0021 Country: South Korea -8.669 2.921 0.0033 Country: USA 7.092 3.471 0.0423 Male gender 6.350 2.465 0.0107 BMI, per kg/m2 -0.604 0.239 0.0121
SF-36: Vitality
Non-viremic 1.594 2.832 0.5742 Country: Italy 9.809 2.730 0.0004 Country: USA 10.139 3.233 0.0020 Male gender 9.909 2.386 0.0000 Fatigue -24.231 11.637 0.0385
SF-36: Social Functioning
Non-viremic 4.494 2.853 0.1167 Depression -16.268 6.387 0.0116
SF-36: Role Emotional
Non-viremic 3.603 3.024 0.2348 Male gender 7.237 2.705 0.0080 Depression -22.161 6.714 0.0011
SF-36: Mental Health
Non-viremic 4.235 2.547 0.0978 Male gender 6.684 2.354 0.0049 BMI, per kg/m2 -0.468 0.236 0.0486 Depression -16.439 5.866 0.0055
SF-36: Physical Summary
Non-viremic -1.111 0.940 0.2383 Country: Italy 3.617 0.887 0.0001 Male gender 2.150 0.812 0.0087 BMI, per kg/m2 -0.166 0.079 0.0362
SF-36: Mental Summary
Non-viremic 2.380 1.295 0.0674 Male gender 3.596 1.158 0.0022 Depression -9.779 2.872 0.0008
SF-6D Utility Non-viremic 0.005 0.021 0.8062 Male gender 0.059 0.019 0.0022 Depression -0.138 0.047 0.0037

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
CLDQ: Abdominal Symptoms
Non-viremic 0.339 0.152 0.0268 Male gender 0.287 0.132 0.0302 Black race -0.607 0.307 0.0495
CLDQ: Activity Non-viremic 0.180 0.142 0.2087 Male gender 0.277 0.123 0.0257 Depression -0.830 0.320 0.0102
CLDQ: Emotional
Non-viremic 0.354 0.162 0.0297 Country: Italy 0.697 0.220 0.0018 Male gender 0.300 0.133 0.0247 Asian 0.799 0.212 0.0002 Insomnia -0.826 0.327 0.0121
CLDQ: Fatigue
Non-viremic 0.224 0.177 0.2083 Country: Italy 0.458 0.166 0.0061 Male gender 0.409 0.143 0.0047 Fatigue -1.687 0.599 0.0053
CLDQ: Systemic Non-viremic 0.383 0.125 0.0025 Depression -0.646 0.283 0.0236
CLDQ: Worry Non-viremic 0.608 0.177 0.0007 Black race -0.915 0.360 0.0116
CLDQ: Total Non-viremic 0.369 0.124 0.0032 Male gender 0.230 0.107 0.0324 Depression -0.621 0.278 0.0266
WPAI:SHP: Work Productivity
Non-viremic -0.016 0.030 0.6031 Country: Italy -0.059 0.029 0.0465
WPAI:SHP: Activity
Non-viremic -0.013 0.024 0.5766 Country: South Korea 0.061 0.023 0.0087 Male gender -0.061 0.021 0.0032

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary Table 3. Correlations (non-parametric) of changes in HBV DNA and ALT with
changes in PROs from the baseline levels (weeks 12, 24, and 48 merged).
HBV DNA change ALT change R p R p SF-36: Physical Functioning 0.011 0.78 0.030 0.45 SF-36: Role Physical 0.011 0.78 -0.016 0.69 SF-36: Bodily Pain 0.043 0.28 0.085 0.03 SF-36: General Health -0.152 0.0001 -0.135 0.0006 SF-36: Vitality -0.040 0.32 -0.050 0.21 SF-36: Social Functioning 0.000 1.00 -0.004 0.92 SF-36: Role Emotional -0.060 0.13 -0.033 0.41 SF-36: Mental Health -0.106 0.0074 -0.069 0.08 SF-36: Physical Summary 0.009 0.82 0.024 0.55 SF-36: Mental Summary -0.122 0.0021 -0.095 0.0169 SF-6D Utility -0.033 0.42 -0.011 0.79 CLDQ: Abdominal -0.115 0.0023 -0.076 0.0449 CLDQ: Activity 0.027 0.48 0.000 1.00 CLDQ: Emotional -0.083 0.0274 -0.010 0.80 CLDQ: Fatigue -0.032 0.39 -0.028 0.45 CLDQ: Systemic -0.039 0.30 -0.045 0.24 CLDQ: Worry -0.163 <.0001 -0.099 0.0087 CLDQ-HCV: Total -0.098 0.0092 -0.073 0.05 WPAI:SHP: Work Productivity -0.130 0.0060 0.007 0.88 WPAI:SHP: Absenteeism -0.090 0.06 -0.052 0.28 WPAI:SHP: Presenteeism -0.089 0.06 0.007 0.89 WPAI:SHP: Activity 0.017 0.66 0.083 0.03

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary Figure 1. Mean treatment-emergent PRO changes from the baseline levels in
patients with HBV treated with (A) OAV+vesatolimod vs. OAV+placebo; (B) TDF+vesatolimod
vs. TDF+placebo.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary Figure 2. Selection of the optimal cut-off for a change in (A) HBV viremia and
(B) ALT; the changes by week 12, 24, and 48 are merged together.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Supplementary Figure 3. Treatment-emergent PRO changes from the baseline level (mean
w/95% CI) in patients with HBV with baseline viremia who had (responders) and did not have
(non-responders) their HBV viremia decreased by at least -2.7 log10 IU/mL by (A) week 24, (B)
week 48.